self-management procedures: a comparison across -
TRANSCRIPT

Self-Management Procedures: A Comparison across theAutism Spectrum
Candice M. Southall and David L. GastThe University of Georgia
Abstract: Individuals with autism spectrum disorders (ASD) have difficulty generalizing learned behavior tovaried environments with independence. This review of 24 empirical studies compares self-management as asystematic procedure for modifying one’s own behavior, to increase target behaviors in students with eitherautistic disorder (AD) or high-functioning autism/Asperger’s syndrome (HFA/AS). Twenty-four single subjectresearch studies are included in the review comparing methodological, demographic, procedural, and outcomeaspects of self-management studies between the two disorders under the umbrella of Pervasive DevelopmentalDisorder (PDD). Results show that self-management procedures, regardless of components and age of child, areeffective in teaching social, vocational, and communication skills, or decreasing restrictive and repetitivepatterns of behaviors for individuals with a PDD. General conclusions are made on how the procedures are useddifferently across levels of functioning within the autism spectrum and PDD. This literature should encourageresearchers and practitioners to continue interventions using self-management procedures with this populationto broaden the research base and improve methodological adequacy.
Empirically based interventions geared towardstudents with a disability can increase inde-pendence and inclusion within schools andsociety (Cooper, Heron, & Heward, 2007).Federal mandates of least restrictive environ-ments for students meeting eligibility criteriafor special education services have increasedinclusion of children within general educa-tion alongside their peers. According toCampbell (2006), “As children with autismcontinue to be educated alongside typicallydeveloping children, professionals must con-tinue to understand how best to educate achild with autism in an inclusive educationalsetting” (p. 268). Students with an autism spec-trum disorder (ASD) often have academic ca-pabilities equal to peers but require directinstruction on behaviors to increase successin mainstreamed environments. Empirically-based strategies must be made available topractitioners for use to increase desired be-haviors by individuals with ASD. Researchers
must also be persistent in their search forresearch-based, generalizable strategies foruse in inclusive environments.
Autism Spectrum Disorders: A Brief History
Kanner (1943) described a peculiar conditionhe found across a number of children in aseminal clinical description (cited in Kanner,1985). The first label of the disorder, infantileautism, was presented in this report. HereKanner asserted that the 11 children observedhad been labeled as “Emotionally Disturbed”or “Mentally Retarded” but displayed no char-acteristics of a slow learner nor fit the profileof emotional problems. The common charac-teristics encompassed across the case studiesincluded a desire for aloneness, sameness,stereotypy, and exhibited functional commu-nication and language delays (Rimland,1985). Based primarily on the work of Kannerand others whom he influenced, the Ameri-can Psychiatric Association included diagnos-tic criteria for autistic disorder (AD) for thefirst time in the third edition of the Diagnosticand Statistical Manual of Mental Disorders(DSM-III, American Psychiatric Association,1980).
Correspondence concerning this article shouldbe addressed to Candice M. Southall, Departmentof Communication Sciences and Special Education,University of Georgia, 516 Aderhold Hall, Athens,GA 30602-7153.
Education and Training in Autism and Developmental Disabilities, 2011, 46(2), 155–171© Division on Autism and Developmental Disabilities
Self-Management Procedures across the Spectrum / 155

In 1944, an Austrian doctor, Hans Asperger,described children with what he called autisticpsychopathy (Wing, 1981). Although the chil-dren spoke at a normal age, Asperger foundimpairment in social communication, similarto that described by Kanner. In 1981, LornaWing’s translation of Asperger’s report be-came widely known in the U.S. Wing ex-plained that although the two conditions de-scribed by Kanner and Asperger appearedremarkably similar it was debated whether thedisorders were “varieties of the same under-lying abnormality or are separate entities”(Wing, 1981, p. 115). Discrepancies betweenclinical features based on Asperger’s work, astranslated by Wing, and Kanner’s work led todiscussion of a separate Autism Spectrum Dis-order (ASD) subtype.
In 1994, the Diagnostic and Statistical Manualof Mental Disorders, fourth edition (DSM-IV;American Psychiatric Association, 1994) estab-lished Asperger syndrome (AS) as one of fivepervasive developmental disorders (PDD). Ac-cording to diagnostic criteria, AS is differenti-ated from AD in that there is no delay inlanguage or cognitive development, and noqualitative impairment in the communicationdomain. Witwer and Lecavalier (2008)showed that some children with AS, underdiagnosis of the Autism Diagnostic Interview-Revised (ADI-R) and Autism Diagnostic Ob-servation Schedule (ADOS) displayed coresymptoms of autism while also having highfull-scale intelligence quotients (IQ). Indeed,approximately 33–59% of children with ASDhave cognitive deficits (� 70 IQ) according tothe Center for Disease Control (2007), how-ever, some children diagnosed with AD ulti-mately display fewer autistic behaviors whilealso having higher IQ and language skills(Ozonoff & Rogers, 2003). These children arecommonly referred to as having high-func-tioning autistic disorder (HFA) (Macintosh &Dissanayake, 2004; Witwer & Lecavalier, 2008).A commonality between AS and HFA are im-pairments in social interactions, restrictiveand repetitive patterns of behavior, interestsand activities; and significant impairment insocial, occupational and other areas of func-tioning (Thede & Coolidge, 2007). Studentswith HFA require a different educationaltreatment approach than persons with ADdue to differences in cognitive ability. This
treatment approach would be more similar tointerventions for children with AS. Since thedistinction between AD and AS remains con-troversial, and some researchers assert thatAS is a milder form of AD along a continuum(Campbell & Morgan, 1998), this review willrefer to HFA as separate from AD and com-bine HFA and AS simply as HFA/AS.
Kanner (1943) purported that these chil-dren within his seminal clinical description ofchildren with autism were not “mentally re-tarded” but displayed poor performance ex-plained by motivational factors. While re-search over the years show below average fullscale IQ for the nearly half of children withAD assessed through developmentally appro-priate tests, it is now accepted that althoughcognition is a deficit for many people withautism, abilities are unusually scattered withnonverbal skills more advanced than verbalskills, with motivation playing a integral rolein performance (Volkmar & Klin, 2005, p. 8).Definitions in the DSM-IV-TR (2000) classify-ing autism subtypes, AD and AS, are generalguidelines of diagnosis for psychologists todetermine appropriate interventions and ed-ucational placement. It is critical to examineempirically-based interventions that increasemotivation and learning in individuals withASD as well as differentiate effectiveness ofinterventions for those identified as AD versusHFA/AS.
Self-Management
Combining empirically-based interventionssuch as differential reinforcement proceduresand naturalistic approaches (Pivotal ResponseTreatment [PRT], incidental teaching, etc.)has been shown to increase desired behaviorsof people with ASD (Koegel, L., Koegel, R.,Harrower, & Carter, 1999; Ozonoff, Rogers, &Hendron, 2003; Scheuermann & Webber,2002). Not only does motivation play into theperformance of people with ASD, these indi-viduals can learn or adopt strategies that willassist in their education, employment, and so-cial life with increased self-awareness (Myles &Southwick, 1999). In accordance with PRT,motivation is critical to learning by childrenwith ASD, as is self-regulation and autonomy.Neurotypical children exhibit the ability togeneralize newly learned behaviors to novel
156 / Education and Training in Autism and Developmental Disabilities-June 2011

