shega reducing hosp with hospice - namcp hospice.pdf• appreciate differences in services provided...
TRANSCRIPT

4/25/2016
1
The Role of Hospice in Reducing Hospital Readmissions
Joseph W. Shega, MDRegional Medical Director
Objectives
• Discuss the role of hospice in preventing hospital readmissions and ensuring value‐based care
• Appreciate differences in services provided by palliative care, home health, and hospice
• Identify characteristics of hospice providers best positioned to prevent hospital readmissions
1

4/25/2016
2
Death in America
US Overall
• 2.6 million deaths in 2013
• ~1.6 million deaths in hospice in 2013
• Causes of death– Heart disease
– Cancer
– Chronic lower respiratory diseases
– Accidents
– Stroke
– Alzheimer's disease
Hospice—2014
• Median LOS 17.4 days – 35.5% LOS < 1 week
– 10.3% LOS >6 months
• Causes of death– Cancer
– Debility unspecified
– Dementia
– Heart disease
– Lung disease
– Other
– Stroke or coma
CDC 2013, NHPCO 20142
Hospice Care• Part A Medicare Benefit
• Interdisciplinary team‐oriented approach to end‐of‐life (EOL) care
• Patient, family center of care
• Goals of care/shared decision‐making
• Aggressive care at the EOL: medical care, pain and symptom management, and emotional and spiritual support
• Provided in any setting
3

4/25/2016
3
Medicare Hospice BenefitBasic Hospice Benefit• Prognosis of 6 months or less if the terminal illness runs its
normal course
• Patients elect hospice via informed consent
• Hospice reimbursed at flat per‐diem based on one of 4 levels of care:
1. Routine home care• Includes patients living in LTC or ALF
2. Continuous home care
3. General inpatient care
4. Respite inpatient care
4
Hospice and Palliative Care
5

4/25/2016
4
• Improved satisfaction with care
• Improved pain and symptom management
• More likely to die in location of choice
• Decreased hospital readmissions
• Decreased condition-specific 30-day hospital-specific mortality
• Decreased healthcare cost
• Live longer
• Family support
• Bereavement services
Conner et al JPSM 2007
Kelly, A et al. Health Affairs 2013
Benefits of Palliative and Hospice Care
6
Outcome Hospice Nursing Home
Home Health
Hospital
Not enough help with pain, %
18.3 31.8 42.6 19.3
Not enough emotional support, %
34.6 56.2 70 51.7
Not always treated with respect, %
3.8 31.8 15.5 20.4
Not enough information about dying, %
29.2 44.3 31.5 50
Quality care excellent, % 70.7 41.6 46.5 46.8
Teno et al. Family Perspectives on End of Life Care. JAMA 2004
Patient Experience
7

4/25/2016
5
Hospital Readmissions and Hospice
8
Hospice Use Decreases Hospital Utilization
Kelly, A. Hospice enrollment saves money and improves quality. Health Affairs 2013
9

4/25/2016
6
2015 Condition‐Specific Hospital 30‐day Mortality
10
11
Hospice and Medicare Cost Savings

4/25/2016
7
Hospice and Life Expectancy
• Hospice patients live on average ~29 days longer
• Prolonged survival
– Lung cancer
– Pancreatic cancer
– Colon cancer
– CHF
• No survival difference
– Prostate cancer
– Breast cancer
Connor S., Comparing Hospice and Nonhospice Patient Survival Among Patients Who Die Within a Three‐Year Window. JPSM 2007 12
Cancer: A Case‐Based Example
13

4/25/2016
8
Case of RC
RC is a 59 y/o male with rectal cancer admitted to hospital with shortness of breath, nausea, vomiting, pain and increased ostomy output five days after receiving third line of chemotherapy. He spends about 50% of his time in a chair or bed.
• Antibiotics for pneumonia• IVF for dehydration• Anti-emetics for nausea and vomiting• Analgesics for pain management
14
Allen L A et al. Circulation 2012;125:1928-1952
• Treat pneumonia
• More chemotherapy
• Full code
• Symptom control
• PT to improve strength
15
Elements Important to Goals‐of‐Care Conversations, Shared Decision‐Making

