shock adult health ii spring, 2009 jerry carley msn, ma, rn, cne
TRANSCRIPT

SHOCK
SHOCK
ADULT HEALTH IISPRING, 2009
Jerry CarleyMSN, MA, RN, CNE


January 2009:Brazilian Super Model Dies

QuestionsTo
Ponder:Shock

• 1. A client arrives in the emergency room in the nonprogressive stage of shock. What clinical manifestations would the nurse expect this client to exhibit?
• A. Decreased heart rate and decreased urinary output• B. Increased heart rate and decreased urinary output• C. Increased pulse pressure and increased heart rate• D. Decreased pulse pressure and decreased heart rate

• 2. Your client has multi-trauma & just arrived in the ER. The client’s urinary output is normal, whereas respiratory rate and heart rate are slightly elevated from baseline. Which of the following should the nurse suspect?
• A. Early stage of shock• B. Compensatory stage of shock• C. Intermediate stage of shock• D. Refractory stage of shock

• 3. A client has been admitted with a gastrointestinal ulcer. The client is NPO and has a nasogastric tube in place connected to low intermittent suction. What form of shock should the nurse suspect / monitor this client for?
• A. Distributive shock• B. Obstructive shock• C. Cardiogenic shock• D. Hypovolemic shock

• 4. A client brought to the emergency room after a motor vehicle accident is suspected of having internal bleeding. What initial clinical manifestation of hypovolemic shock would the nurse expect to find in this client?
• A. Increased respiratory rate• B. Decreased urinary output• C. Increased heart rate• D. Cool, pale skin

• 5. A client in hypovolemic shock has been placed on a dopamine hydrochloride drip. Which parameter would indicate a desired client response to this drug?
• A. Hypotension• B. Tachycardia• C. Increased cardiac output• D. Decreased mean arterial pressure

• 6. A nurse is monitoring a client who is receiving a dopamine hydrochloride drip for the treatment of shock. What symptom would indicate a possible overdose of this medication?
• A. Pallor• B. Hypertension• C. Palmar erythema• D. Increased pulse deficit

• 7. What assessment is most appropriate for the client receiving sodium nitroprusside?
• A. Assess for chest pain.• B. Assess blood pressure every 15 minutes.• C. Monitor urinary output every 30 minutes.• D. Observe the client’s extremities for color
and perfusion.

• 8. Which manifestations should the nurse expect when caring for the client with distributive shock resulting from an anaphylactic event?
• A. Increased heart rate and blood pressure• B. Increased blood pressure and cardiac output• C. Decreased blood pressure and respiratory rate• D. Decreased blood pressure and edema

• 9. The client has all the following clinical manifestations. Which one alerts the nurse to the probability of septic shock?
• A. Hypotension• B. Pale, clammy skin• C. Anxiety and confusion• D. Oozing of blood at the IV site

End of Quiz(answers later)
• 10. The average blood volume for an adult is 65 – 75 mL /Kg
• The client weighs 209 lbs• What is the estimated blood volume for this
patient?

At the conclusion of this presentation, the nurse will be able to:
• 1. Define the concept known as SHOCK.• 2. Name, discuss, compare and contrast the four general
categories of shock.• 3. Name, discuss, compare and contrast the four stages of shock.• 4. Name, discuss, compare and contrast etiology / risk factors
associated with the four general categories of shock.• 5. Name the various diagnostic tests helpful in diagnosing and
monitoring shock.• 6. Identify and Discuss nursing interventions associated with
treatment of clients with shock• 7. Identify and Discuss the stages of shock; compare and contrast
associated assessment findings with the stages of shock.• 8. Identify and discuss pharmacologic medications and
interventions associated with the various types of shock.

• C.O. = HR X SV• (CRAP) • contractility rate afterload preload
• BP= C.O. X PVR
• MAP= (2 x D) + S / 3

A Concept Map: Shock Hypovolemic Shock
Insufficient oxygenation of tissues related to a sustained decrease in
mean arterial pressure (MAP)
*Chief Complaint: S/P MVCPain
Multiple FracturesLower Extremities;
Fractured lower two ribs, bilateral
Medical History: NegativeMedications:
NoneLab Studies:
Hgb 12.2Hct 55%WBC 18.8BS 110
Physical Exam:HR 138Resp 32
BP 88/68Pulse Ox 85%
Restless, Irritable
Risk Factors
Cardiovascular: Tachycardia (+) Hypotension (+) Decreased PO2 (+)
Respiratory: Tachypnea (+) Lungs CTA
Integumentary: Pallor (+) Capillary Refill > 3 sec
Kidney / Urinary:Output < 30 mL/hrSG > 1.035
CNS:Change in level of consciousnessPain, acute Glasgow= 10
Musculoskeletal:Deformity, ecchymosis and edema, both thighsDeformity, ecchymosis, crepitance bilat lower rib cage
HemodynamicRegulation
ShockManagement
F/EManagement
IVTherapy
HypovolemiaManagement
PainManagement
Cardiac / Pump
Effectiveness
CirculationStatus
Fluid Balance
Immobilization / Pain Medications
Seth, 17 y.o.Multi-Trauma
anal
yze
Decreased Cardiac Output
Risk forIneffective Tissue Perfusion
Deficient FluidVolume
Pain
NSG DX NURSING Interventions
PATIENT Outcomes

A Tale of4 Patients
Roseline, 36 y.o. w/ hxAortic Stenosis, CHF
Ian, 26 y.o.Meningococcal meningitis
Frank 32 y.o.Anaphylaxis
Boyd, 17 y.o.S/P MVA,Multiple Trauma
Hypovolemic Shock
ObstructiveShock
DistributiveShock
SepticShock

Defined…
• Shock: a state of inadequate tissue perfusion that impairs maintenance of normal cellular metabolism. Any condition that compromises oxygen delivery to tissues and organs can cause shock.
THE CAUSE OF SHOCK, CATEGORY OF SHOCK, AND STAGE OF SHOCKDIRECT THE SPECIFIC TREATMENT
STAGES:INITIALCOMPENSATORYPROGRESSIVE,REFRACTORY

