second non-neurologists
TRANSCRIPT

Second Edition
NEUROLOGYFORNON-NEUROLOGISTS
Edited byWIGBERT C. WIEDERHOLT, M.D.Professor of Neurosciences, Department of CNeurosciences, University of California, San Diego;Center, San Diego, Lajolla, California [^ t4
1g^g
1988GRUNE & STRATTON
An Imprint of the W. B. Saunders Company
Harcourt Brace Jovanovich, Inc.
Philadelphia, San Diego, London, Toronto, Montreal, Sydtreys Tokyo

Jevelop an insidiously lfunctions equally. Thisalcohol on cerebral
iprovement of cortical fit returning to a normalsidiously progressing iWernicke-Korsakoff s)
e of dementia.
13MULTIPLE SCLEROSIS
li
MARK KRITCHEVSKY, M.D.senic, mercury, and lead are raie presence of other distinctding to dementia, particularly..icluding barbiturates. Meticulamay require obtaining inforn
g stores, may reveal that patieithat render some patients tota.nts and relatives that they of
and, as a matter of fact, shoe:dications. Withdrawal from
drug intake may restore stkccompanying ataxia and distf inactivity, boredom, or physiore every night, and to take a Iis abuse of sedatives, whichdoses. Most elderly subjects
our period. Withdrawal fromd increase of activities duringtern of living. Unfortunately, I
inceptions and convenience. Iage such abnormal and unheal
238, 1986.ative cases, definition, and review. J jA
Li deterioration. Arch Neural 33:658-
6.
35:1-12,1978.
e demyelinating disorders are a broad category of diseases of the central nervousitem (CNS) in which there is destruction of myelin sheaths with relative preserva-n of neuronal axons. The primary demylinating diseases include multiple sclerosis[S) and its uncommon variants which have been called Devic's optic neuromyelitis,1o's concentric sclerosis, transitional sclerosis, and Schilder's diffuse sclerosis. The:ondary demyelinating diseases include a variety of etiologically specific causes ofmyelination such as neoplasm, viral infection, and certain toxic and metabolic dis-lers. This chapter covers MS in depth because it is the only demyelinating disordertt is frequently encountered by clinicians.Multiple sclerosis is a chronic neurological disease that typically begins in earlyulthood and progresses to significant disability in the majority of cases. An un-edictable course and a wide variety of symptoms and signs are remarkable featuresthe disease, which is the most common progressive and disabling neurological con-Lion affecting young adults in the United States. (There are approximately 123,000sown MS patients in the U.S.) Because the onset of the illness is usually in early[ulthood, family life and job productivity are often seriously disrupted. Currenteories favor an immune-mediated pathogenesis of MS secondary to a fundamental:fect in the host, with or without the presence of a triggering viral agent.The mean age of onset of MS is 33 years and the mean age of diagnosis, 37 years. It
,rely appears before age ten and only about 10% of cases begin after the age of fifty.IS occurs more frequently in white women, having a female to male ratio of 1.7 to 1td a white-to-nonwhite ratio of about 2 to 1. It is more common in the cold and tem-
'rate climates of the higher latitudes in both hemispheres. The northern latitudes oftC continental United States lie well within this "MS belt." Studies of the prevalenceF MS in immigrant populations indicate that the chance of a person developing the
UROLOGY FOR NON-NEUROLOGISTS
Fights of reproduction in any form reserved.
177
® 1988 by Grune & StrattonISBN 0-8089-1911-3
"h i1
II

178 Mark Kritchevsky
disease is correlated with having lived in these higher latitudes in the first 15 years of normal (retrobulbarlife,shows residual defit
There is some evidence that genetic factors are involved. MS occurs in 1% to 2% of manifested as a palfirst-degree relatives (parents, siblings or children) of MS patients, and MS however, that notpredominantly affects persons of northern European ancestry. Furthermore, recent previously healthystudies of the distribution of histocompatability antigen (HLA) genetic marker in MS symptoms and signspatients revealed an overrepresentation of A3, B7, and DW2 types. The relation of The other commathese factors to the pathogenesis of the disease is unknown.'
ophthalmoplegia (Dnystagmus of the atof convergence. Itsthe demyelinating 1
SYMPTOMS AND SIGNS with the weakness cor tumor.
two patients with MS are exactly alike, and the clinical manifestations in aNopar-
nc
ticular person are related to the distribution of lesions within the nervous system.dys fuunnctition maymay bes o m be
Lesions may be found virtually anywhere within the white matter of the centralemptp y (atonic or H.
neuraxis, including the white matter of the cerebral hemispheres, optic nerves, brain bo urgency, in.bowelel
c
complaint iisstem, cerebellum, and spinal cord. Although someg patients have evidence oft _ widespread lesions from the outset, others may present with isolated focal involve- Complaints of se:
ment of any of these structures. Symptoms and signs may disappear8 Y ppear or may fluctuateproblems in males
in character and intensity. The sometimes bizarre and transient nature of the symptoms Wcompounded by der
may be mistaken for a psychiatric condition. course.
Muscle weakness and spasticity due to corticospinal tract lesions are among theLesions in the cc:
most frequent symptoms of MS. Spasticity of the lower extremities may be accom-y
mus, prominent gaitSevere intentionpanied byp y painful flexor spasms. Impaired dexterity, slowness of rapid alternating
treeimpossible, and se%
movements, hyperreflexia, extensor plantar responses, and absence of abdominalreflexes may also be noted, along with hemiparesis, muscle strength is a
paraparesis, quadri aresis, or -monoparesis. P Sensory symptorr
Complaints of severe fatigue are common; disablingg exhaustion may be broughtg on
perature sensation,_
by an ordinary day's activities. This symptom is remarkable because in some patientsit
unusual distributionamination may reve
occurs in the presence of normal strength and without any symptoms generally as-Impairment of vibr:sociated with depression.
Visual disturbances include impaired visual acuity, impaired color vision, centralsensory functions. Ls usually described
scotoma, diplopia, and uncommonly such visual field defects as homonymoushemianopsia. Symptoms may be unilateral bilateral.
the extremities 'Thior Optic neuritis and retrobulbar
neuritis are common in MS. The patient complains of loss of vision which progressesother disor ers- affi
_over days and may be mild to severe. Pain in or behind the eye, which sometimes is 'Y ^
proximately 5% toor a pseudoradicular
caused or worsened by movement of the globe, may be an associated complaint. Ex- .;= " Some form of meamination during the episode shows loss of visual acuity, loss of color vision, a central sion is common, anscotoma, and preserved peripheral vision. Examination of the fundus shows a swollen -disc if the lesion is close to the optic nerve head (papillitis) and organic psycho-
otherwise the disc looks .I may be severe in pat

Multiple Sclerosis 179
these higher latitudes in the first 15 a y ars ' 'normal (retrobulbar neuritis). Neurological examination following the episode oftenshow
s residual deficits of visual acuity and color vision, together with optic atrophy:tors are involved. MS occurs in 1% to 2%a :manifested as a pale optic disc, particularly the temporal portion. It must be noted,
or children) of MS patients, and M$, - ."however, that not all patients with optic neuritis have MS. Only 30% to 60% of
:rn European ancestry. Furthermore, receI r ; .previously healthy patients with a first attack of optic neuritis go on to developability antigen (HLA) genetic marker in Ms '. symptoms and signs of MS.)f A3, B7, and DW2 types. The relation o T • . s` The other common visual manifestation, of MS is diplopia caused by an intemuclearease is unknown. X °„ ophthalmoplegia (INO). This is a disorder of conjugate lateral gaze characterized by
sta mus of the abducting eye and weakness of the adducting eye with preservationn Y g g Y g Y P.of convergence. Its presence in a young adult is almost pathognomonic for MS withthe demyelinating lesion in the medial longitudinal fasciculus ipsilateral to the eywith the weakness of adduction. It may also be caused by other lesions such as stroke
Fnor tumor.
"-ike, and the clinical manifestations in a
Disturbance of sphincter control is noted in at least two thirds of patients. Urinarypares
-. 'dysfunction may be due to a failure to store (hypertonic or spastic bladder), failure tolion of lesions within the nervous system,- ' empty (atonic or flaccid bladder), or a mixture of the two. Symptoms include fre-:re within the white matter of the cen : quency, urgency, incontinence, incomplete emptying, and urinary retention. The majorie cerebral hemispheres, optic nerves, brain . bowel complaint is constipation, although fecal incontinence occurs occasionally.though some patients have evidence o Complaints of sexual dysfunction are frequent and include erectile and ejaculatoryrs may present with isolated focal involve- problems in males and loss of orgasmic ability in females. These problems may beis and signs may disappear or may fluctuat compounded by depression or by urinary or fecal incontinence occuring during inter-bizarre and transient nature of the symptoms course.n f ` Lesions in the cerebellar white matter or cerebellar pathways may produce nystag-
corticospinal tract lesions are among the mus, prominent gait and extremity ataxia, and a halting or scanning quality of speech.ty of the lower extremities may be accom- Severe intention tremor of the upper extremities may make the simplest self-care tasksed dexterity, slowness of rapid alternating : impossible, and severe ataxia of gait may prevent effective ambulation even whenstar responses, and absence of abdominal.: . muscle strength is adequate.hemiparesis, paraparesis, quadriparesis, or , Sensory symptoms are diverse and include numbness, tingling, impairment of tem-
^: perature sensation, and abnormal sense of limb position. Vague sensory complaints inon; disabling exhaustion may be brought on ° unusual distributions may mysteriously come and go, confounding the diagnosis. Ex-tom is remarkable because in some patients-, amination may reveal no objective sensory deficit even in the presence of symptoms.th and without any symptoms generally as- - I
mpairment of vibratory perception may be found without any abnormality of other•sensory functions. Lhermitte's phenomenon, which is provoked by flexion of the neck,
'isual acuity, impaired color vision, central.ich visual field defects homonym
ous..his usually described as an electric shock sensation that radiates d own the spine or into
as the extremities. is unusua symptom is of due to MS, buf may also occur with•
I or bilateral. Optic neuritis and retrobulbar
i, other disor3e'rs affecting the posterior columns of the cervical spinal cord. Ap-omplains of loss of vision which progres
ses) Proximately 5% to 10% of MS patients experience either typical trigeminal neuralgian in or behind the eye, which sometimes
isor a pseudoradicular pain of the extremities or trunk.
globe, may be an associated complaint. Ex' : Some form of mental disturbance eventually occurs in half of MS patients. Depres-f visual acuity, loss of color vision, a centra
l , }° Sion is common, and an inappropriate euphoria is seen on occasion. Mild dementiaExamination of the fundus shows a
swollenand organic psychosis due to cerebral involvement occur frequently. These disorder•
ie head (papillitis) otherwise the disc looks• • may be severe in patients with advanced disease.

