shock basic
TRANSCRIPT


DR. Neeraj Kumar Jain
Assistant Professor
Deptt. Of Surgery

Define shock and its different categories
Review basic physiologic and pathophysiologic aspects of shock
Inadequate tissue perfusion to meet tissue
demands. Usually result of inadequate blood
flow and/or oxygen delivery
Circulatory failure is a life-threatening medical
condition that occurs due to inadequate substrate
for aerobic cellular respiration. In the early stages
this is generally an inadequate tissue level of
oxygen.
Shock is not a blood pressure diagnosis

In Adults:◦ systolic BP 90 mm Hg
◦ mean arterial pressure 60 mm Hg
◦ systolic BP > 40 mm Hg from the patient’s
baseline pressure

Oxygen
Demand > Supply
• THE HEART (pump)
• THE BLOOD (circulating fluid)
• THE VASCULAR CAPACITY
(veins and arteries)
• THE MICRO- CIRCULATION

Fluid
Pump
Vessels
Flow

ATP + H2O ADP + Pi + H+ + Energy
Acidosis results from the accumulation of acid
when during anaerobic metabolism the creation
of ATP from ADP is slowed.
H+ shift extracellularly and a metabolic acidosis
develops

• Cellular responses to decreased systemic oxygen delivery•ATP depletion → ion pump dysfunction•Cellular edema•Hydrolysis of cellular membranes and cellular
death• Goal is to maintain cerebral and cardiac perfusion
•Vasoconstriction of splanchnic, musculoskeletal, and renal blood flow
• Leads to systemic metabolic lactic acidosis that overcomes the body’s compensatory mechanisms

DO2O2
CASECADESHEMO
DYNAMICS
VENTILATION
PULMONARY O2
EXCHANGE
O2 TRANSPORT
TISSUE EXCHANGE
QT
HB CONTENT
MICR
CIRCULATION
QT x HB x 10 x 1.36 X SO2 + PO2 x0.003

TISSUE PERFUSION
CONSTANT FLOW
CONSTANT DO2
TARGET FUNCTION OF CVS
REGIONAL PERFUSION PRESSURE

P = F X R
Autorgulation is controlled by;
*** Myogenic *NO
*** Metabolic *H Ione
*ADENOSINE *CO2
*PG *O2
F
P
RP R
F
FCONSTANT
TISSUEPERFUSION
MAP=60mmHg
Tissue perfusion
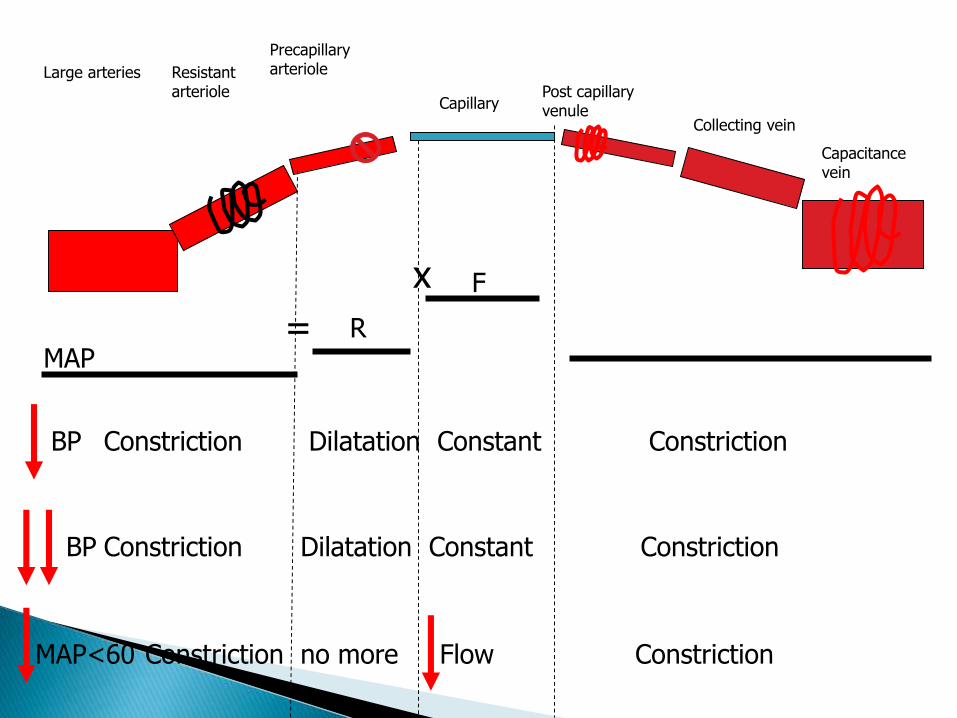
Large arteries Resistant arteriole
Precapillary arteriole
CapillaryPost capillary venule
Collecting vein
Capacitance vein
MAPR
F
BP Constriction Dilatation Constant Constriction
Constriction Dilatation Constant ConstrictionBP
MAP<60 Constriction no more Flow Constriction
=
x