Types of Shock(Classified by underlying cause)
•Cardiogenic•Hypovolemic•Distributive•Obstructive
“Pump Failure” or “Heart Failure”
Decrease in intravascular volume of 10-15% or more
Widespread vasodilation and capillarypermeability (3 types…)(septic, neurogenic, anaphylactic)
Mechanical blockage in the heart or great vessels

Progression of Shock (Stages) Initial
Compensatory
Progressive
Refractory
No visible changes in client parameters, changes are nowoccurring on the cellular level only
Body is mounting measures to increase cardiac output to restore tissue perfusion and oxygenation.
Compensatory mechanisms begin to fail
IRREVERSIBLE;TOTAL BODY FAILURE

Risk Factors
• Cardiogenic• Hypovolemic
• Distributive• Septic• Neurogenic• Anaphylactic• Obstructive
Pump failure due to myocardial infarction, heart failure,Cardiomyopathy, dysrhythmias, cardiac tamponade, valvular rupture or valvular stenosis
Excessive fluid loss from diuresis, vomiting & diarrhea; Blood loss secondary to surgery, trauma, ob-gyn causes;Burns; Diabetic Ketoacidosis
Endotoxins and other mediators causing massive vasodilation. Most common is gram-negative bacteria.
Loss of sympathetic tone causing massive vasodilation. Trauma, spinal shock, and epidural anesthesia are among the causes.
Antigen-antibody reaction causing massive vasodilation.
Blockage of great vessels. Cardiac valve stenosis, pulmonaryEmbolism, and aortic dissection are among the causes.

Diagnostic Procedures• ABG’s• Hemodynamic Monitoring• Cardiogenic Shock:• EKG, Echocardiogram, CT Scans, Cardiac catheterization, CXR, Cardiac
Enzymes• Hypovolemic Shock:• Hgb & Hct; Type & Crossmatch; investigate for source of bleeding• Septic Shock:• Cultures: blood, urine, wound• Coagulation tests: PT, PTT, INR• Obstructive Shock: • Echocardiogram, CT scan, • Monitor Signs & Symptoms• Hypoxia• Hypotension (MAP < 60 mm Hg)• Tachycardia, weak thready pulse
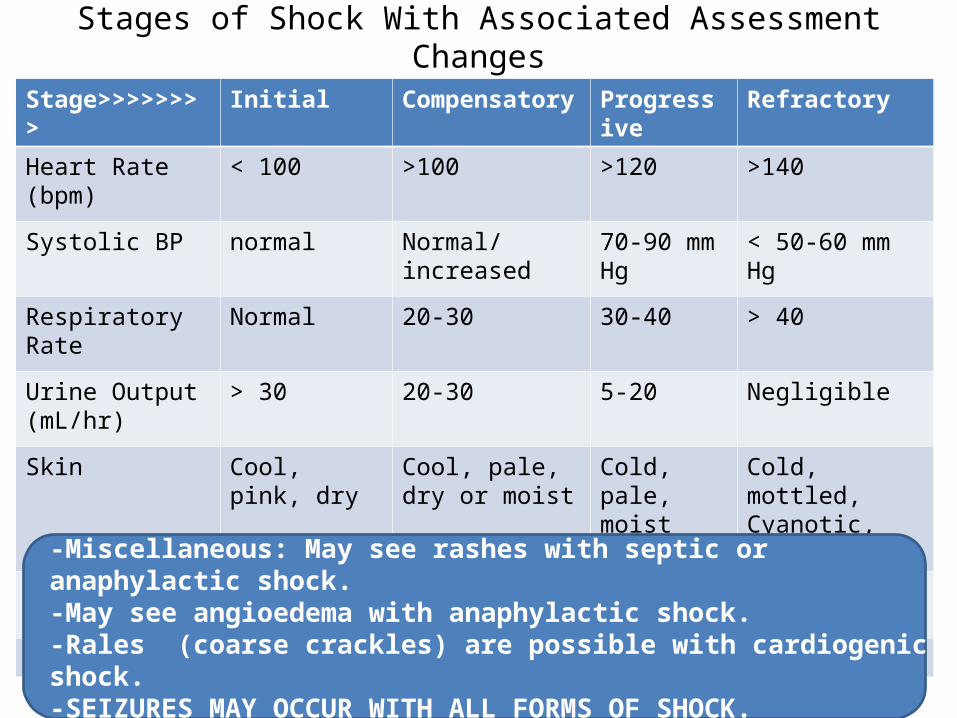
Stages of Shock With Associated Assessment Changes
Stage>>>>>>>> Initial Compensatory Progressive Refractory
Heart Rate(bpm)
< 100 >100 >120 >140
Systolic BP normal Normal/increased
70-90 mm Hg
< 50-60 mm Hg
Respiratory Rate Normal 20-30 30-40 > 40
Urine Output(mL/hr)
> 30 20-30 5-20 Negligible
Skin Cool, pink, dry Cool, pale, dry or moist
Cold, pale, moist
Cold, mottled,Cyanotic, dry
Capillary Refill Normal Slightly delayed Delayed Not noted
-Miscellaneous: May see rashes with septic or anaphylactic shock.-May see angioedema with anaphylactic shock.-Rales (coarse crackles) are possible with cardiogenic shock.-SEIZURES MAY OCCUR WITH ALL FORMS OF SHOCK.-FEVER MAY OCCUR WITH ALL FORMS OF SHOCK— BUT ESPECIALLY SEPTIC SHOCK

Skin Assessment

Shock PositionEvidence-Based Practice Update:
FriedrichTrendelenberg

Assess & Monitor• PRIORITY: ______________• Vital signs• Urinary Output• LOC• Cardiac Rhythm• Skin color, temperature, moisture, capillary refill,
turgor• Symptoms related to system:• chest pain, change in heart sounds, lung
sounds, bowel sounds, neurological status
OXYGENATION
NANDA’s
• Decreased Cardiac Output• Impaired Gas Exchange• Ineffective Tissue Perfusion• Deficient Fluid Volume• Anxiety

Cardiogenic Shock• When thinking about the hemodynamics of
cardiogenic shock, keep it simple:
• The components of cardiac output are: Contractility, Rate, Afterload, and Preload, or “CRAP.” To manage these patients, you’ve got to know CRAP! (This acronym has long been passed down to many a critical care and cath lab staff and is helpful when managing cardiogenic shock).
• Every therapeutic intervention is aimed towards improving or altering a component of cardiac output — or something in CRAP.

