sentinel node in colon cancer f. crafa, a. noviello · sentinel node in colon cancer f. crafa, a....
TRANSCRIPT
Francesco
Crafa
Sentinel node in colon cancer
F. Crafa, A. Noviello
General and Emergency Surgery Unit
Chief: F. Crafa M.D.
San Giuseppe Moscati Hospital
Hospital of National Relevance and High Specialty
Avellino
Italy
Francesco
Crafa
10–25% of the patients with localized colon
cancer (AJCC stage I and II) will develop
disease.
Up to 30 % of patients with colorectal cancer
diagnosed as pN0 following surgery will die
within 5 years owing to regional recurrence or
distant metastases.
Understaging is considered to be around 10–
20% , underlining the need to search for methods
that can help to achieve a correct staging of the
patient.
Saha S, Dan AG, Viehl CT et al (2005) Sentinel lymph node
mapping in colon and rectal cancer: its impact on staging,
limitations, and pitfalls. In: Leong SPL, Kitagawa Y, Kitajima M
(eds) Selective sentinel lymphadenectomy for human solid cancer.
Springer, New York pp 105–122
Mulsow J, Winter DC, O’Keane JC, O’Connell PR (2003) Sentinel
lymph node mapping in colorectal cancer. Br J Surg 90:659–667
Francesco
Crafa
Additional H&E histopathologic analysis of
serial sections allows for the identification of
micrometastatic disease in up to 20 % of
lymph nodes determined to be negative by
standard H&E methods.
Dionigi G, Castano P, Rovera F, et al. The
application of sentinel lymph node mapping in
colon cancer. Surg Oncol. 2007;16 Suppl
1:S129–32.
Francesco
Crafa
Therefore, what would be most useful and relevant is a
more careful evaluation of a selected group of
lymph nodes that have the highest probability of
containing metastatic cells, i.e., the sentinel lymph
nodes (SLNs).
Bilchik AJ, DiNome M, Saha S, et al. Prospective multicenter trial of staging adequacy in colon cancer: preliminary
results. Arch Surg. 2006;141:527–33.
Lim SJ, Feig BW, Wang H, et al. Sentinel lymph node evaluation does not improve staging accuracy in colon cancer.
Ann Surg Oncol. 2008;15:46–51.
Des Guetz G, Uzzan B, Nicolas P, et al. Is sentinel lymph node mapping in colorectal cancer a future prognostic
factor? A meta-analysis. World J Surg. 2007;31:1304–12.
Wood TF, Nora DT, Morton DL, et al. One hundred consecutive cases of sentinel lymph node mapping in early
colorectal carcinoma: detection of missed micrometastases. J Gastrointest Surg. 2002;6:322–9.
Broderick-Villa G, Ko A, O’Connell TX, et al. Does tumor burden limit the accuracy of lymphatic mapping and sentinel
lymph node biopsy in colorectal cancer? Cancer J. 2002;8:445–50.
Saha S, Seghal R, Patel M, et al. A multicenter trial of sentinel lymph node mapping in colorectal cancer: prognostic
implications for nodal staging and recurrence. Am J Surg. 2006;191:305–10.
Francesco
Crafa
In this regard, SLN mapping may allow
identification of a smaller number of
lymph nodes representing the tumor
status of the entire nodal basin. An
exhaustive analysis of SLNs in order to
achieve a more accurate staging of
patients can influence the decision for
adjuvant treatment.
Thorn M (2000) Lymphatic mapping and sentinel
node biopsy: is method applicable to patients with
colorectal and gastric cancer? Eur J Surg
166:755–758
Francesco
Crafa
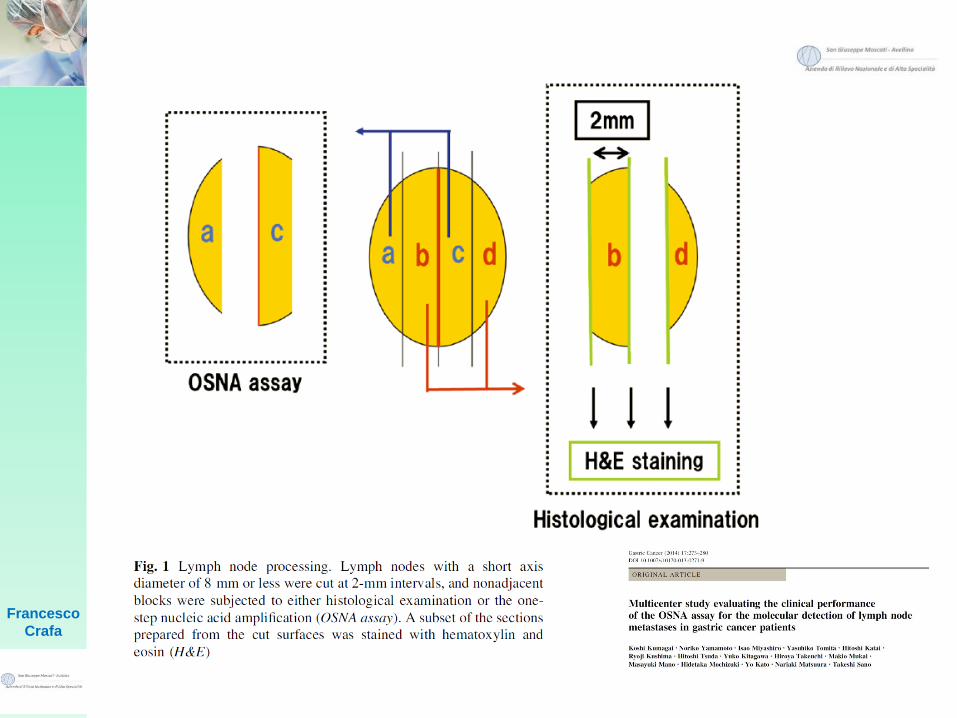
A novel technique for pathological examination,
one step nucleic acid amplification (OSNA),
uses the reverse transcription loop-mediated
isothermal amplification (RTLAMP) method to
amplify cytokeratin 19 (CK19) mRNA. In contrast
to the current routine histopathological
examination, it is able to examine whole lymph
nodes (LNs) and detect metastases in a
sufficiently short time.
Tsujimoto M, Nakabayashi K, Yoshidome K, Kaneko T, Iwase T, Akiyama F,
et al. One-step nucleic acid amplification for intraoperative detection of
lymph node metastasis in breast cancer patients. Clin Cancer Res.
2007;13(16):4807–16.
Francesco
Crafa
CK19 mRNA copy numbers were calculated using a standard
curve that was established beforehand with three calibrators containing
different CK19 mRNA copy numbers. Standard positive and negative
control samples were used for quality assurance in every assay run. On
the basis of previous investigations, OSNA results with CK19 mRNA
copy numbers C 5000 copies/lL were designated as (++), and
OSNA results with CK19 mRNA copy numbers between 250 and
4999 copies/lL were designated as (+). OSNA results with fewer
than 250 copies/lL were considered negative results.
Tsujimoto M, Nakabayashi K, Yoshidome K, Kaneko T, Iwase T, Akiyama F, et al. One-step nucleic acid amplification for
intraoperative detection of lymph node metastasis in breast cancer patients. Clin Cancer Res. 2007;13(16):4807–16.
Notomi T, Okayama H, Masubuchi H, Yonekawa T, Watanabe K, Amino N, et al. Loop-mediated isothermal amplification
of DNA. Nucleic Acids Res. 2000;28(12):E63.
Mori Y, Nagamine K, Tomita N, Notomi T. Detection of loop mediated isothermal amplification reaction by turbidity
derived from magnesium pyrophosphate formation. Biochem Biophys Res Commun. 2001;289(1):150–4.
Francesco
Crafa
OSNA has already been introduced into clinical
settings for breast cancer patients worldwide. The
Japanese Breast Cancer guideline has
recommended OSNA as an alternative to
standard hematoxylin/eosin (H&E) staining for
intraoperative LN examination. OSNA was also
recommended by National Institute for Health
and Clinical Excellence (NICE) in the United
Kingdom, and has been published in the guideline
of the Spanish Society of Senology and
Mammary Pathology.
Visser M, Jiwa M, Horstman A, Brink, AA, Pol RP, van Diest P, et al. Intra-operative rapid diagnostic method based on CK19 mRNA expression for the
detection of lymph node metastases in breast cancer. Int J Cancer. 2008;122(11):2562–7.
Tamaki Y, Akiyama F, Iwase T, Kaneko T, Tsuda H, Sato K, et al. Molecular detection of lymph node metastases in breast cancer patients: results of a
multicenter trial using the one-step nucleic acid amplification assay. Clin Cancer Res. 2009;15(8):2879–84.
Bernet L, Cano R, Martinez M, Duen˜as B, Matias-Guiu X, Morell L et al. Diagnosis of the sentinel lymph node in breast cancer: a reproducible
molecular method: a multicentric Spanish study. Histopathology. 2011;58(6):863–9.
Le Fre`re-Belda MA, Bats AS, Gillaizeau F, Poulet B, Clough KB, Nos C, et al. Diagnostic performance of one-step nucleic acid amplification for
intraoperative sentinel node metastasis detection in breast cancer patients. Int J Cancer. 2012;130(10):2377–86.
National Institute for Health and Care Excellence. NICE diagnostics guidance 8. Intraoperative tests (RD-100i OSNA system and Metasin test) for
detecting sentinel lymph node metastases in breast cancer. 2013.
Berneta L, Pin˜erob A, Vidal-Sicartc S, et al. Consensus on sentinel lymph node biopsy in breast cancer. Review of the Spanish Society of Senology
and Breast Pathology 2013. Revista de Senologı´a y Patologı´a Mamaria. Volume 27, Issue 1, January– March 2014, pp 43–53.
Francesco
Crafa
There are therefore two methods for
SLN mapping:
Staining method
Radioguided method
Francesco
Crafa
SLN mapping can be
performed
in vivo and ex vivo
Francesco
Crafa
Regarding the tracer used to detect the SLNs, three tracers
have been used: dye, RI, and ICG. Each tracer has its
respective disadvantages. The disadvantages of the dye
method are a low recognition rate and a short leveling time.
The high cost and the exposure problem of radioactivity are
disadvantages of RI tracers. The use of the ICG
fluorescence method has officially been approved in
Japan in LNs of breast cancer and malignant
melanoma, and it thus appears that ICG can be an
acceptable tracer for the detection of LNs in gastric and
colon cancer.
Staining Method
Francesco
Crafa
EXPERIENCE

Francesco
Crafa

Francesco
Crafa
Francesco
Crafa
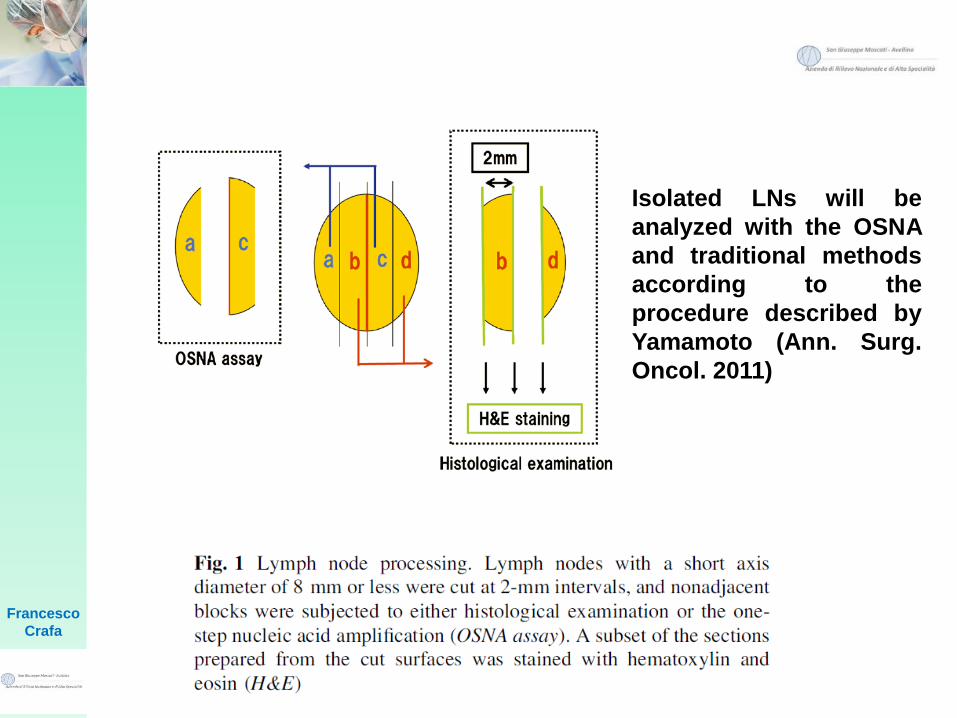
Isolated LNs will be
analyzed with the OSNA
and traditional methods
according to the
procedure described by
Yamamoto (Ann. Surg.
