second stage of labor: when to start and stop€¦ · second stage of labor: when to start and stop...
TRANSCRIPT

6/16/2017
1
Second Stage of Labor: When to Start and Stop
Aaron B Caughey, MD, PhDProfessor and Chair
Department of Obstetrics and GynecologyOregon Health & Science University
Financial Relationships
• No financial disclosures related to this talk• Medical Advisor to:
• Celmatix, Mindchild• Bob’s Red Mill
Objectives
� Second stage of labor� Epidemiology of second stage �Methodologic Challenges
�When to stop - how long is too long?�When to start� Delayed vs. Immediate Pushing
Question36 y.o. G1P0 at 40 wks GA with an epidural labored down for 1 hour (from 0 to +1) and now has pushed for 2 hours (from +1 to +2). What is the plan?
A. continue to push for up to 1 more hour
B. continue to push for up to 2 more hours
C. continue to push for up to 3 more hours
D. Begin conversation about OVDE. Begin conversation about cesarean
c o nt i n u
e t o p u s
h f or u p
t o .. .
c o nt i n u
e t o p u s
h f or u p
t o .. .
c o nt i n u
e t o p u s
h f or u p
t o .. .
B e gi n c
o n ve r s a
t i o n a b o
u t OV D
B e gi n c
o n ve r s a
t i o n a b o
u t ce . . .
40% 35%
6%6%12%

6/16/2017
2
Labor: Friedman Curve
First stage Secon d stage
Friedman EA. Primigravid labor. Obstet Gynecol 1955ACOG Practice bulletin. Dystocia and augmentation of labor. No 49; Obstet Gynecol 2003
� Second stage of labor� Nulliparas: 2 hours� Multiparas: 1 hour
Second Stage of Labor
� Hamilton – 1861 – suggested 2 hours as prolonged second stage� Duration of the second stage of labor� Nulliparas: 54 minutes � Multiparas: 19 minutes� Use of regional anesthesia increases the mean
duration of second stage by 25 minutes
Hamilton G. Classical observations and suggestions in obstetrics. Edinburgh Med J. 1861Zhang et al. Does epidural prolong labor & increas e risk of cesarean delivery. Am J Obstet Gynecol 2001Kilpatrick et al. Characteristics of normal labor. Obstet Gynecol 1989
Second Stage of Labor
� ACOG: Prolonged second stage of labor
� Nulliparas: 2 hours without regional anesthesia3 hours with regional anesthesia
� Multiparas: 1 hour without regional anesthesia2 hours with regional anesthesia
ACOG Practice bulletin. Dystocia and augmentation of labor. No 49; Obstet Gynecol 2003
Zhang: Labor Curve
� Second stage of labor in nulliparous women
Zhang J et al. Reassessing labor curve in nulliparou s women. Am J Obstet Gynecol 2002
StationTime (minutes)
1%ile Median 95%ile
+1 to +2 1 16 176
+2 to +3 1 7 38

6/16/2017
3
Second Stage of LaborFriedman Study
(n=500)Zhang Study
(n=1,162)
Year of data collection early 1950s 1992 - 1996
Birthweight 2.5-4.0kg 85 % 100 %
Induction of labor 4 % 0 %
Epidural anesthesia 8 % 48 %
Oxytocin augment. 9 % 50 %
Low forceps/vacuum 51 % 13 %
Zhang J et al. Reassessing labor curve in nulliparou s women. Am J Obstet Gynecol 2002Friedman EA. Primigravid labor. Obstet Gynecol 1955
Studying the Second Stage
Studying the Second Stage Second Stage of Labor
� Challenges of studying labor duration
� Non-normal distribution�Median, 95 th centile

6/16/2017
4
2nd Stage of Labor: Nulliparas
0
25
50
100
0 2 4 6 8 10
Second Stage of Labor (hour)
Per
cent
Pre
gnan
t
EpiduralNo Epidural
p<0.001 by Log-rank
Cheng YW, et al. The second stage of labor and epidural use: a larger effect than previously suggested. Obstet Gynecol. 2014
2nd Stage of Labor: Multiparas
0 2 4 6 8 10
0
25
50
100
Second Stage of Labor (hour)
Per
cent
Pre
gnan
t
EpiduralNo Epidural
p<0.001 by Log-rank
Cheng YW, et al. The second stage of labor and epidural use: a larger effect than previously suggested. Obstet Gynecol. 2014
Median 95%ile
NulliparasNo Epidural
50 min 201 min
NulliparasEpidural
126 min 339 min
MultiparasNo Epidural
14 min 84 min
MultiparasEpidural
40 min 262 min
Results: Second stage of labor
p<0.001
138 min
Cheng YW, et al. The second stage of labor and epidural use: a larger effect than previously suggested. Obstet Gynecol. 2014
Second Stage of Labor:How long is too long?