REGIONAL PERFUSION PRESSURE MAP
QT
SVR
MAP = QT X SVR
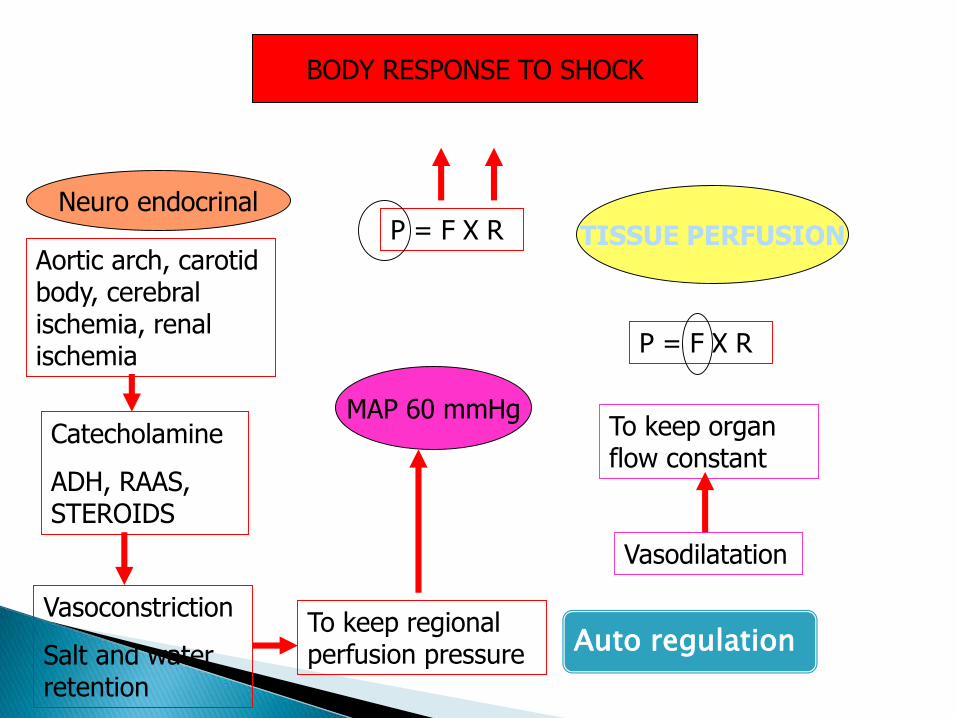
BODY RESPONSE TO SHOCK
Neuro endocrinal
Auto regulation
Aortic arch, carotid body, cerebral ischemia, renal ischemia
Catecholamine
ADH, RAAS, STEROIDS
Vasoconstriction
Salt and water retention
To keep regional perfusion pressure
Vasodilatation
To keep organ flow constant
P = F X R
MAP 60 mmHg
TISSUE PERFUSION
P = F X R

Oxygen content = 1.34 (Hgb x SaO2) + (PaO2 x 0.003)
SaO2: Oxygen saturation
Hgb: Hemoglobin concentration
PaO2: partial pressure Oxygen in plasma
To improve Oxygen content◦ Increase Hemoglobin concentration
◦ Increase saturation
Cardiac output◦ C.O. = Heart rate x stroke volume
To improve Cardiac output◦ Increase Heart rate
◦ Increase Stroke Volume
Preload – volume of blood in the ventricle
Afterload – resistance to contraction
Contractility – force applied

Compensatory mechanisms for shock
1** S.V.R.
vascular capacity
Spasm of large and resistant arteries
Catecholamine
Vasopressin
Angiotensin 2
Cortisol
Aldosterone
2** QT
Effective blood volume
x =BP (MAP> 60mmHg)
*Venous spasm to V.R.
*Salt retention Aldosterone
* Water retention ADH
*Stimulation of thirst Ag.2
*Decrease hydrostatic cap .P.
Tissue fluid reabsorption at rate 15 ml/ kg /h
Target point
Mediators