Oncol. 2011)
Francesco
Crafa
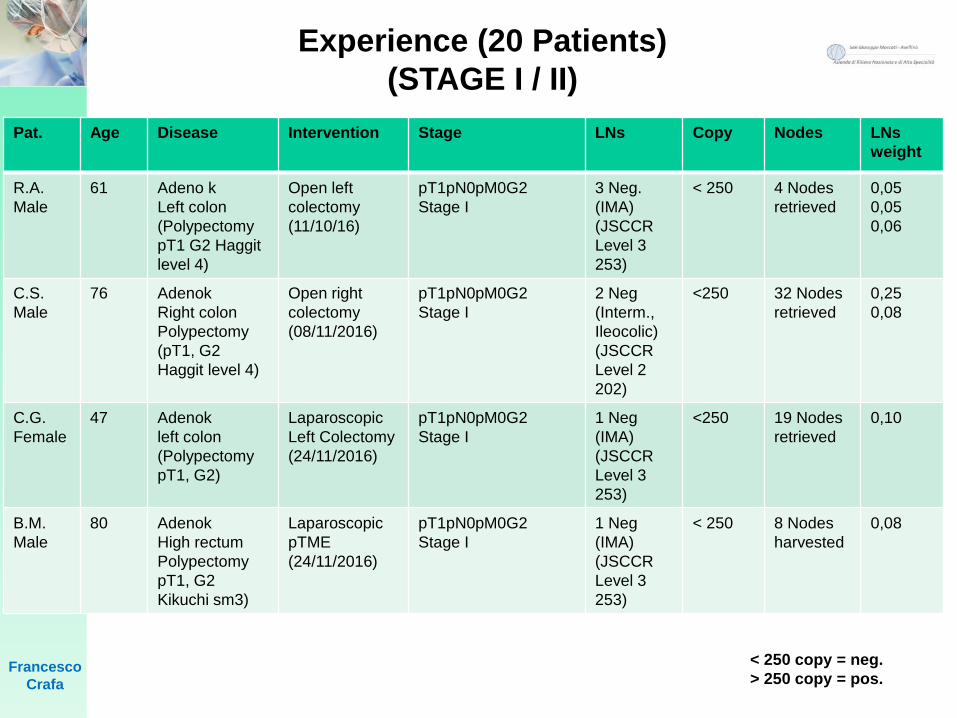
Pat. Age Disease Intervention Stage LNs Copy Nodes LNs
weight
R.A.
Male
61 Adeno k
Left colon
(Polypectomy
pT1 G2 Haggit
level 4)
Open left
colectomy
(11/10/16)
pT1pN0pM0G2
Stage I
3 Neg.
(IMA)
(JSCCR
Level 3
253)
< 250 4 Nodes
retrieved
0,05
0,05
0,06
C.S.
Male
76 Adenok
Right colon
Polypectomy
(pT1, G2
Haggit level 4)
Open right
colectomy
(08/11/2016)
pT1pN0pM0G2
Stage I
2 Neg
(Interm.,
Ileocolic)
(JSCCR
Level 2
202)
<250 32 Nodes
retrieved
0,25
0,08
C.G.
Female
47 Adenok
left colon
(Polypectomy
pT1, G2)
Laparoscopic
Left Colectomy
(24/11/2016)
pT1pN0pM0G2
Stage I
1 Neg
(IMA)
(JSCCR
Level 3
253)
<250 19 Nodes
retrieved
0,10
B.M.
Male
80 Adenok
High rectum
Polypectomy
pT1, G2
Kikuchi sm3)
Laparoscopic
pTME
(24/11/2016)
pT1pN0pM0G2
Stage I
1 Neg
(IMA)
(JSCCR
Level 3
253)
< 250 8 Nodes
harvested
0,08
< 250 copy = neg.
> 250 copy = pos.
Experience (20 Patients)
(STAGE I / II)
Francesco
Crafa
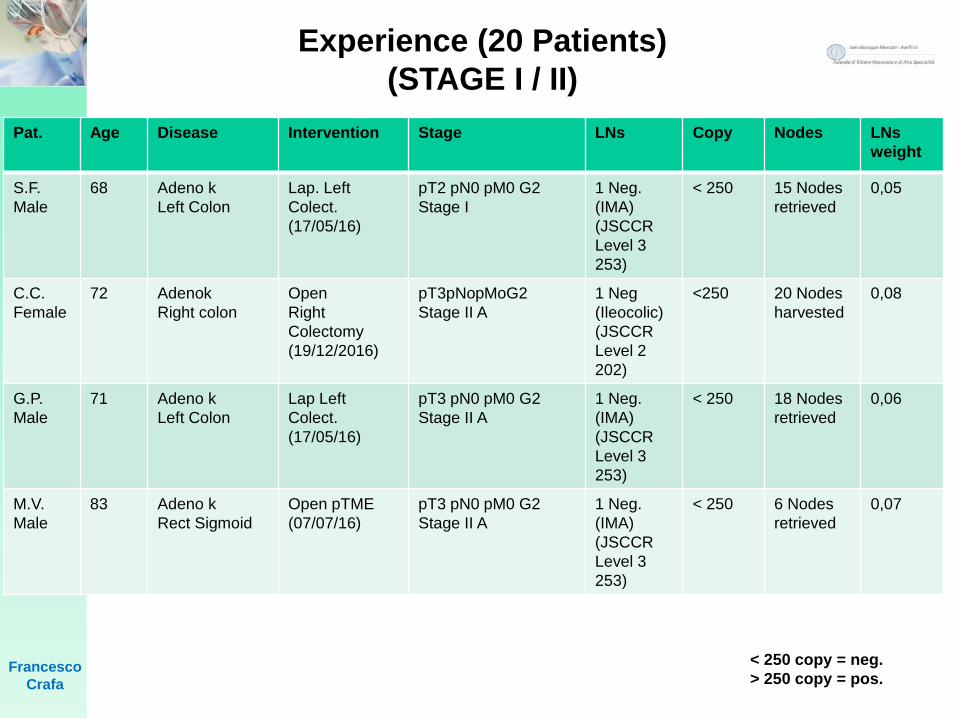
Pat. Age Disease Intervention Stage LNs Copy Nodes LNs
weight
S.F.
Male
68 Adeno k
Left Colon
Lap. Left
Colect.
(17/05/16)
pT2 pN0 pM0 G2
Stage I
1 Neg.
(IMA)
(JSCCR
Level 3
253)
< 250 15 Nodes
retrieved
0,05
C.C.
Female
72 Adenok
Right colon
Open
Right
Colectomy
(19/12/2016)
pT3pNopMoG2
Stage II A
1 Neg
(Ileocolic)
(JSCCR
Level 2
202)
<250 20 Nodes
harvested
0,08
G.P.
Male
71 Adeno k
Left Colon
Lap Left
Colect.
(17/05/16)
pT3 pN0 pM0 G2
Stage II A
1 Neg.
(IMA)
(JSCCR
Level 3
253)
< 250 18 Nodes
retrieved
0,06
M.V.
Male
83 Adeno k
Rect Sigmoid
Open pTME
(07/07/16)
pT3 pN0 pM0 G2
Stage II A
1 Neg.
(IMA)
(JSCCR
Level 3
253)
< 250 6 Nodes
retrieved
0,07
< 250 copy = neg.
> 250 copy = pos.
Experience (20 Patients)
(STAGE I / II)
Francesco
Crafa
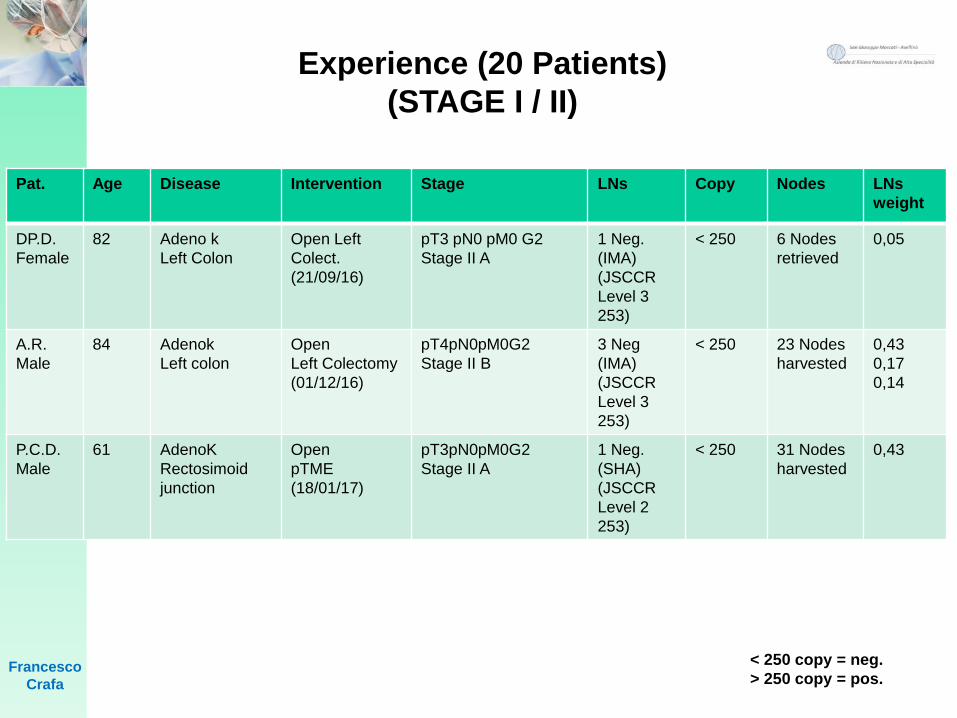
Pat. Age Disease Intervention Stage LNs Copy Nodes LNs
weight
DP.D.
Female
82 Adeno k
Left Colon
Open Left
Colect.
(21/09/16)
pT3 pN0 pM0 G2
Stage II A
1 Neg.
(IMA)
(JSCCR
Level 3
253)
< 250 6 Nodes
retrieved
0,05
A.R.
Male
84 Adenok
Left colon
Open
Left Colectomy
(01/12/16)
pT4pN0pM0G2
Stage II B
3 Neg
(IMA)
(JSCCR
Level 3
253)
< 250 23 Nodes
harvested
0,43
0,17
0,14
P.C.D.
Male
61 AdenoK
Rectosimoid
junction
Open
pTME
(18/01/17)
pT3pN0pM0G2
Stage II A
1 Neg.
(SHA)
(JSCCR
Level 2
253)
< 250 31 Nodes
harvested
0,43
< 250 copy = neg.
> 250 copy = pos.
Experience (20 Patients)
(STAGE I / II)
Francesco
Crafa
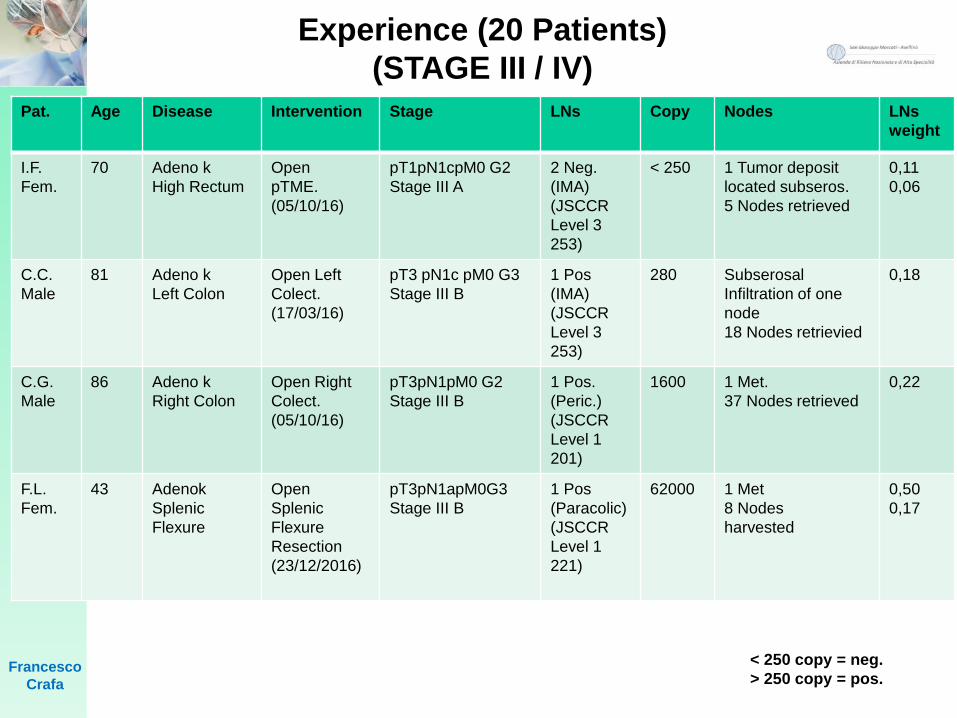
Pat. Age Disease Intervention Stage LNs Copy Nodes LNs
weight
I.F.
Fem.
70 Adeno k
High Rectum
Open
pTME.
(05/10/16)
pT1pN1cpM0 G2
Stage III A
2 Neg.
(IMA)
(JSCCR
Level 3
253)
< 250 1 Tumor deposit
located subseros.
5 Nodes retrieved
0,11
0,06
C.C.
Male
81 Adeno k
Left Colon
Open Left
Colect.
(17/03/16)
pT3 pN1c pM0 G3
Stage III B
1 Pos
(IMA)
(JSCCR
Level 3
253)
280 Subserosal
Infiltration of one
node
18 Nodes retrievied
0,18
C.G.
Male
86 Adeno k
Right Colon
Open Right
Colect.
(05/10/16)
pT3pN1pM0 G2
Stage III B
1 Pos.
(Peric.)
(JSCCR
Level 1
201)
1600 1 Met.
37 Nodes retrieved
0,22
F.L.
Fem.
43 Adenok
Splenic
Flexure
Open
Splenic
Flexure
Resection
(23/12/2016)
pT3pN1apM0G3
Stage III B
1 Pos
(Paracolic)
(JSCCR
Level 1
221)
62000 1 Met
8 Nodes
harvested
0,50
0,17
< 250 copy = neg.
> 250 copy = pos.