Nursing Interventions


Pharmacology & Shock
HYPOVOLEMIC CARDIOGENIC ANAPHYLACTIC SEPTIC NEUROGENIC ALL TYPES
Volume ReplacementColloids & Crystalloids
Afterload reducers
Antihistamines Antibiotics Volume Replacement
ProtonPumpInhibitors
Vasopressors to increase blood pressure(Replace volume first)
InotropicAgents
Epinephrine Nor-epinephrine
Nor-epinephrine
DVTProphylaxis
Vasopressors Heparin,Then clotting factors, platelets, & plasma

MAP Mean Arterial Pressure
• MAP = [(2*D)+S] / 3• [ (2 x 60) + 100] / 3 = 73.3 mm Hg
• It is believed that a MAP that is greater than 60 mmHg is enough to sustain the organs of the average person.
• If the MAP falls significantly below this number for an appreciable time, the end organ will not get enough blood flow, and will become ischemic.
PT’s BP = 100/60 mm Hg

Hypovolemic Shock
• Average Blood Volume = 65-75 mL /kg• 75 ml/Kg X 75 kg = 5625 mL = 5.625 L
5-6 Liters
EBL 10% - 15%Yields Hypovolemic Shock
0.10 x 5625 = 560 mL0.15 x 5625 = 844 ml
BACK !

Shock Pharmacology:“Pressor Agents”

Milrinone / Amrinone
• Belong to new class of agents “Bipyridines”• Non-receptor mediated activity based on
selective inhibition of Phosphodiesterase Type III enzyme resulting in cAMP accumulation in myocardium
• cAMP increases force of contraction and rate and extent of relaxation of myocardium
• Inotropic, vasodilator and lusotropic effect• ( lusotropic= direct improvement of the relaxation phase of the LV.)

Amrinone(Inacor®)
• First generation agent - limited use now • Long half-life (4.4 hours) with potential for
prolonged hypotension after loading dose• Associated with thrombocytopenia• Dosage: Load with 0.75 mg/kg with infusion
rate of 5-10 mcg/kg/min• Milrinone is preferred drug from this group

Milrinone(Primacor®)
• Increases CO by improving contractility, decreased SVR, PVR , lusotropic effect; decreased preload due to vasodilatation
• Unique in beneficial effects on RV function• Half-life is 1-2 hours• Load with 50 mcg/kg over 30 mins followed by
0.3 to 0.75 mcg/kg/min• No increase in myocardial O2 requirement

Epinephrine
Actions are dose dependent (mcg/kg/min):0.02-0.08 = mostly beta1 and beta2 stimulation.
increased cardiac outputmild vasodilation
0.1-2.0 = mix of beta1 and alpha1
increase cardiac outputincrease SVR = vasoconstriction
> 2.0 = mostly alpha1
increase SVR, and may decrease CO by increasing afterload

Dopamine
• Intermediate product in the enzymatic pathway leading to the production of norepinephrine; thus, it indirectly acts by releasing norepinephrine.
• Directly has alpha, beta and dopaminergic actions which are dose-dependent.
• Indications are based on the adrenergic actions desired.

Dopamine
• Improve renal perfusion 2-5 mcg/kg/min• Improve C.O. in mild to moderate Cardiogenic
or Distributive Shock 5-10mcg/kg/min• Post-resuscitation stabilization in patients
with hypotension (in conjunction with fluid therapy) 10-20mcg/kg/min

Venodilators / Vasodilators
Classified by site of action
-Venodilators: reduce preload - Nitroglycerin-Arteriolar dilators: reduce afterload Minoxidil and Hydralazine-Combined: act on both arterial and venous beds and reduce both pre- and afterload Sodium Nitroprusside (Nipride)

Nipride ®nitroprusside
-Vasodilator that acts directly on arterial and venous vascular smooth muscle.-Indicated in hypertension and low cardiac output states with increased SVR.-Also used in post-operative cardiac surgery to decrease afterload on an injured heart.-Action is immediate; half-life is short; titratable action.

Nipride ®
-Toxicity is with cyanide, one of the metabolites of the breakdown of nipride.-Severe, unexplained metabolic acidosis might suggest cyanide toxicity.-Dose starts at 0.5 mcg/kg/min and titrate to 5 mcg/kg/min to desired effect. May go higher (up to 10 mcg/kg/min) for short periods of time.

Nitroglycerin
• Direct vasodilator as well, but the major effect is as a venodilator with lesser effect on arterioles.
• Not as effective as nitroprusside in lowering blood pressure.
• Another potential benefit is relaxation of the coronary arteries, thus improving myocardial regional blood flow and myocardial oxygen demand.

NTG
-Used to improve myocardial perfusion following cardiac surgery-Dose ranges from 0.5 to 8 mcg/kg/min. Typical dose is 2 mcg/kg/min for 24 to 48 hours post-operatively-Methemoglobinemia is potential side effect
Isoproterenol(Isuprel ®)
-Synthetic catecholamine-Non-specific beta agonist with minimal alpha-adrenergic effects.-Causes inotropy, chronotropy, and systemic and pulmonary vasodilatation.-Indications: bradycardia, decreased cardiac output, bronchospasm (bronchodilator).-No longer available in some markets

Isoproterenol
-Occasionally used to maintain heart rate following heart transplantation.
-Dose starts at 0.01 mcg/kg/min and is increased to 1.0 mcg/kg/min for desired effect.

