silicosis himalayan villagepopulation: roleof ... - thoraxthorax: first published as...
TRANSCRIPT

Thorax 1991;46:341-343
Silicosis in a Himalayan village population: role ofenvironmental dust
T Norboo, P T Angchuk, M Yahya, S R Kamat, F D Pooley, B Corrin, I H Kerr,N Bruce, K P Ball
Sonam NorbooMemorial Hospitaland Leh NutritionProject, Leh, Ladakh,India 194101T NorbooP T AngchukM YahyaKing EdwardMemorial Hospital,Bombay, India 400012S R KamatDivision ofMining andMinerals Engineering,University ofWales,Cardiff CF2 1TAF D PooleyCentral MiddlesexHospital, LondonNW1O7NSK P BallRoyal Brompton andNational Heart andLung Hospital, LondonSW3 6NPI H KerrB CorrinRoyal Free Hospital,London NW3 2QGN BruceReprint requests to:Dr Norboo (India) or Dr Ball(The Studio, Mount ParkRoad, London W5 2RP)Accepted 15 February 1991
AbstractThe Himalayan villages of ChuchotShamma and Stok were surveyedbecause silicosis had been suspectedfrom the radiographs of some of theinhabitants. The villages are agricul-tural, and Chuchot is exposed tofrequent dust storms. Chest radiographsof villagers aged 50-62 were assessedblind by two independent observersusing ILO criteria. In Chuchot five ofseven men and all of the nine womenexamined showed varying grades ofsilicosis, compared with three of 13 menand seven of 11 women in Stok, whichlies 300 metres higher and is exposed tofewer dust storms. The difference inprevalence of silicosis between the twovillages was significant, as was the dif-ferences between men and women.Three patients from the village adjoiningChuchot were later found to haveradiological evidence of progressivemassive fibrosis. A necropsy on a man ina neighbouring village in the Indus valleyshowed classical silicosis in a hilarlymph node. Chemical analysis of theinorganic dust in the lung showed that54*4% was elemental silicone. This wassimilar to the silicone content of dustsamples collected from houses inChuchot, which included particles ofrespirable size. X ray microanalysisshowed that quartz formed 16-21% ofthe inorganic lung dust. This study sug-gests that silicosis is common among theolder inhabitants of these Himalayanvillages. The dust exposure is clearlyenvironmental and not industrial.Further studies are needed to define theextent and severity of silicosis in thiscommunity and to examine possiblepreventive measures.
For some years local doctors have been con-cerned at the frequency of chest disease insome villages of the Indus valley in Ladakh, ahigh altitude region of the Himalayas in northwest India. Some chest radiographs had sug-gested the presence of silicosis. To investigatethe problem further we have tried to deter-mine whether radiological evidence of silicosisis common, and whether environmental dustcould be the cause.
MethodsSTUDY VILLAGES AND SUBJECTSThe survey was carried out in two villagessituated about 15 km from Leh, the capital ofLadakh. The first village, Chuchot Shamma,lies in the Indus valley at an altitude of3200 m and is subject to frequent dust stormsin spring, which can be so dense as to obscurenearby mountains. The second village, Stok,lies 6 km away and, being 300 m higher, is lessexposed to dust storms. Both villages aremainly farming communities, each with apopulation of about 1000. The women aremore heavily exposed to dust because they domost of the farming work and they sweep thedusty houses and carry baskets of earth for thetraditional toilets. The houses have mud floorsand are often smoky owing to the lack of aneffective chimney. There is no occupational orother exposure to dust. About 20% of themen but none of the women smoke cigarettes.
Subjects aged 50-62 were drawn from theelectoral list of both villages. From ChuchotShamma every third man and every secondwoman and from Stok every second man andwoman was selected. Each person was invitedto Leh for radiographic chest examination;seven out of 10 men and nine out of 12 womenfrom Chuchot Shamma and all 13 men and 11women from Stok responded.