4/25/2016
9
Communicating News about Serious Illness Is Difficult Because . . .
• Unable to deal with intensity of response
• Fearful of reaction
• Don’t want to take hope away from patient
• Illness as an indication of failure
• The task is unpleasant
• Lack of training
• Stress
• Feelings of inadequacy
• Requests by family to withhold information
• Takes time
• Personal fear
16
Chemotherapy Bias
Weeks JC NEJM 201217

4/25/2016
10
18
Physician Prognosis Estimates
Communication of Prognosis
Lamont et al. Ann Intern Med 2001;134:1096-110519

4/25/2016
11
Concurrent Appropriateness of Hospice and Anti‐Tumor Therapy
• Competing priorities of anti‐tumor therapy versus hospice
– Chemotherapy requires a good performance status
– Phase‐1 chemotherapy typically needs an estimated survival of 3 months
– Hospice enrollment possible at 6 months or less
• Must agree to forgo “curative” treatment and focus on quality of life
• Accurate prediction of prognosis important for good clinical decision‐making
20
Case of RC (Cont.)• Pneumonia and shortness of breath slowly improve with
antibiotics
• Nausea and vomiting resolve with IVF
• IV hydromorphone for pain control
• Ostomy output decreases
• Physical therapy consult
– Participation but unclear prospects for improvement
– Appointment in oncology 4 weeks
• Transferred to skilled rehabilitation
21

4/25/2016
12
Case of RC (cont.)• Week 1
– Completes antibiotics for pneumonia
– Participation in physical therapy
• Improvement in strength but not endurance
– Pain in rectal area develops and worsens—po hydromorphone
• Week 2
– Fever developed
– Increased fatigue
– Purulent drainage from rectum
• Transfer to acute-care hospital, admitted to the ICU
22
Hospital Readmissions
30‐DayReadmission
Skilled Care 22.6%
Home Health 21.4%
Home 18.0%
23

4/25/2016
13
Krueger K et al. Nursing Research and Proactive 2011
Reason for Hospital Admission from Nursing Home
24
Case of RC (Cont.)
• CT scan demonstrated progression of lung and liver metastasis plus rectal abscess
– Rectal drain and antibiotics initiated
– IVF for sepsis
• Patient has 10/10 rectal pain with hyperalgesia
– Parenteral hydromorphone
25

4/25/2016
14
Allen L A et al. Circulation 2012;125:1928-1952
• Treat rectal abscess
• More chemotherapy
• Full code
• Pain control
• PT to improve strength
26
Elements Important to Goals‐of‐Care Conversations, Shared Decision‐Making
Case of RC (Cont.)
• Oncologist and patient talk with hospitalist about additional chemotherapy
– Needs to be stronger
– Resolution of rectal abscess
• Agrees to return to skilled facility
– IV antibiotics for four weeks
– Physical therapy
– Outpatient oncology appointment 4 weeks
27