Selecting inotropic and vasopressor agents for specific hemodynamic disturbances
Normal Decreased Elevated
Septic Shock Stroke index High Stroke Index low to N
None or dopamineDobutamine or
dopamine
NorepinephrineDopamine or epinephrine
(or dobutamine plusnorephinephrine)
NoneDobutamine
plusnitroprusside
Cardiogenic shock Dobutamine or amrinone
or dopamine
Epinephrine or dopamine
Myocardial dysfunction (complicating critical illness)
Dobutamine or dopamine
or amrinone
Epinephrine or dopamine(or dobutamine plus
norepinephrine)
Dobutamineplus
nitroprusside
CHF Dobutamine or dopamine
or amrinone
Dobutamineplus
nitroprusside
Bradycardia None Isoproterenol None
Hemodynamicpattern
BP or SVR>>>>>>>>>>>>>>>>>>>>>>>>>>>>>>>>>>>>>>

• 1. A client arrives in the emergency room in the nonprogressive stage of shock. What clinical manifestations would the nurse expect this client to exhibit?
• A. Decreased heart rate and decreased urinary output• B. Increased heart rate and decreased urinary output• C. Increased pulse pressure and increased heart rate• D. Decreased pulse pressure and decreased heart rate
In the nonprogressive stage of shock, both kidney and cardiovascular compensations, in addition to chemical compensatory mechanisms, are needed. These result in an increase in heart rate and decrease in urinary output to maintain MAP (mean arterial pressure) and volume in the central blood vessels.

An increase in heart and respiratory rates (heart rate first) from the client’s baseline or a slight increase in diastolic blood
pressure may be the only objective manifestations of early shock.
• 2. Your client has multi-trauma & just arrived in the ER. The client’s urinary output is normal, whereas respiratory rate and heart rate are slightly elevated from baseline. Which of the following should the nurse suspect?
• A. Early stage of shock• B. Compensatory stage of shock• C. Intermediate stage of shock• D. Refractory stage of shock

This client is at risk for hypovolemic shock caused by bleeding from gastrointestinal ulcers, leading to fluid volume loss, and from nasogastric suction that can
compound the situation if the client is not sufficiently hydrated with IV fluids.
• 3. A client has been admitted with a gastrointestinal ulcer. The client is NPO and has a nasogastric tube in place connected to low suction. What form of shock should the nurse monitor this client for?
• A. Distributive shock• B. Obstructive shock• C. Cardiogenic shock• D. Hypovolemic shock

The first manifestations of hypovolemic shock result from compensatory mechanisms. Signs of shock are first evident as
changes in cardiovascular function. As shock progresses, changes in skin, respiration, and kidney function progress.
• 4. A client brought to the emergency room after a motor vehicle accident is suspected of having internal bleeding. What initial clinical manifestation of hypovolemic shock would the nurse expect to find in this client?
• A. Increased respiratory rate• B. Decreased urinary output• C. Increased heart rate• D. Cool, pale skin

Dopamine hydrochloride causes vasoconstriction that, in turn, increases cardiac output and mean arterial pressure, thereby
improving tissue perfusion and oxygenation.
• 5. A client in hypovolemic shock has been placed on a dopamine hydrochloride drip. Which parameter would indicate a desired client response to this drug?
• A. Hypotension• B. Tachycardia• C. Increased cardiac output• D. Decreased mean arterial pressure

An overdose of dopamine hydrochloride is manifested by hypertension.
• 6. A nurse is monitoring a client who is receiving a dopamine hydrochloride drip for the treatment of shock. What symptom would indicate a possible overdose of this medication?
• A. Pallor• B. Hypertension• C. Palmar erythema• D. Increased pulse deficit

The client receiving sodium nitroprusside should have his or her blood pressure assessed every 15 minutes.
Higher doses can cause systemic vasodilation and increase shock.
• 7. What assessment is most appropriate for the client receiving sodium nitroprusside?
• A. Assess for chest pain.• B. Assess blood pressure every 15 minutes.• C. Monitor urinary output every 30 minutes.• D. Observe the client’s extremities for color
and perfusion.

Anaphylaxis damages cells and causes release of large amounts of histamine and other inflammatory
chemicals, which results in massive blood vessel dilation and increased capillary leak.
• 8. Which manifestations should the nurse expect when caring for the client with distributive shock resulting from an anaphylactic event?
• A. Increased heart rate and blood pressure• B. Increased blood pressure and cardiac output• C. Decreased blood pressure and respiratory rate• D. Decreased blood pressure and edema

The late phase of sepsis-induced distributive shock is characterized by most of the same cardiovascular manifestations as any other type of shock. The distinguishing feature is the lack of ability to
clot blood, causing the client to bleed from areas of minor trauma and to bleed spontaneously.
• 9. The client has all the following clinical manifestations. Which one alerts the nurse to the probability of septic shock?
• A. Hypotension• B. Pale, clammy skin• C. Anxiety and confusion• D. Oozing of blood at the IV site

(209 lbs /2.2 lbs/kg) = 95 kg65 mL/Kg x 95 kg = 6175 ml75 mL/kg x 95 kg = 7125 mL
Estimated Blood Volume = 6175-7125 mLor
6.175 L – 7.125 L
• 10. The average blood volume for an adult is 65 – 75 mL /Kg
• The client weighs 209 lbs• What is the estimated blood volume for this
patient?