situations and, unlike children with ASD, theyare responsive to environmental cues that leadto their independence. Koegel et al. identifyself-management as a pivotal area of interven-tion for individuals with ASD. They assert thatchildren on the autism spectrum can betaught to discriminate between appropriateand inappropriate behaviors through self-management instructional programs.
Self-management strategies are designed toteach individuals to engage in actions thatchange or maintain a particular behavior(Shapiro, 1981). Within the self-managementparadigm, a specific aspect of a behavior istargeted and individuals are taught to recordthe target behavior when it occurs (Cole &Bambara, 1992). Self-management procedurestypically comprise any combination of self-monitoring (also known as self-observation),self-recording, self-evaluation, and self-rein-forcement or self-punishment. Self-monitor-ing requires the individual to determine theoccurrence or non-occurrence of target be-haviors, which often include self-questioning.For example, at the end of a given time pe-riod, the student may ask, “Am I paying at-tention?” A judgment about the occurrenceor nonoccurrence of the target behavior ismade as the individual records the answerdetermined from self-monitoring by physicallymarking these results on a data collectionform, taking a token, or using a countingdevice (self-recording). The self-evaluationcomponent combines goal setting and deter-mining achievement of the goal. Lastly, self-reinforcement, or self-punishment, is the con-tingent self-delivery of an earned reward, orwith self-punishment, the self-withholdingof the reinforcer. This differential reinforce-ment component is implemented to increasethe likelihood of students engaging in thetarget behavior in the future under self-man-agement procedures.
Cooper et al. (2007) identified a number ofadvantages of self-management over other be-havioral interventions including (a) minimalteacher management along with more timeto teach, (b) greater generality of behaviorchange by the student, and (c) application ofstrategy in varied environments. Executivefunction can be thought of as the cognitivesystem that controls other cognitive processes
including set-shifting, inhibition of responses,self-monitoring, and planning (Happe, Booth,Charlton, & Hughes 2006). Self-reflection andself-monitoring are specific deficits in execu-tive functioning by individuals on the autismspectrum. Also, many inappropriate behaviorsemitted by students with ASD are difficult tocontrol because of poor outcomes (i.e., peerdisapproval). Self-management can serve asa consequence by restricting stimulus condi-tions for undesirable behavior. For example, aclassic study by Koegel, Koegel, Hurley, andFrea (1992) used self-management with fourmale participants diagnosed with autism whowere unresponsive to teacher and parent ver-bal initiation. Each participant had receptiveand expressive language at or above the3-year-old level and exhibited behavior diffi-culties (e.g., tantrums). A multiple baselinedesign across settings and participants com-bined with a withdrawal for two participantswas used to evaluate the effects of self-obser-vation, self-recording, and self-reinforcement.Yes and no questions were created prior to thestudy related to children’s regular activities.Difficulty levels were controlled. During train-ing in the clinic, researchers modeled appro-priate answers to questions and modeled howto record the response on a wrist counter.Researchers followed the same protocol forunacceptable answers to questions and mod-eled not counting on the counter. The wristcounter was worn by children during role-playsessions. At this point, children were rein-forced after every correct response, i.e., CRF.Prompts ware faded after three hours of treat-ment. Self-management procedures were im-plemented at school, in the community, andin home environments. Data were collectedduring all sessions for appropriate and inap-propriate responses, disruptive behavior, andaccuracy of self-recording. Interobserveragreement data were collected throughoutthe study. It was concluded that self-manage-ment procedures were successful in increasingsocial responses by students with autism invaried environments as well as required mini-mal teacher presence. Researchers also founda collateral reduction in disruptive behaviorsdue to possible increased communicationskills and a decreased aversion during socialinteraction.
Lee, Simpson, and Shogren (2007) pub-
Self-Management Procedures across the Spectrum / 157

lished a meta-analysis of the effects of self-management for students with autism. Thisreport analyzed effect size of single subjectresearch on self-management proceduresused to increase target behavior published be-tween 1992 and 2001. They found that self-management procedures have an empower-ing effect on students’ ability to controlbehavior. They concluded that self-manage-ment procedures will facilitate inclusion inthe general curriculum, as well as increasestudents’ self-determination, thus improvingtheir quality of life.
General education teachers report high ac-ceptability of self-management procedures,preferring student monitoring to teachermonitoring because it frees teachers to per-form other instructional and related activities(Prater & Hogan, 1992). Agran, Snow, andSwanner (1999), however, reported that self-monitoring instruction is limited in appliedsettings and is provided by only 35% of specialeducators. At this point, it is imperative thatself-management research be analyzed to de-termine which dimensions of the interven-tions were effective and with what types ofindividuals so educators will be to ascertainthe effectiveness of self-management proce-dures with students on the autism spectrum.
While it is not a common practice in edu-cational settings, experts in the area of ASDadvocate for use of self-management proce-dures (Wilkinson, 2005). The primary pur-pose of this literature review is to examineself-management procedures as an interven-tion for individuals ages 3–25 with ASD fromJanuary 1994 to December 2008. This reviewcompares demographics, procedures, and re-sults of self-management interventions foundin the literature between individuals with ADand HFA/AS. Lastly, this review identifies di-mensions of self-management programs thatneed further research.
Method
To identify empirical studies investigating theeffectiveness of self-management proceduresfor students with AD and HFA/AS publishedover the last 15 years, three types of searchmethods were used (Wolery & Lane, 2010).An electronic search was conducted throughERIC, Academic Search Complete, Science
Direct, and PsycINFO using the advancedsearch method with key terms “self-manage-ment,” “self-monitoring,” “self-recording,”“self-reinforcement,” “autism,” and “Aspergersyndrome.” The text was searched in eacharticle identified with related keywords. Sec-ondly, a hand search of common journalspublishing articles describing interventionsfor the population of interest was conducted.These included the Journal of Applied BehaviorAnalysis, Journal of Autism and DevelopmentalDisorders, Focus on Autism and Developmental Dis-orders, Education and Training in DevelopmentalDisabilities, and Behavioral Disorders. The thirdmethod for searching literature was an ances-tral search of references cited in articles cho-sen through electronic and hand search. Inconsideration of which studies to accept forthis review, criteria included: (a) at least oneparticipant in the study was identified as hav-ing a pervasive developmental disorder (PDD)including AD, AS, or pervasive developmentaldisorder—not otherwise specified (PDD-NOS);(b) intervention included an independentvariable using a procedure that required astudent to take responsibility for behaviorthrough any one or more self-monitoring,self-recording, and self-reinforcement proce-dures; (c) studies were published in a peer-reviewed journal between January 1994 andDecember 2008; and (d) a single-subject re-search design (Gast, 2010) was used to evalu-ate intervention effectiveness.
Results
The search resulted in 16 studies published in11 different journals that targeted behaviorsof students with AD and eight studies fromfive different journals that targeted behaviorsof student with HFA/AS using self-manage-ment procedures: Journal of Applied BehaviorAnalysis (1), Journal of Autism and DevelopmentalDisorders (2), Behavioral Disorders (1), BehavioralInterventions (3), Education and Training in De-velopmental Disabilities (1), Education and Train-ing in Mental Retardation and Developmental Dis-abilities (4), Journal of Emotional and BehavioralDisorders (1), Focus on Autism and Other Devel-opmental Disabilities (2), Journal of Intellectualand Developmental Disability (1), InternationalJournal of Disability (1), Journal of Developmentand Education (1), Journal of Positive Behavior
158 / Education and Training in Autism and Developmental Disabilities-June 2011