Experience (20 Patients)
(STAGE III / IV)
Francesco
Crafa
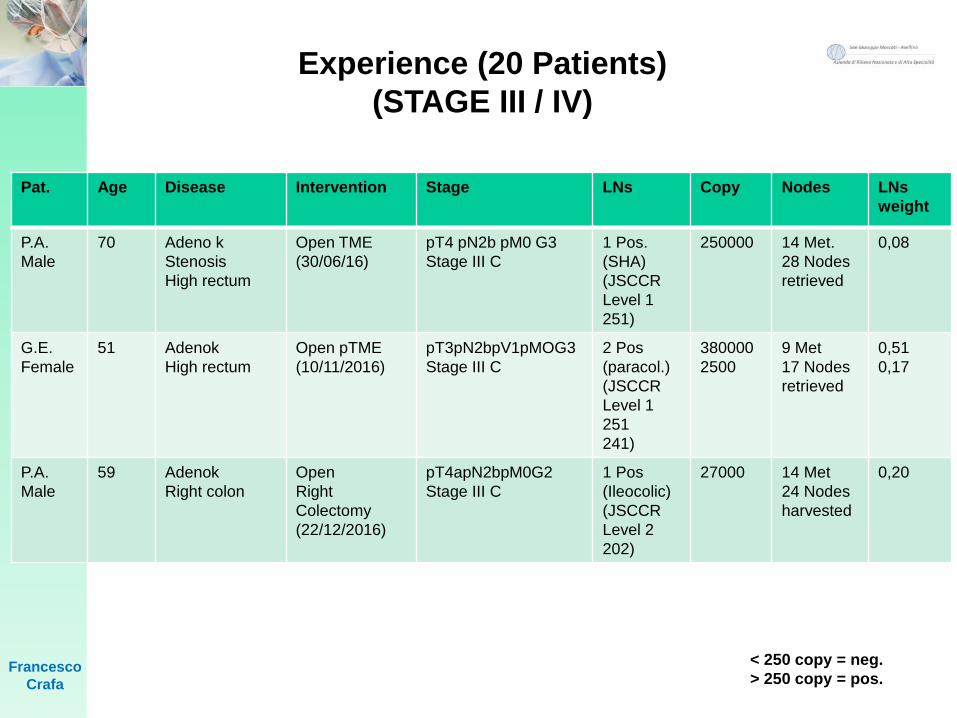
Pat. Age Disease Intervention Stage LNs Copy Nodes LNs
weight
P.A.
Male
70 Adeno k
Stenosis
High rectum
Open TME
(30/06/16)
pT4 pN2b pM0 G3
Stage III C
1 Pos.
(SHA)
(JSCCR
Level 1
251)
250000 14 Met.
28 Nodes
retrieved
0,08
G.E.
Female
51 Adenok
High rectum
Open pTME
(10/11/2016)
pT3pN2bpV1pMOG3
Stage III C
2 Pos
(paracol.)
(JSCCR
Level 1
251
241)
380000
2500
9 Met
17 Nodes
retrieved
0,51
0,17
P.A.
Male
59 Adenok
Right colon
Open
Right
Colectomy
(22/12/2016)
pT4apN2bpM0G2
Stage III C
1 Pos
(Ileocolic)
(JSCCR
Level 2
202)
27000 14 Met
24 Nodes
harvested
0,20
< 250 copy = neg.
> 250 copy = pos.
Experience (20 Patients)
(STAGE III / IV)
Francesco
Crafa
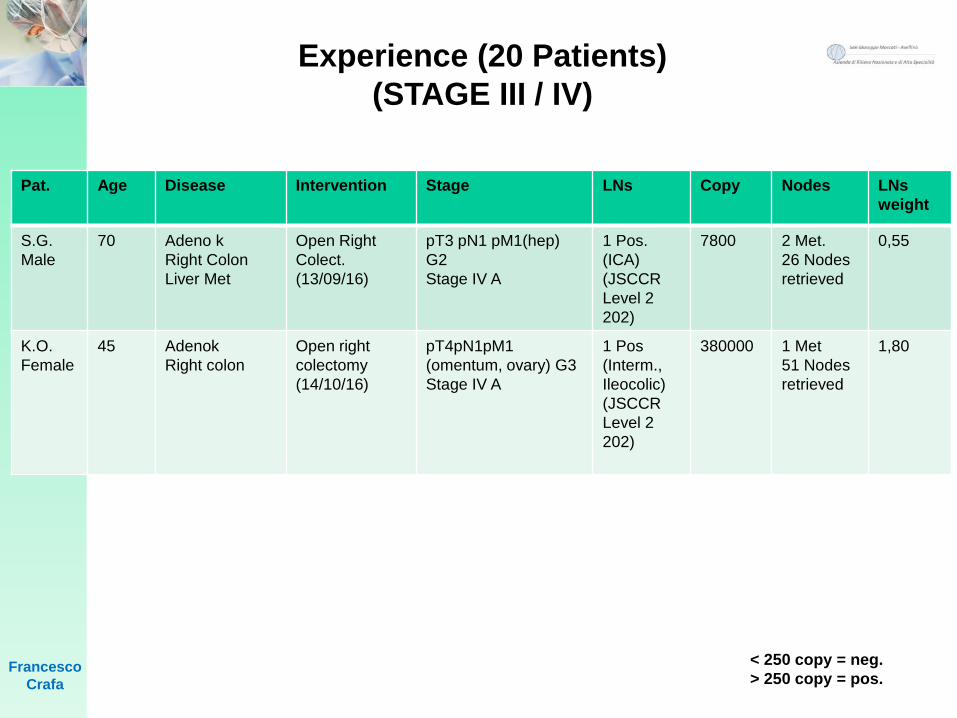
Pat. Age Disease Intervention Stage LNs Copy Nodes LNs
weight
S.G.
Male
70 Adeno k
Right Colon
Liver Met
Open Right
Colect.
(13/09/16)
pT3 pN1 pM1(hep)
G2
Stage IV A
1 Pos.
(ICA)
(JSCCR
Level 2
202)
7800 2 Met.
26 Nodes
retrieved
0,55
K.O.
Female
45 Adenok
Right colon
Open right
colectomy
(14/10/16)
pT4pN1pM1
(omentum, ovary) G3
Stage IV A
1 Pos
(Interm.,
Ileocolic)
(JSCCR
Level 2
202)
380000 1 Met
51 Nodes
retrieved
1,80
< 250 copy = neg.
> 250 copy = pos.
Experience (20 Patients)
(STAGE III / IV)
Francesco
Crafa
DISCUSSION
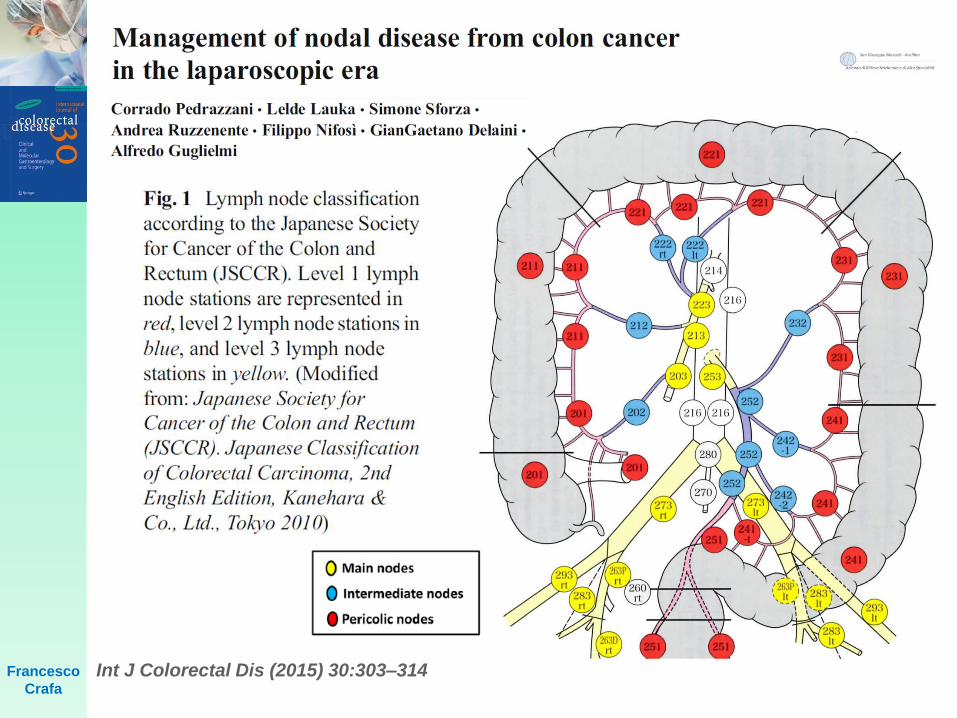
Int J Colorectal Dis (2015) 30:303–314Francesco
Crafa
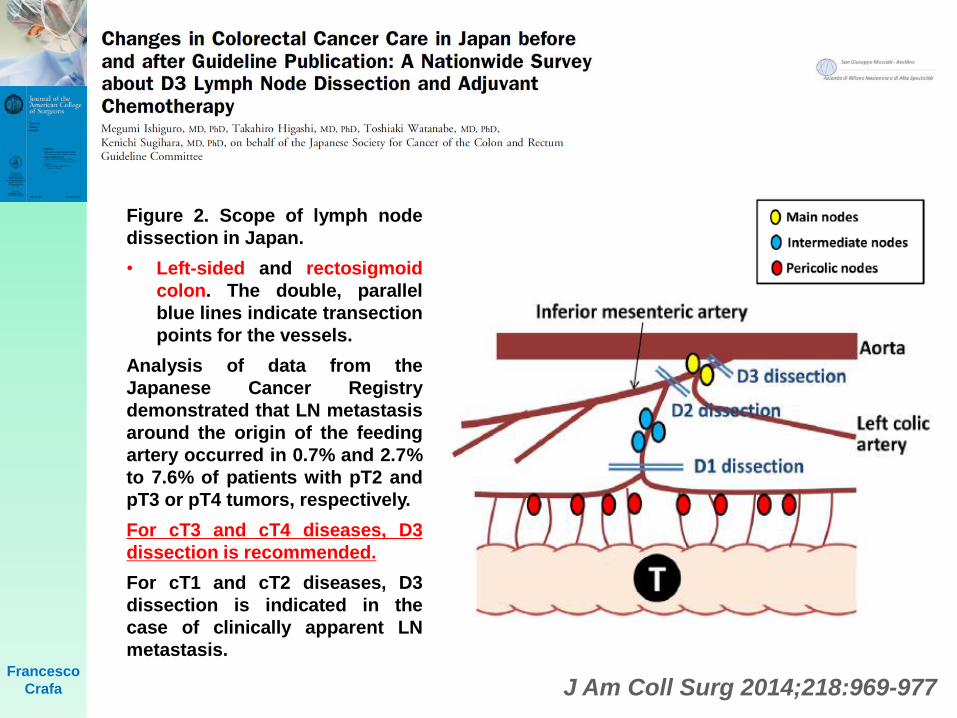
J Am Coll Surg 2014;218:969-977
Figure 2. Scope of lymph node
dissection in Japan.
• Left-sided and rectosigmoid
colon. The double, parallel
blue lines indicate transection
points for the vessels.
Analysis of data from the
Japanese Cancer Registry
demonstrated that LN metastasis
around the origin of the feeding
artery occurred in 0.7% and 2.7%
to 7.6% of patients with pT2 and
pT3 or pT4 tumors, respectively.
For cT3 and cT4 diseases, D3
dissection is recommended.
For cT1 and cT2 diseases, D3
dissection is indicated in the
case of clinically apparent LN
metastasis.Francesco
Crafa
Francesco
Crafa
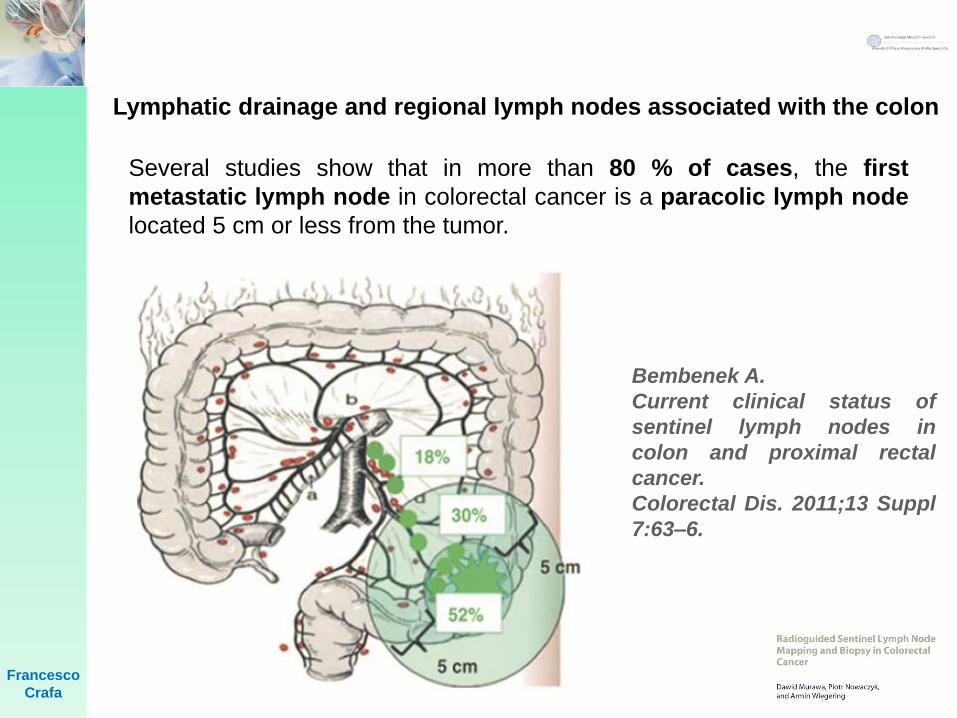
Lymphatic drainage and regional lymph nodes associated with the colon
Several studies show that in more than 80 % of cases, the first
metastatic lymph node in colorectal cancer is a paracolic lymph node
located 5 cm or less from the tumor.
