similarities and differences between icd9cm & icd10 cm · pdf fileconventions: punctuation...
TRANSCRIPT
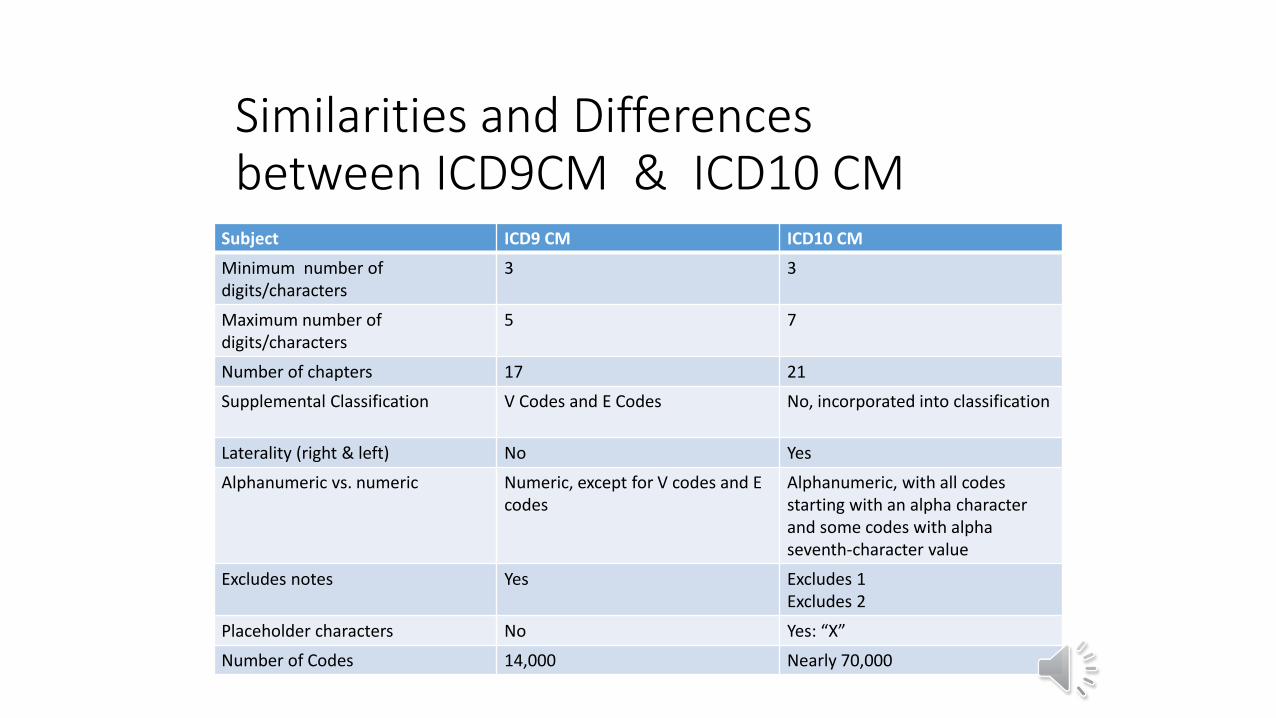
Similarities and Differences between ICD9CM & ICD10 CM
Subject ICD9 CM ICD10 CM
Minimum number of digits/characters
3 3
Maximum number of digits/characters
5 7
Number of chapters 17 21
Supplemental Classification V Codes and E Codes No, incorporated into classification
Laterality (right & left) No Yes
Alphanumeric vs. numeric Numeric, except for V codes and E codes
Alphanumeric, with all codes starting with an alpha character and some codes with alpha seventh-character value
Excludes notes Yes Excludes 1Excludes 2
Placeholder characters No Yes: “X”
Number of Codes 14,000 Nearly 70,000
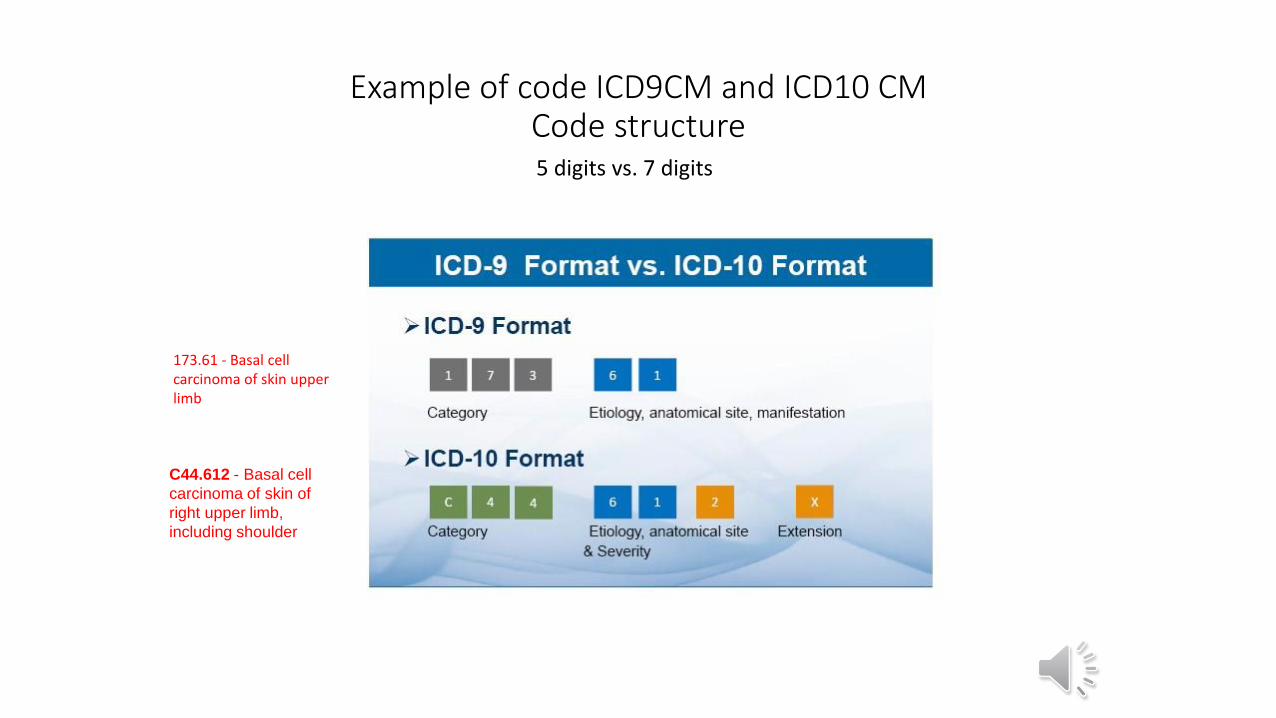
Example of code ICD9CM and ICD10 CM Code structure 5 digits vs. 7 digits
173.61 - Basal cell carcinoma of skin upper limb
C44.612 - Basal cell
carcinoma of skin of
right upper limb,
including shoulder
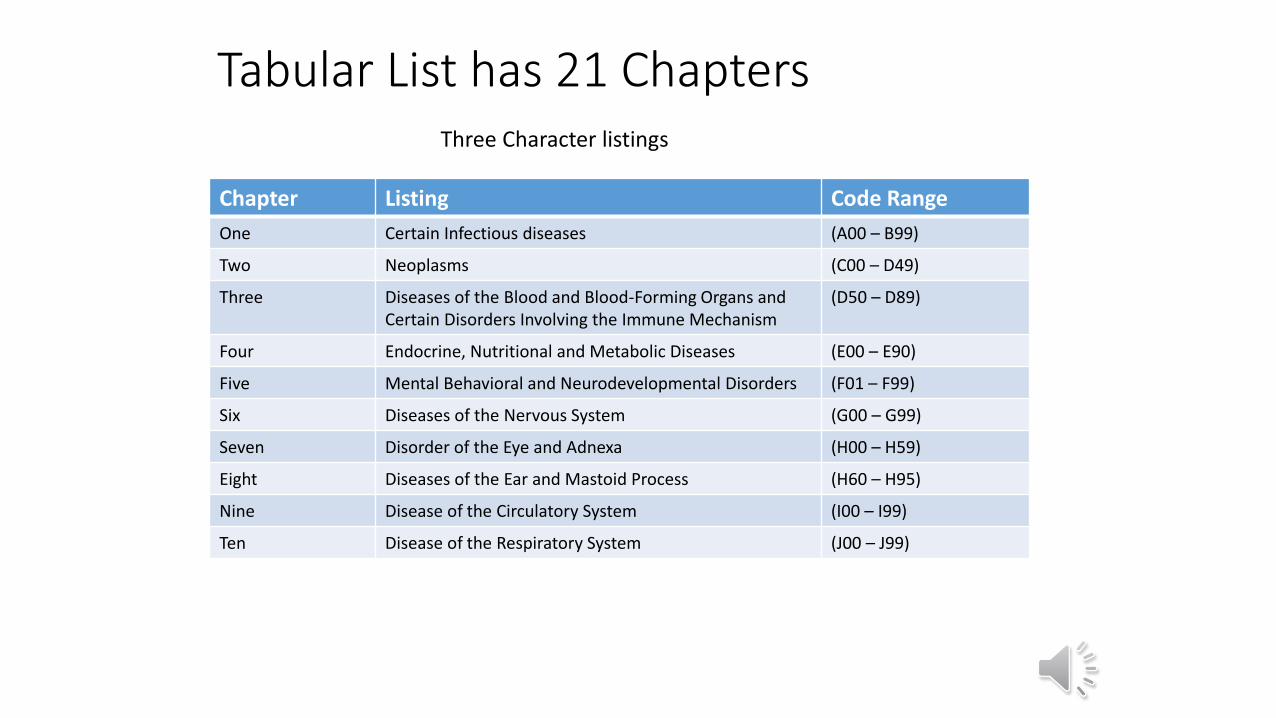
Tabular List has 21 Chapters
Chapter Listing Code Range
One Certain Infectious diseases (A00 – B99)
Two Neoplasms (C00 – D49)
Three Diseases of the Blood and Blood-Forming Organs and Certain Disorders Involving the Immune Mechanism
(D50 – D89)
Four Endocrine, Nutritional and Metabolic Diseases (E00 – E90)
Five Mental Behavioral and Neurodevelopmental Disorders (F01 – F99)
Six Diseases of the Nervous System (G00 – G99)
Seven Disorder of the Eye and Adnexa (H00 – H59)
Eight Diseases of the Ear and Mastoid Process (H60 – H95)
Nine Disease of the Circulatory System (I00 – I99)
Ten Disease of the Respiratory System (J00 – J99)
Three Character listings
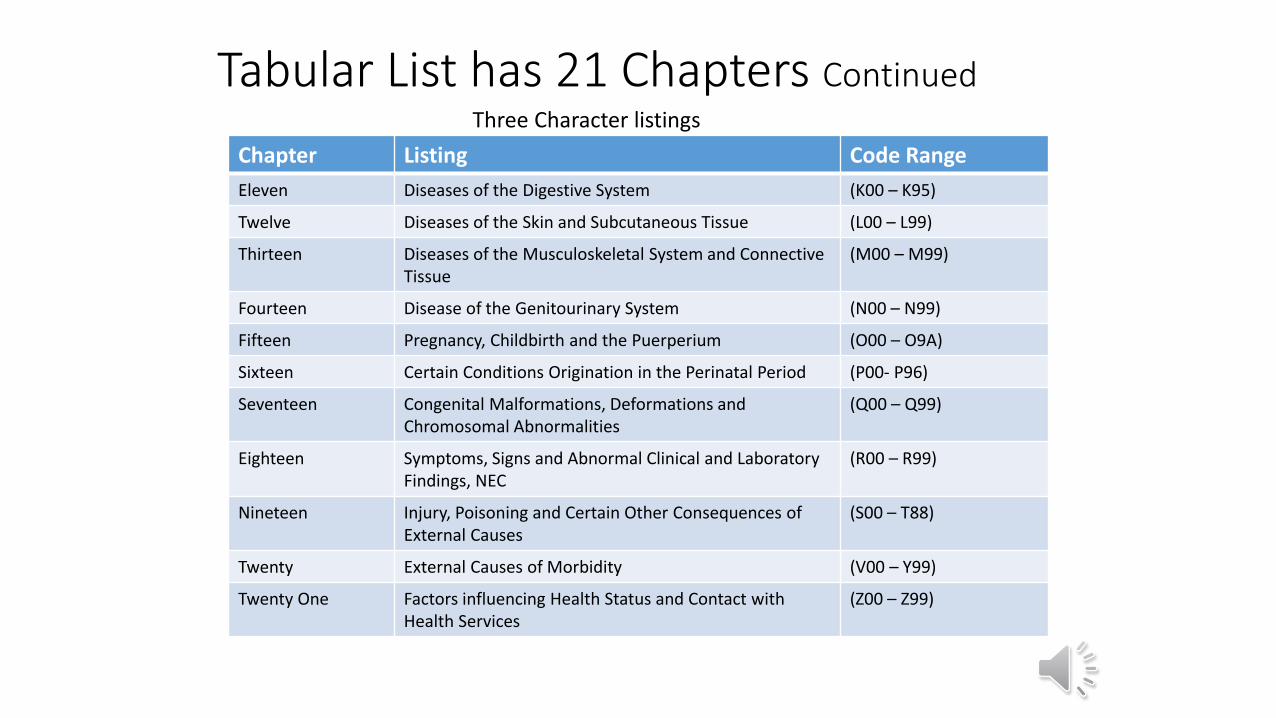
Tabular List has 21 Chapters Continued
Chapter Listing Code Range
Eleven Diseases of the Digestive System (K00 – K95)
Twelve Diseases of the Skin and Subcutaneous Tissue (L00 – L99)
Thirteen Diseases of the Musculoskeletal System and Connective Tissue
(M00 – M99)
Fourteen Disease of the Genitourinary System (N00 – N99)
Fifteen Pregnancy, Childbirth and the Puerperium (O00 – O9A)
Sixteen Certain Conditions Origination in the Perinatal Period (P00- P96)
Seventeen Congenital Malformations, Deformations and Chromosomal Abnormalities
(Q00 – Q99)
Eighteen Symptoms, Signs and Abnormal Clinical and LaboratoryFindings, NEC
(R00 – R99)
Nineteen Injury, Poisoning and Certain Other Consequences of External Causes
(S00 – T88)
Twenty External Causes of Morbidity (V00 – Y99)
Twenty One Factors influencing Health Status and Contact with Health Services
(Z00 – Z99)
Three Character listings
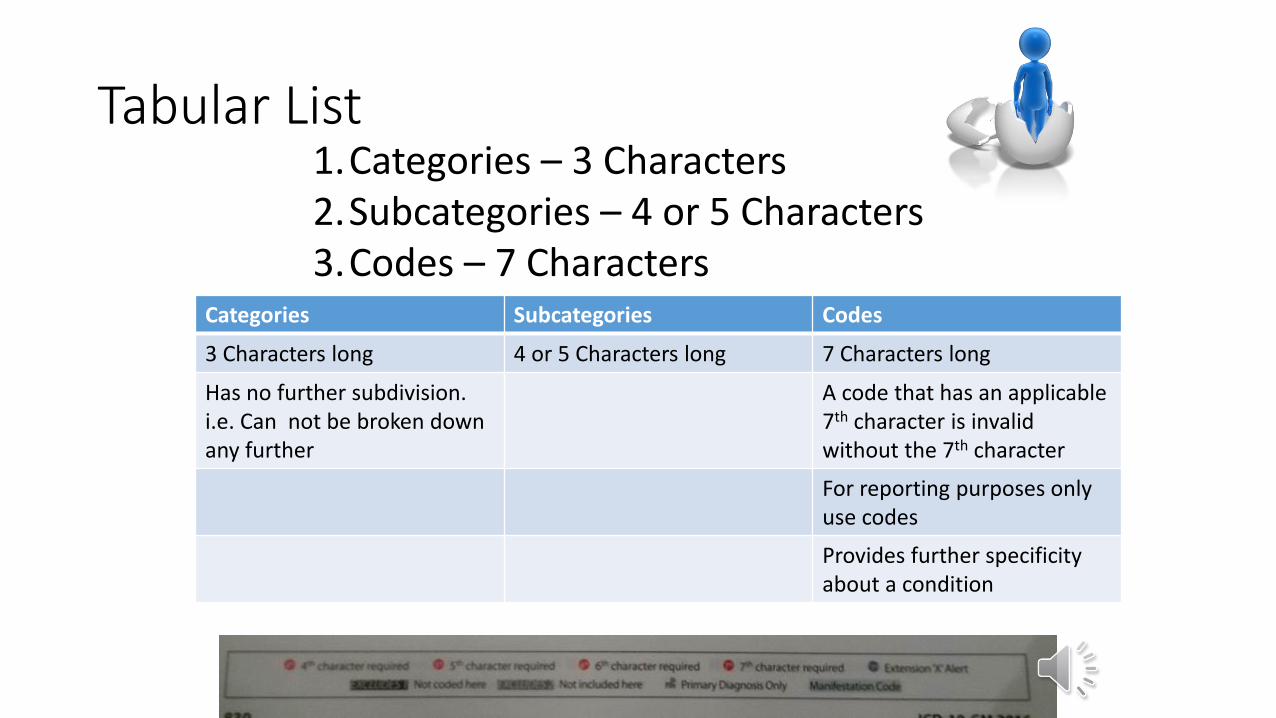
Tabular List
Categories Subcategories Codes
3 Characters long 4 or 5 Characters long 7 Characters long
Has no further subdivision. i.e. Can not be broken down any further
A code that has an applicable 7th character is invalid without the 7th character
For reporting purposes only use codes
Provides further specificity about a condition
1.Categories – 3 Characters2.Subcategories – 4 or 5 Characters3.Codes – 7 Characters
Conventions: Abbreviations
NEC – Not Elsewhere Classifiable NOS – Not Otherwise Specified
Used in both the Index and Tabular list to indicate that there is no separate code for the condition even though the provider’s diagnosis may be very specific
Equivalent of unspecified and is used in both the Index and Tabular list to indicated that the documentation was not specific enough to assign a more specified code
Means the book simply didn’t have enough room for it
Means the doctor wasn’t specific
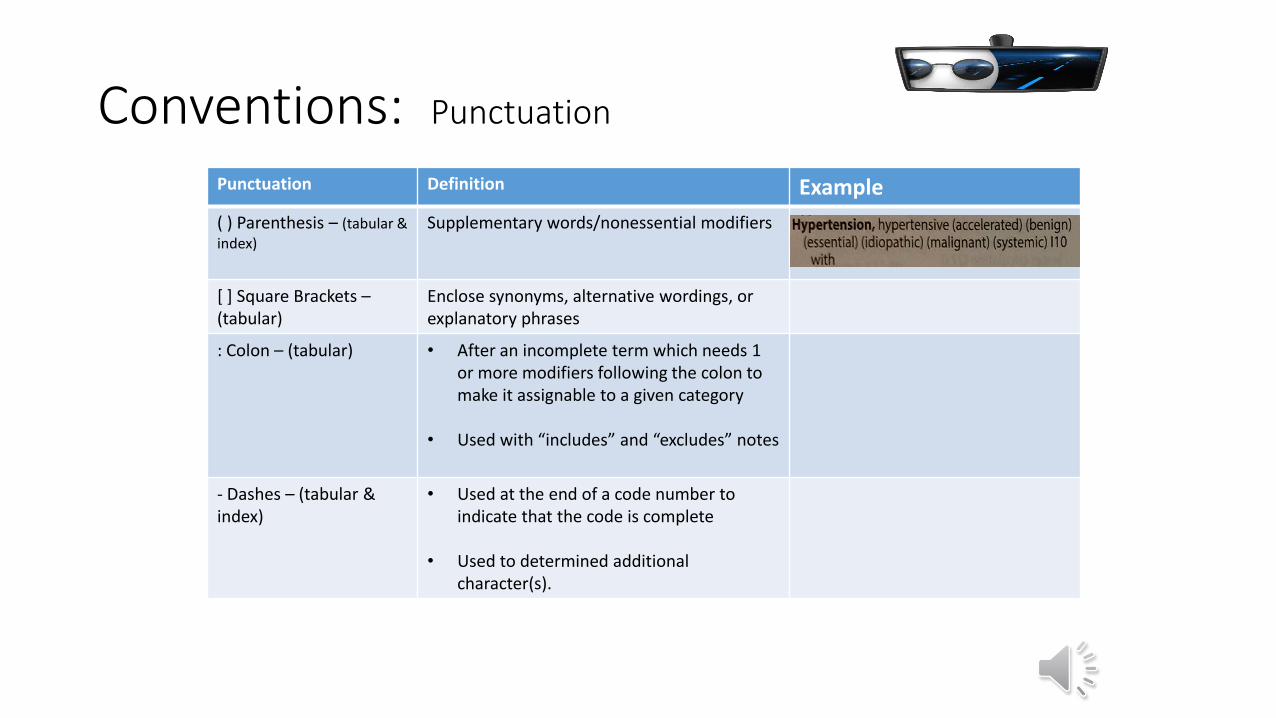
Conventions: Punctuation
Punctuation Definition Example
( ) Parenthesis – (tabular &index)
Supplementary words/nonessential modifiers
[ ] Square Brackets –(tabular)
Enclose synonyms, alternative wordings, or explanatory phrases
: Colon – (tabular) • After an incomplete term which needs 1 or more modifiers following the colon to make it assignable to a given category
• Used with “includes” and “excludes” notes
- Dashes – (tabular &index)
• Used at the end of a code number to indicate that the code is complete
• Used to determined additional character(s).