Interventions (3), Journal of Developmental andPhysical Disabilities (2), Autism: The InternationalJournal of Research and Practice (1), and SchoolPsychology Quarterly (1). Tables 1 and 2 sum-marize pertinent descriptors of each study in-cluding: research design, participant gender,chronological age, diagnosis, setting, and tar-get behavior. Five studies included individualswith a disability other than AD or HFA/AS.For these studies, research methodology, de-
mographic, procedural, and outcome vari-ables are examined for students with an ASD.
Single Subject Research Methodology
The merits of studies can be evaluated withinthe context of single subject research designs.Withdrawal designs provide a demonstrationof experimental control by withdrawing anintervention and returning to a previous base-line condition showing a replication of effect
TABLE 1
Descriptors of Self-Management Studies for Individuals with AD
Authors SS design Gender CADiagnosis/
Functioning Setting Behavior
Agran et al.(2005)
Multiple baselineacrossparticipants
2/males 14 Autism � MIID(NS)
General educationclassroom
% steps ofdirectionsfollowed
15
Coyle & Cole(2004)
A-B-A for twoparticipants
3/males 11 Autism� ID-DSM-IV
Special educationclassroom
Time off-task9
A-B-A-C-A foroneparticipant
9
Embregts(2002)
A-B-A-B 1/male 16 PDD � ADHD� MIID-DSMIV
Residential Setting Frequency ofAppropriatebehavior &Inappropriatebehavior
Ganz &Sigafoos(2005)
ChangingCriterionDesign acrosstwoparticipants
2/males 20 Autism�MoID-School eval.
Self-containedvocationalschool
# of taskscompleted in5 minutes
19
Hughes et al.(2002)
Multiple baselineacrossparticipants
1/male 19 Autism�SID-(NS)
Inclusive highschool in hall
% of correctresponses
Kern et al.(1997)
Multiple baselineacross settingswith awithdrawalimbeddedwithin the firstsetting.
1/male 14 Autism�6grade levelsbelow-(NS)
Rehabilitationhospital
% time withinappropriatevocalizations
Mancina etal. (2000)
Multiple baselineacross settings
1/female 12 Autism�MoID-Schooleligibility
Special educationclassroom
% occurrence ofvocalizations
Newman etal. (1995)
Multiple baselineacrossparticipants
3/males 14 Autism�MIDto MoID-DSM-III-R
ASD after-schoolprogram
# transitionidentified16
17Newman et
al. (1996)A-B-C-A-C across
threeparticipants
3/males teen Autism�ID-Independentevaluation
Integrated schoolin separateroom
% appropriateconversation
Self-Management Procedures across the Spectrum / 159

(Gast & Hammond, 2010). Four (17%) self-management studies for individuals with ASDused a withdrawal design. Changing criteriondesigns evaluate shaping behaviors that arecurrently in an individual’s repertoire provid-ing evidence of experimental control throughsmall increases toward a criterion (Gast &Ledford, 2010). Changing criterion designswere used in three (12.5%) of the studies. Themost common designs to evaluate self-man-agement treatment packages with individualswith ASD were multiple baseline and multipleprobe designs. Their designs show experimen-tal control by first collecting pre-intervention
data across three or more tiers, then stagger-ing the introduction of the intervention acrossparticipants, behaviors, or conditions. Fivestudies (21%) used a multiple baseline acrossbehaviors to evaluate experimental control.Three staggered intervention implementationacross settings (12.5%). Multiple baseline de-sign across participants was used in nine stud-ies (37%).
Procedural Fidelity
Billingsly, White, and Munson (1980) intro-duced the importance of measuring proce-
TABLE 1—(Continued)
Authors SS design Gender CADiagnosis/
Functioning Setting Behavior
Newman et al.(1997)
Multiple baselineacrossparticipants(possiblenoncontingent)
2/males 12 Autism� ID-DSM-IV
ASD after-schoolprogram
% intervals withtarget behavior
1/female 4 -out of seat6 ASD Preschool
Bedroom-nail-flicking
Newman et al.(2000)
Multiple baselineacrossparticipants
2/males 6/PS Autism�MID-DSM-IV
Evan and Nancy-ASD school Dan-home
Degree ofvariations inindividualtargetedbehaviors
1/female 6
Pierce &Schriebiman(1994)
Multiple baselineacrossbehaviorsreplicatedacross threeparticipants
3/males 8 Autism�MoIDto SID-Outsideagency
Clinic room % of 10-s intervalsengaged in on-task behavior &inappropriatebehavior
96
Reinecke et al.(1999)
A-B-A-B acrossthreeparticipants
3/males 4 Autism�MID/MOID (NS)
Preschool (NS) Social and playskills in theform of“sharing”
43
Shabani et al.(2001)
Multiple baselineacross twobehaviors.
1/male 12 Autism � ID�ADHD-(NS)
Univ. therapyroom
% of intervalsrocking
Strain &Kohler(1994)
Multiple baselineacrossparticipantsand settings.
3/males 4 Autism�NS-DSM-III
Integratedpreschool Smallroom Home (2)
% of intervalsengaged insocialinteraction
53
Todd & Reid(2006)
ChangingCriterionDesign acrossthreeparticipants
3/ males 16 Autism�ID-DSM-IV
TEACCHclassroom
Distancesnowshoed/walked/jogged
2015
Legend: PS � preschool; ID � intellectual disability; MID � mild intellectual disability; MoID � moderateintellectual disability; SID � severe intellectual disability; DSM � Diagnostic and Statistical Manual; ADHD �Attention Deficit/Hyperactivity Disorder; NS � not specified; SM � self-management procedures
160 / Education and Training in Autism and Developmental Disabilities-June 2011

TA
BL
E2
Des
crip
tors
ofSe
lf-M
anag
emen
tSt
udie
sfo
rin
divi
dual
sw
ith
HFA
/AS
Aut
hors
SSde
sign
Gen
der
CA
Dia
gnos
is/
Func
tioni
ngSe
tting
Beh
avio
r
App
leet
al.
(200
5)M
ulti
ple
base
line
acro
ssst
uden
ts2/
mal
es5
HFA
/AS
(NS)
Inte
grat
edpr
esch
ool
duri
ng
free
play
tim
e#
ofco
mpl
imen
tsdu
rin
g15
min
.in
terv
al1/
fem
ale
4B
arry
&Si
nge
r(2
001)
Mul
tipl
eba
selin
eac
ross
beh
avio
rs(n
otco
ncu
rren
t)
1/m
ale
10H
FA(N
S)H
ome
%of
inte
rval
sin
wh
ich
repl
acem
ent
beh
avio
rsoc
cur
Del
ano
(200
7)M
ulti
ple
base
line
acro
ssre
spon
ses
1/m
ale
12A
SD
SM-I
V-T
RC
onfe
ren
cero
omin
rese
arch
offi
ceT
otal
wor
dsw
ritt
en,
acti
onw
ords
,de
scri
bin
gw
ords
,re
visi
ons,
qual
ity
rati
ng
Lof
tin
etal
.(2
008)
Mul
tipl
eba
selin
eac
ross
part
icip
ants
3/m
ales
9A
SDD
SM-I
VA
DO
SPu
blic
ES
lun
chan
dre
cess
peri
ods
%of
inte
rval
sof
init
iati
on,
inte
ract
ion
,an
dre
peti
tive
mot
orbe
hav
ior
10 10M
orri
son
etal
.(2
001)
Mul
tipl
eba
selin
eac
ross
beh
avio
rs1/
fem
ale
11A
San
dH
FAD
SM-I
VSe
para
tero
omw
ith
insc
hoo
lfo
rfr
ee-ti
me
acti
vity
%of
inte
rval
sw
ith
targ
etin
itia
tion
sof
requ
ests
,co
mm
ents
and
shar
es3/
mal
es10 13 11
Mru
zek
etal
.(2
007)
Ch
angi
ng
crit
erio
nde
sign
repl
icat
edac
ross
part
icip
ants
2/m
ales
9E
D�
AD
HD
&pr
obab
leA
SH
FA(N
S)
Sp.
Ed.
clas
sroo
mfo
rA
SDin
rura
lpu
blic
elem
.sc
hoo
l
Mea
nda
ily%
ofsu
cces
sful
hou
rs(n
oru
levi
olat
ion
s)10
Palm
enet
al.
(200
8)M
ulti
ple
base
line
acro
ssst
uden
ts7/
mal
es17
–25
ASD
wit
hn
oco
gnit
ive
impa
irm
ents
DSM
-IV
Th
erap
yro
omfo
rba
selin
ean
dtr
ain
ing
and
Nat
ural
tuto
rial
con
vers
atio
nlo
cati
ons
for
SM
%C
orre
ctqu
esti
ons
duri
ng
atu
tori
alco
nve
rsat
ion
and
resp
onse
effi
cien
cy2/
fem
ales
Weh
mey
eret
al.
(200
3)M
ulti
ple
base
line
acro
sspa
rtic
ipan
ts1/
mal
e13
HFA
(NS)
Publ
icH
.S.
Gen
eral
Ed.
clas
sroo
mPe
rcen
tof
inte
rval
sof
inap
prop
riat
eto
uch
ing
and
inap
prop
riat
eve
rbal
izat
ion
Leg
end:
PS�
pres
choo
l;ID
�in
telle
ctua
ldis
abili
ty;M
ID�
mild
inte
llect
uald
isab
ility
;MoI
D�
mod
erat
ein
telle
ctua
ldis
abili
ty;S
ID�
seve
rein
telle
ctua
ldis
abili
ty;
DSM
�D
iagn
osti
can
dSt
atis
tica
lM
anua
l;A
DH
D�
Att
enti
onD
efici
t/H
yper
acti
vity
Dis
orde
r;N
S�
not
spec
ified
;SM
�se
lf-m
anag
emen
tpr
oced
ures
Self-Management Procedures across the Spectrum / 161

