scottish patient safety programme highlight report · scottish patient safety programme highlight...
TRANSCRIPT
SCOTTISH PATIENT SAFETY PROGRAMME HIGHLIGHT REPORT
Clinical Governance Group or Subject
Scottish Patient Safety Programme (SPSP)
Executive Clinical Lead
Dr Alison Graham
Author:
Diane Campbell
Date
March and April 2011
Reporting Period (please click on appropriate box) March and April 2011
√
GENERAL COMMENT: NHS Lanarkshire continues to make good progress with the Scottish Patient Safety Programme (SPSP). SPSP HIGH LEVEL AIMS AHO2: % unadjusted inpatient mortality – target: reduction by 15% The Scottish Patient Safety Programme has monitored unadjusted mortality since the onset of the programme; this is unadjusted and demonstrates variation. However, ISD is now producing HSMR on a quarterly basis. which is influenced by a wide variety of factors such as age and diagnosis of patients HSMR Data One of the overall outcome measures of the SPSP is to demonstrate reduction in HSMR for each Board against its own HSMR baseline from November 2007. The latest quarterly data demonstrates the following reduction from the baseline period in relation to Hospital Standardised Mortality. Data source: From December 2009 Information Services Division (ISD) The baseline quarters are those from October 2006 to September 2007. The data used was linked SMR01 – Acute inpatient and day case records and GRO death records. The outcome of interest was mortality within 30 days from admission.
• Hairmyres -6.6% • Monklands -10.7% • Wishaw -11.7%
