sigmoid myotomy
TRANSCRIPT

REILLY: SIGMOID MYOTOMY 859
HEALEY, J. E., jun. (I954), J. int. Coll. Surg., 22,
KEEN, W. W. (1892), Boston med. surg. J., 126, 405. _ _ (1899), Ann. Surg., 30, 267. LANGENBUSCH, C. (1888), Berl. klin. Wschr., 25, 37. LONGMIRE, W. P., jun. (1965), Ann. Surg., 161, I. _ _ and LIPPMAN, H. N. (1956), Surg. Clins N. Am.,
_ - and SANFORD, M. C. (1948), Surgery, St Louis, 24,
LORTAT-JACOB, J. L., and ROBERT, H. G. ( I~sz) , Presse
542.
36, 849.
264.
nze‘d., 60, 549. MCDERMOTT, W. V., jun., GREENBURGER, N. J., ISSEL-
BACHER, K. L., and WEBER, A. L. (1963), Surgery, St Louis, 54, 56.
MADDING, G. F., and KENNEDY, P. A. (1965), Trauma to the Liver, p. 88. Philadelphia and London: Saunders.
MAKI, T., SATO, T., YAMAGUCHI, I., and SATO, T. (1964), Arcks Surg., Chicago, 88, 260.
PACK, G. T. (1962), Tumors of the Gastrointestinal Tract, Pancreas. Biliarv Svstem and Liver. New York: Hoeber.
PETTINARI,’V. (1G5); Congr. int. SOC. Surg., 16, 1169. SHUMACKER, H. B., jun. (1942), Surgery, St Louis, I I, 209. STEWART, H. L. (1965), in Primary Hepatoma (ed.
BURDETTE, W. J.), p. 31. Salt Lake City: University of Utah Press.
TUNG, TON THAT (1962), Ckirurgie d’Exdrise du Foie. Hanoi : Editions en Langues Estrangkres.
WENDELL, W. ( I ~ I I ) , Arch. klin. ckir., 95, 887.
THE TREATMENT OF PARALYTIC ILEUS BY B. N. CATCHPOLE
ST. BARTHOLOMEW’S HOSPITAI., LONDON
[This is an abstract of the paper read at the meeting.] nerves pharmacologically. However, the stomach and colon frequently require additional motor
THE development of so-called paralytic ileus following stimulation. Therefore, by combining the use of a surgery still causes morbidity and occasional mortality. sympathetic blocking agent and a parasympatho-
Experimental work has indicated that, far from mimetic drug, motility can be restored with resulting being paralysed, the small intestine is generally passage of flatus and defaecation. inhibited by sympathetic overactivity and that gut The results in a series of patients with ileus treated motility may be restored by blocking the sympathetic by this means were presented.
SIGMOID MYOTOMY BY MICHAEL REILLY
PLYMOUTH GENERAL HOSPITAL, DBVONPORT
UNTIL recent years diverticulitis of the colon was considered, as its name implies, primarily as a disease of diverticula. Little attention was paid by surgeons to the reasons why diverticula should develop and, more especially, why they should develop so common- ly and profusely in the sigmoid colon. The thicken- ing in the colon in areas affected by diverticular disease was attributed to inflammation and fibrosis, and if the condition was sufficiently far advanced to cause obstruction the usual method of treatment was to resect the affected length of colon.
In the past few years, however, various workers have returned to the study of the anatomy, physio- logy, histology, and function of the colonic muscle, especially in the region of the lower sigmoid (Slack, 1962; Morson, 1963; Fleischner, Ming, and Henken, 1964). I t is here that there seems something akin to a physiological sphincter which opens to allow the faeces to be passed into the rectum ready for evacua- tion. I t is in the lower half of the sigmoid colon also that diverticula are most commonly found, although diverticula can occur anywhere in the colon.
My own interest in the nature of the thickening of the colon developed some 4 years ago when inspecting a length of sigmoid removed for diverticulitis (Reilly,
1964, 1965). There did not seem to be any serious pathological change in the colon except thickening of the muscle coat and corrugation of the mucous membrane. Apart from signs of past inflammation on the serous coat there was no macroscopic evidence of ulceration or inflammation, nor did the thickening of the muscle layer seem to be due to fibrosis. I t was, however, sufficient to cause a long apparent stricture fairly well demarcated at each end.
