screening, prevention and treatment of viral hepatitis b
TRANSCRIPT

Screening, prevention and treatment of viral hepatitis Breactivation in patients with haematological malignancies
Gadi Lalazar,1 Deborah Rund2 and Daniel Shouval1
1Liver Unit, Departments of Medicine and 2Department of Haematology, Hadassah-Hebrew University Hospital, Jerusalem, Israel
Summary
The prevalence of hepatitis B virus (HBV) infection in patients
with haematological malignancies is increased compared with
the general population worldwide. HBV reactivation is com-
mon following chemotherapy and is associated with a high
mortality despite prompt anti-viral treatment. HBV reactiva-
tion may necessitate interruption of chemotherapy with
adverse prognostic consequences for the haematological dis-
ease. Chemotherapy-induced immune suppression may lead to
increased HBV replication. Immune reconstitution within the
weeks and months following recovery from chemotherapy may
be associated with a flare of hepatitis B manifested by
hepatocellular injury. Risk factors associated with HBV
reactivation include detectable hepatitis B surface antigen
(HBsAg), HBV DNA, Hepatitis B e (HBeAg) antigen,
antibodies to hepatitis B core antigen (anti-HBc), treatment
with corticosteroids, young age and male gender. Lamivudine
is effective during HBV reactivation due to immune suppres-
sion. Clinical trials have demonstrated that pre-emptive
antiviral treatment with lamivudine is superior to deferred
treatment. Current recommendations emphasise screening for
HBV infection in all haematology patients, particularly prior to
chemotherapy. Patients who are HBsAg positive or HBV DNA
positive should receive pre-emptive treatment with lamivudine
before chemotherapy. The duration of lamivudine treatment
may be prolonged commensurate with the degree of immu-
nosuppression. HBV naıve patients should be immunised
against hepatitis B, as should haematopoietic stem cell donors.
In summary, overt and occult HBV pose a serious, but
preventable, threat. Pre-treatment screening of patients at risk
should be practiced diligently by all clinicians that treat
patients with malignancies.
Keywords: immune suppression, leukaemia, lymphoma, anti-
viral treatment, haematopoietic stem cell transplantation.
Approximately 2 billion people worldwide have been
infected with hepatitis B virus (HBV) during their lifetime,
with >350 million remaining chronically infected (Lavanchy,
2004). The prevalence of chronic HBV infection, as deter-
mined by hepatitis B surface antigen (HBsAg) testing, ranges
between 8% and 25% in endemic countries (East Asia and
Africa) to <0Æ5% in the native populations of the Western
hemisphere (Lok et al, 1987; Lavanchy, 2004). The prevalence
of HBsAg in haemato-oncological patients is increased but
proportional to that reported in the general population: 1%
in the USA, 3Æ5% in Western Europe, 5% in Turkey and
10% in Asian Chinese (Lau et al, 1999; Takai et al, 2005).
Chronic HBV carriers, defined as persons with positive
HBsAg for >6 months, have a 15–40% lifetime risk of
developing serious complications of chronic liver disease
(including chronic hepatitis, cirrhosis and hepatocellular
carcinoma) (McMahon, 2005). Most carriers, however,
remain clinically silent for extended periods, lasting from
decades to a lifetime. Some carriers will lose HBsAg over
time but remain positive for antibodies to hepatitis B core
antigen (anti-HBc), with low levels of HBV-DNA, reflecting
occult infection.
Patients with haematological malignancies deserve special
attention regarding their hepatitis B status for several reasons.
First, in endemic countries, the incidence of HBV reactivation
is increased in this group compared with normal subjects
(Takai et al, 2005; Yim & Lok, 2006). Yet, overt and occult
HBV infections are often missed at a stage when pre-emptive
anti-viral treatment may prevent HBV reactivation. Secondly,
HBV reactivation is a common sequella of chemotherapy
occurring in 21–53% of HBsAg carriers (Yeo et al, 2000), and
when left undetected, may carry a grave prognosis despite
therapy. Thirdly, even when full recovery is achieved, reacti-
vation may reduce survival because it may require interruption
of chemotherapy.
During the past decade, new diagnostic tools and efficacious
anti-viral agents have been developed mainly for hepatitis B
but also for hepatitis C. This review discusses the clinical
presentation, diagnosis, treatment and prevention of HBV
reactivation in haemato-oncological patients.
Correspondence: Prof. Daniel Shouval, Director, Liver Unit, Hadassah-
Hebrew University Hospital, PO Box 12000, Jerusalem 91120, Israel.
E-mail: [email protected]
review
ª 2007 The Authors First published online 8 January 2007Journal Compilation ª 2007 Blackwell Publishing Ltd, British Journal of Haematology, 136, 699–712 doi:10.1111/j.1365-2141.2006.06465.x

The ‘natural’ course of hepatitis B virus infectionas relevant to patients with a haematologicalmalignancy
The evolution of chronic HBV infection often depends on the
age at infection and is affected by the balance between the host
immune response and viral replication. Vertical or perinatal
transmission of HBV frequently results in immune tolerance to
the virus. Infection during adulthood induces a neutralising
immune response in over 90% of immunocompetent individ-
uals, with spontaneous resolution of acute infection (McMa-
hon, 2005; Yim & Lok, 2006). In this case, immune memory,
comprising T helper cell type 1 (Th1) responses to nucleo-
capsid epitopes and antibodies to HBsAg (anti-HBs), persist
for decades and generally prevent reinfection (Chisari, 1997;
Bertoletti & Gehring, 2006). Patients who are unable to resolve
an acute infection have an altered natural course of HBV
infection, consisting of four phases: immune tolerance with
enhanced viral replication; immune clearance characterised by
the initial presence of hepatitis B e antigen (HBeAg) and
variable viral load; inactive carrier state frequently associated
with antibodies to HBeAg (anti-HBe) seroconversion with low
viral replication, and HBV reactivation (Yim & Lok, 2006).
Reactivation of HBV infection may occur in a known
asymptomatic HBsAg carrier or in patients with occult or
rarely with resolved hepatitis B. HBV reactivation, either
spontaneous or following chemotherapy, can resolve, persist,
recur or lead to liver failure and death (Fig 1). Such flares have
been attributed to changes in equilibrium due to an enhanced
immunological response to HBV during recovery from
immune suppression, associated with quantitative variations
in viral load. Serological recovery from HBV infection (defined
as anti-HBs antibody titre >10 IU/l, also termed resolved
HBV) usually signifies clearance of viraemia and complete
resolution of hepatocellular injury. However, even after
serological recovery, HBV may persist as an occult infection
in serum, in the liver (with intra-hepatic covalently closed
circular DNA, termed cccDNA) or in extra-hepatic sites, with
resulting risk of reactivation (Yim & Lok, 2006). This is
especially true during recovery from immunosuppression or
disease-associated immunodeficiency (Puoti et al, 2006).
Immune suppression allows enhanced viral replication with
increased viral load and reduced clearance. Immune reconsti-
tution may then lead to a vigorous host-derived inflammatory
response towards HBV, with concomitant hepatic necrosis
(Liaw, 1998).
Risk factors
Patients at risk are those with haematological malignancies (or
solid malignant tumours) who are candidates for chemother-
apy but also patients with non-malignant diseases, such as
immune thrombocytopenic purpura (ITP) or autoimmune
haemolytic anaemia, which require continuous immunosup-
pressive therapy. Most haemato-oncological patients should be
considered at risk either for HBV reactivation or acute
acquired HBV infection. Increased risk is due to increased
exposure to potentially contaminated blood products (despite
conventional screening) as well as disease- and treatment-
related factors (Yeo & Johnson, 2006).
Haemato-oncological diseases reported in association with
HBV reactivation are listed in Table I.
Studies on the clinical significance of HBV genotypes
indicate that genotypes may correlate with key clinical events
(Kao et al, 2000). Although data are scarce, the incidence of
HBV reactivation seems to correlate with distinct HBV
genotypes C and B, prevalent in East Asia, and the East
Mediterranean (Lok & Lai, 1990; Lok et al, 1991; Jazayeri et al,
2004).
Several specific risk factors for HBV reactivation have been
proposed, but few were confirmed in multivariate analysis. In
studies of 78 patients (Yeo et al, 2000, 2004a), univariate
analysis identified an increased risk in younger males who
had HBsAg positive/HBeAg positive lymphoma, while there
was no association with pre-treatment alanine amino trans-
Fig 1. Dynamics of viral load and alanine amino transferase (ALT)
during the course of hepatitis B virus (HBV) reactivation following
chemotherapy-induced immune suppression. Adapted from Xunrong
et al (2001). �John Wiley & Sons Limited with permission.
Table I. Haematological diseases reported in association with hepatitis
B virus reactivation
Group Disease
Acute leukaemia Acute myeloid leukaemia
Acute lymphoblastic leukaemia
Myeloproliferative
disorders
Chronic myeloid leukaemia
Lymphoproliferative
disorders
Chronic lymphocytic leukaemia
Non-Hodgkin lymphoma
Hodgkin disease
Plasma cell dyscrasias Multiple myeloma
Waldenstrom macroglobulinaemia
Plasmacytoma
Other Aplastic anaemia
Myelodysplastic syndrome
Haematopoietic stem cell transplantation
Review
ª 2007 The Authors700 Journal Compilation ª 2007 Blackwell Publishing Ltd, British Journal of Haematology, 136, 699–712

ferase (ALT), bilirubin or HBV DNA. In contrast, in a study
of patients with hepatocellular carcinoma and underlying
liver disease, pre-treatment ALT elevation was shown to be a
risk factor for HBV reactivation (Yeo et al, 2004b). In a study
of 100 patients, male sex was the only risk factor (Lok et al,
1991). In contrast, a study of 137 autologous haematopoietic
cell transplantation (HCT) patients found that pre-immune
suppression HBV DNA level >105 copies/ml was the only
significant risk factor (Lau et al, 2002a). This was also
observed in 138 cancer patients for whom HBV viral load
>3 · 105 copies/ml was a risk factor for reactivation (Yeo
et al, 2004a). Zhong et al (2004) and Hui et al (2005a)
confirmed that high titre viral DNA levels increase the risk of
HBV reactivation.
Different chemotherapeutic agents have been reported in
association with HBV reactivation (Table II), most import-
antly, corticosteroids and anthracyclines (Lok et al, 1991;
Cheng et al, 2003; Yeo & Johnson, 2006). The HBV DNA
contains a glucocorticoid responsive element that facilitates
replication (Tur-Kaspa et al, 1986), while anthracyclines have
been shown in vitro to stimulate HBV DNA secretion (Hsu
et al, 2004). Most important, corticosteroids may also induce a
flare, particularly upon abrupt withdrawal of treatment.