INVESTIGATIONSRadiographs were read blind and indepen-dently by two radiologists (SRK and IHK),who used the shortened ILO classification.'Necropsy material later became available froma Ladakhi resident in a neighbouring villagein the Indus valley. He was a musician aged60 years who had suffered a violent death.Lung tissue and hilar glands were examinedpathologically and representative portionsdigested for dust analysis.Dust from the upper surfaces of beams inthree houses in Chuchot Shamma and thepathological specimens were analysed bymeans of a transmission electron microscopeequipped for x ray diffraction and energydispersive x ray analysis.
ANALYSISStatistical significance was tested with Fisher'sexact test. Two tailed values were obtained bydoubling the probability of the observed ormore extreme values.
341
on March 16, 2020 by guest. P
rotected by copyright.http://thorax.bm
j.com/
Thorax: first published as 10.1136/thx.46.5.341 on 1 M
ay 1991. Dow
nloaded from
on March 16, 2020 by guest. P
rotected by copyright.http://thorax.bm
j.com/
Thorax: first published as 10.1136/thx.46.5.341 on 1 M
ay 1991. Dow
nloaded from
on March 16, 2020 by guest. P
rotected by copyright.http://thorax.bm
j.com/
Thorax: first published as 10.1136/thx.46.5.341 on 1 M
ay 1991. Dow
nloaded from
Norboo, Angchuk, Yahya, et al
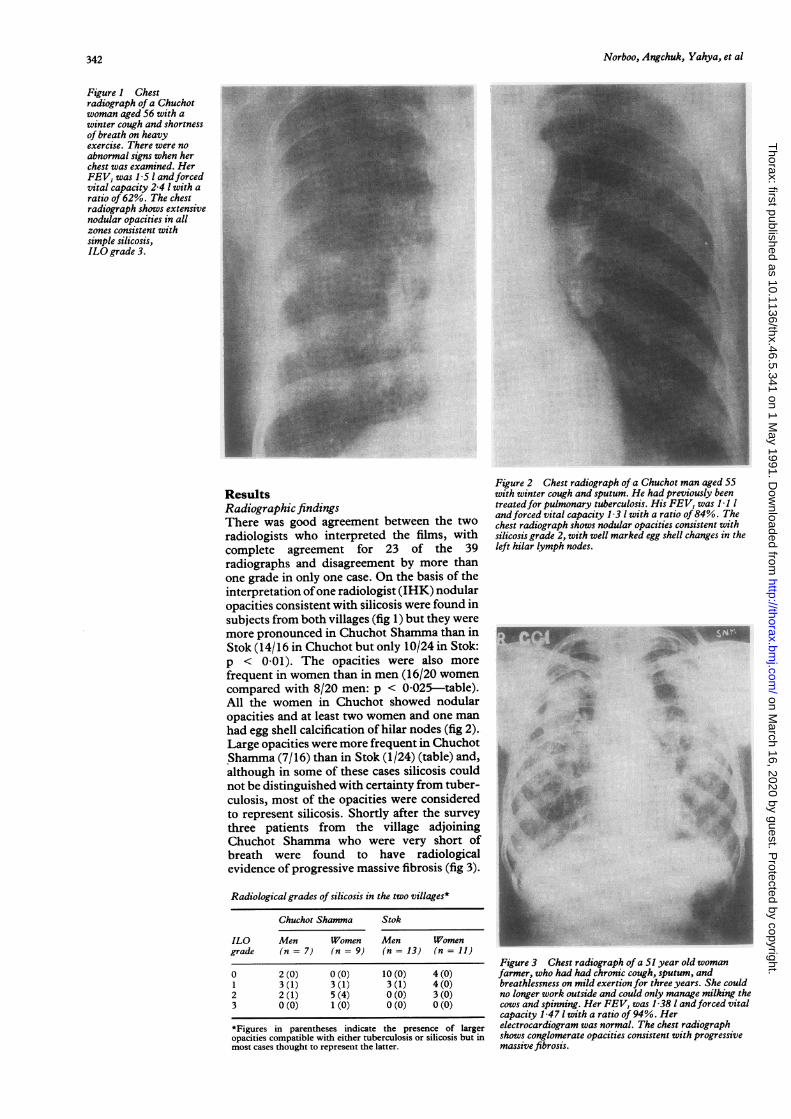
Figure 1 Chestradiograph of a Chuchotwoman aged 56 with awinter cough and shortnessof breath on heavyexercise. There were noabnormal signs when herchest was examined. HerFEV, was 1 5 1 andforcedvital capacity 2-4 1 with aratio of 62%. The chestradiograph shows extensivenodular opacities in allzones consistent withsimple silicosis,ILO grade 3.