It occurred to me that it was a pity to subject a patient to resection of relatively healthy bowel for this condition, especially as the anastomosis may be difficult due to shortening of the mesentery, which is often the only visible result of past inflammation. Such anastomosis may also break down, leaving a faecal fistula. I wondered whether some operation less drastic and hazardous than resection were possible, and thought that a myotomy somewhat similar to a Heller’s or Ramstedt’s operation might give satisfactory results. The risks were obvious. Such an experimental operation should not be lightly undertaken in a potentially infected area with a rela- tively poor blood-supply. I therefore waited until a suitable patient should present. This did not occur until June, 1962, when a woman of 82 years was
860 BRIT. J. SURG., 1966, Vol. 53, No. 10, OCTOBER
admitted who had had a colostomy for diverticulitis 20 years before. The colostomy was unsatisfactory. It had formed a large hernia and was subject to frequent attacks of obstruction and faecal impaction leading to the present admission. She told me that her life was a misery and that any operation would be welcome.
THE OPERATION The operation was eventually performed on this
patient 6 months later, in December, 1962. The abdomen was opened through a lower midline incision. There was no sign of active inflammation. The sigmoid colon was mobilized and straightened
proceed with the application of this operative proce- dure and the next 2 cases presenting with diverticu- litis of sufficient severity to warrant operation were subjected to a simple primary sigmoid myotomy without other operative procedure (Fig. I). The results in both cases were highly satisfactory. The first patient passed a normal motion, the first normal motion for several years, on the second postoperative day and the other patient passed a normal motion on the third postoperative day. There were no complications.
The next patient presented with an obstructing pelvic mass due to perforated diverticulitis with abscess formation. In this case we performed a
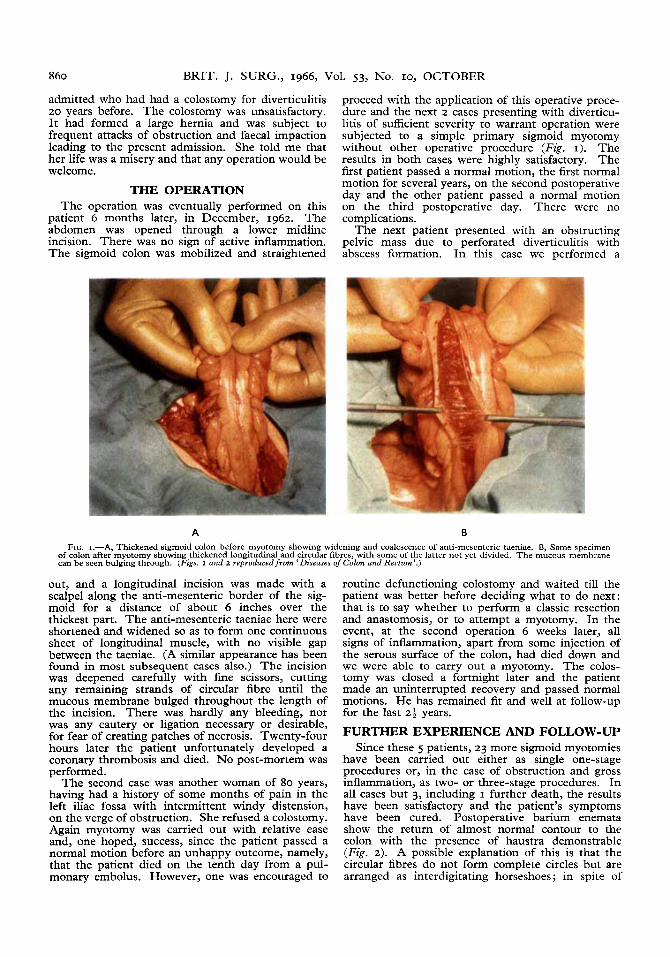
A B FIG. I.-A Thickened sigmoid colon before myotomy showing widening and coalescence of anti-mesenteric taeniae. B Same specimen
of colon afte;myotomy showing thickened longitudinal and circular fibres, with some of the latter not yet divided. The m;cous membrane can be seen bulging through. (Figs. I and z reproduced from ‘Diseases of Colon and Rectum’.)
out, and a longitudinal incision was made with a scalpel along the anti-mesenteric border of the sig- moid for a distance of about 6 inches over the thickest part. The anti-mesenteric taeniae here were shortened and widened so as to form one continuous sheet of longitudinal muscle, with no visible gap between the taeniae. (A similar appearance has been found in most subsequent cases also.) The incisjon was deepened carefully with fine scissors, cutting any remaining strands of circular fibre until the mucous membrane bulged throughout the length of the incision. There was hardly any bleeding, nor was any cautery or ligation necessary or desirable, for fear of creating patches of necrosis. Twenty-four hours later the patient unfortunately developed a coronary thrombosis and died. No post-mortem was performed.