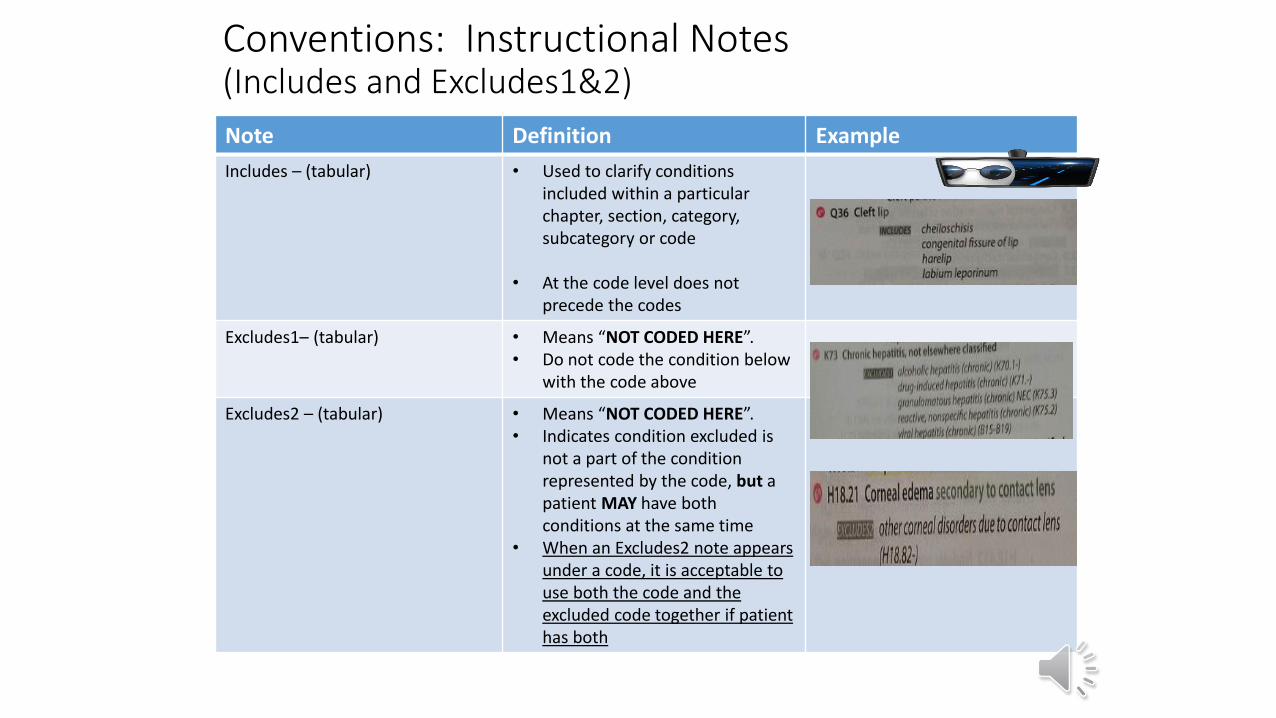
Conventions: Instructional Notes(Includes and Excludes1&2)
Note Definition Example
Includes – (tabular) • Used to clarify conditions included within a particular chapter, section, category, subcategory or code
• At the code level does not precede the codes
Excludes1– (tabular) • Means “NOT CODED HERE”.• Do not code the condition below
with the code above
Excludes2 – (tabular) • Means “NOT CODED HERE”.• Indicates condition excluded is
not a part of the condition represented by the code, but a patient MAY have both conditions at the same time
• When an Excludes2 note appears under a code, it is acceptable to use both the code and the excluded code together if patient has both
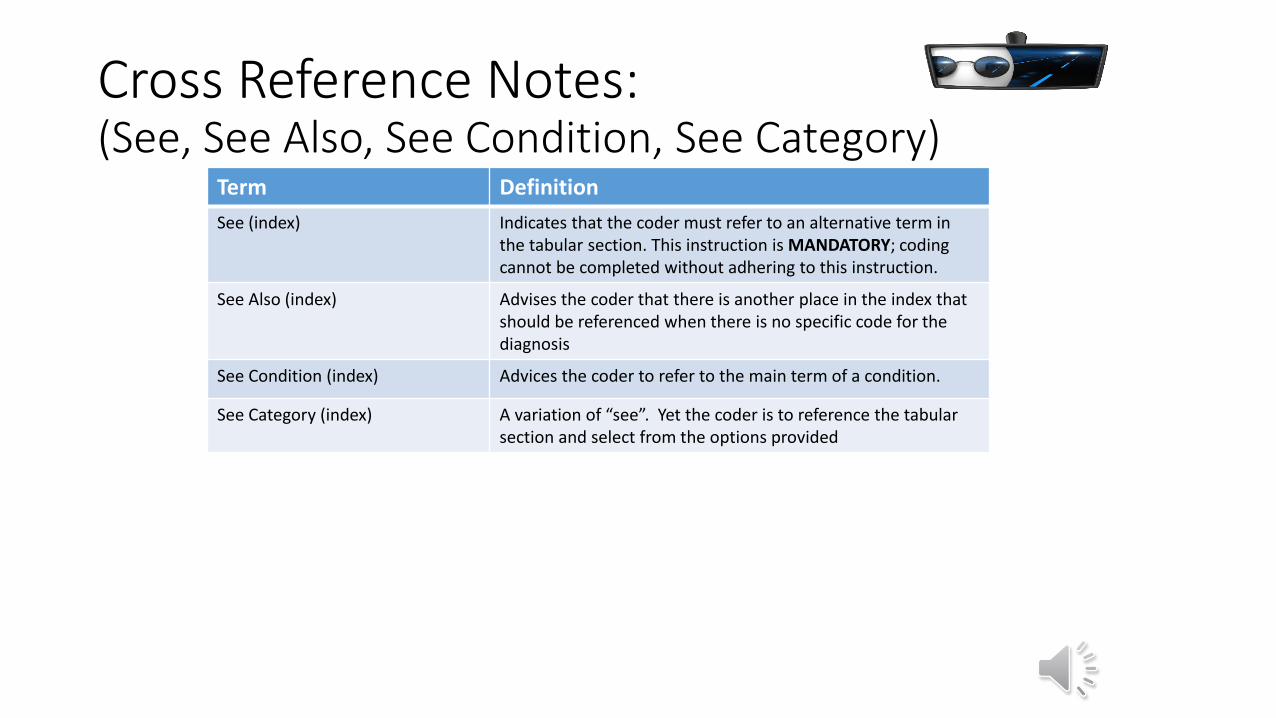
Cross Reference Notes: (See, See Also, See Condition, See Category)
Term Definition
See (index) Indicates that the coder must refer to an alternative term in the tabular section. This instruction is MANDATORY; coding cannot be completed without adhering to this instruction.
See Also (index) Advises the coder that there is another place in the index that should be referenced when there is no specific code for the diagnosis
See Condition (index) Advices the coder to refer to the main term of a condition.
See Category (index) A variation of “see”. Yet the coder is to reference the tabular section and select from the options provided
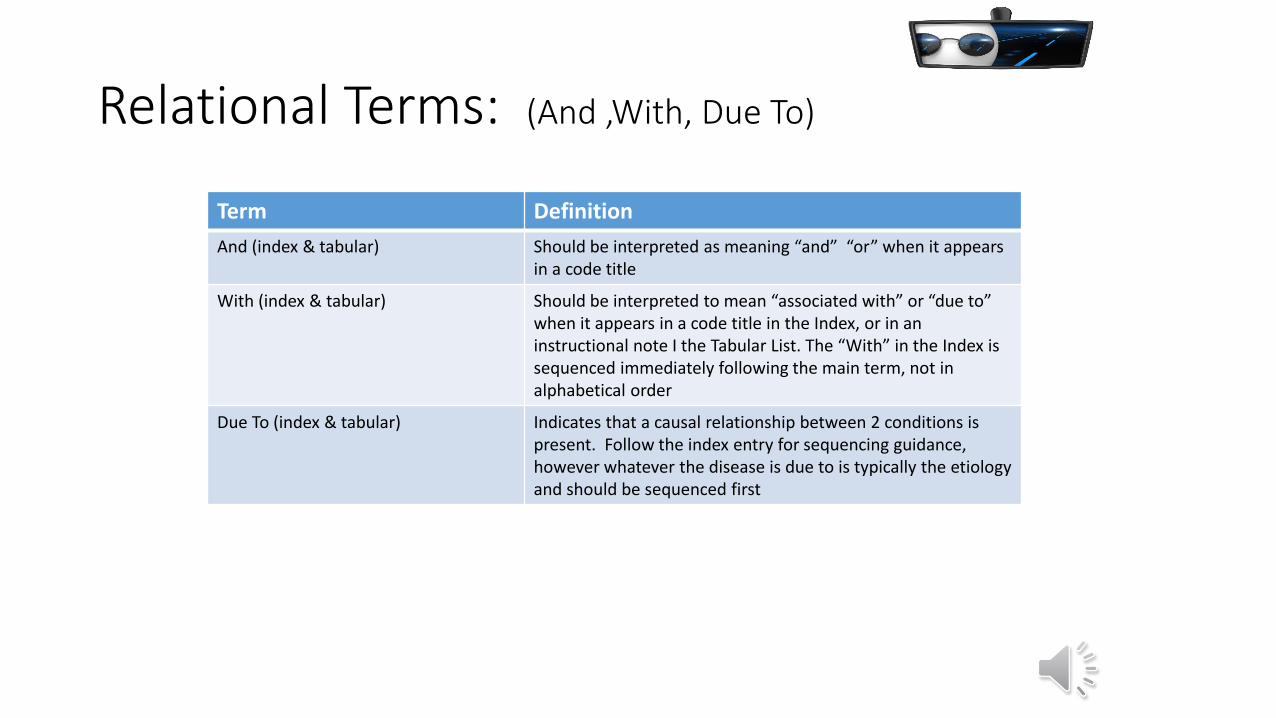
Relational Terms: (And ,With, Due To)
Term Definition
And (index & tabular) Should be interpreted as meaning “and” “or” when it appears in a code title
With (index & tabular) Should be interpreted to mean “associated with” or “due to” when it appears in a code title in the Index, or in an instructional note I the Tabular List. The “With” in the Index is sequenced immediately following the main term, not in alphabetical order
Due To (index & tabular) Indicates that a causal relationship between 2 conditions is present. Follow the index entry for sequencing guidance, however whatever the disease is due to is typically the etiology and should be sequenced first
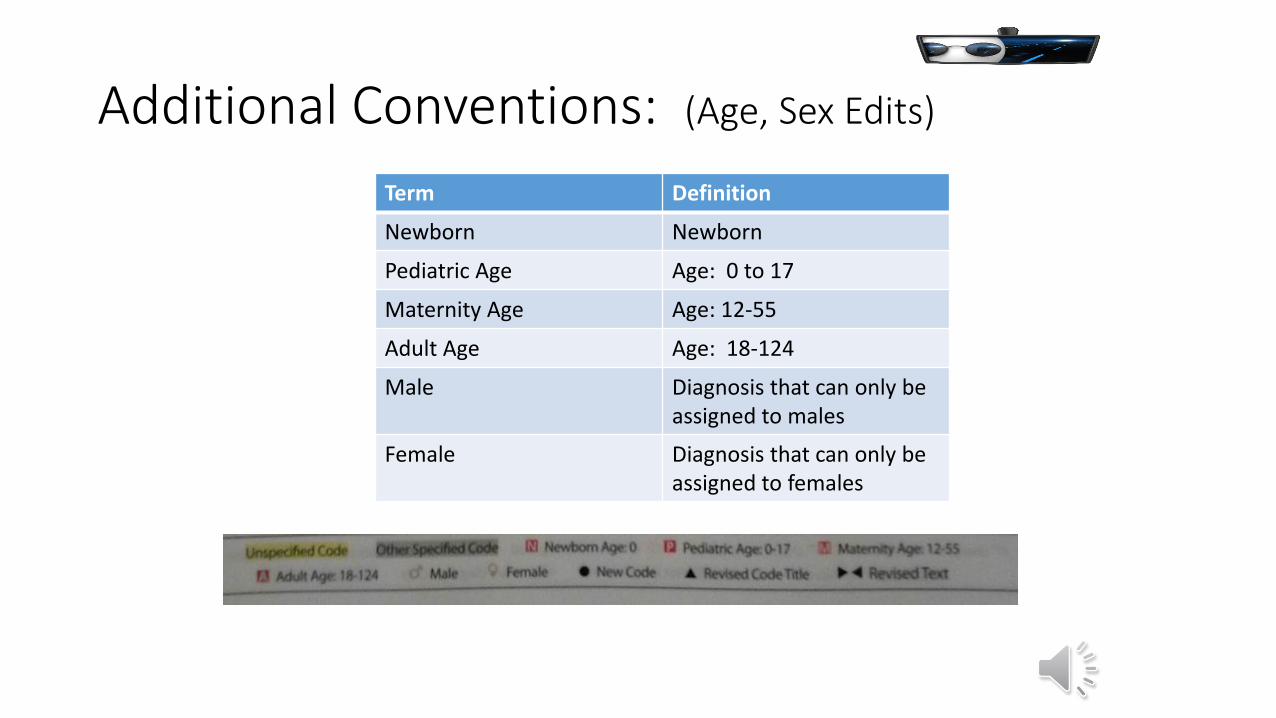
Additional Conventions: (Age, Sex Edits)
Term Definition
Newborn Newborn
Pediatric Age Age: 0 to 17
Maternity Age Age: 12-55
Adult Age Age: 18-124
Male Diagnosis that can only be assigned to males
Female Diagnosis that can only be assigned to females
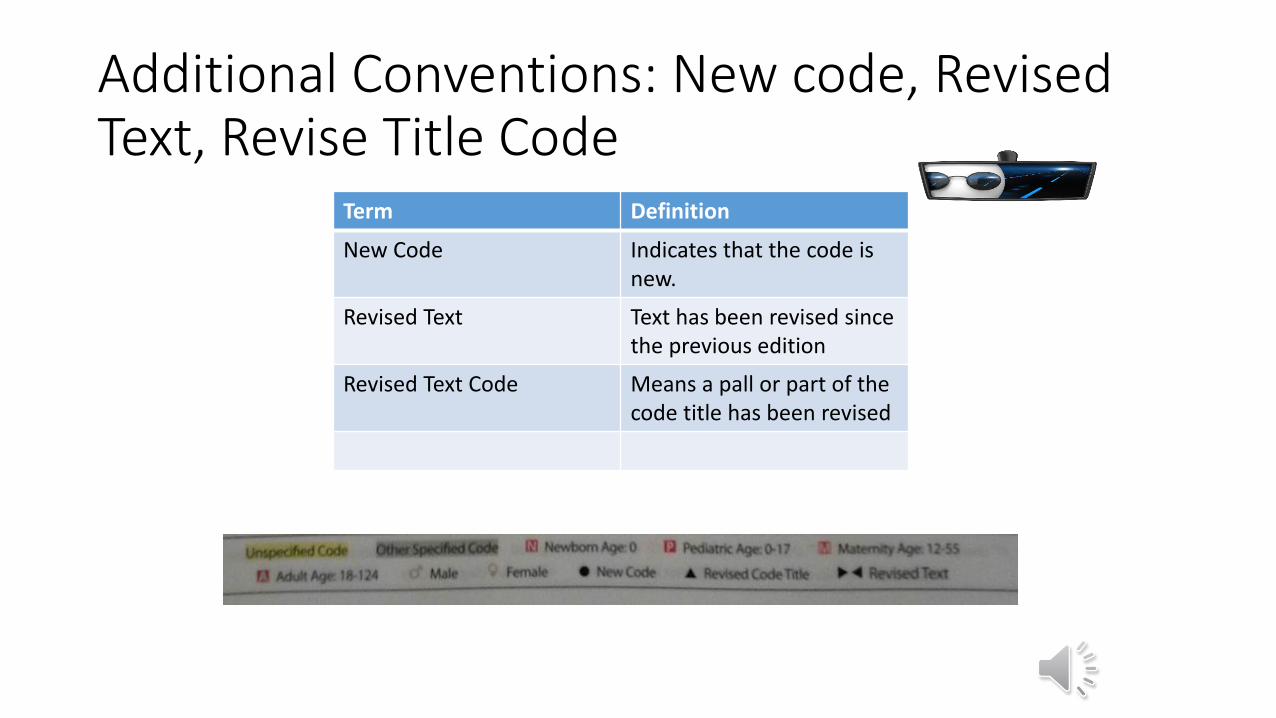
Additional Conventions: New code, Revised Text, Revise Title Code
Term Definition
New Code Indicates that the code is new.
Revised Text Text has been revised since the previous edition
Revised Text Code Means a pall or part of the code title has been revised
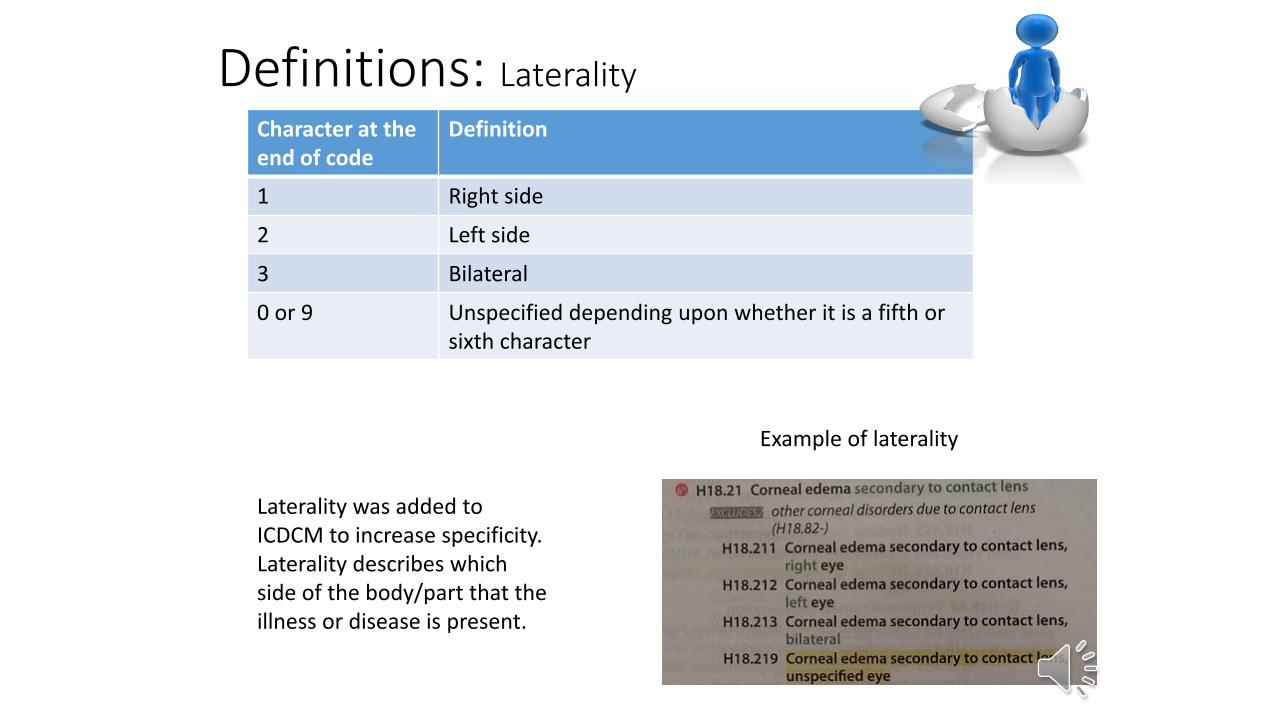
Definitions: Laterality
Character at theend of code
Definition
1 Right side
2 Left side
3 Bilateral
0 or 9 Unspecified depending upon whether it is a fifth or sixth character
Example of laterality
Laterality was added to ICDCM to increase specificity. Laterality describes which side of the body/part that the illness or disease is present.
Definitions: Granularity & Combination code
Term Definition Example
Granularity Refers to the level of hierarchy and the amount of information provided in the code description.
More specific and definitive language within a code
Combination Code Two diagnosis, either a diagnosis with an associated sign or symptom or a diagnosis with an associated complication.
Definition: Principal Diagnosis & First Listed Diagnosis
Term Definition
Principal Diagnosis The condition established after study to be chiefly responsible for occasioning the admission of the patient to the hospital for care
First Listed/Primary The condition established after study to be chiefly responsible for occasioning the admission of the patient to the hospital for care
Definitions: Term Definition ExampleConditions (Signs and Symptoms) that ARE an integral part of a confirmed disease
Do not code Abdominal pain, high fever, the doctor diagnoses the patient with appendicitis, do not code the abdominal pain & high fever only the appendicitis
Conditions (Signs and symptoms) that are NOT an integral part of a confirmed disease or diagnosis
Code them Abdominal pain, high fever the doctordiagnoses the patient with foot pain, code all three: abdominal pain, high fever, and foot pain.
Multiple coding for a single condition When 2 codes are required for a single condition. Reference the notes for sequencing order and for combination codes.
Seek first the combination code, then seek the individual codes
Signs and Symptoms Codes the describe symptoms and signs as opposed to diagnosis and are acceptable to report in the absence of a diagnosis.
Abdominal pain, high fever, the doctor diagnoses the patient with r/o appendicitis, do not code r/o appendicitis. Only code the abdominal pain & high fever.
Acute and Chronic Conditions in thesame setting
Sequence the Acute/subacute condition first then the Chronic Acute Pharyngitis and Chronic Pharyngitis. Sequence Acute Pharyngitis first.
Sequela (late effects) Is the residual effect after the acute phase of an illness or injury has terminated.
CVA (Cerebral Vascular Accident) can cause Dysphasia, or an Acute Fracture can be the cause of a pathological fracture. Its 7th character encounter is ‘S.’ There is no time limit for when a sequela “S” code can be used.
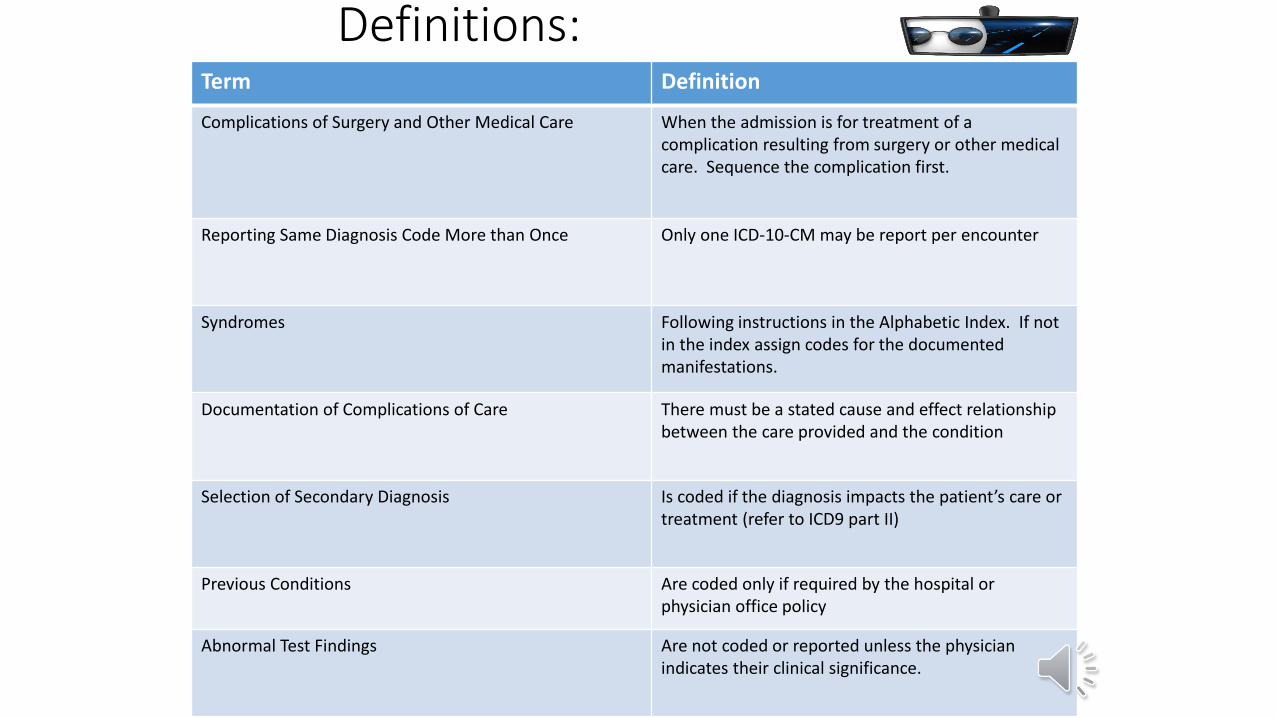
Definitions: Term Definition
Complications of Surgery and Other Medical Care When the admission is for treatment of a complication resulting from surgery or other medical care. Sequence the complication first.
Reporting Same Diagnosis Code More than Once Only one ICD-10-CM may be report per encounter
Syndromes Following instructions in the Alphabetic Index. If not in the index assign codes for the documented manifestations.
Documentation of Complications of Care There must be a stated cause and effect relationship between the care provided and the condition
Selection of Secondary Diagnosis Is coded if the diagnosis impacts the patient’s care or treatment (refer to ICD9 part II)
Previous Conditions Are coded only if required by the hospital or physician office policy
Abnormal Test Findings Are not coded or reported unless the physician indicates their clinical significance.
Other facts about ICD 10 CM
• ICD-10-CM codes are alphanumeric and include all letters except "U," thus providing a greater pool of code numbers.
• ICD-9-CM’s V and E codes are incorporated into the main classification in ICD-10-CM.
• The length of codes in ICD-10-CM can be a maximum of seven characters (digits and letters) as opposed to ICD-9-CM’s five digits.
• ICD-10-CM offers the addition of information relative to ambulatory and managed care encounters.
• Conditions that are new or that were not uniquely identified in ICD-9-CM have been assigned code numbers in ICD-10-CM.
• In ICD-10-CM, some three-character categories are not used in order to allow for revisions and future expansion.
• Instead of grouping by categories of injury or type of wound, ICD-10-CM groups injuries by site of the injury and then the type.