Overall average (mean) reduction in HSMR for NHS Lanarkshire is -9.6% Next Steps The first meeting of the mortality review group has been undertaken and work agreed to include three main reviews: the first to track all emergency patients admitted to Hairmyres Hospital for a 30 day period to identify deaths and undertake ‘real’ time reviews. The second will be to review existing HSMR data to identify unexpected deaths and undertake case note reviews. From this work, it will be intended that we identify issues and themes and develop plans to address these. The third will be work in relation to sepsis and visits to other areas of ‘best practice’ will be undertaken, with consideration also being given to a sepsis assessment tool as part of our EWS. Early work has begun to progress. AHO3: Adverse event rate – target: reduction by 30%. Improve patient safety by reducing unnecessary harm by 30% for NHS Lanarkshire by 31 March 2013 (from a baseline of November 2007) Twenty case notes are reviewed monthly from each acute site and assessed against the Global Trigger Tool, which is a tool to review for adverse events against the main elements of the programme. Adverse event rates continue to demonstrate random variation against target. However, there are general improvements noted, with the most obvious in Early Warning Score compliance.
SCOTTISH PATIENT SAFETY PROGRAMME HIGHLIGHT REPORT
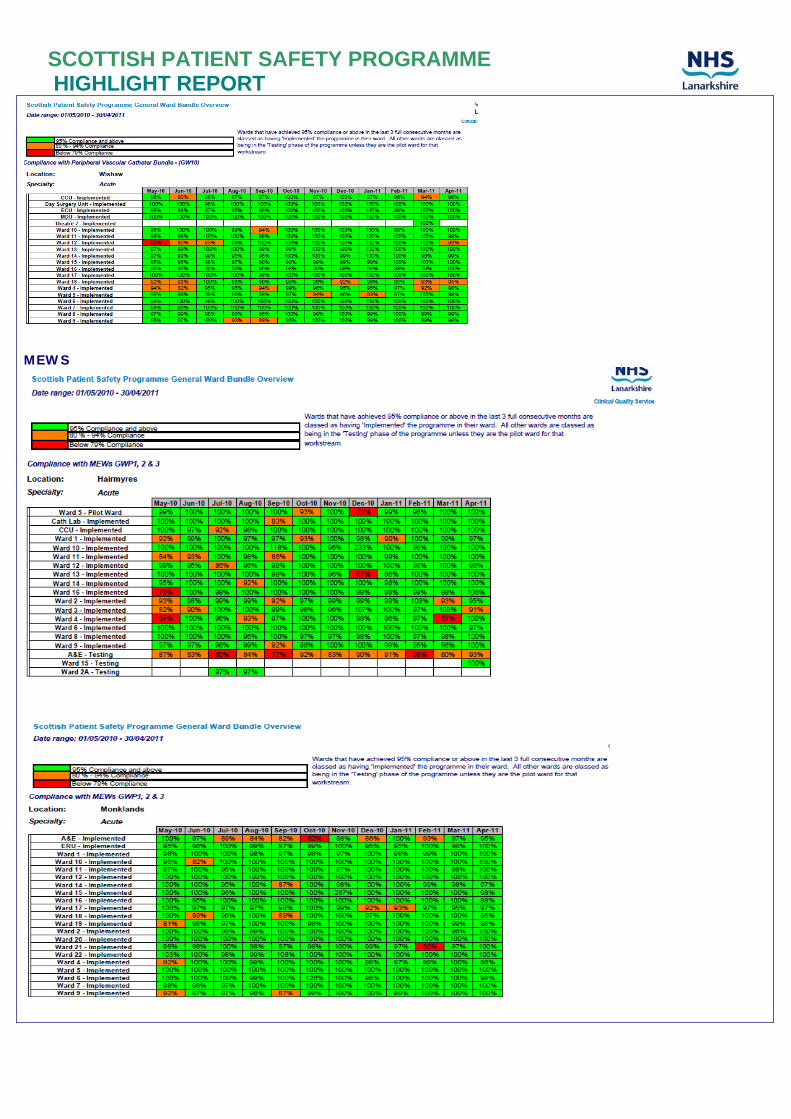
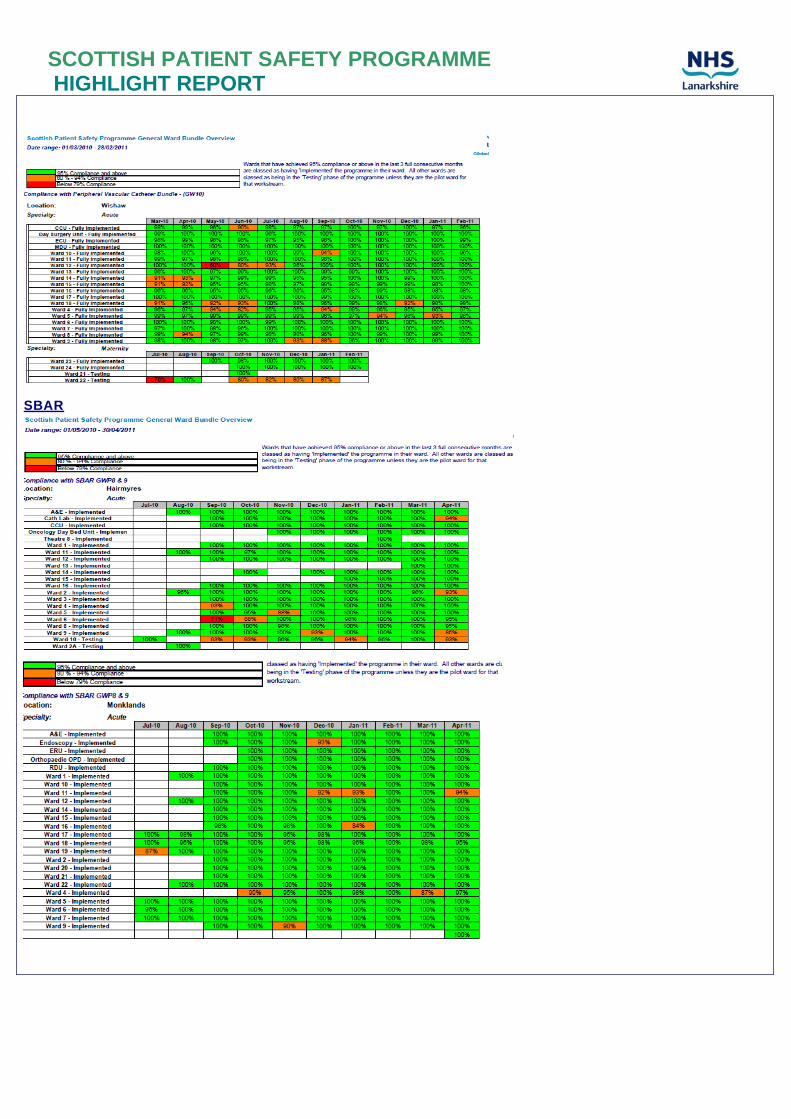
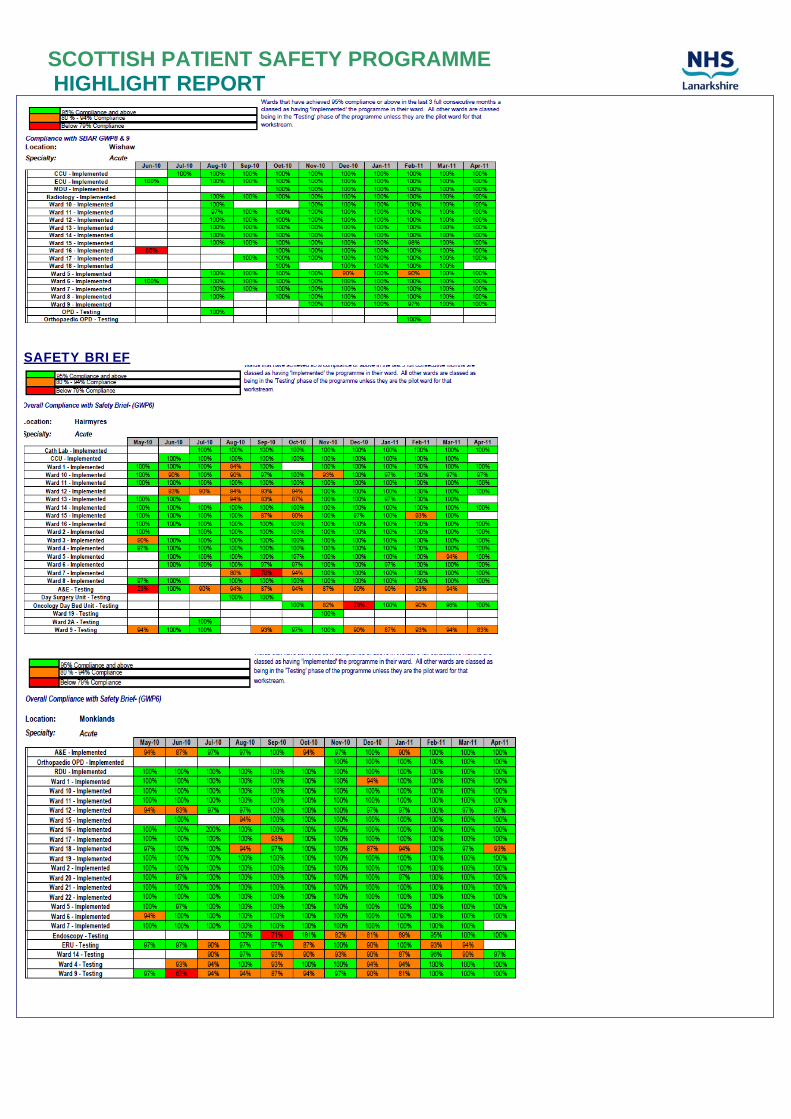