dural fidelity. As interventions become morecomplex and more teacher and practitionersare conducting research in applied settings,it is important that interventions are imple-mented as planned (Gast, 2010). Only 25%(n � 6) of the studies provided evidence ofprocedural fidelity. Half of those took proce-dural fidelity data during all conditions(Delano, 2007; Loftin, Odom, & Lantz, 2008;Newman, Buffington, & Hemmes, 1996); onestudy took procedural fidelity data duringtraining (Agran et al., 2005); two looked atfidelity of procedures during the student self-management phase (Apple, Billingsley, &Schwarz, 2005; Embregts, Didden, Huitink, &Schreuder, 2002).
Demographic Variables
Self-management intervention across gender,age, degree of cognitive impairment, andtraining setting were analyzed. Tables 1 and 2provide a summary of these demographicvariables under “Gender,” “CA,” “Diagnosis/Functioning,” and “Setting” for each study be-tween AD and HFA/AS respectively.
Autistic Disorder (AD). Thirty-two male par-ticipants and three female students with ADreceived an intervention with componentsof self-management. The interventions usingself-management procedures for this popula-tion have been conducted across the spectrumof age and grade levels. Within the preschoolage range of 3 to 6, four studies includedeight participants (Newman, Tutigian, Ryan,& Reinecke, 1997; Newman, Reinecke, &Meinberg, 2000; Reinecke, Newman, & Mein-berg, 1999; Strain & Kohler, 1994). Four stud-ies included nine elementary age children, 6to 11 years old (Coyle & Cole, 2004; Newmanet al., 1997; Newman et al., 2000; Pierce &Schreibman, 1994). Seven middle school agedstudents, 12 to 15 years old, were participantsin five different studies (Agran et al., 2005;Embregts et al., 2002; Kern, Marder, Boyajian,Elliot, & McElhattan, 1997; Mancina, Tan-kersley, Kamps, Kravits, & Parrett, 2000; New-man et al., 1997; Newman et al., 1995; Sha-bani, Wilder, & Flood, 2001) and four studiesimplemented self-management as an interven-tion for eleven high school age adolescents(Ganz & Sigafoos, 2005; Hughes et al., 2002;
Newman et al., 1995; Newman, Buffington, &Hemmes, 1996; Todd & Reid, 2006).
Criteria for inclusion included participantdiagnosis of autism with a cognitive impair-ment. From the 16 studies reviewed, sevenreported using criteria for diagnosis based aversion of the Diagnostic and Statistical Man-ual (Coyle & Cole, 2004; Embregts et al., 2002;Newman et al., 1995; Newman et al., 1997;Newman et al., 2000; Strain & Kohler, 1994;Todd & Reid, 2006). Fourteen of the 16 arti-cles reported specifically that the participantshad an intellectual disability but only Newmanet al. (1996) reported that the students had asevere shortage of appropriate conversationusing short one word utterance and were non-responsive to direct statements and questions,and Kern et al. (1997) reported the partici-pant performing six or more grade levels be-low.
Ten participants with AD received self-man-agement intervention at a separate school orfacility for children with a disability. Four stu-dents were taught self-management in a clinicand two children participated only at home.Ten students were receiving the treatment in apublic school but received intervention in aseparate special education class. Five partici-pants received treatment in an inclusive gen-eral education environment with two of thoseparticipants’ intervention also conducted athome.
High-functioning autism/Asperger syndrome(HFA/AS). In the eight studies, 20 male andfour female students with HFA/AS receivedan intervention with components of self-man-agement. Interventions using self-manage-ment procedures for this group have beenconducted across the spectrum of age andgrade levels. One study included three pre-school children ages 4 to 5 years old (Apple etal., 2005). Three studies used self manage-ment as treatment for a total of six elementaryschool children ages 9 to 10 (Barry & Singer,2001; Loftin et al., 2008; Mruzek, Cohen, &Smith, 2007) and two studies were carried outwith six middle school aged students rangingfrom 10 to 13 years old (Delano, 2007; Morri-son, Garcia, Kamps, Parker, & Dunlap, 2001;Wehmeyer, Yeager, Bolding, Agran, & Hughes,2003). Lastly, the study by Palmen, Didden,and Arts (2008) implemented self-manage-
162 / Education and Training in Autism and Developmental Disabilities-June 2011

ment with nine young adults ranging in agefrom 17 to 25 years.
None of the individuals identified asHFA/AS were identified as having a cognitiveimpairment and only three reported usingcriteria for diagnosis based a version of theDiagnostic and Statistical Manual (Delano,2007; Loftin et al., 2008; Palmen et al. 2008) toidentify the student with a PDD. The settingsfor intervention varied between inclusive class-rooms (Apple et al., 2005; Loftin et al.; Weh-meyer et al., 2003), separate room for therapy(Delano; Morrison et al., 2001; Palmen et al.),a special education class (Mruzek et al., 2007),and in the home (Barry & Singer, 2001).
Procedural Variables
Procedural variables analyzed included com-ponents of single subject design, proceduralfidelity, data collection, self-managementpackages, support materials used, and tar-geted autistic-like behaviors. While Tables 1and 2 show single subject design and depen-dent measures, Tables 3 and 4 display targetskill domain and self-management packagecomponents within each study. Commoncomponents of most self-management pack-ages included: (a) a timer to alert a studentto self-assess, (b) a self-recording form for astudent to document the assessment, and (c) adesired reward as reinforcement to maintainthe behavior. As these materials are typical formost self-management programs, they are notanalyzed across studies. Although each studyincluded an independent variable requiring astudent to participate in the management ofhis/her behavior as part of the intervention,several other components were part of treat-ment packages.
AD. Target behaviors to be modified andmaintained using self-management have beenclassified into four categories for this reviewbased on prominent characteristics of AD.Four studies addressed self-management todecrease restrictive, repetitive, and stereo-typed behavior patterns (Embregts et al.,2002; Kern et al., 1997; Mancina et al., 2000;Newman et al., 1997; Shabani et al., 2001).Five studies attempted to increase social skillsincluding play and social interaction (New-man et al., 2000; Reinecke et al., 1999; Strain& Kohler, 1994; Todd & Reid, 2006). Only
two studies targeted communication skills.Hughes et al. (2002) recorded the percentageopportunities per session in which a partici-pant said, “Thank you,” to customers during acookie sales event, while Newman et al. (1996)provided treatment to increase appropriateconversation. Finally, four studies focused onschool/vocational skills including off-task be-havior (Coyle & Cole, 2004), following direc-tions (Agran et al., 2005), task completion(Ganz & Sigafoos, 2005), transitioning (New-man et al., 1995), and daily living skills (Pierce& Schreibman, 1994).
Self-management packages included self-monitoring, self-recording, and self-reinforce-ment in five of the 16 studies (40%). Fivestudies did not include self-recording but onlyrequired students to self-monitor and self-reinforce. Agran et al. (2005), Kern et al.(1997), and Newman et al. (1996) excludedself-reinforcement using solely self-monitor-ing and self-recording. Lastly, Hughes et al.(2002), required participants to self-monitoralone. Seven studies incorporated a tokeneconomy as reinforcement. Coyle and Cole(2004) and Embregts et al. (2002) used videoto enhance the procedure through videomodeling desired behavior and video self-recording respectively. Two studies used peertraining as a part of social skill interven-tion while the participants self-monitored(Reinecke et al., 1999; Shabani et al., 2001).Pictures were incorporated as prompts inCoyle and Cole (2004) and Pierce andSchreibman (1994). No studies of self-man-agement within the AD population used con-tracts as a component of the package.
Data were systematically collected duringeach study with half (n � 8) using an intervalrecording procedure. Seven studies (44%)used event recording procedures to measurebehavior change. Kern et al. (1997) used totalduration of occurrence recording procedureto calculate percent of time a student engagedin inappropriate vocalizations. In self-manage-ment programs, interventionists often collectdata on dependent measures differently thanstudent self-recording. Eight researchers (50%)used a different method of data collection. Ofthose that used the same recording proce-dures five (31%) used event recording andthree (19%) quantified behavior changes withinterval recording procedures. Agran et al.
Self-Management Procedures across the Spectrum / 163