• Excludes notes were expanded in order to provide guidance on the hierarchy of the chapters and to clarify priority of code assignment.
• Some conditions with a new treatment protocol or perhaps a recently discovered or new etiology have been listed in a more appropriate chapter.
• Combination codes are used for both symptom and diagnosis, and etiology and manifestations—for example K50.03 Crohn’s disease of small intestine with fistula.
• Codes for postoperative complications have been expanded. Also a distinction has been made between intraoperative complications and post-procedural disorders—for example, K91 Intraoperative and postprocedural complications and disorders of digestive system, NEC.
• Implementation of ICD-10 in other Countries
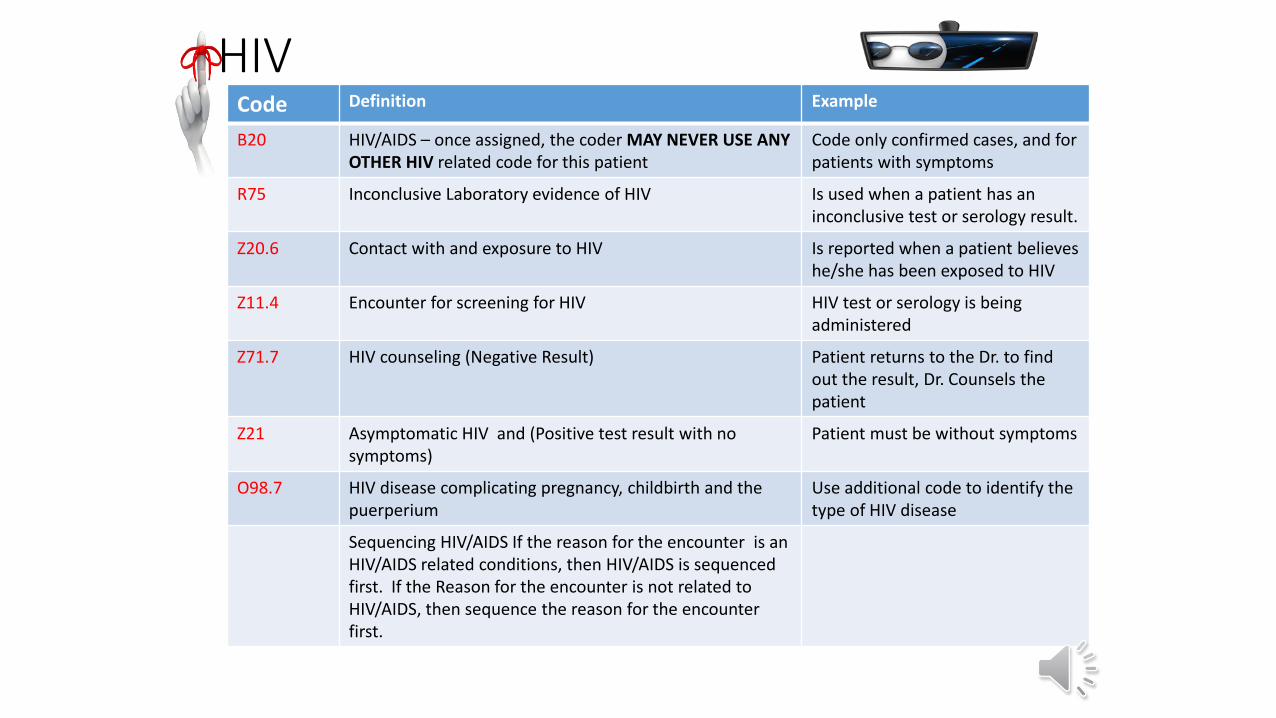
HIVCode Definition Example
B20 HIV/AIDS – once assigned, the coder MAY NEVER USE ANY OTHER HIV related code for this patient
Code only confirmed cases, and for patients with symptoms
R75 Inconclusive Laboratory evidence of HIV Is used when a patient has an inconclusive test or serology result.
Z20.6 Contact with and exposure to HIV Is reported when a patient believes he/she has been exposed to HIV
Z11.4 Encounter for screening for HIV HIV test or serology is being administered
Z71.7 HIV counseling (Negative Result) Patient returns to the Dr. to find out the result, Dr. Counsels the patient
Z21 Asymptomatic HIV and (Positive test result with no symptoms)
Patient must be without symptoms
O98.7 HIV disease complicating pregnancy, childbirth and the puerperium
Use additional code to identify the type of HIV disease
Sequencing HIV/AIDS If the reason for the encounter is an HIV/AIDS related conditions, then HIV/AIDS is sequenced first. If the Reason for the encounter is not related to HIV/AIDS, then sequence the reason for the encounter first.
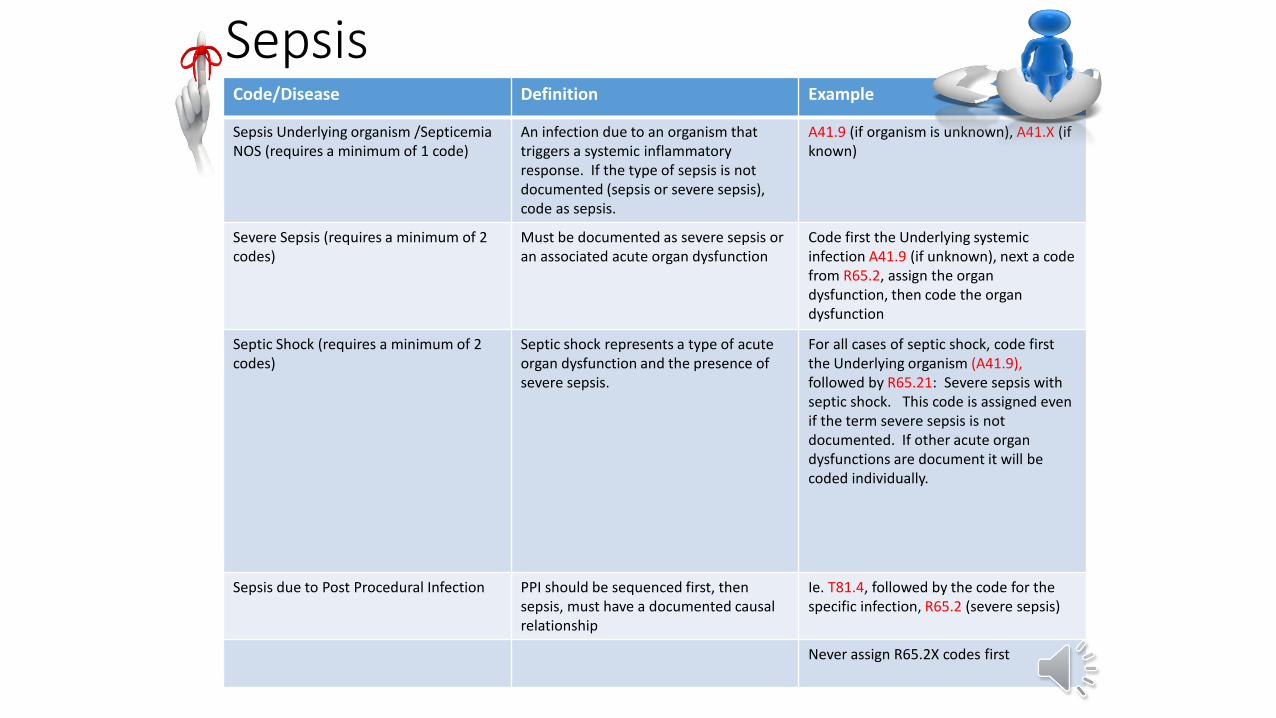
SepsisCode/Disease Definition Example
Sepsis Underlying organism /SepticemiaNOS (requires a minimum of 1 code)
An infection due to an organism that triggers a systemic inflammatory response. If the type of sepsis is not documented (sepsis or severe sepsis), code as sepsis.
A41.9 (if organism is unknown), A41.X (if known)
Severe Sepsis (requires a minimum of 2 codes)
Must be documented as severe sepsis or an associated acute organ dysfunction
Code first the Underlying systemic infection A41.9 (if unknown), next a code from R65.2, assign the organ dysfunction, then code the organ dysfunction
Septic Shock (requires a minimum of 2 codes)
Septic shock represents a type of acute organ dysfunction and the presence of severe sepsis.
For all cases of septic shock, code first the Underlying organism (A41.9), followed by R65.21: Severe sepsis with septic shock. This code is assigned even if the term severe sepsis is not documented. If other acute organ dysfunctions are document it will be coded individually.
Sepsis due to Post Procedural Infection PPI should be sequenced first, then sepsis, must have a documented causal relationship
Ie. T81.4, followed by the code for the specific infection, R65.2 (severe sepsis)
Never assign R65.2X codes first
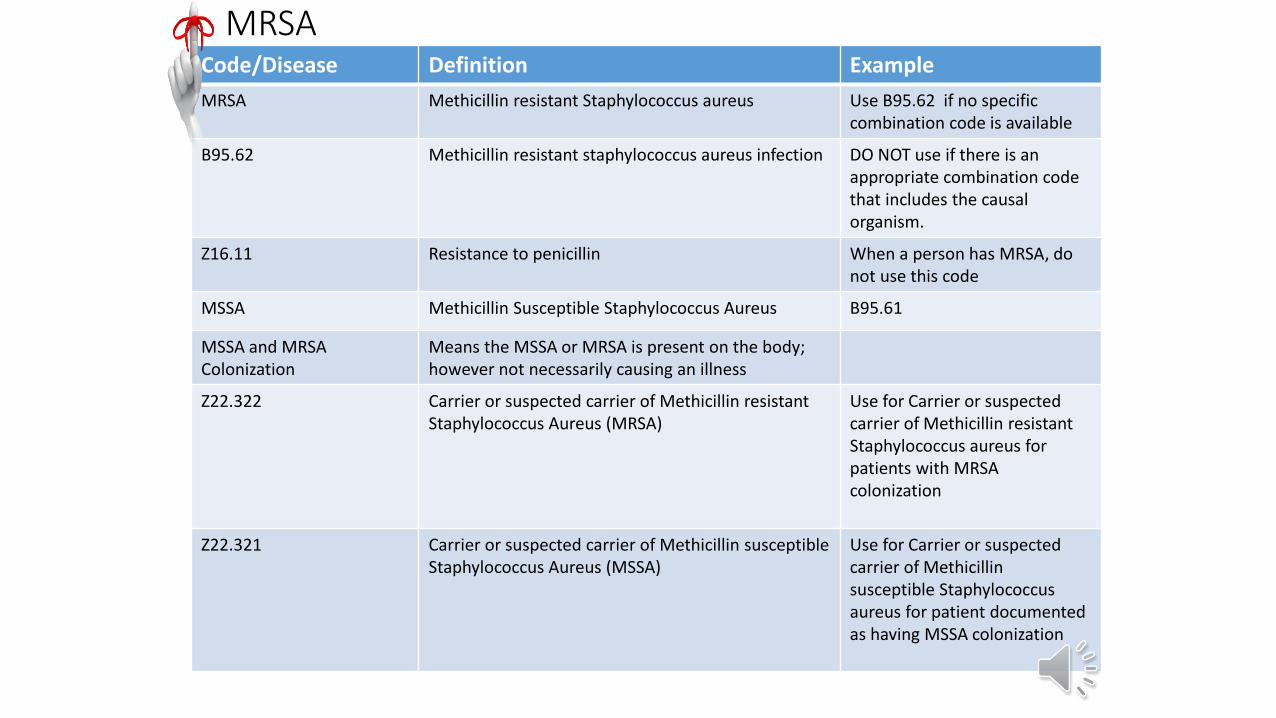
MRSACode/Disease Definition Example
MRSA Methicillin resistant Staphylococcus aureus Use B95.62 if no specific combination code is available
B95.62 Methicillin resistant staphylococcus aureus infection DO NOT use if there is anappropriate combination code that includes the causal organism.
Z16.11 Resistance to penicillin When a person has MRSA, do not use this code
MSSA Methicillin Susceptible Staphylococcus Aureus B95.61
MSSA and MRSA Colonization
Means the MSSA or MRSA is present on the body; however not necessarily causing an illness
Z22.322 Carrier or suspected carrier of Methicillin resistant Staphylococcus Aureus (MRSA)
Use for Carrier or suspected carrier of Methicillin resistant Staphylococcus aureus for patients with MRSA colonization
Z22.321 Carrier or suspected carrier of Methicillin susceptible Staphylococcus Aureus (MSSA)
Use for Carrier or suspected carrier of Methicillinsusceptible Staphylococcus aureus for patient documented as having MSSA colonization
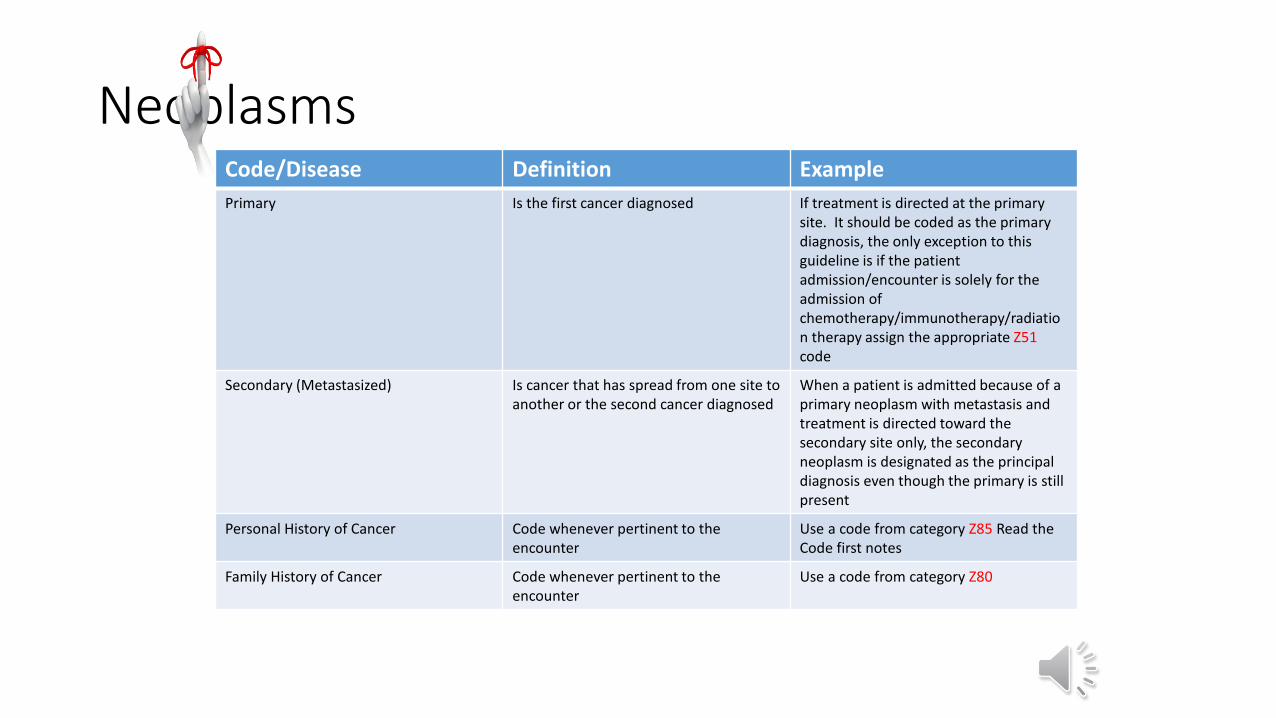
NeoplasmsCode/Disease Definition Example
Primary Is the first cancer diagnosed If treatment is directed at the primary site. It should be coded as the primary diagnosis, the only exception to this guideline is if the patient admission/encounter is solely for the admission of chemotherapy/immunotherapy/radiation therapy assign the appropriate Z51code
Secondary (Metastasized) Is cancer that has spread from one site to another or the second cancer diagnosed
When a patient is admitted because of a primary neoplasm with metastasis and treatment is directed toward the secondary site only, the secondary neoplasm is designated as the principal diagnosis even though the primary is still present
Personal History of Cancer Code whenever pertinent to the encounter
Use a code from category Z85 Read the Code first notes
Family History of Cancer Code whenever pertinent to the encounter
Use a code from category Z80
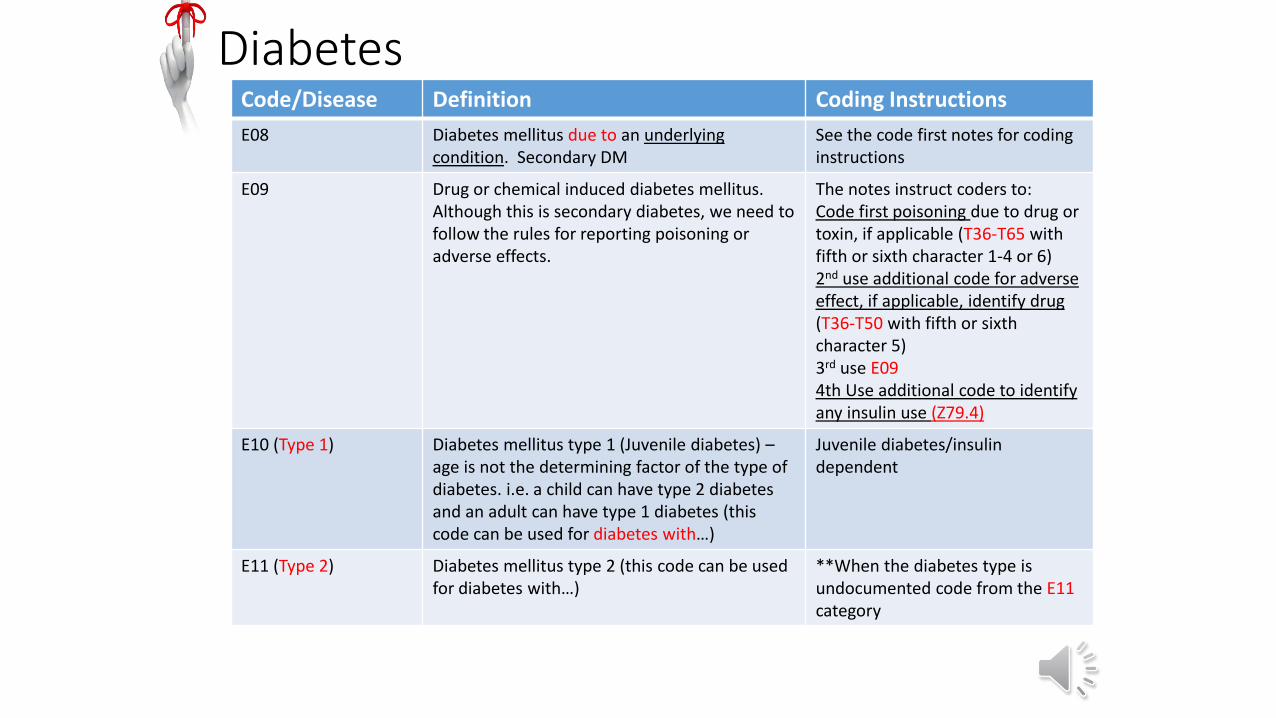
DiabetesCode/Disease Definition Coding Instructions
E08 Diabetes mellitus due to an underlying condition. Secondary DM
See the code first notes for coding instructions
E09 Drug or chemical induced diabetes mellitus. Although this is secondary diabetes, we need to follow the rules for reporting poisoning or adverse effects.
The notes instruct coders to:Code first poisoning due to drug or toxin, if applicable (T36-T65 with fifth or sixth character 1-4 or 6)2nd use additional code for adverse effect, if applicable, identify drug (T36-T50 with fifth or sixth character 5) 3rd use E094th Use additional code to identify any insulin use (Z79.4)
E10 (Type 1) Diabetes mellitus type 1 (Juvenile diabetes) –age is not the determining factor of the type of diabetes. i.e. a child can have type 2 diabetes and an adult can have type 1 diabetes (this code can be used for diabetes with…)
Juvenile diabetes/insulin dependent
E11 (Type 2) Diabetes mellitus type 2 (this code can be used for diabetes with…)
**When the diabetes type is undocumented code from the E11category
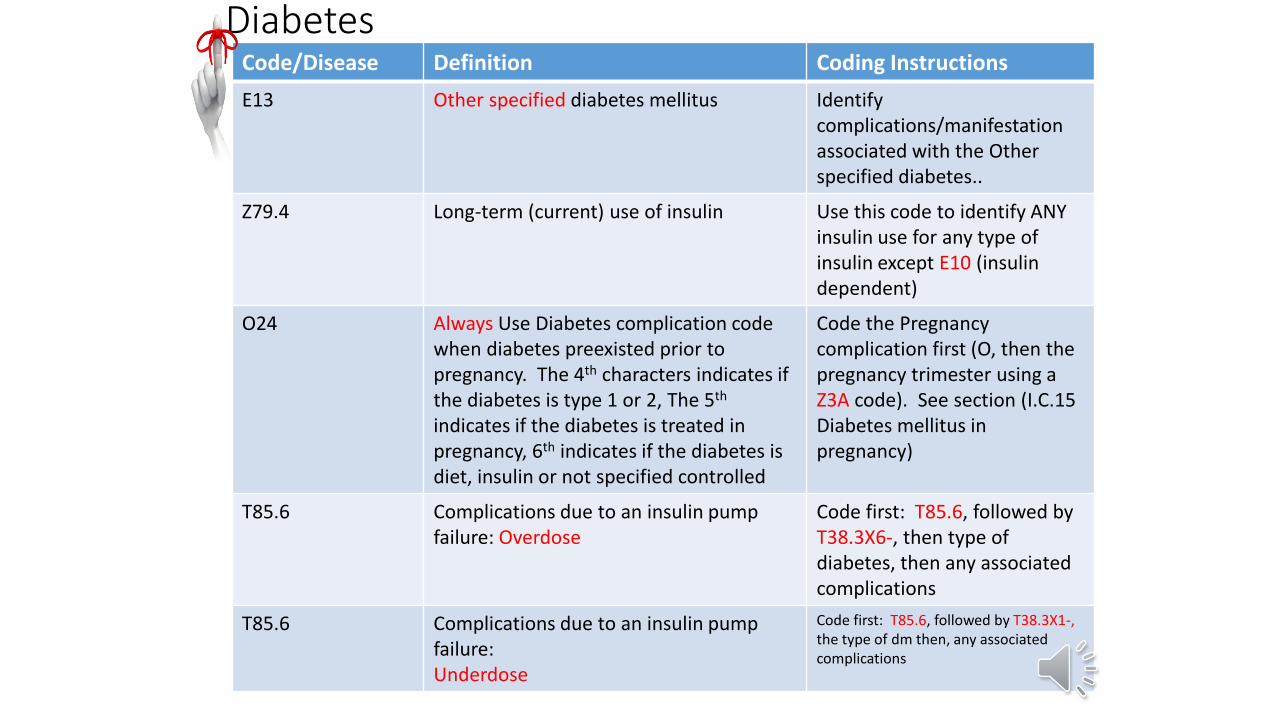
DiabetesCode/Disease Definition Coding Instructions
E13 Other specified diabetes mellitus Identifycomplications/manifestation associated with the Other specified diabetes..