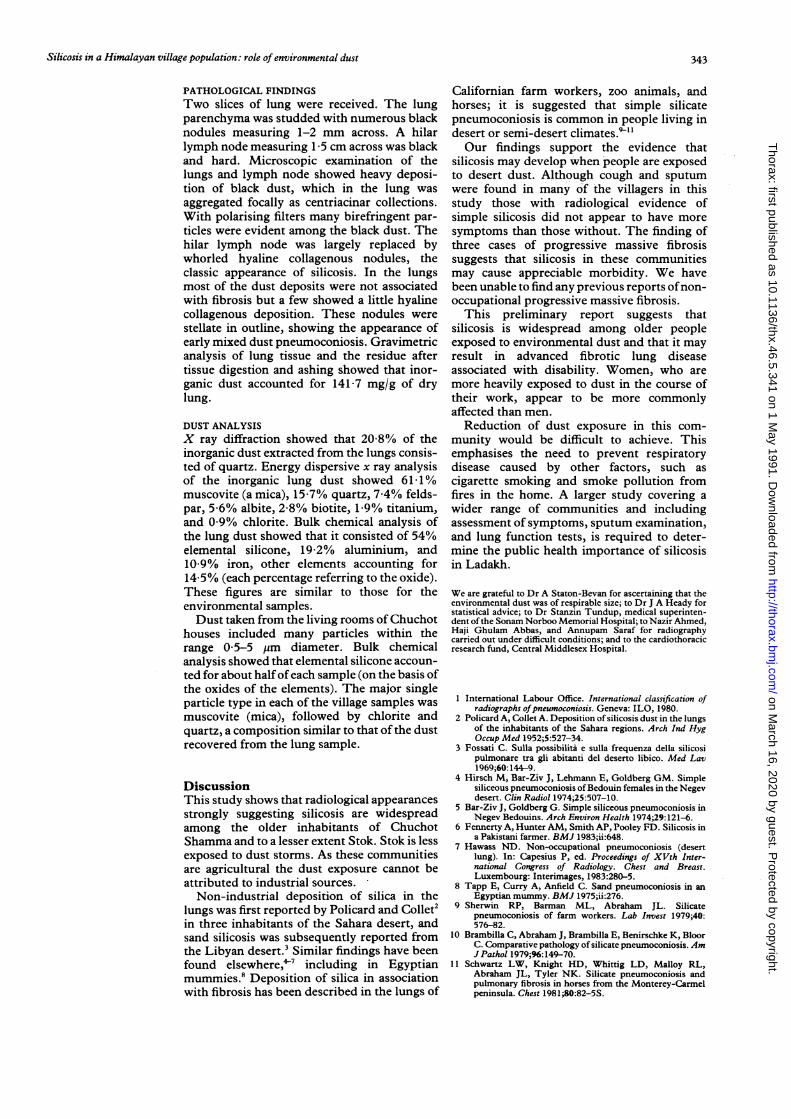
ResultsRadiographic findingsThere was good agreement between the tworadiologists who interpreted the films, withcomplete agreement for 23 of the 39radiographs and disagreement by more thanone grade in only one case. On the basis of theinterpretation ofone radiologist (IHK) nodularopacities consistent with silicosis were found insubjects from both villages (fig 1) but they weremore pronounced in Chuchot Shamma than inStok (14/16 in Chuchot but only 10/24 in Stok:p < 0 01). The opacities were also morefrequent in women than in men (16/20 womencompared with 8/20 men: p < 0-025-table).All the women in Chuchot showed nodularopacities and at least two women and one manhad egg shell calcification of hilar nodes (fig 2).Large opacities were more frequent in ChuchotShamma (7/16) than in Stok (1/24) (table) and,although in some of these cases silicosis couldnot be distinguished with certainty from tuber-culosis, most of the opacities were consideredto represent silicosis. Shortly after the surveythree patients from the village adjoiningChuchot Shamma who were very short ofbreath were found to have radiologicalevidence of progressive massive fibrosis (fig 3).
