should we use different induction regimens for …...should we use different induction regimens for...
TRANSCRIPT

Should we use different induction regimens for transplant eligible and transplant ineligible patients?
Jonathan L. Kaufman, MDAssociate ProfessorWinship Cancer Institute of Emory UniversityMarch 8th 2018

Should we use different regimens?
Yes
And No
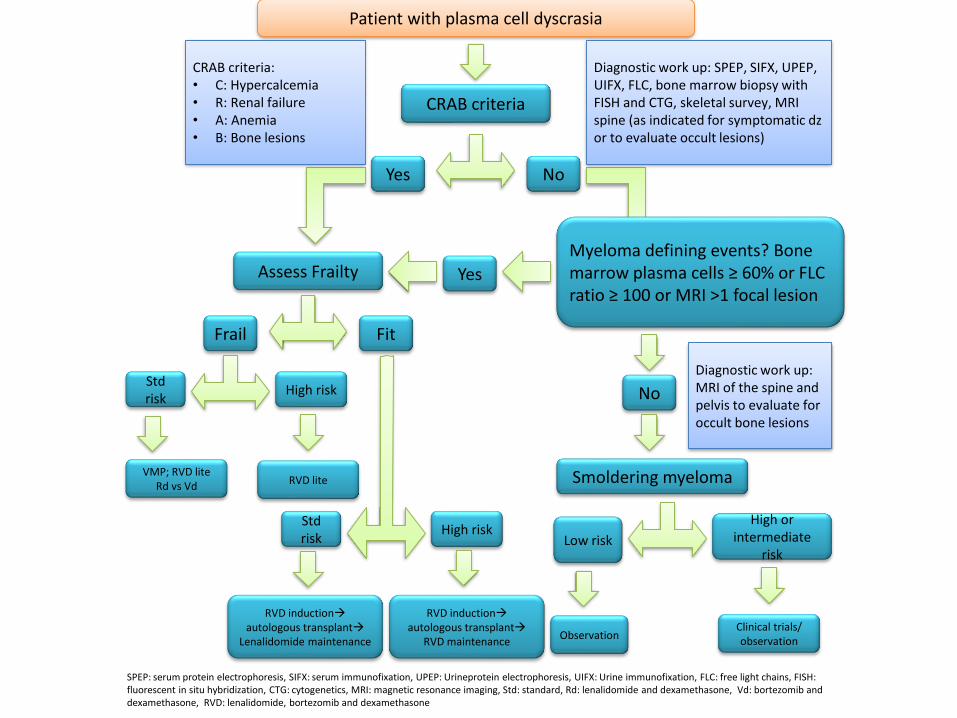
CRAB criteria
Patient with plasma cell dyscrasia
CRAB criteria
Yes No
Myeloma defining events? Bone marrow plasma cells ≥ 60% or FLC ratio ≥ 100 or MRI >1 focal lesion
Assess Frailty Yes
Diagnostic work up: SPEP, SIFX, UPEP, UIFX, FLC, bone marrow biopsy with FISH and CTG, skeletal survey, MRI spine (as indicated for symptomatic dzor to evaluate occult lesions)
CRAB criteria:• C: Hypercalcemia• R: Renal failure• A: Anemia• B: Bone lesions
Frail Fit
Stdrisk
High risk
VMP; RVD liteRd vs Vd RVD lite
Low risk
High orintermediate
risk
ObservationClinical trials/observation
No
Smoldering myeloma
Stdrisk
High risk
RVD inductionautologous transplant
RVD maintenance
RVD inductionautologous transplant
Lenalidomide maintenance
Diagnostic work up: MRI of the spine and pelvis to evaluate for occult bone lesions
SPEP: serum protein electrophoresis, SIFX: serum immunofixation, UPEP: Urineprotein electrophoresis, UIFX: Urine immunofixation, FLC: free light chains, FISH: fluorescent in situ hybridization, CTG: cytogenetics, MRI: magnetic resonance imaging, Std: standard, Rd: lenalidomide and dexamethasone, Vd: bortezomib and dexamethasone, RVD: lenalidomide, bortezomib and dexamethasone
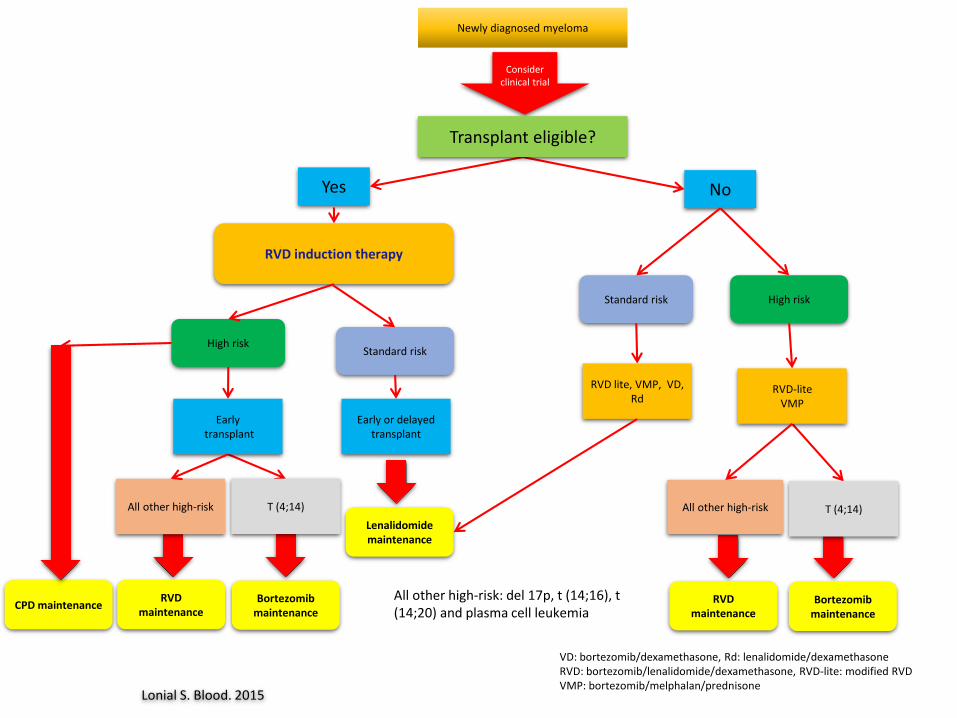
Consider clinical trial
Newly diagnosed myeloma
Yes No
High riskStandard risk
Transplant eligible?
Lenalidomidemaintenance
Early or delayed transplant
RVD induction therapy
Lonial S. Blood. 2015
T (4;14)
Earlytransplant
All other high-risk
Bortezomibmaintenance
RVD maintenance
VD: bortezomib/dexamethasone, Rd: lenalidomide/dexamethasone RVD: bortezomib/lenalidomide/dexamethasone, RVD-lite: modified RVDVMP: bortezomib/melphalan/prednisone
Standard risk High risk
RVD-liteVMP
T (4;14)
RVD lite, VMP, VD, Rd
All other high-risk
Bortezomibmaintenance
RVD maintenance
All other high-risk: del 17p, t (14;16), t (14;20) and plasma cell leukemia
CPD maintenance
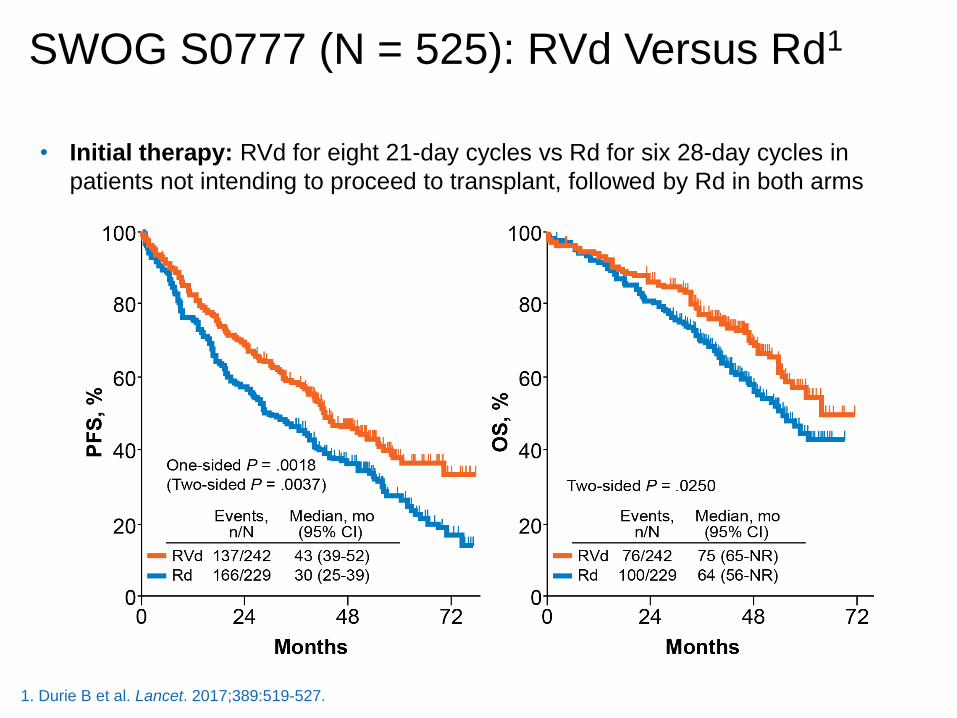
SWOG S0777 (N = 525): RVd Versus Rd1
• Initial therapy: RVd for eight 21-day cycles vs Rd for six 28-day cycles in
patients not intending to proceed to transplant, followed by Rd in both arms
1. Durie B et al. Lancet. 2017;389:519-527.