•Reading / Resources

What is cardiogenic shock?•
By definition, cardiogenic shock is decreased cardiac output and evidence of tissue hypoperfusion in the presence of adequate intravascular volume.1 The presence of adequate intravascular volume is important. This differentiates cardiogenic shock from other types of shock, which typically have a relative or an absolute volume deficit. With cardiogenic shock, the patient usually has enough intravascular volume — it’s just not going to the right place(s) due to pump failure. These patients present with sustained hypotension defined by blood pressure less than 80 mmHg (or 90 mmHg if on pressors, inotropic agents or intraaortic balloon pump support) for greater than 30–60 minutes, a cardiac index under 1.8 liters/ minute, in the presence of a left ventricular end-diastolic pressure (LVEDP) or pulmonary capillary wedge pressure (PCWP) greater than or equal to 18 mmHg.4,5 When dealing with “cardiogenic shock,” think “decreased forward flow” because interventions must be aimed toward restoration of forward volume flow. We lose if we don’t perfuse!
Cath Lab Digest - ISSN: 1073-2667 - Volume 11 - Issue 11 - November 2003 - Pages: 20 - 25
Cardiogenic Shock and Hemodynamic Support: A Realistic Management Approach- Mary Dahling, RN, MSN, CCRN, CNS, Cardiothoracic Surgery, Sentara Norfolk Hospital, Norfolk, Virginia
• What causes cardiogenic shock? The major cause of cardiogenic shock is ischemic disease, both of the left and right ventricle. Valvular heart disease/dysfunction may also result in cardiogenic shock, a classic example being acute mitral insufficiency or regurgitation. Additional causes include:
1. Trauma from a myocardial contusion;
2. Cardiomyopathies: Hypertrophic, restricted, and dilated;
3. Infectious and inflammatory processes (viral myocarditis, infective endocarditis);
4. Pulmonary hypertension resulting in right ventricular failure;
5. Toxic drugs.
The basic concept of cardiogenic shock is pump failure, not a surprise to anyone, but again, impaired forward flow is the key. When cardiac output decreases, the body responds with compensatory mechanisms. Catecholamines (norepinephrine and epinephrine), parasympathetic nervous stimulation, conduction disturbances, and dysrhythmias can all affect heart rate, but typically tachycardia is seen. Systemic vascular resistance (SVR) increases to “tighten” the arterial vascular circuit in an attempt to maintain blood pressure. But these are only temporizing measures. When caring for these patients, it helps to remember that cardiac output = stroke volume x heart rate. So unless immediate intervention is needed for a symptomatic rapid or relatively slow heart rate, efforts are aimed at increasing the stroke volume. Understanding the components of stroke volume helps direct patient management.

• Components of stroke volume: Preload, afterload, and contractility Preload is the amount of volume in the ventricle at end-diastolic filling.6 It is measured directly during heart catheterization via the LVEDP or indirectly measured by utilizing the PCWP. Think of preload as the end-diastolic “stretch” of the muscle determined by the volume of blood in the ventricle. Every heart has an optimal preload. Remember Starling’s Law: Increased stretch results in a more forceful contraction and greater stroke volume up to a physiologic limit. In other words, the muscle fiber can be stretched up to a point and result in a good contraction, but if overstretched, the contraction actually weakens and stroke volume decreases.
Afterload is resistance to ventricular ejection. Increased afterload translates into increased work for the myocardium. Afterload for either ventricle is affected by several factors, the most important being vascular resistance.6 When the arterial vascular circuit constricts in an attempt to maintain pressure, afterload increases. More oxygen and energy is required for the heart to pump volume out against this increased resistance — contributing to further problems for an ischemic ventricle. Afterload is clinically estimated for the right ventricle by calculating the pulmonary vascular resistance (PVR) and for the left ventricle, the systemic vascular resistance (SVR).
Finally, there’s contractility. Contractility is the velocity of myocardial fiber shortening at the cellular level regardless of preload and afterload.6 It’s difficult to measure at the bedside, but one would hope to see evidence of increased contractility when adding an inotropic agent such as dopamine or dobutamine.
When thinking about the hemodynamics of cardiogenic shock, keep it simple: The components of cardiac output are: Contractility, Rate, Afterload, and Preload, or “CRAP.” To manage these patients, you’ve got to know CRAP! (This acronym has long been passed down to many a critical care and cath lab staff and is helpful when managing cardiogenic shock). Every therapeutic intervention is aimed towards improving or altering a component of cardiac output — or something in CRAP.
• The spiral of cardiogenic shock The underlying pathology of cardiogenic shock is profound depression of contractility resulting in a spiral of reduced CO, hypotension, further coronary insufficiency, and further reduction in contractility. Compensatory mechanisms of tachycardia and increased SVR are typically noted. However, a systemic inflammatory response (fever, elevated white count, low SVR) may also be seen.3

• Patient Presentation In addition to tachycardia, patients often present with a narrow pulse pressure (PP). Pulse pressure is the difference between systolic and diastolic blood pressure and reflects stroke volume. Decreased stroke volume causes the pulse pressure to narrow (as is seen in cardiac tamponade). Signs and symptoms of hypotension are present: Weak or absent peripheral pulses; mottled extremities from low flow states; diaphoresis; and pallor. Patients may be restless with changes in level of consciousness. Remember that the kidneys are “seeing” a low flow state when not receiving adequate blood flow — with a response of retaining volume and concentrating urine output.

• If left ventricular failure is present, pulmonary edema and dyspnea are hallmarks of cardiogenic shock. An extra heart sound, S-3 or a ventricular gallop, is an early sign of LV failure.5 A murmur may be appreciated as the ventricle dilates from volume overload, resulting in regurgitant flow. Murmurs may also occur with papillary muscle dysfunction from ischemia. Chest pain, which can be typical or atypical, might be present if the cause of failure is ischemic disease.
If right ventricular failure is the culprit, the patient will present without pulmonary edema — clear lungs and a normal to slightly raised PCWP. Persistent hypotension, elevated RA (CVP) pressure, and jugular vein distention are often noted as volume “backs up” from the right ventricle and forward flow declines. Suspect a right ventricular infarction in patients exhibiting these symptoms who present with an inferior wall MI. The reduction of preload (hypovolemia, diuretic use, nitroglycerin) intensifies hypotension in these individuals.5 Recording right-sided precordial leads and utilizing echocardiography assists in the diagnosis.