� Hard to even know the natural course� Particularly with epidural
� What about outcomes with shorter or longer second stage?� How do interventions improve these
outcomes?
6/16/2017
5
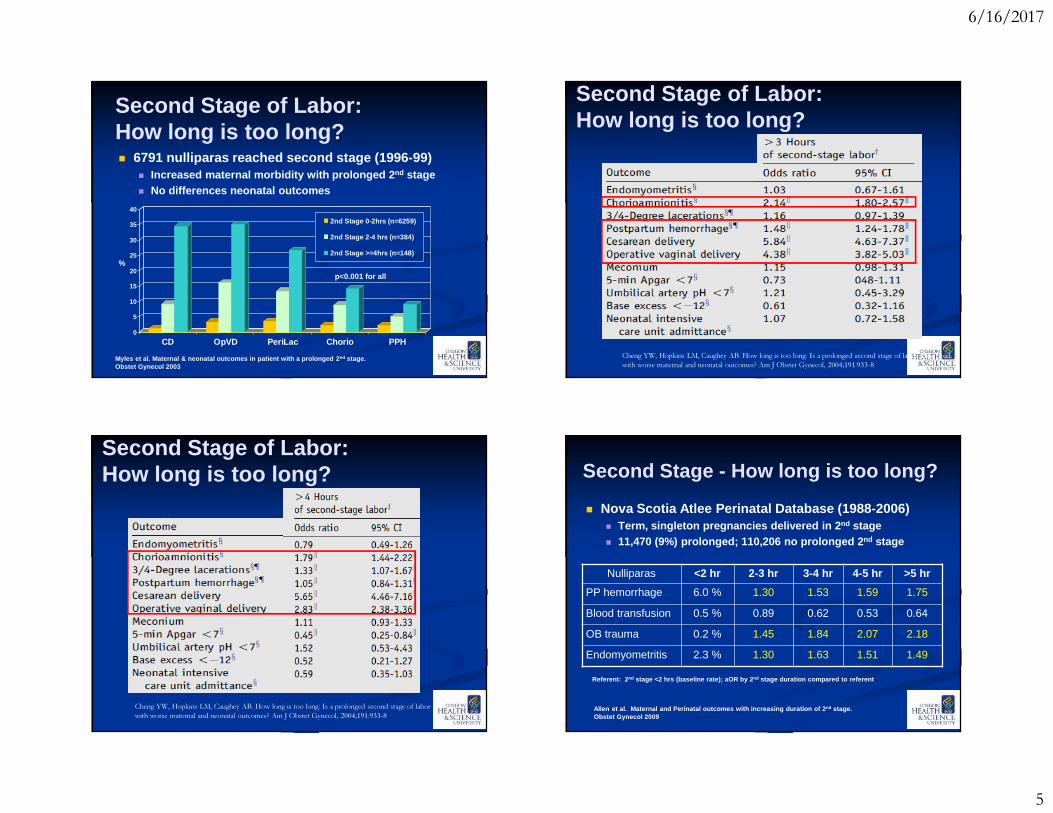
Second Stage of Labor:How long is too long?� 6791 nulliparas reached second stage (1996-99)� Increased maternal morbidity with prolonged 2 nd stage� No differences neonatal outcomes
0
5
10
15
20
25
30
35
40
CD OpVD PeriLac Chorio PPH
2nd Stage 0-2hrs (n=6259)
2nd Stage 2-4 hrs (n=384)
2nd Stage >=4hrs (n=148)
%
p<0.001 for all
Myles et al. Maternal & neonatal outcomes in patien t with a prolonged 2 nd stage. Obstet Gynecol 2003
Cheng YW, Hopkins LM, Caughey AB. How long is too long: Is a prolonged second stage of labor associated with worse maternal and neonatal outcomes? Am J Obstet Gynecol, 2004;191:933-8
Second Stage of Labor:How long is too long?