Weil and Shubin in 1972 classification
Four major categories◦ Hypovolemic
◦ Cardiogenic
◦ Extracardiac Obstructive
◦ Distributive
Overlap exists, and also concomitant categories exist
TYPES OFSHOCK
Compensated Organ perfusion is maintained
Uncompensated Circulatory failure with end organ dysfunction
Irreverisble◦ Irreparable loss of essential organs
#1 cause of death world wide◦ Gastroenteritis
◦ Hemorrhagic – Trauma, GI bleed

THE BLOOD
WHOLEBLOOD
EXTERNALHG.
INTERNALHG.
PLASMA
GUT
*VOMITING
*NGT. DRAIN
*DIARRHOEA
* FISTULA
SKIN
•SWEAT
•* BURN
KIDNEY
*DM
*DI
*DIURETIC
3rd SPACE
* ASCITES
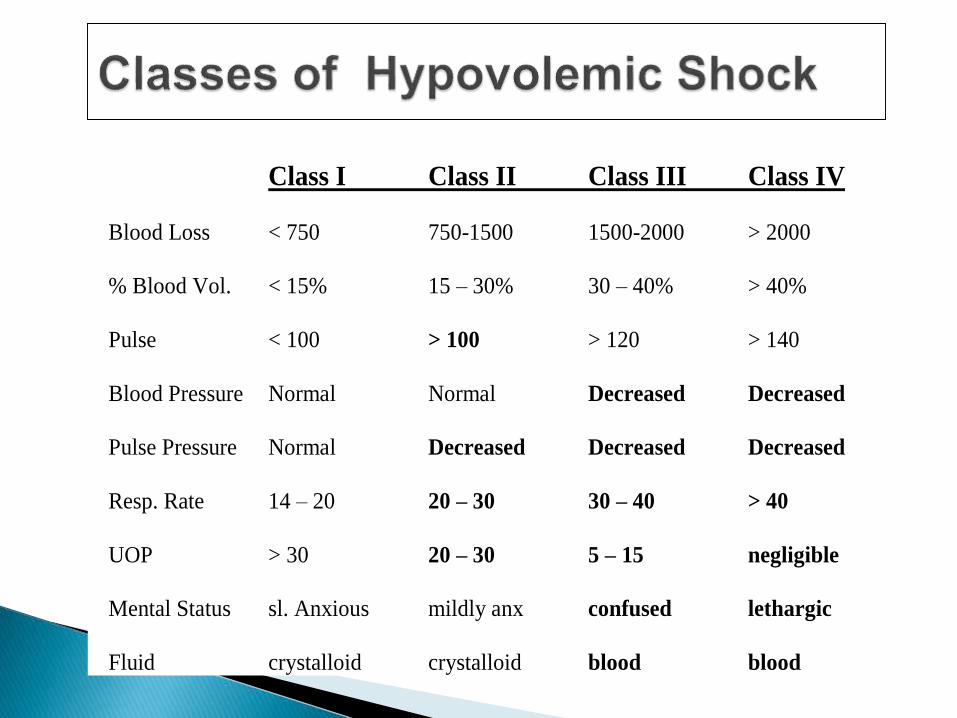
Class I Class II Class III Class IV
Blood Loss < 750 750-1500 1500-2000 > 2000
% Blood Vol. < 15% 15 – 30% 30 – 40% > 40%
Pulse < 100 > 100 > 120 > 140
Blood Pressure Normal Normal Decreased Decreased
Pulse Pressure Normal Decreased Decreased Decreased
Resp. Rate 14 – 20 20 – 30 30 – 40 > 40
UOP > 30 20 – 30 5 – 15 negligible
Mental Status sl. Anxious mildly anx confused lethargic
Fluid crystalloid crystalloid blood blood

Early◦ Increase HR◦ Decrease perfusion◦ Normal BP, decrease pulse pressure
Late◦ Sign increase HR◦ Sign decrease perfusion ◦ Decrease BP◦ End organ dysfunction


Pump failure/malfunction
(decreased contractility)