‘Steroid free’ chemotherapy has been proposed to minimise
the risk of HBV reactivation (Lok et al, 1992; Nakamura et al,
1996), but is of dubious benefit. In a prospective study of 50
patients with aggressive non-Hodgkin lymphoma (NHL) (75%
diffuse large B-cell NHL in both the steroid-free and the
steroid-inclusive arms), the use of ‘steroid-free’ chemotherapy
resulted in a significant decrease in the rate of HBV reactiva-
tion (73% vs. 38%, P ¼ 0Æ03). However, patients in the
‘steroid-free’ arm had a significantly lower rate of complete
remission and shorter overall survival, presumably due to
suboptimal therapy (Cheng et al, 2003).
Theoretically, any form of immune suppression, including
agents not mentioned in Table II, may lead to HBV reactiva-
tion. Standard chemotherapy has frequently been documented
to cause HBV reactivation in HBsAg negative patients with
occult HBV infection (Lok et al, 1991; Hui et al, 2006).
Immune suppression of greater intensity may be a risk factor.
One study found the incidence of HBV reactivation increased
with second or third line chemotherapy (Kumagai et al, 1997),
but this was not subsequently confirmed (Yeo et al, 2000).
In contrast, mildly immune suppressive chemotherapy, such as
Table II. Chemotherapeutic and immune modulating agents involved in hepatitis B virus reactivation and their potential for hepatotoxicity*.
Class Agents associated with HBV reactivation Potential hepatotoxicity
Alkylators Cyclophosphamide VOD, hepatocellular injury
Ifosfamide Hepatocellular injury, cholestasis
Chlorambucil Hepatocellular injury
Carboplatin, cisplatin hepatocellular injury, cholestasis, steatosis, peliosis
Antimetabolites Cytarabine VOD, hepatocellular injury
Fluorouraril Hepatocellular injury
Gemcitabine Hepatocellular injury, cholestasis
Mercaptopurine Hepatocellular injury, cholestasis
Methotrexate Hepatocellular injury, steatosis, fibrosis, hepatic neoplasm
Thioguanine VOD, hepatocellular injury, NRH, peliosis
Antitumor antibiotics Anthracyclines Hepatocellular injury, VOD
Bleomycin Steatosis
Mitomycin C VOD, steatosis
Actinomycin D VOD, steatosis
Corticosteroides Prednisone/dexamethasone etc. hepatomegaly (rare association)
Immunotherapy Rituximab (anti-CD20) Hepatocellular injury
Alemtuzumab (anti-CD52) Hepatocellular injury
Infliximab (anti-TNF) Hepatocellular injury, steatosis
Plant Alkaloids Vincristine VOD, hepatocellular injury
Vinblastine Hepatocellular injury
Others Asparginase Hepatocellular injury, steatosis
Procarbazine VOD
Docetaxel Hepatocellular injury
Etoposide Hepatocellular injury
Fludarabine Hepatocellular injury
Imatinib Mesylate Hepatocellular injury, cholestasis
Interferon alpha Hepatocellular injury
*Only predominant forms of liver injury are cited for the purpose of differential diagnosis of abnormal liver function tests.
Modified from Yeo and Johnson (2006) with permission from John Wiley & Sons, Inc.�, and Bonkovsky et al (2006) with permission from Elsevier.
VOD, veno-occlusive disease; NRH, nodular regenerative hyperplasia.
Review
ª 2007 The AuthorsJournal Compilation ª 2007 Blackwell Publishing Ltd, British Journal of Haematology, 136, 699–712 701

5-fluorouracil, for colon cancer carried a lower risk (Liaw,
1998).
Allogeneic haematopoietic stem cell transplantation (HSCT)
frequently leads to reactivation (Chen et al, 1990, 1993; Martin
et al, 1995; Picardi et al, 1998; Strasser & McDonald, 1999;
Iwai et al, 2000; Nordbo et al, 2000; Goyama et al, 2002); the
rate of HBV reactivation varies between 14% and 50% (Chen
et al, 1990; Dhedin et al, 1998; Seth et al, 2002; Knoll et al,
2004; Onozawa et al, 2005). Suggested risk factors include
corticosteroid use, lack of anti-HBs in the donor, and graft
versus host disease (GVHD). Conversely, in autologous-HSCT,
there have been fewer reports (Webster et al, 1989; Goyama
et al, 2002). One case series showed that one of 37 patients
developed non-fulminant hepatitis B (Lau et al, 2002a).
Newer therapeutic monoclonal antibodies, such as Rituxim-
ab (anti-CD20) (Westhoff et al, 2003; Law et al, 2005; Niscola
et al, 2005; Sarrecchia et al, 2005), Alemtuzumab (anti-CD52)
(Iannitto et al, 2005) and infliximab (anti-TNF) (Calabrese
et al, 2006) have been associated with HBV reactivation in
HBsAg carriers as well as in HBsAg negative patients, which may
progress to fulminant hepatitis. These agents cause profound
and long-lasting immunosuppression (Osterburg et al, 1997;
van der Kolk et al, 2002), which may account for the risk of
HBV reactivation following treatment.
The patient’s HBV serological profile is linked to the risk of
HBV reactivation. HBsAg positive patients are at highest risk;
patients with anti-HBs levels >10 IU/l are at the lowest risk.
HBeAg positivity, previously considered to signify high level
viral replication, has been replaced by more sensitive viral load
assays (Locarnini, 2004) that have a threshold of detection of
as low as 300 copies/ml and a wide dynamic range (Gish &
Locarnini, 2006). HBV DNA assays are also useful in HBeAg
negative/anti-HBe positive patients in whom viraemia can still
be significant. Even in patients who have cleared HBsAg and
undergone seroconversion, residual HBV DNA, in the form of
cccDNA ‘hidden’ in hepatocytes, can be used as a template for
reactivation following immune suppression (Hui et al, 2005b).
Furthermore, HBV DNA has been found in peripheral blood
mononuclear cells recovered from immune suppressed trans-
planted patients with a serologic profile anti-HBc positive/
HBsAg negative/anti-HBs negative, in the absence of HBV
DNA in the serum (Mason et al, 1998; Locarnini, 2004).
A similar rule applies for patients following treatment for
HBV. Even with successful therapy, some patients remain at
lifelong risk for reactivation (Osborn & Lok, 2006). Therefore,
while anti-HBs positive patients are at low risk (Lok et al,
1991; Lau et al, 2002a; Knoll et al, 2004; Onozawa et al, 2005),
these patients are not absolutely protected against reactivation.
Subclinical changes in the immune profile of such patients may
lead to asymptomatic rise of ALT, which may progress to overt
disease. In a report of 17 patients with haematological
malignancies (Wands et al, 1975), 12 had a marked reduction
in their anti-HBs titre; five developed ‘seroreversion’, with
reappearance of HBsAg, and two remained persistently HBsAg
positive despite the cessation of chemotherapy. Others have
reported changes in the HBV serological profile following
chemotherapy (Iannitto et al, 2005; Avettand-Fenoel et al,
2006).
In summary, proven risk factors include: positive HBsAg
(especially when associated with high viral load), positive HBeAg,
positive anti-HBc in the absence of HBsAg and anti-HBs, use of
corticosteroids or anthracyclines, higher intensity chemotherapy
(suchasforHSCT),malegenderandyoungage.
Clinical manifestations and laboratory diagnosisof a hepatitis B flare in the immune suppressedpatient
Hepatitis B virus reactivation is characterised by two main
parameters: rising serum HBV DNA levels followed by rising
ALT. Monitoring of HBV DNA requires an available sensitive
assay with a wide dynamic range (Gish & Locarnini, 2006).
Reactivation may be symptomatic or remain asymptomatic.
Rising HBV DNA levels usually precede ALT elevation, which
frequently lags by several days (range 1–11 weeks) after an
increase in viral load (Lau et al, 2003). Furthermore, HBV
DNA levels may be declining or undetectable by the time a rise
in ALT is noticed (Xunrong et al, 2001; Yeo & Johnson, 2006)
(Fig 1). Therefore, there are no clear cut diagnostic criteria for
HBV reactivation. One proposed definition was a sudden rise
in serum ALT more than five times the upper limit of normal
or more than three times baseline level, whichever was higher
(Lok et al, 1987). Other definitions include a 10-fold rise in
viral load or HBV DNA levels exceeding approximately
6 log10 copies/ml (Yeo et al, 2000). Essentially, measuring
viral load (Gish & Locarnini, 2006) and ALT are the key to
diagnosing and monitoring reactivation. A liver biopsy,
although usually not imperative, can potentially yield im-
portant information, by excluding other or concomitant
factors involved in liver injury. It may also reveal a potentially
wide spectrum of histological changes associated with HBV
infection. If present, coagulopathy or thrombocytopenia may
necessitate a transjugular approach.
Reactivation most frequently follows cessation of che-
motherapy, but may occur during chemotherapy. The reported
interval ranges from 4 to 36 weeks (median, 16 weeks) from
initiation of chemotherapy (Liang et al, 1999; Lau et al, 2003).
An acute flare may also be induced by HBV genotypic
variations, such as precore or DNA polymerase mutants as well
as superinfection by other hepatotrophic viruses, such as
hepatitis D, hepatitis C and hepatitis A as well as cytomeg-
alovirus (CMV) and Epstein–Barr virus (EBV). Interaction
with HIV or hepatotoxicity of anti-HIV agents may also
contribute (Puoti et al, 2006). An acute flare may be indistin-
guishable from acute viral hepatitis B including the detection
of anti-HBc IgM, potentially leading to a misdiagnosis of acute
HBV infection in patients with previously undiagnosed
chronic disease. HBV-reactivation can easily be missed,
particularly in early stages, when salvage anti-viral therapy
could be life saving. Reactivation can also be associated with an
Review
ª 2007 The Authors702 Journal Compilation ª 2007 Blackwell Publishing Ltd, British Journal of Haematology, 136, 699–712

increase in alpha-feto-protein, raising concern about the
development of hepatocellular carcinoma (Lok & Lai, 1989).
Hepatitis B virus reactivation may resolve spontaneously.
Symptomatic patients may develop the classical symptoms of
hepatitis, including fatigue, jaundice, ascites, hepatic encepha-
lopathy and coagulopathy. Patients with underlying cirrhosis
may rapidly develop liver failure; their mortality ranges from
4% to 41% (Lok et al, 1991; Kumagai et al, 1997; Liang et al,
1999; Markovic et al, 1999; Tillman et al, 2003).
Since many patients are asymptomatic, regular monitoring
of ALT and HBV DNA is essential although there is no
consensus regarding frequency of testing. As reactivation may
be transient, more frequent HBV DNA and ALT monitoring
will lead to a higher rate of diagnosis.