CRITICAL CARE: All green, except Multidisciplinary rounds which is amber / green (depending on site). Some excellent outcomes are being achieved. CCP1 / CCP2: % Compliance with Ventilator Associated Pneumonia (VAP) Bundle: Compliance at goal in all units. Variation remains with ALOS on mechanical ventilation – all sites. Reintubation rates low and fairly stable. CCO1:Ventilator Pneumonia Rate: Nil at Wishaw since August 2009, Hairmyres since December 2009 with isolated recent VAPs at Monklands CCP3: % Compliance with Central Line Insertion Bundle and Central Venous Catheter Maintenance Bundle: All at target for insertion bundle. All units at target with maintenance bundle. CCO2: Central line bloodstream infections: Nil at Hairmyres since November 2008, nil at Monklands since September 2009 and nil at Wishaw since March 2010. CCO6: Glucose Control: In place across all three critical care areas. All units at goal of >95% compliance CCP4: Hand Hygiene: At goal in all three critical care units. CCO8:C.difficle associated disease rate: Nil at Monklands since July 2010 with periodic individual cases at the other two sites over recent months CCP5: % Achievement of multidisciplinary rounds: Making excellent progress at Monklands and Wishaw with both at goal. CCP6: Daily Goals: Daily goals sheet in place in all three areas and compliance good. CCP8: Peripheral Vascular Cannula: All at goal. CCO4: SABs per 1000 AOBDS: Nil SABs at Hairmyres since July 2010, nil at Monklands since August 2010 and nil at Wishaw since