• CRAP — Optimizing Preload Does the patient have too much or too little preload? Higher filling pressures may actually be necessary in some patients, but typically those in cardiogenic shock have too much preload in the ventricle. The higher the PCWP (preload) and the lower the cardiac index, the higher the mortality.4 If too much volume is present for the heart to handle, there are the three well-recognized “P”s for dealing with excessive preload: Pee the excess volume, park the excess volume, or pump it on forward!
1. Patients have pulmonary edema and high PCWP? Diurese them — but avoid hypovolemia (may worsen blood pressure—especially with a RV MI).
2. Poor contractility and decreased forward flow? Pump it forward with inotropic support!
3. “Pull” extra volume off the heart (decrease venous return)—i.e., nitroglycerin to dilate venous beds. Park the volume if blood pressure tolerates.
•Intravenous diuretics such as furosemide and bumetanide not only cause diuresis but also have an acute effect to increase venous capacity and decrease venous return to the heart. Morphine, in addition to decreasing pain and anxiety, also increases venous pooling.5 Even before there’s urine in the Foley bag (if you’re lucky enough to see any urine in cardiogenic shock), these drugs have already parked some excess volume. Now, pumping it forward usually means some inotropic help with dopamine, dobutamine, inamrinone, or milrinone (Inocor® and Primacor®, Sanofi-Synthelab Inc., New York, NY).

• CRAP — Optimizing Contractility Inotropic support with a sympathomimetic agent is indicated. With low blood pressure less than 70 mmHg, norepinepherine 2 to 10 mg /kg/min would be considered.5 Norepinepherine is an alpha and beta-1 agonist, meaning it causes vasoconstriction and increases contractility and heart rate. Clinically, the alpha or vasoconstrictive properties (increases SVR) are greater than beta-1 effects, so its use should be limited for temporary stabilization if possible.4
• Dopamine is a first-line inotropic agent in cardiogenic shock. It is usually initiated at 3-5 mg/kg/min and titrated up to 10 mcg/kg/min. At higher doses, dopamine provides vasopressor support. Doses greater than 10 mcg/kg/min may have undesirable effects such as tachycardia and increased pulmonary shunting along with the potential to decrease splanchnic perfusion and increase pulmonary arterial wedge pressure.1 Another inotropic agent, dobutamine, is a sympathomimetic amine with stronger beta effects than alpha effect, producing vasodilation (decreasing SVR) and increasing contractility. Dobutamine is initiated usually at 2.5–5mg /kg/min and titrated up to 10 mg/kg/min.4 As it decreases SVR, it may also decrease blood pressure making it difficult to use in those with systolic pressures below 90 mmHg.5

• Working via a different mechanism than dopamine and dobutamine are the phosphodiesterase inhibitors milrinone and inamrinone (formerly amrinone). These drugs have both inotropic and vasodilating effects, thus increasing stroke volume with both their contractile and afterload–reducing properties. These vasodilator effects may cause hypotensive episodes to develop and careful titration is needed. A loading dose may be given for both inamrinone and milrinone. The loading dose for inamrinone (Inocor®) is 0.75 mg/kg followed by an infusion of 5 to 10 mg/kg/min with total doses not to exceed 10 mg/kg/day.1 Milrinone (Primacor®) is approximately 15–20 times more potent than inamrinone. In addition, clinical studies have reported significantly less thrombocytopenia with milrinone as compared to inamrinone. Loading dose for milrinone is 50 mg/kg followed by a maintenance dose of 0.375-0.750 mg /kg/min.6 Careful dosing consideration of these drugs is required with hepatic and renal dysfunction.
By increasing contractility, all inotropic agents increase myocardial workload and in addition, may cause tachyarrhythmias, exacerbating myocardial ischemia.

• CRAP — Optimizing Heart Rate With cardiogenic shock, bradycardia is usually not the problem, but if present, a pacing wire may be necessary to sustain an adequate rate and output. Tachycardia is typically present and is related to sympathetic stimulation, a compensatory mechanism or may result from inotropic drug support. Increased heart rates not only decrease diastolic filling time, but also decrease coronary artery perfusion time. In addition myocardial workload is increased. Clearly, if the patient is in a lethal tachycardia or rapid supraventricular tachycardia (SVT), the rhythm will need termination.
It is important to try to maintain the atrial contribution to stroke volume. Asynchrony between the atria and ventricles or the absence of atrial contraction (development of atrial fibrillation) may significantly reduce cardiac output.

• CRAP — Optimizing Afterload It’s important to facilitate stroke volume ejection and forward flow by reducing the SVR if blood pressure permits. Some inotropic agents reduce SVR. Vasodilators such as nitroglycerin and sodium nitroprusside may also help. Intravenous nitroglycerin is a coronary vasodilator, but also tends to be at normal doses, a venodilator predominately dilating the venous bed. Nitroglycerin helps “park” volume. Nitroprusside, on the other hand, is a more balanced venous arterial vasodilator.6

• It is often a challenge to add these drugs because of low blood pressure. As a result, these agents must be used cautiously, if at all, for besides hypotension, a reflex tachycardia may occur and coronary perfusion pressure can drop significantly. Vasodilator therapy should not be attempted in patients with systolic pressure below 90 mmHg.6 So use caution when reducing afterload in the presence of ischemic disease.
Afterload reduction is also the mainstay of stabilization for acute mitral regurgitation (MR). In acute MR, blood flow is diverted back through the mitral valve. There is less resistance to flow into the lower pressure left atrium, verses forward flow out the aortic valve against arterial resistance (SVR). Forward flow out the “front door” (aortic valve) needs to be “encouraged”; therefore, therapies are targeted to reducing the SVR. The optimal mechanical afterload reducer is the intraaortic balloon pump, where a balloon is placed in the aorta distal to the subclavian artery and counterpulsates the heart.

