services & trusts integrating to improve care in self-harm · services & trusts integrating...
TRANSCRIPT

Services & Trusts Integrating To improve Care in self-Harm
STITCH Director: Salena Williams
Sal Ball
Robert Carroll


and ‘the HITs’: Health Integrated Teams

Background: Self-harm
• Approximately 200,000 hospital attendances in England annually; 3,000 in Bristol.
• 20-25% repeat self-harm in the next 12 months; 1% die by suicide.
• Past self-harm is the strongest predictor of suicide
• Approx. 1 in 5 Bristol suicides present with self-harm in the year before death

The Self Harm Surveillance Register
•Identify trends in self-harm since Oct 2010
•Identify Repeat attenders
•Methods of self-harm
•Seen for psychiatric review?
•Timely evaluation of new services
•Appropriate targeting of services (timing of attendance)
•Children’s hosptial
•Extended to Southmead in 2013 – contrast services
Self Harm Presentations to Bristol Hospitals

Aims of
Treatment and care is equitable, fully evidence based and non-stigmatising for all people who self harm and to reduce suicides in Bristol
• Improve service user engagement in service planning and delivery throughout the care pathway and with research
• Provide a psychosocial assessment following self harm
• Ensure closer inter-organisational and inter-agency working
• Reduce the ‘the science to service’ gap
• Improve self-harm training

What would you do?
If you lived in a city of 600,000 people and you are considering ending your life by suicide or you used self harm:
what would help you, and what would you change?
We have concentrated on 3 areas. Discuss on your tables
Please take 5 minutes

Emergency Departments (A+E)
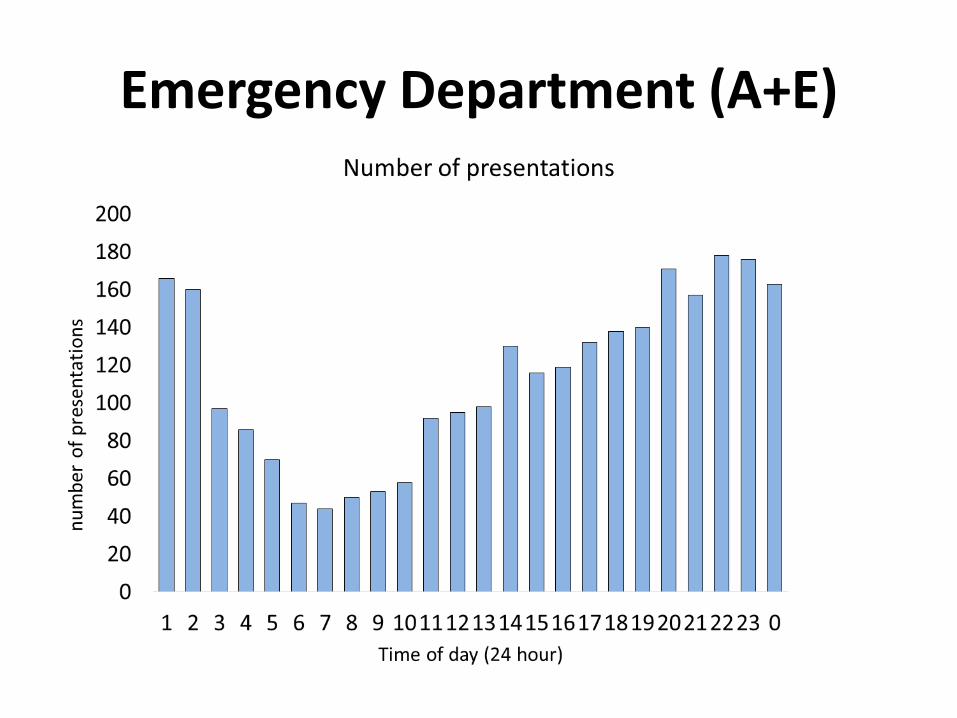
Emergency Department (A+E)
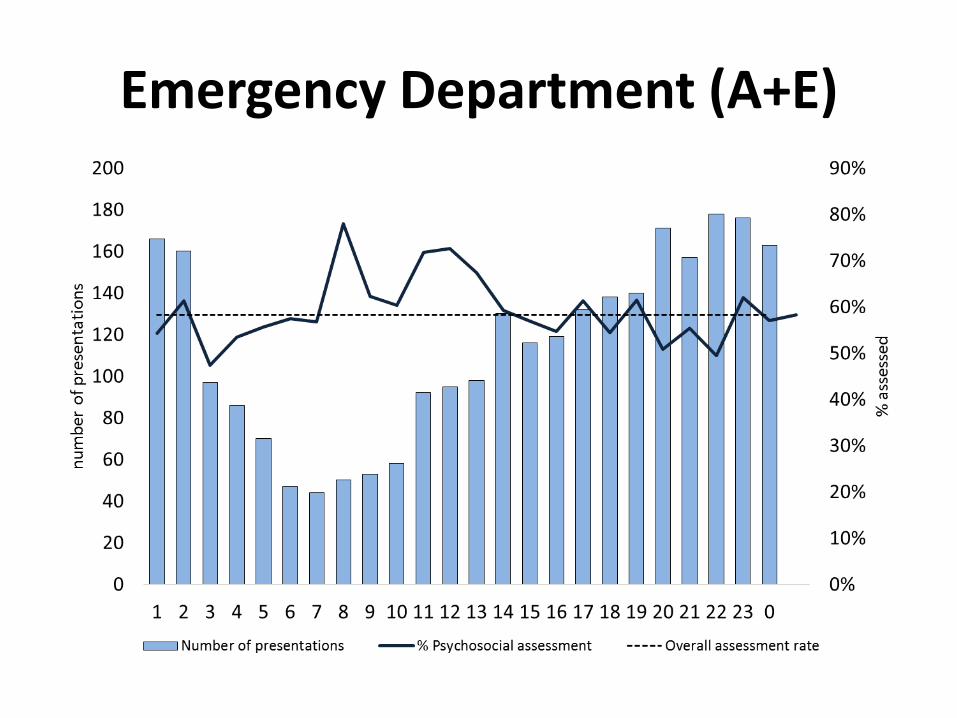
Emergency Department (A+E)

