session #7 dohrmann.ppt - c.ymcdn.com · wpw mimicking inferior infarct (the inferior qs are delta...
TRANSCRIPT

4/17/2013
1
10 ECGs No Practitioner Can Afford to Miss
Mary L. Dohrmann, MDProfessor of Clinical Medicine
Division of Cardiovascular MedicineUniversity of Missouri School of Medicine
No disclosures
Objectives
1. Review basic principles
2. Have some fun with some ECGs
3. Go home with some motivation

4/17/2013
2
Resources
• Complete Guide to ECGs 3rd ed., 2009, ed. O’Keefe et al: 88 practice ECGs
• Great website for practice http://ecg.bidmc.harvard.edu/maven
Stages of ECG expertise
• Observation
• Observation + conclusion
• Above plus clinical context/application
(takes into account all available information)

4/17/2013
3
What is “Normal”?
‐ Not deviating from a norm, rule, or principle
‐ Conforming to a type, standard, or regular pattern
The “standard” ECG
– Patient position
– Proper lead locations
– Voltage standardization
– Paper speed
4/17/2013
4
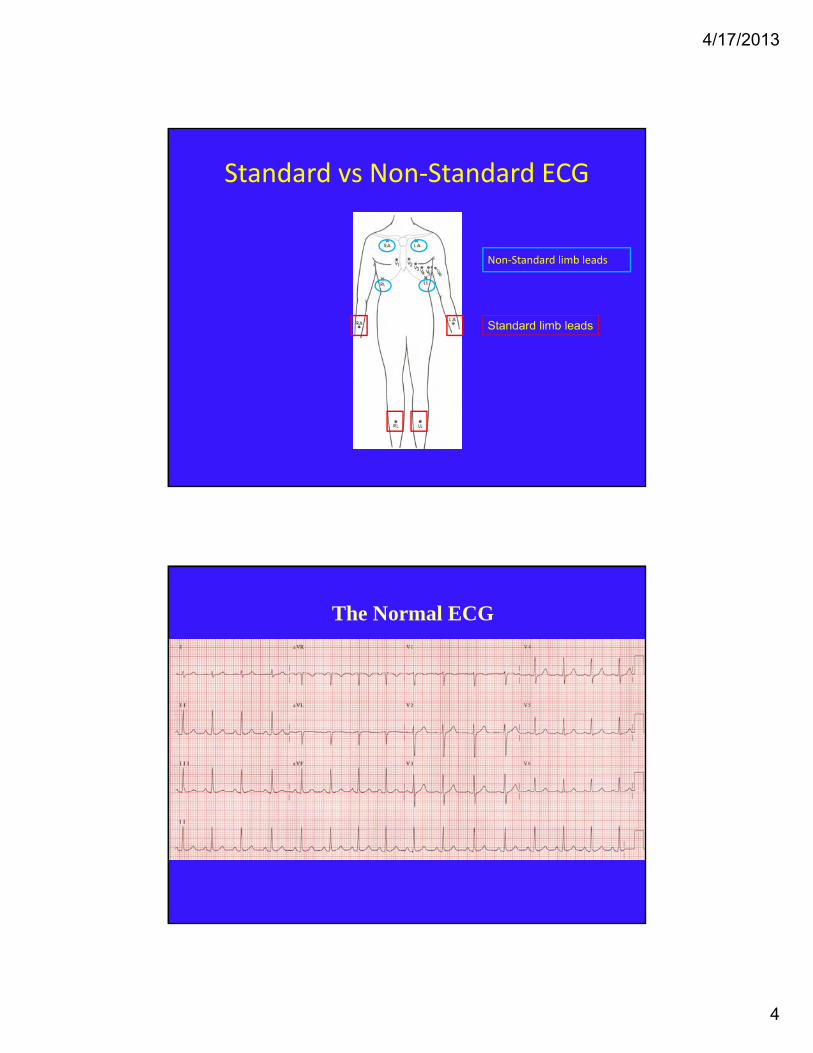
Standard vs Non‐Standard ECG
Standard limb leads
Non‐Standard limb leads
The Normal ECG