Bembenek A.
Current clinical status of
sentinel lymph nodes in
colon and proximal rectal
cancer.
Colorectal Dis. 2011;13 Suppl
7:63–6.
Francesco
Crafa
Lymphatic drainage and regional lymph nodes associated with the colon
Beside this classic lymphatic drainage, aberrant
drainage within the regional lymph nodes can exist.
Such drainage leads directly to main lymph node
stations near the superior and inferior mesenteric
vessels or to colic and paracolic lymph nodes
located at a significant distance from the tumor.
The prevalence of aberrant lymphatic drainage has
generally been reported to be up to 20 % .
Bilchik AJ, Saha S, Wiese D, et al. Molecular staging of early colon cancer on the basis of sentinel node
analysis: a multicenter phase II trial. J Clin Oncol. 2001;19:1128–36.
Wood TF, Tsioulias GJ, Morton DL, et al. Focused examination of sentinel lymph nodes upstages early
colorectal carcinoma. Am Surg. 2000;66:998–1003.
Saha S, Johnston G, Korant A, et al. Aberrant drainage of sentinel lymph nodes in colon cancer and its
impact on staging and extent of operation. Am J Surg. 2013;205:302–5.
Francesco
Crafa
Lymphatic drainage and regional lymph nodes associated with the colon
Drainage of this nature influences the scope of lymphadenectomy
since “aberrant” lymph nodes are potential locations for “skip
metastases”. In some cases, the first lymph nodes to become
dyed are those on the opposite side of the colon. Instances of
lymphatic drainage from the transverse colon through the
greater omentum to the splenic hilar lymph nodes have also
been published. Moreover, tumors located in the hepatic flexure
can, in about 5 % of cases, metastasize to lymph nodes located
around the head of pancreas and in about 4 % of cases to
omental lymph nodes .
Iddings D, Bilchik A. The biologic significance of micrometastatic disease and sentinel lymph node
technology on colorectal cancer. J Surg Oncol. 2007;96:671–7.
Wood TF, Nora DT, Morton DL, et al. One hundred consecutive cases of sentinel lymph node mapping in
early colorectal carcinoma: detection of missed micrometastases. J Gastrointest Surg. 2002;6:322–9.
Saha S, Monson KM, Bilchik A, et al. Comparative analysis of nodal upstaging between colon and rectal
cancers by sentinel lymph node mapping: a prospective trial. Dis Colon Rectum. 2004;47:1767–72.
Tsioulias GJ, Wood TF, Spirt M, Morton DL, Bilchik AJ. A novel lymphatic mapping technique to improve
localization and staging of early colon cancer during laparoscopic colectomy. Am Surg. 2002;68:561–5.
Hohenberger W, Weber K, Matzel K, et al. Standardized surgery for colonic cancer: complete mesocolic
excision and central ligation-technical notes and outcome. Colorectal Dis. 2009;11: 354–64.
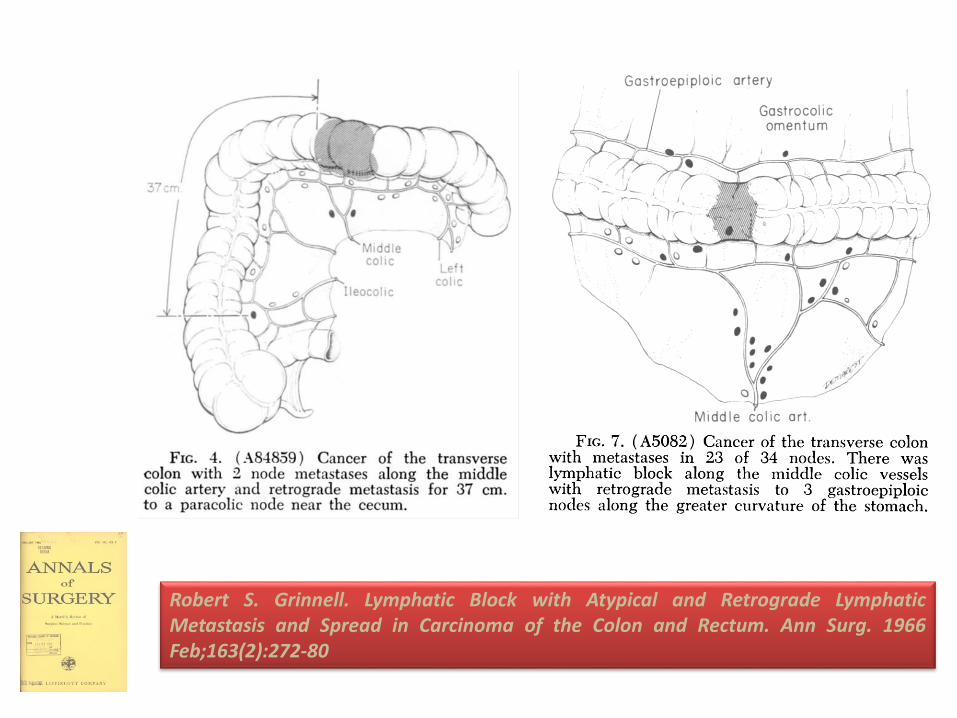
Robert S. Grinnell. Lymphatic Block with Atypical and Retrograde LymphaticMetastasis and Spread in Carcinoma of the Colon and Rectum. Ann Surg. 1966Feb;163(2):272-80
Francesco
Crafa
One of the largest studies analyzed 192 patients with colon cancer.
In 42 (22 %) patients, aberrant lymphatic drainage was observed
which changed the scope of the resection. In 19 patients with
extended scope of resection, metastases were found in lymph
nodes located beyond the standard resection margin, and in two
of these patients, these lymph nodes were the only sites of
metastases. Furthermore, metastases to lymph nodes were
detected in 62 % of patients in whom the scope of resection was
extended after lymphatic mapping, compared with only 43 % of
those who underwent standard resection. In the extended resection
group, an average of 17.6 lymph nodes was examined, while in the
standard resection group, the average was 15.8. Analysis of the data
indicates that aberrant lymphatic drainage influences disease
management, assessment of the disease stage, and, to a limited
extent, survival.
Saha S, Johnston G, Korant A, et al. Aberrant drainage of
sentinel lymph nodes in colon cancer and its impact on staging
and extent of operation. Am J Surg. 2013;205:302–5.
Francesco
Crafa
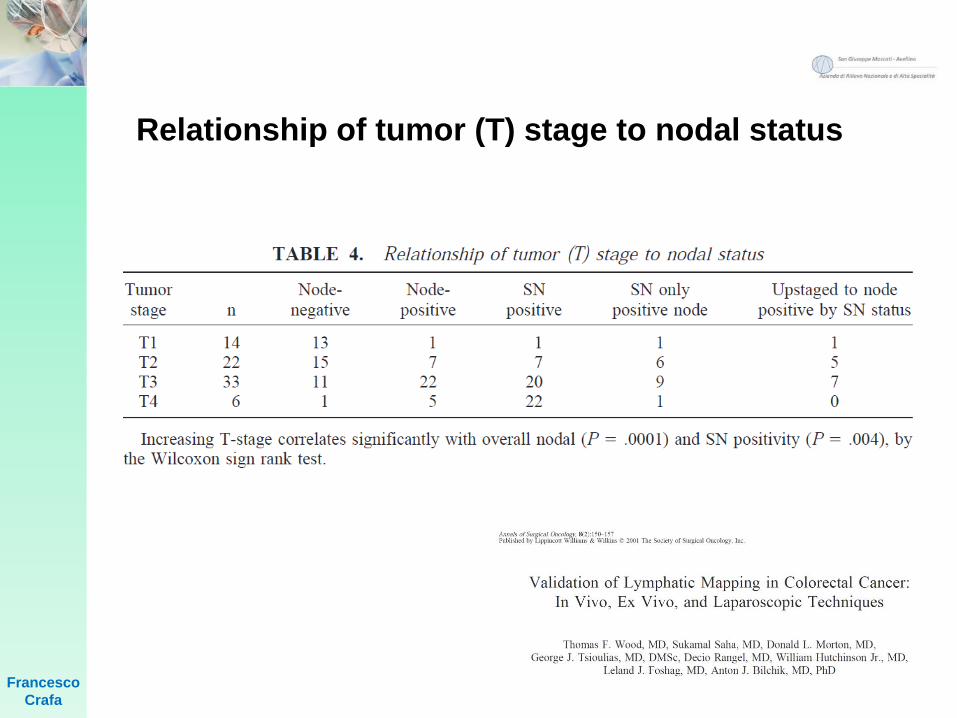
Relationship of tumor (T) stage to nodal status
Francesco
Crafa
In a study in 2014, 55 patients with colon cancer after
SLN biopsy were compared with a control group of 110
patients adjusted for tumor-related factors and operated
on without SLN biopsy. The average number of
examined lymph nodes in the clinical and control
group differed significantly, being nine and seven,
respectively ( p = 0.03).
Braat AE, Pol RA, Oosterhuis JW, et al. Excellent prognosis of node negative
patients after sentinel node procedure in colon carcinoma: a 5-year follow up study.
Eur J Surg Oncol. 2014;40:747–55.
Francesco
Crafa
Immunochemistry resulted in upstaging owing to the
detection of metastases in 3 of 38 SLNs initially
considered true negative. The 5-year survival rates
differed significantly in the two groups: 83 % in the SLN
biopsy group vs. 69 % in the control group with no
SLN biopsy ( p = 0.03). Furthermore, within the SLN
group, the 5-year survival rate was higher in SLN
negative patients (91 % vs. 76 %; p = 0.04). The authors
emphasized the excellent prognosis in SLN-negative
patients when using H&E stain and immunochemistry
together with automated microscopy.
Braat AE, Pol RA, Oosterhuis JW, et al. Excellent prognosis of node negative
patients after sentinel node procedure in colon carcinoma: a 5-year followup study.
Eur J Surg Oncol. 2014;40:747–55.
Francesco Crafa
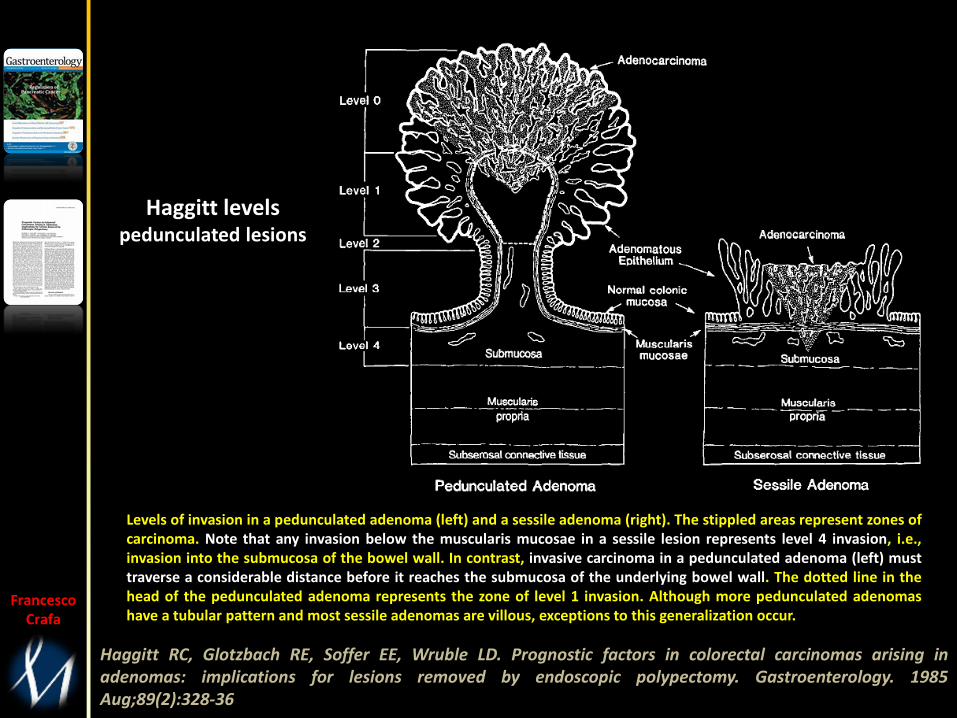
Haggitt RC, Glotzbach RE, Soffer EE, Wruble LD. Prognostic factors in colorectal carcinomas arising inadenomas: implications for lesions removed by endoscopic polypectomy. Gastroenterology. 1985Aug;89(2):328-36
Levels of invasion in a pedunculated adenoma (left) and a sessile adenoma (right). The stippled areas represent zones ofcarcinoma. Note that any invasion below the muscularis mucosae in a sessile lesion represents level 4 invasion, i.e.,invasion into the submucosa of the bowel wall. In contrast, invasive carcinoma in a pedunculated adenoma (left) musttraverse a considerable distance before it reaches the submucosa of the underlying bowel wall. The dotted line in thehead of the pedunculated adenoma represents the zone of level 1 invasion. Although more pedunculated adenomashave a tubular pattern and most sessile adenomas are villous, exceptions to this generalization occur.