Cheng YW, Hopkins LM, Caughey AB. How long is too long: Is a prolonged second stage of labor associated with worse maternal and neonatal outcomes? Am J Obstet Gynecol, 2004;191:933-8
Second Stage of Labor:How long is too long? Second Stage - How long is too long?
� Nova Scotia Atlee Perinatal Database (1988-2006)� Term, singleton pregnancies delivered in 2 nd stage� 11,470 (9%) prolonged; 110,206 no prolonged 2 nd stage
Allen et al. Maternal and Perinatal outcomes with increasing duration of 2 nd stage. Obstet Gynecol 2009
Nulliparas <2 hr 2-3 hr 3-4 hr 4-5 hr >5 hr
PP hemorrhage 6.0 % 1.30 1.53 1.59 1.75
Blood transfusion 0.5 % 0.89 0.62 0.53 0.64
OB trauma 0.2 % 1.45 1.84 2.07 2.18
Endomyometritis 2.3 % 1.30 1.63 1.51 1.49
Referent: 2 nd stage <2 hrs (baseline rate); aOR by 2 nd stage duration compared to referent
6/16/2017
6
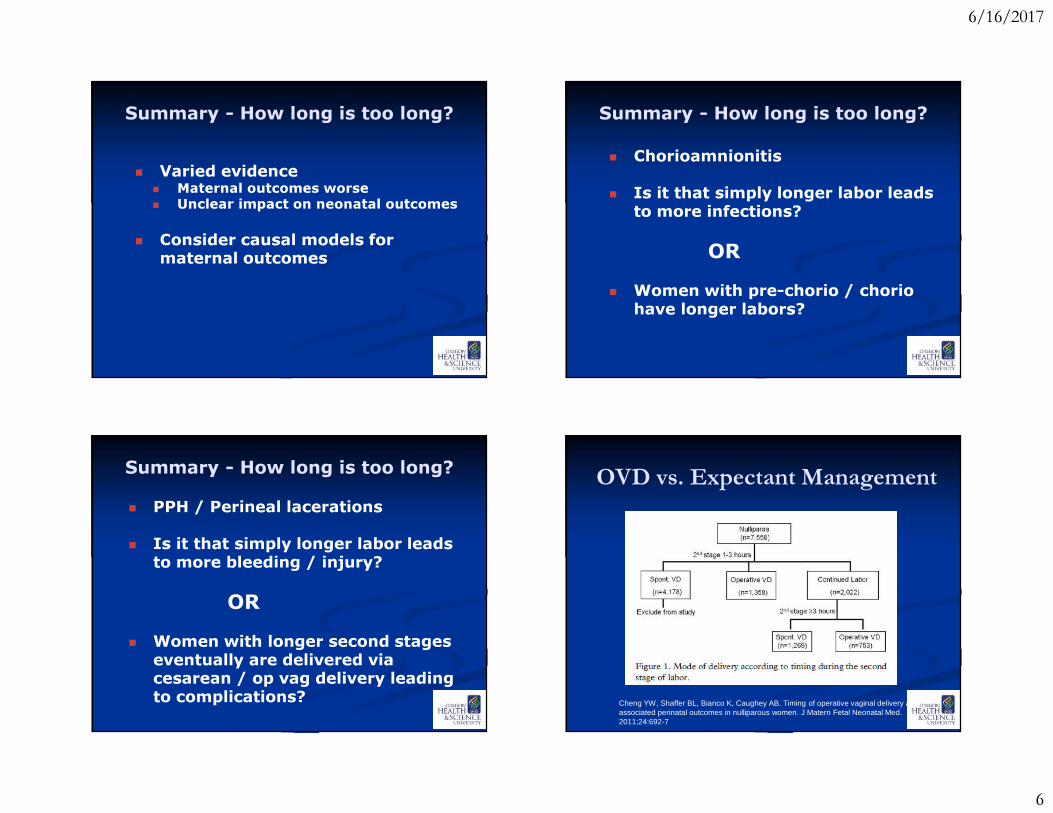
Summary - How long is too long?