The second case was another woman of 80 years, having had a history of some months of pain in the left iliac fossa with intermittent windy distension, on the verge of obstruction. She refused a colostomy. Again myotomy was carried out with relative ease and, one hoped, success, since the patient passed a normal motion before an unhappy outcome, namely, that the patient died on the tenth day from a pul- monary embolus. However, one was encouraged to
routine defunctioning colostomy and waited till the patient was better before deciding what to do next: that is to say whether to perform a classic resection and anastomosis, or to attempt a myotomy. In the event, at the second operation 6 weeks later, all signs of inflammation, apart from some injection of the serous surface of the colon, had died down and we were able to carry out a myotomy. The colos- tomy was closed a fortnight later and the patient made an uninterrupted recovery and passed normal motions. He has remained fit and well at follow-up for the last 24 years.
FURTHER EXPERIENCE AND FOLLOW-UP Since these 5 patients, 23 more sigmoid myotomies
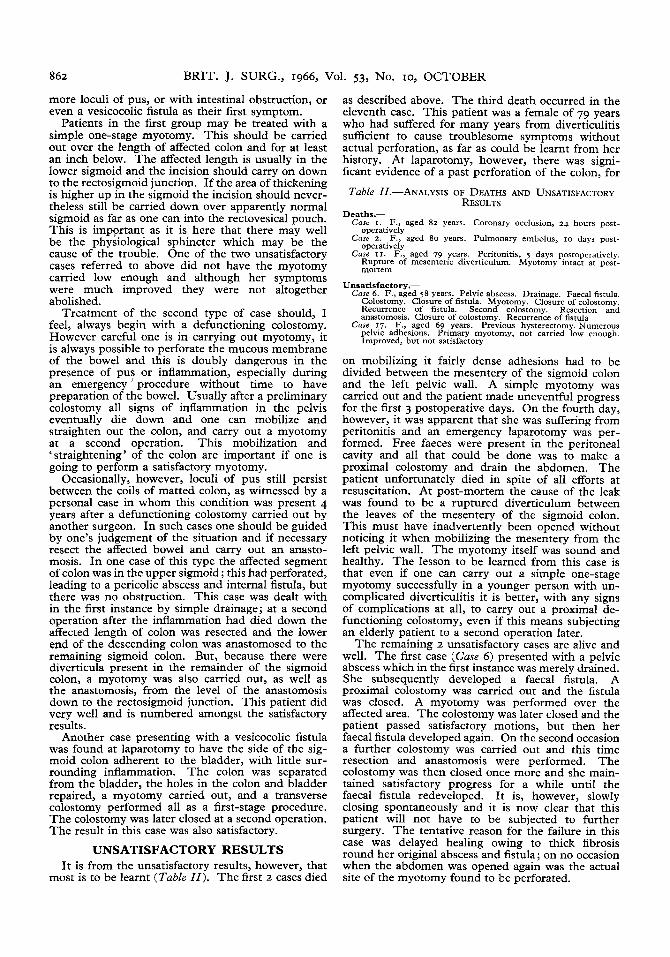
have been carried out either as single one-stage procedures or, in the case of obstruction and gross inflammation, as two- or three-stage procedures. In all cases but 3, including I further death, the results have been satisfactory and the patient’s symptoms have been cured. Postoperative barium enemata show the return of almost normal contour to the colon with the presence of haustra demonstrable (Fig. 2). A possible explanation of this is that the circular fibres do not form complete circles but are arranged as interdigitating horseshoes; in spite of

REILLY: SIGMOID MYOTOMY 861
the myotomy numerous bundles are left uncut and should still be capable of active contraction. Diverti- cula already present are left unaffected, except that there is no increase in their intraluminar pressure from isolated uncoordinated segmental contractions, such as have been demonstrated by Painter and Truelove (1964a, b). I t is this intraluminar increase in pressure in the diverticula which, I believe, leads to pressure necrosis and diverticulitis. From this it
years, has subsequently died or come to post-mortem, so far as can be traced. She succumbed to a coronary thrombosis in another hospital 9 months after opera- tion. Necropsy was performed, but no special attention was paid to the gastro-intestinal tract, which was reported ‘normal’.