180 Mark Kritchevsky
PRECIPITATING AND EXACERBATING FACTORS
Although the cause of MS is unknown, certain factors sometimes precipitate attacks ::in known MS patients. Trauma, infection, and surgery have all been associated withworsening of MS. There may be a slight increase in risk of exacerbation during and in the 6 months following pregnancy. There is no evidence that immunization is aprecipitating factor. .
Elevation of body temperature has a different effect. Fever, heavy physical exertion,hot weather, a hot shower or bath, and exposure to sunlight may all cause a transient` and reversible worsening of existing symptoms. For example, weakness may become =-?worse to the point where a normally ambulatory patient is unable to get out of thebathtub after a hot bath. Neurological function then returns to baseline within minutesto several hours of when the patient is helped out of the bath. Similarly, a person whocan usually transfer independently may require assistance in this activity during veryhot weather. Occasionally a symptom such as visual difficulty in one eye may bepresent only during exposure to heat. Interestingly, lowering of body temperature byswimming in a cold pool or taking a cold shower may result in a temporary improve-ment of function.
THE COURSE OF MS
The natural progression of MS is unpredictable. In approximately 40% of MSpatients, the disease is initially exacerbating-remitting, with or without completerecovery between episodes. After several years, there is a transition to a slow andrelentless chronic progression. In another 20% to 30% of patients, the diseasemaintains an exacerbating-remitting course. In 10% to 20% of patients, the coursefrom the outset is chronically progressive, a pattern that is seen most often in patientswho are older at the time of onset of the illness. Finally, in about 20% of MS patients,the course is benign, the patient suffering only one or two mild exacerbations and no
• permanent functional disability.• The rate of progression of MS is variable and ranges from the occasional malignant
course, with death within weeks or months after onset, to life-long benign disease withminimal symptoms and disability. In general, those who have either chronic progres-sion or frequent severe relapses from the outset of the illness have a less favorableprognosis. Patients who have been in the chronic progressive stage of the illness for anumber of years may experience decline in the rate of deterioration. =r
Over the last half century advances in antibiotic therapy and in the management of = `.complications have increased the lifespans of MS patients. In 1936, only 8% of _ T
patients were reported to survive beyond 20 years after the onset. By 1961, survivalhad increased tenfold, over 80% of patients surviving for 20 years after onset of ill- >'ness. Of those patients surviving for 20 years or more, approximately 30% remained

FACTORS
tain factors sometimes precipitate attacksid surgery have all been associated with:ase in risk of exacerbation during and inis no evidence that immunization is a
ant effect. Fever, heavy physical exertion,;ure to sunlight may all cause a transientns. For example, weakness may becomestory patient is unable to get out of then then returns to baseline within minutesout of the bath. Similarly, a person who
re assistance in this activity during veryas visual difficulty in one eye may betingly, lowering of body temperature by)wer may result in a temporary improve-
Multiple Sclerosis 181
gainfully employed. This indicates that the long-term prognosis in MS is morefavorable now than in the past.
CLINICAL DIAGNOSIS
The diagnosis of MS remains a clinical one; there is no specific laboratory test forthe disease. The clinician generally makes the diagnosis of MS when there is evidenceof multiple lesions in time and space. The history includes at least one clear attack ofneurological dysfunction which lasted at least 24 hours and had some degree of subse-quent recovery. The neurological and laboratory examinations should show evidenceof two or more lesions that are not contiguous in space. If the age of onset is between10 and 50 years, and the patient has lived in the higher latitudes during part of the first15 years of life, and the symptoms worsen transiently with exposure to heat, thediagnosis is more likely. There must be no better neurological explanation for thepatient's symptoms and signs.
Often the diagnosis cannot be made at the time of presentation. In the young personwith a single attack which consisted of a single lesion in space, laboratory tests mayfail to show evidence of other subclinical lesions. MS can then only be suspected.Similarly, in the older patient with a gradually progressive deficit which can be ex-plained by one lesion at a specific location, MS is a diagnosis of exclusion.
iictable. In approximately 40% of MSig-remitting, with or without completegars, there is a transition to a slow and20% to 30% of patients, the diseaseIn 10% to 20% of patients, the course)attern that is seen most often in patientsss. Finally, in about 20% of MS patients,ly one or two mild exacerbations and no
nd ranges from the occasional malignant!er onset, to life-long benign disease withthose who have either chronic progres-
itset of the illness have a less favorablemic progressive stage of the illness for a
rate of deterioration.biotic therapy and in the management ofof MS patients. In 1936, only 8% ofyears after the onset. By 1961, survivalsurviving for 20 years after onset of ill-s or more, approximately 30% remained
LABORATORY EXAMINATION
There is no specific laboratory test for MS. Laboratory tests are, however, importantfor ruling out other nervous system diseases that may mimic MS. They are also in-
;. valuable for demonstrating evidence of a second lesion which is subclinical andtherefore not detectable by history or neurological examination. The demonstration ofthe second lesion is generally the key to making the diagnosis of MS in the patientwith early disease. Laboratory tests are also important in the patient who hassymptoms suggestive of MS but who lacks objective signs of nervous system disease.One or more definite lesions of the nervous system may be shown to be present.
The hot bath test may be done in the clinic or on the hospital ward. The patient isimmersed in a bathtub of hot water and then examined neurologically for the transientappearance of additional deficits. A patient with subclinical optic neuritis may developan abnormality of visual acuity or color vision. In other patients, an internuclear oph-thalmoplegia, nystagmus, or ataxia may become apparent. Weakness, hyperreflexia,and Babinski signs may also develop.
Visual, auditory, and somatosensory evoked responses are sensitiveelectrophysiologic procedures that can identify clinically silent lesions. If all three
3. tests are performed, approximately 80% to 85% of patients with a clinically definitediagnosis will have an abnormality on at least one of the tests. The visual and auditory