IFM2009: RVd Alone Vs RVd + ASCT1
RVd 1Lenalidomide
12 mo
RVd 2-3 → PBSC collection → RVd 4-8
RVd 2-3 → PBSC collection → ASCT → RVd 4-5
1. Attal M et al. N Engl J Med. 2017;376:1311-1320.

IFM2009: Response1
OutcomeRVd-Alone
Group (n = 350)
Transplantation Group
(n = 350)
AdjustedPa
Best response during study, n (%)
CR
VGPR
PR
SD
169 (48)
101 (29)
70 (20)
10 (3)
205 (59)
102 (29)
37 (11)
6 (2)
.02
CR, n (%) 169 (48) 205 (59) .003
CR or VGPR, n (%) 270 (77) 307 (88) .001
Minimal disease not detected during study, n/total n with CR or VGPR (%)b 171/265 (65) 220/278 (79) < .001
a P values were adjusted for multiplicity with the use of the Holm procedure to control the family-wise error rate at 0.05. b MRD was detected by means of flow cytometry. As a result of decisions made by the patient or the investigator, 5 patients
in the RVd-alone group and 29 patients in the transplantation group were not tested.
1. Attal M et al. N Engl J Med. 2017;376:1311-1320.

There is a 26% reduction in risk of death, representing an estimated 2.5-year increase in median survivala
Lenalidomide Maintenance: Meta-Analysis1
Median OS(95% CI), mo
HR (95% CI)P
Len maintenance
NR(NR-NR) 0.74 (0.62-0.89)
.001Placebo/observation
86.0(79.8-96.0)
a Log-rank test and Cox model stratified by study to assess impact of Len maintenance on OS. Median for len
treatment arm was extrapolated to be 115 mo based on median of control arm and HR (median, 86 mo; HR = 0.74).
1. Attal M et al. 2016 American Society of Clinical Oncology Annual Meeting (ASCO 2016). Abstract 8001.
Len maintenance 605 578 555 509 474 431 385 282 200 95 20 1 0
Placebo/observation 604 569 542 505 458 425 350 271 174 71 10 0
No. at Risk
0.2
1.0
0.8
0.6
0.4
0
OS
Pro
bab
ilit
y
0 10 20 30 40 50 60 70 80 90 100 110 120
Months
7-y OS
62%
50%