(2005) and Hughes et al. (2002) did not in-corporate self-recording into their self-man-agement treatment package. Embregts et al.(2002) required students to record their be-havior using a 20 s to 30 s whole intervalrecording procedure, while the data were col-
lected using a 15 s partial interval recordingprocedure. Kern et al. measured treatmenteffects using total duration recording of vo-calization. Three studies evaluated behaviorchange with interval recording while studentsself-recorded frequency of the target behavior
TABLE 3
Comparison of Self-Management Treatment Package and Skill Addressed–AD
Self-Management Components Behavior Addressed
Self-
mon
itori
ng
Self-
reco
rdin
g
Self-
rein
forc
emen
t
Self-
initi
atio
n
Peer
Tra
inin
g
Con
trac
t
Tok
enEc
onom
y
Pict
ures
Vide
o
Res
tric
tive
Beh
avio
rPa
ttern
s
Soci
alSk
ills
Com
mun
icat
ion
Scho
ol/V
ocat
iona
lSk
ills
Agran et al.(2005) x x x
Coyle & Cole(2004) x x x x x x
Embregts (2002) x x x x x xGanz & Sigafoos
(2005) x x x x xHughes et al.
(2002) x xKern et al.
(1997) x x x xMancina et al.
(2000) x x x x xNewman et al.
(1995) x x x xNewman et al.
(1996) x x xNewman et al.
(1997) x x x xNewman et al.
(2000) x x x xPierce &
Schriebiman(1994) x x x x x
Reinecke et al.(1999) x x x x x
Shabani et al.(2001) x x x x
Strain & Kohler(1994) x x x x x
Todd & Reid(2006) x x x x x
Percentage 100% 56.25% 75% 25% 12.5% 0% 43.75% 13.3% 12.25% 25% 31.25% 12.5% 31.25%
164 / Education and Training in Autism and Developmental Disabilities-June 2011
using event recording (Newman et al., 1996;Pierce & Schriebiman, 1994; Reinecke et al.,1999).
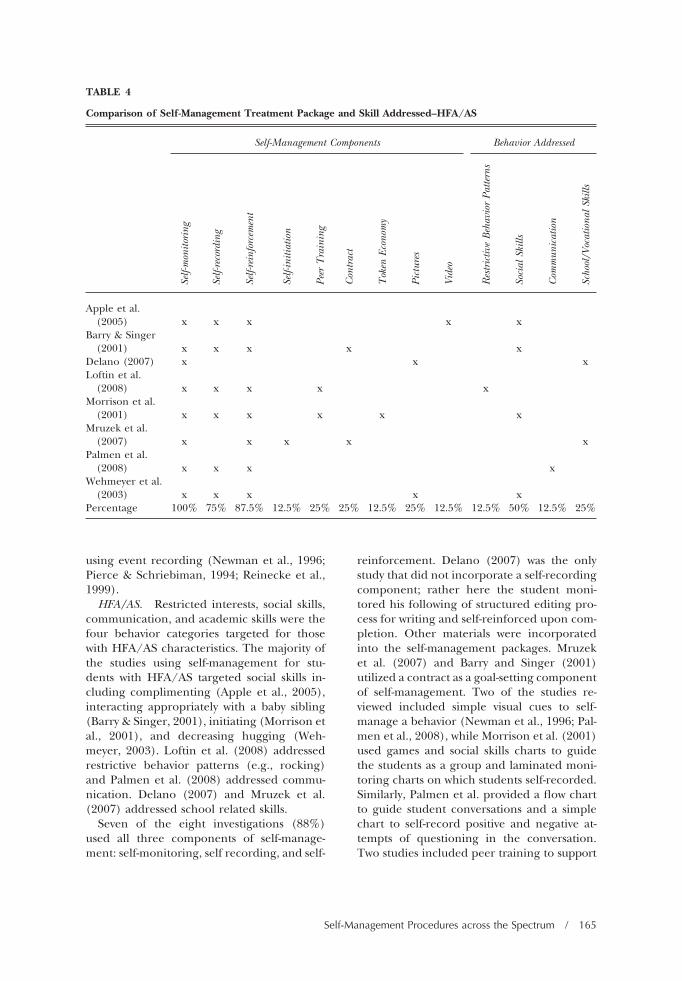
HFA/AS. Restricted interests, social skills,communication, and academic skills were thefour behavior categories targeted for thosewith HFA/AS characteristics. The majority ofthe studies using self-management for stu-dents with HFA/AS targeted social skills in-cluding complimenting (Apple et al., 2005),interacting appropriately with a baby sibling(Barry & Singer, 2001), initiating (Morrison etal., 2001), and decreasing hugging (Weh-meyer, 2003). Loftin et al. (2008) addressedrestrictive behavior patterns (e.g., rocking)and Palmen et al. (2008) addressed commu-nication. Delano (2007) and Mruzek et al.(2007) addressed school related skills.
Seven of the eight investigations (88%)used all three components of self-manage-ment: self-monitoring, self recording, and self-
reinforcement. Delano (2007) was the onlystudy that did not incorporate a self-recordingcomponent; rather here the student moni-tored his following of structured editing pro-cess for writing and self-reinforced upon com-pletion. Other materials were incorporatedinto the self-management packages. Mruzeket al. (2007) and Barry and Singer (2001)utilized a contract as a goal-setting componentof self-management. Two of the studies re-viewed included simple visual cues to self-manage a behavior (Newman et al., 1996; Pal-men et al., 2008), while Morrison et al. (2001)used games and social skills charts to guidethe students as a group and laminated moni-toring charts on which students self-recorded.Similarly, Palmen et al. provided a flow chartto guide student conversations and a simplechart to self-record positive and negative at-tempts of questioning in the conversation.Two studies included peer training to support
TABLE 4
Comparison of Self-Management Treatment Package and Skill Addressed–HFA/AS
Self-Management Components Behavior Addressed
Self-
mon
itori
ng
Self-
reco
rdin
g
Self-
rein
forc
emen
t
Self-
initi
atio
n
Peer
Tra
inin
g
Con
trac
t
Tok
enEc
onom
y
Pict
ures
Vide
o
Res
tric
tive
Beh
avio
rPa
ttern
s
Soci
alSk
ills
Com
mun
icat
ion
Scho
ol/V
ocat
iona
lSk
ills
Apple et al.(2005) x x x x x
Barry & Singer(2001) x x x x x
Delano (2007) x x xLoftin et al.
(2008) x x x x xMorrison et al.
(2001) x x x x x xMruzek et al.
(2007) x x x x xPalmen et al.
(2008) x x x xWehmeyer et al.
(2003) x x x x xPercentage 100% 75% 87.5% 12.5% 25% 25% 12.5% 25% 12.5% 12.5% 50% 12.5% 25%
Self-Management Procedures across the Spectrum / 165