October 2010. CCB1: ALOS: Reduced at Wishaw since programme onset General Wards: All green: Excellent progress with all measures and spread throughout all general wards and most associated hospitals (latter as relevant) GWP1: Early Warning Scoring System (EWS): GWP2: % time respiratory rate recorded: GWP3:% appropriate interventions: Compliance remains excellent and this is also seen at casenote reviews. GWO1: Crash call rate: Crash calls rates reducing below baseline levels, especially Monklands, some variation at other two sites. GWP10: % compliance with hand hygiene: At target in the three sites and maternity. Spread to all associated hospitals GWO4 C. difficle associated disease rate: excellent results. GWP6: %compliance with Safety Briefings: All acute sites at target. Being used as a main vehicle for the review of run charts and actions as well as other core questions and topics. Also being used to distribute theme of the week. GWP4: Rapid Response: Hospital Emergency Care Teams (HECT) in Place. Number of calls reducing variation at Wishaw where there has been a recent rise (although not to baseline level). Overall reduction may be in response to earlier identification of deteriorating patient (MEWS scoring). GWP8: SBAR (reporting): All at target. Reporting % trained challenging as SBAR is now incorporated into
Work stream Elements and Progress: Blue – Completed Green – On target Amber – Delayed, but expected to recover in-year Red – Delayed, not expected to recover in-year
Process measure compliance target - ALL measures 95%