Z79.4 Long-term (current) use of insulin Use this code to identify ANY insulin use for any type of insulin except E10 (insulin dependent)
O24 Always Use Diabetes complication code when diabetes preexisted prior to pregnancy. The 4th characters indicates if the diabetes is type 1 or 2, The 5th
indicates if the diabetes is treated in pregnancy, 6th indicates if the diabetes is diet, insulin or not specified controlled
Code the Pregnancy complication first (O, then the pregnancy trimester using a Z3A code). See section (I.C.15 Diabetes mellitus in pregnancy)
T85.6 Complications due to an insulin pump failure: Overdose
Code first: T85.6, followed by T38.3X6-, then type of diabetes, then any associated complications
T85.6 Complications due to an insulin pump failure:Underdose
Code first: T85.6, followed by T38.3X1-, the type of dm then, any associated complications
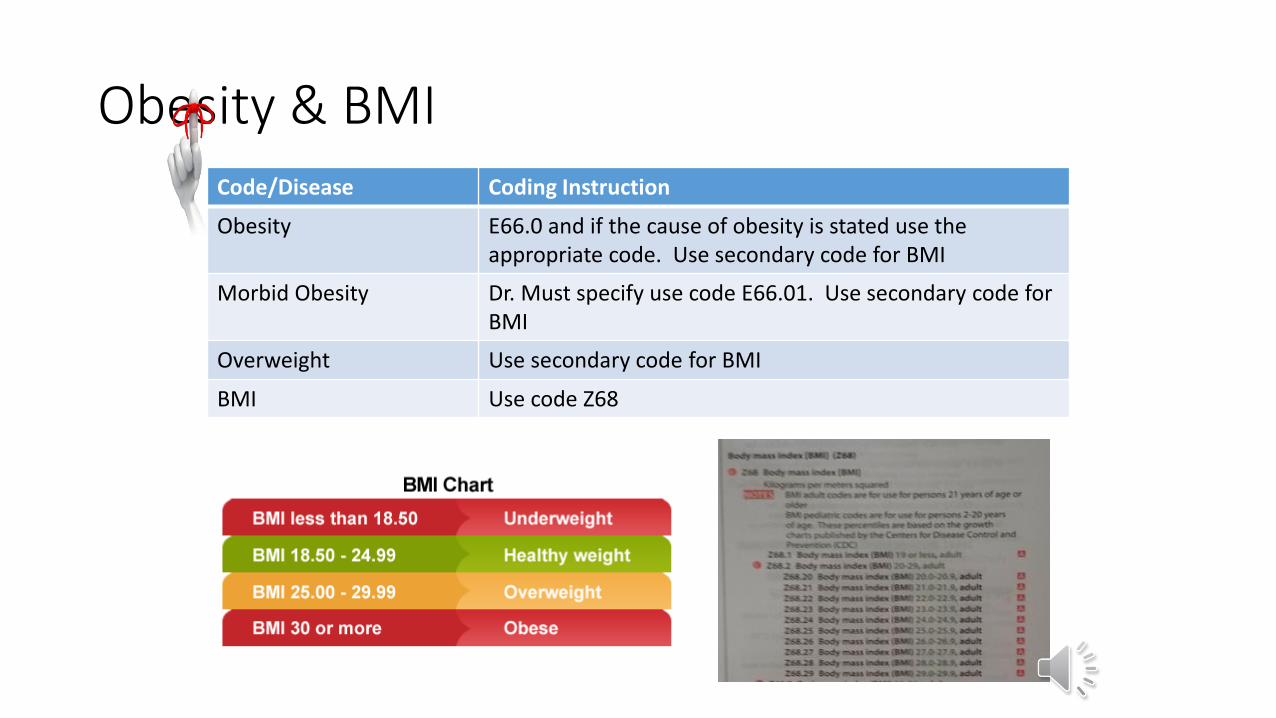
Obesity & BMICode/Disease Coding Instruction
Obesity E66.0 and if the cause of obesity is stated use the appropriate code. Use secondary code for BMI
Morbid Obesity Dr. Must specify use code E66.01. Use secondary code for BMI
Overweight Use secondary code for BMI
BMI Use code Z68
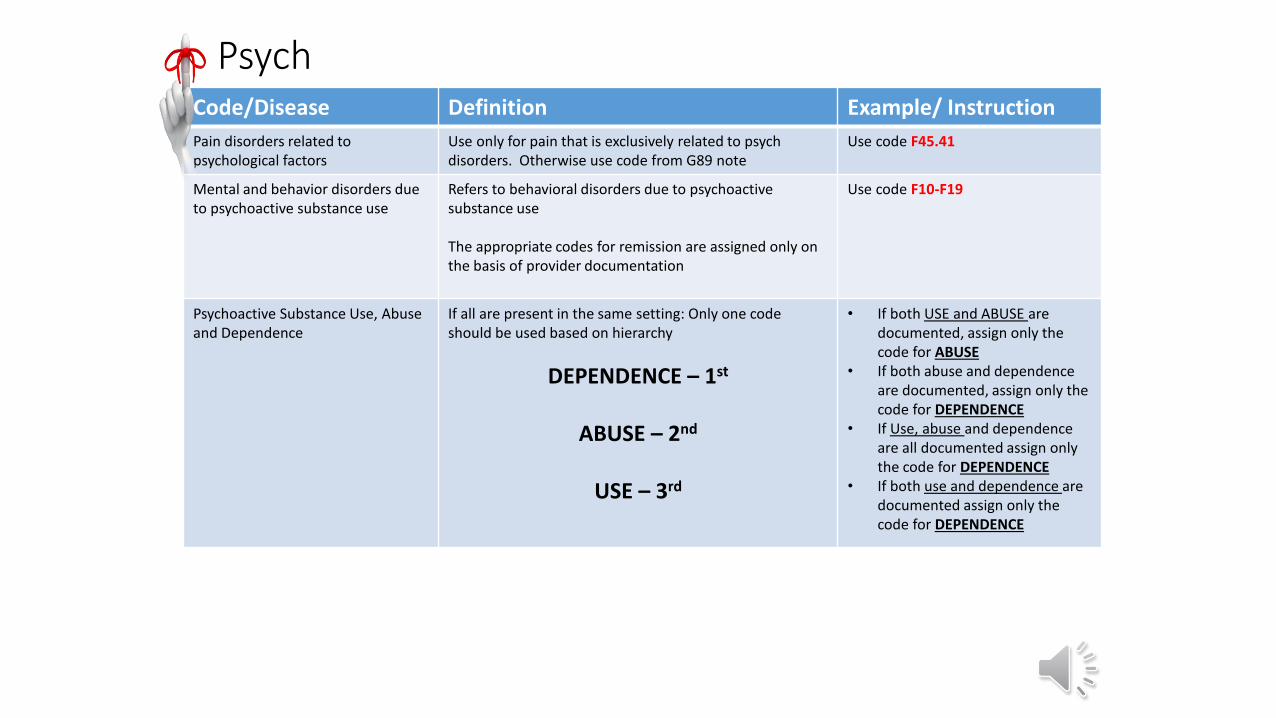
PsychCode/Disease Definition Example/ Instruction
Pain disorders related to psychological factors
Use only for pain that is exclusively related to psych disorders. Otherwise use code from G89 note
Use code F45.41
Mental and behavior disorders due to psychoactive substance use
Refers to behavioral disorders due to psychoactive substance use
The appropriate codes for remission are assigned only on the basis of provider documentation
Use code F10-F19
Psychoactive Substance Use, Abuse and Dependence
If all are present in the same setting: Only one code should be used based on hierarchy
DEPENDENCE – 1st
ABUSE – 2nd
USE – 3rd
• If both USE and ABUSE are documented, assign only the code for ABUSE
• If both abuse and dependence are documented, assign only the code for DEPENDENCE
• If Use, abuse and dependence are all documented assign only the code for DEPENDENCE
• If both use and dependence are documented assign only the code for DEPENDENCE
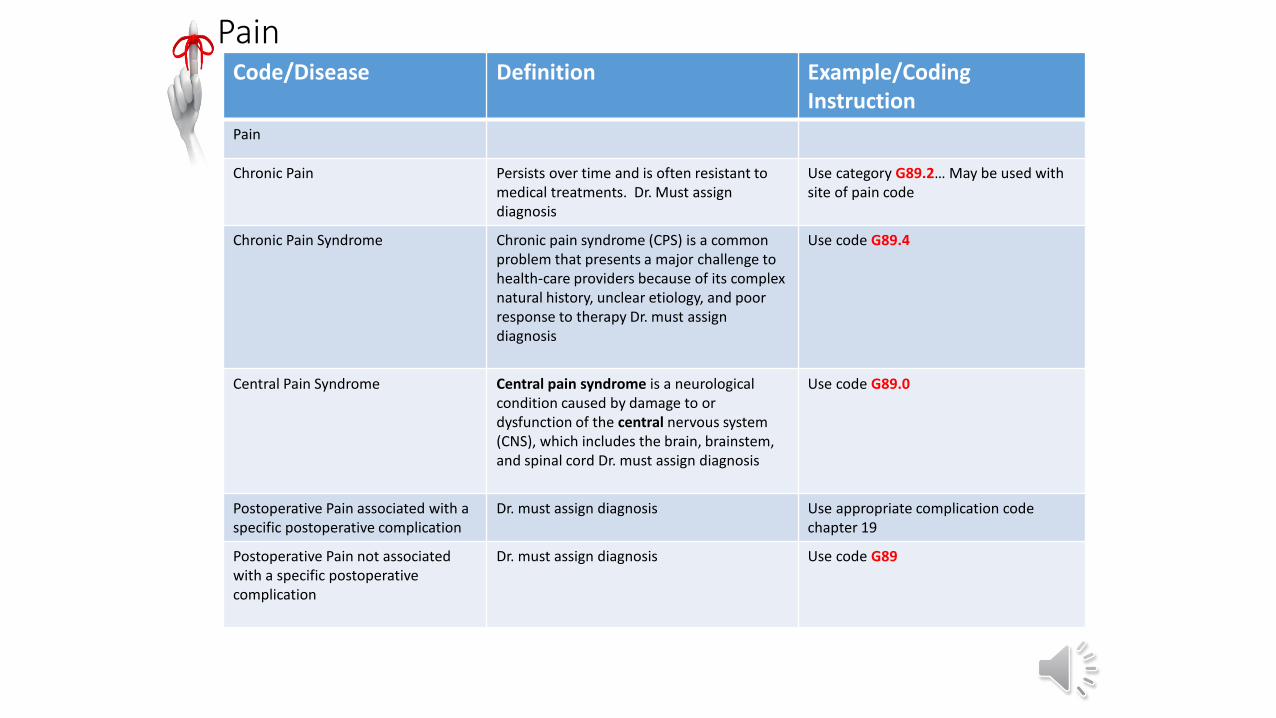
PainCode/Disease Definition Example/Coding
Instruction
Pain
Chronic Pain Persists over time and is often resistant to medical treatments. Dr. Must assign diagnosis
Use category G89.2… May be used with site of pain code
Chronic Pain Syndrome Chronic pain syndrome (CPS) is a common problem that presents a major challenge to health-care providers because of its complex natural history, unclear etiology, and poor response to therapy Dr. must assign diagnosis
Use code G89.4
Central Pain Syndrome Central pain syndrome is a neurological condition caused by damage to or dysfunction of the central nervous system (CNS), which includes the brain, brainstem, and spinal cord Dr. must assign diagnosis
Use code G89.0
Postoperative Pain associated with a specific postoperative complication
Dr. must assign diagnosis Use appropriate complication code chapter 19
Postoperative Pain not associated with a specific postoperative complication
Dr. must assign diagnosis Use code G89
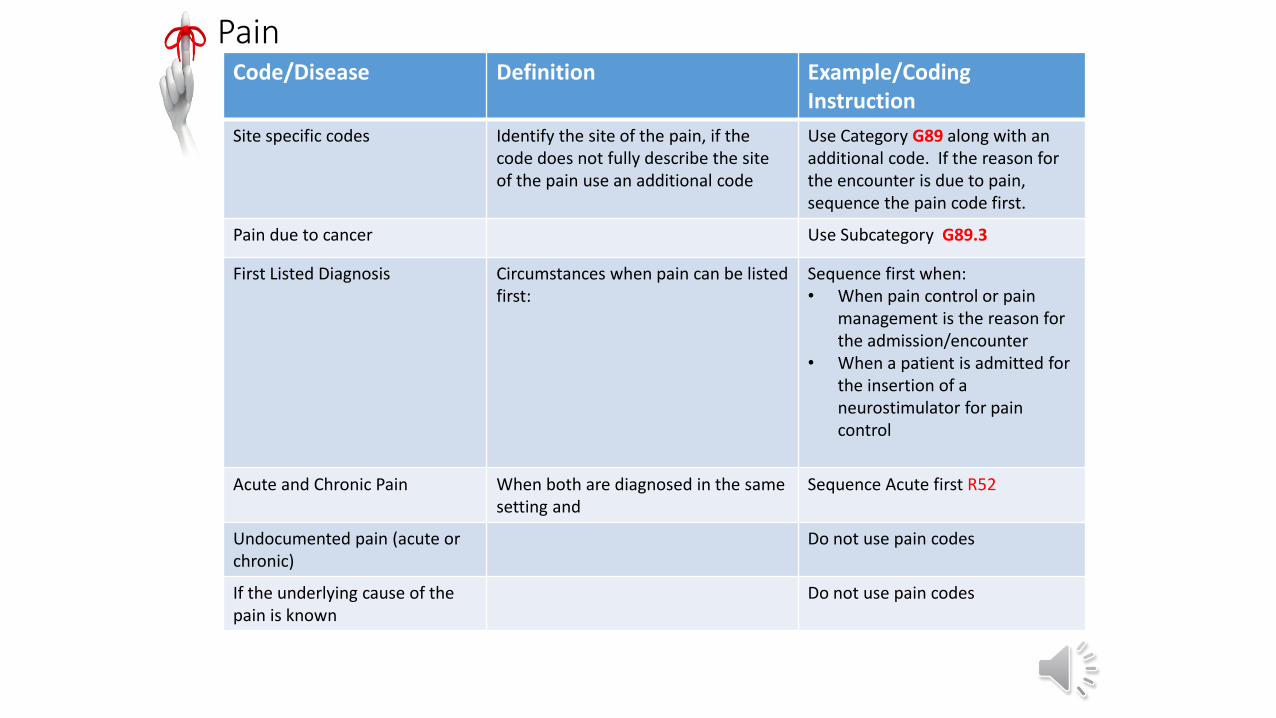
PainCode/Disease Definition Example/Coding
Instruction
Site specific codes Identify the site of the pain, if the code does not fully describe the site of the pain use an additional code
Use Category G89 along with an additional code. If the reason for the encounter is due to pain, sequence the pain code first.
Pain due to cancer Use Subcategory G89.3
First Listed Diagnosis Circumstances when pain can be listed first:
Sequence first when:• When pain control or pain
management is the reason for the admission/encounter
• When a patient is admitted for the insertion of a neurostimulator for pain control
Acute and Chronic Pain When both are diagnosed in the same setting and
Sequence Acute first R52
Undocumented pain (acute or chronic)
Do not use pain codes
If the underlying cause of the pain is known
Do not use pain codes
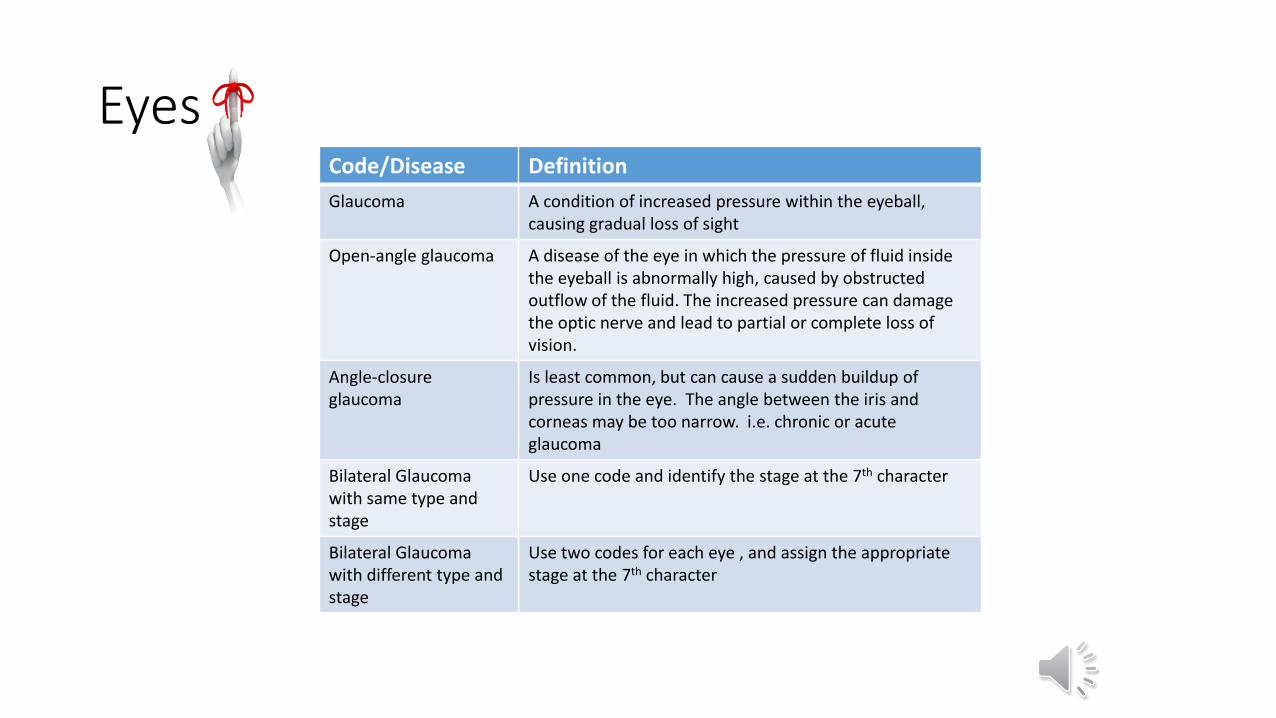
EyesCode/Disease Definition
Glaucoma A condition of increased pressure within the eyeball, causing gradual loss of sight
Open-angle glaucoma A disease of the eye in which the pressure of fluid inside the eyeball is abnormally high, caused by obstructed outflow of the fluid. The increased pressure can damage the optic nerve and lead to partial or complete loss of vision.
Angle-closure glaucoma
Is least common, but can cause a sudden buildup of pressure in the eye. The angle between the iris and corneas may be too narrow. i.e. chronic or acute glaucoma
Bilateral Glaucoma with same type and stage
Use one code and identify the stage at the 7th character
Bilateral Glaucoma with different type and stage
Use two codes for each eye , and assign the appropriate stage at the 7th character
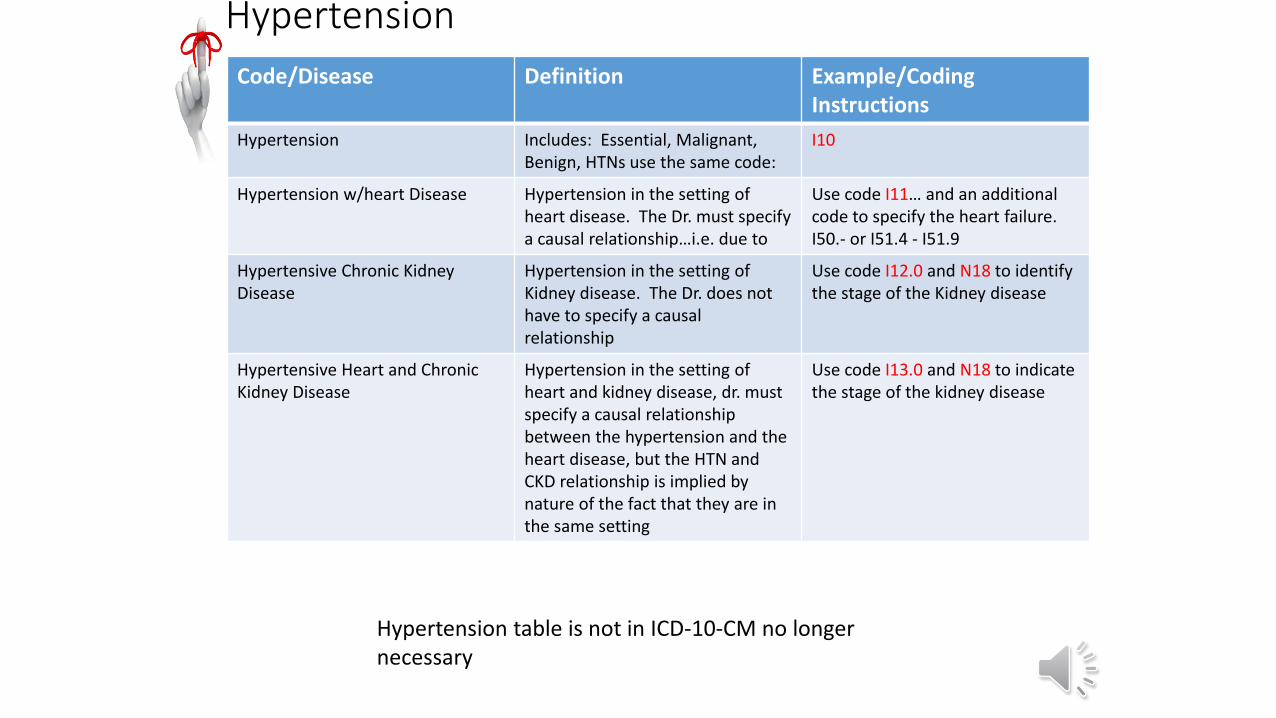
Hypertension
Code/Disease Definition Example/Coding Instructions
Hypertension Includes: Essential, Malignant, Benign, HTNs use the same code:
I10
Hypertension w/heart Disease Hypertension in the setting of heart disease. The Dr. must specify a causal relationship…i.e. due to
Use code I11… and an additional code to specify the heart failure. I50.- or I51.4 - I51.9
Hypertensive Chronic Kidney Disease
Hypertension in the setting of Kidney disease. The Dr. does not have to specify a causal relationship
Use code I12.0 and N18 to identify the stage of the Kidney disease
Hypertensive Heart and Chronic Kidney Disease
Hypertension in the setting of heart and kidney disease, dr. must specify a causal relationship between the hypertension and the heart disease, but the HTN and CKD relationship is implied by nature of the fact that they are in the same setting
Use code I13.0 and N18 to indicate the stage of the kidney disease
Hypertension table is not in ICD-10-CM no longer necessary
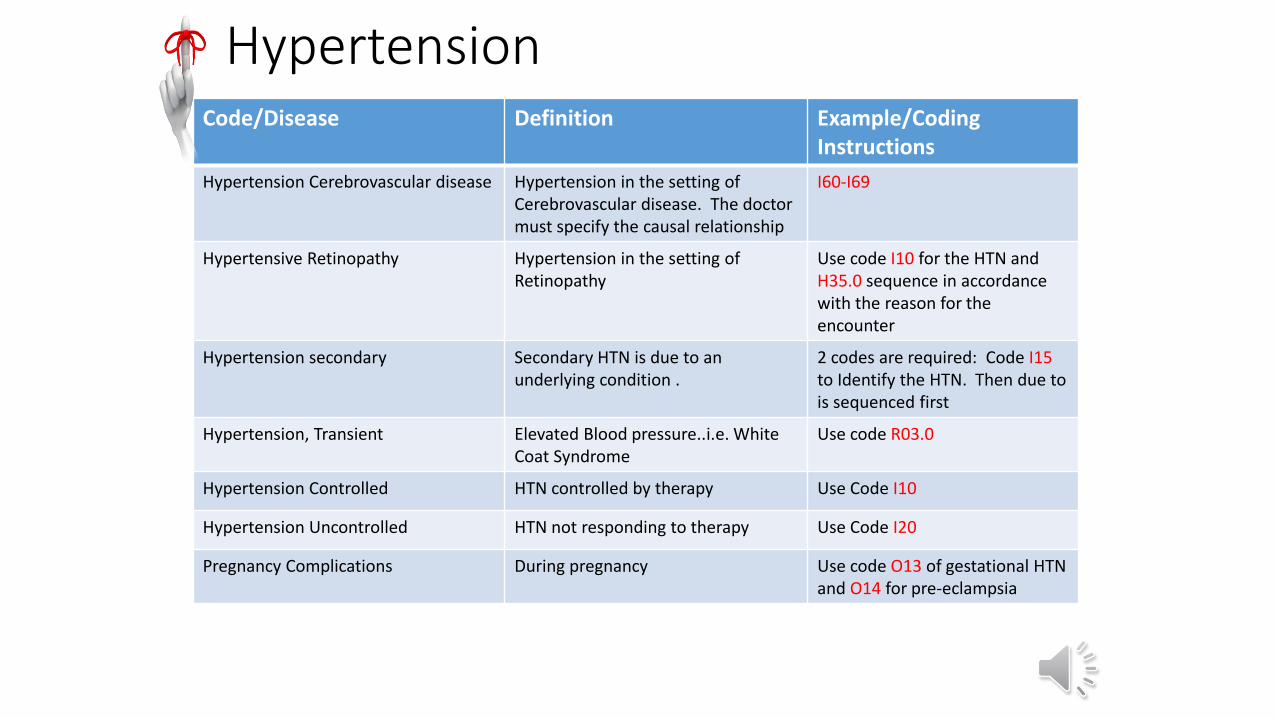
Hypertension Code/Disease Definition Example/Coding
Instructions
Hypertension Cerebrovascular disease Hypertension in the setting of Cerebrovascular disease. The doctor must specify the causal relationship
I60-I69
Hypertensive Retinopathy Hypertension in the setting of Retinopathy
Use code I10 for the HTN and H35.0 sequence in accordance with the reason for the encounter
Hypertension secondary Secondary HTN is due to an underlying condition .