Lenalidomide, bortezomib, and dexamethasone (RVD) as induction therapy in newly diagnosed multiple myeloma
Nisha Joseph ASH 2017
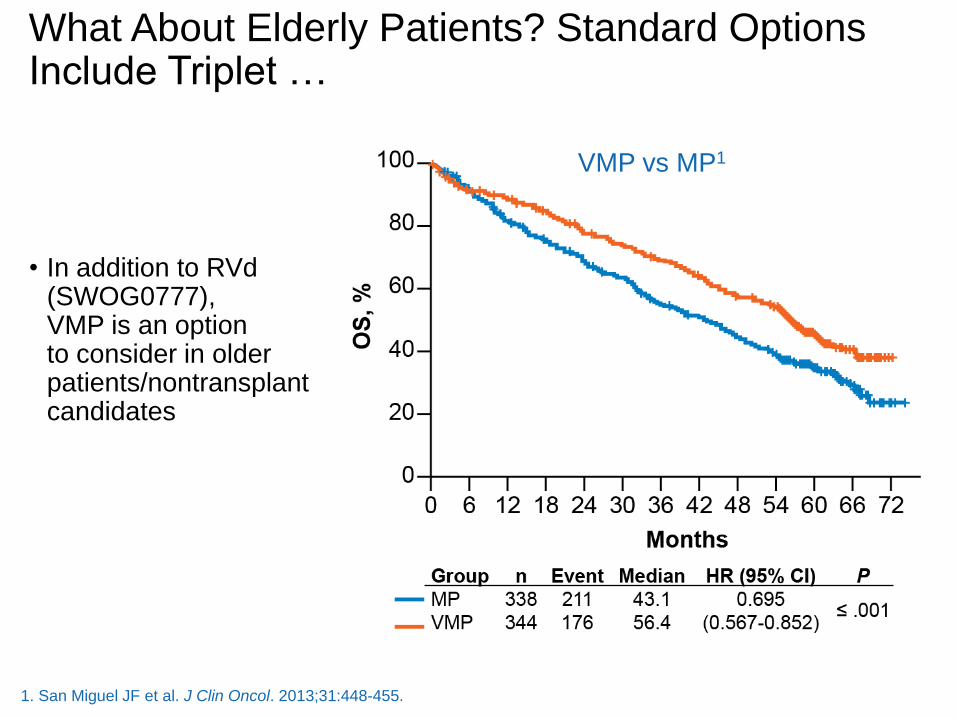
• In addition to RVd (SWOG0777), VMP is an option to consider in older patients/nontransplant candidates
What About Elderly Patients? Standard Options Include Triplet …
1. San Miguel JF et al. J Clin Oncol. 2013;31:448-455.
VMP vs MP1
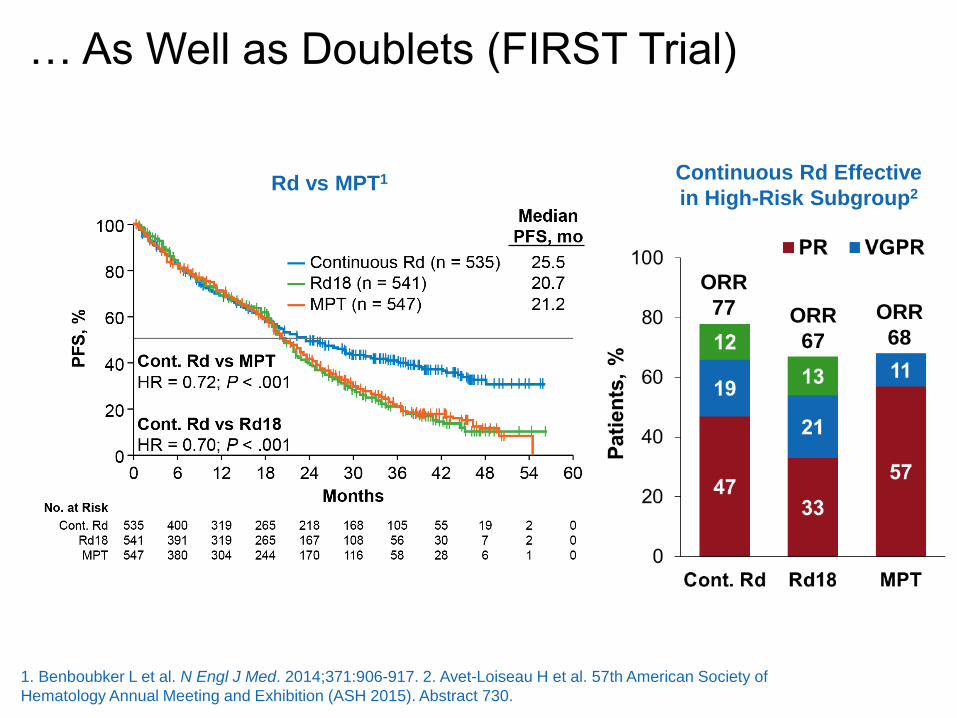
… As Well as Doublets (FIRST Trial)
Continuous Rd Effective
in High-Risk Subgroup2Rd vs MPT1
1. Benboubker L et al. N Engl J Med. 2014;371:906-917. 2. Avet-Loiseau H et al. 57th American Society of
Hematology Annual Meeting and Exhibition (ASH 2015). Abstract 730.
ORR
77 ORR
67
ORR
68

35-Day CycleLenalidomide •15 mg/d on days 1-21
Bortezomib•1.3 mg/m2 once weekly subQ on days 1, 8, 15, and 22
Dexamethasone •20 mg on days 1, 2, 8, 9, 15, 16, 22, and 23 for patients aged ≤75 y, and days 1, 8, 15, and 22 for patients aged >75 y
How to Modify Upfront Therapy: RVd-Lite1
Response After 4 Cycles (N = 30) n (%)
ORR (≥PR) 27 (90.0)
CR 5 (16.7)
VGPR 11 (36.7)
PR 11 (36.7)
SD 3 (10.0)
≥VGPR 16 (53.3)
1. O'Donnell EK et al. ASH 2014. Abstract 4217.
1. Demo SD, et al. Cancer Res. 2007; 67:6383-6391. 2. Kirk CJ, et al, Blood.
2008;112:abstract 2765. 3. Siegel DS, et al. Blood 2012:120:2817-2825.
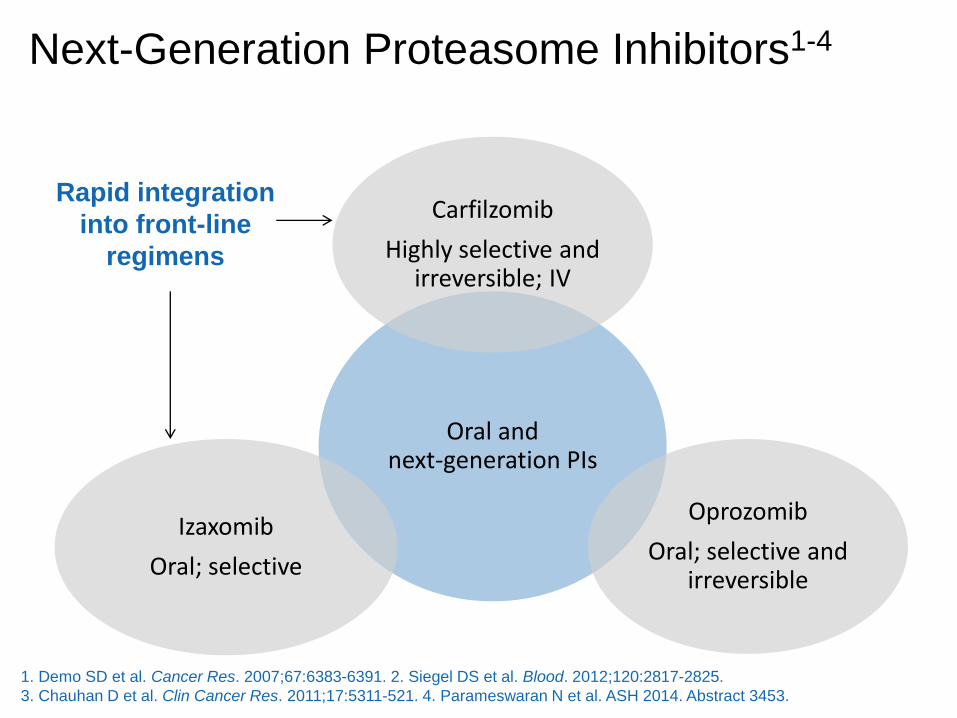
Next-Generation Proteasome Inhibitors1-4
Oral and next-generation PIs
Carfilzomib
Highly selective and irreversible; IV
Oprozomib
Oral; selective and irreversible
Izaxomib
Oral; selective
Rapid integration
into front-line
regimens
1. Demo SD et al. Cancer Res. 2007;67:6383-6391. 2. Siegel DS et al. Blood. 2012;120:2817-2825.
3. Chauhan D et al. Clin Cancer Res. 2011;17:5311-521. 4. Parameswaran N et al. ASH 2014. Abstract 3453.