4/17/2013
5
The Normal ECG
Sinus rhythm (P before @ QRS)P wave axis (+ I,II,III, aVF)
Rate 50 – 100 bpm; paper speed 25 mm/secQRS Axis +90o (youth) to –30o (elderly)Intervals: PR .12‐.21 sec, QRS < .10 secQTc <.46 sec (observed QT/√RR interval)
QRS voltage (n/a < age 35)(use 10mV standard)Precordial R waves (transition V3‐V4)
ST segment (baseline or early repolarization pattern)T wave (concordant with frontal plane QRS vector)
Is this person older or younger than pt in prior ECG?
Normal ECG

4/17/2013
6
This ECG is in an older individual than prior normal ECG –why? axis is more leftward!
Normal ECG
Rhythm
Sinus Not sinus
VentricularSupravent.Morphology
4/17/2013
7
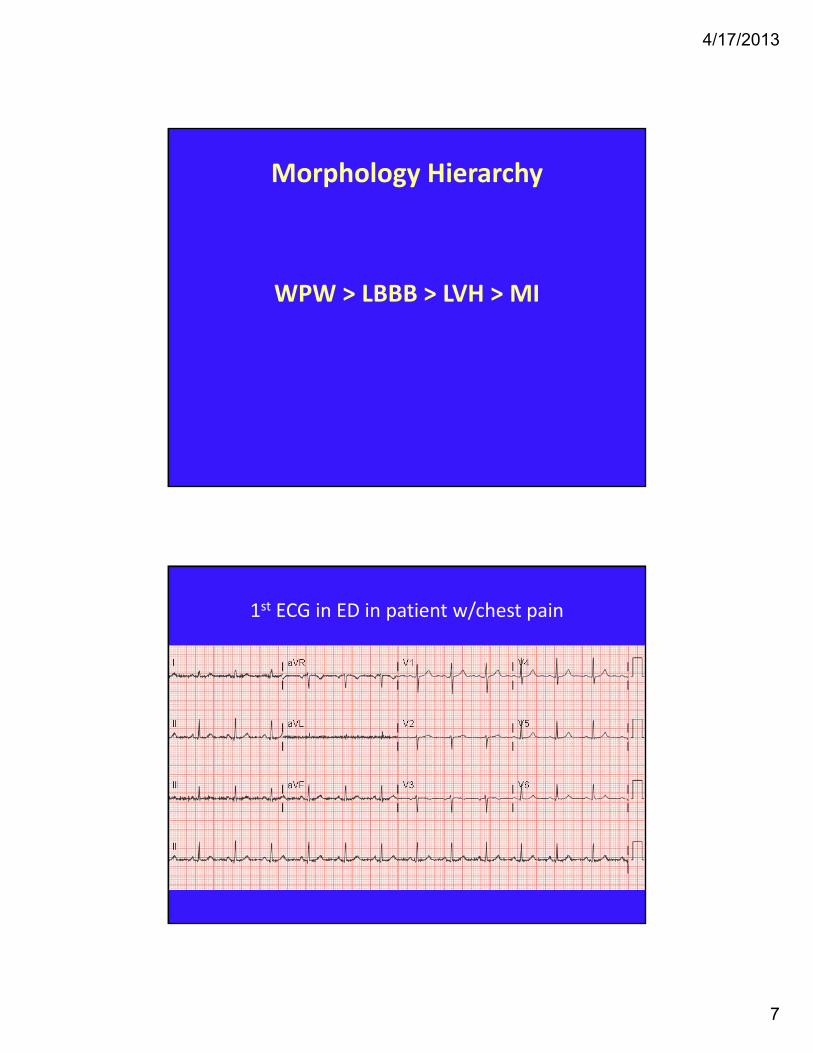
Morphology Hierarchy
WPW > LBBB > LVH > MI
1st ECG in ED in patient w/chest pain

4/17/2013
8
Next steps?
A. Get a VQ scan
B. Take the patient to the cath lab
C. Repeat the ECG
D. Get an echo
The R wave progression does not make sense! Negative P and T in V3 are clues that this V3 is really V1. Note: an isolated Q in III is NORMAL!
Repeat the ECG: Reversed V1 and V3 leads

4/17/2013
9
Prior ECG with V lead positions corrected now appears normal!
1st ECG in ED in patient w/chest pain

