severe thrombocytopenia in iron deficiency anemia
TRANSCRIPT

American Journal of Hematology 24:425-428 (1987)
Severe Thrombocytopenia in Iron Deficiency Anemia Mark Berger and Lawrence F. Brass
Hematology-Oncology Section, Department of Medicine and the Coagulation and Thrombosis Laboratory, Department of Pathology and Laboratory Medicine, University of Pennsylvania, Philadelphia
Mild-to-moderate thrombocytopenia has been reported as an occasional finding in patients with iron deficiency. The present case describes a multiparous woman who presented with increased menorrhagia, severe anemia (3 .O g/dl) and thrombocyto- penia (9,000 platelets/mm3). Her bone marrow examination showed iron deficiency, megakaryocytopenia, and erythroid hypoplasia but no other evidence of a primary marrow disorder. Her symptoms, the thrombocytopenia and the megakaryocytopenia, resolved with iron replacement. This case demonstrates the profound degree to which thrombopoiesis can be affected in iron deficiency.
Key words: iron deficiency, thrombocytopenia, megakaryocytopenia, thrombopoiesis
INTRODUCTION
Thrombocytopenia has been reported as a rare complication of iron deficiency anemia in both children [1,2] and adults [3-71. In general in the cases that were described, the degree of thrombocytopenia was mild to moderate (ie > 40,000 platelets mm3) and did not appear to be the cause of clinically significant bleeding. We now describe a patient with severe iron deficiency anemia that was apparently due to a combination of chronic and acute menstrual blood loss, multiple pregnancies, and poor iron intake who developed severe thrombocytopenia (9,000/mm3) and mega- karyocytopenia that resolved completely with iron replacement. No other causes of thrombocytopenia were identified. The appearance of her bone marrow at the time of presentation and after resolution of the thrombocytopenia are described.
CASE DESCRIPTION
The patient is a 30-year-old black woman who was seen with complaints of pedal edema and increasing menorrhagia without other blood loss. Her past medical history was significant for three term pregnancies with the last child being born 3 years prior to admission. At that time her hemoglobin was 14.5 g/dl. Her only medication at the time of admission was an occasional “once a day” vitamin said to contain iron. Physical examination showed a pale young woman who was afebrile
Received for publication August 22, 1986; accepted October 2, 1986. L.F.B. is an Established Investigator of the American Heart Association. Address reprint requests to Dr. Brass at the Hematology Section, Silverstein 7, Hospital of the University of Pennsylvania, 3400 Spruce St, Philadelphia, PA 19104.
0 1987 Alan R. Liss, Inc.
426 Brief Report: Berger and Brass
and had a blood pressure of 130/75, heart rate of 100, and respirations of 2O/minute. Her skin had a waxy yellow color. No petechiae or ecchymoses were seen. Her fingernail beds were pale. There was no adenopathy. Her lungs were clear. Cardiac exam revealed a systolic flow murmur. There was no hepatosplenomegaly, and her stool tested negative for occult blood. Pelvic exam showed no masses or tenderness, but vaginal bleeding was present. There was pitting edema to midcalf bilaterally.