Extended Therapy With KRd in Newly Diagnosed Myeloma1
Newly diagnosed MM, ASCT
eligible
KRd
(4 cycles)
ASCT
No ASCT
KRd
(4 cycles)
KRd
(10 cycles)
MRD MRD MRD
• KRd plus ASCT shows high rates of deep responses in newly diagnosed MM, with
higher rates of sCR compared with KRd without ASCT
• High rates of MRD-negative disease, up to 97% by MFC and 71% by NGS, which
appear higher than with KRd without ASCT
• Deep responses with KRd plus ASCT are associated with high rates of PFS and OS
• KRd regimen is generally well tolerated, and ASCT does not appear to add significant
toxicity
• Randomized studies needed to confirm results
Induction Consolidation Maintenance
1. Zimmerman T et al. ASH 2016. Abstract 675.
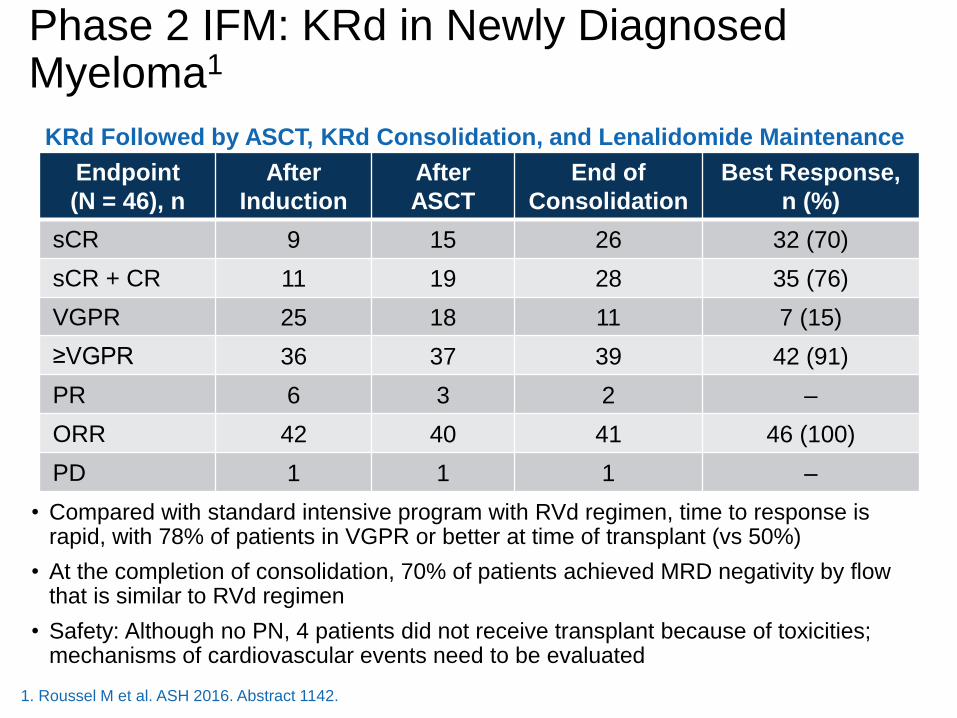
• Compared with standard intensive program with RVd regimen, time to response is rapid, with 78% of patients in VGPR or better at time of transplant (vs 50%)
• At the completion of consolidation, 70% of patients achieved MRD negativity by flow that is similar to RVd regimen
• Safety: Although no PN, 4 patients did not receive transplant because of toxicities; mechanisms of cardiovascular events need to be evaluated
Phase 2 IFM: KRd in Newly Diagnosed Myeloma1
Endpoint
(N = 46), n
After
Induction
After
ASCT
End of
Consolidation
Best Response,
n (%)
sCR 9 15 26 32 (70)
sCR + CR 11 19 28 35 (76)
VGPR 25 18 11 7 (15)
≥VGPR 36 37 39 42 (91)
PR 6 3 2 –
ORR 42 40 41 46 (100)
PD 1 1 1 –
KRd Followed by ASCT, KRd Consolidation, and Lenalidomide Maintenance
1. Roussel M et al. ASH 2016. Abstract 1142.
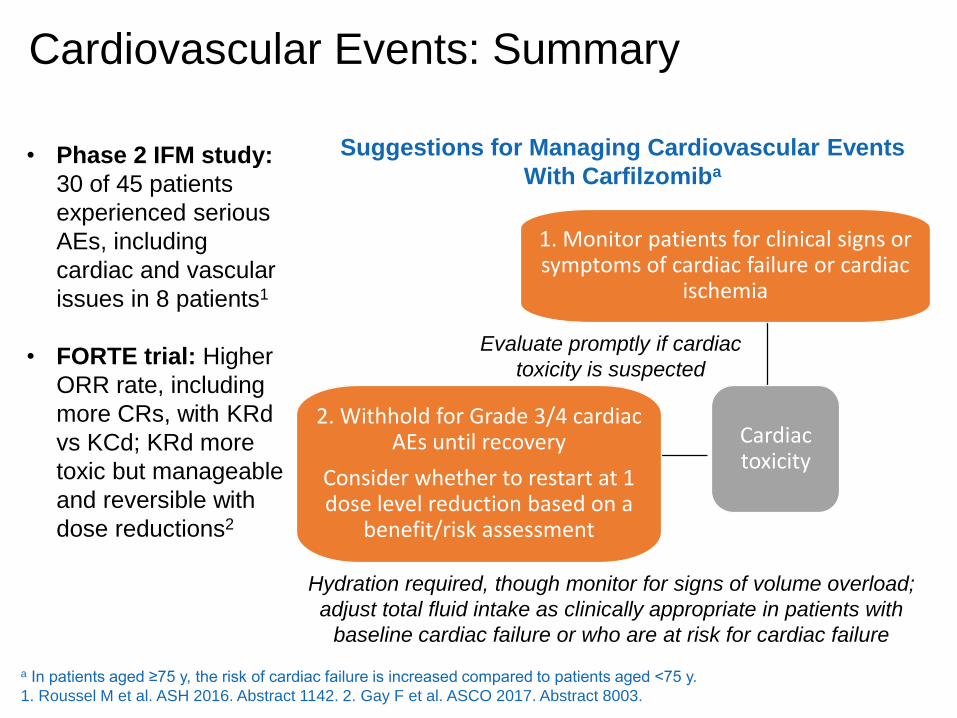
Cardiovascular Events: Summary
• Phase 2 IFM study:
30 of 45 patients
experienced serious
AEs, including
cardiac and vascular
issues in 8 patients1
• FORTE trial: Higher
ORR rate, including
more CRs, with KRd
vs KCd; KRd more
toxic but manageable
and reversible with
dose reductions2
Cardiac toxicity
1. Monitor patients for clinical signs or symptoms of cardiac failure or cardiac
ischemia
2. Withhold for Grade 3/4 cardiac AEs until recovery
Consider whether to restart at 1 dose level reduction based on a
benefit/risk assessment
Evaluate promptly if cardiac
toxicity is suspected
Suggestions for Managing Cardiovascular Events
With Carfilzomiba
Hydration required, though monitor for signs of volume overload;
adjust total fluid intake as clinically appropriate in patients with
baseline cardiac failure or who are at risk for cardiac failure
a In patients aged ≥75 y, the risk of cardiac failure is increased compared to patients aged ˂75 y.
1. Roussel M et al. ASH 2016. Abstract 1142. 2. Gay F et al. ASCO 2017. Abstract 8003.