Differential diagnosis of a hepatitis flare
Most hepatitis flares in patients with chronic HBV are of viral
aetiology. However, there are a number of other causes for
liver dysfunction including chemotherapy or other drug-
induced toxic hepatitis, veno-occlusive disease (VOD), pelio-
sis, hepatic steatosis, hepatic fibrosis and nodular regenerative
hyperplasia (NRH). Table II lists various types of chemother-
apy agents involved in HBV reactivation that may also induce
toxic hepatocellular or cholestatic dysfunction. Hepatotoxicity
of anti-cancer agents may frequently result from an interaction
between two or more agents. ALT elevation can also be caused
by bacterial, viral or fungal infection [i.e. sepsis, CMV, EBV,
herpes or human immunodeficiency virus (HIV)]. Super-
infection with other hepatitis viruses, i.e. delta virus (HDV)
infection in HBsAg carriers, hepatitis C or even hepatitis A can
cause as many as 20–30% of flares (Perrillo, 2001). HBV-
related fibrosing cholestatic hepatitis and GVHD are reported
to be more frequent in HBsAg carriers (Lau et al, 1999). Other
causes of hepatocellular or cholestatic injury should be
considered where appropriate, such as exposure to alcohol,
total parentral nutrition, acalculous cholecystitis, tumour
infiltration, or radiation toxicity. About 12% of ALT elevations
remain unexplained (Yeo et al, 2000).
Haemato-oncological patients previously treated for HBV
are at risk for developing resistance against the antiviral agent,
such as reported for lamivudine for which 16–60% of recipients
develop a mutation known as the YMDD motif within 1–
4 years of treatment, respectively (Locarnini, 2004; Osborn &
Lok, 2006; Wong & Lok, 2006). Hepatitis flares in such patients
with a high viral load despite lamivudine treatment, must
therefore be evaluated for this mutation, followed by optional
treatment with adefovir or entecavir (see below).
Hepatitis B reactivation: screening andprevention
Prevention of HBV reactivation is superior to intervention at
the time of reactivation. Preventive measures start with proper
screening for HBV markers before initiation of chemotherapy
followed by active immunisation of all HBV susceptible
patients (also including bone-marrow and stem cell donors).
Candidate patients with overt or occult HBV must be
identified and protected against HBV by an anti-viral agent.
Screening of haemato-oncological patients prior toinitiation of chemotherapy
All patients diagnosed with a haematological disease should be
screened for HBV infection. Initial screening is based on
serological tests for anti-HBc antibodies, HBsAg and anti-HBs
antibodies (see flow chart: Fig 2). Seronegative patients should
be actively vaccinated against HBV. HBsAg positive patients
are considered carriers and should be protected pre-emptively
against HBV reactivation by an anti-viral agent before
initiation of chemotherapy (see below). Frequently, the
diagnosis of an HBsAg carrier state cannot be verified at time
of initiation of chemotherapy, as it is based on 6 months’
observation. In such a situation, the presence of a positive
HBsAg test should be interpreted as representing an HBsAg
carrier state, provided there is no evidence for acute hepatitis B
which may result in delay of cytotoxic treatment. All HBsAg
positive patients should be further tested for HBeAg, anti-HBe,
HBV DNA and if possible, anti-HBc IgM. A liver biopsy may
be considered in patients with pre-chemotherapy abnormal
liver function tests, the result of which may have implications
on the selection and dosing of chemotherapy. HBsAg negative
patients who are anti-HBc positive, require further testing. A
positive anti-HBs test in this context signifies a patient who
recovered from HBV infection; while a negative anti-HBs test
may signify either occult HBV infection, recovery from
infection with a waning antibody titre or a false positive
anti-HBc result. Differentiation between these fundamentally
different states may be accomplished by repeating the
serological profile after administration of an HBV vaccine
booster dose to anti-HBc positive patients negative for HBsAg
and anti-HBs (Fig 2). A rise in the anti-HBs antibody titre
above 10 IU/l (and preferably >100 IU/l) within 2–4 weeks is a
result of an anamnestic immune response and signifies
immunity to HBV. In anti-HBc positive non-responders to
the HBV vaccine, HBV-DNA should be measured by a
sensitive polymerase chain reaction (PCR) assay. Detectable
HBV-DNA implies occult HBV infection which will require
pre-emptive antiviral therapy before initiation of chemother-
apy (Fig 2). Since a patient’s serological profile may change
during the course of chemotherapy (i.e. seroreversion from a
state of anti-HBs positivity to HBsAg positivity) it is advised to
perform serologic re-testing before the continuation of
chemotherapy in case ALT levels rise (Wands et al, 1975;
Chen et al, 1990; Dhedin et al, 1998; Seth et al, 2002; Knoll
et al, 2004; Onozawa et al, 2005). In cases where urgent
chemotherapy treatment is required this may be accomplished
by saving an adequate blood sample for serological analysis
prior to the institution of therapy and making a decision on
anti-viral treatment once results are available.
Review
ª 2007 The AuthorsJournal Compilation ª 2007 Blackwell Publishing Ltd, British Journal of Haematology, 136, 699–712 703

Immunisation against hepatitis B infection
The cornerstone of prevention for patients who are HBV
seronegative is immunisation. Currently available HBV vac-
cines are very safe and have an efficacy of >90% in immuno-
competent young individuals. Non-response is associated with
a number of factors including genetically determined resist-
ance, advanced age, obesity, chronic liver disease, smoking,
male gender and miscellaneous systemic diseases including
renal failure (Shouval, 2003; Yu et al, 2006). Although
universal vaccination of newborns has been implemented
worldwide according to World Health Organisation recom-
mendations, it will take several decades until the majority of
the world’s adult population will be immune. Unfortunately,
vaccination rates are low in many countries either due to lack
of funding or because of the misconception that vaccination is
only necessary in high-risk groups (Banatvala et al, 2006).
It is strongly recommended that all haemato-oncological
patients be screened for HBV markers and immunisation
against hepatitis B should be performed when appropriate (see
algorithm, Fig 2). The conventional regimen for the HBV
vaccine requires three doses at 0, 1 and 6 months. Delaying
administration of the third dose in healthy individuals (up to
1 year) may increase anti-HBs antibody levels. Frequently, in
haemato-oncological patients, urgent administration of che-
motherapy does not allow completion of the three-dose
regimen. In such cases, an effort should be made to immunise
patients with at least two doses within a 3–4 week interval. The
third dose can then be given a few months after chemotherapy
is completed.
In most countries, immunity against HBV infection is
defined as an anti-HBs titre >10 IU/l and in the UK the
recommended titre is >100 IU/l. Non-response to HBV
vaccines is not rare in haemato-oncological patients due to
disease-associated or treatment-induced immune suppression.
Thus, protection against HBV may not be achieved until all
doses have been administered. Although immune suppressed
patients have significantly lower response rates to vaccination,
successful anti-HBs seroconversion following a three dose
vaccine schedule has been reported in 57% of cancer patients,
15–68% of bone marrow transplant recipients, and in 10% in
acute lymphoblastic leukaemia (ALL) patients (Yu et al, 2006).
Documentation of post-vaccination anti-HBs seroconversion
is recommended. There are a number of means to augment the
immune response to HBV immunisation in non-responders,
including adding three additional doses; doubling the vaccine
dose; intradermal injection of the vaccine and use of new,
more immunogenic HBV vaccines (Shouval, 2003; Yu et al,
2006). Finally, after allogeneic HSCT, immunity to HBV
acquired through active immunisation may rarely be abolished
by immune suppression and/or transplantation of HBV naıve
bone marrow cells (Dhedin et al, 1998).
Fig 2. Guidelines for prevention of hepatitis B virus reactivation in haemato-oncologic patients: patients management according to status of hepatitis
B virus markers.
Review
ª 2007 The Authors704 Journal Compilation ª 2007 Blackwell Publishing Ltd, British Journal of Haematology, 136, 699–712

Agents for treatment of patients with occult or overtHBV infection
Recently, new and efficacious anti-viral agents have signifi-
cantly improved our ability to intervene in and prevent HBV
reactivation in immune suppressed patients (Osborn & Lok,
2006; Wong & Lok, 2006). Standard therapy currently consists
of lamivudine, a nucleoside analogue introduced in 1995,
which inhibits the viral DNA polymerase, thus rapidly and
effectively interfering with viral replication, with minimal
toxicity.
In addition, several new potent anti-viral agents been
developed and licensed for the treatment of chronic HBV,
including adefovir dipivoxil in 2002 (Osborn & Lok, 2006),
entecavir in 2005 (Chang et al, 2006; Lai et al, 2006) and
others are awaiting approval. Both adefovir and entecavir are
effective against YMDD mutants. While adefovir and lamivu-
dine seem to suppress hepatitis B viral load equally well,
entecavir is the currently most potent agent against HBV,
leading to a 5–6 log suppression in viral load in HBsAg/HBeAg
positive patients after 48 weeks of treatment with no HBV
resistant strains reported thus far. There have been a few
reports on the successful use of adefovir for HBV reactivation
by a YMDD mutant during lamivudine therapy in haemato-
oncological and immune suppressed patients (Nunez &
Soriano, 2005; Cortelezzi et al, 2006; Fouillard et al, 2006).
Interferon alpha, used for the treatment of chronic HBV, has
been shown to control chronic HBV infection during chemo-
therapy to a certain degree (Lok et al, 1992; Kumagai et al,
1997; Leaw et al, 2004; Osborn & Lok, 2006). However,
adverse effects, such as thrombocytopenia and or leucopenia,
often limit its use during chemotherapy. A more serious
concern is the enhancement of hepatocellular injury by
augmentation of the host immune response against HBV.
Thus, the use of interferon for an HBV flare has now been
practically discontinued.
Protection and management of immunesuppressed patients with overt or occult HBVagainst HBV reactivation
There are currently two approaches in management of patients
at risk, namely intervention by treatment of HBV reactivation
when it is diagnosed, or prevention through pre-emptive
treatment prior to or upon initiation of chemotherapy.
Intervention upon diagnosis of hepatitis B reactivation
When HBV reactivation is diagnosed, prompt anti-viral
therapy is vital. In patients who develop signs of HBV
reactivation, end points of treatment include normalisation of
ALT, suppression of HBV viral load to undetectable levels and
HBeAg seroconversion to anti-HBe. In anti-HBe positive
patients, ALT normalisation and viral load suppression are the
main goals of treatment. Aggressive supportive therapy should
be instituted and cessation of chemotherapy and withdrawal of
potential hepatotoxic agents should be considered. Patients
should be monitored, closely testing liver enzymes, coagulation
function and viral load. Consultation with an expert hepato-
logist or early referral to a hepatology centre should be
considered in patients with a severe course, although liver
transplantation may not be feasible in patients with a
malignancy.
Currently lamivudine is the primary agent for treatment for
HBV reactivation in the setting of immune suppression.