the self-management program (Loftin et al.,2008; Morrison et al.).
Researcher dependent variable measure-ment systems were the same as students withHFA/AS self-recording in three (31%) of theeight studies (Apple et al., 2005; Delano, 2007;Mruzek et al., 2007). The remaining studiesrequired students to self-record using eventrecording where the researcher used intervalrecording procedures.
Outcomes
Self-management procedures were successfulin increasing target behaviors for studentswith ASD.
AD. Self-management procedures in-creased target behaviors for students with AD.A total of 16 research studies met the originalsearch criteria. All 35 participants using a ver-sion of self-management improved and main-tained targeted skills. Four of the studies for-mally collected social validity (Wolf, 1978)data using questionnaires and rating forms.The participant with AD in Hughes et al.(2002) made noticeable significant gains insaying “thank you” to customers using self-management as perceived by a peer andteacher. Both peer and teacher also con-firmed that they enjoyed being around thestudent with AD more after the positive effectsof self-management. Kern et al. (1997) re-ported that school staff perceived self-manage-ment as easy to implement and effective in ashort duration of time while not being dis-tracting to students. Embregts et al. (2002)reported that video feedback and student self-management was a non-obtrusive and non-confrontational method of changing behav-ior. Staff reported that self-managementproduced substantial changes in aggressive be-havior of four of five individuals including thestudent with autism.
HFA/AS. Self-management procedures re-sulted in increased target behaviors and inde-pendence in treatment for 23 of 26 partici-pants. Three out of nine participants in thePalmen et al. (2008) study made gains of 4 to12 percent of appropriate questions and re-sponses made during a conversation. Other-wise, the range of percent increase of baselinemean to intervention mean in this study was23 to 96. The independent variable in Palmen
et al. was a game format with individuals usinga flowchart to self-observe and move tokenson a game board as a form of self-recording.Intervention could not be staggered acrossparticipants as they were all involved in theintervention simultaneously. Although theself-management intervention was replicatedacross two more groups of three, it was con-sidered a nonconcurrent multiple baselinedecreasing the internal validity (Gast, 2010).Palmen et al. was the only study on self-management for adolescents with HFA/AS.All other studies involved 4- year-old to 13-year-old children with HFA/AS.
Five of the eight studies using self-manage-ment to change behavior in HFA/AS reportedsocial validity. Loftin et al. (2008) used IEP’sto determine target behaviors; teachers andparents gave positive reviews of the goals oftreatment, procedures and outcomes. Appleet al. (2005) collected social validity informa-tion using parent and teacher reports indicat-ing a perception of increase in general socialskills by three of four participants and gener-alization to nontraining settings after self-management to increase complement-givingbehaviors. Palmen et al. (2008) reported self-management as a socially valid intervention toincrease conversation skills in adolescentswith HFA/AS. Both student participants andcoaches found the training effective and ac-ceptable, while meaningful increases in con-versation generalized to the natural contexts.Wehmeyer et al. (2003) stated that teacherperceptions of student progress using the self-management were more than expected. Barryand Singer (2001) found replacing the aggres-sive behavior of a child with autism toward aninfant sibling socially valid. Self-managementchanged potentially dangerous behaviors andparents reported that siblings had developed agood relationship. This indicates that futureresearch might examine improved impact onsibling relationships on parents and otherfamily members.
Discussion
The belief that all individuals have the right todirect their own lives through the choices theymake has been emphasized in Individuals withDisabilities Improvement Act (IDEIA, 2004).Self-determination skills indicate a more suc-
166 / Education and Training in Autism and Developmental Disabilities-June 2011

cessful transition to adulthood (Wehmeyer etal., 2003). As a critical component of self-determination, self-management should betaught to students with an ASD. As implied byliterature on self-determination (Wehmeyer,1999), research in the area of learning disabil-ities and behavior disorders shows that tech-niques to increase self-management are suc-cessful for changing behavior in higherfunctioning individuals with well-establishedverbal language. The current review indicatesthat individuals with HFA/AS effectively usedself-management procedures to address defi-cits related to the core characteristics of ASD.Furthermore, added technologies were help-ful adaptations to typical self-managementprocedures (e.g., tokens, pictures, video) tomake the interventions viable with lower-func-tioning individuals with AD.
Children with ASD specifically have beenfound to have difficulty “directing, control-ling, inhibiting, maintaining, and generalizingbehaviors required for adjustment both in andoutside of the classroom without external sup-port and structure from others” (Wilkinson,2008, p. 151). Attention should be drawn tothe fact that self-management procedures fo-cus on behaviors already in a student’s reper-toire, behaviors where differential reinforce-ment and other interventions alone have notbeen sufficient to maintain the behavior ininclusive settings. An examination of themethodological adequacy, demographics, andprocedures found in 24 single subject re-search design studies was used to evaluate self-management procedures for teaching skills tostudents with an ASD. Data show that acrossparticipants, settings, or behaviors, self-man-agement interventions resulted in improve-ments in desired behaviors.
Future Research
While self-management procedures have beenused across all age groups for youth, there aregaps in the literature. Tables 3 and 4 displayskills addressed using self-management byindividuals with AD and HFA/AS. Analyses ofthese data suggest that future research shouldfocus on the effectiveness of self-managementprocedures for increasing communicationskills in people with ASD. It is also essentialthat researchers begin to focus on specific
components of self-management programs toevaluate each component’s relative contribu-tion to program effectiveness. Most impor-tantly, future research should evaluate meth-ods for taking self-management proceduresinto the homes of children with ASD. Studiesin the present literature review indicate thatstudents tend to remain reliant on self-man-agement procedures and materials. Research-ers need to investigate making the materialsand equipment as unobtrusive as possible sothey can be generalized to home and commu-nity environments and not draw attention tothe individual. Examining the use of a Per-sonal Digital Assistant (PDA) as a tool forself-management for individuals with ASD haspotential. For individuals with HFA/AS,PDA’s require little training while enablingtechnologically adept students to emit targetbehavior and become more independent(Ferguson, Myles, & Hagiwara, 2005; Myles,Ferguson, & Hagiwara, 2007). Further re-search on the use of PDA’s across age andcognitive levels of individuals on the spectrumis needed.
Limitations of Self-management Research
Effects of self-management procedures as anintervention to increase target behaviors, in-dependence, and generalization of skills forpeople with autism are limited due to con-founding variables. Controlling for variouscomponents of the self-management packageis difficult. As seen in Tables 3 and 4, eachstudy included various self-management com-ponents. It is difficult to make comparisons ofeffectiveness when treatment packages vary,and it would be premature to say that anyspecific component of self-management is theprimary cause of behavior change. Also, mostof self-management procedures were imple-mented with an existing positive reinforce-ment procedure. Although some studies at-tempted to control for reinforcement as aconfounding variable by applying noncontin-gent reinforcement before self-management,the contingency of reinforcement itself thenbecame confounding. Was contingent rein-forcement simply more powerful than non-contingent reinforcement?
Procedural fidelity data and social validityof treatment were limited in use across the
Self-Management Procedures across the Spectrum / 167