2 codes are required: Code I15 to Identify the HTN. Then due to is sequenced first
Hypertension, Transient Elevated Blood pressure..i.e. White Coat Syndrome
Use code R03.0
Hypertension Controlled HTN controlled by therapy Use Code I10
Hypertension Uncontrolled HTN not responding to therapy Use Code I20
Pregnancy Complications During pregnancy Use code O13 of gestational HTN and O14 for pre-eclampsia
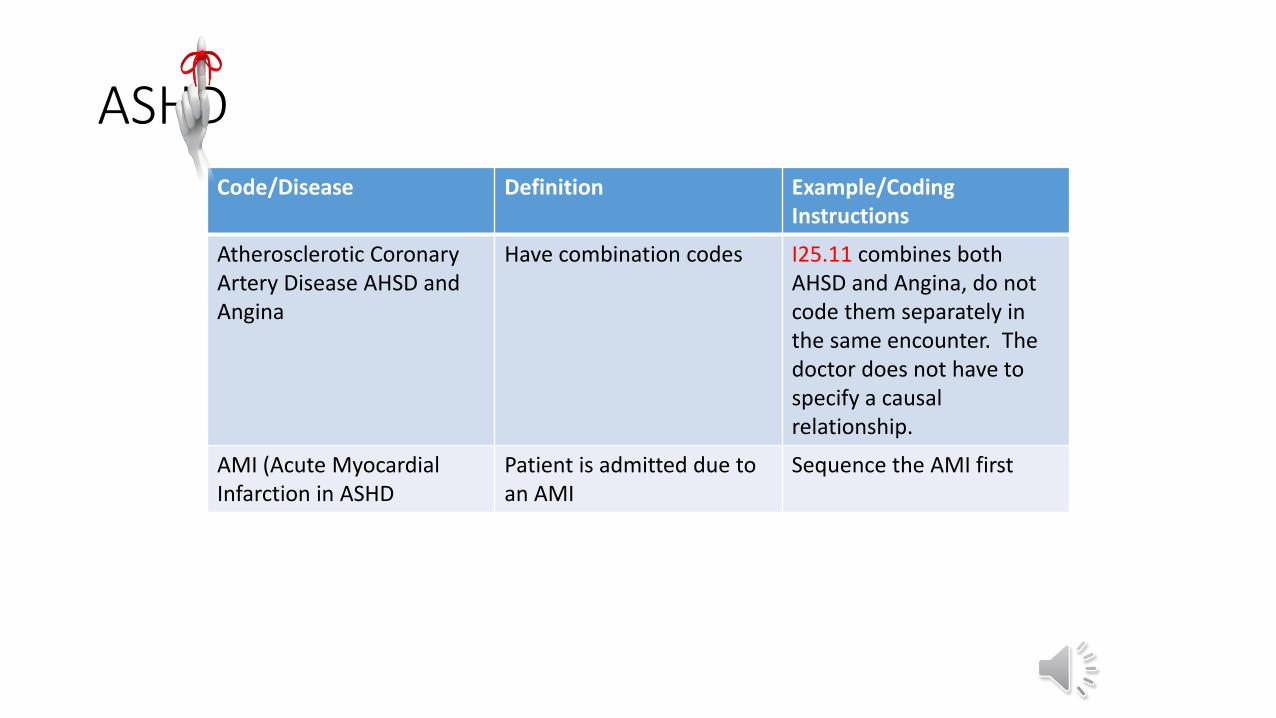
ASHDCode/Disease Definition Example/Coding
Instructions
Atherosclerotic CoronaryArtery Disease AHSD and Angina
Have combination codes I25.11 combines both AHSD and Angina, do not code them separately in the same encounter. The doctor does not have to specify a causal relationship.
AMI (Acute Myocardial Infarction in ASHD
Patient is admitted due to an AMI
Sequence the AMI first
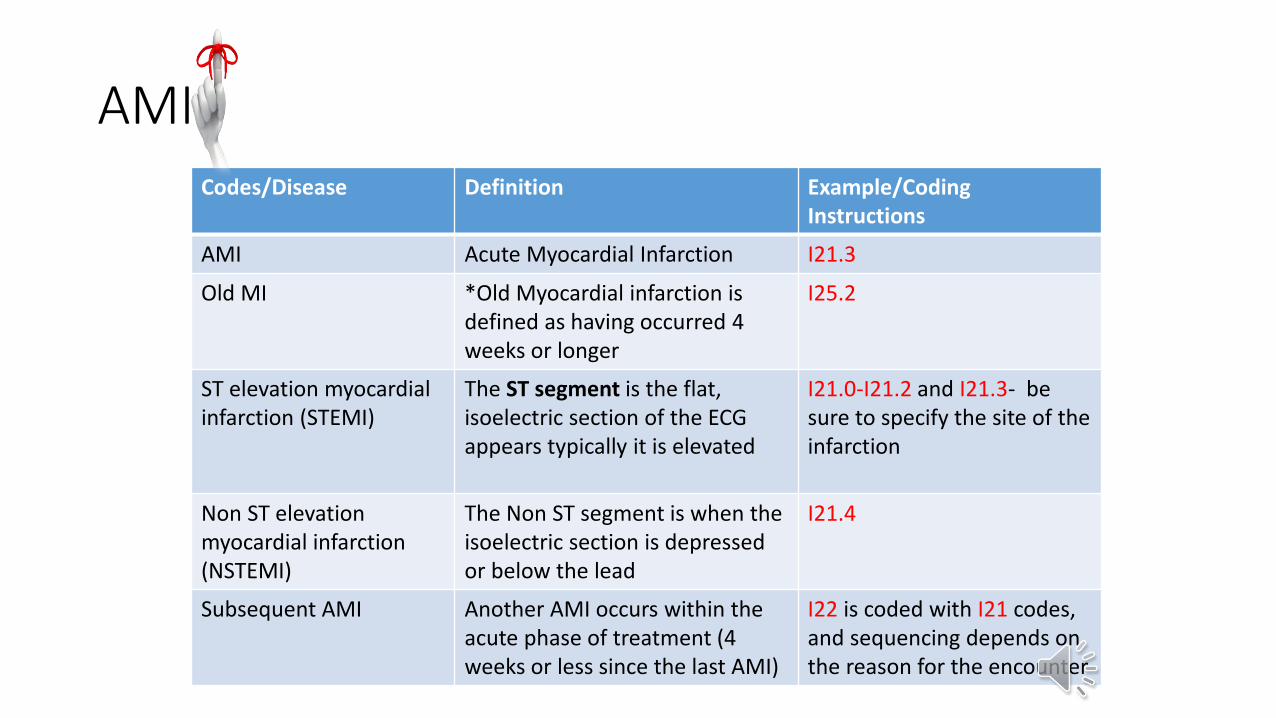
AMICodes/Disease Definition Example/Coding
Instructions
AMI Acute Myocardial Infarction I21.3
Old MI *Old Myocardial infarction is defined as having occurred 4 weeks or longer
I25.2
ST elevation myocardial infarction (STEMI)
The ST segment is the flat, isoelectric section of the ECG appears typically it is elevated
I21.0-I21.2 and I21.3- be sure to specify the site of the infarction
Non ST elevation myocardial infarction (NSTEMI)
The Non ST segment is when the isoelectric section is depressed or below the lead
I21.4
Subsequent AMI Another AMI occurs within the acute phase of treatment (4 weeks or less since the last AMI)
I22 is coded with I21 codes, and sequencing depends on the reason for the encounter
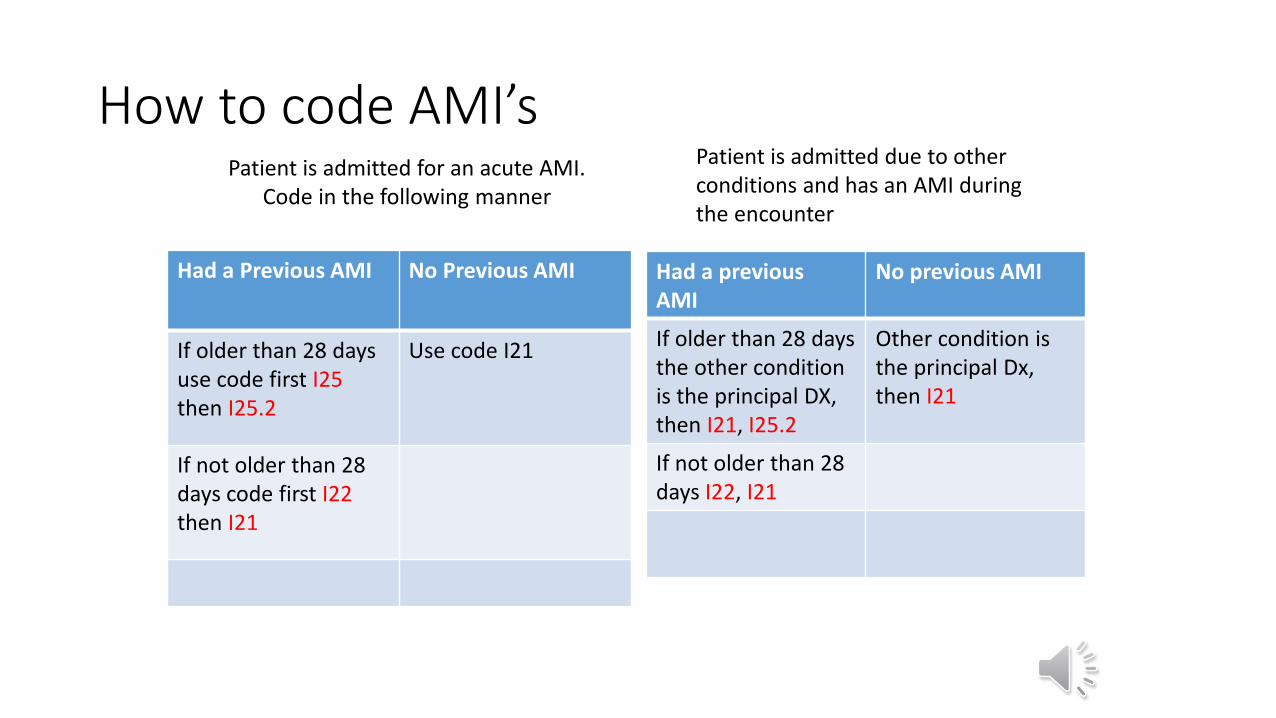
How to code AMI’s
Had a Previous AMI No Previous AMI
If older than 28 daysuse code first I25then I25.2
Use code I21
If not older than 28 days code first I22then I21
Had a previousAMI
No previous AMI
If older than 28 days the other condition is the principal DX, then I21, I25.2
Other condition is the principal Dx, then I21
If not older than 28 days I22, I21
Patient is admitted for an acute AMI. Code in the following manner
Patient is admitted due to other conditions and has an AMI during the encounter
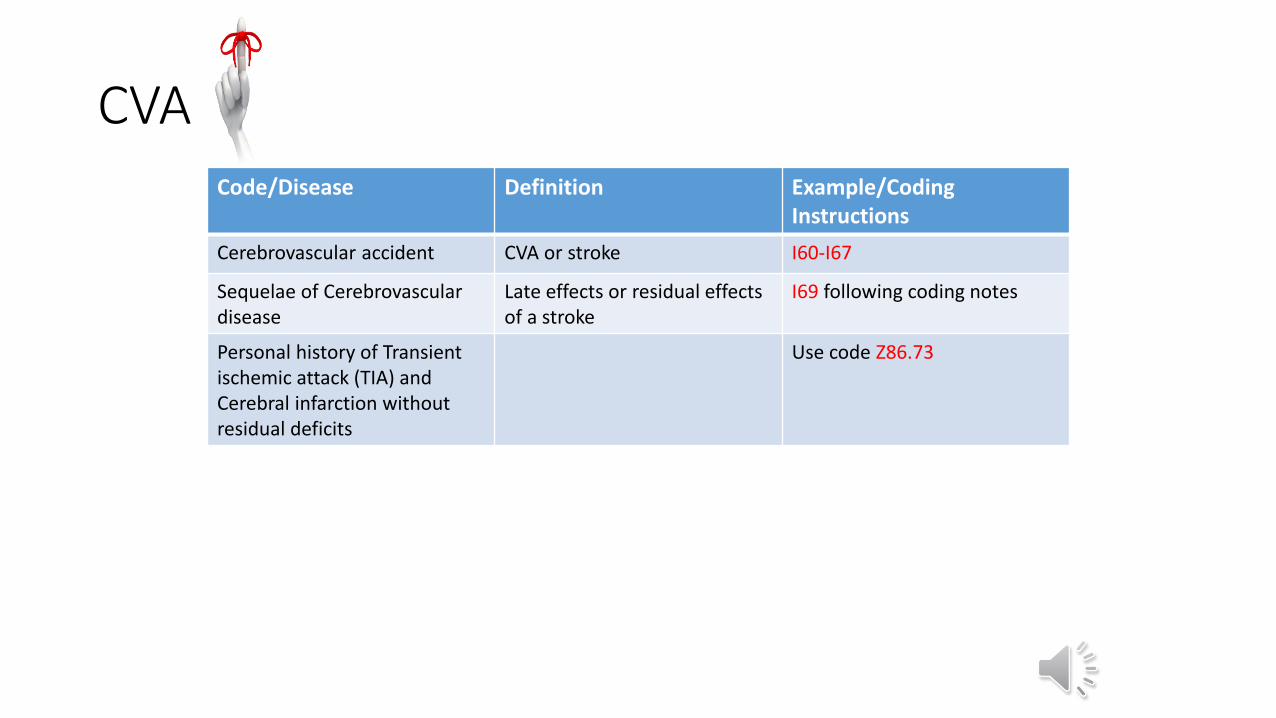
CVA Code/Disease Definition Example/Coding
Instructions
Cerebrovascular accident CVA or stroke I60-I67
Sequelae of Cerebrovasculardisease
Late effects or residual effects of a stroke
I69 following coding notes
Personal history of Transient ischemic attack (TIA) and Cerebral infarction without residual deficits
Use code Z86.73
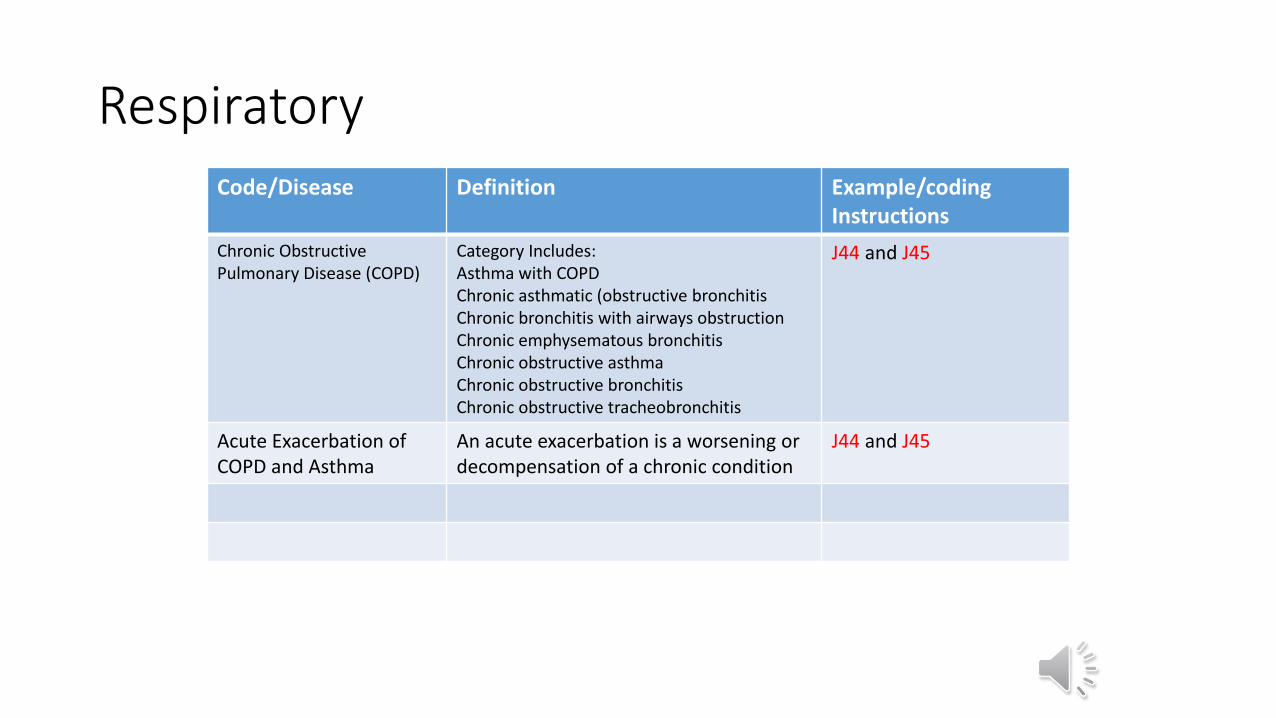
Respiratory Code/Disease Definition Example/coding
Instructions
Chronic Obstructive Pulmonary Disease (COPD)
Category Includes:Asthma with COPDChronic asthmatic (obstructive bronchitisChronic bronchitis with airways obstructionChronic emphysematous bronchitisChronic obstructive asthmaChronic obstructive bronchitisChronic obstructive tracheobronchitis
J44 and J45
Acute Exacerbation of COPD and Asthma
An acute exacerbation is a worsening or decompensation of a chronic condition
J44 and J45
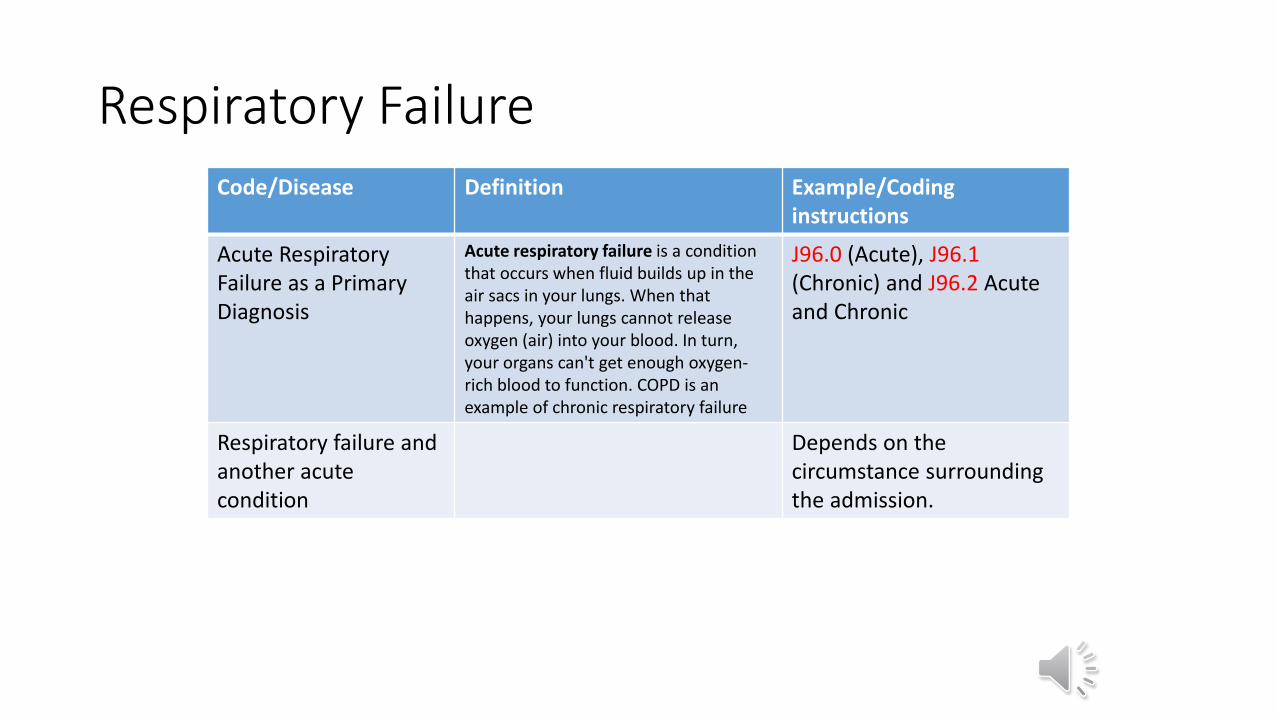
Respiratory Failure Code/Disease Definition Example/Coding
instructions
Acute Respiratory Failure as a PrimaryDiagnosis
Acute respiratory failure is a condition that occurs when fluid builds up in the air sacs in your lungs. When that happens, your lungs cannot release oxygen (air) into your blood. In turn, your organs can't get enough oxygen-rich blood to function. COPD is an example of chronic respiratory failure
J96.0 (Acute), J96.1(Chronic) and J96.2 Acute and Chronic
Respiratory failure and another acute condition
Depends on the circumstance surrounding the admission.
