screening in the patient’s medical home
TRANSCRIPT

SCREENINGIN THE
PATIENT’S MEDICAL HOMEMirella Chiodo, Lee Green, Sudha Koppula
Faculty/Presenter Disclosure
• Faculty/Presenter: Sudha Koppula and Mirella Chiodo• Relationships with commercial interests: Grants/Research Support: Not applicable Speakers Bureau/Honoraria: Not applicable Consulting Fees: Not applicable Other: This presentation received support from the Alberta
College of Family Physicians.
• Faculty/Presenter: Lee Green• Relationships with commercial interests: Grants/Research Support: Not applicable Speakers Bureau/Honoraria: Not applicable Consulting Fees: Not applicable Other: This presentation received support from the Alberta
College of Family Physicians in the form of a speaker fee.

INTRODUCTIONS
• Who are we?• Who are you?
– Where are you from?– Who already does screening in their practice?– Thinking about it?

Outline
• The Patient’s Medical Home
• Improvement Model (Clinical Care)
• Screening in the Patient’s Medical Home
– Department of Family Medicine, University of Alberta Academic Centres (Success story!)
– Example of one such clinic

THE PATIENT’S MEDICAL HOME

©The College of Family Physicians of Canada 2011 All rights reserved.
THE PATIENT’S MEDICAL HOME
• What is your understanding of this model?• Three key elements
– Team-based care– Systems-based care– Access
• What is the importance of screening, especially within this model?
• Alberta perspective• If we don’t do this, who will?

IMPROVEMENT MODEL(CLINICAL CARE)

Outcomes
Process
Identification
Clinical Care Improvement Methodology

10
The Model for Improvement
Source: Langley, Gerald; Kevin Nolan; Thomas Nolan; Cliff Norman; and Lloyd Provost; “The Improvement Guide” Second Edition San Francisco, CA; Jossey-Bass, 2009
What are we trying to accomplish?How will we know a change is an
improvement?What change can we make that will
result in improvement?
Act Plan
Study Do

SCREENING INTHE PATIENT’S MEDICAL HOME
Department of Family MedicineUniversity of Alberta Academic Centres
Success story!

Identification• Primary Provider assigned• Active panel– seen in the past 36 months• Verified panel– Reception asks• What are we trying to accomplish?
1. Panel clean up. (Accurate patient registries.)2. Verified panel.3. Who is at risk? Those not coming in regularly?4. What are we trying to accomplish? What is our Aim?

Process• How do we engage patients?• Who’s job is it anyway?• How is it done?
1. Agree on preventive screening guidelines to follow.
2. Build rules into the EMR based on guidelines to automate process
3. Proactive versus opportunistic?4. Who is responsible? For updating
goal page, for management of goal page.
5. Preventative screening only versus addition of Chronic Disease Management maneuvers.
6. Map process.7. Consider current documentation.
How should we be documenting in the future.
8. Standardize as much as possible.9. How will we know we are improving?


EMR Tools – Goals Page

EMR Tools –CDS Triggers

Outcomes• Has this process made a difference?• How do we know we’ve improved?• Are we achieving our AIM?
1. Measured baseline. Measure yearly.2. Patient perspective.3. Physician and team perspectives.4. TOP ASaP audits vs. panel reports.5. Review guidelines regularly.
Measurement Tools
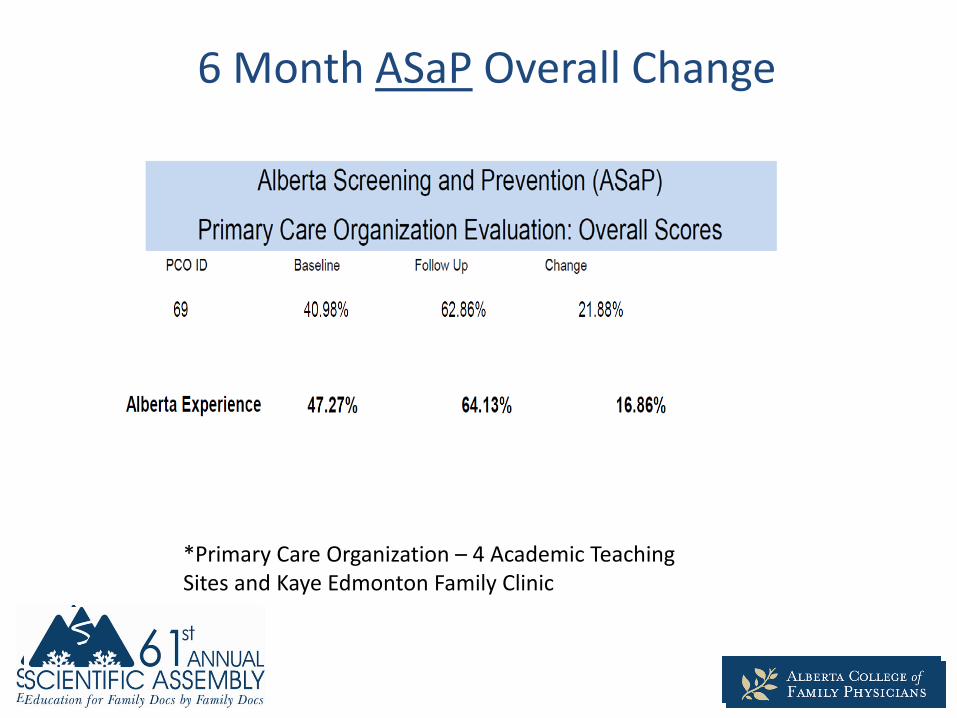
6 Month ASaP Overall Change
*Primary Care Organization – 4 Academic Teaching Sites and Kaye Edmonton Family Clinic