� Varied evidence� Maternal outcomes worse� Unclear impact on neonatal outcomes
� Consider causal models for maternal outcomes
Summary - How long is too long?� Chorioamnionitis� Is it that simply longer labor leads
to more infections?
OR� Women with pre-chorio / chorio
have longer labors?
Summary - How long is too long?� PPH / Perineal lacerations� Is it that simply longer labor leads
to more bleeding / injury?
OR� Women with longer second stages
eventually are delivered via cesarean / op vag delivery leading to complications?
OVD vs. Expectant Management
Cheng YW, Shaffer BL, Bianco K, Caughey AB. Timing of operative vaginal delivery and associated perinatal outcomes in nulliparous women. J Matern Fetal Neonatal Med. 2011;24:692-7

6/16/2017
7
OVD vs. Expectant Management
Cheng YW, Shaffer BL, Bianco K, Caughey AB. Timing of operative vaginal delivery and associated perinatal outcomes in nulliparous women. J Matern Fetal Neonatal Med. 2011;24:692-7
How long is too long? - Summary� If progress is being made, duration of the 2nd stage alone
DOES NOT mandate intervention by operative delivery.
� A specific absolute maximum length of time spent in second stage of labor beyond which all women should undergo operative delivery has not been identified.
� Before diagnosing arrest of labor in second stage, if maternal and fetal conditions permit, allow for following: � At least 2 h of pushing in multiparous women� At least 3 h of pushing in nulliparous women
� Longer durations may be appropriate on individualized basis (eg, with use of epidural analgesia or withfetal malposition).
ACOG / SMFM, Caughey AB, Cahill AG, Guise J-M, Rouse DJ. Obstetric Care Consensus Document No. 1. Safe Prevention of the Primary Cesarean Delivery. Obstet Gynecol. 2014 Mar;123:693-711.
‘Prolonged’ Second Stage Question – When to Start?36 y.o. G1P0 at 40 wks GA with an epidural
labored down is at 0 station. What is the plan?
A. Labor down until urge to pushB. Labor down for up to 2 hoursC. Discuss options of pushing and
laboring down with patientD. Start pushing
L a bo r d
o w n u n t
i l u rg e t
o p us h
L a bo r d
o w n f o r
u p t o 2
h o ur s
D i s cu s s
o p ti o n s
o f pu s h
i n g . . .
S t a rt p u
s h i ng
25%
8%
47%
20%

6/16/2017
8
Delayed Pushing – “Laboring Down”
� Brought to us by the epidural� Facilitated by the loosening of the
“3 hour” rule for second stage� Attempts to address the
association between epidural and operative vaginal deliveries
Delayed Pushing - PEOPLE� Largest RCT is the PEOPLE study
(Pushing Early or Pushing Late with Epidural)
� Multi-site trial from Canada, et al. with a total of 1862 nulliparouswomen randomized into two groups
� “Delay” = ~2 hrs Fraser et al. Multicentered, RTC of delayed pushin g for nulliparas in the second stage with continuous epidural analgesia. Am J Obstet Gynecol 2000
Delayed Pushing - PEOPLE
� PEOPLE: 1,862 with epidural;1994-1996
Fraser et al. Multicentered, RTC of delayed pushin g for nulliparas in the second stage with continuous epidural analgesia. Am J Obstet Gynecol 2000
Delayed Push (n=926)