So far I have carried out myotomies only on patients over the age of 50 years who have had either a long history of troublesome diverticulitis without
A B FIG. z.-A, Preoperative barium enema showing narrowing and irregularity of lower sigmoid. 6, Same colon 3 months after operation
showing return of almost normal contour, although diverticula can still be seen. (The appearance above the affected segment is out of the operative area and is due to an overlap of dependent transverse colon.)
follows that if a long segment of colon is the seat of diverticular change, say the whole of the sigmoid colon, then, even if a diverticulum perforates at one point and is dealt with by resection in the classic manner, other points in the colon are still at risk
Table I.-TWENTY-EIGHT CASES TREATED BY MYOTOMY, 1962-5 - -
15 Females.-.lgc range 51-82 years, average age 68 years Simple myotomy, iur uncomplicated diverticulitis I t hlyotomy, uith other procedurei, fur complicated diverticulitis 4
13 Males.-Age range 53-84 years, average age 64 years Simple myotomy, for uncomplicated diverticulitis I 0 Myotomy, with other procedures, for complicated diverticulitis 3
Total 28
Satisfactory Unsatisfactory z (one simple myotomy, one with other
Died
-
Results.- 23 (passing normal, regular, comfortable stools)
procedures) 3 (Cases I, 2, and 11)
later. Resection and anastomosis of a foot or more of colon is a major procedure and if one can avoid this by a myotomy, so much the better. In most cases I have found a myotomy of about 6-8 inches to be sufficient, but in several cases have felt that a longer myotomy was indicated and have carried out the procedure for a length of nearly 2 feet.
The macroscopic or microscopic appearance of the sigmoid colon is as yet unknown after a myotomy. Only I of the ‘satisfactory’ cases, a female aged 74 55
complications or who have presented with an acute complication of diverticulitis (Table I ) . It is possible that with increasing experience one may feel justified in carrying out myotomies on younger age-groups. I t may even be shown that spastic colon in the twenties, especially in females, is a precursor of diverticulitis, but I would not advocate routine myo- tomies for spastic colon: in the early stages spastic colon may be a reversible condition, and a return to a less refined diet, with more roughage than is the rule nowadays, may be all that is necessary in the way of treatment. Only when the condition has become structurally and functionally irreversible should myotomy be considered.
INDICATIONS FOR MYOTOMY The indications which at the moment appear to
justify myotomy are as follows:- I. Those cases with a long history of lower
abdominal discomfort, flatulence, and irregular bowel habit with small, pebbly faeces. Such patients may have acute exacerbations necessitating admis- sion to hospital for observation and medical treat- ment, if not operation and drainage of small abscesses. They also tend to bleed per rectum, sometimes in alarming quantities.
2. Cases who present as an emergency, sometimes with a very short history of any bowel abnormality. Such patients may present with a large pelvic mass due to adherent coils of matted colon with one or
862 BRIT. J. SURG., 1966, Vol. 53, No. 10, OCTOBER
more loculi of pus, or with intestinal obstruction, or even a vesicocolic fistula as their first symptom.
Patients in the first group may be treated with a simple one-stage myotomy. This should be carried out over the length of affected colon and for at least an inch below. The affected length is usually in the lower sigmoid and the incision should carry on down to the rectosigmoid junction. If the area of thickening is higher up in the sigmoid the incision should never- theless still be carried down over apparently normal sigmoid as far as one can into the rectovesical pouch. This is important as it is here that there may well be the physiological sphincter which may be the cause of the trouble. One of the two unsatisfactory cases referred to above did not have the myotomy carried low enough and although her symptoms were much improved they were not altogether abolished.
Treatment of the second type of case should, I feel, always begin with a defunctioning colostomy. However careful one is in carrying out myotomy, it is always possible to perforate the mucous membrane of the bowel and this is doubly dangerous in the presence of pus or inflammation, especially during an emergency ’ procedure without time to have preparation of the bowel. Usually after a preliminary colostomy all signs of inflammation in the pelvis eventually die down and one can mobilize and straighten out the colon, and carry out a myotomy at a second operation. This mobilization and ‘straightening’ of the colon are important if one is going to perform a satisfactory myotomy.