Laboratory data included a hemoglobin of 3.0 g/dl, an MCV of 49 fl, and an MCH of 16 pg. The platelet count was 33,000/mm3, and total leukocyte count was 3,100/mm3 (64% polys, 2% bands, 25% lymphocytes, 6% monos, 1% atypical lymphocytes, 1 % eosinophils, and 1 % basophils). Examination of the peripheral blood smears showed microcytic, hypochromic red blood cells with teardrop forms and a few schistocytes. No nucleated red blood cells were seen. The platelets were normal in appearance, but markedly decreased in number. The reticulocyte count was 2.7%. The total bilirubin was 0.6 mg/dl. Serum B12 was 802 ng/ml (normal 200- 1,550 ng/ml). Serum folate was 5.5 pg/liter (normal >2.4 pglliter). Serum lactate dehydrogenase was 213 U/liter (normal < 250 units/liter). The leukocyte alkaline phosphatase 22 was slightly decreased. Serum ferritin was markedly decreased ( < 4 ng/ml). A sugar water test was negative. The prothrombin time and activate partial thromboplastin time were within normal limits. Fibrin split products were < 5 ng/ml, and the fibrinogen was 201 mg/dl. Rheumatoid factor and antinuclear antibody tests were negative, as was a stool examination for ova and parasites. A chest X-ray showed that the heart size was at the upper limits of normal. An abdominal CT scan showed a somewhat “prominent spleen” but no adenopathy . A posterior iliac crest bone marrow aspirate and biopsy were notable for a hypercellular marrow with granulocytic hyperplasia, an increased mye1oid:erythroid ratio and decreased numbers of megakaryocytes and erythroid precoursors. Myeloid and megakaryocyte morphol- ogy were normal. There was no stainable iron. There was no evidence of tumor.
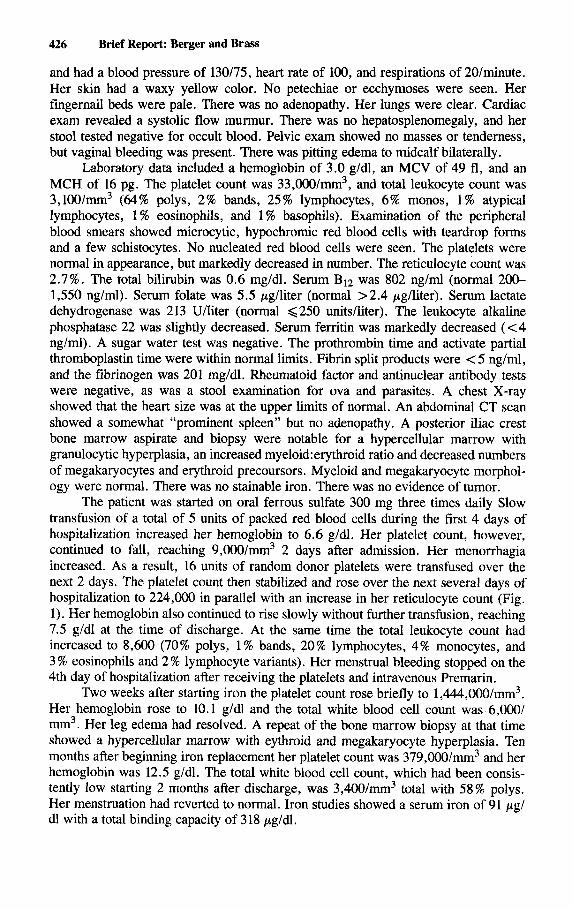
The patient was started on oral ferrous sulfate 300 mg three times daily Slow transfusion of a total of 5 units of packed red blood cells during the first 4 days of hospitalization increased her hemoglobin to 6.6 g/dl. Her platelet count, however, continued to fall, reaching 9,000/mm3 2 days after admission. Her menorrhagia increased. As a result, 16 units of random donor platelets were transfused over the next 2 days. The platelet count then stabilized and rose over the next several days of hospitalization to 224,000 in parallel with an increase in her reticulocyte count (Fig. 1). Her hemoglobin also continued to rise slowly without further transfusion, reaching 7.5 g/dl at the time of discharge. At the same time the total leukocyte count had increased to 8,600 (70% polys, 1% bands, 20% lymphocytes, 4% monocytes, and 3 % eosinophils and 2 % lymphocyte variants). Her menstrual bleeding stopped on the 4th day of hospitalization after receiving the platelets and intravenous Premarin.