Haggitt levelspedunculated lesions
Francesco Crafa
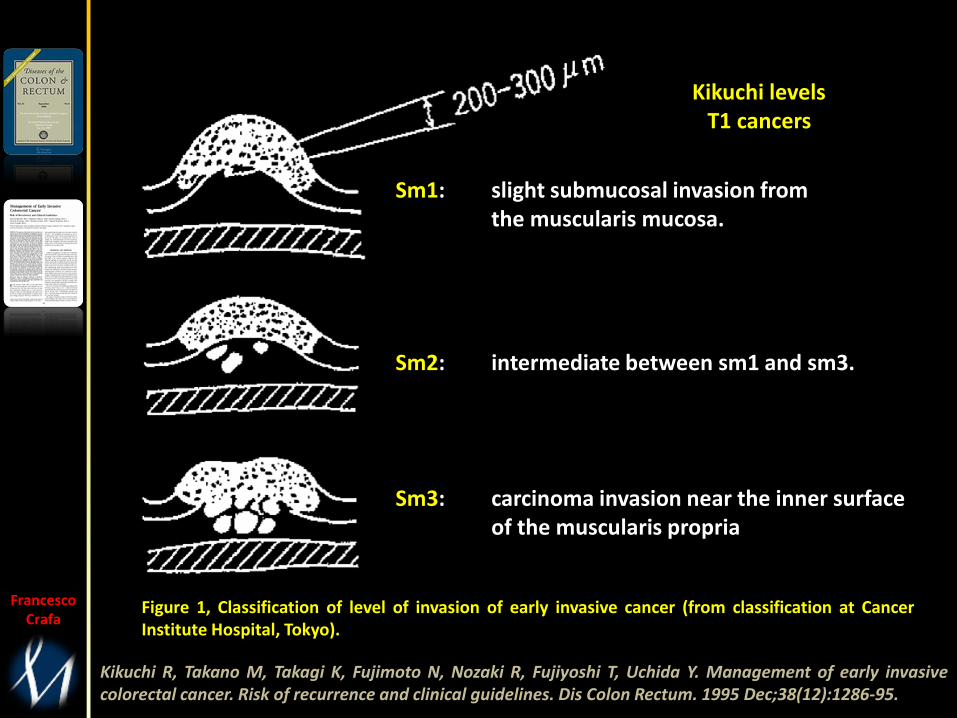
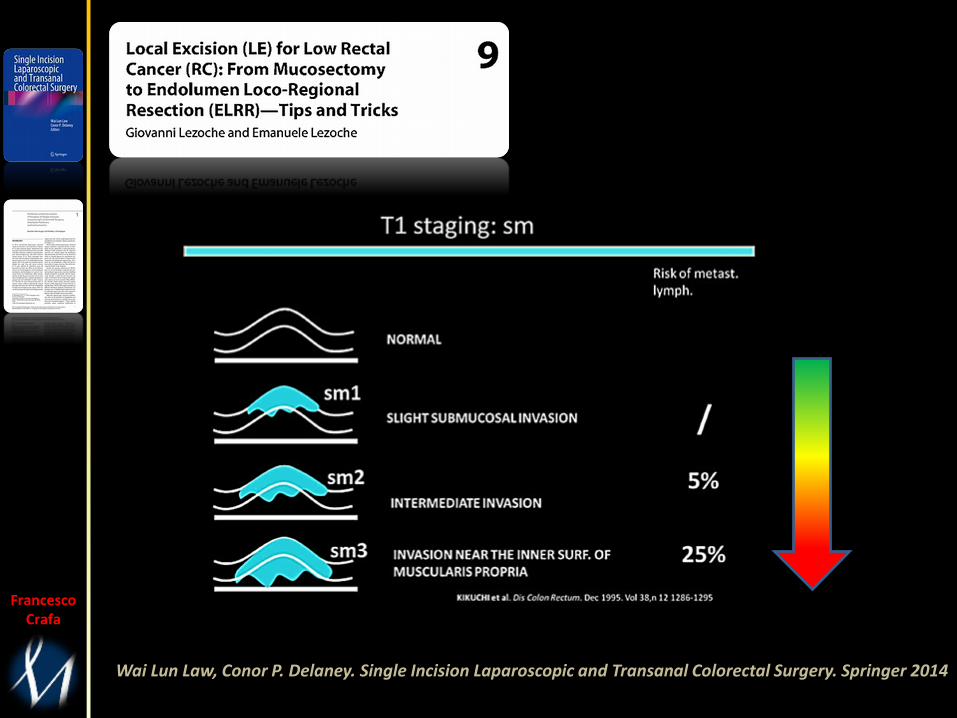
Kikuchi R, Takano M, Takagi K, Fujimoto N, Nozaki R, Fujiyoshi T, Uchida Y. Management of early invasivecolorectal cancer. Risk of recurrence and clinical guidelines. Dis Colon Rectum. 1995 Dec;38(12):1286-95.
Figure 1, Classification of level of invasion of early invasive cancer (from classification at CancerInstitute Hospital, Tokyo).
Sm1: slight submucosal invasion fromthe muscularis mucosa.
Sm2: intermediate between sm1 and sm3.
Sm3: carcinoma invasion near the inner surfaceof the muscularis propria
Kikuchi levelsT1 cancers
Francesco Crafa
Wai Lun Law, Conor P. Delaney. Single Incision Laparoscopic and Transanal Colorectal Surgery. Springer 2014
Francesco Crafa
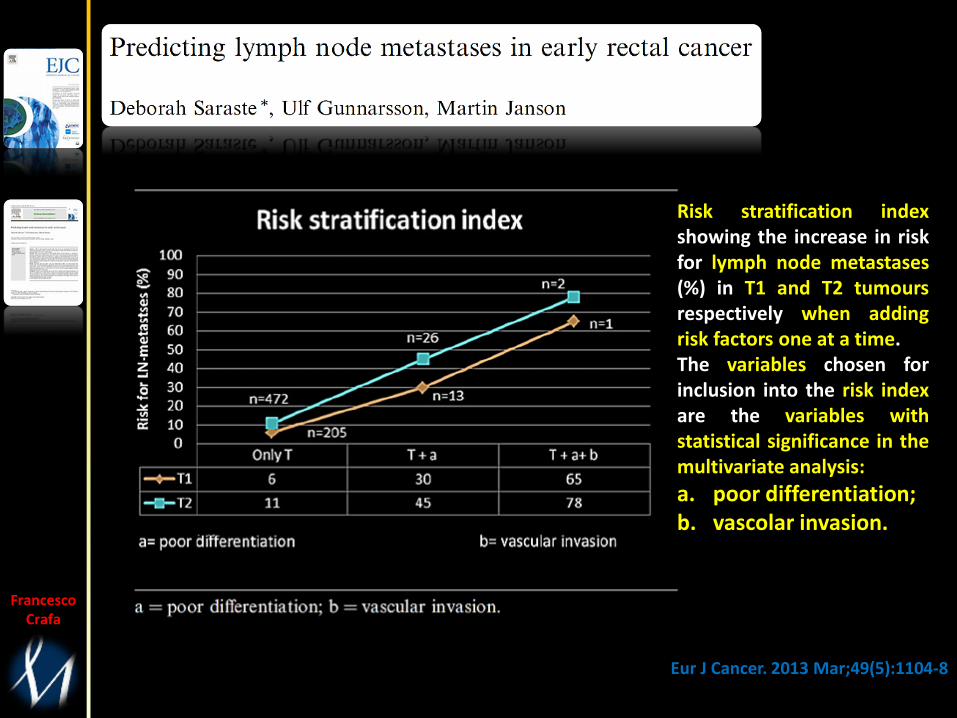
Eur J Cancer. 2013 Mar;49(5):1104-8
Risk stratification indexshowing the increase in riskfor lymph node metastases(%) in T1 and T2 tumoursrespectively when addingrisk factors one at a time.The variables chosen forinclusion into the risk indexare the variables withstatistical significance in themultivariate analysis:
a. poor differentiation;b. vascolar invasion.
Francesco Crafa
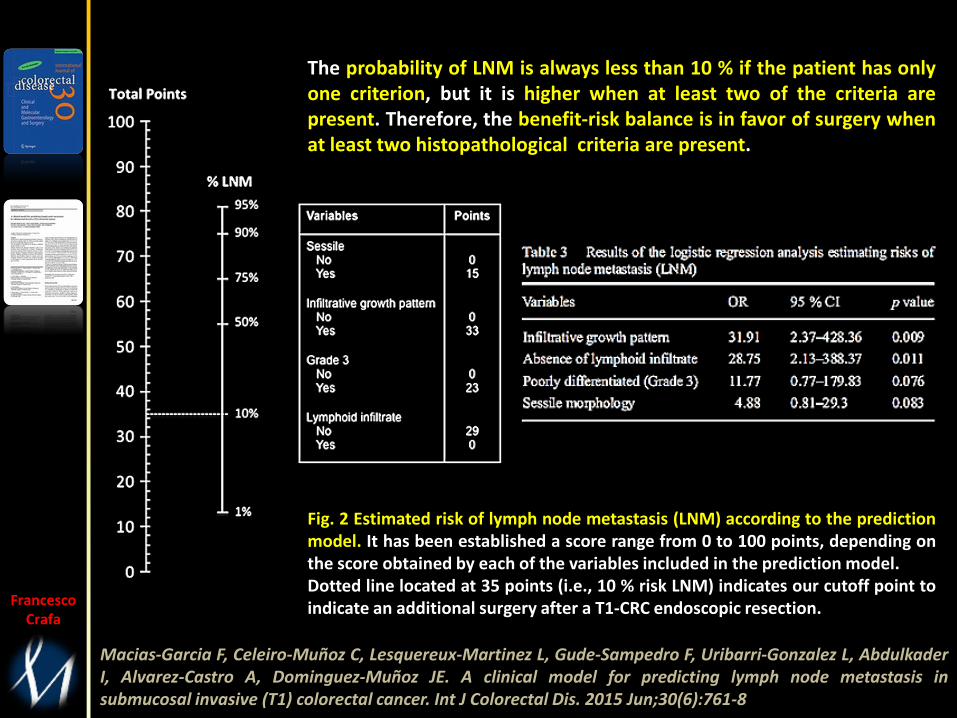
Macias-Garcia F, Celeiro-Muñoz C, Lesquereux-Martinez L, Gude-Sampedro F, Uribarri-Gonzalez L, AbdulkaderI, Alvarez-Castro A, Dominguez-Muñoz JE. A clinical model for predicting lymph node metastasis insubmucosal invasive (T1) colorectal cancer. Int J Colorectal Dis. 2015 Jun;30(6):761-8
Fig. 2 Estimated risk of lymph node metastasis (LNM) according to the predictionmodel. It has been established a score range from 0 to 100 points, depending onthe score obtained by each of the variables included in the prediction model.Dotted line located at 35 points (i.e., 10 % risk LNM) indicates our cutoff point toindicate an additional surgery after a T1-CRC endoscopic resection.
The probability of LNM is always less than 10 % if the patient has onlyone criterion, but it is higher when at least two of the criteria arepresent. Therefore, the benefit-risk balance is in favor of surgery whenat least two histopathological criteria are present.
Francesco
Crafa
Francesco
Crafa
Published evidence
Three prospective observational studies were
selected for inclusion (n=2,232 lymph node [LN]
specimens from 253 people) and reported that
the diagnostic performance of OSNA was
better than standard histopathology.
Francesco
Crafa
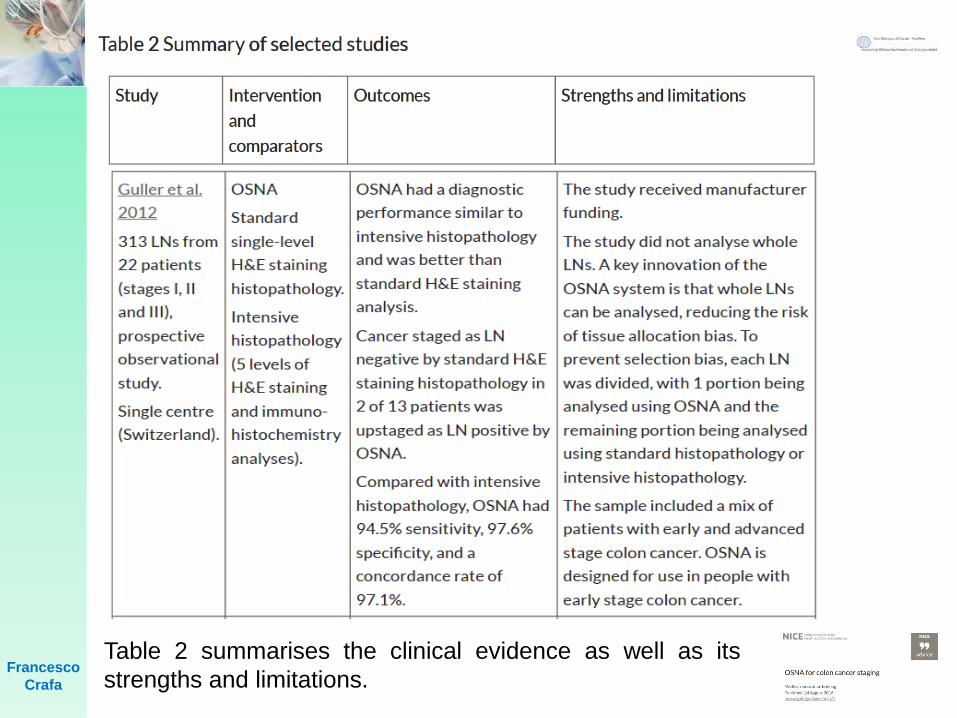
Table 2 summarises the clinical evidence as well as its
strengths and limitations.