Several reports have shown clinical improvement and effective
control of viral replication (Clark et al, 1998; Picardi et al,
1998; Ahmed & Keeffe, 1999; Al-Taie et al, 1999; Vento et al,
2002). The true rate of HBV reactivation in immune
suppressed patients is not known and spontaneous resolution
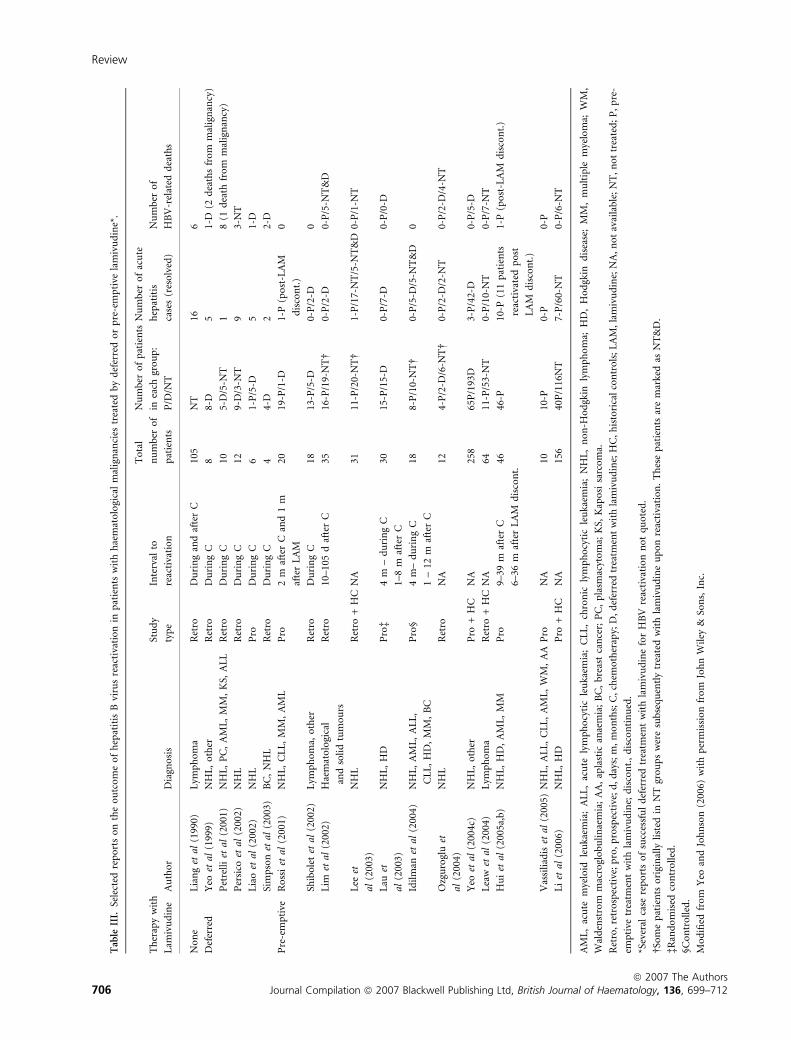
may occur (Table III). Thus, the reported efficacy rates of
antiviral treatment may be somewhat overestimated (Yeo &
Johnson, 2006). None of the studies reporting the success of
lamivudine for HBV reactivation in these patients is a truly
prospective, blinded, placebo controlled trial. Presently, it is
unlikely that such a study is ethically feasible. Despite this
caveat, there is no doubt that lamivudine is effective in
suppression of HBV replication and thus has dual importance,
as it may enable the continuation of chemotherapy without
risking further hepatic deterioration. Lamivudine is efficacious
for HBV reactivation but less so if hepatic decompensation has
occurred (ter Borg et al, 1998; Clark et al, 1998). Mortality
may be as high as 40% despite lamivudine (Markovic et al,
1999) if severe hepatic injury is present (Iwai et al, 2000; Yeo
et al, 2000; Yeo & Johnson, 2006). Thus, it is imperative to
begin antiviral therapy immediately once a flare is diagnosed.
As stated earlier, HBV DNA rises prior to ALT elevation
(Fig 1). Ideally, in cases where lamivudine is not administered
pre-emptively, viral load should be monitored periodically
during chemotherapy, although there is no consensus as to
how frequently. Once a rise in HBV DNA is identified, it is
strongly advised to immediately administer lamivudine, prior
to the appearance of clinical manifestations. However, this
recommendation is difficult to implement due to cost and the
time required for assessment of HBV DNA levels.
Pre-emptive anti-viral therapy against hepatitis Breactivation
Several reports have demonstrated the benefit of pre-emptive
treatment with lamivudine in patients at risk of HBV
reactivation. The rational for initiation of pre-emptive treat-
ment with lamivudine in patients at risk is based on
observations that viraemia, defined as HBV DNA >104 cop-
ies/ml, usually precedes ALT elevation by a day to several
months. Thus, early suppression of viral load prior to hepatic
injury is superior to deferred intervention. Reports on the
efficacy of pre-emptive treatment may be divided into
retrospective studies and prospective studies with historical
controls, listed in Table III. In 12 studies conducted in 208
Review
ª 2007 The AuthorsJournal Compilation ª 2007 Blackwell Publishing Ltd, British Journal of Haematology, 136, 699–712 705
Tab
leII
I.Se
lect
edre
po
rts
on
the
ou
tco
me
of
hep
atit
isB
viru
sre
acti
vati
on
inp
atie
nts
wit
hh
aem
ato
logi
cal
mal
ign
anci
estr
eate
db
yd
efer
red
or
pre
-em
pti
vela
miv
ud
ine*
.
Th
erap
yw
ith
Lam
ivu
din
eA
uth
or
Dia
gno
sis
Stu
dy
typ
e
Inte
rval
to
reac
tiva
tio
n
To
tal
nu
mb
ero
f
pat
ien
ts
Nu
mb
ero
fp
atie
nts
inea
chgr
ou
p:
P/D
/NT
Nu
mb
ero
fac
ute
hep
atit
is
case
s(r
eso
lved
)
Nu
mb
ero
f
HB
V-r
elat
edd
eath
s
No
ne
Lia
ng
etal
(199
0)L
ymp
ho
ma
Ret
roD
uri
ng
and
afte
rC
105
NT
166
Def
erre
dY
eoet
al(1
999)
NH
L,
oth
erR
etro
Du
rin
gC
88-
D5
1-D
(2d
eath
sfr
om
mal
ign
ancy
)
Pet
rell
iet
al(2
001)
NH
L,
PC
,A
ML
,M
M,
KS,
AL
LR
etro
Du
rin
gC
105-
D/5
-NT
18
(1d
eath
fro
mm
alig
nan
cy)
Per
sico
etal
(200
2)N
HL
Ret
roD
uri
ng
C12
9-D
/3-N
T9
3-N
T
Lia
oet
al(2
002)
NH
LP
roD
uri
ng
C6
1-P
/5-D
51-
D
Sim
pso
net
al(2
003)
BC
,N
HL
Ret
roD
uri
ng
C4
4-D
22-
D
Pre
-em
pti
veR
oss
iet
al(2
001)
NH
L,
CL
L,
MM
,A
ML
Pro
2m
afte
rC
and
1m
afte
rL
AM
2019
-P/1
-D1-
P(p
ost
-LA
M
dis
con
t.)
0
Shib
ole
tet
al(2
002)
Lym
ph
om
a,o
ther
Ret
roD
uri
ng
C18
13-P
/5-D
0-P
/2-D
0
Lim
etal
(200
2)H
aem
ato
logi
cal
and
soli
dtu
mo
urs
Ret
ro10
–105
daf
ter
C35
16-P
/19-
NT�
0-P
/2-D
0-P
/5-N
T&
D
Lee
et
al(2
003)
NH
LR
etro
+H
CN
A31
11-P
/20-
NT�
1-P
/17-
NT
/5-N
T&
D0-
P/1
-NT
Lau
et
al(2
003)
NH
L,
HD
Pro
�4
m–
du
rin
gC
1–8
maf
ter
C
3015
-P/1
5-D
0-P
/7-D
0-P
/0-D
Idil
man
etal
(200
4)N
HL
,A
ML
,A
LL
,
CL
L,
HD
,M
M,
BC
Pro
§4
m–
du
rin
gC
1–
12m
afte
rC
188-
P/1
0-N
T�
0-P
/5-D
/5-N
T&
D0
Ozg
uro
glu
et
al(2
004)
NH
LR
etro
NA
124-
P/2
-D/6
-NT�
0-P
/2-D
/2-N
T0-
P/2
-D/4
-NT
Yeo
etal
(200
4c)
NH
L,
oth
erP
ro+
HC
NA
258
65P
/193
D3-
P/4
2-D
0-P
/5-D
Lea
wet
al(2
004)
Lym
ph
om
aR
etro
+H
CN
A64
11-P
/53-
NT
0-P
/10-
NT
0-P
/7-N
T
Hu
iet
al(2
005a
,b)
NH
L,
HD
,A
ML
,M
MP
ro9–
39m
afte
rC
6–36
maf
ter
LA
Md
isco
nt.
4646
-P10
-P(1
1p
atie
nts
reac
tiva
ted
po
st
LA
Md
isco
nt.
)
1-P
(po
st-L
AM
dis
con
t.)
Vas
sili
adis
etal
(200
5)N
HL
,A
LL
,C
LL
,A
ML
,W
M,
AA
Pro
NA
1010
-P0-
P0-
P
Li
etal
(200
6)N
HL
,H
DP
ro+
HC
NA
156
40P
/116
NT
7-P
/60-
NT
0-P
/6-N
T
AM
L,
acu
tem
yelo
idle
uka
emia
;A
LL
,ac
ute
lym
ph
ocy
tic
leu
kaem
ia;
CL
L,
chro
nic
lym
ph
ocy
tic
leu
kaem
ia;
NH
L,
no
n-H
od
gkin
lym
ph
om
a;H
D,
Ho
dgk
ind
isea
se;
MM
,m
ult
iple
mye
lom
a;W
M,
Wal
den
stro
mm
acro
glo
bu
lin
aem
ia;
AA
,ap
last
ican
aem
ia;
BC
,b
reas
tca
nce
r;P
C,
pla
smac
yto
ma;
KS,
Kap
osi
sarc
om
a.
Ret
ro,
retr
osp
ecti
ve;
pro
,p
rosp
ecti
ve;
d,
day
s;m
,m
on
ths;
C,
chem
oth
erap
y;D
,d
efer
red
trea
tmen
tw
ith
lam
ivu
din
e;H
C,
his
tori
cal
con
tro
ls;
LA
M,
lam
ivu
din
e;N
A,
no
tav
aila
ble
;N
T,
no
ttr
eate
d;
P,
pre
-
emp
tive
trea
tmen
tw
ith
lam
ivu
din
e;d
isco
nt.
,d
isco
nti
nu
ed.