IRd in Newly Diagnosed Myeloma1
CR plus
stringent
response
VGPR
PR
100
80
60
40
20
0Cycle 3
(85%)
90
70
50
30
10
Patients
, %
Cycle 6
(90%)
Cycle 9
(90%)
Cycle 12
(90%)
Time of Response Assessment
4842
3228
35
27
33
25
25
23
33
4
1. Kumar SK et al. Lancet Oncol. 2014;15:1503-1512.
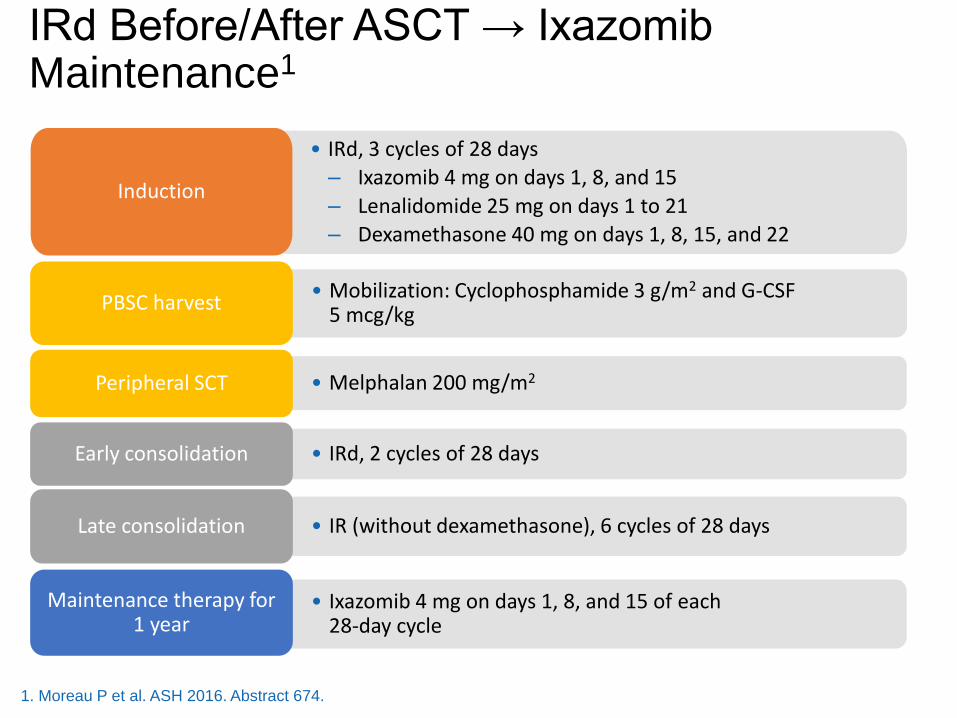
IRd Before/After ASCT → Ixazomib Maintenance1
• IRd, 3 cycles of 28 days
– Ixazomib 4 mg on days 1, 8, and 15
– Lenalidomide 25 mg on days 1 to 21
– Dexamethasone 40 mg on days 1, 8, 15, and 22
Induction
• Mobilization: Cyclophosphamide 3 g/m2 and G-CSF 5 mcg/kg
PBSC harvest
• Melphalan 200 mg/m2Peripheral SCT
• IRd, 2 cycles of 28 daysEarly consolidation
• IR (without dexamethasone), 6 cycles of 28 daysLate consolidation
• Ixazomib 4 mg on days 1, 8, and 15 of each 28-day cycle
Maintenance therapy for 1 year
1. Moreau P et al. ASH 2016. Abstract 674.