182 Mark Kritchevsky
evoked response tests are especially useful in identifying a second subclinical lesion inpatients who have clinical evidence of only a single spinal cord lesion. In this instance,
the demonstration of a second lesion remote from the spinal cord may help establish =z`' 3the diagnosis of MS. *1
The neuroimaging test that is often helpful in the patient with suspected MS is mag.netic resonance (MR) imaging of the brain and spinal cord. It may be used to exclude =t^,other CNS diseases which may mimic MS. Additionally, it frequently demonstratescharacteristic lesions of MS within the CNS white matter. In patients with only one 6known lesion, the MRI may demonstrate a second lesion, thereby making MS the slikely clinical diagnosis. MS lesions appear as areas of increased signal on spin-echo ' images and decreased signal on inversion-recovery images. Computed tomography 4(CT) of the brain is of limited usefulness because only 20% of patients with clinicallydefinite MS will have CT abnormalities.
Nonspecific abnormalities present in the cerebrospinal fluid (CSF) are frequentlyuseful in supporting the diagnosis of MS by suggesting the presence of an in- .,flammatory CNS lesion. The CSF cell count commonly shows a modest increase inmononuclear cells. The total CSF protein is mildly or moderately elevated in less than W.,half of MS patients. In approximately 60% to 75% of patients there is an abnormal = Relevation of the CSF IgG. Furthermore, 85% of patients with clinically definite MS '..have abnormal oligoclonal bands in the IgG zone on CSF electrophoresis. If IgG andoligoclonal bands are both measured, 90% of such MS patients have abnormalities. TOne limitation of these tests is that they are less frequently abnormal in early or verymild cases of MS. Additionally, abnormalities of the more sensitive tests may also beproduced by other CNS inflammatory processes and by chronic CNS infections.
In summary, the patient with reliable historical or clinical evidence of two separate _'-CNS lesions should have a CSF exam to rule out infection. He should also generally "-have an MR scan of the brain and in some cases of the spinal cord, to rule out anotherpathological process that may mimic MS. The patient with only one established lesionand the patient who is an MS suspect without any definite CNS lesions should undergothese tests together with the hot bath test and evoked responses. In these patients, thelaboratory tests are done in an attempt to rule out other CNS pathology and to 5<demonstrate the presence of at least two separate CNS lesions required to make theclinical diagnosis of MS.
DIFFERENTIAL DIAGNOSIS
The differential diagnosis of multiple sclerosis depends on the syndrome of CNSdysfunction which is present at the time of diagnosis. When an isolated optic neuritisis secondary to local orbital or sinus infection, the causative process can generally bedemonstrated with CT or MR. Similarly, serology and spinal fluid examination showwhether the optic nerve lesion is due to a meningeal process such as neurosyphilis orcarcinomatous meningitis.
it= : scnd subclinical lesion ii-_ = cord lesion. In this instance,
;jrai cord may help establish
.-e with suspected MS is mag-It may be used to exclude
_r'riT frequently demonstrates-^ In i+atients with only one
thereby making MS the- ^ T x e sed signal on spin-echo
•_ . Computed tomography2Y i patients with clinically
- i '_uid (CSF) are frequently'the presence of an in-.
_ : ows a modest increase in_ - =ci xeiv elevated in less than- T _.mar- there is an abnormal;- --^ - :ah clinically definite MS',
::ectrophoresis. If IgG and5 ,,meat; have abnormalities."
aonormal in early or veryz--- sensitive tests may also bey
—cic CNS infections.= c evidence of two separate
T He should also generally; iii cord. to rule out another
-__ :niv- one established lesion15 lesions should undergo
- z tsees. In these patients, theCNS pathology and to
= ions required to make the
Multiple Sclerosis 183
2n the syndrome of CNS an isolated optic neuritis
process can generally be_ = ^-yi fluid examination show
such as neurosyphilis or
A presentation which can be entirely explained by a single posterior fossa lesioncould be produced by a benign or malignant tumor, basilar impression of the skull,
developmental diseases such as Arnold-Chiari malformation, or occasionally by
cerebrovascular disease. MR scan generally rules out these conditions. The uncommonchronic meningeal process which began in the posterior fossa would be ruled out byan examination of the spinal fluid for infection or tumor.
If an isolated spinal cord lesion is caused by spondylosis, tumor, or syrinx, it will beseen with MR or CT myelography. When no cause is found for an isolated spinal cordlesion, and the history and spinal fluid are suggestive of a mild acute or subacute in-flammatory process, an idiopathic transverse myelitis is the probable diagnosis. Only afew percent of these patients go on to develop MS.
On the rare occasions when MS presents clinically as a subacute or chronic in-tracerebral mass lesion, low-grade glioma is generally suspected. MRI or, if necessary,brain biopsy will reveal the true cause of the lesion.
In any patient with remitting-relapsing neurological illness, collagen vascular dis-ease, sarcoidosis, and Behret's syndrome must be considered. All three commonly
i. have associated involvement of other organ systems. MS in contrast, is a strictlyneurological disease. In the patient with collagen vascular disease, there may also beabnormal rheumatologic blood tests. Many patients with sarcoidosis will have an ab-normal level of angiotensin converting enzyme (ACE).
Finally, neuroimaging tests rule out mass lesions, particularly tumor or spondylosis,in the patient with gradually progressive illness. Neurodegenerative diseases may alsopresent in this fashion and may sometimes be demonstrated by family history or actual
examination of family members.The diagnosis of possible or probable MS is made after ruling out the appropriate
conditions in the differential diagnosis. Except for the rare cases where the diagnosisis proved pathologically, the diagnosis is and remains presumptive. For this reason, fu-ture changes in neurological status generally warrant reconsideration of the differentialdiagnosis at a number of times during the course of the disease.
THERAPEUTICS
The management of MS can be divided into four categories: (a) treatment aimed atmodification of the disease course, including treatment of the acute exacerbation andtreatment directed at long-term suppression of the disease; (b) treatment of thesymptoms of MS; (c) prevention and treatment of medical complications; and (d)management of secondary personal and social problems.
The short-term use of either adrenocorticotropic hormone (ACTH) or oral corticos-teroids is the only specific therapeutic measure available for the treatment of thepatient with an acute exacerbation of MS. Controlled studies of such therapy haveshown that patients with ACTH treatment have a faster recovery, although there is no
difference in the final amount of recovery.
i a ^

184 Mark Kritchevsky
ACTH gel, 40 units intramuscularly (IM) twice daily, may be given for 10 days andthen tapered at a rate of 10 units every day. Pretreatment evaluation should include a Ti
search for tuberculosis, uremia, high blood pressure, diabetes, electrolyte disturbance, ">:and peptic ulcer, which are relative contraindications to the use of ACTH. BecauseACTH produces a variable amount of salt and water retention, weight and blood pres.sure should be checked regularly during treatment, and a low sodium diet with oralpotassium supplementation should be prescribed. The occurrence of complicationsnecessitating early discontinuation of therapy are infrequent, although intensificationof preexisting depression or euphoria; emotional lability, insomnia, and frank
f psychosis are among the most common troublesome side effects.Prednisone may be given orally on an outpatient basis. The total daily dose is
determined by weight: 50 mg b.i.d. for weight greater than 180 pounds, 40 mgfor patients weighing 110 to 180 pounds, and 30 mg b.i•d. for patients weighing les
110 pounds. This weight-adjusted dose is given for 7 consecutive days. On the ? ` weighth day the total daily amount is given as a single morning dose, and the dose isthereafter gradually tapered to 0 mg at the rate of 10 mg per day. = ;
There is no established treatment that suppresses MS on a long-term basis. ChronicACTH or prednisone therapies have not proved beneficial in reducing the number ofexacerbations or in slowing gradually progressive disability. High-dose cyclophos-phamide has recently been shown to have some favorable effect on the course ofpatients with severe progressive disease. However, the therapy is potentially quitetoxic, and retreatment is necessary because the majority of patients regress. For thepresent, this treatment is reserved for patients with severe MS that is progressing at asignificant rate.
• Effective symptom management and assistance in coping with the problems of -:-everyday living can improve the quality of life for the MS patient. For example, spas-ticit may be alleviated by drug therapy Baclofen, 40 to 80 mg per day dividedY Y Y g PY• g P Y in•doses, is usually of value in reducing severe spasticity as well as involuntary flexorspasms. Mild spasticity generally should not be treated, but most patients withmoderate to severe spasticity warrant a trial of therapy. Increased weakness anddeterioration in gait are, unfortunately, a limiting side effect of baclofen in some am- _=--
' bulatory patients. Such weakness clears up within 24 to 48 hours after reduction indose or discontinuation of therapy. This side effect is especially prominent in patientswho are relying on their spasticity as a support during standing or walking. Dantrolene -
sodium is an alternative antispasticity drug that offers no major advantage overbaclofen and has the disadvantage of potential hepatotoxicity. Diazepam is also effec-
x rive in reducing spasticity, but the dosage required for relief of spasticity oftenproduces an unacceptable degree of sedation. In some patients, a bedtime dose of 10mg of diazepam may quiet nighttime flexor spasms and allow uninterrupted sleep. ,
Gait difficulty in MS is often due to combinations of weakness, spasticity, and in- ` r
coordination. Evaluation by a physical therapist with instruction in the use of walkin and, in some instances, customized braces, may be very beneficial for ambulatory
patients.Bladder dysfunction in MS is common. Referral to a urologist for urodynam
ic ,