Occasionally, however, loculi of pus still persist between the coils of matted colon, as witnessed by a personal case in whom this condition was present 4 years after a defunctioning colostomy carried out by another surgeon. I n such cases one should be guided by one’s judgement of the situation and if necessary resect the affected bowel and carry out an anasto- mosis. In one case of this type the affected segment of colon was in the upper sigmoid; this had perforated, leading to a pericolic abscess and internal fistula, but there was no obstruction. This case was dealt with in the first instance by simple drainage; at a second operation after the inflammation had died down the affected length of colon was resected and the lower end of the descending colon was anastomosed to the remaining sigmoid colon. But, because there were diverticula present in the remainder of the sigmoid colon, a myotomy was also carried out, as well as the anastomosis, from the level of the anastomosis down to the rectosigmoid junction. This patient did very well and is numbered amongst the satisfactory results.
Another case presenting with a vesicocolic fistula was found at laparotomy to have the side of the sig- moid colon adherent to the bladder, with little sur- rounding inflammation. The colon was separated from the bladder, the holes in the colon and bladder repaired, a myotomy carried out, and a transverse colostomy performed all as a first-stage procedure. The colostomy was later closed at a second operation. The result in this case was also satisfactory.
UNSATISFACTORY RESULTS I t is from the unsatisfactory results, however, that
most is to be learnt (Table 11). The first z cases died
as described above. The third death occurred in the eleventh case. This patient was a female of 79 years who had suffered for many years from diverticulitis sufficient to cause troublesome symptoms without actual perforation, as far as could be learnt from her history. At laparotomy, however, there was signi- ficant evidence of a past perforation of the colon, for
Table II.-ANALYSIS OF DEATHS AND UNSATISFACTORY RESULTS
Deaths.- - .~ ~~~. Care I . F., aged 82 years. Coronary occlusion, 24 hours post-
Care 2. F., aged 80 years. Pulmonary embolus. 10 davs oost- operatively
. . operatively
Care XI. F., aged 79 years. Peritonitis, 5 days postoperatively. Rupture of mesenteric diverticulum. Myotomy intact at post- mortem
Unsatisfactory.- Care 6. F., aged 58 years. Pelvic abscess. Drainage. Faecal fistula.
Colostomy. Closure of fistula. Myotomy. Closure of colostomy. Recurrence of fistula. Second colostomy. Resection and anastomosis. Closure of colostomy. Recurrence of fistula
Case 17. F., aged 69 years. Previous hysterectomy. Numerous pelvic adhesions. Primary myotomy, not carried low enough. Improved, but not satisfactory
on mobilizing it fairly dense adhesions had to be divided between the mesentery of the sigmoid colon and the left pelvic wall. A simple myotomy was carried out and the patient made uneventful progress for the first 3 postoperative days. On the fourth day, however, it was apparent that she was suffering from peritonitis and an emergency laparotomy was per- formed. Free faeces were present in the peritoneal cavity and all that could be done was to make a proximal colostomy and drain the abdomen. The patient unfortunately died in spite of all efforts at resuscitation. At post-mortem the cause of the leak was found to be a ruptured diverticulum between the leaves of the mesentery of the sigmoid colon. This must have inadvertently been opened without noticing it when mobilizing the mesentery from the left pelvic wall. The myotomy itself was sound and healthy. The lesson to be learned from this case is that even if one can carry out a simple one-stage myotomy successfully in a younger person with un- complicated diverticulitis it is better, with any signs of complications at all, to carry out a proximal de- functioning colostomy, even if this means subjecting an elderly patient to a second operation later.
The remaining z unsatisfactory cases are alive and well. The first case (Case 6) presented with a pelvic abscess which in the first instance was merely drained. She subsequently developed a faecal fistula. A proximal colostomy was carried out and the fistula was closed. A myotomy was performed over the affected area. The colostomy was later closed and the patient passed satisfactory motions, but then her faecal fistula developed again. On the second occasion a further colostomy was carried out and this time resection and anastomosis were performed. The colostomy was then closed once more and she main- tained satisfactory progress for a while until the faecal fistula redeveloped. It is, however, slowly closing spontaneously and it is now clear that this patient will not have to be subjected to further surgery. The tentative reason for the failure in this case was delayed healing owing to thick fibrosis round her original abscess and fistula; on no occasion when the abdomen was opened again was the actual site of the myotomy found to be perforated.