IRd Induction/Consolidation → IxazomibMaintenance
Response, %Post-Induction
(n = 42)
Post-ASCT
(n = 37)
Post–Early
Consolidation
(n = 37)
Post–Late
Consolidation
(n = 34)
sCR 2.4 9.5 23.8 38.2
CR 9.5 7.1 4.8 5.9
VGPR 23.8 45.2 38.1 32.4
PR 42.9 21.4 19 17.6
SD 14.3 4.8 0 0
PD 4.8 0 2.4 5.9
NE 2.4 11.9 11.9 0
>PR 81 83.3 85.7 94.1
>VGPR 38.1 61.9 66.7 76.5
>CR 11.9 16.7 28.6 44.1
1. Moreau P et al. ASH 2016. Abstract 674.
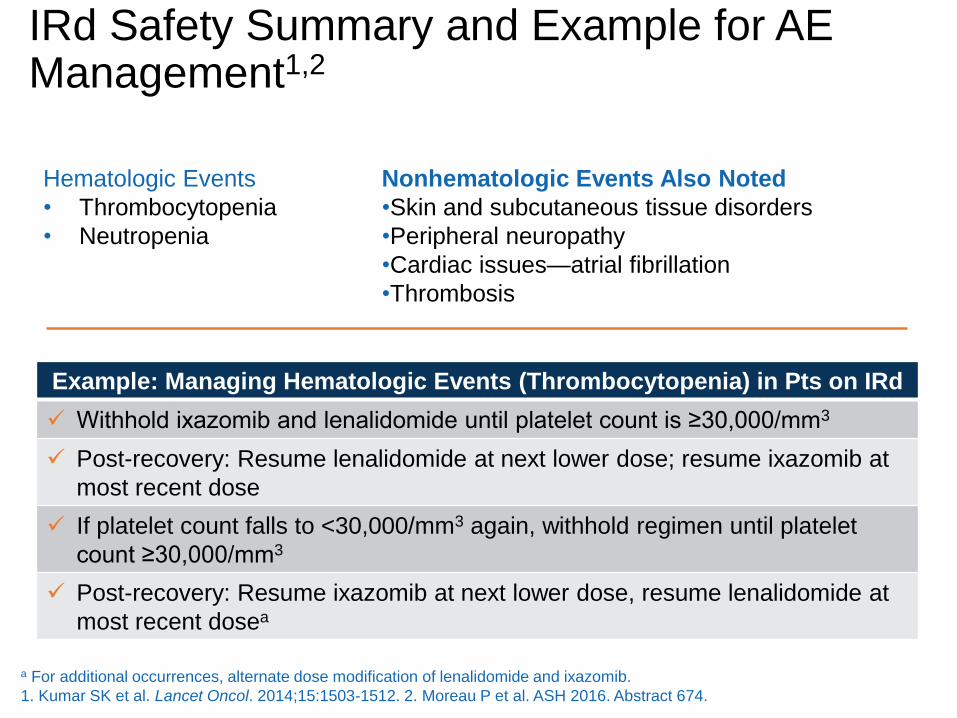
IRd Safety Summary and Example for AE Management1,2
Hematologic Events
• Thrombocytopenia
• Neutropenia
Nonhematologic Events Also Noted
•Skin and subcutaneous tissue disorders
•Peripheral neuropathy
•Cardiac issues—atrial fibrillation
•Thrombosis
Example: Managing Hematologic Events (Thrombocytopenia) in Pts on IRd
✓ Withhold ixazomib and lenalidomide until platelet count is ≥30,000/mm3
✓ Post-recovery: Resume lenalidomide at next lower dose; resume ixazomib at
most recent dose
✓ If platelet count falls to <30,000/mm3 again, withhold regimen until platelet
count ≥30,000/mm3
✓ Post-recovery: Resume ixazomib at next lower dose, resume lenalidomide at
most recent dosea
a For additional occurrences, alternate dose modification of lenalidomide and ixazomib.
1. Kumar SK et al. Lancet Oncol. 2014;15:1503-1512. 2. Moreau P et al. ASH 2016. Abstract 674.
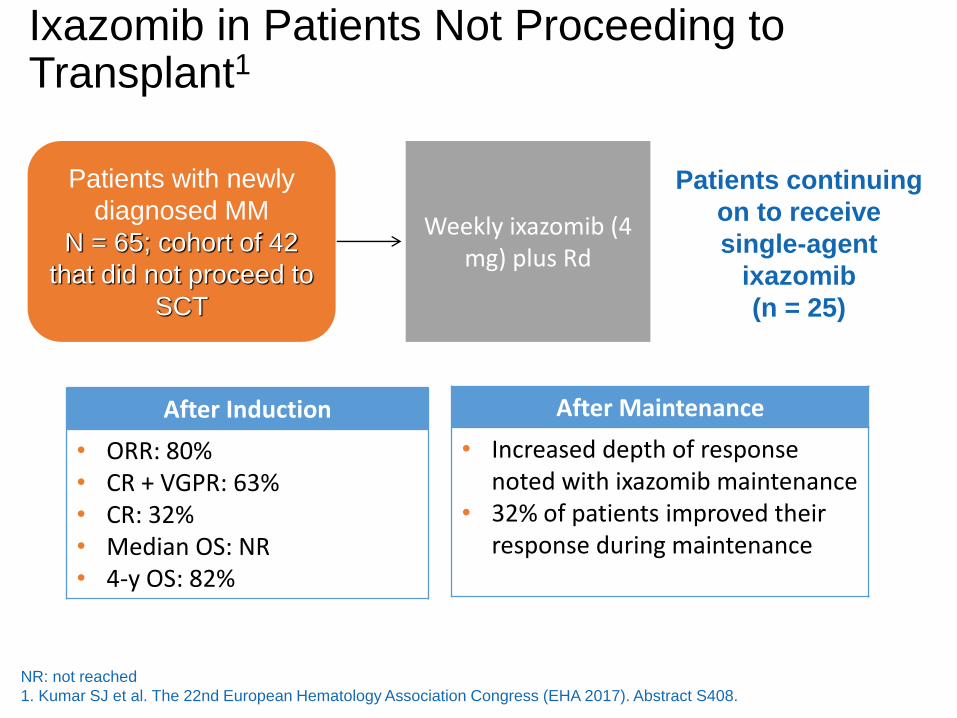
Ixazomib in Patients Not Proceeding to Transplant1
Patients with newly
diagnosed MM
N = 65; cohort of 42
that did not proceed to
SCT
Weekly ixazomib (4 mg) plus Rd
Patients continuing
on to receive
single-agent
ixazomib
(n = 25)
After Induction
• ORR: 80%• CR + VGPR: 63%• CR: 32%• Median OS: NR• 4-y OS: 82%
After Maintenance
• Increased depth of response noted with ixazomib maintenance
• 32% of patients improved their response during maintenance
NR: not reached
1. Kumar SJ et al. The 22nd European Hematology Association Congress (EHA 2017). Abstract S408.