Multiple Sclerosis 185
Lily, may be given for 10 days and ` ..studies and measurement of post-voiding residual urine are often required to define the
[ment evaluation should include atype of bladder dysfunction and determine the proper therapy. The failure-to-store
diabetes, electrolyte disturbance,: bladder may produce simple urinary urgency and occasional accidental incontinence.symptoms can be effectively managed by intermittent restriction of fluid intake
''ns to the use of ACTH. Because ,'retention, weight and blood pres- .,.
Theseand/or small intermittent doses of oxybutynin chloride. When there is severe urgency
bladder may be converted to a failure-and a low sodium diet with oral :
of complications
and frequent incontinence, the failure-to-storeto-empty bladder by the regular administration of oxybutynin chloride (5 mg, two or
The occurrence;frequent, although intensification _:. s, Y three times a day). Treatment then proceeds as described below. The failure-to-empty
incontinence, recurrent infection, or symptoms ofal lability, insomnia, and frank ; bladder produces frequent overflow
The use of chronic indwelling catheters for treatment should beside effects. I:nt basis. The total daily dose is
urinary retention.avoided where possible because complicating infection invariably develops. Intermit-
is well tolerated. It is,iter than 180 pounds, 40 mg b.i.d. - tent self-catheterizatio
n is a far safer therapy that surprisingly
however, only in patients who have reasonably well-preserved dexterity in thepossible=:tg b.i.d. for patients weighing lessen for 7 consecutive days. On the _" '
hands. Constipation is frequent in patients with spinal cord involvement and should be
gle morning dose, and the dose is .". =F treated by conventional methods.
=Pain as a direct result of MS lesions within the CNS may occur as a typical
I mg per day. ,: ;MS on a long-term basis. Chronic ,• trigeminal neuralgia or as pseudoradicula
r pain, usually in one leg, sometimes in anthe trunk. The trigeminal neuralgia may be treated with carbamazepine,
:neficial in reducing the number of =°`'
arm or part ofsuch treatment can be associated with undesirable transient weakness similaralthoughe disability. High-dose cyclophos- t:..
favorable effect on the course of ; .to that occasionally encountered with baclofen. Surgical procedures such as per-
:r, the therapy is potentially quite _ cutaneous rhizotomy have been emssuch
ractorprocedures inses papatients is not wellges-the long-term effectiveness of althoughiajority of patients regress. For the
i severe MS that is progressing at a ;_: - tablished. When pseudoradicular pain is chronic, it is usually refractory to treatment.posture is common inLow backache related to weak trunk muscles and poor
in those who have gait disturbance. Conventional therapeutice in coping with the problems of wheelchair patients or
for low back strainthingmeasures of these musclesiinthe MS patient. For example, spas- :
40 to 80 mg per day in divided -need physical h ll therapy for tretight hamstring muscles may Ysical
ro r osture inine. A firm bed, p pe p;n,sticity as well as involuntary flexor
order to relieve tension on the lumbosacral spregular swimming, along with physical therapy, are also usually
wheelchair, and^e treated, but most patients with _f therapy. Increased weakness and beneficial for low back pain. little
to Surgicalv side effect of baclofen in some am- -' . Intention tremor unfortunately respondsd ugg therapy.
for treatment otremor;
is severin 24 to 48 hours after reduction in:t is especially prominent in patient
scryothalamotomy reserved
; useful function in oneand
extremitybeto
managed shmply by thecoften
llextrem
ring standing or walking. Dantrolene wise totally helpless. Diplopia is temporary
visualand often temporarynoacuity,
at offers no major advantage over use of an eye patch. sinree there effective treatment for these sym ptoms. Whe
Diazepam is also effec-1 This is fortunate,
luired for relief of spasticity often0a bedtime dose of 10some patients,
sbeneficial.c fatigue andloass de arylsevere andworthwhile and maylbetsurprisingly in some
^.., imipramine P
is and allow uninterrupted sleep..n- are impotent. oPePenile prostheses should not beamplantedain men
lions of weakness, spasticity, andinstruction in the use of walking
selected patients whopwho have a signficant degree of sensory impairment of the penis or perineum lest the
withnay be very beneficial for ambulatory •F
penis painlesslycomplications of MS are either preventable or treatable.
for is :'°All ofAll medical
These include contractures of limbs, pressure sores, and pulmonary and urinary tractferral to a urologist urodynam

The motsand uppecal pictupredomitmusclespredomiihyporethintact bthand, prloss ofmusclestem ("f
The tchronicusuallyherited,it permi
NEUROU
All rights c
fi N
186 Mark Kritchevsky
infections. Every wheelchair and bedridden patient should be involved in a regularprogram to prevent contractures and pressure sores. Wheelchair patients with goodarm function should be taught how to press down on the arms of the chair at frequentintervals in order to relieve pressure on the sacrum and buttocks. Bed-ridden patientsrequire special air or water flotation mattresses, and should be carefully positioned andturned every 2 to 3 hours. Pressure points must be examined frequently, and nursingcare efforts must be intensified at the earliest sign of a developing sore. The smallestulceration should be considered as a potentially life-threatening complication andtreated appropriately and vigorously. Patients with progressing pressure sores may re-quire surgical treatment for debridement or skin grafting.
The secondary complications of MS cover a broad spectrum of personal and socialdifficulties—marital, occupational, psychosexual, recreational, legal, and financial.Most physicians are not traditionally prepared to deal in depth with many of theseproblems though, ironically, it is often in this area that the most can be done to helpsome patients. In order to deal effectively with these problems, the physician must be-come familiar with resources in the community and enlist the help of other profes-sionals such as psychologists, social workers, marriage counselors, vocationalrehabilitation counselors, and lawyers. The local chapter of the National MultipleSclerosis Society may be able to help directly or can recommend referral to peoplewho are qualified and experienced in working with MS patients. The patient can alsobe encouraged to participate in support groups, which are often sponsored and or-ganized by the local Multiple Sclerosis Society.
The physician's attitude may have a powerful psychological impact on the MSpatient. There is sometimes a tendency by both physicians and patients to view thedisease as incurable and untreatable. Such a view is excessively negative and unwar-ranted. A positive but realistic approach by a knowledgeable and sympatheticphysician can greatly improve the patient's sense of well-being and perhaps even havea beneficial effect on the course of the disease. Hope is a powerful elixir that should beencouraged. Helplessness should be discouraged. Many patients gravitate toward Un-proven popular therapies, such as special diets. If the putative therapy is both low-riskand affordable, the physician can be most helpful by taking a tolerant position. An ad-ditional benefit of this approach is that the patient thereby learns that the physician isopen minded and eager to support the patient in his search for legitimate therapy. At alater date the patient will be more likely to follow the physician's advice against someother therapy which might be unreasonably expensive or potentially harmful.
GENERAL REFERENCES
Matthews WB (ed): McAlpine's Multiple Sclerosis. Edinburgh, Churchill Livingstone, 1985.
Poser CM (ed): The Diagnosis of Multiple Sclerosis. New York, Thieme-Stratton Inc., 1984.
Sibley WA: Management of the patient with multiple sclerosis. Semin Neurol 5:134-145, 1985.
Smith CR, Scheinberg LC: Clinical features of multiple sclerosis. Semin Neurol 5:85-93, 1985.

Evoked Potentials 89
ni iv v
_10., NV I II vl VII
ri– vi
—v
}-.iv
I I I .Ip 2 4 6 8 to
--^ SOUND msec
om the scalp and their presumed origin. TheNould be elicited by a click at several levels inBAEP is seen on the top right, recorded fromear (Aips). The approximate latency from
marker.
ies from the stimulus to each wave aregearing loss and end-organ disease sinceichlear origin. The interpeak latencies,
degree of poststimulus peak latencyloss. Brain stem auditory evoked poten-ype of hearing loss (conductive or sen-lly useful in the evaluation of hearing instandard audiometric testing.
ce interpeak latencies are little affectedhan poststimulus peak latencies in the
evaluation of neurological disorders. Ex tra-axial posterior fossa lesions involving theauditory nerve, such as cerebellopontine angle tumors, may result in a normal wave Iand prolonged latency or absence of all subsequent waves to stimulation of the invol-ved ear. If enough of the auditory nerve has been destroyed, wave I may also beabolished. If a large lesion causes brain stem disto rtion, the III–V interpeak latency tocontralateral stimulation may be prolonged as well.
Intra-Axial Posterior Fossa Lesions. Intramedullary posterior fossa lesionsusually do not affect wave I. However, all of the subsequent waves may be delayed orobliterated by direct involvement of the generating structures or by interruption of thepathways to them. The I–III interpeak latency is prolonged in lesions at the pon-
:: tomedullary level, and the III–V interpeak latency is prolonged by pontine andmidbrain lesions. Brain stem auditory evoked potential abnormalities can be caused bytumors, including astrocytomas, pinealomas, fourth ventricle ependymom as, andmetastases. Brain stem infarction or hematoma, trauma, infection, degenerative dis-eases, such as olivopontocerebellar degeneration, central pontine myelinolysis, multi-pie sclerosis (MS), and other diseases involving the brain stem auditory pathways alsolead to BAEP abnormalities. Brain stem auditory evoked potentials are of particularvalue in the diagnosis of MS, since they may demonstrate subclinical lesions at multi-pie levels that escape detection by other diagnostic tests, including CT. About.,one
r third of patients with possible MS and no clinical evidence of brain stem involvementhave abnormal BAEPs; this suggests an additonal central nervous system (CNS) le-
=` r_ sion and supports the diagnosis of MS. Thus, the BAEP may obviate neuroradiologicalexaminations to exclude other pathological conditions. Magnetic resonance imaging(MRI), very sensitive in the detection of brain stem and cerebellar lesions, appears tohave a higher diagnostic yield th an BAEPs and may become the test of first choice inthese patients.
Supratentorial Structural Lesions. Unless supratentorial lesions distort the brainstem, they do not alter waves I–V. Wave VI and VII abnormalities may be found, but
° they must be interpreted with caution in view of the normal variability of these waves.
Metabolic and Toxic Encephalopathies. Brain stem auditory evoked potentials aregenerally not affected by metabolic and toxic encephalopathies such as drug overdose,diabetic ketoacidosis, uremia, and liver disease. Hypothermia, on the other hand, in-duces reversible BAEP abnormalities.
=^ Coma. Brain stem auditory evoked potentials are useful in the evaluation of com-• atose patients because they remain relatively unchanged in coma due to cortical
damage, metabolic encephalopathy, or drug overdose, whereas they usually displaysevere abnormalities in coma secondary to brain stem structural damage. Patients
)f- - fulfilling the clinical c riteria of brain death have either no BAEPs or only wave 1. On
the other hand, normal BAEPs have been found in metabolic or toxic coma, despite. c
linical findings suggesting brain stem dysfunction, and they may still be present• despite anesthetic doses of barbiturates causing electrocerebral silence on EEG.