Radiological grades of silicosis in the two villages*
Chuchot Shamma Stok
ILO Men Women Men Womengrade (n = 7) (n = 9) (n= 13) (n = 11)
0 2 (0) 0 (0) 10 (0) 4 (0)1 3 (1) 3 (1) 3 (1) 4 (0)2 2 (1) 5 (4) 0 (0) 3 (0)3 0(0) 1 (0) 0(0) 0(0)
*Figures in parentheses indicate the presence of largeropacities compatible with either tuberculosis or silicosis but inmost cases thought to represent the latter.
Figure 2 Chest radiograph of a Chuchot man aged 55with winter cough and sputum. He had previously beentreatedfor pulmonary tuberculosis. His FEV, was 1 1 1andforced vital capacity 1 31 with a ratio of 84%. Thechest radiograph shows nodular opacities consistent withsilicosis grade 2, with well marked egg shell changes in theleft hilar lymph nodes... .......
*_ ;:u.r_.....
,. e sixSA
eSA ^
*.X.
,@ :.. ^.... ..
Figure 3 Chest radiograph of a 51 year old womanfarmer, who had had chronic cough, sputum, andbreathlessness on mild exertion for three years. She couldno longer work outside and could only manage milking thecows and spinning. Her FEV, was 1-38 1 andforced vitalcapacity 1 471 with a ratio of 94%. Herelectrocardiogram was normal. The chest radiographshows conglomerate opacities consistent with progressivemassive fibrosis.
342
Z..
on March 16, 2020 by guest. P
rotected by copyright.http://thorax.bm
j.com/
Thorax: first published as 10.1136/thx.46.5.341 on 1 M
ay 1991. Dow
nloaded from
Silicosis in a Himalayan village population: role of environmental dust
PATHOLOGICAL FINDINGSTwo slices of lung were received. The lungparenchyma was studded with numerous blacknodules measuring 1-2 mm across. A hilarlymph node measuring 1 5 cm across was blackand hard. Microscopic examination of thelungs and lymph node showed heavy deposi-tion of black dust, which in the lung was
aggregated focally as centriacinar collections.With polarising filters many birefringent par-ticles were evident among the black dust. Thehilar lymph node was largely replaced bywhorled hyaline collagenous nodules, theclassic appearance of silicosis. In the lungsmost of the dust deposits were not associatedwith fibrosis but a few showed a little hyalinecollagenous deposition. These nodules were
stellate in outline, showing the appearance ofearly mixed dust pneumoconiosis. Gravimetricanalysis of lung tissue and the residue aftertissue digestion and ashing showed that inor-ganic dust accounted for 1417 mg/g of drylung.
DUST ANALYSISX ray diffraction showed that 20-8% of theinorganic dust extracted from the lungs consis-ted of quartz. Energy dispersive x ray analysisof the inorganic lung dust showed 61 1%muscovite (a mica), 15-7% quartz, 7*4% felds-par, 5-6% albite, 2-8% biotite, 1-9% titanium,and 0 9% chlorite. Bulk chemical analysis ofthe lung dust showed that it consisted of 54%elemental silicone, 19-2% aluminium, and10-9% iron, other elements accounting for14-5% (each percentage referring to the oxide).These figures are similar to those for theenvironmental samples.Dust taken from the living rooms ofChuchot
houses included many particles within therange 05-5 ,um diameter. Bulk chemicalanalysis showed that elemental silicone accoun-ted for about halfofeach sample (on the basis ofthe oxides of the elements). The major singleparticle type in each of the village samples was
muscovite (mica), followed by chlorite andquartz, a composition similar to that of the dustrecovered from the lung sample.