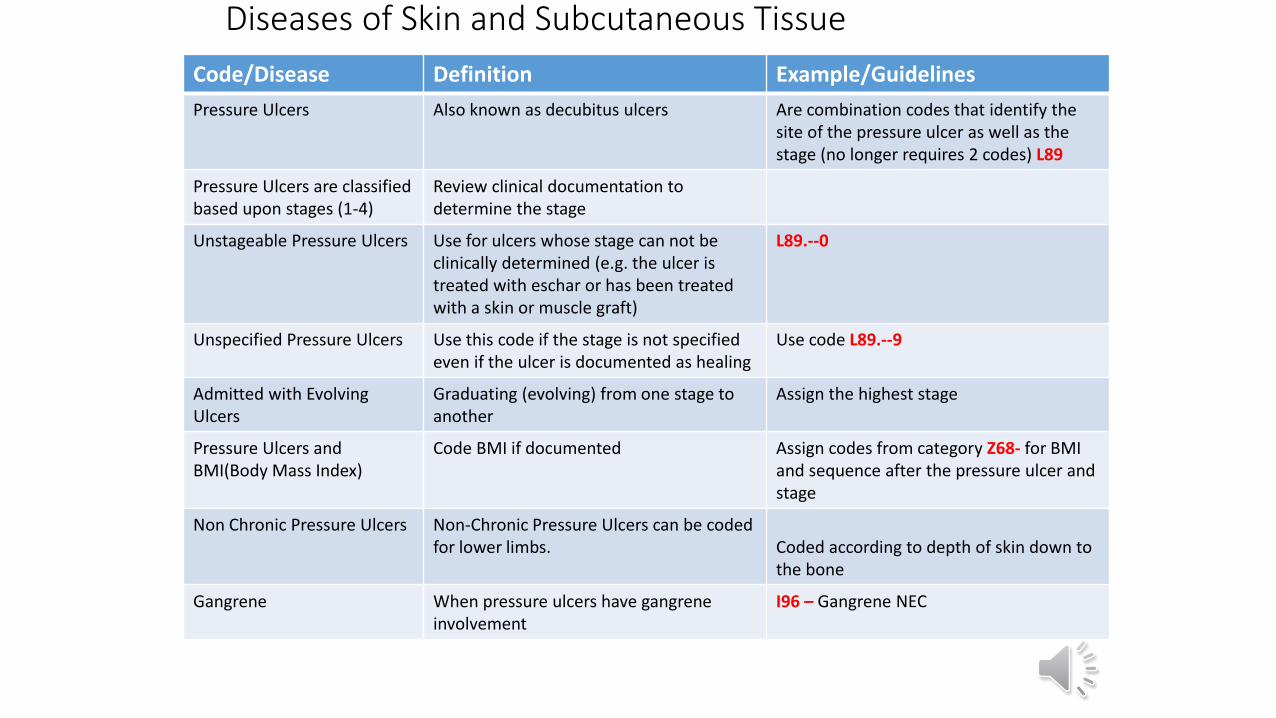
Diseases of Skin and Subcutaneous Tissue
Code/Disease Definition Example/Guidelines
Pressure Ulcers Also known as decubitus ulcers Are combination codes that identify the site of the pressure ulcer as well as the stage (no longer requires 2 codes) L89
Pressure Ulcers are classified based upon stages (1-4)
Review clinical documentation to determine the stage
Unstageable Pressure Ulcers Use for ulcers whose stage can not be clinically determined (e.g. the ulcer is treated with eschar or has been treated with a skin or muscle graft)
L89.--0
Unspecified Pressure Ulcers Use this code if the stage is not specified even if the ulcer is documented as healing
Use code L89.--9
Admitted with EvolvingUlcers
Graduating (evolving) from one stage to another
Assign the highest stage
Pressure Ulcers and BMI(Body Mass Index)
Code BMI if documented Assign codes from category Z68- for BMI and sequence after the pressure ulcer and stage
Non Chronic Pressure Ulcers Non-Chronic Pressure Ulcers can be coded for lower limbs. Coded according to depth of skin down to
the bone
Gangrene When pressure ulcers have gangrene involvement
I96 – Gangrene NEC
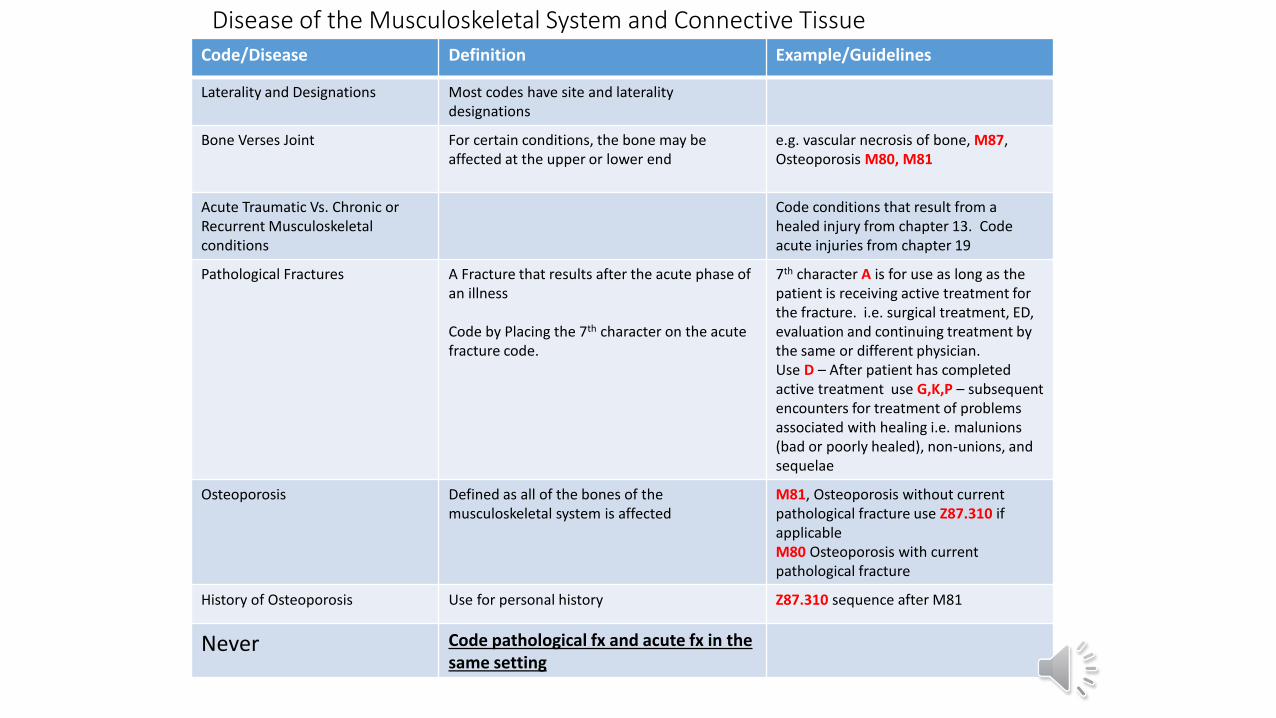
Disease of the Musculoskeletal System and Connective TissueCode/Disease Definition Example/Guidelines
Laterality and Designations Most codes have site and laterality designations
Bone Verses Joint For certain conditions, the bone may be affected at the upper or lower end
e.g. vascular necrosis of bone, M87, Osteoporosis M80, M81
Acute Traumatic Vs. Chronic or Recurrent Musculoskeletal conditions
Code conditions that result from a healed injury from chapter 13. Code acute injuries from chapter 19
Pathological Fractures A Fracture that results after the acute phase of an illness
Code by Placing the 7th character on the acute fracture code.
7th character A is for use as long as the patient is receiving active treatment for the fracture. i.e. surgical treatment, ED, evaluation and continuing treatment by the same or different physician.Use D – After patient has completed active treatment use G,K,P – subsequent encounters for treatment of problems associated with healing i.e. malunions(bad or poorly healed), non-unions, and sequelae
Osteoporosis Defined as all of the bones of the musculoskeletal system is affected
M81, Osteoporosis without current pathological fracture use Z87.310 if applicable M80 Osteoporosis with current pathological fracture
History of Osteoporosis Use for personal history Z87.310 sequence after M81
Never Code pathological fx and acute fx in the same setting
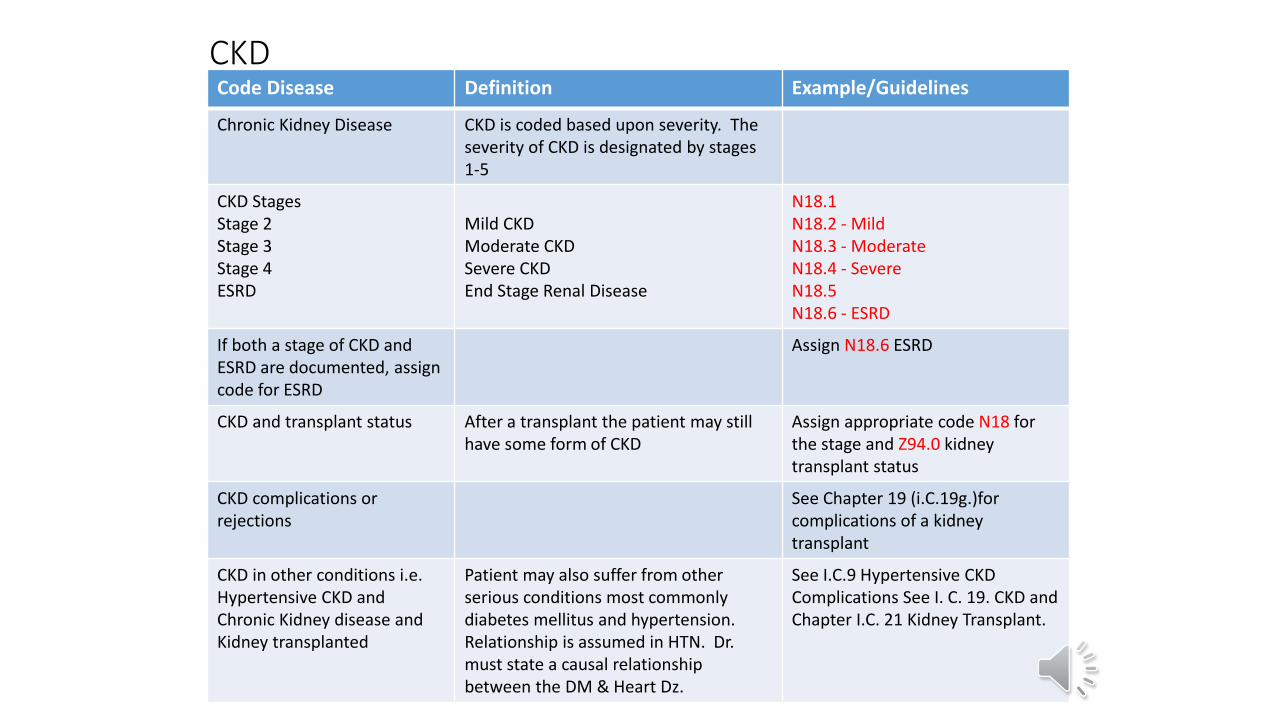
CKDCode Disease Definition Example/Guidelines
Chronic Kidney Disease CKD is coded based upon severity. The severity of CKD is designated by stages 1-5
CKD StagesStage 2Stage 3Stage 4ESRD
Mild CKDModerate CKDSevere CKDEnd Stage Renal Disease
N18.1N18.2 - MildN18.3 - ModerateN18.4 - SevereN18.5N18.6 - ESRD
If both a stage of CKD and ESRD are documented, assign code for ESRD
Assign N18.6 ESRD
CKD and transplant status After a transplant the patient may still have some form of CKD
Assign appropriate code N18 for the stage and Z94.0 kidney transplant status
CKD complications or rejections
See Chapter 19 (i.C.19g.)for complications of a kidney transplant
CKD in other conditions i.e.Hypertensive CKD and Chronic Kidney disease and Kidney transplanted
Patient may also suffer from other serious conditions most commonly diabetes mellitus and hypertension.Relationship is assumed in HTN. Dr. must state a causal relationship between the DM & Heart Dz.
See I.C.9 Hypertensive CKDComplications See I. C. 19. CKD and Chapter I.C. 21 Kidney Transplant.
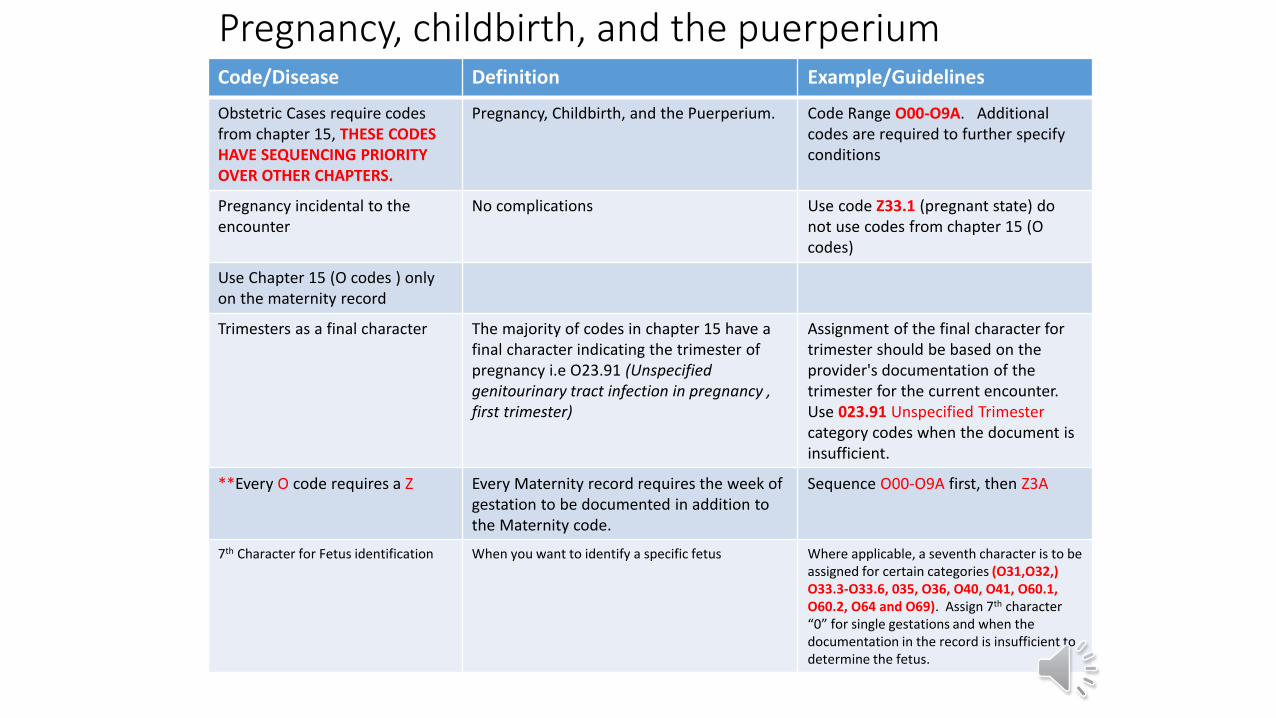
Pregnancy, childbirth, and the puerperiumCode/Disease Definition Example/Guidelines
Obstetric Cases require codes from chapter 15, THESE CODES HAVE SEQUENCING PRIORITY OVER OTHER CHAPTERS.
Pregnancy, Childbirth, and the Puerperium. Code Range O00-O9A. Additional codes are required to further specify conditions
Pregnancy incidental to the encounter
No complications Use code Z33.1 (pregnant state) donot use codes from chapter 15 (O codes)
Use Chapter 15 (O codes ) only on the maternity record
Trimesters as a final character The majority of codes in chapter 15 have a final character indicating the trimester of pregnancy i.e O23.91 (Unspecified genitourinary tract infection in pregnancy , first trimester)
Assignment of the final character for trimester should be based on the provider's documentation of the trimester for the current encounter. Use 023.91 Unspecified Trimestercategory codes when the document is insufficient.
**Every O code requires a Z Every Maternity record requires the week of gestation to be documented in addition to the Maternity code.
Sequence O00-O9A first, then Z3A
7th Character for Fetus identification When you want to identify a specific fetus Where applicable, a seventh character is to be assigned for certain categories (O31,O32,) O33.3-O33.6, 035, O36, O40, O41, O60.1, O60.2, O64 and O69). Assign 7th character “0” for single gestations and when the documentation in the record is insufficient to determine the fetus.
Pregnancy, childbirth, and the puerperium
Code/Disease Definition Example/Guidelines
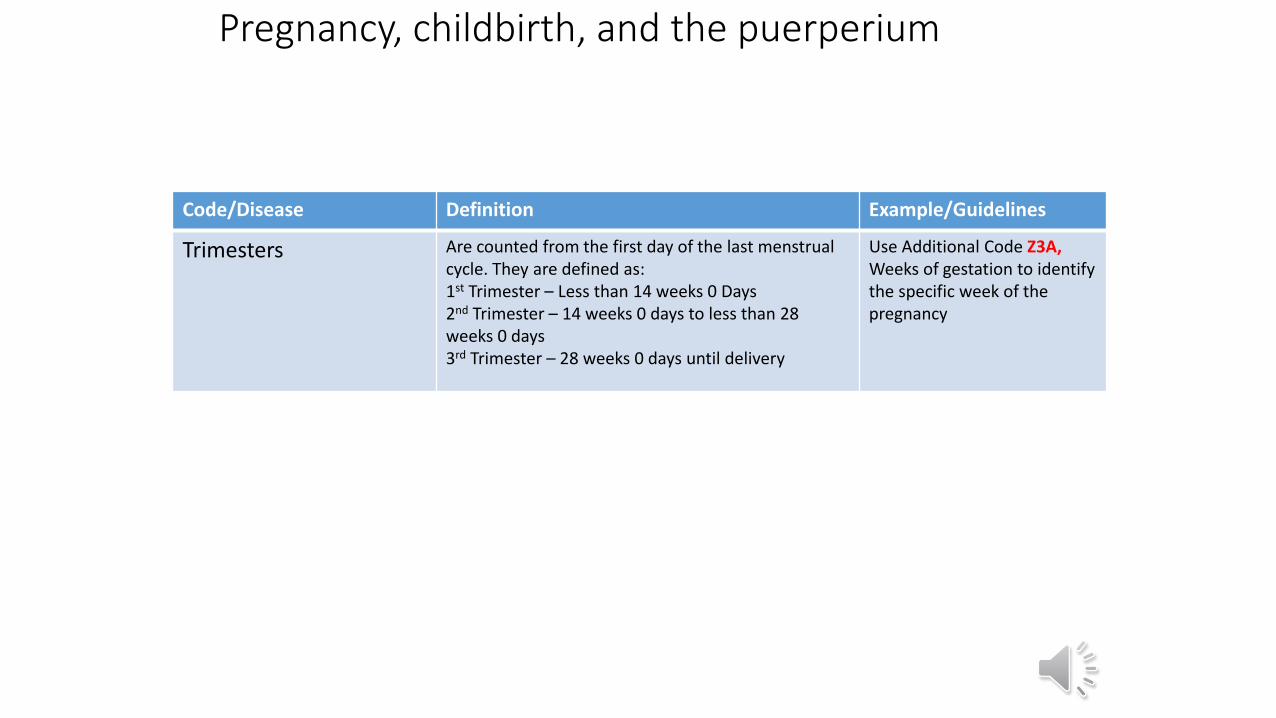
Trimesters Are counted from the first day of the last menstrual cycle. They are defined as:1st Trimester – Less than 14 weeks 0 Days2nd Trimester – 14 weeks 0 days to less than 28 weeks 0 days3rd Trimester – 28 weeks 0 days until delivery
Use Additional Code Z3A, Weeks of gestation to identify the specific week of the pregnancy
Pregnancy, childbirth, and the puerperium
Code/Disease Definition Example/Guidelines
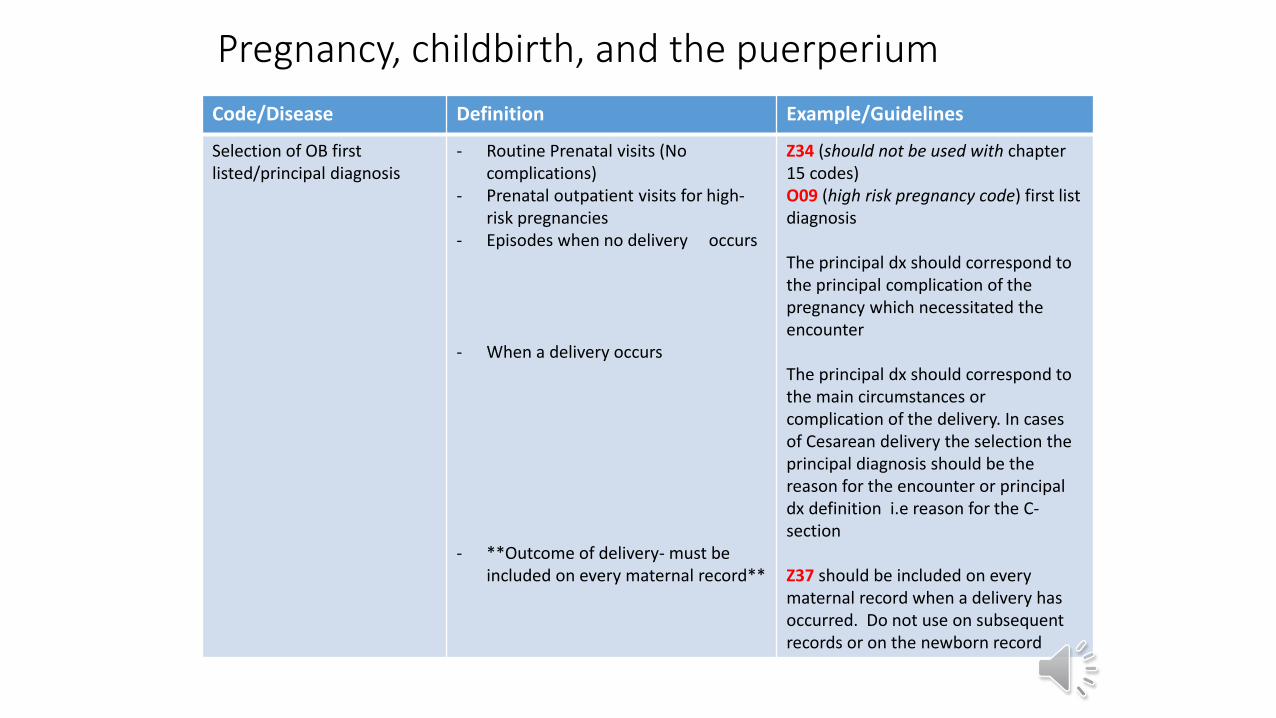
Selection of OB firstlisted/principal diagnosis
- Routine Prenatal visits (No complications)
- Prenatal outpatient visits for high-risk pregnancies
- Episodes when no delivery occurs
- When a delivery occurs
- **Outcome of delivery- must be included on every maternal record**
Z34 (should not be used with chapter 15 codes)O09 (high risk pregnancy code) first list diagnosis
The principal dx should correspond to the principal complication of the pregnancy which necessitated the encounter
The principal dx should correspond to the main circumstances or complication of the delivery. In cases of Cesarean delivery the selection the principal diagnosis should be the reason for the encounter or principal dx definition i.e reason for the C-section
Z37 should be included on every maternal record when a delivery has occurred. Do not use on subsequent records or on the newborn record
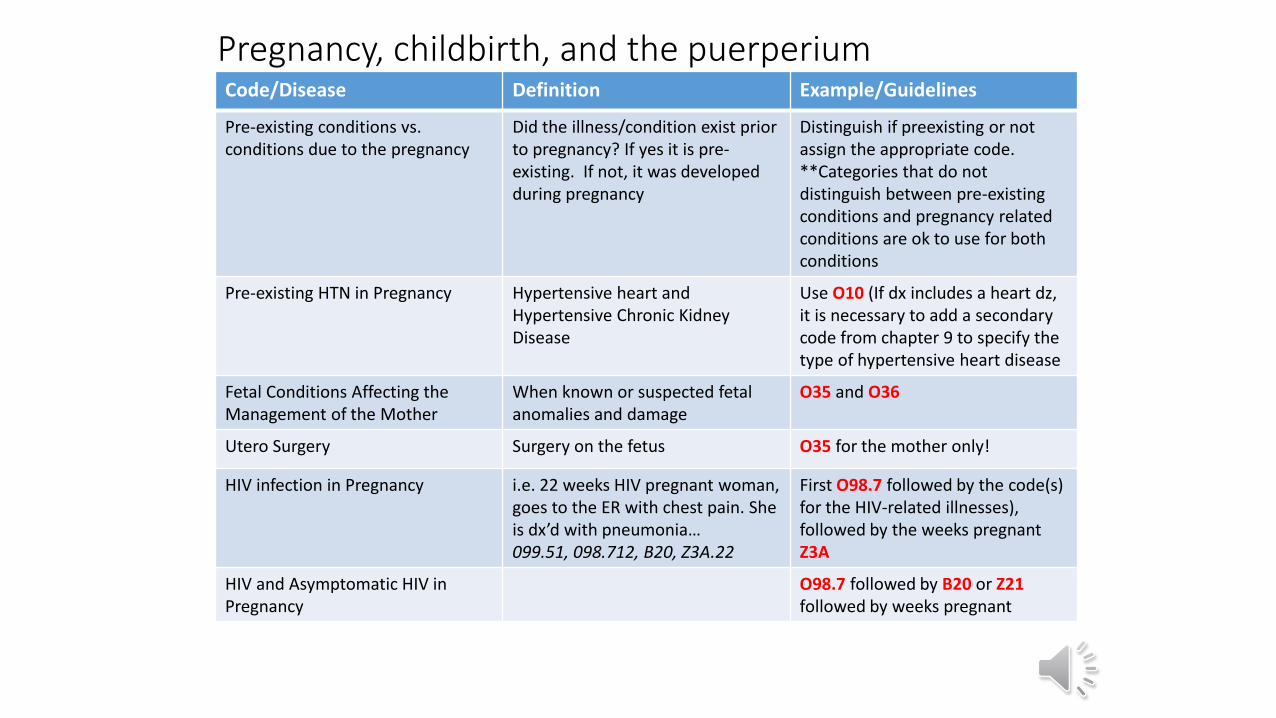
Pregnancy, childbirth, and the puerperiumCode/Disease Definition Example/Guidelines
Pre-existing conditions vs.conditions due to the pregnancy
Did the illness/condition exist prior to pregnancy? If yes it is pre-existing. If not, it was developed during pregnancy
Distinguish if preexisting or not assign the appropriate code. **Categories that do not distinguish between pre-existing conditions and pregnancy related conditions are ok to use for both conditions
Pre-existing HTN in Pregnancy Hypertensive heart and Hypertensive Chronic Kidney Disease
Use O10 (If dx includes a heart dz, it is necessary to add a secondary code from chapter 9 to specify the type of hypertensive heart disease
Fetal Conditions Affecting the Management of the Mother
When known or suspected fetal anomalies and damage
O35 and O36
Utero Surgery Surgery on the fetus O35 for the mother only!