REILLY: SIGMOID MYOTOMY 863
The second unsatisfactory case (Case 17) had had diverticular disease. First, in the long-standing case a previous hysterectomy. There were numerous of diverticulitis without complications, but suffici- adhesions in the pelvis and the sigmoid colon was ently severe to cause incapacitating symptoms at coiled down in the pouch of Douglas. The colon intervals, and, secondly, in some of the complicated was mobilized, but the lower portion of it remained cases of diverticulitis presenting with obstruction,
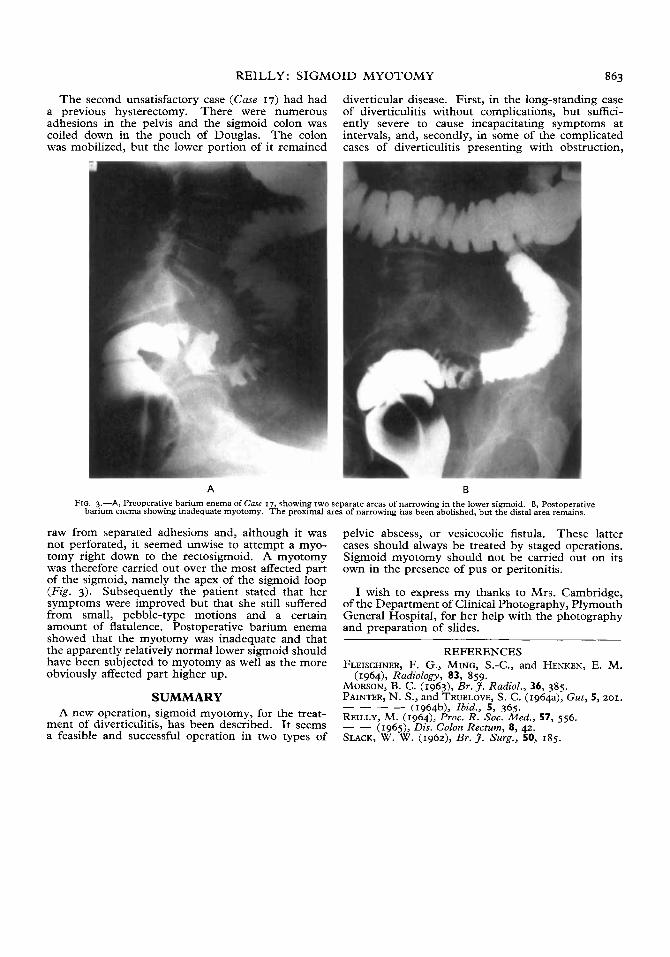
A B FIG. 3.-A, Preoperative barium enema of Case 17, showing two separate areas of narrowing in the lower sigmoid. B, Postoperative
barium enema showing inadequate myotomy. The proximal area of narrowing has been abolished, hut the distal area remains.
raw from separated adhesions and, although it was not perforated, it seemed unwise to attempt a myo- tomy right down to the rectosigmoid. A myotomy was therefore carried out over the most affected part of the sigmoid, namely the apex of the sigmoid loop (Fig. 3). Subsequently the patient stated that her symptoms were improved but that she still suffered from small, pebble-type motions and a certain amount of flatulence. Postoperative barium enema showed that the myotomy was inadequate and that the apparently relatively normal lower sigmoid should have been subjected to myotomy as well as the more obviously affected part higher up.
SUMWRY A new operation, sigmoid myotomy, for the treat-
ment of diverticulitis, has been described. I t seems a feasible and successful operation in two types of
pelvic abscess, or vesicocolic fistula. These latter cases should always be treated by staged operations. Sigmoid myotomy should not be carried out on its own in the presence of pus or peritonitis.
I wish to express my thanks to Mrs. Cambridge, of the Department of Clinical Photography, Plymouth General Hospital, for her help with the photography and preparation of slides.
REFERENCES FLEISCHNER, F. G., MING, S.-C., and HENKEN, E. M.
MORSON, B. C. (1963), Br.3. Radiol., 36, 385. PAINTER, N. S., and TRUELOVE, S. C. (1964a), Gut, 5,201. _ _ _ _ (1964b), Ibid., 5, 365. REILLY, M. (1964), Proc. R. Soc. Med., 57, 556. - _ (1965), Dis. Colon Rectum, 8, 42. SLACK, W. W. (1962), Br. J. Surg., 50, 185.
(1964), Radiology, 83, 859.