sexual dysfunctions chapter 15. learning objectives types of sexual dysfunctions origins of sexual...
TRANSCRIPT

Sexual Dysfunctions
Chapter 15
Learning ObjectivesTypes of Sexual Dysfunctions
Origins of Sexual Dysfunctions
Treatment of Sexual Dysfunctions
Types of Sexual Dysfunctions
Sexual Dysfunction
s
• Persistent or recurrent difficulties in becoming sexually aroused or reaching orgasm
People with dysfunctions
• Often avoid sexual opportunities • Feel inadequate or incompetent• Find it difficult to talk about
Types of Sexual Dysfunctions
No precise figures on
occurrence of sexual
dysfunctions
• Surveys indicate• Women report higher prevalence• Prevalence increases with age• Most prevalent for women are
low sexual desire and difficulty reaching orgasm
• Least prevalent are pain disorders
• Many men report low sexual desire
Types of Sexual Dysfunctions
Sexual desire disorders
• Lack of interest in sex or aversion to sexual contact
Sexual arousal
disorders• Failure to
become adequately sexually aroused to engage in or sustain sexual intercourse
Orgasmic disorders
• Difficulty reaching orgasm or reaching orgasms more rapidly than one would like
Sexual pain disorders
• Persistent or recurrent experience of pain during coitus
DSM proposes four categories
Types of Sexual Dysfunctions
• Lifelong• Acquired
Sexual dysfunctions can be
• Generalized• Occur in all situation
• Situational • Occur only in some situations
Sexual dysfunctions classified as
Critical Thinking
When does a sexual problem
become a sexual dysfunction?
How can concern about a sexual problem develop into a dysfunction?
Sexual Desire DisordersHypoactive sexual desire disorder
Little or no sexual interest or desire
Absence of sexual fantasies
Most commonly diagnosed sexual dysfunction
Does not indicate physical inability
More common in women than men
Cause unclear
Sexual Arousal DisordersMale erectile disorder or erectile dysfunction
Persistent difficulty achieving or maintaining an erection sufficient to complete sexual activity
Can be situational or generalized
May occur due to performance anxiety
Anxiety concerning one’s ability to perform behaviors, especially behaviors that may be evaluated by other people
May have physical causes
Sexual Arousal DisordersFemale sexual arousal disorder
Persistent difficulties becoming sufficiently lubricated in response to sexual stimulation
Can be lifelong or situational
May have physical causes
Usually has psychological causes, such as anger, resentment, or trauma
Orgasmic DisordersFemale orgasmic disorder
Anorgasmic Never having reached orgasm
Women who try to force an orgasm may assume a spectator role
A role in which people observe rather than fully participate in their sexual encounters
Orgasmic DisordersMale orgasmic disorder
This is also termed delayed ejaculation, retarded ejaculation, or ejaculatory incompetence
Orgasmic DisordersPremature ejaculation
Ejaculation occurs with minimal sexual stimulation and before the man desires it
Hard to define what is meant by premature
Rapid female orgasm
Can women reach orgasm too quickly?
It is not classified as a sexual dysfunction
May result in sexual relationship issues
Orgasmic disorders can have physical or psychological causes
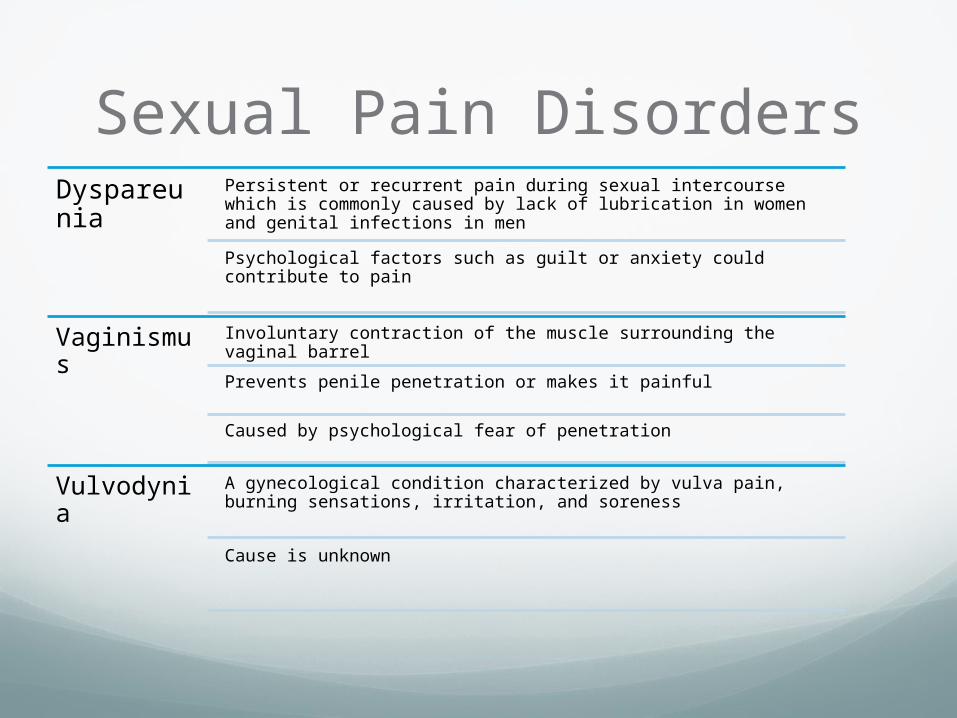
Sexual Pain DisordersDyspareunia
Persistent or recurrent pain during sexual intercourse which is commonly caused by lack of lubrication in women and genital infections in men
Psychological factors such as guilt or anxiety could contribute to pain
Vaginismus Involuntary contraction of the muscle surrounding the vaginal barrel
Prevents penile penetration or makes it painful
Caused by psychological fear of penetration
Vulvodynia A gynecological condition characterized by vulva pain, burning sensations, irritation, and soreness
Cause is unknown
Origins of Sexual Dysfunctions
Biopsychosocial model
• Considering interaction of biological, psychological, and social factors in sexual dysfunctions
Origins of Sexual Dysfunctions
Biological Causes
Testosterone deficiency• Hypogonadism• Reductions with age
Fatigue
Medical conditions• Heart disease,
diabetes, MS, spinal cord injuries, surgical complications, hormonal problems
Origins of Sexual Dysfunctions
Biological Causes
HIV• Therapy changes hormone
levels
Medications• Hypertension• SSRI’s • Treat depression, panic
disorder, OCD, anorexia• Impair sexual arousal
Substance use• Marijuana, cocaine, alcohol,
heroin, etc.