*Sev
eral
case
rep
ort
so
fsu
cces
sfu
ld
efer
red
trea
tmen
tw
ith
lam
ivu
din
efo
rH
BV
reac
tiva
tio
nn
ot
qu
ote
d.
�So
me
pat
ien
tso
rigi
nal
lyli
sted
inN
Tgr
ou
ps
wer
esu
bse
qu
entl
ytr
eate
dw
ith
lam
ivu
din
eu
po
nre
acti
vati
on
.T
hes
ep
atie
nts
are
mar
ked
asN
T&
D.
�Ran
do
mis
edco
ntr
oll
ed.
§Co
ntr
oll
ed.
Mo
difi
edfr
om
Yeo
and
Joh
nso
n(2
006)
wit
hp
erm
issi
on
fro
mJo
hn
Wil
ey&
Son
s,In
c.
Review
ª 2007 The Authors706 Journal Compilation ª 2007 Blackwell Publishing Ltd, British Journal of Haematology, 136, 699–712

patients at risk treated pre-emptively with lamivudine during
chemotherapy for various malignancies, HBV reactivation
could be reduced from 25–85% to 0–9%. Thus a large body of
clinical trials strongly supports pre-emptive therapy in patients
undergoing chemotherapy.
The optimal timing for beginning pre-emptive anti-viral
therapy has not been established and requires further study. It
is preferable to begin pre-emptive treatment 2–3 weeks prior
to chemotherapy, and we suggest no later than the first day of
chemotherapy.
The optimal duration of prophylactic anti-viral therapy in
patients at risk is unclear. Various studies have reported
lamivudine discontinuation within 1–12 months after cessa-
tion of chemotherapy (Hui et al, 2005a; Hsiao et al, 2006).
Premature discontinuation may lead to delayed HBV reacti-
vation, as shown in Fig 3. Re-treatment with lamivudine may
be successful, but delay in intervention may lead to serious
liver injury and may be life threatening (Dai et al, 2004). The
natural history of patients who stopped prophylactic therapy
has not been well-studied. Despite the absence of well
controlled trials we suggest that treatment be maintained for
at least 6 months and preferably 12 months after completion
of chemotherapy (Idilman, 2006). Extended treatment for
>12 months after chemotherapy may be advisable in patients
who initially had high serum HBV DNA levels, at the
discretion of the treating physician. More definitive recom-
mendations require a prospective controlled study.
Guidelines for screening, immunisation and pre-emptive
anti-viral treatment for patients at risk are suggested in Fig 2.
A potential concern related to the use of prophylactic
lamivudine is the development of resistant mutants. At
present, reports on lamivudine resistance in haemato-onco-
logical patients with HBV reactivation are scarce, probably
because of the relatively short duration of therapy. Newer and
more potent anti-viral agents described above will enable
effective protection despite the emergence of escape mutants.
Thus, in case of emergence of YMDD mutant-associated
hepatitis, adefovir or entecavir may be used for rescue.
It should, however, be remembered that HBV reactivation
may occur in up to 9% of patients at risk, despite pre-emptive
lamivudine treatment. The reason(s) for this breakthrough
phenomenon are still not understood.
Adoptive transfer of immunity to hepatitis Bthrough immunisation of haematopoietic celldonors
Candidates for allogeneic HSCT require special attention. They
are very poor responders to conventional vaccination against
hepatitis B. Such patients may benefit from the acquired
immune memory obtained through transplantation of HBV
immune lymphocytes from their human leucocyte antigen
(HLA) matched donors. The donors can be either immunised
against HBV or may be immune following natural HBV
infection with seroconversion (anti-HBc positive/anti-HBs
positive). Indeed, adoptive transfer of immunity to HBsAg
was shown to occur in HBV naıve bone marrow recipients and
in recipients of peripheral lymphocytes and stem-cells trans-
ferred from immunised anti-HBs positive donors (Shouval &
Ilan, 1995; Ilan et al, 2000). Immunity to HBsAg could be
boosted after transplantation by HBV vaccination. Studies in
various animals confirmed that immunity to HBV can be
adoptively transferred, even under conditions of immune
suppression (Shouval et al, 1993; Li et al, 2002; Dahmen et al,
2004).
A number of studies have provided further evidence that
immunisation of donors may induce HBV immunity in
recipients within several days to weeks of transplantation (Ilan
et al, 1993a; Lindemann et al, 2003; Shouval, 2007). Immuni-
sation of stem cell donors is simple, practically risk-free and
should be planned in advance, so that donors can be
adequately vaccinated prior to harvesting. Both donor and
recipient can then receive a booster vaccine. The optimal
timing and the number of booster doses required depends on
the immune status of the recipient and should be documented
by anti-HBs testing (Ilan et al, 1993a). Administration of the
third vaccine dose to the donor at 6 months should not be
forgotten after the primary immunisation to maximise anti-
HBs seroconversion if future cell donations are required. It is
not yet established if a booster dose is required in transplant
recipients from cell donors who had previously recovered
spontaneously from HBV infection and were anti-HBc posit-
ive/anti-HBs positive at time of donation. However, there is a
rational for administering a booster vaccine dose to such
recipients once they recover immunologically.
If an HBsAg positive patient requires haematopoietic call
transplantation (HCT) or HSCT, it may be possible to
adoptively transfer immunity to HBV by these procedures. A
number of observations suggest that this is possible. Clearance
of HBV was first documented in an HBsAg positive/anti-HBe
positive/HBV DNA positive chronic lymphocytic leukaemia
Fig 3. The effect of premature withdrawal of antiviral treatment on
hepatitis B viral load and alanine amino transferase (ALT) in a patient
with diffuse large B cell lymphoma treated pre-emptively with lami-
vudine. Reproduced from Dai et al (2004) with kind permission of
Springer Science and Business Media.
Review
ª 2007 The AuthorsJournal Compilation ª 2007 Blackwell Publishing Ltd, British Journal of Haematology, 136, 699–712 707

(CLL) patient who received a bone marrow transplant from his
anti-HBc positive/anti-HBs positive brother (Ilan et al, 1993b).
Lau et al (1997, 2002a) confirmed and extended this observa-
tion in HBsAg positive transplant recipients in whom HBV
clearance and anti-HBs seroconversion was achieved following
receipt of an HBV immune bone-marrow, without serious
adverse events. Furthermore, donor-derived core antigen
reactive T-cells were linked to the clearance of HBV in the
recipients (Lau et al, 1999, 2002b). The probability of iden-
tifying an HLA-matched HBV immune donor with an anti-
HBc positive/anti-HBs positive serological profile for an
HBsAg positive recipient is low, albeit not negligible, especially
in HBV endemic countries. Utilisation of such donors,
together with pre-emptive lamivudine treatment may therefore
be beneficial in patients with chronic HBV infection. Finally,
there already is a report suggesting anti-HBs seroconversion in
HBsAg negative patients transplanted with livers from HBV
immune donors (Shouval, 2007).
Summary of recommendations
(1) All patients who are candidates for immune suppressive
therapy should be screened for HBV markers.
(2) All HBV naıve patients, including potential bone marrow
and stem cell donors, should be immunised against HBV
as soon as possible with preferably three doses and no less
than two. The quantitative anti-HBs response should be
documented several weeks after the last injection. Non-
responders should receive another course of three injec-
tions, when possible.
(3) Early, pre-emptive anti-viral therapy is superior to inter-
vention at time of HBV reactivation. Patients who are
HBsAg positive should be evaluated for presence of liver
disease and receive pre-emptive treatment with lamivu-
dine at 100 mg/d, regardless of their HBeAg or HBV DNA
status. Anti-viral treatment should be started preferably
within 2–3 weeks prior to initiation and no later than the
first day of chemotherapy. Lamivudine treatment should
be continued for at least 6 months after discontinuation of
chemotherapy and preferably for 12 months.
(4) Patients who are anti-HBc positive/HBsAg negative/anti-
HBs negative should receive one dose of a hepatitis B
vaccine and quantitative anti-HBs response measured
within 2–4 weeks. Those who develop an anti-HBs
response will not require pre-emptive anti-viral treat-
ment. Non-responders to the vaccine should be tested for
HBV-DNA by PCR. Patients with viraemia should be
started on pre-emptive lamivudine 100 mg/d.
(5) Patients who are anti-HBc positive/HBsAg negative/anti-
HBs negative/HBV DNA negative do not require pre-
emptive lamivudine. However, continuous monitoring
for ALT is advised. In case of ALT elevation, HBV DNA
should be tested.
(6) Antiviral treatment should be started promptly in
immune suppressed patients who demonstrate symptoms
compatible with a hepatitis flare attributed to HBV
reactivation.
In conclusion, surveillance for HBV status is an integral part
of the care of the haematology patient. By implementing good
medical practice, virtually all patients should be prevented
from contracting or reactivating HBV, in view of the
potentially serious consequences of this infection.
Acute hepatitis B – Hepatic injury that resolves within6 months after exposure to HBV or onset of symptoms. ElevatedALT and AST, HBsAg positive/anti-HBc IgM, positive.Chronic hepatitis B – Hepatic injury which continues >6 months.HBsAg positive >6 months, elevated ALT and AST, HBV-DNAin serum positive or negative.Inactive HBsAg Carrier state – ALT and AST levels persistentlynormal, HBsAg positive >6 months, HBV DNA negative or lowpositive <105 copies/ml in serum.Occult HBV – Normal or abnormal ALT levels, anti-HBcpositive/HBsAg negative, anti-HBs negative or positive, HBVDNA positive (in serum or liver tissue).Overt HBV – Clinically, biochemically and virologically apparenthepatitis B.Resolved HBV – HBsAg negative, HBV DNA negative, normalALT, history of HBV infection/anti-HBc positive/anti-HBspositive or negative.
References
Ahmed, A. & Keeffe, E.B. (1999) Lamivudine therapy in chemother-
apy-induced reactivation of hepatitis B virus infection. American
Journal of Gastroenterology, 94, 249–251.
Al-Taie, O.H., Mork, H., Gassel, A.M., Wilhelm, M., Weissbrich, B. &
Scheurlen, M. (1999) Prevention of hepatitis B flare-up during
chemotherapy using lamivudine: case report and review of the lit-
erature. Annals of Hematology, 78, 247–249.
Avettand-Fenoel, V., Thabut, D., Katlama, C., Poynard, T. &
Thibault, V. (2006) Immune suppression as the etiology of
failure to detect anti-HBc antibodies in patients with chronic
hepatitis B virus infection. Journal of Clinical Microbiology, 44,
2250–2253.
Banatvala, J., Van Damme, P. & Emiroglu, N. (2006) Hepatitis B
immunisation in Britain: time to change? British Medical Journal
332, 804–805.
Bertoletti, A. & Gehring, A.J. (2006) The immune response during
hepatitis B virus infection. Journal of General Virology, 87, 1439–
1449.