24 articles reviewed on self-management as anintervention. Procedural fidelity issues maynot have been of primary concern since self-management is “driven” by the student, notthe practitioner. In terms of social validity,self-management procedures have been wellestablished throughout the research overmany years (Cooper et al., 2007). Eleven ofthe 24 articles reviewed included a measure ofsocial validity specific to the self-managementprocedure and effect implemented. The re-sults of such measures were all positive inregard to the acceptability and feasibility ofthe procedures.
Generalization of the treatment into thehome was seldom assessed with home imple-mentation in four out of 24 studies (17%)with only four of 35 individuals with AD(11%) and one of 24 individuals with HFA/AS(4%). Educators should be encouraged toteach parents to use interventions at hometo increase skills taught in school (Heflin &Alberto, 2001).
Research to Practice
There is an increasing awareness that studentswith an ASD require an intervention approach
that addresses not only academic and voca-tional skills, but one that addresses the threecore deficits that characterize the disorder.Figure 1 compares ASD core characteristicaddressed by self-management studies in-cluded in this review. The defining character-istic impacting independence in individualswith ASD is social impairment (Heflin &Alaimo, 2006). For this reason it is not surpris-ing that self-management has been widelyused to increase social skills, however, datashow that an individualized self-managementprogram may be effective in behavior changeacross all ASD core characteristics.
Self-management has three primary com-ponents: self-monitoring, self-recording, andself reinforcement/punishment. Self-monitor-ing was basic to all interventions reviewed.Tables 3 and 4 show that combinations ofself-monitoring and (a) self-recording (b) self-reinforcement or (c) both, while incorporat-ing additional components (e.g., peer train-ing, contracts, token economy, pictures, andvideo), were individual to each study. Socialvalidity data supported the individualizednature and meaningful outcomes these treat-ment packages provided. Teachers and par-
Figure 1. Comparison of percent of studies that used self-management procedures to address core deficitsof ASD and school or vocational skills and a second comparison between AD and HFA/AS.
168 / Education and Training in Autism and Developmental Disabilities-June 2011

ents should feel confident that, when appro-priately implemented and individualized forthe student needs, self-management can bean effective, unobtrusive intervention strategywithin the least restrictive environment.
Self-management interventions are easy todesign, simple to use, potentially portable,and practical for teachers. It has been assertedthat self-management is a pivotal skill that cangeneralize behaviors, support autonomy, andproduce behavioral improvements across var-ious contexts for children with ASD (Koegelet al., 1999). Based on this idea and currentliterature presenting self-management as a vi-able procedure, practical use of self-manage-ment procedures is recommended for foster-ing independence and inclusion of peoplewith ASD.
References
Agran, M., Sinclair, T., Alper, S., Cavin, M., Weh-meyer, M., & Hughes, C. (2005). Using self-monitoring to increase following-direction skillsof students with moderate to severe disabilities ingeneral education. Education and Training in De-velopmental Disabilities, 40, 3–13.
Agran, M., Snow, K., & Swaner, J. (1999). Teacherperceptions and self-determination: Benefits,characteristics, strategies. Education and Trainingin Mental Retardation and Developmental Disabilities,34, 293–301.
American Psychiatric Association.(1980). Diagnosticand Statistical Manual of Mental Disorders, (3rd ed.).Washington, DC: Author.
American Psychiatric Association.(1994). Diagnosticand Statistical Manual of Mental Disorders, (4th ed.).Washington, DC: Author.
American Psychiatric Association.(2000). Diagnosticand Statistical Manual of Mental Disorders, (4th ed.Text Revision). Washington, DC: Author.
Apple, L. A., Billingsley, F., & Schwartz, I. (2005).Effects of video modeling alone and with self-management on compliment-giving behaviors ofchildren with high-functioning ASD. Journal ofPositive Behavior Interventions, 7, 33–46.
Barry, L., & Singer, G. (2001). A family in crisis:Replacing the aggressive behavior of a child withautism toward an infant sibling. Journal of PositiveBehavior Interventions, 3, 28–38.
Billingsly, F., White, O. R., & Munson R. (1980).Procedural reliability: A rationale and example.Behavioral Assessment, 2, 229–241.
Campbell, J. M. (2006). Changing children’s atti-tudes toward autism: A process of persuasive com-
munication. Journal of Developmental and PhysicalDisabilities, 18, 251–272.
Campbell, J. M., & Morgan, S. B. (1998). Asperger’sdisorder. In L. Phelps (Ed.), Health-related disordersin children and adolescents (pp. 68–73). Washing-ton, DC: American Psychological Association.
Center for Disease Control. (2007). Autism Informa-tion Center. Retrieved from Web site: http://www.cdc.gov/ncbddd/autism/symptoms.htm
Cole, C., & Bambara, L. (1992). Issues surroundingthe use of self-management interventions in theschools. School Psychology Review, 21, 193–202.
Cooper, J. O., Heron, T. E., & Heward, W. L.(2007). Applied behavior analysis (2nd ed.). UpperSaddle River, NJ: Pearson Merrill Prentice Hall.
Coyle, C., & Cole, P. (2004). A videotaped self-modeling and self-monitoring treatment programto decrease off-task behavior in children with au-tism. Journal of Intellectual & Developmental Disabil-ity, 29, 3–15.
Delano, M. (2007). Improving written language per-formance of adolescents with Asperger syndrome.Journal of Applied Behavior Analysis, 40, 345–351.
Embregts, P., Didden, R., Huitink, C., & Schreuder,N. (2009). Contextual variables affecting aggres-sive behavior in individuals with mild to border-line intellectual disabilities who live in a residen-tial facility. Journal of Intellectual Disability Research,53, 255–264.
Ferguson, H., Myles, B., & Hagiwara, T. (2005).Using a Personal Digital Assistant to Enhance theIndependence of an Adolescent with AspergerSyndrome. Education and Training in DevelopmentalDisabilities, 40, 60–67.
Ganz, J. B., & Sigafoos, J. (2005). Self-monitoring:Are young adults with MR and autism able toutilize cognitive strategies independently? Educa-tion and Training in Developmental Disabilities, 40,24–33.
Gast, D. L. (Ed.).(2010). Single subject research meth-odology in behavioral sciences. New York: Routledge.
Gast, D. L., & Hammond, D. (2010). Withdrawaland reversal designs. In D. L. Gast (Ed.), Singlesubject research methodology in behavioral sciences (pp.234–275). New York: Routledge.
Gast, D. L. & Ledford, J. (2010). Multiple baselineand multiple probe designs. In D. L. Gast (Ed.),Single subject research methodology in behavioral sci-ences (pp. 276–328). New York: Routledge.
Happe, F., Booth, R., Charlton, R., & Hughes, C.(2006). Executive function deficits in autism spec-trum disorders and attention-deficit/hyperactiv-ity disorder: Examining profiles across domainsand ages. Brain & Cognition, 61, 25–39.
Heflin, J. L. & Alberto, P. A. (2001). Establishing abehavioral context for learning with students withautism. Focus on Autism & Other Developmental Dis-abilities, 16, 93-101.
Self-Management Procedures across the Spectrum / 169