Myocardial◦ Infarction, contusion, myocarditis,
cardiomyopathy, pharmacologic, depressant factors
Mechanical◦ Valvular stenosis, regrurgitation
◦ Septal Defects
Arrhythmogenic
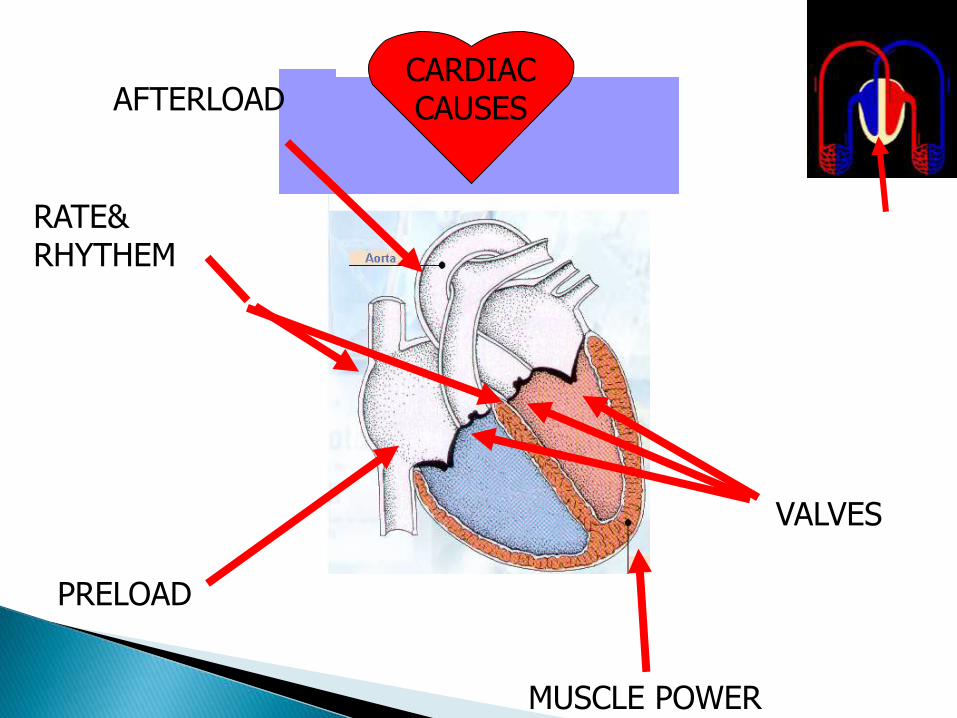
CARDIACCAUSESAFTERLOAD
PRELOAD
VALVES
MUSCLE POWER
RATE& RHYTHEM

Tachycardia
Tachypnea
Respiratory distress
Mental status change
Cool extremities
Poor perfusion
Signs of dehydration


Extrinsic Vascular Compression◦ tumors, fibrosis
Increased Intrathoracic Pressure◦ Tension pneumo; high autopeep in PPV
Flow obstruction◦ PE, Air embolism, tumors, Ao dissection, Ao
coarctation, acute pulmonary HTN, tamponade.

•Tension pneumothorax•Air trapped in pleural space with 1 way valve,
air/pressure builds up
•Mediastinum shifted impeding venous return
•Chest pain, SOB, decreased breath sounds
•No tests needed!
•Rx: Needle decompression, chest tube

•Cardiac tamponade•Blood in pericardial sac prevents venous return to
and contraction of heart
•Related to trauma, pericarditis, MI
•Beck’s triad: hypotension, muffled heart sounds, JVD
•Diagnosis: large heart CXR, echo
•Rx: Pericardiocentisis
•Pulmonary embolism•Virscow triad: hypercoaguable, venous injury,
venostasis
•Signs: Tachypnea, tachycardia, hypoxia
•Low risk: D-dimer
•Higher risk: CT chest or VQ scan
•Rx: Heparin, consider thrombolytics


SIRS-related As sepsis (infectious); pancreatitis; trauma; burns.
Anaphylactic/anaphylactoid
Spinal Trauma (low pulse, SVR low)
Toxic, pharmacologic (B-blockers overdose)
Endocrine (thyroid, adrenal crisis)

Abnormal vessel tone
(decreased afterload)

Vasodilitation Venous Pooling
Decreased Afterload
Maldistribution of regional blood flow
Neurogenic or Anaphylactic Shock
Diminished or absent sympathetic tone
Reduce peripheral vascular tone
Peripheral pooling of blood volume
Inadequate venous return
Decreased perfusion, acidosis, hypotension