DiscussionThis study shows that radiological appearancesstrongly suggesting silicosis are widespreadamong the older inhabitants of ChuchotShamma and to a lesser extent Stok. Stok is lessexposed to dust storms. As these communitiesare agricultural the dust exposure cannot beattributed to industrial sources.
Non-industrial deposition of silica in thelungs was first reported by Policard and Collet2in three inhabitants of the Sahara desert, andsand silicosis was subsequently reported fromthe Libyan desert.3 Similar findings have beenfound elsewhere, 7 including in Egyptianmummies.8 Deposition of silica in associationwith fibrosis has been described in the lungs of
Californian farm workers, zoo animals, andhorses; it is suggested that simple silicatepneumoconiosis is common in people living indesert or semi-desert climates."'1Our findings support the evidence that
silicosis may develop when people are exposedto desert dust. Although cough and sputumwere found in many of the villagers in thisstudy those with radiological evidence ofsimple silicosis did not appear to have moresymptoms than those without. The finding ofthree cases of progressive massive fibrosissuggests that silicosis in these communitiesmay cause appreciable morbidity. We havebeen unable to find any previous reports ofnon-occupational progressive massive fibrosis.This preliminary report suggests that
silicosis is widespread among older peopleexposed to environmental dust and that it mayresult in advanced fibrotic lung diseaseassociated with disability. Women, who aremore heavily exposed to dust in the course oftheir work, appear to be more commonlyaffected than men.
Reduction of dust exposure in this com-munity would be difficult to achieve. Thisemphasises the need to prevent respiratorydisease caused by other factors, such ascigarette smoking and smoke pollution fromfires in the home. A larger study covering awider range of communities and includingassessment of symptoms, sputum examination,and lung function tests, is required to deter-mine the public health importance of silicosisin Ladakh.
We are grateful to Dr A Staton-Bevan for ascertaining that theenvironrmental dust was of respirable size; to Dr J A Heady forstatistical advice; to Dr Stanzin Tundup, medical superinten-dent ofthe Sonam Norboo Memorial Hospital; to Nazir Ahmed,Haji Ghulam Abbas, and Annupam Saraf for radiographycarried out under difficult conditions; and to the cardiothoracicresearch fund, Central Middlesex Hospital.
1 International Labour Office. International classification ofradiographs ofpneumoconiosis. Geneva: ILO, 1980.
2 Policard A, Collet A. Deposition of silicosis dust in the lungsof the inhabitants of the Sahara regions. Arch Ind HygOccup Med 1952;5:527-34.
3 Fossati C. Sulla possibilita e sulla frequenza della silicosipulmonare tra gli abitanti del deserto libico. Med Lav1969;60:144-9.
4 Hirsch M, Bar-Ziv J, Lehmann E, Goldberg GM. Simplesiliceous pneumoconiosis ofBedouin females in the Negevdesert. Clin Radiol 1974;25:507-10.
5 Bar-Ziv J, Goldberg G. Simple siliceous pneumoconiosis inNegev Bedouins. Arch Environ Health 1974;29:121-6.
6 Fennerty A, Hunter AM, Smith AP, Pooley FD. Silicosis ina Pakistani farmer. BMJ 1983;ii:648.
7 Hawass ND. Non-occupational pneumoconiosis (desertlung). In: Capesius P, ed. Proceedings of XVth Inter-national Congress of Radiology. Chest and Breast.Luxembourg: Interimages, 1983:280-5.
8 Tapp E, Curry A, Anfield C. Sand pneumoconiosis in anEgyptian mummy. BMJ 1975;ii:276.
9 Sherwin RP, Barman ML, Abraham JL. Silicatepneumoconiosis of farm workers. Lab Invest 1979;40:576-82.
10 Brambilla C, Abraham J, Brambilla E, Benirschke K, BloorC. Comparative pathology of silicate pneumoconiosis. AmJ Pathol 1979;%:149-70.
11 Schwartz LW, Knight HD, Whittig LD, Malloy RL,Abraham JL, Tyler NK. Silicate pneumoconiosis andpulmonary fibrosis in horses from the Monterey-Carmelpeninsula. Chest 1981;80:82-5S.