Two weeks after starting iron the platelet count rose briefly to l , ~ , 0 0 0 / m m 3 , Her hemoglobin rose to 10.1 g/dl and the total white blood cell count was 6,000/ mm3. Her leg edema had resolved. A repeat of the bone marrow biopsy at that time showed a hypercellular marrow with eythroid and megakaryocyte hyperplasia. Ten months after beginning iron replacement her platelet count was 379,000/mm3 and her hemoglobin was 12.5 g/dl. The total white blood cell count, which had been consis- tently low starting 2 months after discharge, was 3,400/mm3 total with 58% polys. Her menstruation had reverted to normal. Iron studies showed a serum iron of 91 pg/ dl with a total binding capacity of 318 pgldl.

Brief Report: Thrombocytopenia 427
14 - Tx Tx Tx
6 .- I
-.
-.
1600
-. 1400
-. 1200 B
-800 5 % -. 1000 . 0
3 -. 600 400
200
0
9
- 0 1 2 3 4 5 6 7 8 9 12 18 31 52 108 124171 297
DAYS AFTER ADMISSION
Fig. 1. This figure displays the results of serial determinations of this patient’s Hb (bars) and platelet count (+) starting with the day of admission. The arrows indicate the dates on which red blood cells were transfused (see text). The numbers above some of the bars are the uncorrected reticulocyte count.
COMMENTS
Both thrombocytosis and thrombocytopenia have been reported in patients with iron deficiency anemia. Although it has been suggested that these apparently contra- dictory observations can be resolved if iron plays both a synthetic and a regulatory role in thrombopoiesis, the mechanisms involved are not well understood [8]. The patient described in the present report is noteworthy because she had thrombocyto- penia to a degree not previously reported with iron deficiency anemia, and her thrombocytopenia appeared to be contributing to her vaginal bleeding. Despite its severity, there was no evidence of any cause for her thrombocytopenia other than iron deficiency, and her thrombocytopenia resolved completely with iron replacement. Previous descriptions of bone marrow samples from patients with thrombocytopenia and iron deficiency have shown either normal or decreased numbers of megakaryo- cytes. In some cases the megakaryocytes appeared to have aberrant morphology [2]. The initial bone marrow examination in the present case showed a marked reduction in the number of megakaryocytes, an observation that is consistent with the postulated role of iron in thrombopoiesis. The scattered megakaryocytes that were present were normal in appearance. The megakaryocytopenia, like the thrombocytopenia, had resolved by the time of a repeat bone marrow examination performed 18 days after the start of oral iron replacement.
Leukopenia and neutropenia was also noted in this patient on presentation. Mild leukopenia has been reported in patients with iron deficiency [2,4]. Although in the present case both of these values improved within 2 days of starting iron replacement, they have subsequently stabilized at levels similar to those present on admission. In the absence of any other evidence of systemic illness or bone marrow abnormality, this appears to reflect the normal function of this patient’s bone marrow and not to be directly related to iron deficiency.
REFERENCES
1. Gross S, Keefer V, Newman A.T: The platelet in iron deficiency anemia. I. The response to oral and parented iron. Pediatrics 34:315-323, 1964.

428
2. Lopas H, Rabiner SF: Thrombocytopenia associated with iron deficiency anemia. Clin Pediatr (Phila)
3. Sonneborn D: Thrombocytopenia and iron deficiency. Ann Intern Med 80:111, 1974. 4. Sahud MA, Olsen H, Pedemont L: Thrombocytopenia and iron deficiency. Ann Intern Med 81:132-
5. Scher H, Silber R: Iron responsive thrombocytopenia. Ann Intern Med 84:571-572, 1976. 6. Beard MEJ, Johnson SAN: Thrombocytopenia and iron deficiency anemia in a patient with alphal-
7. Dincol K, Aksoy M: On the platelet levels in chronic iron deficiency anemia. Acta Haematol (Basel)
8. Karpatkin S , Garg SK, Freedman ML: Role of iron as a regulator of thrombopoiesis. Am J Med
Brief Report: Berger and Brass
5:609-616, 1966.
133, 1974.
thalassemia trait. Response to iron therapy. Acta Haematol (Basel) 59: 114-118, 1978.
41: 135-143, 1969.
57: 52 1-525, 1974.