4/17/2013
10
Next steps?
A. Get a VQ scan
B. Take the patient to the cath lab
C. Repeat the ECG
D. Get a CXR
1st ECG in ED in patient w/chest painPatient with dextrocardia! A CXR would tell you this!
Dextrocardia – negative P wave in lead I; abnormal R wave progression with diminished voltage in V6

4/17/2013
11
Dextrocardia – ECG in same patient as previousCorrected leads for anatomy (purposely
reversed arm leads and used right‐sided V leads)
Reversed arm leadsnegative P in I, positive P in aVR

4/17/2013
12
Prior ECG with arm leads corrected
29 y/o with chest pain
4/17/2013
13
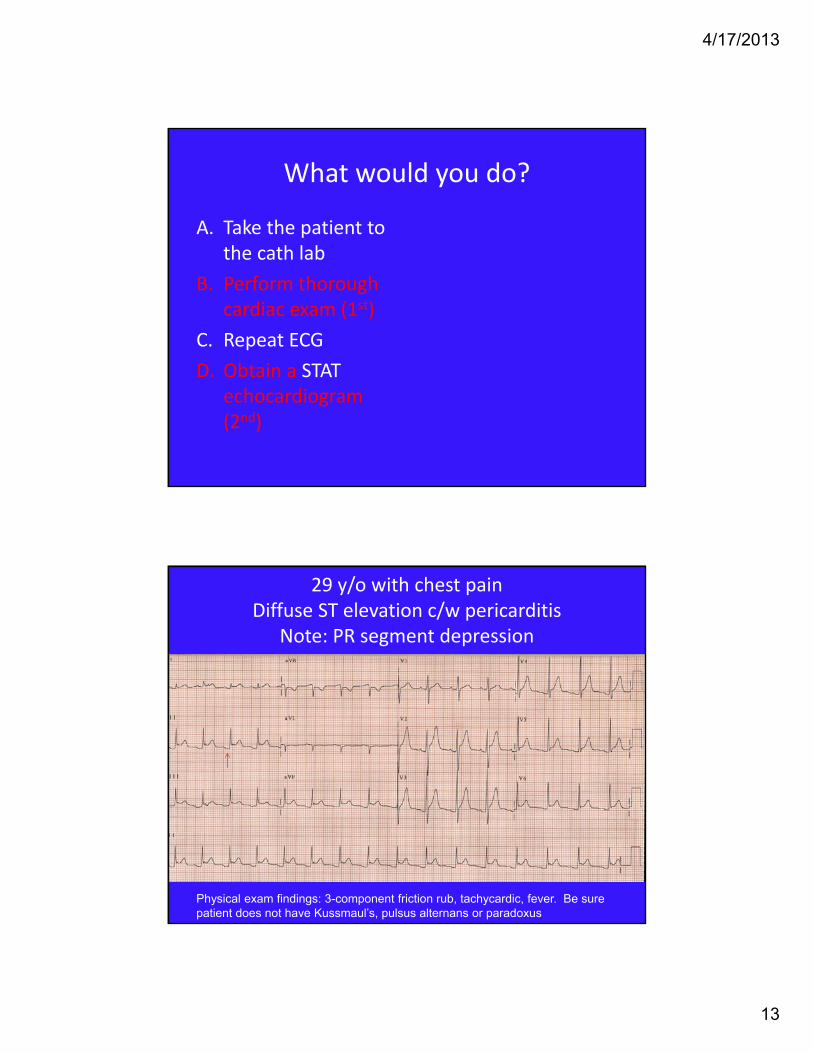
What would you do?
A. Take the patient to the cath lab
B. Perform thorough cardiac exam (1st)
C. Repeat ECG
D. Obtain a STAT echocardiogram (2nd)
29 y/o with chest pain Diffuse ST elevation c/w pericarditis
Note: PR segment depression
Physical exam findings: 3-component friction rub, tachycardic, fever. Be sure patient does not have Kussmaul’s, pulsus alternans or paradoxus

4/17/2013
14
47 y/o male with chest painAcute inferior MI
41 y/o male with severe SOBExtensive anterior/anterolateral MI

4/17/2013
15
54 y/o male with exertional chest pain
What test would you obtain?
A. Cardiac catheterization
B. Exercise stress test
C. Exercise stress test combined with imaging
D. Echocardiogram
In a patient with angina and prior infarct, proceeding directly to cardiac catheterization would be the optimal choice; however, you might also want to get an echocardiogram prior to cardiac cath to assess LV function.