Evoked Potentials . 91
i 1 9 20 23 25 msec
Tuna AUI I RADIATION
►r-field SEPs to median nerve stimulation. Noteem, P14 in the brain stem (medial lemriiscus),ourtesy of Byron Budnick)
IALS (SEPs)
)brained by electrical stimulation of aSequential activation of peripheral nervesrecorded from scalp electrodes. There is
p to about 70 msec after the stimulus arei no significant contribution from the:d potentials to median nerve stimulationthat overlie the primary somatosensory
lals and their presumed sites of origin are
simulation can also be recorded fromspine, which, when combined with scalpnduction time in various segments of theJition, the conduction time in peripheralsomatosensory sytem can be examined
Clinical Applications
Peripheral Neuropathy. Somatosensory evoked potentials may be used in theevaluation of peripheral nerve sensory conduction velocity. This is particularly helpfulin patients with axonal neuropathies affecting large sensory fibers, such as Friedreich'sataxia, when peripheral nerve compound action potentials cannot be obtained. SEPsmay be delayed or absent in patients with radiculopathies, plexopathies, orneuropathies.
Spinal Cord Disease. Peroneal nerve SEPs may be of value in patients with spinal;n _` cord disease at the thoracic or lumbosacral level, and they complement median nerve
SEPs in the evaluation of cervical myelopathies. Recordings from electrodes over the spine provide complementary information to scalp recordings. Patients with clinically
complete cord transections have absent SEPs to peroneal stimulation in leads rostradto the lesion, whereas patients with incomplete transections may have delayed or nor-
;; mal responses. The absence of peroneal SEPs in cord-injured patients may, therefore,
indicate completeness of the lesion. Abnormal SEPs are frequently seen in patientswith myelopathies of various etiologies that cause loss of proprioceptive sense,
= - whereas loss of pain and temperature sensation is associated with normal SEPs.
Posterior Fossa Lesions. In posterior fossa lesions, all waves after P10 may bedelayed or absent. The P1—N19 interpeak latency provides an estimate of conduction
= _ time in the cervical and brain stem somatosensory pathways from brachial plexus tothalamus. Normal SEPs are characteristic of patients with lateral medullaryp syndrome,syndrome of the cerebral peduncle, and other brain stem lesions in which sparing ofposition sense suggests functional integrity of the medial lemniscus. This is in spite ofany impairment of pain and temperature sensation resulting from involvement of the
i spinothalamic system.Patients with lesions involving the medial lemniscus, as confirmed by impaired joint
position sense, display abnormal SEPs. A large number of patients with MS have ab-normal SEPs, often in the absence of sensory abnormalities either by history or physi-cal examination. SEPs, may, therefore, contribute to the early diagnosis of MS bydemonstrating subclinical lesions.
Supratentorial Structural Lesions. Thalamic and hemispheric lesions spare earlypotentials of the SEP, but subsequent waves may be delayed or absent. Patients withlesions involving the ventral posterior thalamus, thalamocortical sensory radiations, orsomatosensory cortex may have abnormal SEPs. As in spinal cord and brain stem
lesions, there is usually a good correlation between impaired joint position sense andSEP abnormalities.
nantly a contralateral pathway, in contrast _
i, therefore, provide lateralizing inform
Coma. Somatosensory evoked potentials are useful in evaluating coma followinghead trauma and coma from structural brain disease, particularly if serial studies arePerformed. Patients so affected may have prolonged P15—N19 interpeak latency, sug-gesting brain stem dysfunction, in addition to abnormalities of later waves. Toxic

Lumbar Puncture and Cerebrospinal Fluid Examination 67
TABLE.4-9. CSF SYNDROMES.S OF.IN - pressure PMNs Lymphs Glucose Protein
CSF syndrome (mm H 20) Fluid (per mm3) (per mm3) (mg/dl) (mg/dl)
Bacterial meningitis 200-1000 Clear to 10-10,000 Occur after 0-40 40-1000
cloudy treatment (normalserumglucose)
:- Viral Increased Clear to 6-1000 Normal 20-200
n a CSF VDRL. Though classic `meningitis or normal cloudy
Tuberculous Increased Clear to 0-25 25-500 0-40 40-5000
forms of CNS syphilitic infection y meningitis cloudyFungal meningitis Normal or Clear to 0-500 Usually 40-60
cloudy 0sometimes
med if meningeal carcinomatosis is '1Z: normal
:SF abnormality. Tumor cells from _ Cerebral abscess Increased Clear 0 0-40 Normal 20-300
tifiedd on a cytological examination. (no meningitis) and
:ed, Gram stain, acid-fast stain, and
subdural empyemaBrain tumor Increased Clear 0 0-100 Normal 20-500
0 0-500 0-100 20-500
triate cultures for bacteria, anerobicarc or Clear,meningitis increased cloudy,
red when needed. Cryptococcal an- - malignantare extremely useful in diagnosing-"
cells oncytology
,s parasites, including cysticercosis, Multiple sclerosis Normal Clear 0 0-100 Normal 20-1005
Control in Atlanta, Georgia. Viral r Guillain-Barre Normal Clear 0 Occasionally Normal -1000
adil available in the future, re uir-y Q0
Peripheral Normal Clear 0 0-5 Normal 20-200
lescent stages. ,, • .^ Reuropathies,al meningitis, the patient must be : - diabetes, uremia,
trove or disprove baterial infection. alcholismLow Xanthochromic 0 0-50 Normal 500-3000
th tuberculosis, the patient must beSpinal
subarachnoid block Normal Normal!r positive or negative. Herpes en- Pseudotumor cerebri increased Clear 0 0-5
7mphocytic pleocytosis with normal -However, polymorphonuclear cells CSF of Premature Infants or Neonates. The normal CSF of premature infants and
[is with xanthochromia (sometimes neonates is not the same as adults'. The fluid is typically clear but slightly xan-
of the hemorrhagic necrosis of the thochromic, contains less than 40 WBC per mm3. RBCs are frequently found, the
protein varies between 20 and 150 mg per dl, and the CSF glucose level is ap-
proximately equal to that of the plasma.ELEVATED Patterns of CSF abnormalities found in a varie ty of neurologic disorders are shownWLIN
in Table 4-9.
s(SSPE)
tPRPE) CEREBROSPINAL FLUID PATHWAYS AND HYDROCEPHALUS
Normal Flow and Absorption of CSF
carcinoma Cerebrospinal fluid is formed by the choroid plexus in both lateral ventricles, third,vngal infections, and fourth ventricles. The CSF volume in adults is estimated to be 90 to 150 ml, 500vascular disease ml being formed per day. When CSF flows out of the fourth vent ricle, it follows the
III('•

290 Frank R. Sharp
TABLE 21-6. CENTRAL CAUSES OF VERTIGOVascular disease Demyelinating disease
TIAs of the vertebrobasilar system Multiple sclerosisStrokes of posterior circulation Postinfectious demyelinationCerebellar hemorrhage Progressive multifocal leukoencephalopathyCerebellar infarction Degenerative diseaseSubclavian steal syndrome Friedreich's ataxiaArteriovenous malformation Olivopontocerebellar degenerationAneurysm Opthalmoplegia plus syndromeVasculitis Refsum's disease
Posterior fossa lesions Temporal lobe epilepsyPrimary brain tumors (glioma, meningioma, Vestibulogenic reflex epilepsy
epidermoid, sarcoma) Cranial neuropathies affecting the 8th nerveEpendymoma SarcoidMetastases Cancer (meningeal carcinomatosis)Subdural hematoma Sjogren's syndrome, Vogt-Koyagnami-HaradasTemporal bone cyst syndromeHydrocephalus Guillain-Barre syndromeSyringobulbia Paget's diseasePlatybasia OsteopetrosisArnold-Chiari syndrome Infections
Basilar artery migraine MeningitisTrauma Herpes zoster (Ramsay Hunt)
Abscess (parenchmymal, epidural. subdural)
barometric pressure in an airplane, or examiner induced increases or decreases (Hen-nebert's sign) of pressure. Perilymph fistulas may occur after trauma, infection, andother causes, and can be corrected surgically.
Occlusion of the Internal Auditory Artery
The sudden onset of acute vertigo and deafness without change of consciousness orother neurological signs can occur when the patient suffers an occlusion of the internalauditory artery. This artery either comes directly from the basilar artery or can be abranch of the anterior inferior cerebellar artery. Occlusion occurs in patients with vas-culitis, atherosclerosis, or other arterial abnormalities.
Central Causes of Vertigo
Vertigo due to central causes is usually associated with other central nervous system(CNS) symptoms or signs. If a central lesion is suspected from history and examina-tion, audiogram, ENG, BAER, and CT and/or MR are usually indicated. Specific dis-eases which cause central vertigo are listed in Table 21-6.
VASCULAR DISEASE. Transient Ischemic Attacks (TIAs). VertebrobasilarTIAs are often associated with vertigo and ataxia. Vertigo alone may be the first signof vertebrobasilar insufficiency. However, most patients will have had one other ac-companying sign or symptom of brain stem dysfunction within several months of the