SCOTTISH PATIENT SAFETY PROGRAMME HIGHLIGHT REPORT
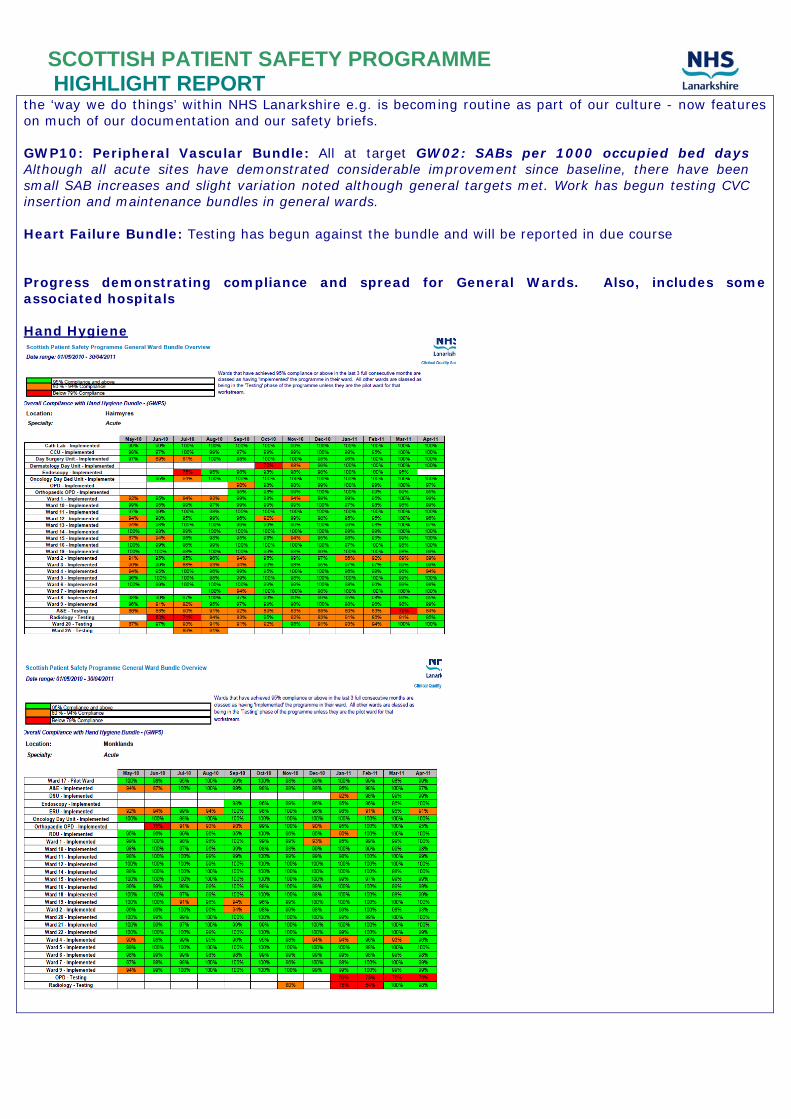
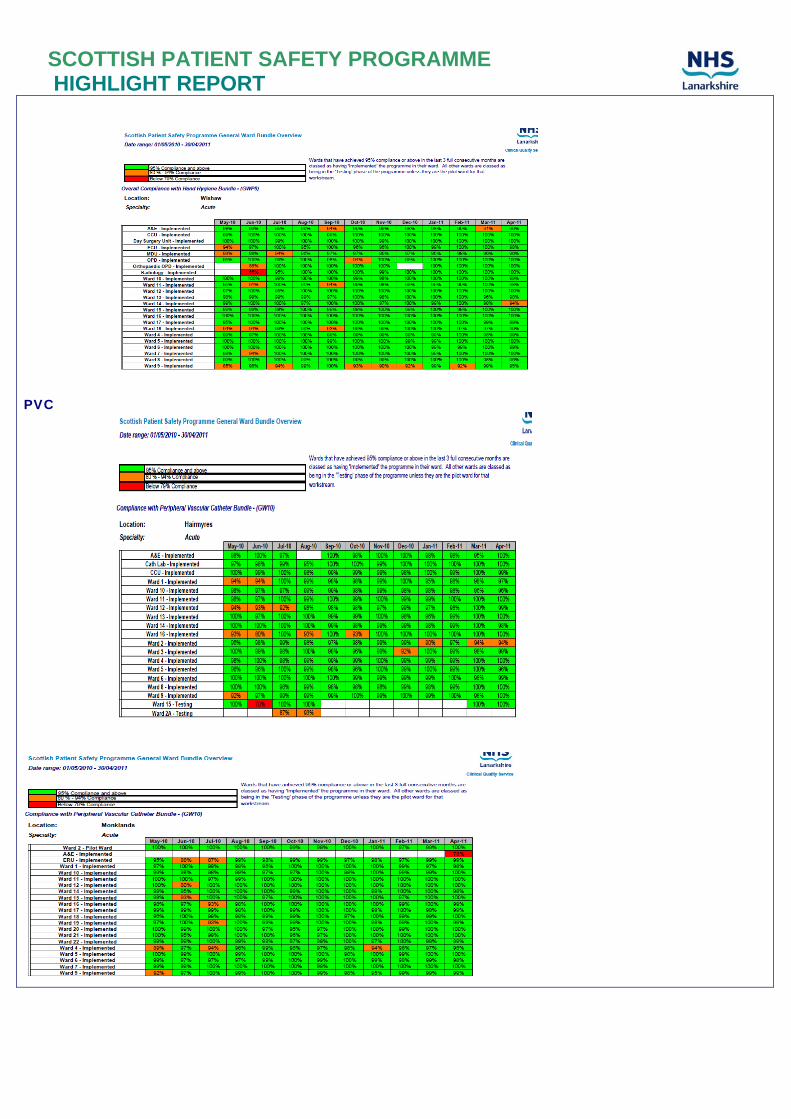
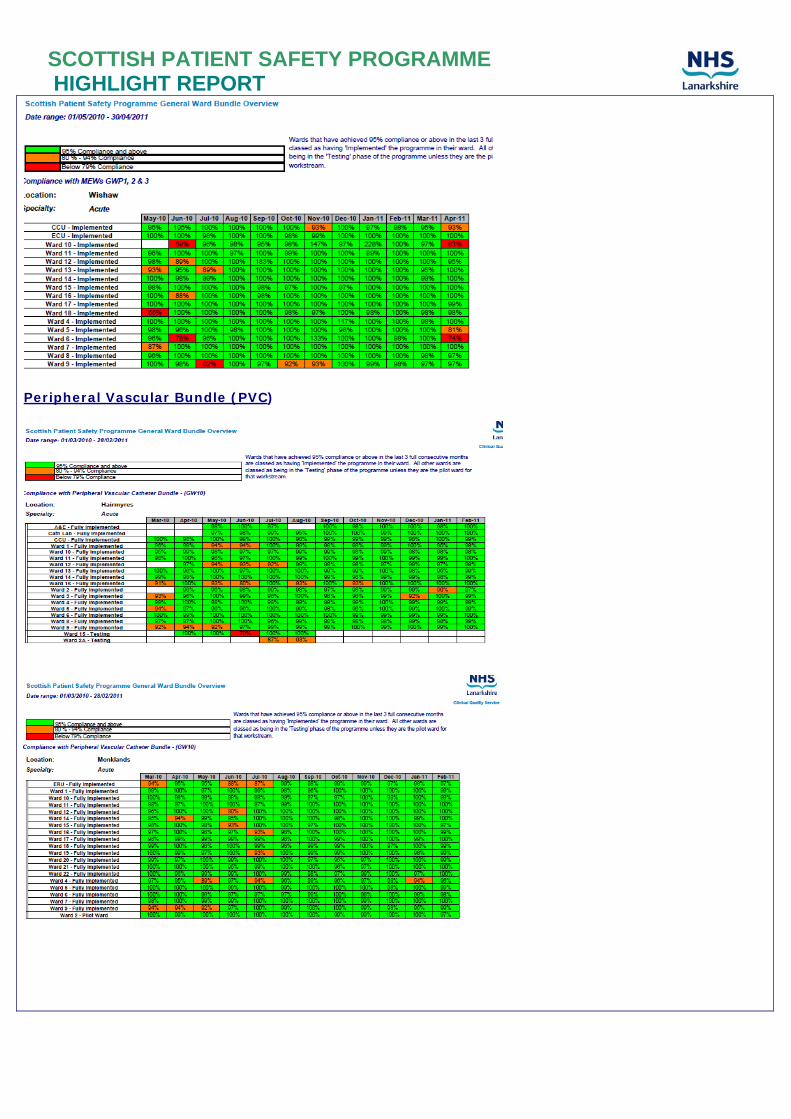
the ‘way we do things’ within NHS Lanarkshire e.g. is becoming routine as part of our culture - now features on much of our documentation and our safety briefs. GWP10: Peripheral Vascular Bundle: All at target GW02: SABs per 1000 occupied bed days Although all acute sites have demonstrated considerable improvement since baseline, there have been small SAB increases and slight variation noted although general targets met. Work has begun testing CVC insertion and maintenance bundles in general wards. Heart Failure Bundle: Testing has begun against the bundle and will be reported in due course Progress demonstrating compliance and spread for General Wards. Also, includes some associated hospitals Hand Hygiene
SCOTTISH PATIENT SAFETY PROGRAMME HIGHLIGHT REPORT
PVC
SCOTTISH PATIENT SAFETY PROGRAMME HIGHLIGHT REPORT
MEWS
SCOTTISH PATIENT SAFETY PROGRAMME HIGHLIGHT REPORT
Peripheral Vascular Bundle (PVC)
SCOTTISH PATIENT SAFETY PROGRAMME HIGHLIGHT REPORT
SBAR
SCOTTISH PATIENT SAFETY PROGRAMME HIGHLIGHT REPORT
SAFETY BRIEF
SCOTTISH PATIENT SAFETY PROGRAMME HIGHLIGHT REPORT
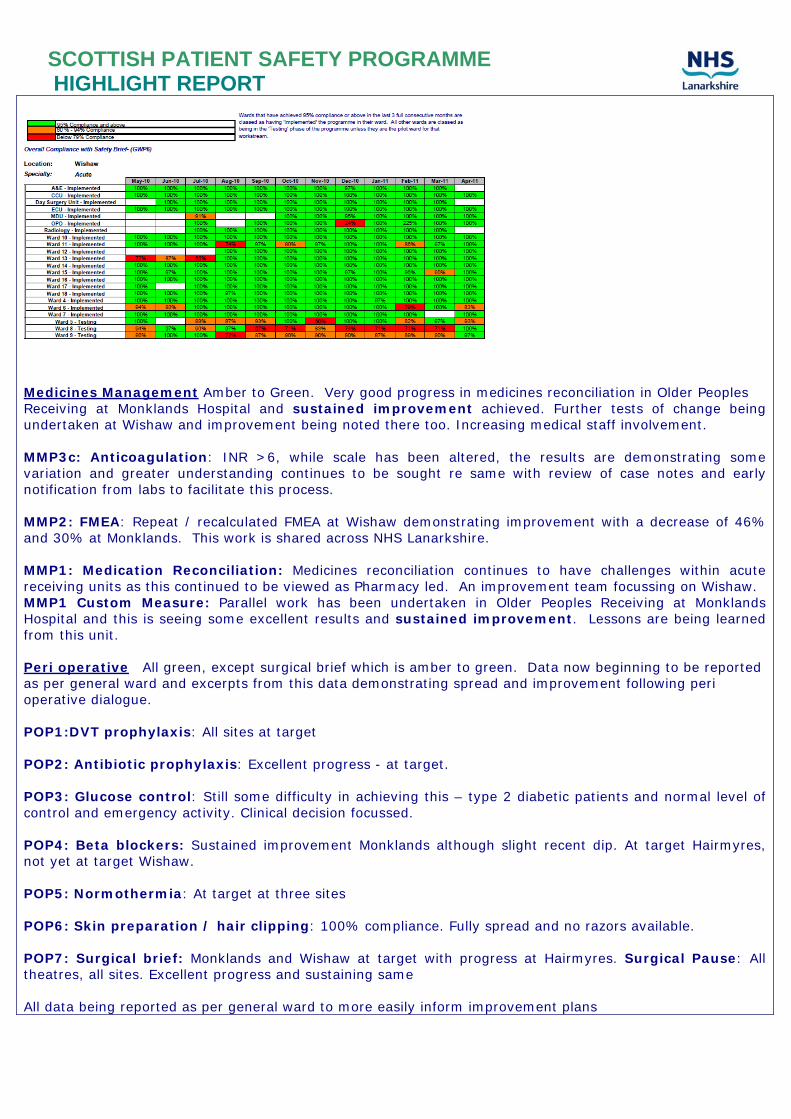