Early Push(n=936) RR 95% CI
Duration 2nd stage (min) 187min (86-314)
123min (49-248)
----
“Difficult” deliveryMidpelvic proceduresLow-pelvic procedureCesarean delivery
17.8 %9.3 %3.5 %5.0 %
22.5 %13.0 %
3.8 %5.7 %
0.79 0.66-0.950.72 0.55-0.930.93 0.58-1.490.88 0.60-1.29
Other OVD 24.5% 24.3% NS
Delayed Pushing - PEOPLE
� Maternal Outcomes
Fraser et al. Multicentered, RTC of delayed pushin g for nulliparas in the second stage with continuous epidural analgesia. Am J Obstet Gynecol 2000
Delayed Push (n=926)
Early Push(n=936)
RR (95% CI)P value
3rd/4th degree lac 9.3 % 9.5 % NS
Fever (38’ C) 8.5% 4.5% 1.88 (1.31-2.71)
EBL>500ml 17.6 % 16.8 % NS

6/16/2017
9
Delayed Pushing - PEOPLE
� Neonatal Outcomes
� No difference – Respiratory, blood cultures, fractures, Apgars
Fraser et al. Multicentered, RTC of delayed pushin g for nulliparas in the second stage with continuous epidural analgesia. Am J Obstet Gynecol 2000
Delayed Push (n=926)
Early Push(n=936)
RR (95% CI)P value
Abnormal uapH (<7.10) 4.5% 1.8% 2.45 (1.35-4.43)
Ventilation 6.9% 6.3% NS
Delayed Pushing - Meta
� Delayed pushing vs. Active pushing� Meta-analysis of 7 RCTs (n=2,827)
Relative Risk 95% CI
Spontaneous VD 1.08 1.01 – 1.15
Operative VD 0.77 0.77 – 0.85
Cesarean delivery 0.80 0.57 – 1.12
Duration of pushing (hrs) -0.19 -0.27 – -0.12
Perineal lacerations 0.88 0.72 – 1.07
Episiotomies 0.97 0.88 – 1.06
Broncato et al. A meta-analysis of passive descent versus immediate pushing in nulliparous women with epidural analgesia in the 2 nd stage of labor. J Obstet Gynecol Neonatal Nurs 2008
Summary: Second Stage of Labor
� Delayed vs. Active� Sounds good� Data are mixed� Is benefit only achieved in settings of poor patien ce?� Potential tradeoffs between:�Mode of delivery� Fever / pH� ? Pelvic floor
Optimizing Management of the Second Stage of Labor
To assess the effectiveness of immediate vs. delayed pushing at complete cervical dilation in nulliparous women on:
1) Rate of spontaneous vaginal delivery2) Composite neonatal morbidity, and3) Maternal pelvic floor dysfunction

6/16/2017
10
Optimizing Management of the Second Stage of Labor
Study Sites:1) Washington University (Cahill, Tuuli)2) UAB (Tita)3) U Penn (Srinivas)4) OHSU (Caughey)
Enrolling 3200 women - 2014-2018
Future Research Directions
� Large, prospective, observational, multicenter study of second stage
� Prospective, interventional trials:� Prolonged second stage definitions� 3 hours vs. 4/5/6 hours
� Epidural use / regimens� Manual rotation / Operative vaginal delivery� Etc.
Question36 y.o. G1P0 at 40 wks GA with an epidural labored down is at 0 station. What is the plan?
A. Labor down until urge to pushB. Labor down for up to 2 hoursC. Discuss options of pushing and
laboring down with patientD. Start pushing
L a bo r d
o w n u n t
i l u rg e t
o p us h
L a bo r d
o w n f o r
u p t o 2
h o ur s
D i s cu s s
o p ti o n s
o f pu s h
i n g . . .
S t a rt p u
s h i ng
5%15%
73%
7%
How long is too long?
Friedman E, Sachtleben M. Dysfunctional Labor II. Obstet Gynecol . 1961;17:566-78

6/16/2017
11
How long is too long?