JSES OF VERTIGOyelinating diseaseiltiple sclerosisstinfectious demyelination)gressive multifocal leukoencephalopathynerative diseaseiedreich's ataxiaivopontocerebellar degenerationnhalmoplegia plus syndrome:fsum's diseasepoml lobe epilepsy:stibulogenic reflex epilepsyiial neuropathies affecting the 8th nerveucoidancer (meningeal carcinomatosis)ogren's syndrome, Vogt-Koyagnami-Haradas,ndromeuillain-Barrd syndrometget's diseasesteopetrosisctionsleningitislerpes zoster (Ramsay Hunt),bscess (parenchmymal, epidural, subdural)
x induced increases or decreases (Hen-may occur after trauma, infection, and
.-a
Dizziness and Vertigo 291
less without change of consciousness orttient suffers an occlusion of the internalctly from the basilar artery or can be a(. Occlusion occurs in patients with vas-ialities.
tciated with other central nervous systemis suspected from history and examina-
r MR are usually indicated. Specific dis-Table 21-6.heneic Attacks (TIAs). Vertebrobasilar[axia. Vertigo alone may be the first signost patients will have had one other ac-Jysfunction within several months of the
onset of vertigo. In order to make a definite diagnosis of vertebrobasilar insufficiencyin vertiginous patients, they must have had nonvestibular brain stem dysfunction com-bined with vestibular dysfunction at least once. This might be vertigo combined withdiplopia, numbness, dysarthria, or dysphagia. Total blindness, numbness or weaknesson both sides of the body, and ataxia usually indicate posterior fossa ischemia. TIAsgenerally last 10 to 20 minutes and resolve. Neurological testing is normal between at-tacks. Vertigo is seldom a feature of carotid artery disease.
Stroke. Infarction of the brain stem may cause vertigo and is invariably as-
sociated with other brain stem signs. The most common of these syndromes is a lateralmedullary stroke, often caused by occlusion of the vertebral or posterior inferior
cerebellar artery.Cerebellar Hemorrhage. The acute onset of headache, nausea, vomiting, depres-
sed consciousness, and ataxia suggests the possibility of a cerebellar hemorrhage,usually a surgical emergency. This syndrome may mimic acute labyrinthitis exceptthat patients with cerebellar hemorrhage often have a severe headache and becomelethargic or comatose. In many cases of cerebellar hemorrhage there may be othersigns including diplopia, facial weakness and numbness, pupillary abnormalities,dysarthria, dysphagia, limb ataxia, and long tract signs. Cerebellar hemorrhage re-quires emergency CT and immediate surgical evacuation of the blood clot in the pos-
terior fossa if it is endangering the patient's life.Subclavian Steal Syndrome. This rare syndrome is characterized by symptoms of
brain stem ischemia produced by exercise or movement of one arm, usually with adecreased or absent peripheral pulse and decreased blood pressure in that arm. Thissyndrome is caused by a stenosis of the left subclavian artery proxima
by
iml toto the origin e in ofthe vertebral artery or a st
enosis of the right subclavian artery pproximal itated b variousof the vertebral artery. Increased blood flow to the left arm, precipitated
factors, results in retrograde flow down the vertebral artery, causing brain stem is-chemia. Patients may experience TIAs with vertigo as one of the symptoms.
Basilar Artery Migraine. Some patients have definite vertigo or other brainstemsymptoms which occur prior to, during, or after their otherwise typical migraineheadaches. Severe nausea, vomiting, and vertigo may occur. Structural lesions shouldbe ruled out. The syndrome occurs most often in young women and may resolve withtreatment for migraine. Rarely, patients have loss of consciousness associated with thesyndrome. Dilantin, propanolol, and sansert are useful for treating this disorder.
POSTERIOR FOSSA LESIONS. Any posterior fossa lesion may produce vertigo
or dizziness. There are usually cranial nerve or cerebellar symptoms or signs whichmay be associated with alterations of consciousness. Posterior fossa lesions can pressdirectly on brain stem structures or compress the aqueduct and produce hyd-rocephalus. Masses around the fourth ventricle can give rise to Brunn's syndrome.This syndrome includes (a) vertigo, nystagmus, and vomiting sometimes associatedwith loss of consciousness on head turning, (b) freedom from symptoms until the headis turned, and (c) maintenance of the head in a particular position in order to preventattacks. Most posterior fossa lesions can be diagnosed by contrast CT or MR.
DEMYELINATING DISEASES. Multiple sclerosis can cause isolated vertigo or

292 Frank R. Sharp
vertigo associated with other brain stem findings during an acute exacerbation. Chan-ges of hearing do not usually occur in MS. The vertiginous symptoms usually resolve.
Epilepsy. Some patients have vertigo as the initial manifestation of a generalizedseizure or a complex partial (psychomotor or temporal lobe) seizure. It is assumed thatthe seizure focus in these cases is located in the temporal lobe. Vertigo can be elicitedby electrical stimulation of portions of the temporal and inferior frontal lobe inhumans. Vestibulogenic epilepsy is a rare type of reflex epilepsy in which vestibular
s sensory input precipitates a generalized seizure.
GENERAL REFERENCES
Baloh, RW, Homrubia V: Clinical Neurophysiology of the Vestibular System. Philadelphia, F A Davis, 1979.Brandt R, Paroll R: The multisensory physiological and pathological syndromes. Ann Neurol 7:195-203,
1980.Daroff RB: Evaluation of dizziness and vertigo. In Glaser JS (ed): Neurophthalmology, vol 9 pp 39-54, St.
Louis, CV Mosby, 1977.Drachman D, Hart C: An approach to the dizzy patient. Neurology, 22:323, 1972.Fisher CM: Vertigo in cerebrovascular disease. Arch Otolaryngol 85:529-534, 1967.Hybels RL: Drug toxicity of the inner ear. Med Clin North Amer 63:309-19, 1979. Spector M (ed): Dizziness and vertigo. New York, Grune and Stratton, 1976.Troost BT: Dizziness and vertigo in vertebrobasilar disease. Stroke 11:301-303, 413-415 1980; .Jannetta PJ, Moller MB, Moller AR: Disabling positional vertigo.N Engl J Med 310:1700, 1984.Lechtenberg R, Shulman A: The neurological implications of tinnitus. Arch Neurol 41:718, 1984.
A varietytiating anmajor altemay damain adults cethanol cayet been Ii
A congtsome infraned manntmonths or
EMBRYC
The nercells fold C
NEUROLOGIAll rights of rel

Neurologic History and Examination 29
.nau in exa nination of the heart, orientation as to place is seen in moderate disturb ances of cerebral function, and im-aticc. i blood vessels, includ- pairment of orientation as to person is present with severe ce rebral dysfunction.
cr . . y e examination and when ex-ral ', imnion is readily incor- Speechn. s.` : e history taking and therva i Vi=a_ abnormal movements Speech is produced by the delicate coordination of respiratory muscles, vocal cords,-fec - t :moons are made. The dif- soft palate, tongue, and lips. Dysfunction in any of these produces distinctive speechire aei ± = the following sections. abnormalities. Partial or complete paralysis of one vocal cord produces hoarseness;
paralysis of both vocal cords results in aphonia. Dysfunction of the soft palateproduces a distinctive hypernasal speech: The classic pseudobulbar speech associatedwith bilateral subcortical lesions is characterized by hypernasality, slur ring of words,and an apparently great effort with reduced output. Patients with multiple sclerosis(MS) frequently exhibit "scanning" speech, in which each syllable is pronounced with
I sta. w e of the patient's social, equal strength and the intonation of normal speech is lost. In patients with parkin-3 iy te normal for someone sonism, speech becomes very soft and may be barely audible, Most speech abnor-
nor....i a with higher intellect. malities are easily detected during normal conversation with the patient. Lipi hic i _.mctions, it will be in- movements can be tested by asking the patient to say rapidlyNs: "memememememememe," tongue movements by "lalalalala" and palatal movements
by "gagagagagagagaga." In addition, phrases such as "around the rugged rock the rag-ged rascal ran" may be used. Practically all speech abnormalities except for speechapraxia imply peripheral, brain stem, and/or cerebellar dysfunction.
Language
As opposed to speech dysfunction, impairment of the ability to use abstractlanguage symbols almost always implies cortical damage, usually of the dominanthemisphere. Aphasic patients may have difficulty expressing themselves in speakingor in writing, or may have difficul ty comprehending spoken or written language. Al-though one of these functions may be prominently impaired, more often than not allfour functions are disturbed to some degree. Language comprehension is best tested byasking the patient to follow both spoken and written commands, and by determining if
.ndi..- : or improvement of a the patient comprehends what has been said or written. Language production is testedant:: changes. The range by asking the patient to talk and write. Eight types of aphasia can usually be recog-ligf: — . -crundation, light coma nized. These aphasias and their typical features are presented in Table 2-1.
b i.". and deep coma (in In Broca's aphasia, the lesion is located in the inferior and posterior portion of thepr:. .^sL . Conditions seen in the dominant frontal lobe. Patients typically are nonfluent but use subst antive words; their
.ion = ii hallucinations and speech is slow, produced with great effort, and poorly articulated. There is a markedreduction of language output, but comprehension is usually good. The same mistakesare almost always seen when the patient writes. The ability to name objects is also af-fected frequently. This type of aphasia is usually accompanied by a hemipa resis on thecontralateral side that is worse in the arm th an the leg. The patient is aware of the defi-
Ia – Orientation to time isp rcit and frequently is frustrated and depressed.
ion; -_-::rsin syndromes. Dis- In Wemicke's aphasia, the lesion is located in the posterior and superior portion ofthe dominant temporal lobe. Language production is fluent, with normal articulation