343
on March 16, 2020 by guest. P
rotected by copyright.http://thorax.bm
j.com/
Thorax: first published as 10.1136/thx.46.5.341 on 1 M
ay 1991. Dow
nloaded from

Thorax 1991;46:544
LETTERS TOTHE EDITOR
Risk of tuberculosis in immigrantAsians: culturally acquired immuno-deficiency
I was interested to see that in the paper by DrPJ Finch and colleagues (January 1991;46: 1-5) the theory that vitamin D deficiency causesimmunosuppression and increased host sus-ceptibility to tuberculosis was put forward asa possible cause of the increased incidence oftuberculosis, particularly glandular tuber-culosis, in Hindu immigrants.' Perhapsbecause of the authors' gastroenterologicalinterests they see dietary factors as a majorcause of vitamin deficiency and thereforesusceptibility to disease. Dietary patterns,however, probably do not differ greatly be-tween Britain and their country of origin, andare therefore unlikely to make much con-tribution to the cause of this apparent"acquired immunodeficiency of immi-gration. " A Hindu Vegan in Wandsworth wasprobably a Hindu Vegan in India. Vitamin Dreduction due to decreased exposure to sun-light on immigration to Britain, however,may well be a major factor. Mean serumvitamin D concentrations (25(OH)D,) havebeen shown to drop four-fold, or more, onemigration from Asia to Britain.'
Asian individuals with tuberculous infec-tion who are able to contain the infectionbecause of satisfactory host immunity whilein their sunny country of origin suffer adramatic fall in the storage form of vitamin D25(OH)D, on emigrating to the UnitedKingdom. In some individuals this may affectlocal production of the active hormone1,25(OH)2D,, resulting in a relative decline oflymphocyte and macrophage activation.2 Thepreviously contained infection then causesovert disease. This would explain why mostindividuals present within a relatively shorttime (five years) of arrival in Britain.The fact that the pattern of tuberculosis in
HIV positive patients seems to resemble thepattern of disease in Asian individuals inBritain has been pointed out before.' Thesequence of events is probably similar in thesepatients. An individual with tuberculosisinfection becomes immunocompromised(either from HIV infection or from vitamin Dreduction) and the extrapulmonary and glan-dular pattern of disease emerges.Much more detailed work on the immun-
ology of both tuberculosis and HIV infectionis needed; it may even be that vitamin D has arole in the treatment of AIDS.
PDO DAVIESSouth Liverpool Chest Clinic,
Sefton General Hospital,Liverpool L15 2HE
1 Rashid A, Mohammed T, Stephens WP,Warrington S, Berry JL, Mauren EB. VitaminD state of Asians living in Pakistan. BMJ1983;286: 182-4.
2 Rook GAW. The role of vitamin D in tuber-culosis. Am Rev Respir Dis 1988;138:768-70.
3 Davies PDO. Vitamin D and tuberculosis. AmRev Respir Dis 1989;139:1571.
AUTHORS' REPLY We are grateful to DrDavies for his letter and support for oursuggestion that vitamin D lack and resultantdecline in monocyte activation may be impor-tant in explaining the pronounced differencesin risk of tuberculosis among Asianimmigrants in the United Kingdom. Weaccept that Asian dietary practices are un-likely to change with emigration, but it hasbeen shown that where exposure to the sun islimited the risk of metabolic bone disease isdetermined by dietary factors.' In a prospec-tive study of Asians presenting to a generalmedical outpatient clinic in Wandsworth wehave found that osteomalacia is almostexclusively a disease of vegetarian HinduAsians, and we believe that this may help toexplain why it is the Hindus who are atparticular risk of developing tuberculosisrather than the Muslims, who have verysimilar exposure to the sun.The mechanism by which vegetarianism
may produce vitamin D deficiency is not clearas the contribution of ingested ergocalciferolto the physiological economy of vitamin D isthought to be negligible. It has been sugges-ted that calcium depletion caused by bindingto fibre and phytate may lead to secoindaryhyperparathyroidism and acceleratedcatabolism of 25-hydroxy vitamin D.2Another possibility is that the absence of thenormal dietary inducers of hepatic mixedfunction oxidases found in meat, eggs, andcheese may constrain the hydroxylation ofcholecalciferol.'