Efficacy of Antibody Therapy in Newly Diagnosed Myeloma: Daratumumab Regimens in MMY10011,2
0
1
2
3
4
5
6
VD +DARA(n = 6)
VMP +DARA (n
= 6)
VTD +DARA (n
= 6)
POM-D +DARA (n
= 6)
Pati
en
ts,
n
PD
MR
PR
VGPR
sCR
Daratumumab-KRd in
Newly Diagnosed MM
12-mo PFS 94%
1. Mateos MV et al. ASH 2014. Abstract 176. 2. Jakubowiak A et al. ASCO 2017. Abstract 8000.
Best Response
Vd + Dara
(n = 6)
VMP + Dara
(n = 6)
VTd +Dara
(n = 6)
Pom/Dex+ Dara (n = 6)
ORR was 100% in newly diagnosed group, 50% in the relapsed group

• Triplets preferred: RVd, VCd, VMP; IRd, all oral regimen
• Doublets only in frail patients: Rd or Vd at reduced doses
Transplant Candidates
Transplant Ineligible
• Triplets preferred: RVd or VCd; KRd if neuropathy
• Doublets: Rarely used (ie, Vd to improve renal dysfunction, then
add lenalidomide)
• Maintenance: Lenalidomide in standard-risk patients; bortezomib
or RV in high-risk patients
Summary of Initial Therapy for Newly Diagnosed Myeloma

Efficacy of Antibody Therapy in Newly Diagnosed Myeloma: Daratumumab Regimens in MMY10011,2
0
1
2
3
4
5
6
VD +DARA(n = 6)
VMP +DARA (n
= 6)
VTD +DARA (n
= 6)
POM-D +DARA (n
= 6)
Pati
en
ts,
n
PD
MR
PR
VGPR
sCR
Daratumumab-KRd in
Newly Diagnosed MM
12-mo PFS 94%
1. Mateos MV et al. ASH 2014. Abstract 176. 2. Jakubowiak A et al. ASCO 2017. Abstract 8000.
Best Response
Vd + Dara
(n = 6)
VMP + Dara
(n = 6)
VTd +Dara
(n = 6)
Pom/Dex+ Dara (n = 6)
ORR was 100% in newly diagnosed group, 50% in the relapsed group

25
ECOG, Eastern Cooperative Oncology Group; ISS, International Staging System; EU, European Union; SC, subcutaneously; PO, oral ly;D, daratumumab; IV, intravenously; PD, progressive disease; PFS, progression-free survival; ORR, overall response rate; VGPR, very good partial
response; CR, complete response; MRD, minimal residual disease; NGS, next-generation sequencing; OS, overall survival. a8-month PFS improvement over 21-month median PFS of VMP.
ALCYONE Study Design
Key eligibility
criteria:
• Transplant-
ineligible
NDMM
• ECOG 0-2
• Creatinine
clearance
≥40 mL/min
• No peripheral
neuropathy
grade ≥2
Stratification factors
• ISS (I vs II vs III)
• Region (EU vs other)
• Age (<75 vs ≥75 years)
1:1
Ran
dom
iza
tion (
N =
70
6)
D-VMP × 9 cycles (n = 350)
Daratumumab: 16 mg/kg IV
Cycle 1: once weekly
Cycles 2-9: every 3 weeks
+
Same VMP schedule
Follow-up
for PD
and
survival
Primary endpoint:
• PFS
Secondary endpoints:
• ORR
• ≥VGPR rate
• ≥CR rate
• MRD (NGS; 10–5)
• OS
• Safety
VMP × 9 cycles (n = 356)
Bortezomib: 1.3 mg/m2 SC
Cycle 1: twice weekly
Cycles 2-9: once weekly
Melphalan: 9 mg/m2 PO on Days 1-4
Prednisone: 60 mg/m2 PO on Days 1-4
DCycles 10+
16 mg/kg IV
Every
4 weeks:
until PD
Statistical analyses
• 360 PFS events: 85% power for
8-month PFS improvementa
• Interim analysis: ~216 PFS events
• Cycles 1-9: 6-week cycles
• Cycles 10+: 4-week cycles
26
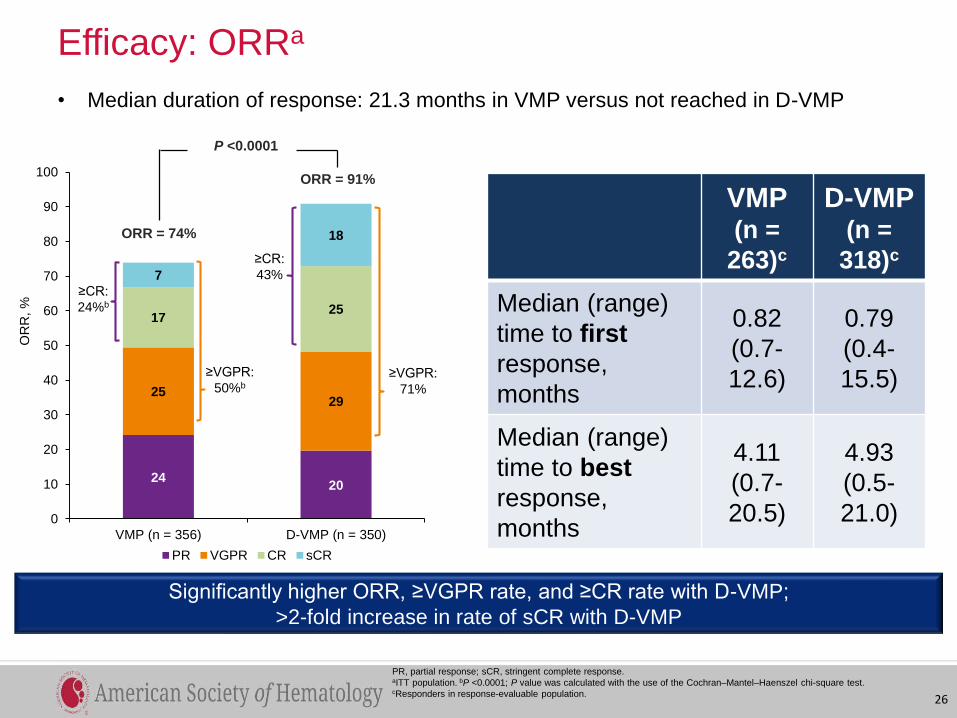
Efficacy: ORRa
PR, partial response; sCR, stringent complete response.aITT population. bP <0.0001; P value was calculated with the use of the Cochran–Mantel–Haenszel chi-square test. cResponders in response-evaluable population.
• Median duration of response: 21.3 months in VMP versus not reached in D-VMP
Significantly higher ORR, ≥VGPR rate, and ≥CR rate with D-VMP;
>2-fold increase in rate of sCR with D-VMP
VMP(n =
263)c
D-VMP(n =
318)c
Median (range)
time to first
response,
months
0.82
(0.7-
12.6)
0.79
(0.4-
15.5)
Median (range)
time to best
response,
months
4.11
(0.7-
20.5)
4.93
(0.5-
21.0)
2420
2529
1725
7
18
0
10
20
30
40
50
60
70
80
90
100
VMP (n = 356) D-VMP (n = 350)
OR
R, %
PR VGPR CR sCR
P <0.0001
ORR = 74%
ORR = 91%
≥CR:
24%b
≥VGPR:
50%b
≥CR:
43%
≥VGPR:
71%