4/25/2016
15
Case of RC (Cont.)
• Week 1
– Participates in PT and gains some strength but not endurance
– Continues IV antibiotics with some improvement in abscess and pain
• Week 2
– PT recommends discharge with home health, as not making any more progress
– Also needs 2 more weeks of IV antibiotics
28
Only 1.5% enrolled in hospice at discharge
SNF Use by Older Adults in Last 6 Months of Life
29
4/25/2016
16
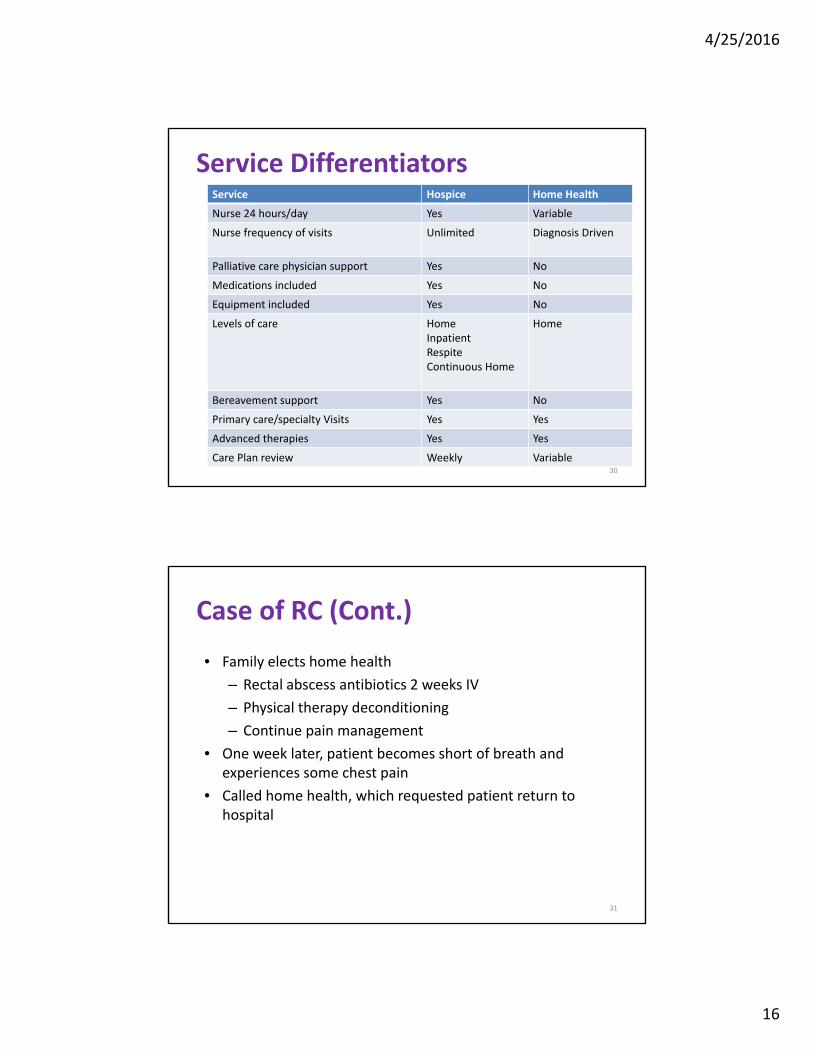
Service Hospice Home Health
Nurse 24 hours/day Yes Variable
Nurse frequency of visits Unlimited Diagnosis Driven
Palliative care physician support Yes No
Medications included Yes No
Equipment included Yes No
Levels of care HomeInpatientRespiteContinuous Home
Home
Bereavement support Yes No
Primary care/specialty Visits Yes Yes
Advanced therapies Yes Yes
Care Plan review Weekly Variable
Service Differentiators
30
Case of RC (Cont.)
• Family elects home health
– Rectal abscess antibiotics 2 weeks IV
– Physical therapy deconditioning
– Continue pain management
• One week later, patient becomes short of breath and experiences some chest pain
• Called home health, which requested patient return to hospital
31