4/17/2013
16
54 y/o male with exertional chest painAMI, indeterminate age; RBBB ± LAFB
Cath findings: 100% proximal LAD, 90% D1, 90% D2, 100% mid-RCA; LVEF 25%
40 y/o resuscitated from VF

4/17/2013
17
40 y/o resuscitated from VFBrugada syndrome
This patient received an AICD
Check out this website!
www.brugada.org

4/17/2013
18
34 year old with syncope
What’s next?
A. Admit for cardiac monitoring
B. Obtain electrolytes
C. Review current medications
D. All of the above

4/17/2013
19
34 year old with syncopeLong‐QT syndrome
Calculate the QTc using Basett’s formula: QTcorrected = QTobserved ÷ √RR
Torsades de pointes

4/17/2013
20
Drugs that can prolong QT
http://www.qtdrugs.org
Insulin‐dependent diabetic with nausea
4/17/2013
21
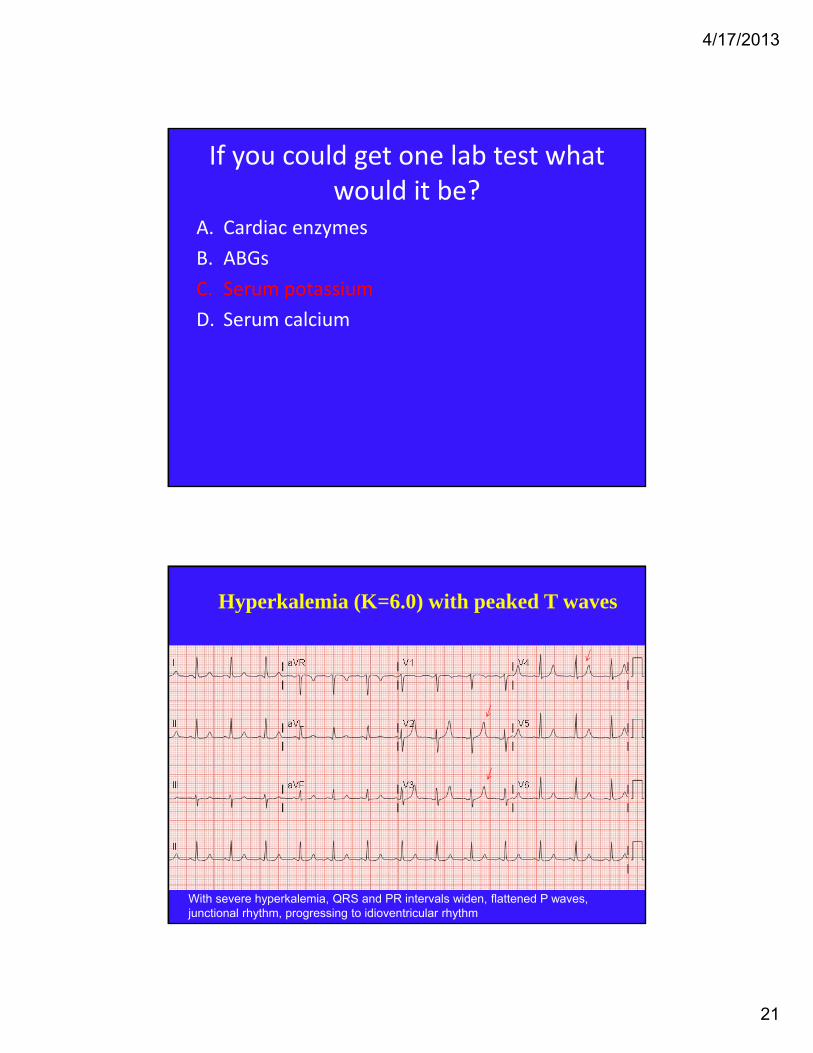
If you could get one lab test what would it be?
A. Cardiac enzymes
B. ABGs
C. Serum potassium
D. Serum calcium
Hyperkalemia (K=6.0) with peaked T waves
With severe hyperkalemia, QRS and PR intervals widen, flattened P waves, junctional rhythm, progressing to idioventricular rhythm