Francesco
Crafa
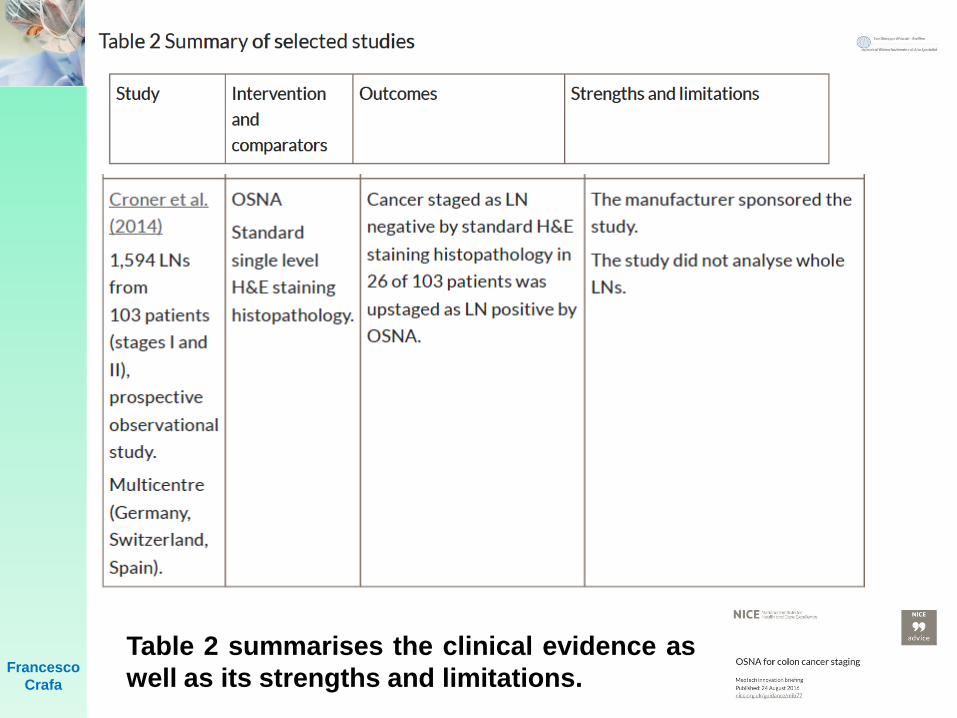
Table 2 summarises the clinical evidence as
well as its strengths and limitations.
Francesco
Crafa
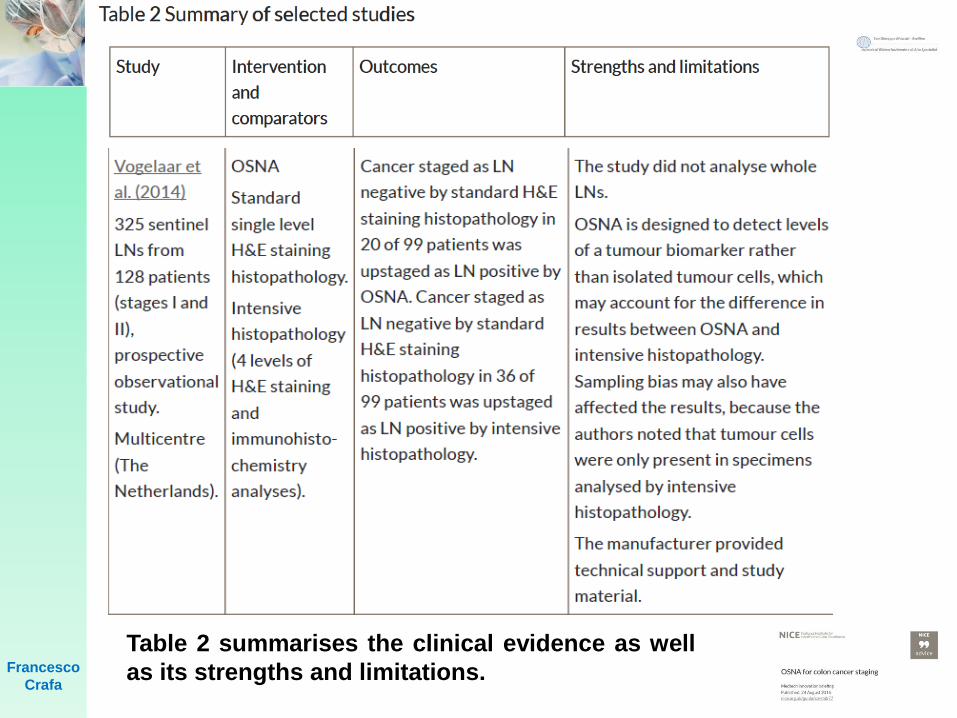
Table 2 summarises the clinical evidence as well
as its strengths and limitations.
Francesco
Crafa
Strengths and limitations of the
evidence
Although all the studies were prospective in design,
none were randomised controlled trials which would
have helped to systematically control for biases. All 3
studies were observational rather than randomised
controlled studies.
Two studies investigated OSNA in LNs, and 1 study
assessed OSNA in sentinel LNs. LNs have a differing
potential to sentinel LNs to harbour metastases, so
the study results may not be directly comparable.
Francesco
Crafa
Yamamoto performed a clinical study based on
385 LNs, and concluded that OSNA is
comparable to a 2 mm interval
histopathological examination in its ability to
detect LN metastases.
Yamamoto H, Sekimoto M, Oya M, Yamamoto N, Konishi F, Sasaki J, et al.
OSNA-based novel molecular testing for lymph node metastases in colorectal
cancer patients: results from a multicenter clinical performance study in Japan.
Ann Surg Oncol. 2011;18(7):1891–8.
Francesco
Crafa
Francesco
Crafa
Examination of 1925 LNs at a variety of TNM
stages revealed 95.7 % concordance, 86.2 %
sensitivity, and 96.5 % specificity when every LN
was halved and examined using both H&E staining
and the OSNA assay. Only 20 of 1925 LNs (1.0%)
were H&E-positive and OSNA-negative. This
discrepancy could be attributed to allocation bias
(uneven location of metastatic tumor cells), as
previously described.
Yamamoto H, Sekimoto M, Oya M, Yamamoto N, Konishi F, Sasaki J, et
al. OSNA-based novel molecular testing for lymph node metastases in
colorectal cancer patients: results from a multicenter clinical performance
study in Japan. Ann Surg Oncol. 2011;18(7):1891–8.
Francesco
Crafa
In contrast, 63 of 1925 LNs were H&E-
negative, yet OSNA-positive (3.3 %).
Overall, the results led to the upstaging
of TNM stage in 11.3 % of patients with
stage I and stage II disease and 7.1 %
for stage III patients.
Francesco
Crafa
Among 204 CRC patients, 124 cases were
node-negative at stage I and stage II. OSNA
positive cases were observed in 2.0 % of
stage I CRC and 17.6 % (13 of 74 cases) of
stage II CRC; these cases had more advanced
features of CRC, such as deeper invasion to
the colonic wall and severe invasion to
lymphatic invasion compared with OSNA-
negative cases.
Francesco
Crafa
CONCLUSION
Francesco
Crafa
IMPROVE STAGING BY A FOCUSED ULTRASTAGING
EXAMINATION OF THE SNs
OSNA IS SIMILAR TO A 2 MM INTERVAL H.E. WITH
H&E SECTIONS.
OSNA STAGING USING THE WHOLE LNs
UPSTAGE COLONIC CANCER
ADDITIONAL RISK FACTOR FOR D.R. IN STAGE II
CRC
ADJUVANT TREATMENT
ORGAN SPARING SURGERY
TAILORED LYMPHADENECTOMY
ABERRANT AND SKIP METASTASES
QUALITY OF THE LIMPHADENECTOMY
NOVEL MOLECULAR STAGING
Francesco
Crafa
Therefore, false-negative cases would be exceptional if whole
LNs were subject to OSNA. UICC classification distinguishes
TNM stages between < 3 LN metastases and > 4 LN metastases.
Yamamoto found that the sum of CK19 mRNA increased as the
number of histologically positive LNs increased. Indeed, the
median value of CK19 mRNA was significantly smaller in
patients with < 3 regional LN metastases than in those with >
4 regional LN metastases.
These findings indicate that sum of CK19 mRNA assessed by
OSNA displays a trend compatible to the current pathological
diagnosis system. These findings suggest the future possibility
of novel molecular staging using OSNA, based on metastasis
volume (amount of CK19 mRNA) rather than number of LN
metastases.

Francesco
Crafa
ICG AND OSNA are the
route to tailor-made
surgery

Francesco Crafa
Francesco
Crafa
Sentinel node in gastric cancer
F. Crafa, A. Noviello
General and Emergency Surgery Unit
Chief: F. Crafa M.D.
San Giuseppe Moscati Hospital
Hospital of National Relevance and High Specialty
Avellino
Italy
Francesco
Crafa
SN is defined as the first LN to receive
cancer cell drainage from the primary
tumor, and the LN to which cancer cells
metastasize at the beginning. The idea that
the tumor status of SN reflects
“efficiently” the status of the other LNs
represents the main concept of this
technique.
Sentinel node (SN)
Francesco
Crafa
Minimally invasive surgery such as limited
LN dissection and reduced extent of
resection based on SN mapping is termed
SN navigation surgery (SNNS). This
surgery may prevent the post-operative
complications and serve as a useful tool
for avoiding an over invasive surgery.
Sentinel node navigation surgery
(SNNS)
Francesco Crafa
Chang-Ming Huang, Chao-Hui Zheng. Laparoscopic Gastrectomy for Gastric Cancer. Springer 2015
The lymphatic drainage of the stomach is customarily divided intofour areas according to the four feeding arteries of the gastric walls:
District I(right gastroepiploic artery (RGEA) group): This lymphaticnetwork mainly drains the greater curvature of the lower half ofthe gastric body and the pylorus.
District II
(left gastroepiploic and short gastric arteries group): Thislymphatic network mainly drains the greater curvature of the lefthalf of the gastric fundus and the greater curvature of the upperhalf of the gastric body.
District III(left gastric artery (LGA) group): This lymphatic network mainlydrains the right half of the fundus, left half of the lessercurvature, and cardia of the stomach.
District IV(right gastric artery (RGA) group): This area mainly drains thelesser curvature of the gastric pylorus.
Francesco Crafa
In addition to the general LNM pattern via the lymph vessels, someparticular LNM patterns may occur as follows:
Chang-Ming Huang, Chao-Hui Zheng. Laparoscopic Gastrectomy for Gastric Cancer. Springer 2015
Retrograde metastasis
The lymph vessels among different districts communicate with oneanother, and retrograde motion may exist even under normal conditions.Additionally, cancer emboli may obstruct the lymphatic vessels or LNs,increasing the risk of retrograde movement.
Skipmetastasis
Metastatic spread may skip regional draining LNs to form distant nodalmetastases via the collateral branches of the lymph vessels. Therefore, itis important for the surgeon to dissect the distal LNs during surgery.
Virchow ’ s metastasis
The supraclavicular LNs are located at the point at which the thoracicduct drains into the left jugular vein. Metastasis of these LNs is calledVirchow’s metastasis. Metastasis of Virchow’s node is considered to bestrongly indicative of the presence of extensive metastasis in theretroperitoneal tissue around the abdominal aorta.
Francesco
Crafa
In general, SN mapping and biopsy is
indicated in:
(I) patients with T1 or T2 tumors;
(II) primary lesions < than 4 cm in
diameter;
(III) clinical N0 gastric cancer.
Sentinel node navigation surgery
(SNNS)
Takeuchi H, Kitagawa Y. New sentinel node mapping technologies for early gastric
cancer. Ann Surg Oncol 2013;20:522-32.
Kitagawa Y, Takeuchi H, Takagi Y, et al. Sentinel node mapping for gastric cancer: a
prospective multicenter trial in Japan. J Clin Oncol 2013;31:3704-10.
Francesco
Crafa
A recent study demonstrated that 91% of patients with
T1 tumors and 88% with T2 tumors had stained SLNs
as compared to only 68% of patients with T3 tumors.
SN mapping in T1 and T2 gastric cancers may be
useful in the decision-making process with regard to
the extent of lymphadenectomy.
As well as for other cancer types, SN mapping should
not be performed in cases with positive LN metastasis
identified by preoperative imaging diagnostic modalities
such as ultrasonography and CT
Sentinel node navigation surgery
(SNNS)
Takeuchi H, Kitagawa Y. New sentinel node mapping technologies for early gastric
cancer. Ann Surg Oncol 2013;20:522-32.
Kitagawa Y, Takeuchi H, Takagi Y, et al. Sentinel node mapping for gastric cancer: a
prospective multicenter trial in Japan. J Clin Oncol 2013;31:3704-10.