•Anaphylaxis – a severe systemic hypersensitivity reaction characterized by multisystem involvement •IgE mediated
•Anaphylactoid reaction – clinically indistinguishable from anaphylaxis, do not require a sensitizing exposure•Not IgE mediated

•What are some symptoms of anaphylaxis?
• First- Pruritus, flushing, urticaria appear
•Next- Throat fullness, anxiety, chest tightness, shortness of breath and lightheadedness
•Finally- Altered mental status, respiratory distress and circulatory collapse

• Risk factors for fatal anaphylaxis • Poorly controlled asthma • Previous anaphylaxis
• Reoccurrence rates• 40-60% for insect stings• 20-40% for radiocontrast agents• 10-20% for penicillin
• Most common causes• Antibiotics• Insects• Food

• Mild, localized urticaria can progress to full anaphylaxis
• Symptoms usually begin within 60 minutes of exposure
• Faster the onset of symptoms = more severe reaction
• Biphasic phenomenon occurs in up to 20% of patients• Symptoms return 3-4 hours after initial reaction has cleared
• A “lump in my throat” and “hoarseness” heralds life-threatening laryngeal edema

•Clinical diagnosis
•Defined by airway compromise, hypotension, or involvement of cutaneous, respiratory, or GI systems
•Look for exposure to drug, food, or insect
•Labs have no role

•Occurs after acute spinal cord injury•Sympathetic outflow is disrupted leaving
unopposed vagal tone•Results in hypotension and bradycardia•Spinal shock- temporary loss of spinal
reflex activity below a total or near total spinal cord injury (not the same as neurogenic shock, the terms are not interchangeable)

•Loss of sympathetic tone results in warm and dry skin
•Shock usually lasts from 1 to 3 weeks
•Any injury above T1 can disrupt the entire sympathetic system•Higher injuries = worse paralysis

Terminology in Sepsis◦ Infection = response to micro organism
◦ Bacteremia = bug in blood
◦ Systemic Inflammatory Response Syndrome (SIRS)
T>38, <36
Increase HR
Increase RR, paCO2<32
WBC>12,000, <4,000, >10% bands

Terminology in Sepsis◦ Sepsis = SIRS (systemic inflammatory response
syndrome) as response to a known infection
◦ Severe sepsis = Sepsis + organ dysfunction
◦ Septic Shock = Sepsis + inadequate oxygen delivery
◦ Multiple Organ Dysfunction Syndrome (MODS) –organ dysfunction that requires intervention
Components of Septic shock◦ Decreased volume
◦ Decreased pump function
◦ Abnormal vessel tone

Therapy for Caridovascular Support
Preload Volume
Contractility Inotropes
Afterload Vasodilators

Etiologies
Inflammatory: too much, too little
Coagulation pathway: DIC-bleeding, pro-coagulant, microthombosis
Multiple organ system failure

Early – warm shock – similar to neurogenic shock
Late – Cold shock – similar to cardiogenic shock

Early Late
Heart rate Tachycardia Tachycardia/
bradycardia
Blood pressure Normal decreased
Peripheral
Perfusion
Warm/cool
Dec./inc. pulses
Cool
Dec. pulses

Early Late
End-organ: skin Dec. cap refill Very dec. cap
Refill
Brain Irritable, restless
Lethargic, unresponsive
Kidneys Oliguria Oliguria, anuria