• With the normal arterial waveform, the dicrotic notch signifies closure of the aortic valve closure and the beginning of diastole. Inflation of the balloon at this time augments diastolic pressure. This in turn increases coronary perfusion pressure. When the balloon deflates, aortic end-diastolic pressure decreases, making it easier for the next stroke volume to be ejected by the left ventricle. The IABP is effective for the initial stabilization of patients with cardiogenic shock. However, an IABP is not definitive therapy; definitive diagnostic and therapeutic interventions (surgical repair of the valve or revascularization) need to be performed.

References Cardiogenic Shock• 1. Sharma S, Zevitz ME. (2003). Cardiogenic shock.
www.Emedicine.com/MED/topic285.htm. [Electronic], retrieved 10/12/03.2. Hostetler MA. (2002). Cardiogenic shock. www.Emedicine.com/EMERG/topic530.htm. [Electronic], retrieved 10/12/03.3. Hochman J. Cardiogenic Shock Complicating Acute Myocardial Infarction: Expanding the Paradigm. Circulation 2003;107(24):2998-3002.4. Lee J, Lee PC. Cardiology at a glance. New York City: McGraw-Hill, 2002.5. Braunwald E. Recognition and management of patients with acute myocardial infarction. In Goldman L, Braunwald E (eds). Primary Cardiology. Philadelphia: WB Saunders, 1998.6. Darovic GO. Hemodynamic Monitoring: Invasive and non-invasive clinical application. Philadelphia: WB Saunders, 2002.7. Hollenberg SM, Kavinsky CJ, Parrillo JE. Cardiogenic shock. Ann Intern Med 1999;131(1):47-59.8. Pfisterer M. Right ventricular involvement in myocardial infarction and cardiogenic shock. Lancet 2003;362(9381):392-394.


EVIDENCE-BASED PRACTICE (EBP) GUIDELINE
• Use of Trendelenburg Position during Hypotensive Episodes
• Nursing Research Council of United Hospital – 3/06
• HISTORY AND CLINICAL PRACTICE
• In the middle of the nineteenth century it was recognized that by raising the hips of a supine patient the• bulk of abdominal viscera would slide downward toward the diaphragm thereby providing a less cluttered• operative field for procedures involving the lower abdomen and pelvis. Friedrich Trendelenburg, a• pioneering German surgeon, adopted and popularized this practice in his surgical text of 1873. Then in• the early twentieth century, other physicians began advocating the use of Trendelenburg position in the• treatment of hemorrhagic shock because of its ability to divert blood from the lower extremities to the• central circulation, augmenting cardiac filling by increasing right and left ventricular preloads, stroke• volume and cardiac output. Despite leading physicians later questioning the efficacy of this position in• the 1950s, Trendelenburg continued as a mainstay of resuscitation in a wide variety of populations.1

• REVIEW OF EVIDENCE• Several studies have measured the effects of Trendelenburg on hemodynamic parameters. These studies• have been conducted with healthy and acute/critical care populations using both observational and• experimental methods. Specific dependent variables measured include: Heart rate, blood pressure (BP),• cardiac output/cardiac index (CO/CI), central venous pressure (CVP), pulmonary artery wedge pressure• (PAWP), right and left atrial pressures (RA/LA), right and left end-systolic and end-diastolic ventricular• index (RVESVI/LVESVI), circulation time, carotid blood flow, internal jugular vein velocity, segmental• arm & leg blood flow, intrathoracic blood volume, and total blood volume displacement. Limitations of• these studies are the small sample sizes (N=10-76), lack of homogeneity of populations studied, as well as• variations in the angle (10-30o, and modified Trendelenburg with passive leg raising ranging from 45o to• 60o) and duration (range 1-30 minutes) of the position.

• Fifteen studies from the medical and nursing literature were reviewed from 1964 to 2003. Three studies 2-• 4 (20%) demonstrated a statistically significant increase in BP and CO/CI in both healthy and critically ill• populations (N=10-22). In one study, 3 these changes disappeared after 10 minutes. The other 13 studies• (80%) did not find that Trendelenburg significantly increased either BP or CO/CI in a variety of samples• (animal model, healthy individuals, surgical and critically ill patients).5-17 Sample sizes of these studies• were also small, ranging from 8-76. Four of these studies showed a slight increase (~8-10%) in CO/CI in• a small percentage of patients (7-16 %).7-8,12-13 However, these significant changes appeared to be• transient and lasted for only 1-7 minutes after the change in position. It is unlikely these changes have• clinically significant effects on patients with hypotension or low CO.

• The majority of studies on the effects of Trendelenburg position do not lend support that this intervention• significantly increases either arterial BP or CO/CI. The level of evidence for this intervention is thought• to represent “Class III” evidence, indicating that Trendelenburg position is not useful in improving BP or• CO/CI in the hypotensive patient.
• In addition, expert opinion exists with regard to the possible harmful• effects associated with this intervention. In a review of physiological changes associated with this• position, Martin 1 delineates that the sequence of symptoms* that typically occur after placing a patient in
Trendelenburg position include:
• Anxiety & restlessness• Onset of pounding vascular headache• Nasal congestion that may force mouth breathing• Progressive dyspnea• Loss of cooperation (may include overt hostility)• Struggling efforts to sit upright

• * Hypotensive and mentally obtunded patients may first become transiently more alert and then subsequently
• lose the will to struggle• The presence of cardiovascular, pulmonary and central nervous system disease can make the position• harmful by increasing myocardial oxygen consumption and dysrhythmias; reducing respiratory expansion• and promoting hypoventilation and atelectasis, as well as altering ventilation/perfusion ratios from• gravitation of blood to poorly ventilated apex; and increasing venous congestion within and outside the• cranium leading to increased intracranial pressure. As a result, the Trendelenburg position may have• detrimental effects in patients with coronary artery disease and ischemia of the lower limbs, decreased• vital capacity such as in the obese, and increased intraocular and intracranial pressure and cerebral• edema.18 Because many of the studies reviewed assessed the effects of 200 or less, the presumption is• tenable that steeper angulation could produce greater physiological abnormalities. Similarly, the longer• the head down tilt is continued, it is likely the more pronounced the abnormalities might be.