Bristol-based peer support group formed in 1998
Currently facilitates weekly support groups, Making Changes groups, Wellbeing workshops
Future Plans: increase number of support groups; talks/training by people with lived experience
Evaluation of A&E by People who Self Injure:
– SISH funded by Bristol public health to gather views
of people who self-injure who use A&E, evaluation of service and recommendations for improvements
– Working closely with the Psychiatric Liaison Team
Self Injury Self Help (SISH):

• Basic Underlying Principle: Experience-led from start to finish
• Used SISH database of contacts and other local and public networks
• Initially sought views on ‘what questions should be asked?’
• Online survey and face-to-face interviews based on these suggestions, questions deliberately left open ended to capture personal perspectives
• Data obtained from: 40 online surveys and 4 face-to- face interviews; time spent in A&E observing
Methodology

Process: Thinking about
Power Imbalance Impact of taking part:
• Need to be anonymous in case it affects treatment
• Impact of discussing very personal experiences for others to analyse
• Meeting staff who may have treated you to discuss improvements
• Meeting in health-related environments
• Being outnumbered by staff • Meeting staff who you know
have different views to you • Having to ask for
expenses/support to take part

Use of A&E Services
In the last 18 Months: • Bristol Royal Infirmary
48%
• Frenchay 30%
• Southmead 3%
• Other/None 13%

Majority - felt that they were given appropriate physical treatment
Majority - felt that the care and support they were given for emotional and psychological needs is not helpful and in some cases puts them off attending.
Overall feeling - inconsistency and not being sure what type of service would be on offer
Summary of Results

• User produced information leaflet
• Body Maps
• ‘It’s ok not to say’ signs
• Training for ED staff
• Better communication with GP/Mental health teams
• Improved access to Psychiatric Liaison Service, when wanted
• REPEAT evaluation survey to monitor effectiveness
Action taken as a result of survey

G.P.

General Practitioner: GP

General Practitioner: GP
• 5% of self-poisoning involve highly lethal tricyclic anti-depressants
• 11% of patients taking these medications in overdose are admitted to ITU.
• STITCH pilot through collaboration with GPs is ongoing looking at dispensing medicines lethal in overdose in small quantities.

GP prescriptions pilot
Stigma

Training/education
Over 150 GPs in Bristol:
- Avon GP Education
- CCG ½ days
- GP forums
South West Ambulance Service
Regular Medical and Nursing staff in both A+E’s
• All with people with lived experience of self harm
• All evaluated: knowledge, confidence, motivation

Psychological support

Psychological support
30%
40%
50%
60%
70%
80%
90%
2013
-Oct
2013
-Oct
2013
-Nov
2013
-Dec
2013
-Dec
2014
-Jan
2014
-Feb
2014
-Mar
2014
-Mar
2014
-Apr
2014
-May
2014
-May
2014
-Jun
2014
-Jul
2014
-Jul
2014
-Aug
2014
-Sep
2014
-Sep
2014
-Oct
2014
-Nov
2014
-Dec
2014
-Dec
2015
-Jan
2015
-Feb
2015
-Feb
2015
-Mar
2015
-Apr
2015
-Apr
2015
-May
2015
-Jun
2015
-Jun
2015
-Jul
2015
-Aug
2015
-Sep
2015
-Sep
% a
sses
sed
Time period
Proportion of self-harm patients receiving a specialist psychosocial assessment (3-week moving average) and pre/post average proportion
assessed (Oct-2013 to Sep-2014 vs. Oct-2014 to Sep-2015)
3-week moving average 12-month average

Psychological support
O’Connor 2013 Annals of Internal Medicine

Psychological support
• Growing body of evidence from trials suggesting cognitive behaviour therapy can reduce risk of repetition.
• STITCH has facilitated the introduction of clinics offering this therapy for SH patients.
• Register will be well placed to evaluate outcomes from this work

Psychological support
• Business case – investment – 7 day service to A+E
• Psychosocial assessments + 60%
• Standardised across Bristol
• Personal support plans
• Self harm clinic
• Self harm enhanced clinic

Other STITCH achievements
• SING: University counsellors, young peoples services, school educators, CAMHS workers
• Carers leaflet
• Research: internet, recession, risk assessment, paracetemol, DV and LGBT
• CLARHC – public and patient participation in research
• Later life equality care