4/25/2016
17
Cumulative Incidence of ED Use—Last 6 Months of Life
• 41% > 1 ED visit in last 6 months of life• 12% > 1 ED visit in last month of life• Almost 10% in ED last day of life 32
Case of RC (Cont.)
• In ED, patient hypotensive and tachycardia
• Severe respiratory acidosis
– PE and pneumonia diagnosed
– Anticoagulation and antibiotics initiated
• Less responsive over next hour and intubated
• Transferred from ED to ICU
• One week later, family stops life‐sustaining therapy; patient dies in hospital
33
4/25/2016
18
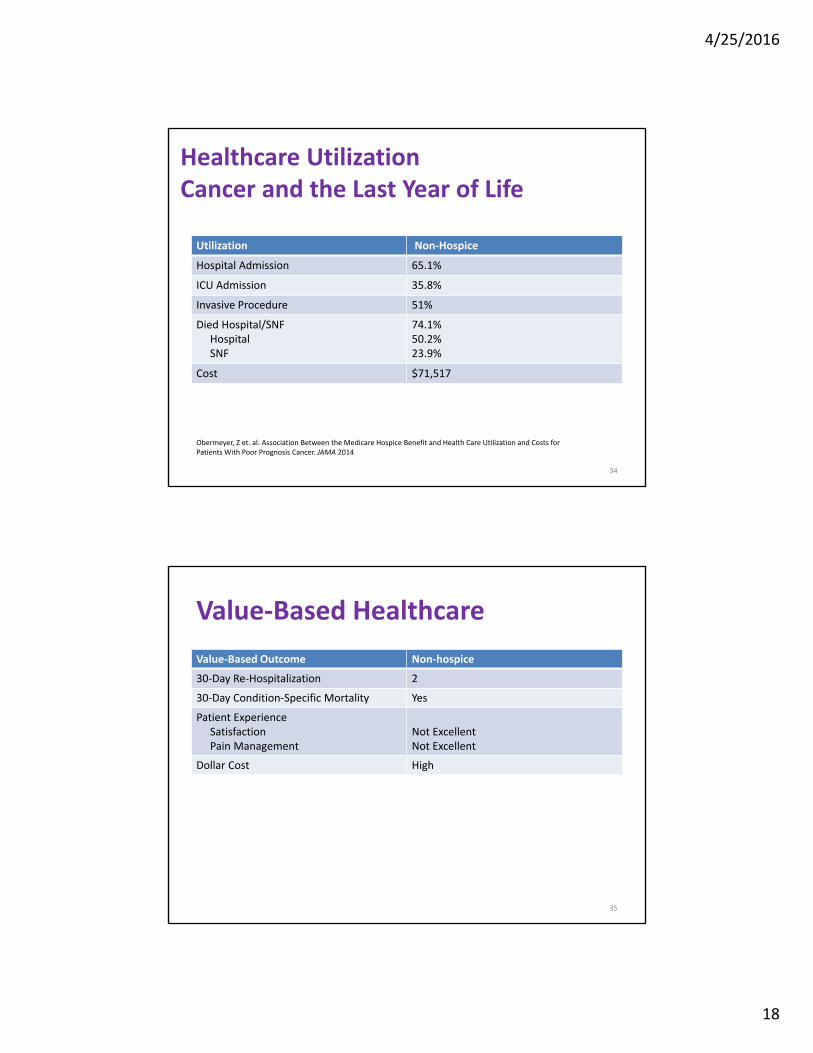
Healthcare Utilization Cancer and the Last Year of Life
Utilization Non‐Hospice
Hospital Admission 65.1%
ICU Admission 35.8%
Invasive Procedure 51%
Died Hospital/SNFHospitalSNF
74.1%50.2%23.9%
Cost $71,517
Obermeyer, Z et. al. Association Between the Medicare Hospice Benefit and Health Care Utilization and Costs for Patients With Poor Prognosis Cancer. JAMA 2014
34
Value‐Based Healthcare
Value‐Based Outcome Non‐hospice
30‐Day Re‐Hospitalization 2
30‐Day Condition‐Specific Mortality Yes
Patient ExperienceSatisfactionPain Management
Not ExcellentNot Excellent
Dollar Cost High
35

4/25/2016
19
Case of RC
RC is a 59 y/o male with rectal cancer admitted to hospital with shortness of breath, nausea, vomiting, pain and increased ostomy output five days after receiving third line of chemotherapy. He spends about 50% of his time in a chair or bed.• Antibiotics for pneumonia• IVF for dehydration• Anti-emetics for nausea and vomiting• Analgesics for pain management
36
RC Health Status• Nutrition: Lost approximately 5% of weight in last 30 days,
fair appetite
• Function: No falls; now walks with a walker; 50% of time in a bed or chair
• Cognition: Intact
• Disease specific: Progression of pulmonary and hepatic metastasis. New malignant pleural effusions
• Healthcare utilization: Current hospitalization
• Symptoms: Fair appetite, worsening pain, nausea and vomiting
37