Heflin, J. L., & Alaimo, D. (2006). Autism spectrumdisorders: Effective instructional practices. Upper Sad-dle River, NJ: Prentice Hall.
Hughes, C., Copeland, S. R., Agran, M., Wehmeyer,M., L., Rodi, M. S., & Presley, J. A. (2002). Usingself-monitoring to improve performance in gen-eral education high school classes. Education andTraining in Mental Retardation Developmental Dis-abilities, 37, 262–272.
Individuals with Disabilities Education Improve-ment Act of 2004, 20 U.S.C. § 1400 et seq. (2004)(reauthorization of the Individuals with Disabili-ties Education Act of 1990).
Kanner, L. (1943). Autistic disturbances of affectivecontact. Nervous Child, 2, 217–250.
Kanner, L. (1985). Autistic disturbances of affectivecontact. In A. Donnellan (Ed.), Classic readings inautism (pp. 11–52). New York: Teacher’s CollegePress. (Reprinted from Nervous Child, 2, 217-250,1943).
Kern, L., Marder, T. J., Boyajian, A., Elliot, C. M., &McElhattan, D. (1997). Augmenting the indepen-dence of self-management procedures by teach-ing self-initiation across settings and activities.School Psychology Quarterly, 12, 23–32.
Koegel, L. K., Koegel, R. L., Hurley, C., & Frea,W. D. (1992). Improving social skills and disrup-tive behavior in children with autism throughself-management. Journal of Applied Behavior Anal-ysis, 25, 341–353.
Koegel, L., Koegel, R., Harrower, J., & Carter, C.(1999). Pivotal response intervention: Overviewof approach. Journal of the Association for Personswith Severe Handicaps, 24, 174–185.
Lee, S., Simpson, R., & Shoran, K. (2007). Effectsand implications of self-management for studentswith autism: A meta-analysis. Focus on Autism &Other Developmental Disabilities, 22, 2–13.
Loftin, R., Odom, S., & Lantz, J. (2008). Socialinteraction and repetitive motor behaviors. Jour-nal of Autism & Developmental Disorders, 38, 1124–1135.
Macintosh, K. E., & Dissanayake, C. (2004). Anno-tation: The similarities and differences betweenautistic disorder and Asperger’s disorder: A re-view of the empirical evidence. Journal of ChildPsychology and Psychiatry, 45, 421–434.
Mancina, C., Tankersley, M., Kamps, D., Kravits, T.,& Parrett, J. (2000). Brief report: Reduction ofinappropriate vocalizations for a child with au-tism using a self-management treatment pro-gram. Journal of Autism & Developmental Disorders,30, 599.
Morrison, L., Kamps, D., Garcia, J., Parker, D., &Dunlap, G. (2001). Peer mediation and monitor-ing strategies to improve initiation and socialskills for students with autism. Journal of PositiveBehavior Interventions, 3, 237.
Mruzek, D., Cohen, C., & Smith, T. (2007). Contin-gency contracting with students with autism spec-trum disorders in a public school setting. Journalof Developmental & Physical disabilities, 19, 103–114.
Myles, B., Ferguson, H., & Hagiwara, T. (2007).Using a personal digital assistant to improve therecording of homework assignments by an ado-lescent with asperger syndrome. Focus on Autismand Other Developmental Disabilities, 22, 96–99.
Myles, B. S., & Southwick, J. (1999). Asperger syn-drome and difficult moments: Practical solutions fortantrums, rage, and meltdowns. Shawnee Mission,Kansas: Autism Asperger Publishing Co.
Newman, B., Buffington, D. M., & Hemmes, N. S.(1996). Self-reinforcement used to increase theappropriate conversation of autistic teenagers. Ed-ucation and Training in Mental Retardation and De-velopmental Disabilities, 31, 304–309.
Newman, B., Buffington, D. M., O’Grady, M. A.,McDonald, M. E., Poulson, C. L., & Hemmes,N. S. (1995). Self-management of schedule fol-lowing in three teenagers with autism. BehavioralDisorders, 10, 190–196.
Newman, B., Reinecke, D. R., & Meinberg, D. L.(2000). Self-management of varied responding inthree students with autism, Behavioral Intervention,15, 145–151.
Newman, B., Tuntigian, L., Ryan, C., & Reinecke, D.(1997). Self-management of a DRO procedureby three students with autism. Behavioral Interven-tions, 12, 149–156.
Ozonoff, S., & Rogers, S (2003). From Kanner tothe millennium: Scientific advances that haveshaped clinical practice. In Ozonoff, S., Rogers,S., & Hendron, R. L. (Eds.), Autism spectrum dis-orders: A research review for practitioners (pp. 3–36).Arlington, VA: American Psychiatric Publishing,Inc.
Ozonoff, S., Rogers, S., & Hendron, R. L. (2003).Autism spectrum disorders: A research review for prac-titioners. Arlington, VA: American Psychiatric Pub-lishing, Inc.
Palmen, A., Didden, R., & Arts, M. (2008). Improv-ing question asking in high-functioning adoles-cents with autism spectrum disorders. Autism: TheInternational Journal of Research & Practice, 12, 83–98.
Pierce, K. L., & Schreibman, L. (1994). Teachingdaily living skills to children with autism in unsu-pervised settings through pictorial self-manage-ment. Journal of Applied Behavior Analysis, 27, 471–481.
Prater, M., & Hogan, S. (1992). Using self-monitor-ing to improve of-task behavior and academicskills of an adolescent with mild. Education &Treatment of Children, 15, 43–58.
Reinecke, D. R., Newman, B., & Meinberg, D. L.(1999). Self-management of sharing in three pre-
170 / Education and Training in Autism and Developmental Disabilities-June 2011

schoolers with autism. Education and Training inMental Retardation and Developmental Disabilities,34, 312–317.
Rimland, B. (1985). The etiology of infantile au-tism: The problem of biological versus psycholog-ical causation. In A. Donnellan (Ed.), Classic read-ings in autism (pp. 84–104). New York: Teacher’sCollege Press. (Reprinted from Infantile autism,pp. 39–66, by B. P. Rimland, 1964, New York:Appleton-Century-Crofts).
Scheuermann, B., & Webber, J. (2002). Autism:Teaching does make a difference. Belmont, CA: Wads-worth Thompson Learning.
Shabani, D., Wilder, D., & Flood, W. (2001). Reduc-ing stereotypic behavior through discriminationtraining, differential reinforcement of other be-havior, and self-monitoring. Behavioral Interven-tions, 16, 279–286.
Shapiro, H. (1981). Implementing P.L. 94-142 inthe high school: A successful in-service trainingmodel. Education, 102, 47–52.
Strain, P., & Kohler, F. (1994). Teaching preschool-ers with autism to self-monitor their social inter-actions: An analysis of results in home and schoolsettings. Journal of Emotional & Behavioral Disor-ders, 2, 78–92.
Thede, L. L., & Coolidge, F. L. (2007). Psychologi-cal and neurobehavioral comparisons of childrenwith Asperger’s disorder versus high-functioningautism. Journal of Autism and Developmental Disor-ders, 37, 847–854.
Todd, T., & Reid, G. (2006). Increasing physicalactivity in individuals with autism. Focus on Autismand Other Developmental Disabilities, 21, 167–176.
Volkmar, F. R., & Klin, A. (2005). Issues in theclassification of autism and related conditions. InVolkmar, F. R., Rhea, P., Ami, K., & Cohen, D.(Eds.), Handbook of autism and pervasive develop-
mental disorders volume one (pp. 5–41). New Jersey:John Wiley & Sons, Inc.
Wehmeyer, M. (1999). A functional model of self-determination: Describing development and im-plementing instruction. Focus on Autism and OtherDevelopmental Disabilities, 14, 53-61.
Wehmeyer, M., Yeager, D., Bolding, N., Agran, M.,& Hughes, C. (2003). The effects of self-regula-tion strategies on goal attainment for studentswith developmental disabilities in general educa-tion classrooms. Journal of Developmental & PhysicalDisabilities, 15, 79–91.
Wilkinson, L. (2005). Supporting the inclusion ofa student with Asperger syndrome: A case studyusing conjoint behavioral consultation and self-management. Educational Psychology in Practice, 21,307–326.
Wilkinson, L. (2008). Self-Management for childrenwith high-functioning autism spectrum disorders.Intervention in School & Clinic, 43, 150–157.
Wing, L. (1981). Asperger’s disorder: A clinical ac-count. Psychological Medicine, 11, 115–129.
Witwer, A. N., & Lecavalier, L. (2008). Examiningthe validity of autism spectrum disorder subtypes.Journal of Autism Developmental Disorders, 38, 1611–1624.
Wolery, M., & Lane, K. L. (2010). Writing tasks:Literature reviews, research proposals, and finalreports. In D. L. Gast (Ed.), Single subject researchmethodology in behavioral sciences (pp. 57–90). NewYork: Routledge.
Wolf, M. (1978). Social validity: The case for subjec-tive measurement or how applied behavior anal-ysis is finding its heart. Journal of Applied BehaviorAnalysis, 11, 203–214.
Received: 11 January 2010Initial Acceptance: 15 March 2010Final Acceptance: 10 June 2010
Self-Management Procedures across the Spectrum / 171