4/17/2013
22
Resolution of peaked T waves following treatment of hyperkalemia
40 y/o with chest pain & palpitations

4/17/2013
23
The most likely diagnosis is:
A. Right bundle branch block
B. Acute inferior infarct
C. Left bundle branch block
D. Ventricular preexcitation (WPW)
40 y/o with chest pain & palpitationsshort PR/delta wave c/w preexcitation

4/17/2013
24
WPW mimicking anterior infarct
WPW mimicking inferior infarct (The inferior Qs are delta waves!)
4/17/2013
25
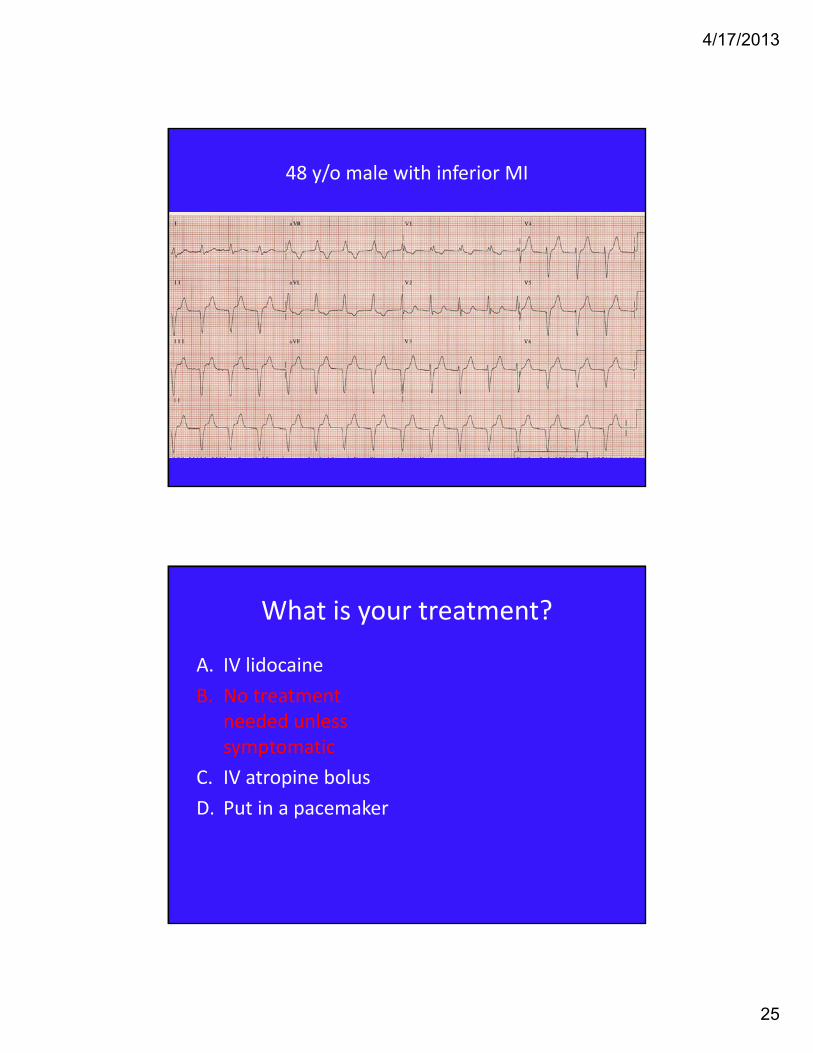
48 y/o male with inferior MI
What is your treatment?
A. IV lidocaine
B. No treatment needed unless symptomatic
C. IV atropine bolus
D. Put in a pacemaker

4/17/2013
26
Accelerated idioventricular rhythm in context of inferior infarct
May represent reperfusion arrhythmia; may be provoked by increased vagal tone and is as an escape rhythm; well tolerated clinically
80 y/o man with syncope

4/17/2013
27
Right bundle branch block & LAD, 2:1 block and/or complete heart block, with ventricular escape
complexes
This patient needs a pacemaker!
More fun ECGs to review at home!