Medicines Management Amber to Green. Very good progress in medicines reconciliation in Older Peoples Receiving at Monklands Hospital and sustained improvement achieved. Further tests of change being undertaken at Wishaw and improvement being noted there too. Increasing medical staff involvement. MMP3c: Anticoagulation: INR >6, while scale has been altered, the results are demonstrating some variation and greater understanding continues to be sought re same with review of case notes and early notification from labs to facilitate this process. MMP2: FMEA: Repeat / recalculated FMEA at Wishaw demonstrating improvement with a decrease of 46% and 30% at Monklands. This work is shared across NHS Lanarkshire. MMP1: Medication Reconciliation: Medicines reconciliation continues to have challenges within acute receiving units as this continued to be viewed as Pharmacy led. An improvement team focussing on Wishaw. MMP1 Custom Measure: Parallel work has been undertaken in Older Peoples Receiving at Monklands Hospital and this is seeing some excellent results and sustained improvement. Lessons are being learned from this unit. Peri operative All green, except surgical brief which is amber to green. Data now beginning to be reported as per general ward and excerpts from this data demonstrating spread and improvement following peri operative dialogue. POP1:DVT prophylaxis: All sites at target POP2: Antibiotic prophylaxis: Excellent progress - at target. POP3: Glucose control: Still some difficulty in achieving this – type 2 diabetic patients and normal level of control and emergency activity. Clinical decision focussed. POP4: Beta blockers: Sustained improvement Monklands although slight recent dip. At target Hairmyres, not yet at target