Bonkovsky, H.L., Jones, B.P., LaBrecque, D.R. & Shedlofsky, S.I. (2006)
Drug induced liver injury. In: Zakim and Boyer’s Hepatology (ed. by
T.D. Boyer, T.L. Wright & M.P. Mann), pp. 503–550. Elsevier,
Saunders.
ter Borg, F., Smorenburg, S., De Man, R.A., Rietbroek, R.C., Chamu-
leau, R.A.F.M. & Jones, E.A. (1998) Recovery from life-threatening
corticosteroid-unresponsive, chemotherapy-related reactivation of
hepatitis B associated with lamivudine therapy. Digestive Disease
Science, 43, 2267–2270.
Calabrese L.H., Zein N.N. & Vassilopoulos D. (2006) Hepatitis B virus
reactivation with immunosuppressive therapy in rheumatic dis-
Review
ª 2007 The Authors708 Journal Compilation ª 2007 Blackwell Publishing Ltd, British Journal of Haematology, 136, 699–712

eases:assessment and preventive strategies. Annals of Rheumatic
Diseases, 65, 983–989.
Chang, T.T., Gish, R.G., de Man, R., Gadano, A., Sollano, J., Chao,
Y.C., Lok, A.S., Han, K.H., Goodman, Z., Zhu, J., Cross, A., De-
Hertogh, D., Wilber, R., Colonno, R. & Apelian, D. (2006) A
comparison of entecavir and lamivudine for HBeAg-positive chronic
hepatitis B. BEHoLD AI463022 Study Group. New England Journal
of Medicine, 354, 1001–1010.
Chen, P.M., Fan, S., Liu, C.J., Hsieh, R.K., Liu, J.H., Chuang, M.W.,
Liu, R.S. & Tzeng, C.H. (1990) Changing of hepatitis B virus mar-
kers in patients with bone marrow transplantation. Transplantation,
49, 708–713.
Chen, P.M., Fan, S., Liu, J.H., Chiou, T.J., Hsieh, S.R., Liu, R.S. &
Tzeng C.H. (1993) Reactivation of hepatitis B virus in two chronic
GVHD patients after transplant. International Journal of Hematology,
58, 183–188.
Cheng, A.L., Hsiung, C.A., Su, I.J., Chen, P.J., Chang, M.C., Tsao, C.J.,
Kau, W.Y., Uen, W.C., Hsu, C.H., Tien, H.F., Chen, L.T. & Whang-
Peng, J. (2003) Steroid-free chemotherapy decreases risk of hepatitis
B virus (HBV) reactivation in HBV-carriers with lymphoma. He-
patology, 37, 1320–1328.
Chisari, F.V. (1997) Cytotoxic T cells and viral hepatitis. Journal of
Clinical Investigation, 99, 1472–1477.
Clark, F.L., Drummond, M.W., Chambers, S., Chapman, B.A. &
PaHon, W.N. (1998) Successful treatment with lamivudine for
fulminant reactivated hepatitis B infection following intensive
therapy for high-grade Hodgkin’s lymphoma. Annals of Oncology, 9,
385–387.
Cortelezzi, A., Vigano, M., Zilioli, V.R., Fantini, N.N., Pasquini, M.C.,
Deliliers, G.L., Colombo, M. & Lampertico P. (2006) Adefovir added
to lamivudine for hepatitis B recurrent infection in refractory B-cell
chronic lymphocytic leukemia on prolonged therapy with Campath-
1H. Journal of Clinical Virology, 35, 467–469.
Dahmen, U., Dirsch, O., Li, J., Fiedle, M., Lu, M., Rispeter, K., Picucci,
M., Broelsch, C.F. & Roggendorg, M. (2004) Adoptive transfer of
immunity: a new strategy to interfere with severe hepatitis virus
re-infection after woodchuck liver transplantation. Transplantation,
77, 965–972.
Dai, M.S., Chao, T.Y., Kao, W.Y., Shyu, R.Y. & Liu, T.M. (2004)
Delayed hepatitis B reactivation after cessation of preemptive
lamivudine in lymphoma patients treated with rituximab plus
CHOP. Annals of Hematology, 83, 769–774.
Dhedin, N., Douvin, C., Kuentz, M., Saint Marc, M.F., Reman, O.,
Rieux, C., Bernandi, F., Novol, F., Cordonnier, C., Bobin, D.,
Metreau, J.M. & Vernaut, J.P. (1998) Reverse seroconversion of
hepatitis B after allogeneic bone marrow transplantation: a retro-
spective study of 37 patients with pre-transplant anti-HBs and anti-
HBc. Transplantation, 66, 616–619.
Fouillard, L., Serfaty, L. & Gozlan, J. (2006) Adefovir therapy for
lamivudine escape and hepatitis B virus reactivation after reduced
intensity conditioning allogeneic stem cell transplantation. Bone
Marrow Transplantation, 37, 625–626.
Gish R.G. & Locarnini S.A. (2006) Chronic heapatitis B: current testing
strategies. Clinical Gastroenterology and Hepatology, 4, 666–676
Goyama, S., Kanda, Y., Nannya, Y., Kawazu, M., Takeshita, M., Niino,
M., Komeno, Y., Nakamoto, T., Kurokawa, M., Tsujino, S., Ogawa,
S., Aoki, K., Chiba, S., Motokura, T., Shiratory, Y. & Hirai, H.
(2002) Reverse seroconversion of hepatitis B virus after hemato-
poietic stem cell transplantation. Leukemia and Lymphoma, 43,
2159–2163.
Hsiao, L.T., Chiou, T.F., Liu, F.H., Chu, C.J., Lin, Y.C., Chao, T.C.,
Wang, W.S., Yen, C.C., Yang, M.H., Tzeng, C.H. & Chen, P.M.
(2006) Extended lamivudine therapy against hepatitis B virus in-
fection in hematopoietic stem cell transplant recipients. Biology of
Blood Marrow Transplantation, 12, 84–94.
Hsu, C.H., Hsu, H.C., Chen, H.L., Gao, M., Yeh, P.Y., Chen, P.J &
Cheng, A.L. (2004) Doxorubicin activates hepatitis B virus (HBV)
replication in HBV-harboring hepatoblastoma cells. A possible novel
mechanism of HBV reactivation in HBV carriers receiving systemic
chemotherapy. Anticancer Research, 24, 3035–3040.
Hui, C.K., Cheung, W.W., Au, W.Y., Lie, A.K., Zhang, H.Y., Yueng,
Y.H., Wong, B.C., Leung, N., Kwong, Y.L., Liang, R. & Lau, G.K.
(2005a) Hepatitis B reactivation after withdrawal of pre-emptive
lamivudine in patients with haematological malignancy on com-
pletion of cytotoxic chemotherapy. Gut, 54, 1597–1603.
Hui, C.K., Bowden, S., Jackson, K., Au, W.Y., Fong, D.Y., Lie, A.K.,
Chim, C.S., Liang, R. & Lau, G.K. (2005b) Clinical significance of
intrahepatic hepatitis B virus covalently closed circular DNA in
chronic hepatitis B patients who received cytotoxic chemotherapy.
Blood, 105, 2616–2617.
Hui, C.K., Cheung, W.W.W., Zhang, H.Y., Au, W.Y., Yueng, Y.H.,
Leung, A.Y.H., Leung, N., Luk, J.M., Lie, A.K.W., Kwong, Y.L., Li-
ang, R. & Lau, G.K.K. (2006) Kinetics and risk of de novo hepatitis B
infection in HBsAg negative patients undergoing chemotherapy.
Gastroenterology, 131, 59–68.
Iannitto, E., Minardi, V., Calvaruso, G., Mule, A., Ammatuna, E., Di
Trapani, R., Ferraro, D., Abbadessa, V., Craxi, A. & Di Stefano, R.
(2005) Hepatitis B virus reactivation and alemtuzumab therapy.
European Journal of Haematology, 74, 254–258.
Idilman R. (2006) Duration of lamivudine prophylaxis in inactive
hepatitis B virus carriers with haemato oncological malignancies
whon receive chemotherapy. Gut (letter), 55, 1208–1209.
Idilman, R., Arat, M., Soydan, E., Toruner, M., Soykan, I., Akbulut, H.,
Arslan, O., Ozcan, M., Turkyilmaz, A.R., Bozdayi, M., Karayalcin, S.,
Van Thiel, D.H., Ozden, A., Beksac, M. & Akan, H. (2004) Lami-
vudine prophylaxis for prevention of chemotherapy-induced hepa-
titis B virus reactivation in hepatitis B virus carriers with
malignancies. Journal of Viral Hepatology, 11, 141–147.
Ilan, Y., Nagler, A., Adler, R., Naparstek, E., Or, R., Slavin, S., Brautbar,
C. & Shouval, D. (1993a) Adoptive transfer of immunity to hepatitis
B virus after T cell-depleted allogeneic bone marrow transplantation.
Hepatology, 18, 246–252.
Ilan, Y., Nagler, A., Adler, R., Tur-Kaspa, R., Slavin, S. & Shouval, D.
(1993b) Ablation of persistent hepatitis B by bone marrow trans-
plantation from an hepatitis B immune donor: a case report. Gas-
troenterology, 104, 1818–1821.
Ilan, Y., Nagler, A., Zeira, E., Adler, R., Slavin, S. & Shouval D. (2000)
Maintenance of immune memory to hepatitis B envelope protein
following adoptive transfer of immunity in bone marrow transplant
recipients. Bone Marrow Transplantation, 26, 633–638.
Iwai, K., Tashima, M., Itoh, M., Okazaki, T., Yamamoto, K., Ohno, H.,
Marusawa, H., Ueda, K., Nakamura, T., Chiba, T. & Uchiyama, T.
(2000) Fulminant hepatitis B following bone marrow transplanta-
tion in an HBsAg-negative, HBsAb-positive recipient; reactivation of
dormant virus during the immunosuppressive period. Bone Marrow
Transplantation, 25, 105–108.
Review
ª 2007 The AuthorsJournal Compilation ª 2007 Blackwell Publishing Ltd, British Journal of Haematology, 136, 699–712 709

Jazayeri, M.S., Basuni, A.A., Cooksley, G., Locarnini, S. & Carman,
W.F. (2004) Hepatitis B virus genotypes core gene variability and
ethnicity in the pacific region. Journal of Hepatology, 41, 139–146.
Kao, J.H., Chen, P.J. & Lai, M.Y. (2000) Hepatitis B genotypes cor-
relate with clinical outcomes in patients with chronic hepatitis B.
Gastroenterology, 118, 554–559.
Knoll, A., Boehm, S., Hahn, J., Holler, E. & Jilg, W. (2004) Reactivation
of resolved hepatitis B virus infection after allogeneic haemato-
poietic stem cell transplantation. Bone Marrow Transplantation, 33,
925–929.
van der Kolk, L.E., Baars, J.W., Prins, M.H. & van Oers, M.H. (2002)
Rituximab treatment results in impaired secondary humoral im-
mune responsiveness. Blood, 100, 2257–2259.