Origins of Sexual Dysfunctions
Psychosocial causes
Cultural influences• More common in sexually repressive cultures
• Sexual double standard• Negative sexual attitudes
Psychosexual trauma• Sexual victimization can negatively affect sexual arousal
Origins of Sexual Dysfunctions
Psychosocial causes
Sexual orientation• Sexual dysfunctions within a heterosexual relationship can reflect a lack of heteroerotic interests
Ineffective sexual techniques• Include failure to diversify, brevity, and lack of communication
Emotional factors• Include fear of losing control, depression, and stress
Origins of Sexual Dysfunctions
Psychosocial causes
Problems in the relationship• Communication problems• Resentment
Lack of sexual skills
Irrational beliefs• When one instance of erectile
or orgasmic disorder leads to false, catastrophic beliefs
Performance anxiety• Can create a vicious cycle of
failure and increased anxiety
Treatment of Sexual Dysfunctions
• A collective term for short-term behavioral models for treatment of sexual dysfunctions, which aim to• Change self-defeating beliefs and
attitudes• Enhance sexual knowledge• Teach sexual skills• Improve sexual communication• Reduce performance anxiety
Sex Therapy
Biological treatments
Treatment of Sexual Dysfunctions
• Psychosexual therapy• Combines behavioral
and psychoanalytic methods
• Improve sexual communication
• Eliminate performance anxiety
• Increase sexual skills and knowledge
The Helen Singer Kaplan
Approach
Treatment of Sexual Dysfunctions
Sexual Desire
Disorders
• Treatments include• Self-stimulation exercises
combined with erotic fantasies
• Sensate focus exercises• Enhancing communication• Expanding repertoire of
couple’s sexual skills• Testosterone replacement
therapy• Use of anti-anxiety
medications• Couples therapy
Treatment of Sexual Dysfunctions
Male Sexual Arousal Disorders
• Erectile disorder• Sensate focus exercises
are used to reduce performance anxiety
• Biological approaches to treatment of erectile disorder • Surgery (i.e., vascular
surgery or penile implants)
• Medication (e.g., Viagra)• Vacuum pumps
Treatment of Sexual Dysfunctions
Female Sexual
Arousal Disorder
• Sex education• Cognitive therapy• Create non-demanding
situations• Work on relationship
problems• Use of artificial lubricants• Biological treatments • Vacuum pump used on the
clitoris• Medications also are being
investigated - controversial
Treatment of Sexual Dysfunctions
Female Orgasmic Disorders
• Sensate focus exercises to reduce performance anxiety
• Use of the female-superior position
• Individual therapy (typically for women) involves directed masturbation programs which include• Education• Self-exploration and self-
massage• Giving oneself permission• Use of fantasy• Use of a vibrator• Involvement of the partner
Treatment of Sexual Dysfunctions
Male Orgasmic Disorder
• Increase sexual stimulation• Decrease performance
anxiety
Treatment of Sexual Dysfunctions
Premature ejaculatio
n
• Partner uses the squeeze technique• Tip of the penis is squeezed
temporarily to prevent ejaculation
• An alternative method is the “stop-start” method
• Biological approaches to treatment of premature ejaculation include the use of psychiatric medications
Treatment of Sexual Dysfunctions
Sexual Pain
Disorders
• Dyspareunia• Treatment includes medical
procedures to treat infections
• Vaginismus• Treatment involves the
insertion of vaginal dilators of increasing size to help relax the vaginal musculature • Woman controls the pace
and depth of penetration• Psychological therapy also
may be needed
Critical Thinking
Are there any sex therapy methods
that seem
“over the top” to you?
Explain.