4/25/2016
20
Patient-Centered Care•Treat pneumonia•More chemotherapy•Full code•Symptom control•PT to improve strength
Right Care, Right Place, Right Time• Patient experience• Other quality metrics• Hospital readmissions• Mortality• Cost
38
Goals of Care
Case of RC (Cont.)
• Pneumonia and shortness of breath slowly improve with antibiotics
• Nausea and vomiting resolve with IVF
• IV hydromorphone for pain control
• Ostomy output decreases
• Physical therapy consult
– Participation but unclear prospects for improvement
– Appointment in oncology 4 weeks
• Palliative care consulted
39

4/25/2016
21
Palliative Care Versus HospiceCharacteristic Hospice Palliative Care
Prognosis 6 months or less Advanced illness
Team Members PhysicianNurseSocial workerPastoral servicesNursing assistantVolunteer
Program‐dependent
Other services MedicationsMedical equipmentAfter‐hours careBereavement
None
Funding Medicare Part A Medicare Part BGrants
Location Patient‐dependent Traditionally hospital
40
SPIKES Protocol
• Setting up the Interview and listening skills
• Patient perception
• Invitation
• Knowledge
• Explore emotions and empathize
• Strategy and summary
Baile WF et al. Oncologist 2000
41

4/25/2016
22
Cancer Prognosis
• Performance status is key determinant
– Activity and energy
– Lose about 70% in last 3 months of life
• How much time do you spend sitting in a chair or lying down?
– >50% then prognosis less than 3 months
• Patients with solid tumor and not receiving chemotherapy prognosis less than 6 months
42
Index/symptoms Value Median Survival
>50% of day sleeping
Present ~3mos or less
KPS < 40 ~< 3 months
Anorexia Present <58 days
Confusion Present <38 days
Dysphagia Present <30 days
Dyspnea Present <30 days
Xerostomis Present <50 days
Physician Estimate
3 months 30 days
43
Cancer and Prognosis Clinical Indicators

4/25/2016
23
Cancer Prognosis: Helpful Numbers
Cancer Syndrome Estimated Survival
Malignant Hypercalcemia 8 weeks (except newly diagnosed breastor MM)
Malignant Pericardial Effusion 8 weeks
Carcinomatous Meningitis 8‐12 weeks
Multiple brain mets 1‐2 months no XRT, 3‐6 months with XRT
Malignant Ascites Less than 6 months
Malignant pleural effusion Less than 6 months
Malignant bowel obstruction Less than 6 months
Fast Fact 13
44
45
In‐Hospital CPR

4/25/2016
24
46
EOL Discussions and Psychological Well‐Being
47
EOL Discussions and Medical Care in Last Week of Life

4/25/2016
25
Quality of Life and Aggressive EOL Care
Wright AA. JAMA 2008;30048
AfferentPainFiber
Brainstem
CognitiveBehaviorTherapy
NSAIDs/DEX
LA/Anticonvulsants
Opioids/NMDA/α2-δ Ca Channel
TCA/SNRI’s49
Pain Management

4/25/2016
26
Wood GJ, Shega JW, Lynch B, Von Roenn JH. Management of Intractable Nausea and Vomiting in Patients at the End of Life: “I Was Feeling Nauseous All of the Time . . . Nothing Was Working." JAMA. 2007;298(10):1196‐1207 50
Nausea and Vomiting Pathways
Case of RC (cont.)
• Wants to complete treatment for pneumonia
• Not sure about more chemotherapy
• DNR
• Some physical therapy
• Hospice informational visit
– Agreed to hospice
– Oral antibiotics, PT and symptom control
51

4/25/2016
27
Case of RC (cont.)• Week 1
– Completes antibiotics for pneumonia
– Participation in physical therapy
• Improvement in strength but not endurance
– Pain in rectal area continued to worsen po hydromorphone
• Week 2
– Fever developed
– Increased fatigue
– Purulent drainage from rectum
• Calls hospice. Nurse instructs patient to take more pohydromorphone and will be there in one hour
52
Case of RC (Cont.)
• Patient and family become anxious and goes to ED– CT scan demonstrated progression of lung and liver metastasis plus
rectal abscess
• Rectal drain and antibiotics initiated
• IVF for sepsis
• Patient has 10/10 rectal pain with hyperalgesia
– Parenteral hydromorphone
53