PJ FINCHFJC MILLARDJD MAXWELL
Department of Biochemical Medicine,St George's Hospital Medical School
London SWl 7 ORE
1 Henderson JB, Dunnigan MG, McIntosh WB,Abdul-Motaal AA, Hole D. Asianosteomalacia is determined bv dietary factorswhen exposure to ultra-violet radiation isrestricted-a risk factor model. Q J Med1990;281:923-33.
2 Clements MR, Johnson L, Fraser DR. A newmechanism for induced vitamin D deficiencyin calcium deprivation. Nature 1987;325:62-5.
3 Dollery CT, Fraser HS, Davies D, Macintyre I.Vitamin D status in different subgroups ofBritish Asians. Br Med J 1977;i: 104.
Measures of reversibility in responseto bronchodilators in chronic airflowobstruction
Drs DC Weir and PS Burge (January 1991;46:43-5) have looked at various indices ofreversibility in response to bronchodilators inchronic airflow obstruction and correlatedthese indices with the prebronchodilatorforced expiratory volume in one second(FEV,). They showed that two out of the fourindices of reversibility they used correlatedwith prebronchodilator FEV. It is, however,doubtful whether their analysis and con-clusions are valid.The difficulty in interpreting this type of
data is that the indices of reversibility allinclude prebronchodilator FEV,. This valuetherefore influences both of the variablesbeing correlated. A significant association isthus likely to arise because of this mathe-matical association alone. This is not to denythat there may be a true biological associationbetween prebronchodilator FEVy and one ormore of the indices of reversibility, but it islikely to be masked by the mathematicalassociation.
The vexed subject of examining the rela-tion between a measurement and its changeafter a therapeutic intervention is one thatregularly surfaces.' 2
GE PACKEChest Clinic,
City Hospital,Aberdeen AB9 8A U
1 Oldham PD. A note on the analysis of repeatedmeasurements of the same subject. J ChronicDis 1963;15:969-77.
2 Gill JS, Zezulka AV, Beevers DG, Davies P.Relation between initial blood pressure and itsfall with treatment. Lancet 1985;i:567-9.
AUTHOR'S REPLY I thank Dr Packe for rais-ing this point, but believe that our con-clusions are still valid. The inclusion ofprebronchodilator FEV, in each index maywell cause a correlation to be present becauseof mathematical rather than biologicalassociation. Hence it is difficult to know ifthe statistically significant correlations seenbetween prebronchodilator FEV, and rever-sibility, expressed as a percentage of theinitial FEV, or as a percentage of the "pos-sible" reversibility, reflect true biologicalassociation. But as reversibility expressed asthe absolute change in FEV, and reversibilityas a percentage of the individual's predictedFEV, show no significant correlation it wouldappear preferable to use either of theseindices if a measure independent of FEV, isneeded.
DAVID C WEIRDepartment of Respiratory Medicine,
East Birmingham Hospital,Birmingham B9 SST
NOTICE
Thoracic surgery review course
The second biennial thoracic surgery reviewcourse will be held in Birmingham on 12 and13 October 1991. Details and applicationforms may be obtained from UniversalConference Consultants, 145-147 AlcesterRoad, Birmingham B13 8JP (021 442 4307).
CORRECTION
Hut lung: a domestically acquiredpneumoconiosis of mixed aetiology
Silicosis in a Himalayan village popula-tion: role of environmental dust
We regret that "silicon" is misspelt as"silicone" in these two papers-in the firstpaper, by Drs JP Grobbelaar and EDBateman (May 199 1;46:334-40), on page 339,column 1, line 5; and in the second paper, bvDr T Norboo and others (May 1991;46:341-3), on page 341, lines 28 and 29 of theabstract, and on page 343, lines 9 and 17 of"Results."
544