Francesco
Crafa
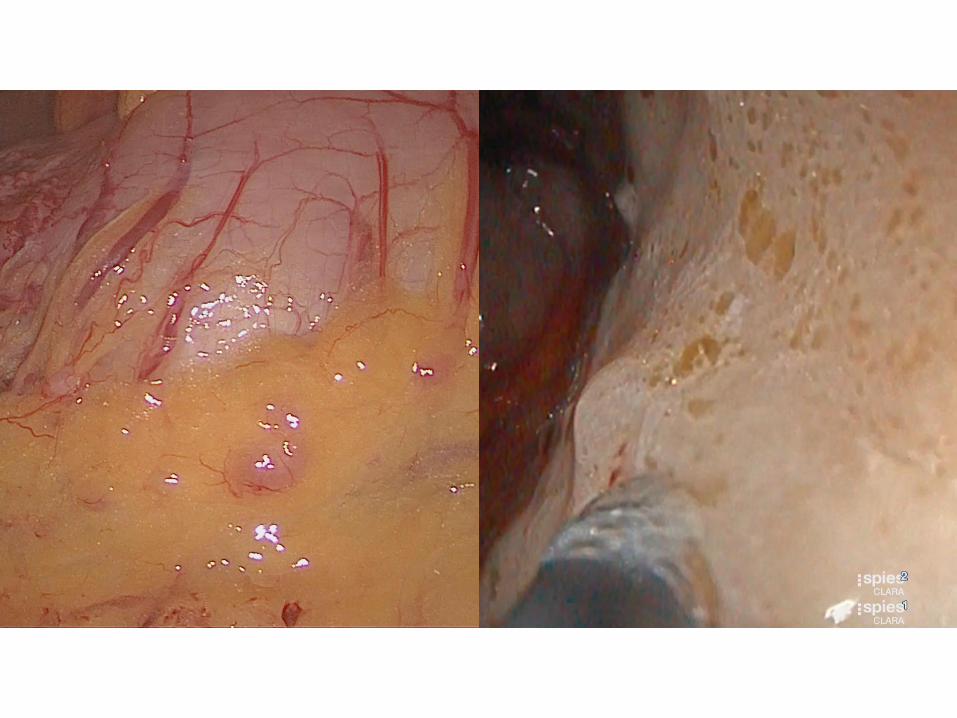
Moreover, a different and innovative type of
fluorescence imaging system was recently developed
for SN navigation surgery. The photodynamic eye
(PDE) is able to visualize ICG fluorescence emitted by
a light-emitting diode. The PDE visualizes SNs and
lymphatic vessels more clearly than the usual ICG
method. However, it is necessary to make the
operating room pitch-darkness for detecting SLNs
while performing SN mapping.
Sentinel node navigation surgery
(SNNS)
Kusano M, Tajima Y, Yamazaki K, et al. Sentinel node mapping guided by indocyanine
green fluorescence imaging: a new method for sentinel node navigation surgery in
gastrointestinal cancer. Dig Surg 2008;25:103-8.
Francesco
Crafa
Novel, sophisticated ICG fluorescence systems
such as the D-light P system do not need for
switching off the lights in order to detect SN.
What is more, with this novel system, SN
examination even in laparoscopic surgery can
be safely performed. Therefore, in the near
future, this method could become the standard
method to detect SN in GI malignancies.
Sentinel node navigation surgery
(SNNS)
Francesco
Crafa
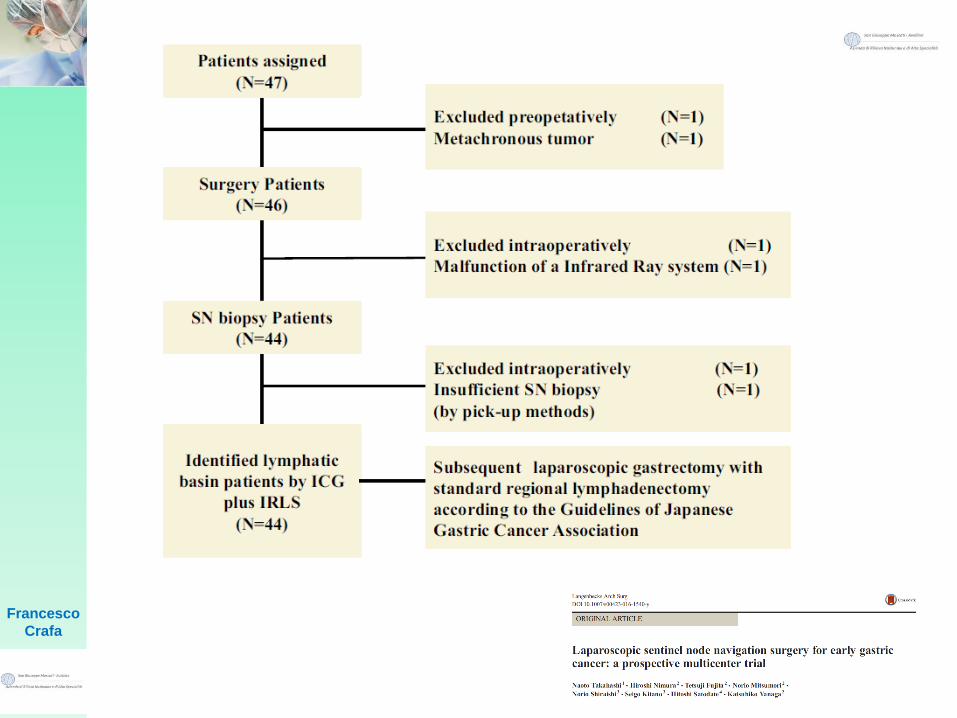
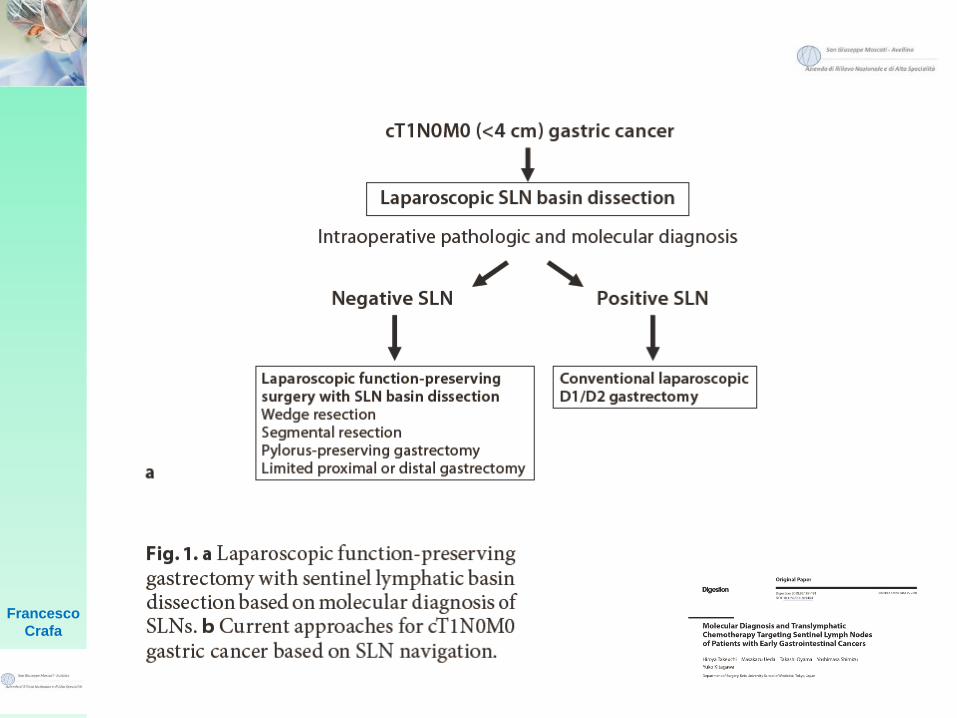
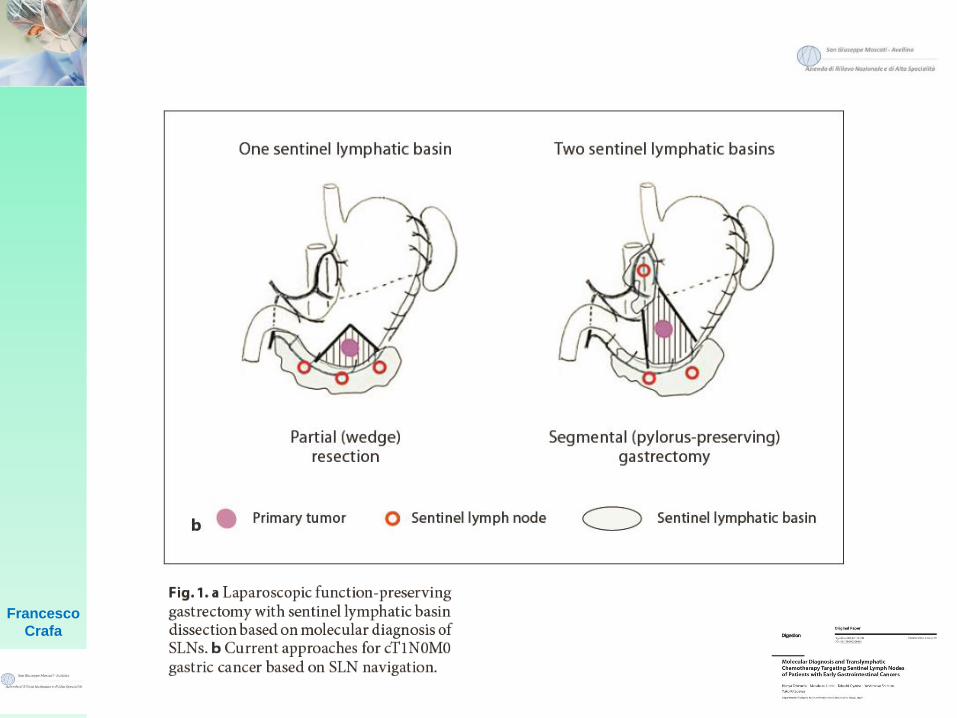
Francesco
Crafa
Patients with previously untreated
Ct1n0m0 gastric adenocarcinomas
less than 4 cm in gross diameter
were eligible for inclusion in this
study.
Francesco
Crafa
Francesco
Crafa
Francesco
Crafa
Francesco
Crafa
Notably, the diagnostic accuracy
of SN mapping for cT2 tumors is
currently suboptimal; therefore,
we believe that the clinical
application of SN mapping should
be limited to cT1 tumors.
Francesco
Crafa
Francesco
Crafa
Francesco
Crafa
Francesco
Crafa
Francesco
Crafa
Francesco
Crafa
Francesco
Crafa
Francesco
Crafa
Francesco
Crafa
In addition, after detecting the SN, the next step is the biopsy.
Intraoperative diagnosis using hematoxylin and eosin (H-E)
staining of a frozen section from the LN represents the gold
standard technique for SN biopsy. However, the reliability of frozen
section examination has been under evaluation. In this way, in a
Japanese multicenter trial, it was found that ~25% of patients
with SN metastases that were diagnosed using permanent
sections could not be identified using H-E staining of frozen
sections collected intraoperatively.
Sentinel node navigation surgery
(SNNS)
Japanese Gastric Cancer Association. Japanese gastric cancer treatment guidelines 2010
(ver. 3). Gastric Cancer 2011;14:113-23.
Kitagawa Y, Takeuchi H, Takagi Y, et al.
Sentinel node mapping for gastric cancer: a prospective multicenter trial in Japan. J Clin
Oncol 2013;31:3704-10.
Francesco
Crafa
Multistep level sections, immunohistochemistry,
reverse transcription polymerase chain reaction
(RT-PCR), and the one-step nucleic acid
amplification assay (OSNA), have all been
developed to reduce the false-negative rates
and provide reliable diagnostic tools for
micrometastases in SN.
Sentinel node navigation surgery
(SNNS)
Takeuchi H, Ueda M, Oyama T, et al. Molecular diagnosis and translymphatic chemotherapy targeting sentinel
lymph nodes of patients with early gastrointestinal cancers. Digestion 2010;82:187-91.