Individual Maneuver ChangeManeuver Baseline 6 month Change
Alcohol Screening
17.78% 50.56% 32.78%
Blood Pressure 72.78% 81.39% 8.61%
Colorectal 48.32% 70.73% 22.41%
CV Risk 10.06% 41.18% 31.12%
Diabetes 82.38% 76.50% -5.88%
Exercise 20.00% 62.22% 42.22%
Flu 5.83% 43.06% 37.22%
Height and Weight
40.83% 58.89% 18.06%
Lipids 79.89% 75.40% -4.49%
Mammogram 61.84% 75.31% 13.47%
Pap 64.36% 74.19% 9.84%
Tobacco 38.06% 64.72% 26.67%

Accountability Metrics

Accountability Metrics (Cont’d)

SCREENING INTHE PATIENT’S MEDICAL HOME
An Example

OUR CLINIC WORKFLOW – An example
• MD group agreed on population screening (by age and sex)
• Used ASaP guidelines (facilitated by QC)• Recommendations from Chronic Disease Management
(CDM) nurse
• Automated goals page for each patient created based on above, can be edited at the patient level
MD work vs Teamwork
System for Tracking/EMR
Use

OUR CLINIC WORKFLOW (cont’d)• Initially:
– Screening Coordinator reviews patient chart
– Screening Coordinator tasks MD with recommendations for each patient.
(Uses info from EMR chart and Netcare to do this.)• what screening is up to date/not• when next screen is due• if population screening applies or doesn’t
– MD reviews each task (one for each patient)Enabled individualization, thenTasks Screening Coordinator back.TOOK TIME!
– Care plan created, reqs prepared
– Screening Coordinator screens (i.e. creates care package) per MD choice:
• Birthdays – outreach but no discussion prior to providing reqs, or• Opportunistic – no outreach but discussion prior to providing reqs
System for Tracking/EMR
Use
Outreach vs Opportunistic
Screening

OUR CLINIC WORKFLOW (cont’d)
• Now:– Screening Coordinator reviews chart
Individualizes based on info (on EMR chart and Netcare)
– Tasks MD with questions/clarification onlyTAKES MUCH LESS TIME!
– Care plan created, reqs prepared
– Screening Coordinator screens (i.e. creates care package) per MD Choice
• Birthdays – outreach but no discussion prior to providing reqs, or• Opportunistic – no outreach but discussion prior to providing reqs
System for Tracking/EMR
Use
Outreach vs Opportunistic
Screening

SO … WHAT DO YOU THINK?
• How would this workflow go over in your setting?
• How does your workplace decide:- MD work vs teamwork?- System for tracking/EMR use?- Outreach vs Opportunistic screening?

THINK … PAIR … SHARE!
• THINK about screening in your setting
• PAIR up with your neighbour
• SHARE among whole group

Lessons Learned
• Patient-centered approach• Consensus on screening and process is difficult• Documentation MUST be standardized• Don’t get lost in PERFECT – (Process, measures)• Not necessarily doctor work
KEY POINTS:
– MD work vs teamwork– System for tracking/EMR use– Outreach vs Opportunistic screening

ANY QUESTIONS?

THANKS FOR JOINING US
Mirella ChiodoQuality and Informatics SupervisorDepartment of Family Medicine, University of [email protected]
Sudha KoppulaFamily PhysicianDepartment of Family Medicine, University of [email protected]