4/17/2013
28
2nd degree AV block, Type I (Wenckebach)
(Note the gradually increasing PR interval and subsequent non‐conducted P resulting in a greater than 2 second pause)
Atrial flutter 2:1 conduction
4/17/2013
29
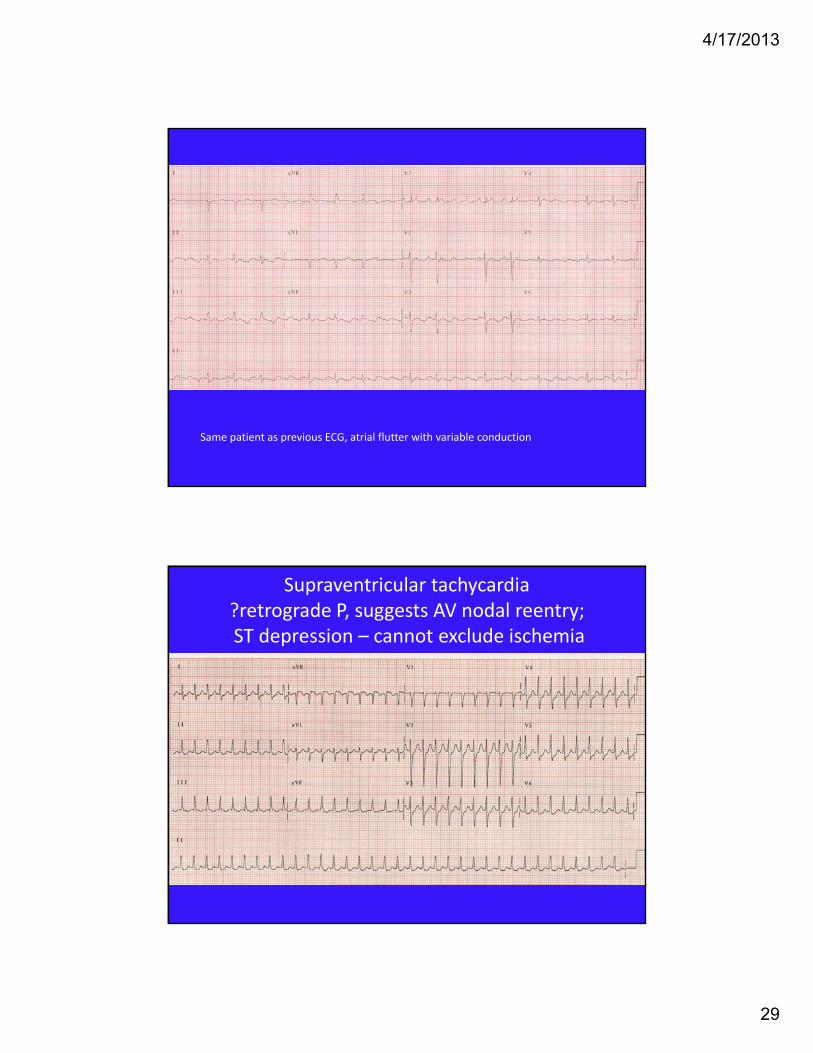
Same patient as previous ECG, atrial flutter with variable conduction
Supraventricular tachycardia ?retrograde P, suggests AV nodal reentry;ST depression – cannot exclude ischemia

4/17/2013
30
Junctional tachycardia with retrograde P waves
Wide complex tachycardia = VT !

4/17/2013
31
Multifocal atrial tachycardia(Note multiple P wave morphologies)
51 y/o male with chest painST elevation I, aVL, V2 c/w acute injury/infarct
(Note: reciprocal depression in II, III, aVF)
Patient had 100% occlusion of diagonal branch from the LAD

4/17/2013
32
70 y/o with exertional chest painECG shows LBBB ‐ cannot interpret for
ischemia or infarct!
LBBB causes false positive exercise imaging! The stress test of choice would be an adenosine sestamibi.
Right bundle branch block, left anterior fasicular block, and first degree AV block