4/25/2016
28
Allen L A et al. Circulation 2012;125:1928-1952
• Be at home
• Treat rectal abscess
• Pain control
• DNR
• PT to improve strength
54
Elements Important to Goals‐of‐Care Conversations, Shared Decision‐Making
Hospital(ED/CC/Telemetry/Med-Surg)
IPU GIP or Home
ICC ICC
Home Home
Visit VisitICC ICCTelecare Telecare
VisitFrequency
VirtualED
MobileIntensive Palliative
Care
Visit Frequency
VirtualED
MobileIntensive Palliative
Care
Patient
ED
55

4/25/2016
29
Hospital Readmissions
30‐DayReadmission
VITAS Healthcare(Hospice)
3.2%
Skilled Care 22.6%
Home Health 21.4%
Home 18.0%
56
Case of RC (Cont.)
• Transfer to home on CC with PICC line
– IV antibiotics for 4 weeks
– Rectal drain
– IVF for sepsis for 2 days
• Patient has 10/10 rectal pain with hyperalgesia
– oral hydromorphone titration at home
57

4/25/2016
30
Case of RC (Cont.)
• After 6 days of CC, transitions to routine level of care– Continue IV antibiotics daily for abscess
– Physical therapy for deconditioning
– Pain management
– Ongoing education about disease progression and poor prognosis
– Social worker and patient work on funeral plans and write letters for him to leave for wife and kids
– Massage and music therapy also initiated and helpful
58
Case of RC (Cont.)
• One week later, patient become short of breath and experiences some chest pain
• Nurse comes out and places patient on CC
• Goal of care determined to be comfort
• Patient dies peacefully at home several days later, surrounded by family
• Death attendance and bereavement process begin
59

4/25/2016
31
Healthcare Utilization Cancer Last Year of Life
Utilization Non‐Hospice Hospice Odds
Hospital Admission 65.1% 42.3% 1.5 (1.5‐1.6)
ICU Admission 35.8% 14.8% 2.4 (2.2‐2.5)
Invasive Procedure 51% 26.7% 1.9 (1.9‐2.0)
Died Hospital/SNFHospitalSNF
74.1%50.2%23.9%
14.0%3.4%10.5%
5.3 (5.1‐5.5)14.6 (13.5‐15.8)2.3 (2.2‐2.4)
Obermeyer, Z et. Al. Association Between the Medicare Hospice Benefit and Health Care Utilization and Costs for Patients With Poor‐Prognosis Cancer. JAMA 2014
60
Healthcare Costs Cancer Last Year of Life
Exposure (weeks) Non‐Hospice Hospice Difference
1 $71,582 $66,779 $4,803
2 $70,987 $63,013 $7,848
3‐4 $72,660 $59,595 $13,065
5‐8 $74,890 $56,986 $17,903
9‐26 $72,432 $60,326 $12,106
27‐52 $66,035 $65,300 $735
>52 $48,918 $56,368 ‐$7.387
Total $71,517 $62,819 $8,697
Obermeyer, Z et. Al. Association Between the Medicare Hospice Benefit and Health Care Utilization and Costs for Patients With Poor‐Prognosis Cancer. JAMA 2014
61

4/25/2016
32
Value‐Based Healthcare
Value‐Based Outcome Non‐hospice Hospice
30‐Day Re‐Hospitalization 2 0
30‐Day Condition‐Specific Mortality
Yes No
Patient ExperienceSatisfactionPain Management
Not ExcellentNot Excellent
ExcellentExcellent
Dollar Cost Higher Lower
62
Summary
• Hospice is value‐based healthcare
– Patient experience
– Hospital re‐admissions
– Condition‐specific 30‐day hospital‐specific mortality
– Healthcare costs
• Hospice—not home health or palliative care— provides comprehensive EOL care
• Differentiators of value: continuous care, visit frequency and after‐hours service
63