v
mm
z
N
-i
X77 .^'"^ 0^ t\ ^^J y «J• y
m
m
o
00C•m mo
,w is cn _^ o a • ,t0
o j w{ u^
N'. 5' ^° ^°- o ' - C M —f°
d C eq
a•
CD
y w "p pw c
^' "f 0wyNwa3o' wv, O
i
O a <c
C»C^ m yN CDN b m W m m CD 0N `< = c9
v y C N
0
Cr]^f
wC ^+,
-D ...N N N M>>
3e.
^.j 0 CD .^ y R g@ym7 ^^^
W w y p' C- m N Ill wCDD
`< ^j 0
m NN <ON O ^'
o w c3E
o aN as_ _,oO o 7C O w" n
Ny l7 _ to
5 3 n
O '^ G N 'G .^ N 9 0: N N^t
D
0i n a' co f^ C N o o o' o ' -'a' °' r < °, F o °^ x oa CD R E. ^ A ao o ^, ^oz rL ao'm c^a,'°. a y `^ o ° ^_ ' G ° Co`< C a a' n
to
N Z a y fn ^' S' < w p' O C w (9 ^T1 N N '3' N rnM¢• n :; o' a =° " a ^. ° A ^,' S' Z ►d co a b o °, a `° o c c
o C `^ n w n o '^ C o cn R as y - `^ 0 o o o d ., CD CD CD
0 N ~ O a .v° < ccoo ^r^+ °° 0 G• p O fD ^. X ry„ n ^' m w C o l. i
c Z f o < R' h vii m x co' o - 0 0 c^ ° .^G m CCD "' "' n cu ° p •°' ° `^' 'oZ
o r°, ° o a_' ^^ o io o C cooCD
w ^' can "' ° ^^^, b Go. ^n o `^ a, w o 0 o a c G n 4,^9 ° m ^' ^'i, O ^. jC 0- co '» m b a R Crl m ,^ :' w y. c^ o w
CD
o Cr1 w w a- "I o 0 o w co 0 0 < y' +s a o 0CD
o w o a b O .2 ° ^• y c •a a G^ cu y ti `^ <^••f, Q_ • t o co o a " b '"' ao w .e CD _- O<cco O co N o a° o ° ^' ° c^'c ~- c oO °° co E3 w n n O O
CD < Ow p o
f K'
IA < 2 ^• c^i a 0 0 o ro coo G '? o an7 ^'
0 c+ ^' i y N o co "d oa < aCD
o ^; o ° C^ < co r? v^' cn b.- cu bo ar " ° co co cu co
ow o cu y
_• o to N o N ry N R pi - CO `° ==, 0
o ^, c^u o can o a^ b l< 0° a ^n Z +d Asti '" p cu ^n p. Oo
CL^
^n
co +'. b ° a " c
oo w a a 'd p ^• co p Q a.
0(D
'b `° ^y' o c)' "`' v, ct, 9 ^'' 0 S FN'. y' R ro ° ,n g coo o o ^' b< o w • or An a a a ; b ° cs ° y
o awo ° N o r te `o C ,, (oa9 C° 0 `< f °c 7 0^' `^ ° ^' °•^. c v ^o -4 0 0
O rwi, 00 .vGi
^' ^J ? < n ° OQ .ni 0 G- ' a n n y y ^' a' .^ O
ao g''^ o '^ a ^'j F-• C G p N O
O 7 - O^ N N O ^ fD ^ 9" y O.
< a cr o- Cii ^ ^n 0 co o CD C io w p ' o °mu 0 o _oO d v' ^, a
'L° a c. = ^• ,^ o 0. g b
5-C :3 y "^ n ° y 0 oo y
t<n G co F y ? r^^i ^. cwi fe w e<v ^^
w °^ '^ a `^ ° o a G ' m w° `° . f^ o a o^• t G o
<
N N r.• ry1 [D Q- (^ ^' o rte. • o,fit, p' - w r? n r N in O, T 9 Q. I N w `< n. iy = i 7' in D .°-y to ^G
A
AU)
A
U0N
m
CDav0CD

scan of brain.
; ±e:. It is thus possible to discern featuresft ':asiry, or abnormal fluid or gas collec-cr. -..-,anent film, is made as a permanent
:. _y one should keep in mind that a CT-_- : a computer-generated representation_=ined slice of the brain. Unexpected
eam hardening" artifact, a detector-anial pathology.
_i^_: 0.5% of the entire range of densities^:. to white matter of the brain can be dis-____ ._ with different scanners from 0.7 cm
Neuroradiology 103
to about 0.2 cm. Objects that contrast strongly against the background are much easierto discern than those that have a density close to that of surrounding structures. To im-prove the detectability of a lesion, the radiologist may elect to inject intravenousradiographic contrast medium. Many lesions then are enhanced and show a markedlyincreased density. This is particularly true of lesions in which the blood-brain barrier isdestroyed (e.g., infarct, many tumors, abscesses), where the contrast medium leavesthe circulating blood pool and leaks out into the abnormal tissue. Hypervascularity ofa lesion is another factor that will contributes to enhancement of contrast medium.Radiographic contrast media may also be injected intrathecally in order to opacify thecerebrospinal fluid and render the extracerebral cisterns clearly visible.
DIAGNOSTIC POWER AND LIMITATIONS. CT is capable of excellent densityresolution as well as linear resolution and will consequently reveal both structural andmorphological abnormalities. For about 15 years this dual capability has made CT anunsurpassed diagnostic modality for a wide variety of intracranial diseases.
In congenital malformations all major anatomical aberrations, such as abnormallyshaped ventricles or underdeveloped parts of the brain are clearly displayed. In a-queductal stenosis, the narrow aqueduct itself may not be visible, but the level ofobstruction can be inferred from the appearance of the ventricles.
In trauma to the brain, CT is the preferred modality. Extracerebral and intracerebralhematomas, cerebral edema, and herniation of the brain are accurately shown (Fig. 8-4), as are important sequelae of trauma such as chronic hematomas, porencephaliccysts, and cerebral atrophy.
The yield of CT is also high in cerebrovascular diseases. Intracerebral hemorrhages,visible as areas of increased x-ray attenuation, are consistently demonstrated. Thedetection rate of cerebral infarcts is not quite as high, probably in the range of 80%.Most infarcts are not detectable during the first 2 to 3 days after the clinical incidentbut become visible during the ensuing 7 to 21 days. Transient ischemic attacks fre-quently leave no trace on CT scans because in most instances no organic brain injuryof sufficient magnitude has occurred. Arterial aneurysms are detected by most CTscanners, provided that their diameter exceeds 4 to 5 mm. After rupture of an
aneurysm, the scanner reveals the extent of the intracranial hemorrhage. The location
of the aneurysm may be inferred from the distribution of the hematoma. The presenceof an arteriovenous malformation is suggested by curvilinear calcifications and dilatedserpentine vascular spaces. Most of the vascular abnormalities diagnosed or suggested
by CT require angiography for definitive diagnosis.Localized inflammatory processes are shown with a high degree of accuracy. They
usually evolve from a solid inflammatory focus to an area of cerebritis that later may
Produce an abscess with a vascular capsule and a necrotic core. The final result isca
vitation or resolution. All these stages are recognizable by CT. Diffuse inflammatoryPr
ocesses, such as viral encephalitis, are detectable, although with less accuracy.De
myelinating diseases, previously not diagnosable by any radiological modality,may be shown by CT, although not consistently. Important examples are multifocalleukoe
ncephalopathy (PML) and multiple sclerosis (MS). In the latter disorder