• A. The evidence supporting the hemodynamic effects of Trendelenburg in treating shock is small and• does not reveal significant, beneficial or sustained changes in BP or CO/CI. Overall, the general• conclusion from all the evidence is that Trendelenburg is probably not a useful position in• resuscitative situations to improve BP or CO/CI. Since Trendelenburg may also be associated with• harmful effects to the respiratory, neurological and vascular systems (especially in the presence of• pathology) this position should be used with caution.• B. The available evidence on Trendelenburg position lacks strength due to limitations in scientific rigor.• High-quality clinical studies of the risks and benefits of Trendelenburg position in hypotensive• patients are warranted. Trials that investigate optimal positions for resuscitation are also needed.18

References: EBP Trendelenberg• 1. Martin J. (1995). The Trendelenburg position: A review of current slants about head down tilt. J• Amer Assoc Nurs Anesths. 63 (1): 29-36.• 2. Pricolo V, Burchard K, Singh A, Moran J, & Gann D. (1986). Trendelenburg versus PASG• application: Hemodynamic response in man. J Trauma. 26 (8): 718-726.• 3. Gentili D, Benjamin E, Berger S, & Iberti T. (1988). Cardiopulmonary effects of the head-down• tilt position in elderly postoperative patients: A prospective study. Southern Medical J. 81 (10):• 1258-1260.• 4. Terai C, Anada H, Matsushima S, Shimizu S, & Okada (1995). Effects of mild Trendelenburg on• central hemodynamics and internal jugular vein velocity, cross-sectional area, and flow.• American J Emerg Med. 13 (3): 255-258.• 5. Guntheroth W. (1964). The effect of Trendelenburg’s position on blood pressure and carotid• flow. Surgery, Gyn & Obstet pp. 345-348.• 6. Taylor J, & Weil M. (1967). Failure of the Trendelenburg position to improve circulation during• clinical shock. Surgery, Gyn & Obstet , pp. 1005-1010.• 7. Sibbald W, Paterson N, Holliday R, & Baskerville J. (1979). The Trendelenburg position:• Hemodynamic effects in hypotensive and normotensive patients. Critical Care Med. 7 (5): 218-• 224.• 8. Gaffney F, Bastian B, Thal E, Atkins J, & Blomquist C. (1982). Passive leg raising does not• produce a significant or sustained Autotransfusion effect. J Trauma. 22 (3): 190-193.• 9. Sing R, O’Hara D, Sawyer M, & Marino P. (1994). Trendelenburg position and oxygen• transport in hypovolemic adults. Annals Emerg Med. 23 (3): 564-567.• 10. Bivins H, Knopp R, dos Santos. (1985). Blood volume distribution in the Trendelenburg• position. Annals Emerg Med. 14 (7): 641-643.• 11. Haennel R, Teo K, Snydmiller G, Qinnery J, & Kappagoda C. (1988). Short-term cardiovascular• adaptations to vertical head-down suspension. Arch Physical Med Rehab. 69: 352-357.

• 12. Wong D, Tremper K, Zaccari J, Hajduczek J, Konchiegeri J, & Hufstedler S. (1988). Acute• cardiovascular response to passive leg raising. Critical Care Med 16 (2): 123-125.• 13. Reich D, Konstadt S, Raissi S, Hubbard M, & Thys D. (1989). Trendelenburg position and• passive leg raising do not significantly improve cardiopulmonary performance in the anesthetized• patient with coronary artery disease. Critical Care Med. 17 (4): 313-317.• 14. McHugh G, Robinson B, & Galletly D. (1994). Leg elevation compared with Trendelenburg• position: Effects on autonomic cardiac control. British J Anaesthesia. 73: 836-837.• 15. Ostrow L, Hupp E, & Topjian D. (1994). The effect of Trendelenburg and modified Trendelenburg• positions on cardiac output, blood pressure and oxygenation: A preliminary study. Amer J Critical• Care. 3 (5): 382-386.• 16. Boulain T, Achard J, Teboul J, Richard C, Perrotin D, & Ginies G. (2002). Changes in BP• induced by passive leg raising predict response to fluid loading in critically ill patients. Chest.• 121 (4): 1245-1252.• 17. Reuter D, Felbinger T, Schmidt C, Moerstedt K, Kilger E, Lamm P et al. (2003). Trendelenburg• positioning after cardiac surgery: Effects of intrathoracic blood volume index and cardiac• performance. European J Anaesth. 20: 17-20.• 18. Bridges N, Jarquin-Valdivia A. (2005). Use of the Trendelenburg position as the resuscitation• position : To T or not to T ? Amer J Critical Care. 14 (5): 364-368.

Class IIIMay be harmful; no benefit documentedNot acceptable, not useful, may beharmful.Class III refers to interventions with noevidence of any benefit; often someevidence of harm
• Class I• Definitely recommended• Supported by excellent evidence,• with at least 1 prospective• randomized, controlled trial.• Class I interventions are always• acceptable, safe & effective.• Considered definitive standard of care• Class IIa• Acceptable & useful• Supported by good to very good• evidence. Weight of evidence and• expert opinion strongly in favor.• Class IIa interventions are acceptable,• safe & useful. Considered intervention• of choice by majority of experts.
• Class IIb• Acceptable & useful• Supported by fair to good• evidence. Weight of evidence and• expert opinion not strongly in• favor.• Class IIb interventions are also• acceptable, safe and useful. Considered• optional or alternative interventions by• majority of experts.• Indeterminate• Promising, evidence• lacking, immature• Preliminary research stage.• Evidence: No harm but no• benefit. Evidence insufficient to• support a final class decision.• Indeterminate: Describes treatments• of promise but limited evidence.
LEVELS OF EVIDENCE