Kumagai, K., Takagi, T., Nakamura, S., Sawada, U., Kura, U., Kodama,
F., Shimano, S., Kudoh, I., Nakamura, H., Sawada, K. & Ohnoshi, T.
(1997) Hepatitis B virus carriers in the treatment of malignant
lymphomas: an epidemiological study in Japan. Annals of Oncology,
8 (Suppl. 1), 107–109.
Lai, C.L., Shouval, D., Lok, A.S., Chang, T.T., Cheinquer, H., Good-
man, Z., DeHertogh, D., Wilber, R., Zink, R.C., Cross, A., Colonno,
R. & Fernandes, L. BEHoLD AI463027 Study Group, (2006)
Entecavir versus lamivudine for patients with HBeAg-negative
chronic hepatitis B. New England Journal of Medicine, 354, 1011–
1020. Erratum in: New England Journal of Medicine, 2006, 354, 1863.
Lau, G.K.K., Lok, A.S., Liang, R.H., Lai, C.L., Chiu, E.K., Lau, Y.L. &
Lam, S.K. (1997) Clearence of hepatitis B surface antigen after bone
marrow transplantation: role of adoptive immune transfer. Hepa-
tology, 25, 1497–1501.
Lau, G.K.K., Lee, C.K. & Liang, R. (1999) Hepatitis B virus infection
and bone marrow transplantation. Clinical Reviews in Oncology and
Hematology, 31, 71–76.
Lau, G.K.K., Leung, Y.H., Fong, D.Y., Au, W.Y., Kwong, Y.L., Lie, A.,
Hou, J.L., Wen, Y.M., Nanji, A. & Liang, R. (2002a) High hepatitis B
virus (HBV) DNA viral load as the most important risk factor for
HBV reactivation in patients positive for HBV surface antigen un-
dergoing autologous hematopoietic cell transplantation. Blood, 99,
2324–2330.
Lau, G.K.K., Suri, D., Liang, R., Rigopoulou, E., Thomas, M.G.,
Mullerova, I., Nanji, A., Yuen, S.T., Williams, R. & Naoumov, N.V.
(2002b) Resolution of chronic hepatitis B and anti-HBs ser-
oconversion in humans by adoptive transfer of immunity to hepa-
titis B core antigen. Gastroenterology, 122, 614–624.
Lau, G.K.K., Yiu, H.H., Fong, D.Y., Cheng, H.C., Au, W.Y., Lai, L.S.,
Cheung, M., Zhang, H.Y., Lie, A., Ngan, R. & Liang, R. (2003) Early
is superior to deferred preemptive lamivudine therapy for hepatitis
B patients undergoing chemotherapy. Gastroenterology, 125, 1742–
1749.
Lavanchy, D. (2004) Hepatitis B virus epidemiology, disease burden,
treatment, and current and emerging prevention and control
measures. Journal of Viral Hepatology, 11, 97–107.
Law, J.K., Ho, J.K., Hoskins, P.J., Erb, S.R., Steinbrecher, U.P. &
Yoshida, E.M. (2005) Fatal reactivation of hepatitis B post-che-
motherapy for lymphoma in a hepatitis B surface antigen-negative,
hepatitis B core antibody-positive patient: potential implications for
future prophylaxis recommendations. Leukemia and Lymphoma, 46,
1085–1089.
Leaw, S.J., Yen, C.J., Huang, W.T., Chen, T.Y., Su, W.C. & TSao, C.J.
(2004) Preemptive use of interferon or lamivudine for hepatitis B
reactivation in patients with aggressive lymphoma receiving che-
motherapy. Annals of Hematology, 83, 270–275.
Lee, G.W., Ryu, M.H., Lee, J.L., Oh, S., Kim, E., Lee, J.H., Kim, S.B.,
Kim, S.W., Suh, C., Lee, K.H., Kim, W.K., Lee, J.S. & Kang, Y.K.
(2003) The prophylactic use of lamivudine can maintain dose-in-
tensity of adriamycin in hepatitis B surface antigen positive patients
with non-Hodgkin’s lymphoma who receive cytotoxic chemother-
apy. Journal of Korean Medical Science, 18, 849–854.
Li, J., Dahmen, U., Dirsch, O.R., Gu, Y., Polywka, S. & Broelsch, C.E.
(2002) The potential role of BMT in augmenting donor derived
immunity to hepatitis B after rat liver transplantation. Liver
Translantation, 8, 397–404.
Li, Y.H., He, Y.F., Jiang, W.Q., Wang, F.H., Lin, X.B., Zhang, L., Xia,
Z.J., Sun, X.F., Huang, H.Q., Lin, T.Y., He, Y.J. & Guan, Z.Z. (2006)
Lamivudine prophylaxis reduces the incidence and severity of he-
patitis in hepatitis B virus carriers who receive chemotherapy for
lymphoma. Cancer, 106, 1320–1325.
Liang, R.H., Lok, A.S., Lai C.L., Chan, T.K., Todd, D. & Chiu, E.K.
(1990) HepatitisB infection in patients with lymphomas. Hematology
and Oncology, 8, 261–270.
Liang, R., Lau, G.K.K & Kwong, Y.L. (1999) Chemotherapy and bone
marrow transplantation for cancer patients who are also chronic
hepatitis B carriers: a review of the problem. Journal of Clinical
Oncology, 17, 394–398.
Liao, C.A., Lee, C.M., Wu, H.C., Wang, M.C., Lu, S.N. & Eng, S.L.
(2002) Lamivudine for the treatment of hepatitis B virus reactivation
following chemotherapy for non-Hodgkin’s lymphoma. British
Journal of Haematology, 116, 166–169.
Liaw, Y.F. (1998) Hepatitis viruses under immunosuppressive agents.
Journal of Gastroenterology and Hepatology, 13, 14–20.
Lim, L.L., Wai, C.T., Lee Y.M., Kong, H.L., Lim, R., Kaoy, F. & Lim, G.
(2002) Prophylactic lamivudine prevents hepatitis B reactivation in
chemotherapy patients. Alimentary Pharmacology and therapeutics,
16, 1939–1944.
Lindemann, M., Barsegian, V., Runde, V., Fiedler, M., Heerman, K.H.,
Schaefer, U.W., Roggendorf, M. & Grosse-Wilde, H. (2003) Transfer
of humoral and cellular hepatitis B immunity by allogeneic hema-
topoietic cell transplantation. Transplantation, 75, 833–838.
Locarnini, S. (2004) Molecular virology of hepatitis B virus. Seminars
in Liver Diseases, 24 (Suppl. 1), 3–10.
Lok, AS. & Lai, C.L. (1989) Alpha-fetoprotein monitoring in Chinese
patients with chronic hepatitis B virus infection: role in the early
detection of hepatocellular carcinoma. Hepatology, 9, 110–115.
Lok, A.S. & Lai, C.L. (1990) Acute exacerbations in Chinese patients
with chronic hepatitis B virus (HBV) infection. Incidence, predis-
posing factors and etiology. Journal of Hepatology, 10, 29–34.
Lok, AS., Lai, C.L., Wu, P.C., Leung, E.K. & Lam, T.S. (1987) Spon-
taneous hepatitis B e antigen to antibody seroconversion and re-
version in Chinese patients with chronic hepatitis B virus infection.
Gastroenterology, 92, 1839–1843.
Lok, A.S., Liang, R.H., Chiu, E.K. Wong, K.L., Chan, T.K. & Todd, D.
(1991) Reactivation of hepatitis B virus replication in patients re-
ceiving cytotoxic therapy. Report of a prospective study. Gastro-
enterology, 100, 182–188.
Lok, A.S., Wu, P.C., Lai, C.L., Lau, J.Y., Leung, E.K., Wong, L.S., Ma,
O.C., Lauder, I.J., Ng, C.P. & Chung, H.T. (1992) A controlled trial
of interferon with or without prednisone priming for hepatitis B.
Gastroenterology, 102, 2091–2097.
Review
ª 2007 The Authors710 Journal Compilation ª 2007 Blackwell Publishing Ltd, British Journal of Haematology, 136, 699–712

Markovic, S., Drozina, G., Vovk, M. & Fidler-Jenko, M. (1999) Re-
activation of hepatitis B but not hepatitis C in patients with ma-
lignant lymphoma and immunosuppressive therapy. A prospective
study in 305 patients. Hepato-Gastroenterology, 46, 2925–2930.
Martin, B.A., Rowe, J.M., Kouides, P.A. & DiPersio, J.F. (1995) He-
patitis B reactivation following allogeneic bone marrow transplan-
tation: case report and review of the literature. Bone Marrow
Transplantation, 15, 145–148.
Mason, A.L., Xu, L., Guo, L. Kuhns, M. & Perrillo, R.P. (1998) Mo-
lecular basis for persistent hepatitis B infection in the liver after
clearance of serum hepatitis B surface antigen. Hepatology, 27, 1736–
1742.
McMahon, B.J. (2005) Epidemiology and natural history of hepatitis B.
Seminars in Liver Diseases, 25 (Suppl. 1), 3–8.
Nakamura, Y., Motokura, T., Fujita, A., Yamashita, T. & Ogata, E.
(1996) Severe hepatitis related to chemotherapy in hepatitis B virus
carriers with hematologic malignancies. Survery in Japapn, 1987–
1991. Cancer, 78, 2210–2215.
Niscola, P., Del Principe, M.I., Maurillo, L., Venditti, A., Buccisano, F.,
Piccioni, D., Amadori, S. & Del Poeta, G. (2005) Fulminant B he-
patitis in a surface antigen-negative patient with B-cell chronic
lymphocytic leukaemia after rituximab therapy. Leukemia, 19, 1840–
1841.
Nordbo, S.A., Skaug, K., Holter, E., Waage, A. & Brinch, L. (2000)
Reactivation of hepatitis B virus infection in an anti-HBc and anti-
HBs positive patient after allogeneic bone marrow transplantation.
European Journal of Haematology, 65, 86–87.
Nunez, M. & Soriano, R. (2005) Management of patients co-infected
with hepatitis B and HIV. Lancet Infectious Diseases, 5, 374–382.
Onozawa, M., Hashino, S., Izumiyama, K., Kahata, K., Chuma, M.,
Mori, A., Kondo, T., Toyoshima, N., Ota, S., Kobayashi, S., Hige, S.,
Toubai, T., Tanaka, J., Imamura, M. & Asaka, M. (2005) Progressive
disappearance of anti-hepatitis B surface antigen antibody and re-
verse seroconversion after allogeneic hematopoietic stem cell
transplantation in patients with previous hepatitis B virus infection.
Transplantation, 79, 616–619.