Efficacy: PFS
50% reduction in the risk of progression or death in patients receiving D-VMP
HR, hazard ratio; CI, confidence interval.aKaplan-Meier estimate.
• Median (range) follow-up: 16.5 (0.1-28.1) months
27
VMP
Median: 18.1 months
D-VMP
Median: not reached
% s
urv
ivin
g w
ith
ou
t p
rogre
ssio
n
0
20
40
60
80
0 3 6 9 12 15 18 27
Months
356
350
303
322
276
312
261
298
231
285
127
179
61
93
0
0
2
10
No. at risk
VMP
D-VMP
21 24
18
35
100
12-month PFSa 18-month PFSa
HR, 0.50
(95% CI, 0.38-0.65; P <0.0001)
87%
72%
76%
50%
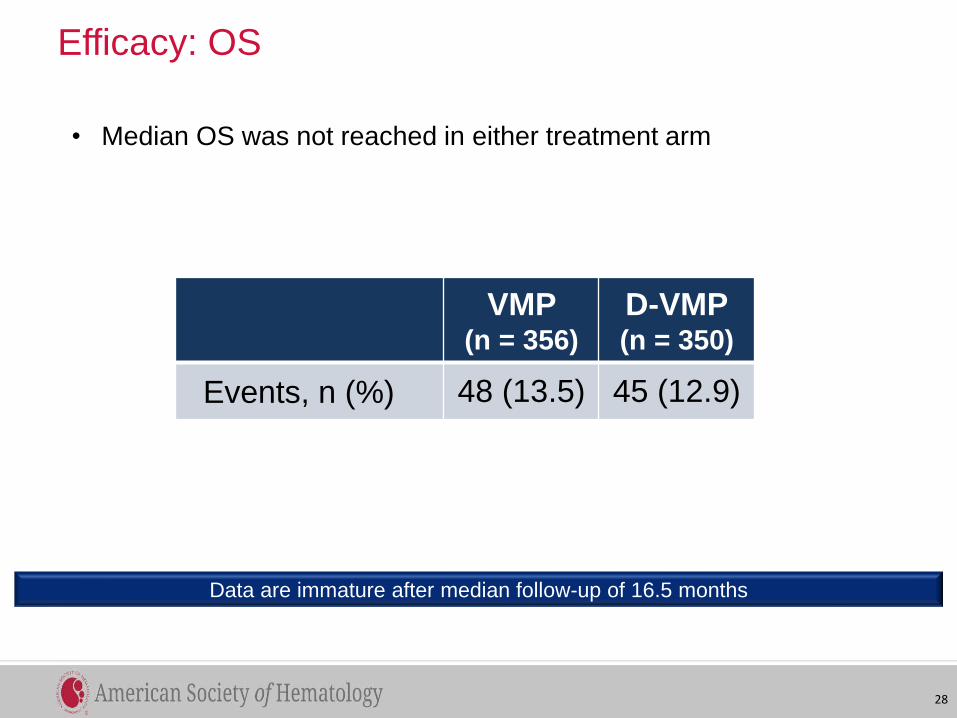
Efficacy: OS
VMP (n = 356)
D-VMP(n = 350)
Events, n (%) 48 (13.5) 45 (12.9)
• Median OS was not reached in either treatment arm
28
Data are immature after median follow-up of 16.5 months

Safety: Most Common TEAEsa
TEAE, treatment-emergent adverse event.aAny grade TEAEs in ≥20% of patients and grade 3 or 4 TEAEs in ≥10% of patients in either treatment group.
VMP (n = 354) D-VMP (n = 346)
Any
Grade
Grade 3
or 4
Any
Grade
Grade 3
or 4
Hematologic, n (%)
Neutropenia 186 (53) 137 (39) 172 (50) 138 (40)
Thrombocytopenia 190 (54) 133 (38) 169 (49) 119 (34)
Anemia 133 (38) 70 (20) 97 (28) 55 (16)
Nonhematologic, n (%)
Peripheral sensory
neuropathy121 (34) 14 (4) 98 (28) 5 (1)
Upper respiratory tract
infection49 (14) 5 (1) 91 (26) 7 (2)
Diarrhea 87 (25) 11 (3) 82 (24) 9 (3)
Pyrexia 74 (21) 2 (1) 80 (23) 2 (1)
Nausea 76 (22) 4 (1) 72 (21) 3 (1)
Pneumonia 17 (5) 14 (4) 53 (15) 39 (11)
• 1 patient in each
arm discontinued
treatment due to
pneumonia
• 1.4% and 0.9% of
patients receiving
VMP and D-VMP,
respectively,
discontinued
treatment due to
infection
29
VMP (n = 354) D-VMP (n = 346)
Deaths due to TEAEs, n
(%)19 (5) 19 (6)

Safety: IRRs
IRR, infusion-related reaction.
• Most IRRs occurred during the first infusion
• 5 (1.4%) patients discontinued daratumumab due to IRRs
• Montelukast was allowed as additional premedication and was used
in <5% of patients
D-VMP (n = 346)
All Grades Grade 3 Grade 4 Grade 5
Patients with IRRs,
n (%)96 (28) 15 (4) 2 (1) 0
30

Should we use different regimens?
Yes
Use best available agents upfront
Treat to progression
And No
Doses need modification
Not all patients can tolerate triplet regimens
Will Monoclonal antibodies change treatment for newly diagnosed patients?