Friedman E, Sachtleben M. Dysfunctional Labor II. Obstet Gynecol . 1961;17:566-78
Thank You
Thank You
No negative neonatal effects with inc duration AFTER controlling for confounding factors
Maternal Morbidity inc sig after 2 hours for IP fever, and PPH

6/16/2017
12
� Secondary Analysis of Fetal Pulse OxTrial� Nulliparous women N=5341� 96% epidural use, 87% oxytocin use, 38.6% IOL
� 75% NSVD, 18.5% OVD, 7.4% CD� In >3 hours of 2nd Stage labor, increased risk for: � Chorioamnionitis� 3rd & 4th deg lacerations� PPH (atony) � No negative neonatal outcomes
0
2
4
6
8
10
12
14
0-2 Hours (n=4662)
2-3 Hours (n=550)
>=3 Hours (n=257)
Second Stage of Labor� 5158 multiparas reached second stage (1991-2001)� Increased maternal complications� Increased neonatal morbidity
%
5minApgar<7 UA pH<7.0 NICU Neo M orbidity Prolong Hosp
Cheng et al. Duration of 2 nd stage of labor in multiparous women. Am J Obstet Gynecol 2007
p<0.001 p<0.001
p=0.002
p=0.006
p=0.015
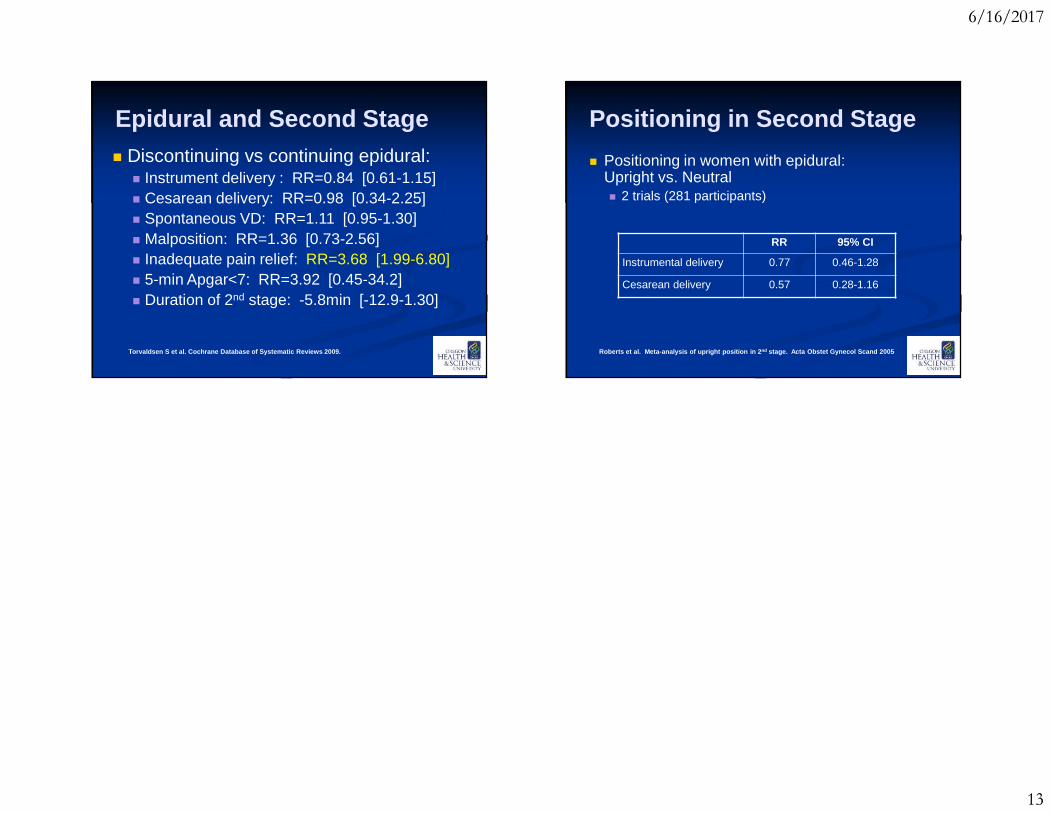
Epidural and Second Stage� Cochrane Systematic Review � 5 RCTs (462 participants)
� Assess impact of discontinuing epidural on:� Rates of instrumental delivery and outcomes� Analgesia and satisfaction with labor care
Torvaldsen S et al. Cochrane Database of Systematic Reviews 2009.
6/16/2017
13
Epidural and Second Stage� Discontinuing vs continuing epidural: � Instrument delivery : RR=0.84 [0.61-1.15]� Cesarean delivery: RR=0.98 [0.34-2.25]� Spontaneous VD: RR=1.11 [0.95-1.30]� Malposition: RR=1.36 [0.73-2.56]� Inadequate pain relief: RR=3.68 [1.99-6.80]� 5-min Apgar<7: RR=3.92 [0.45-34.2]� Duration of 2nd stage: -5.8min [-12.9-1.30]
Torvaldsen S et al. Cochrane Database of Systematic Reviews 2009.
Positioning in Second Stage
� Positioning in women with epidural: Upright vs. Neutral� 2 trials (281 participants)
RR 95% CI
Instrumental delivery 0.77 0.46-1.28
Cesarean delivery 0.57 0.28-1.16
Roberts et al. Meta-analysis of upright position i n 2nd stage. Acta Obstet Gynecol Scand 2005