Osborn, M.K. & Lok, A.S. (2006) Antiviral options for the treatment of
chronic hepatitis B. Journal of Antimicrobial Chemotherapy, 57,
1030–1034; epub 4 April 2006.
Osterburg, A., Dyer, M.J., Bunjes, D., Pangalis, G.A., Bastion, Y.,
Catoysky, D. & Mellstedt, H. (1997) Phase II multicenter study of
human CD52 antibody in previously treated chronic lymphocytic
leukemia. European Study Group of CAMPATH-1H treatment in
chronic lymphocytic leukemia. Journal of Clinical Oncology, 15,
1567–1574.
Ozguroglu, M., Bilici, A., Turna, H. & Serdengecti, S. (2004)
Reactivation of hepatitis B infection with cytotoxic therapy in non-
Hodgkin lymphoma. Medical Oncology, 21, 67–72.
Perrillo, R.P. (2001) Acute flares in chronic hepatitis B: the natural and
unnatural history of an immunologically mediated liver disease.
Gastroenterology, 120, 1009–1022.
Persico, M., De Marino, F, Russo, G.D., Morante, A., Rotoloi, B. &
Torella, R., De Renzo, A. (2002) Efficay of lamivudine to prevent
hepatitis reactivation in hepatitus B virus infected patients treated
for non-Hodgkin lymphoma. Blood, 99, 724–725.
Petrelli, E., Balducci, M., Pieretti, C., Rocchi, M.B., Clementi, M. &
Manzin, A. (2001) Lamivudine treatment failure in preventing fatal
outcome of de novo severe acute hepatitis B in patients with hae-
matological diseases. Journal of Hepatology, 35, 823–826.
Picardi, M., Selleri, C., De Rosa, G., Raiola, A., Pezzullo, L. & Rotoli, B.
(1998) Lamivudine treatment for chronic replicative hepatitis B
virus infection after allogeneic bone marrow transplantation. Bone
Marrow Transplantation, 21, 1267–1269.
Puoti, M., Torti, C., Bruno, R., Filice, G. & Carosi, G. (2006)
Natural history of chronic hepatitis B in co-infected patients.
Journal of Hepatology, 44 (Suppl. 1), S65–S70; epub 28 November
2005.
Rossi, G., Pelizzari, A., Motta, M. & Puoti, M. (2001) Primary pro-
phylaxis with lamivudine of hepatitis B virus reactivation in chronic
HBsAg carriers with lymphoid malignancies treated with che-
motherapy. British Journal of Haematology, 115, 58–62.
Sarrecchia, C., Cappelli, A. & Aiello, P. (2005) HBV reactivation with
fatal fulminat hepatitis during rituximab treatment in a subject
negative for HBsAg and positive for HBsAb and HBcAb. Journal of
Infection and Chemotherapy, 11, 189–191.
Seth, P., Alrajhi, A.A., Kagevi, I., Chaudhary, M.A., Colcol, E., Sahovic,
E., Aljurf, M. & Gyger, M. (2002) Hepatitis B virus reactivation with
clinical flare in allogeneic stem cell transplants with chronic graft-
versus-host disease. Bone Marrow Transplantation, 30, 189–194.
Shibolet, O., Ilan, Y., Gillis, S., Hubert, A., Shouval, D. & Safadi, R.
(2002) Lamivudine therapy for prevention of immunosuppressive-
induced hepatitis B virus reactivation in hepatitis B surface antigen
carriers. Blood, 100, 391–396.
Shouval, D. (2003) Hepatitis B vaccines. Journal of Hepatology, 39, S70-
S76.
Shouval, D. (2007) Adoptive transfer of immunity to HBV in liver
transplant patients: a step forward toward the proof of concept for
therapeutic vaccination or a transient immunologic phenomenon?
Liver Transplantation (Editorial, in press).
Shouval, D. & Ilan, Y. (1995) Transplantation of hepatitis B immune
lymphocytes as means for adoptive transfer of immunity to hepatitis
B virus. Journal of Hepatology 23, 98–101.
Shouval, D., Adler, R. & Ilan, Y. (1993) Adoptive transfer of immunity
to hepatitis B virus in mice by bone marrow transplantation from
HBV immune donors. Hepatology, 17, 955–959.
Simpson, N.D., Simpson, P.W., Ahmed, A.M., Nguyen, M.H., Garcia,
G., Keeffe, E.B. & Ahmed, A. (2003) Prophylaxis against che-
motherapy-induced reactivation of hepatitis B virus infection with
Lamivudine. Journal of Clinical Gastroenterology, 37, 68–71.
Strasser, S.I. & McDonald, G.B. (1999) Hepatitis viruses and hema-
topoietic cell transplantation: a guide to patient and donor man-
agement. Blood, 93, 1127–1136.
Takai, S., Tsurumi, H., Ando, K., Kasahara, S., Sawada, M., Yamada,
T., Hara, T., Fukuno, K., Takahashi, T., Oyama, M., Onishi, H.,
Tomita, E., Takami, M., Imawari, M. & Moriwaki, H. (2005) Pre-
valence of hepatitis B and C virus infection in haematological ma-
lignancies and liver injury following chemotherapy. European
Journal of Haematology, 74, 158–165.
Tillman, H.L., Wedemeyer, H. & Manns, M.P. (2003) Treatment of
hepatitis B in special patient groups: hemodialysis, heart and renal
transplant, fulminant hepatitis, hepatitis B virus reactivation. Journal
of Hepatology, 39 (Suppl. 1): 206–211.
Tur-Kaspa, R., Burk, R.D., Shaul, Y. & Shafritz, D.A. (1986) Hepatitis
B virus DNA contains a glucocorticoid-responsive element. Pro-
ceedings of the National Academy of Science, USA, 83, 1627–1631.
Vassiliadis, T., Garipidou, V., Tziomalos, K., Perifanis, V., Giouleme,
O. & Vakalopoulou, S. (2005) Prevention of hepatitis B reactivation
with lamivudine in hepatitis B virus carriers with hematologic ma-
Review
ª 2007 The AuthorsJournal Compilation ª 2007 Blackwell Publishing Ltd, British Journal of Haematology, 136, 699–712 711

lignancies treated with chemotherapy – a prospective case series.
American Journal of Hematology, 80, 197–203.
Vento, S, Cainelli, F & Longhi M.S. (2002) Reactivation of replication
of hepatitis B and C viruses after immunosuppression therapy: an
unresolved issue. Lancet Oncology, 3, 333–340.
Wands, J.R., Chura, C.M., Roll, F.J. & Maddrey, W.C. (1975) Serial
studies of hepatitis associated antigen and antibody in patients re-
ceiving antitumor chemotherapy for myeloproliferative and lym-
phoproliferative disorders. Gastroenterology, 68, 105–112.
Webster, A., Brenner, M.K., Prentice, H.G. & Griffiths, P.D. (1989)
Fatal hepatitis B reactivation after autologous bone marrow trans-
plantation. Bone Marrow Transplantation, 4, 207–208.
Westhoff, T.H., Jochimsen, F., Schmittel, A., Stoffler-Meilicke, M.,
Schafer, J.H., Zidek, W., Gerlich, W.H. & Thiel, E. (2003) Fatal
hepatitis B virus eactivation by an escape mutant following ritux-
imab therapy. Blood, 102, 1930.
Wong, S.N. & Lok, A.S. (2006) Update on viral hepatitis: 2005. Current
Opinions in Gastroenterology, 22, 241–247.
Xunrong, L, Yan, A.W., Liang, R & Lau, G.K.K. (2001) Hepatitis B
reactivation after cytotoxic or immunosuppressive therapy-patho-
genesis and management. Reviews in Medical Virology, 11, 287–299
Yeo, W. & Johnson, P.J. (2006) Diagnosis prevention and management
of hepatitis B virus reactivation during anticancer therapy. Hepa-
tology, 43, 209–220
Yeo, W., Steinberg, J.L., Tam, J.S., Chan, P.K., Leung, N.W., Lam, K.C.,
Mok, T.S. & Johnson, P.J. (1999) Lamivudine in the treatment of
hepatitis B virus reactivation during cytotoxic chemotherapy. Jour-
nal Medical Virology, 59, 263–269.
Yeo, W., Chan, P.K.S., Zhong, S., Ho, W.M., Steinberg, J.L., Tam, J.S.,
Hui, P., Leung, N.W.Y., Zee, B. & Johnson, P.J. (2000) Frequency of
hepatitis B virus reactivation in cancer patients undergoing cytotoxic
chemotherapy: a prospective study of 626 patients with identifica-
tion of risk factors. Journal of Medical Virology, 62, 299–307.
Yeo, W., Zee, B., Zhong, S., Chan, P.K.S., Wong, W.L., Ho, W.M.,
Lam, K.C. & Johnson, P.J. (2004a) Comprehensive analysis of risk
factors associating with hepatitis B virus (HBV) reactivation in
cancer patients undergoing cytotoxic chemotherapy. British Journal
of Cancer, 90, 1306–1311.
Yeo, W., Lam, K.C., Zee, B., Chan, P.S.K., Mo, F.K.F., Ho, W.M.,
Wong, W.L., Leung, T.W.T., Chan, A.T.C., Ma, B., Mok, T.S.K. &
Johnson, P.J. (2004b) Hepatitis B reactivation in patients with he-
patocellular carcinoma undergoing systemic chemotherapy. Annals
of Oncology, 15, 1661–1666.
Yeo, W., Chan, P.K., Ho, W.M., Zee, B., Lam, K.C., Lpi, I.K., Chan,
A.T.C., Mok, T.S.K., Lee, J.J., Leung, T.W.T., Zhong, S. & Johnson,
P.J. (2004c) Lamivudine for the prevention of hepatitis B virus re-
activation in Hepatitis B s-antigen seropositive cancer patients un-
dergoing cytotoxic chemotherapy. Journal of Clinical Oncology, 22,
927–934.
Yim, H.J. & Lok, A.S. (2006) Natural history of chronic hepatitis B
virus infection: what we knew in 1981 and what we know in 2005.
Hepatology, 43 (2 Suppl. 1), 173–181.
Yu, A.S., Cheung, R.C. & Keefe, E.B. (2006) Hepatitis B vaccines.
Infectious Disease Clinics of North America, 20, 27–45.
Zhong, S, Yeo W, Schroder, C, Chan, P.K., Wong, W.L., Ho, W.M.,
Mo, F, Zee, B & Johnson, P.J. (2004) High hepatitis B virus (HBV)
DNA viral load is an important risk factor for HBV reactivation in
breast cancer patients undergoing cytotoxic chemotherapy. Journal
of Viral Hepatology, 11, 55–59.
Review
ª 2007 The Authors712 Journal Compilation ª 2007 Blackwell Publishing Ltd, British Journal of Haematology, 136, 699–712