HIV infection in Pregnancy i.e. 22 weeks HIV pregnant woman, goes to the ER with chest pain. She is dx’d with pneumonia…099.51, 098.712, B20, Z3A.22
First O98.7 followed by the code(s) for the HIV-related illnesses), followed by the weeks pregnant Z3A
HIV and Asymptomatic HIV in Pregnancy
O98.7 followed by B20 or Z21 followed by weeks pregnant
Pregnancy, childbirth, and the puerperiumCode/Disease Definition Example/Guidelines
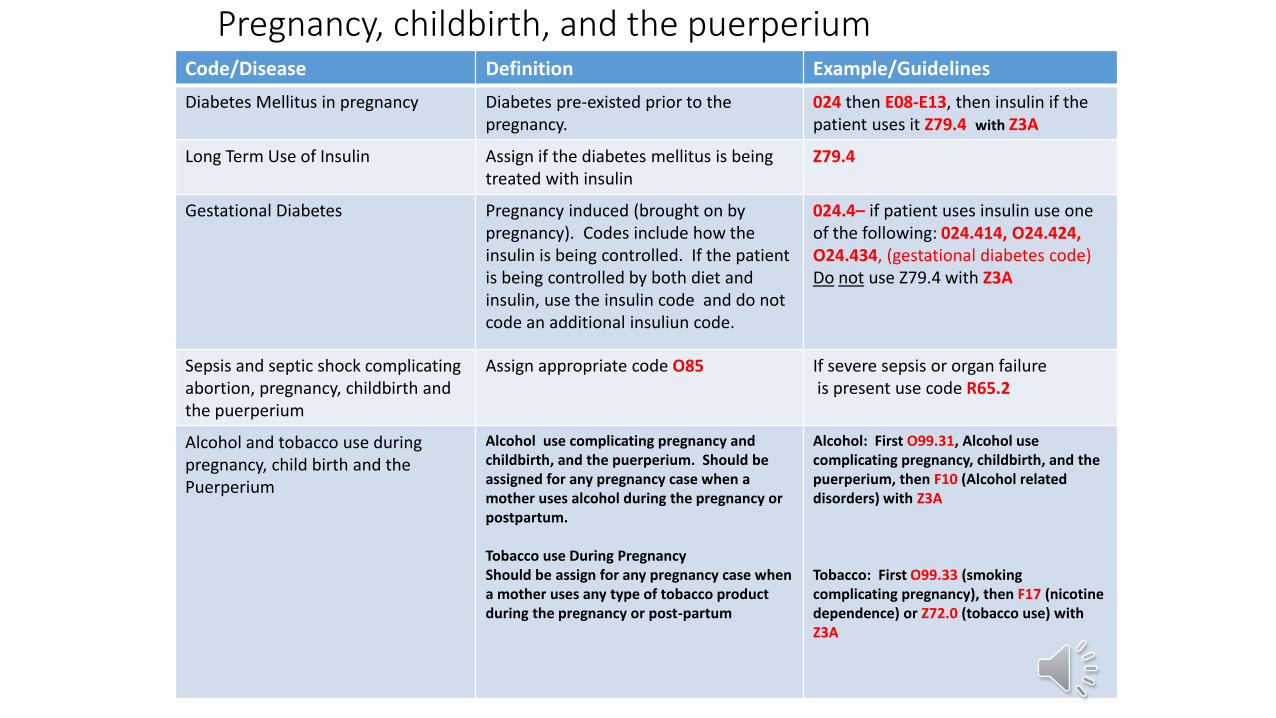
Diabetes Mellitus in pregnancy Diabetes pre-existed prior to the pregnancy.
024 then E08-E13, then insulin if the patient uses it Z79.4 with Z3A
Long Term Use of Insulin Assign if the diabetes mellitus is being treated with insulin
Z79.4
Gestational Diabetes Pregnancy induced (brought on by pregnancy). Codes include how the insulin is being controlled. If the patient is being controlled by both diet and insulin, use the insulin code and do not code an additional insuliun code.
024.4– if patient uses insulin use one of the following: 024.414, O24.424, O24.434, (gestational diabetes code) Do not use Z79.4 with Z3A
Sepsis and septic shock complicating abortion, pregnancy, childbirth and the puerperium
Assign appropriate code O85 If severe sepsis or organ failureis present use code R65.2
Alcohol and tobacco use during pregnancy, child birth and the Puerperium
Alcohol use complicating pregnancy and childbirth, and the puerperium. Should be assigned for any pregnancy case when a mother uses alcohol during the pregnancy or postpartum.
Tobacco use During PregnancyShould be assign for any pregnancy case when a mother uses any type of tobacco product during the pregnancy or post-partum
Alcohol: First O99.31, Alcohol use complicating pregnancy, childbirth, and the puerperium, then F10 (Alcohol related disorders) with Z3A
Tobacco: First O99.33 (smoking complicating pregnancy), then F17 (nicotine dependence) or Z72.0 (tobacco use) with Z3A
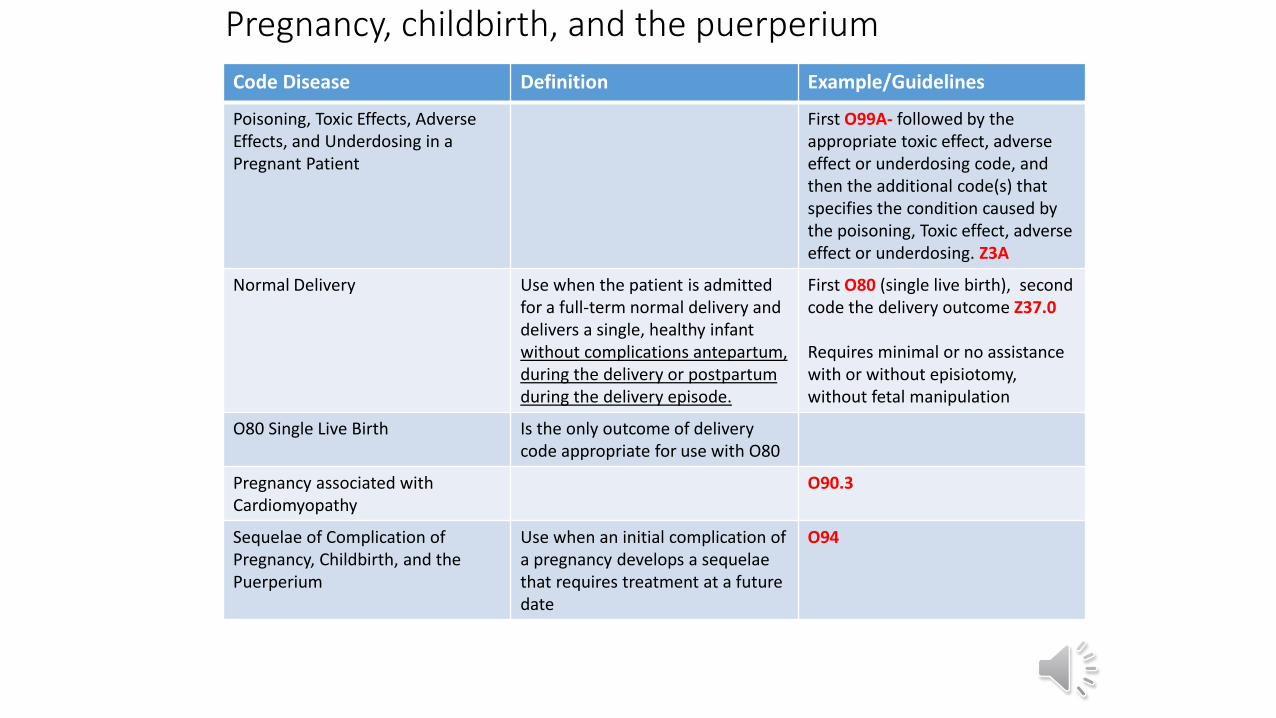
Pregnancy, childbirth, and the puerperium
Code Disease Definition Example/Guidelines
Poisoning, Toxic Effects, Adverse Effects, and Underdosing in a Pregnant Patient
First O99A- followed by the appropriate toxic effect, adverse effect or underdosing code, and then the additional code(s) that specifies the condition caused by the poisoning, Toxic effect, adverse effect or underdosing. Z3A
Normal Delivery Use when the patient is admitted for a full-term normal delivery and delivers a single, healthy infant without complications antepartum, during the delivery or postpartum during the delivery episode.
First O80 (single live birth), second code the delivery outcome Z37.0
Requires minimal or no assistance with or without episiotomy, without fetal manipulation
O80 Single Live Birth Is the only outcome of delivery code appropriate for use with O80
Pregnancy associated with Cardiomyopathy
O90.3
Sequelae of Complication of Pregnancy, Childbirth, and the Puerperium
Use when an initial complication of a pregnancy develops a sequelae that requires treatment at a future date
O94
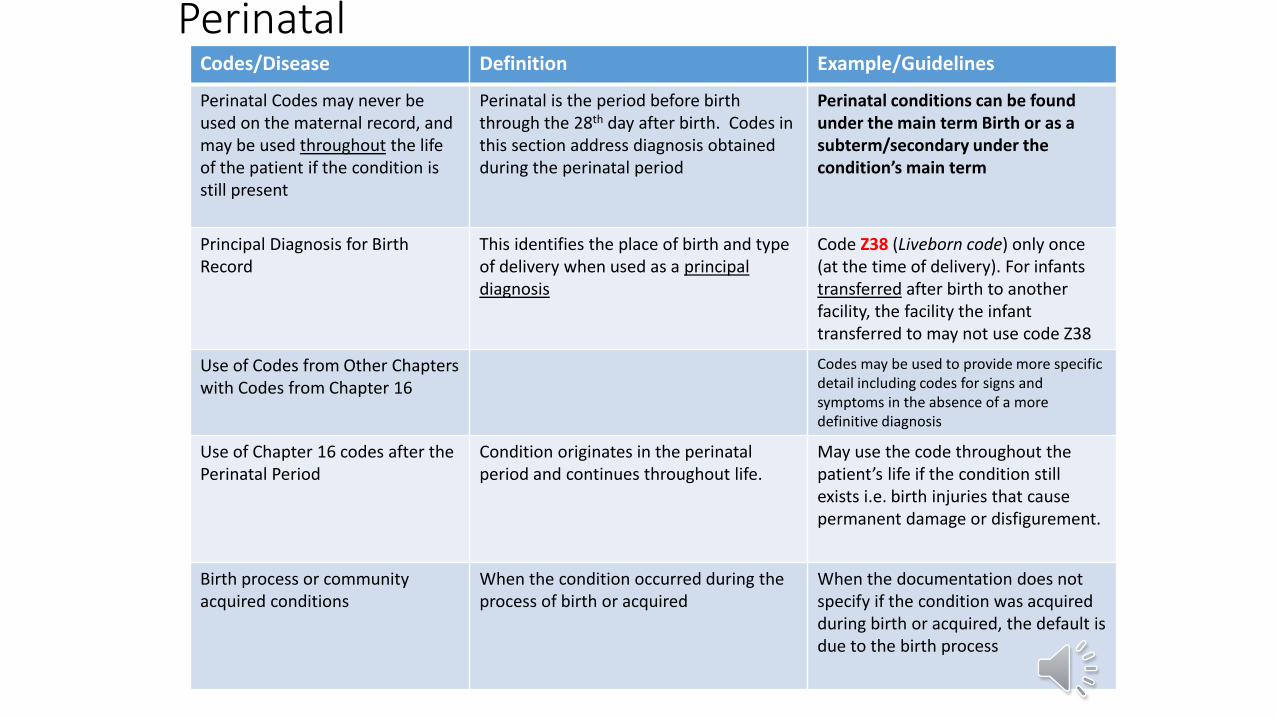
PerinatalCodes/Disease Definition Example/Guidelines
Perinatal Codes may never be used on the maternal record, and may be used throughout the life of the patient if the condition is still present
Perinatal is the period before birth through the 28th day after birth. Codes in this section address diagnosis obtained during the perinatal period
Perinatal conditions can be found under the main term Birth or as a subterm/secondary under the condition’s main term
Principal Diagnosis for BirthRecord
This identifies the place of birth and type of delivery when used as a principal diagnosis
Code Z38 (Liveborn code) only once(at the time of delivery). For infants transferred after birth to another facility, the facility the infant transferred to may not use code Z38
Use of Codes from Other Chapterswith Codes from Chapter 16
Codes may be used to provide more specific detail including codes for signs and symptoms in the absence of a more definitive diagnosis
Use of Chapter 16 codes after thePerinatal Period
Condition originates in the perinatal period and continues throughout life.
May use the code throughout the patient’s life if the condition still exists i.e. birth injuries that cause permanent damage or disfigurement.
Birth process or community acquired conditions
When the condition occurred during the process of birth or acquired
When the documentation does not specify if the condition was acquired during birth or acquired, the default is due to the birth process
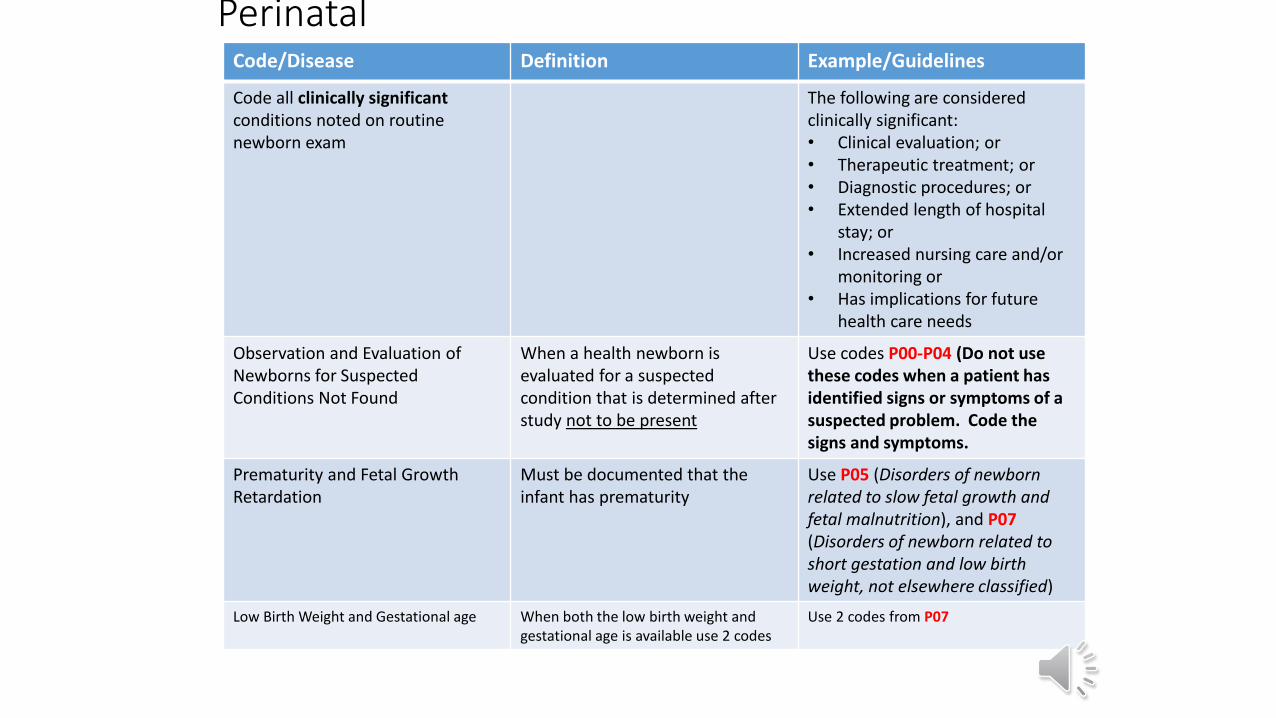
PerinatalCode/Disease Definition Example/Guidelines
Code all clinically significant conditions noted on routine newborn exam
The following are consideredclinically significant: • Clinical evaluation; or• Therapeutic treatment; or• Diagnostic procedures; or • Extended length of hospital
stay; or• Increased nursing care and/or
monitoring or• Has implications for future
health care needs
Observation and Evaluation of Newborns for Suspected Conditions Not Found
When a health newborn is evaluated for a suspected condition that is determined after study not to be present
Use codes P00-P04 (Do not use these codes when a patient has identified signs or symptoms of a suspected problem. Code the signs and symptoms.
Prematurity and Fetal Growth Retardation
Must be documented that the infant has prematurity
Use P05 (Disorders of newborn related to slow fetal growth and fetal malnutrition), and P07(Disorders of newborn related to short gestation and low birth weight, not elsewhere classified)
Low Birth Weight and Gestational age When both the low birth weight and gestational age is available use 2 codes
Use 2 codes from P07
Perinatal
Code/Disease Definition Example/Guidelines
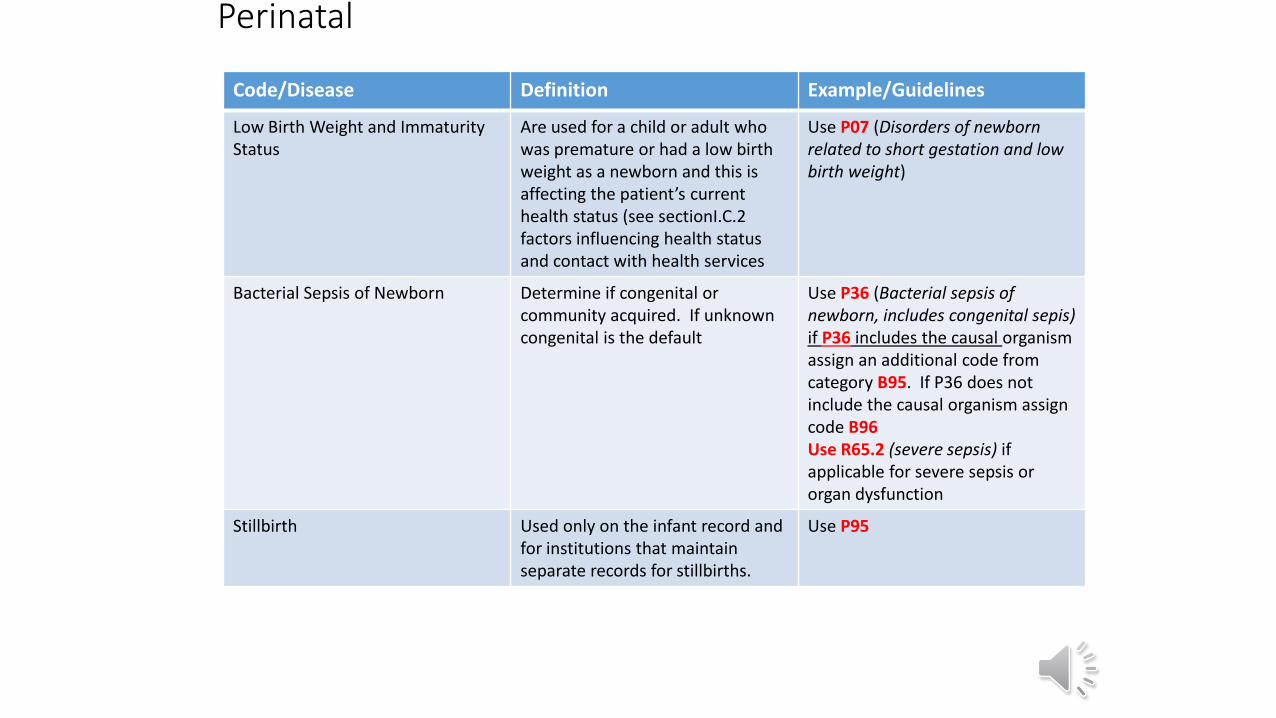
Low Birth Weight and ImmaturityStatus
Are used for a child or adult who was premature or had a low birth weight as a newborn and this is affecting the patient’s current health status (see sectionI.C.2 factors influencing health status and contact with health services
Use P07 (Disorders of newborn related to short gestation and low birth weight)
Bacterial Sepsis of Newborn Determine if congenital or community acquired. If unknown congenital is the default
Use P36 (Bacterial sepsis of newborn, includes congenital sepis) if P36 includes the causal organism assign an additional code from category B95. If P36 does not include the causal organism assign code B96Use R65.2 (severe sepsis) if applicable for severe sepsis or organ dysfunction
Stillbirth Used only on the infant record and for institutions that maintain separate records for stillbirths.
Use P95
Congenital Malformations, Deformations, and Chromosomal Abnormalities
Code/Disease Definition Example/Guidelines
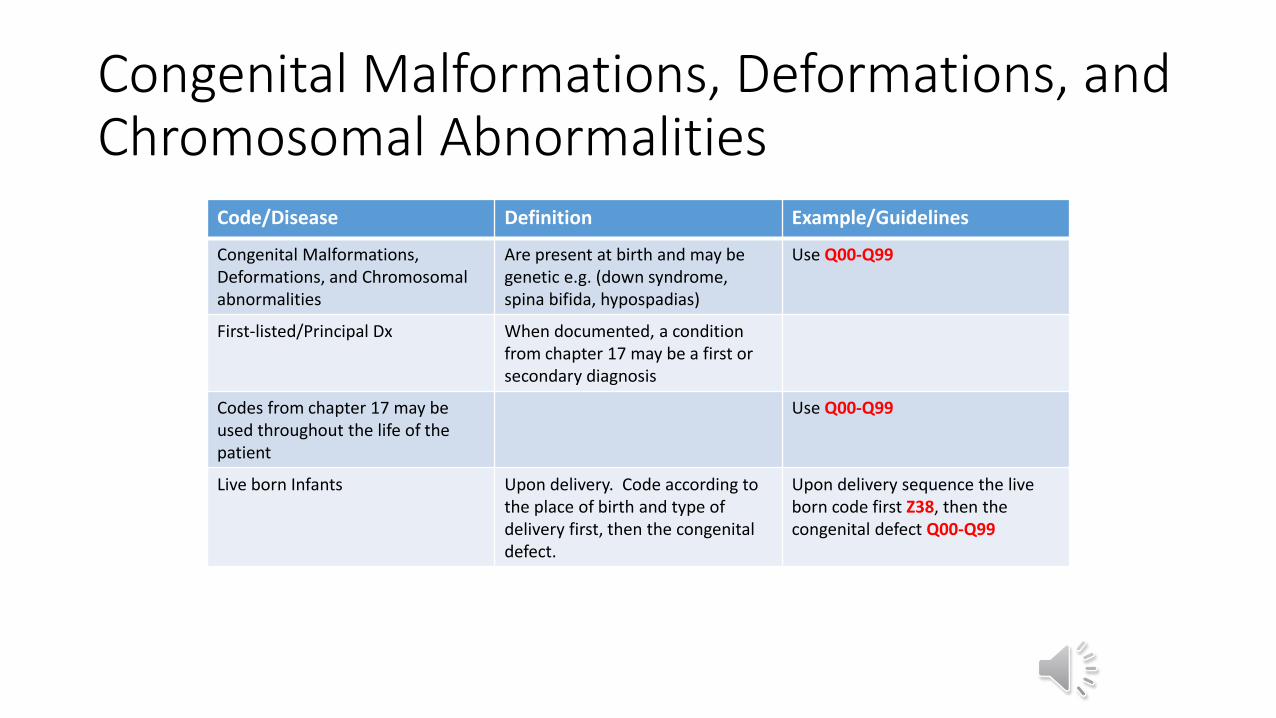
Congenital Malformations, Deformations, and Chromosomal abnormalities
Are present at birth and may be genetic e.g. (down syndrome, spina bifida, hypospadias)
Use Q00-Q99
First-listed/Principal Dx When documented, a condition from chapter 17 may be a first or secondary diagnosis
Codes from chapter 17 may be used throughout the life of the patient
Use Q00-Q99
Live born Infants Upon delivery. Code according to the place of birth and type of delivery first, then the congenital defect.