HYPOXICFAILURE
COMPENSATORY
POST CAP.VASO-CON.
STRESS
PRE&POST CAP.V.CON.
PRECAPILLARY SHUNT
FAILURE
OPEN PRECAP
LEAKAGE
RECOVARY
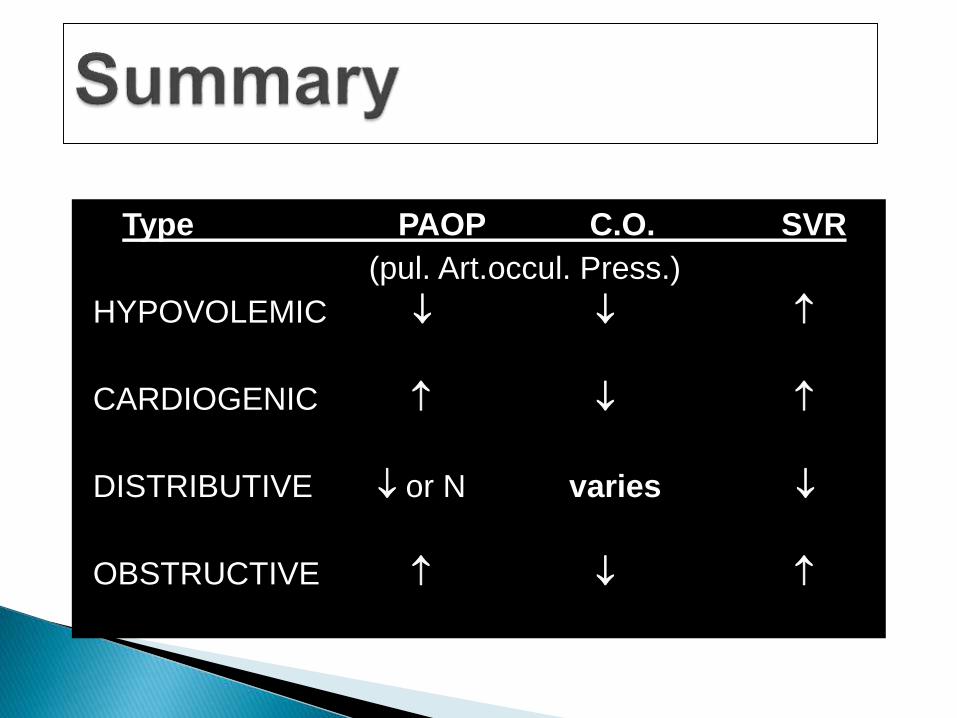
Type PAOP C.O. SVR
(pul. Art.occul. Press.)
HYPOVOLEMIC
CARDIOGENIC
DISTRIBUTIVE or N varies
OBSTRUCTIVE
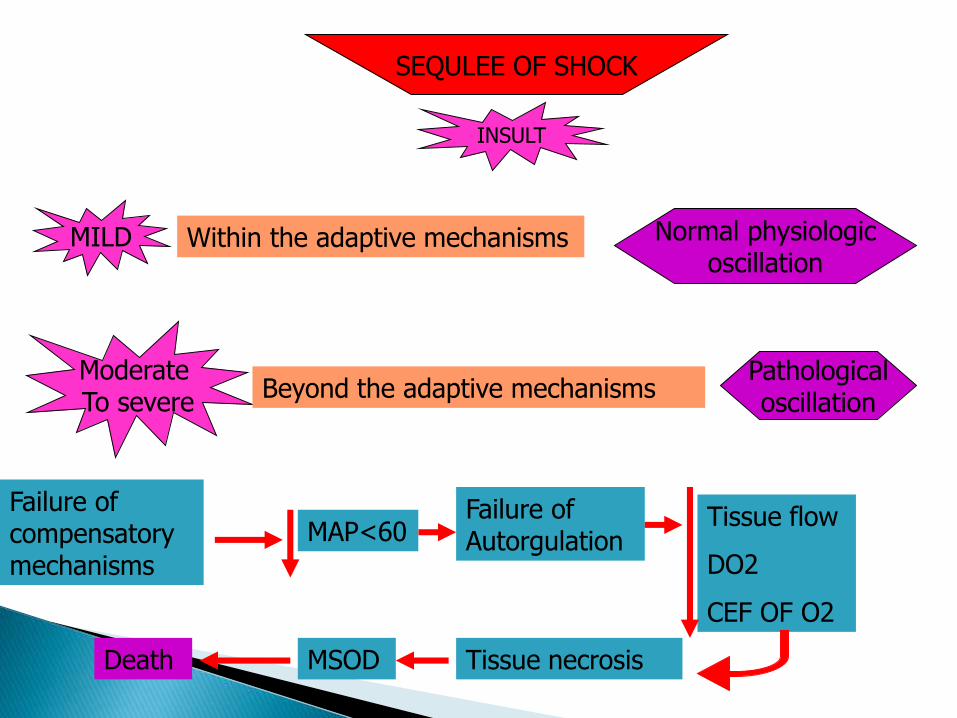
SEQULEE OF SHOCK
INSULT
MILD Within the adaptive mechanisms
Moderate To severe
Beyond the adaptive mechanisms
Normal physiologicoscillation
Pathologicaloscillation
Failure of compensatory mechanisms
MAP<60Failure of Autorgulation
Tissue flow
DO2
CEF OF O2
Tissue necrosisMSODDeath


THANK YOU