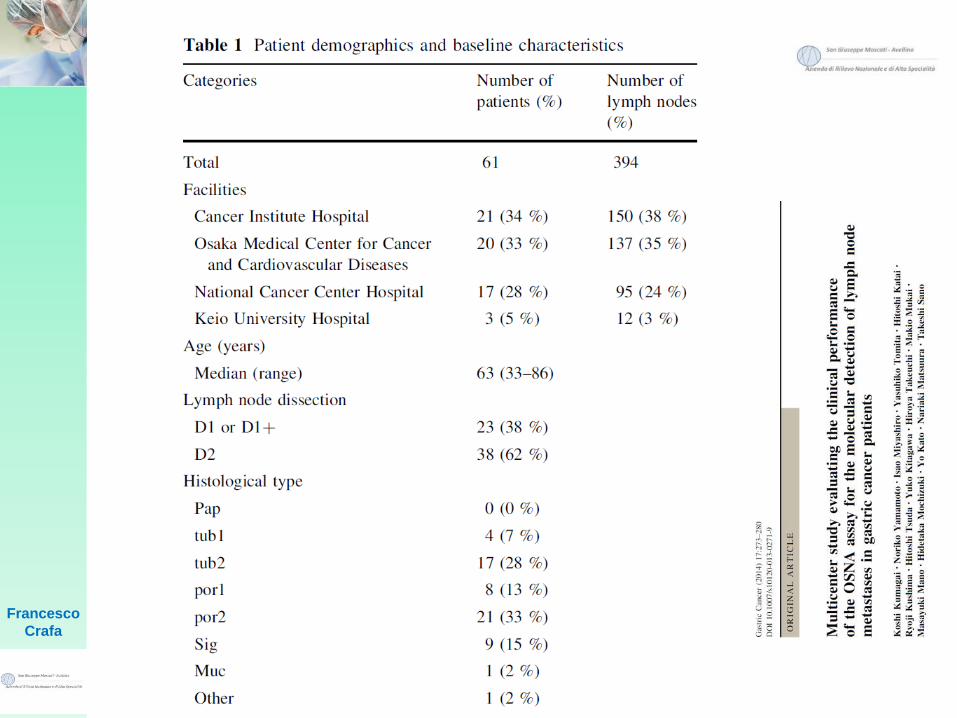
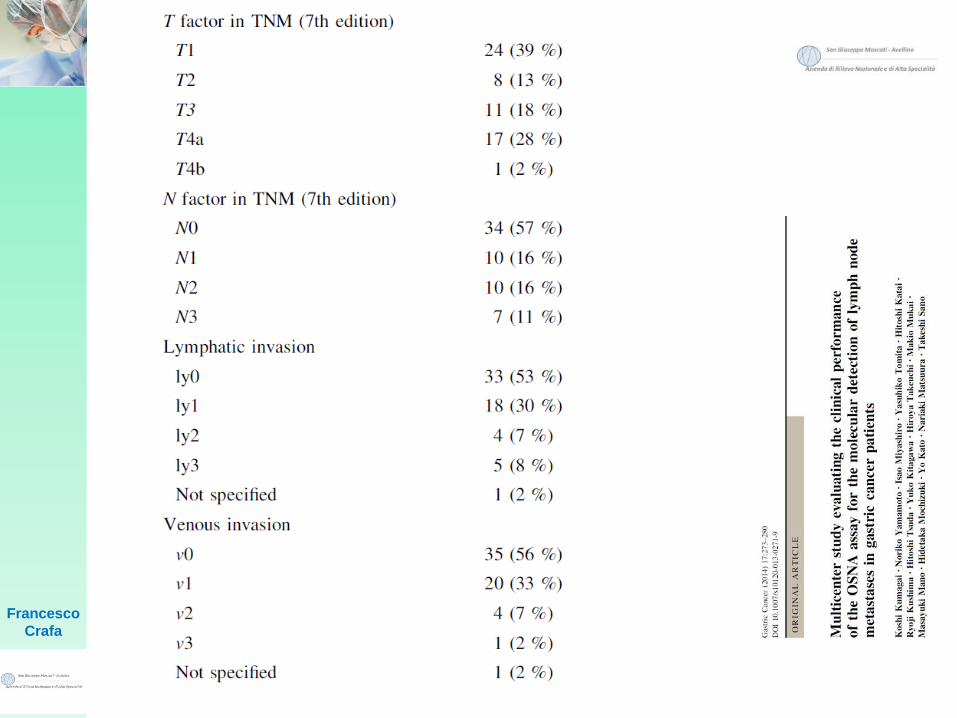
Kumagai K, Yamamoto N, Miyashiro I, et al. Multicenter study evaluating the clinical performance of the OSNA
assay for the molecular detection of lymph node metastases in gastric cancer patients. Gastric Cancer
2014;17:273-80.
Yanagita S, Natsugoe S, Uenosono Y, et al. Detection of micrometastases in sentinel node navigation surgery
for gastric cancer. Surg Oncol 2008;17:203-10.
Francesco
Crafa
Moreover, Kumagai et al. demonstrated that the
sensitivity and specificity of the OSNA assay was
higher than conventional examination. Recently, it
has been possible to reduce the detection time to ~30
min, and these innovative techniques have also raised
the sensitivity to detect SN metastases as part of the
intraoperative diagnostic algorithm.
Sentinel node navigation surgery
(SNNS)
Takeuchi H, Ueda M, Oyama T, et al. Molecular diagnosis and translymphatic chemotherapy targeting sentinel
lymph nodes of patients with early gastrointestinal cancers. Digestion 2010;82:187-91.
Kumagai K, Yamamoto N, Miyashiro I, et al. Multicenter study evaluating the clinical performance of the OSNA
assay for the molecular detection of lymph node metastases in gastric cancer patients. Gastric Cancer
2014;17:273-80.
Yanagita S, Natsugoe S, Uenosono Y, et al. Detection of micrometastases in sentinel node navigation surgery
for gastric cancer. Surg Oncol 2008;17:203-10.
Francesco
Crafa
Francesco
Crafa
Francesco
Crafa
Francesco
Crafa
Francesco
Crafa
Francesco
Crafa
Francesco
Crafa
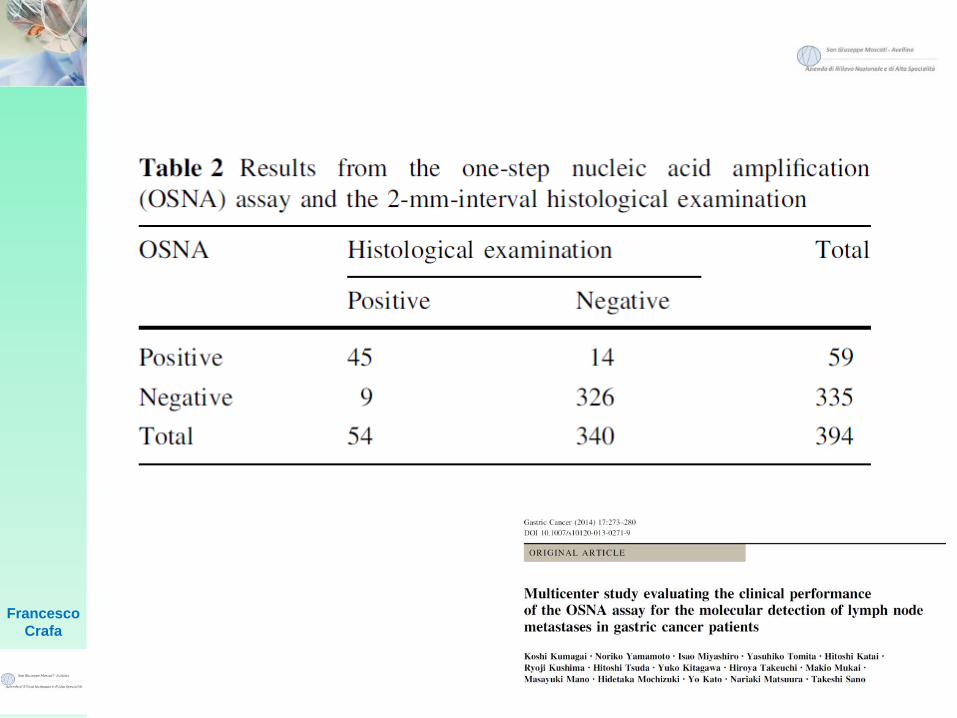
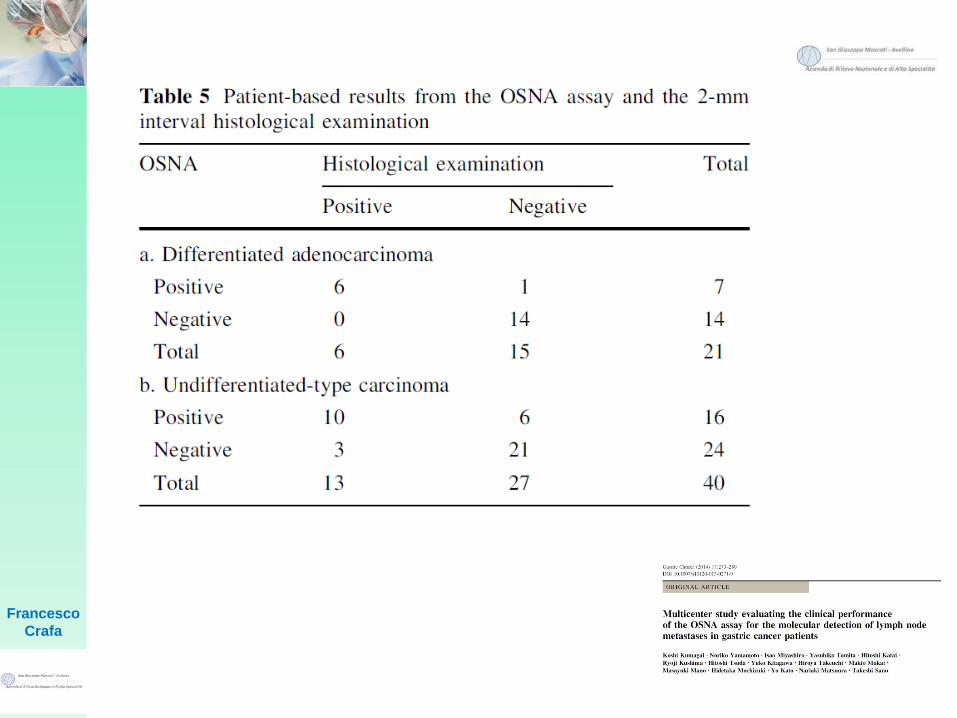
In this study, the OSNA assay was shown to provide a
diagnostic ability equivalent to that of the
postoperative 2-mm-interval histological
examination, as the concordance rate between the
two methods for 394 LNs from 61 patients was 0.942
(95 % CI, 0.914–0.963), in which the lower limit of the
95 % CI exceeded the predetermined target value of
0.83. In addition, this study also showed that the
specificity of the OSNA assay for detecting LN
metastases in 32 ‘‘node-negative patients’’ was 0.991
(95 % CI, 0.966–0.999).
Francesco
Crafa
There were 23 discordant results between the OSNA
assay and histological examination: 14 LNs were
histologically negative but positive in the OSNA
assay, and 9 LNs were histologically positive but
negative in the OSNA assay. As the LN blocks used
for the OSNA assay and histological examination were
obtained from different parts of the LN, discordant
results between the methods cannot be completely
avoided for reasons of tissue allocation bias: the
metastasis could be localized in the blocks used for the
OSNA assay or in the blocks for histology.
Francesco
Crafa
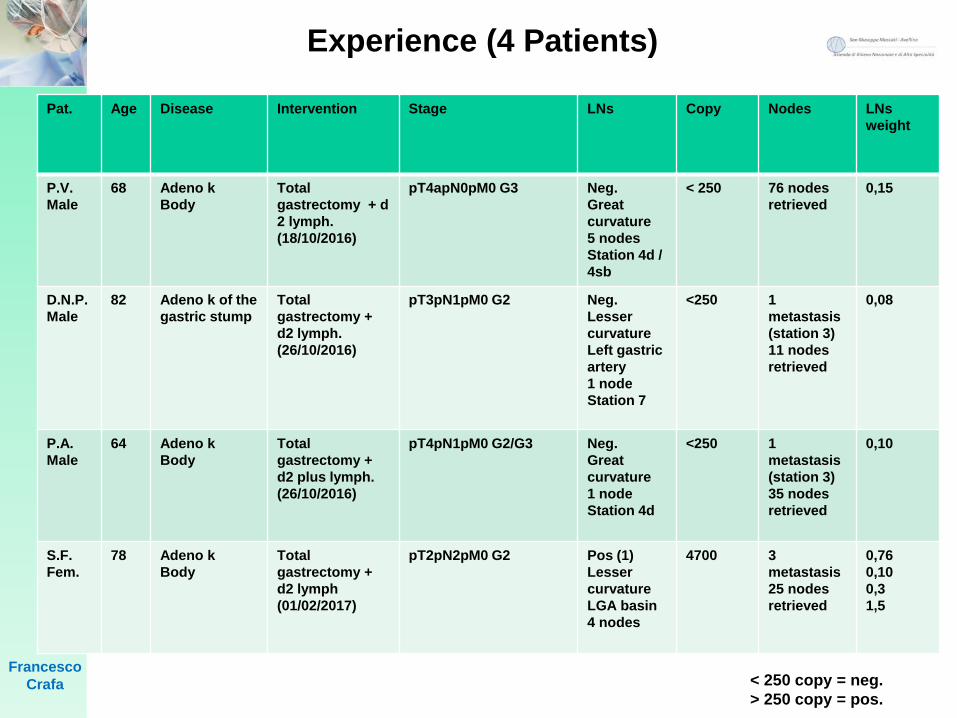
Pat. Age Disease Intervention Stage LNs Copy Nodes LNs
weight
P.V.
Male
68 Adeno k
Body
Total
gastrectomy + d
2 lymph.
(18/10/2016)
pT4apN0pM0 G3 Neg.
Great
curvature
5 nodes
Station 4d /
4sb
< 250 76 nodes
retrieved
0,15
D.N.P.
Male
82 Adeno k of the
gastric stump
Total
gastrectomy +
d2 lymph.
(26/10/2016)
pT3pN1pM0 G2 Neg.
Lesser
curvature
Left gastric
artery
1 node
Station 7
<250 1
metastasis
(station 3)
11 nodes
retrieved
0,08
P.A.
Male
64 Adeno k
Body
Total
gastrectomy +
d2 plus lymph.
(26/10/2016)
pT4pN1pM0 G2/G3 Neg.
Great
curvature
1 node
Station 4d
<250 1
metastasis
(station 3)
35 nodes
retrieved
0,10
S.F.
Fem.
78 Adeno k
Body
Total
gastrectomy +
d2 lymph
(01/02/2017)
pT2pN2pM0 G2 Pos (1)
Lesser
curvature
LGA basin
4 nodes
4700 3
metastasis
25 nodes
retrieved
0,76
0,10
0,3
1,5
< 250 copy = neg.
> 250 copy = pos.
Experience (4 Patients)
Francesco
Crafa
Improve staging by a focused ultrastaging
examination of the SLNs:
OSNA is similar to a 2 mm interval HE and
is using the whole LN.
Concordance rate between the two
methods for 394 LNs from 61 patients was
0.942
Specificity of the OSNA assay for
detecting LN metastases in 32 ‘‘node-
negative patients’’ was 0.991
Conclusions
Francesco
Crafa
We have to take into account histological
type of primary tumour, CK19 expression
of primary tumour, tissue allocation bias.
Usefull for organ sparing surgery, tailored
and successful lymphadenectomy and
aberrant and skip metastases.(Sentinel
nodes navigation surgery)
Conclusions