N
110 Fo(ke J. Brahme
1d^i7
Ja
Figure 8-8. MR image scan of brain (coronal plane) showing a largemeningioma.
inflammatory foci in patients with AIDS, in whom no abnormalities have been ob- n '
served on CT. On the other hand, old calcified inflammatory foci are poorly seen byMRI. .r
Chronic sequelae of head trauma—contusions, hematomas, substance loss—arereadily diagnosed by MRI, but acute trauma is at present better examined by CT. Freshhematomas, fracture lines and depressed bone fragments are poorly seen by MRI. Inaddition, acute trauma patients may be attached to respirators and monitoring devices;all these factors favor the use of CT rather than MR in the emergency situation.
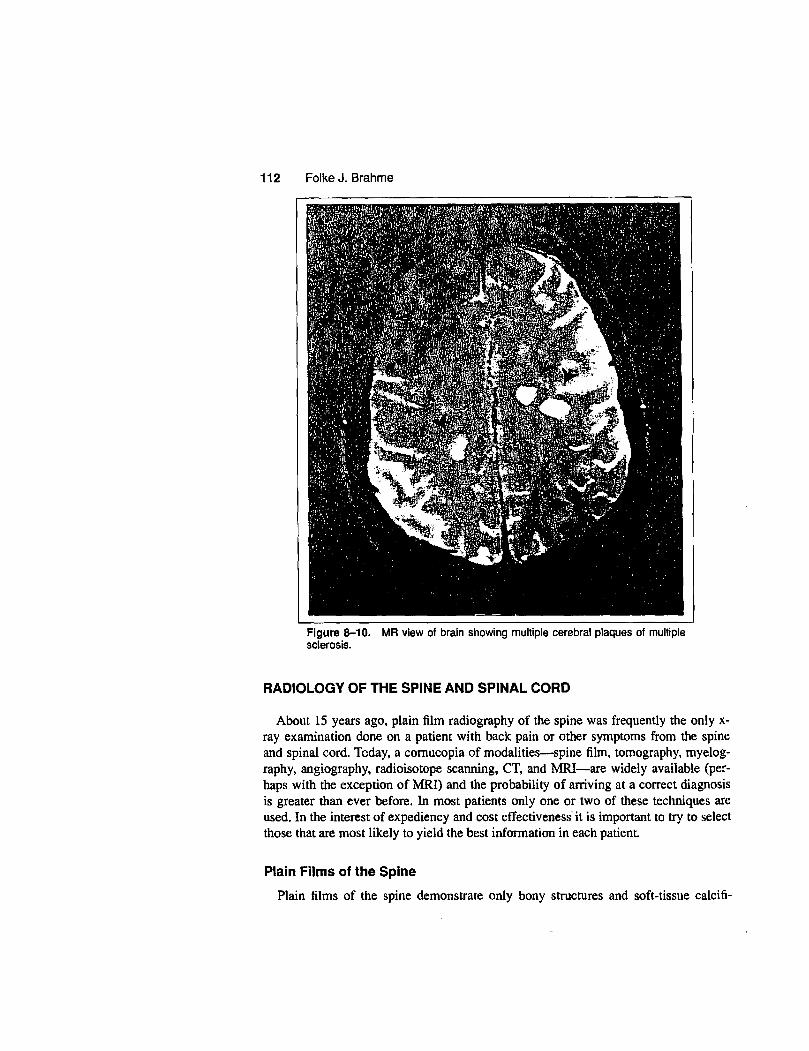
One of the more notable strengths of MRI lies in its ability to reveal abnormalitiesof the white matter. Small, but numerous, ischemic lesions of white matter are com-monplace in older persons; these are difficult to see on CT scans but are quite apparenton MRI. The white matter plaques of multiple sclerosis, only occasionally seen by CTin acute cases, are very obvious on MR scans whether they are new or old (Fig. 8-10) -`and the diagnosis may be confirmed by the findings of additional plaques deep in Thecerebellum and in the spinal cord.
The diagnostic limitation of MRI for diagnosis of CNS diseases is mainly its rela-tive inability to detect calcifications and to demonstrate fresh hematomas. Another dis-

in (coronal plane) showing a large
Neuroradiology 111
in whom no abnormalities have been ob-fled inflammatory foci are poorly seen by
tusions, hematomas, substance loss—areis at present better examined by CT. Freshme fragments are poorly seen by MRI. Inhed to respirators and monitoring devices;ian MR in the emergency situation..I lies in its ability to reveal abnormalitiesschemic lesions of white matter are corn-
to see on CT scans but are quite apparentle sclerosis, only occasionally seen by CTis whether they are new or old (Fig. 8-10)findings of additional plaques deep in the
;nosis of CNS diseases is mainly its rela-emonstrate fresh hematomas. Another dis-
Figure 8-9. MR scan of brain (sagittal plane) showing large ependymomaof cerebellum.
advantage, apart from the high cost of the equipment, is that contraindications to MRexamination exist for certain patient categories. Patients with surgically implantedmetallic devices should in many cases not be placed in the strong magnetic field of thescanner, and patients with ' pacemakers cannot be examined. Further, severely illpatients attached to monitors and other equipment with ferromagnetic componentscannot be examined. In spite of these shortcomings MR imaging represents a very realadvance in the diagnosis of diseases of the brain.
Magnetic resonance has for many years been successfully used for chemical andbiochemial analysis. Examination of metabolic abnormalities of the brain by MRspectroscopy is still in its infancy but there is not the slightest doubt that this modalitywill become a clinical reality within the next few years. The cost of an MR scan of thebrain is in the range of $700 to $900.
^R N /; 1 f clr :'; --4 1. ,• ^ s ^ 17i
r :I'L f .f[r4;Y;7 "Ye'
r{
r ti , r H;Ti Y ': K 4 P.`+ jt r i k e iy [YttiM"^.^-+
y' - li^ : 'l' '.-I^,^" ^'. X^'C' . 'I a 1 ul.- It 1 1:1 N'n,^f S y 'a^ T•,T l t .3 1,: q-.d Y ^. (' rrl . 3 ^t .t L.
L l 1 , J^' i^ 4:/, rs 1 t S3 a 3^ j v j l ;{>f1.r r ,. ^. ^'' t r ^ 1 3 l'1' R ^x l ^'_ I ^ _} ^Ii
1„ 1
f '^ S t rr .=1
•: i X r^s t i '^ ^ r .r ^ ^' :.- !- y^ , '
- erl'4M ^G'+ ';,r re •i ^} 1
^...
?, .t y ' 9S /f t:i 4 a LS< rj 1
.. l c L t 4 vr. F' SCI ۥ;^H r^l '..^,^^ r h :; ^ r^la3 ^;k^?^ l
-..
-^^>A^3 i71^"'a^1 [}+.;t{J^ i ^l.'yEt'^F^r^^lr ^j f r^:,'^^}}^.,,^k y';1,.^T^i ^r\.
lr r i l4 k•h+ '. r"^7^^fl^+.f'^.•'PiE^t, S..^I.r^. 1 .1'^y¢
yam , t 4 s x r ^ y 1 ^^ ^r j1 ^f t 7^^
r : ^l 1_ ^ ?^ l ^^ a ^,r ^ • a
rt nyS ^ S
cl
k•tl^ 1 ^ 1 i 7 q^ .z ^S ^7 ^" 11i>s° '^r7 [' _^cS li,. x 3: S .f _A in ' 1 ^ S ! _ 7 Y^. . I Pi 11 - ^5
N 4 i, r }' i r 1: - +t , F t < 1 c J' 1 ,f t f ^... i
j ; : 1.' r-. ^^r
^ti,,,.r^ a } a sy^s. '1^+^J^^[r "i ^^ rr+, k S '^Y ^4S JIJ,^IaI I
i q ^E \ ti 1A.
of ^r iv 't'- l^ ^ '+ ^,: 1 r :N 1, JN^^"^, e - [^•c 4 y, ,^f St,
1 r }r,i' 'c^ ,^^ r `r r rR 1rr
µvrt
fy^ t I"
i
^rk^„ 1 1P-,rr ^ •
sir i SN^ -. '.jl ^^,^ l . i i P 1 1
1[yl^;.
i I ^ LI
Wi^ ^ a
Y^ P^ ktltk^cr+
}!+1'7 N ^ 11^4^^^ t , [ o ^ ^ rf^'; ^ i, r• JI ?'h (^ a^ f q
0 (ff^j,^a1 '^'N. 1[f
5 t,l 4t '. I^ til j ^ 'l4 f^ $ ^ ^ f^^ p rr sit S. i
^^i s t ^1 ^'!^ i 'L 151 t } >3
G yFt ^s -1 s i,r _ 1
y 1i J l r {! ^q i .s^i E'e{'^ 3S` n^ t^
rS^ N. L
13 tt l:i yf ^
S^SG,^
`1 p;' s °^`arq'1 ^M1 -•yh
-,^r .
^ ^^ , n w ^i^ '^,^ ^ it ^ r^^^^'t 4^ [t^^ lrt E y^^^a ^^ ti
rd:Il^yf,x 'r i } . [ _,
'1 -y , C1 Ytt J'"^ IAti J„ J^ ;.
1 lt f: J. r; ,. I• I.. ^, k} 4 '; f' a q k'- f L r 1'r+a IBS y t A 1
J r^,^b^' w^71 .r E "^ brb.^r4`+'
^h` ^^. : _, ^ ,^• 1^, s i r 1•i ii'^ -h ^'! l^l.l, ^. }^f3,vn j•{t ^
Yk ter: Y '^ ^.1 X11 I ,ktr:vlLr nAf ^-"rt ^^^ '^ ^f^
,y ^. Z s. Y3y r t^ J^ PP[ 1 r. t ^'1 ^.{^.^^ ^^• lr : E r X114 ^^^ ^!°k'^. ^^0. ^ r ^ ^^^} ^^^k^ i' 'r'w^^'t tl ^th-:: ri 11 : . r j'A Jr h' T'}S
E A , '^h.e ^ 1 r -^.
{
^ 1 wl. ^' + r r s Y^ ^^'i^^k4 Id^7^ r [^iSFr^r
S til "s ^^` -^ Y.r'$ ^xry ^ ^}ivtrl kt [^. pp
..^ i e .
.E } ,'•; .,g 7b t^ b f i 5y `Yi W3 i i ^r r!r` " •: ,H j i f E e a+ ay a 3^^ q fir,
^,^ ' : ^ r .F,•n x • v^,s^^; d^' r ^^ ` r a h #F ^ 1 ^,,^ E^ Y iE ^ . .
. ; d Jiy ,} ' txr <^'n dx ,S ,rt .
I " '-'I
S 1 '^ 1.wr >'^ e ^y .> r'.Fw i t ^t} -^.' SS+ii ^i ?+ r7 yt r {
t t le ^S, ". s rdl , x1 ^ P Lei ^ e'^ ^-^ ^F{y r ^ X^, ^ ^^ / ^ +!i^tr L^ •" -
i'f S 1 4 r ^r^C^ ,^ti^M^^ ^Yf 1Y; +}+,• 1 Y,Y^ c.. r ^?• 1
'1iJ I 1 I..1;1'
- . .. .. .^...; r.ti..,., ^., i^ i, .:l^,: Ir.,, r. .o.3u. ... ... ,.r . .