Wishaw. POP5: Normothermia: At target at three sites POP6: Skin preparation / hair clipping: 100% compliance. Fully spread and no razors available. POP7: Surgical brief: Monklands and Wishaw at target with progress at Hairmyres. Surgical Pause: All theatres, all sites. Excellent progress and sustaining same All data being reported as per general ward to more easily inform improvement plans
SCOTTISH PATIENT SAFETY PROGRAMME HIGHLIGHT REPORT
Walkrounds: Forty nine executive leadership walk rounds have been undertaken to date. Excellent representation from Executive and Non Executive Directors. Walk rounds scheduled at two per month for next calendar year. Emerging themes remain HAI, storage, clinical environment and small equipment issues. Data is entered to demonstrate actions completed on an ongoing basis now. New system in place to track % of actionable items resolved and Extranet updated. Very good relationships with PSSD to resolve Estates issues. Quarterly Leadership work stream meetings are scheduled to enable direction to be given to the work streams and practice to be shared as relevant Paedriatic Initial work has begun and making good progress. Of note is the EWS are being posted outside bedded area which acts as an alert to all staff if necessary. Heart Failure Initial work has begun and this will be reported in due course Relevant Bundle Spread This well underway in associated hospitals and mental health to include safety brief and SBAR. Efforts are being made to firmly align with other quality measures such as food fluid and nutrition, pressure area care, etc. Data Management We have now obtained funding from the Scottish Government eHealth Department to enable us to further develop our data management system: Lanarkshire Quality Improvement Portal (LanQIP), which brings together all of our quality measure via a web based portal. Along with other support funding, this enables us to appoint three system developers to further develop and ‘roll out’ to most of the other NHS Scotland Boards who have indicated interest. Comments on variations from plan (where exists):
• No variation from plan.
• Funding secured for one year for SPSP Clinical Facilitators to ensure spread capability and capacity as this programme moves outwith acute hospitals.
• Funding achieved centrally to spread our data management system – Lanarkshire Quality
Improvement Portal (LanQIP) to interested NHS Boards who have requested this system. Actions planned for the next 6 months:
• Begin reporting Paediatric Work stream progress
• Begin reporting Heart Failure bundle progress
Develop capacity within areas not yet participating in SPSP. Improvement teams (SPSP, Leading Better care, Better Together, HAI) to visiting areas such as attached hospitals to continue spread and improve monitoring for all NHS Lanarkshire Hospitals
Refine Spread plan as per above
Develop reporting system further to have in place as per general ward
Continue review of data to target improvement
Complete LanQIP and begin to spread this to other interested NHS Boards.