Upon delivery sequence the live born code first Z38, then the congenital defect Q00-Q99
Signs and SymptomsCode/Disease Definition Example/Guidelines
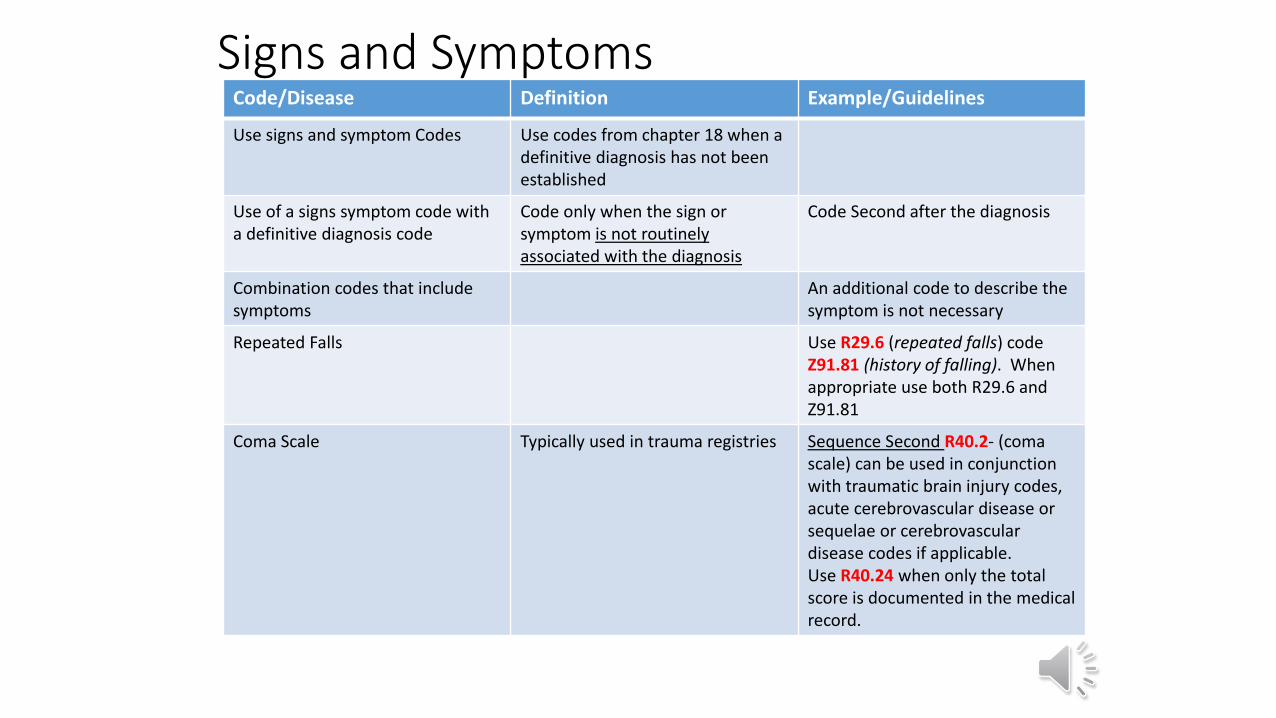
Use signs and symptom Codes Use codes from chapter 18 when a definitive diagnosis has not been established
Use of a signs symptom code with a definitive diagnosis code
Code only when the sign or symptom is not routinely associated with the diagnosis
Code Second after the diagnosis
Combination codes that include symptoms
An additional code to describe the symptom is not necessary
Repeated Falls Use R29.6 (repeated falls) code Z91.81 (history of falling). When appropriate use both R29.6 and Z91.81
Coma Scale Typically used in trauma registries Sequence Second R40.2- (coma scale) can be used in conjunction with traumatic brain injury codes, acute cerebrovascular disease or sequelae or cerebrovascular disease codes if applicable. Use R40.24 when only the total score is documented in the medical record.
Signs and SymptomsCode/Disease Definition Example/Guidelines
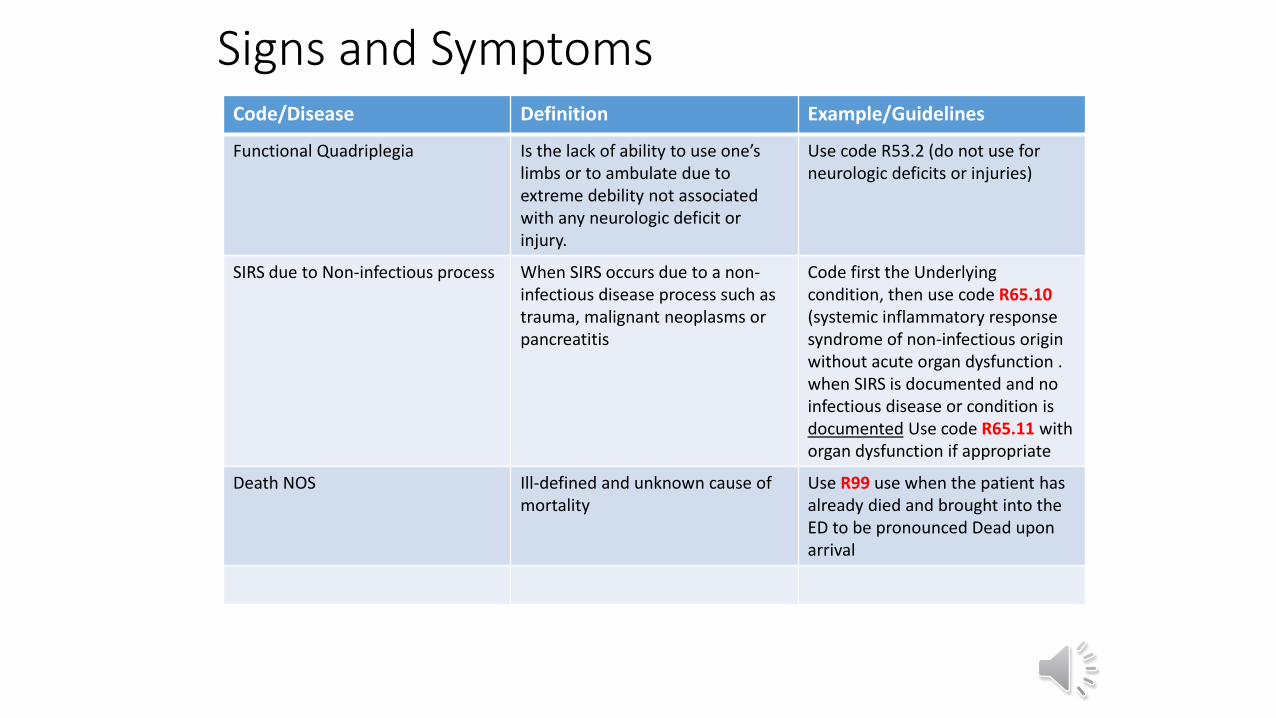
Functional Quadriplegia Is the lack of ability to use one’s limbs or to ambulate due to extreme debility not associated with any neurologic deficit or injury.
Use code R53.2 (do not use for neurologic deficits or injuries)
SIRS due to Non-infectious process When SIRS occurs due to a non-infectious disease process such as trauma, malignant neoplasms or pancreatitis
Code first the Underlying condition, then use code R65.10(systemic inflammatory response syndrome of non-infectious origin without acute organ dysfunction . when SIRS is documented and no infectious disease or condition is documented Use code R65.11 with organ dysfunction if appropriate
Death NOS Ill-defined and unknown cause of mortality
Use R99 use when the patient has already died and brought into the ED to be pronounced Dead upon arrival
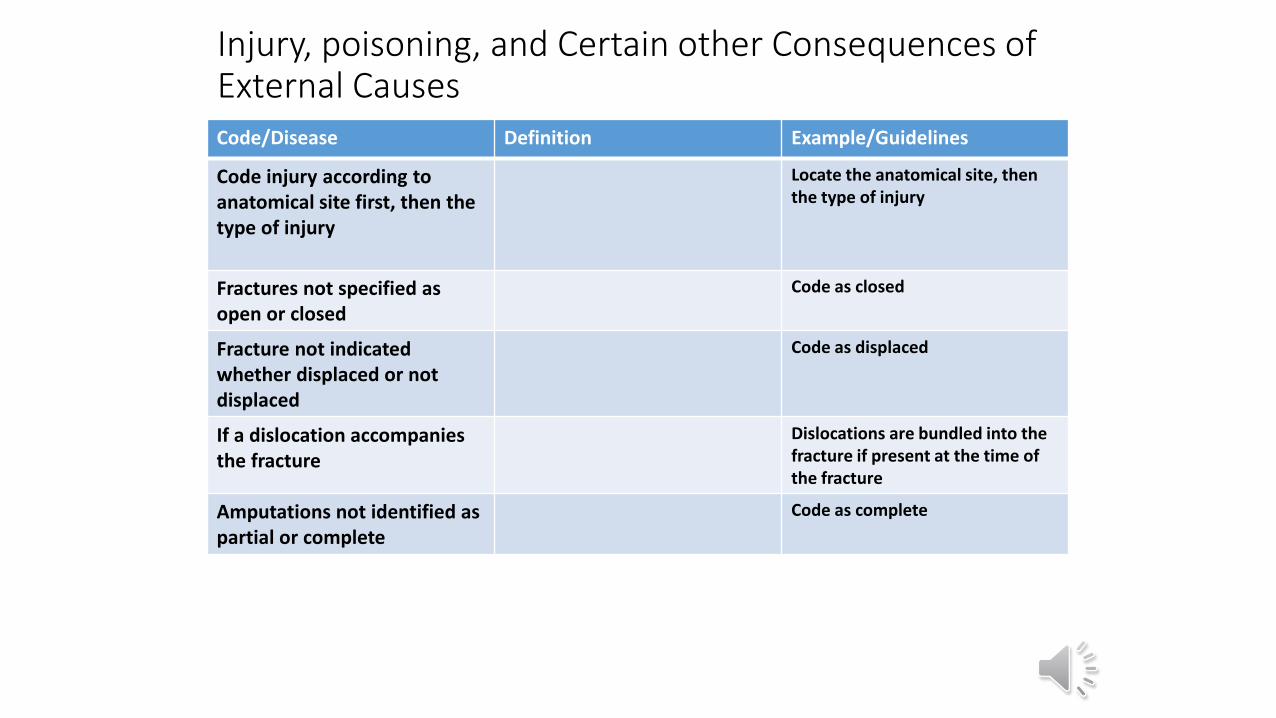
Injury, poisoning, and Certain other Consequences of External CausesCode/Disease Definition Example/Guidelines
Code injury according to anatomical site first, then the type of injury
Locate the anatomical site, then the type of injury
Fractures not specified as open or closed
Code as closed
Fracture not indicated whether displaced or not displaced
Code as displaced
If a dislocation accompanies the fracture
Dislocations are bundled into the fracture if present at the time of the fracture
Amputations not identified as partial or complete
Code as complete
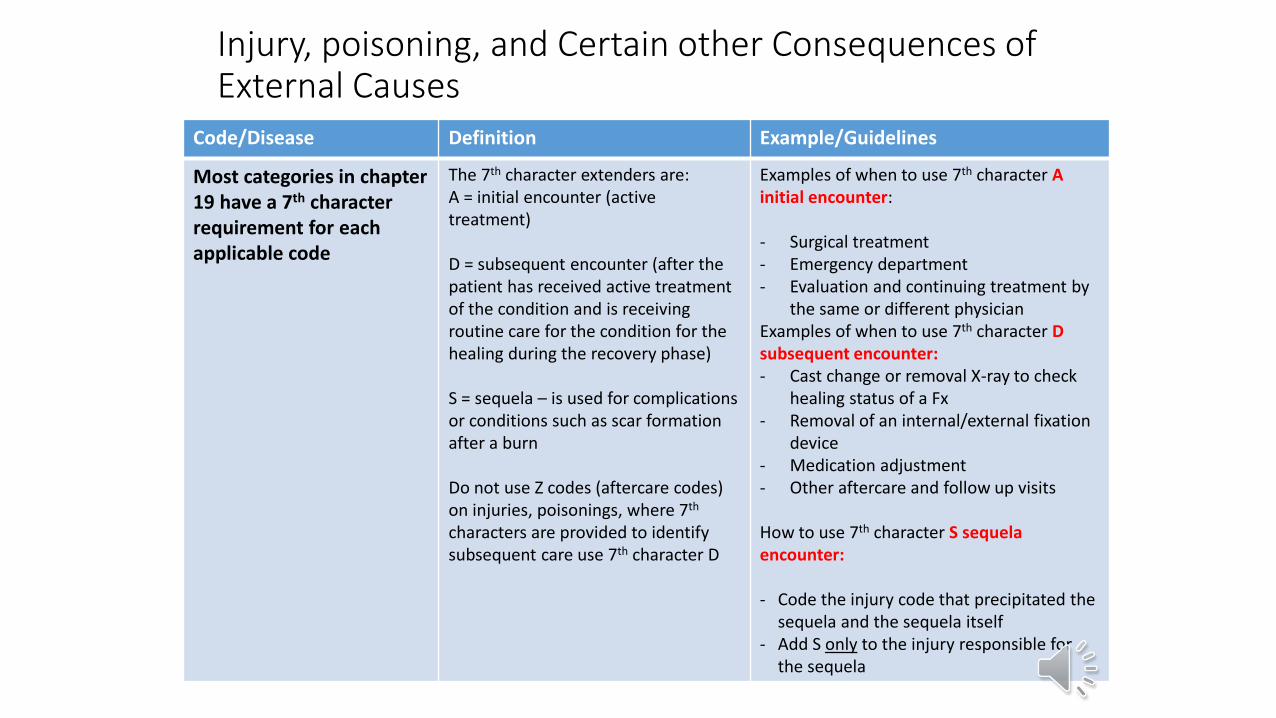
Injury, poisoning, and Certain other Consequences of External Causes
Code/Disease Definition Example/Guidelines
Most categories in chapter 19 have a 7th character requirement for each applicable code
The 7th character extenders are:A = initial encounter (active treatment)
D = subsequent encounter (after the patient has received active treatment of the condition and is receiving routine care for the condition for the healing during the recovery phase)
S = sequela – is used for complications or conditions such as scar formation after a burn
Do not use Z codes (aftercare codes) on injuries, poisonings, where 7th
characters are provided to identify subsequent care use 7th character D
Examples of when to use 7th character A initial encounter:
- Surgical treatment- Emergency department- Evaluation and continuing treatment by
the same or different physicianExamples of when to use 7th character D subsequent encounter:- Cast change or removal X-ray to check
healing status of a Fx- Removal of an internal/external fixation
device- Medication adjustment- Other aftercare and follow up visits
How to use 7th character S sequela encounter:
- Code the injury code that precipitated the sequela and the sequela itself
- Add S only to the injury responsible for the sequela
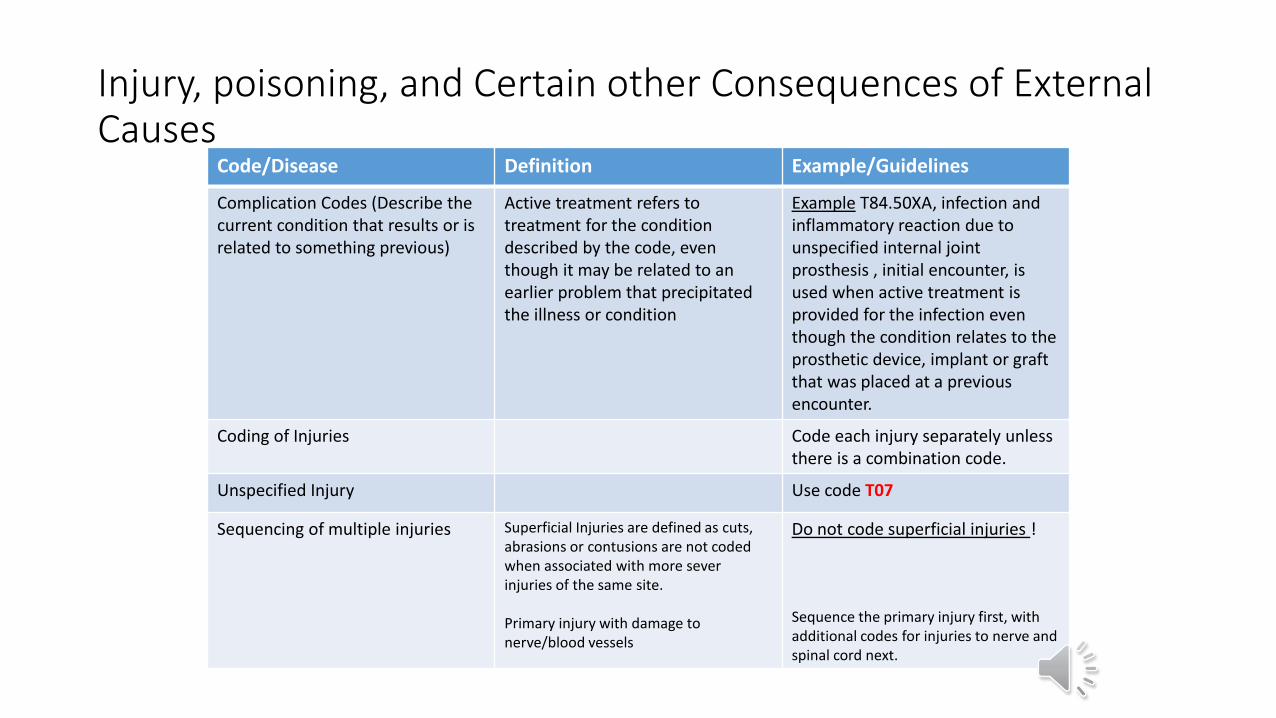
Injury, poisoning, and Certain other Consequences of External Causes
Code/Disease Definition Example/Guidelines
Complication Codes (Describe the current condition that results or is related to something previous)
Active treatment refers to treatment for the condition described by the code, even though it may be related to an earlier problem that precipitated the illness or condition
Example T84.50XA, infection and inflammatory reaction due to unspecified internal joint prosthesis , initial encounter, is used when active treatment is provided for the infection even though the condition relates to the prosthetic device, implant or graft that was placed at a previous encounter.
Coding of Injuries Code each injury separately unless there is a combination code.
Unspecified Injury Use code T07
Sequencing of multiple injuries Superficial Injuries are defined as cuts,abrasions or contusions are not coded when associated with more sever injuries of the same site.
Primary injury with damage to nerve/blood vessels
Do not code superficial injuries !
Sequence the primary injury first, with additional codes for injuries to nerve and spinal cord next.
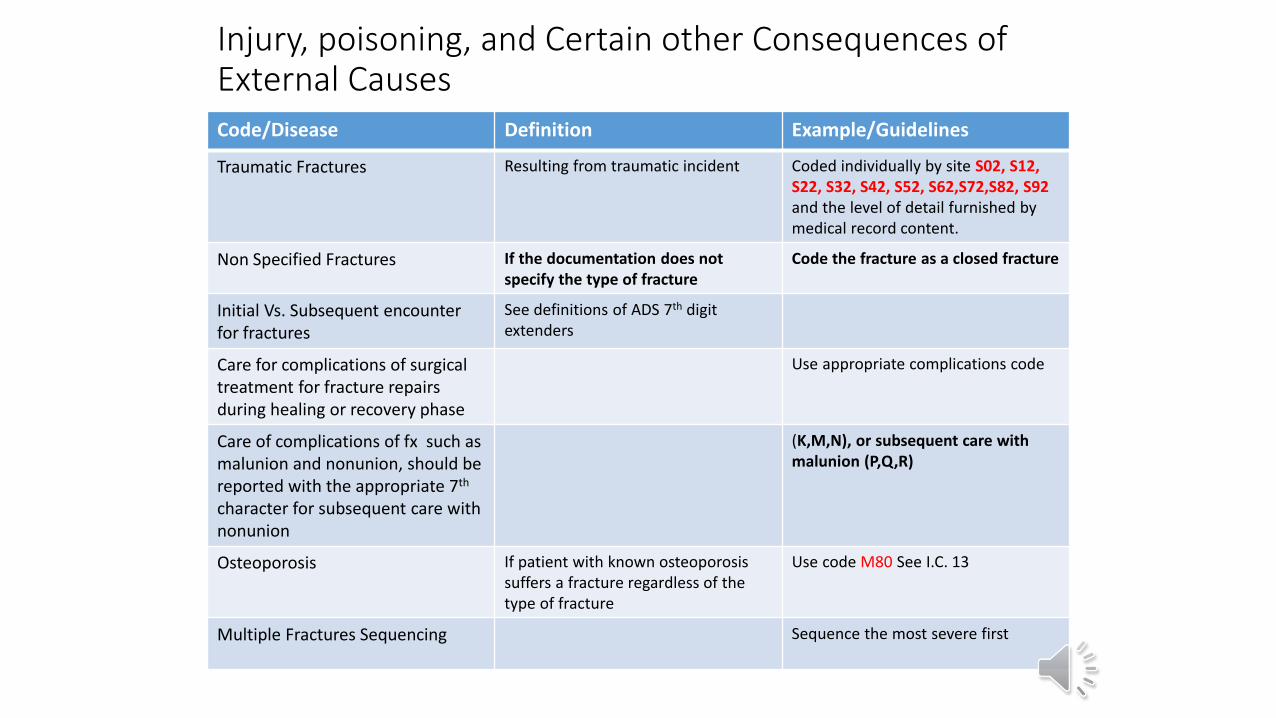
Injury, poisoning, and Certain other Consequences of External CausesCode/Disease Definition Example/Guidelines
Traumatic Fractures Resulting from traumatic incident Coded individually by site S02, S12, S22, S32, S42, S52, S62,S72,S82, S92and the level of detail furnished by medical record content.
Non Specified Fractures If the documentation does not specify the type of fracture
Code the fracture as a closed fracture
Initial Vs. Subsequent encounter for fractures
See definitions of ADS 7th digit extenders
Care for complications of surgical treatment for fracture repairs during healing or recovery phase
Use appropriate complications code
Care of complications of fx such as malunion and nonunion, should be reported with the appropriate 7th
character for subsequent care with nonunion
(K,M,N), or subsequent care with malunion (P,Q,R)
Osteoporosis If patient with known osteoporosissuffers a fracture regardless of the type of fracture
Use code M80 See I.C. 13
Multiple Fractures Sequencing Sequence the most severe first
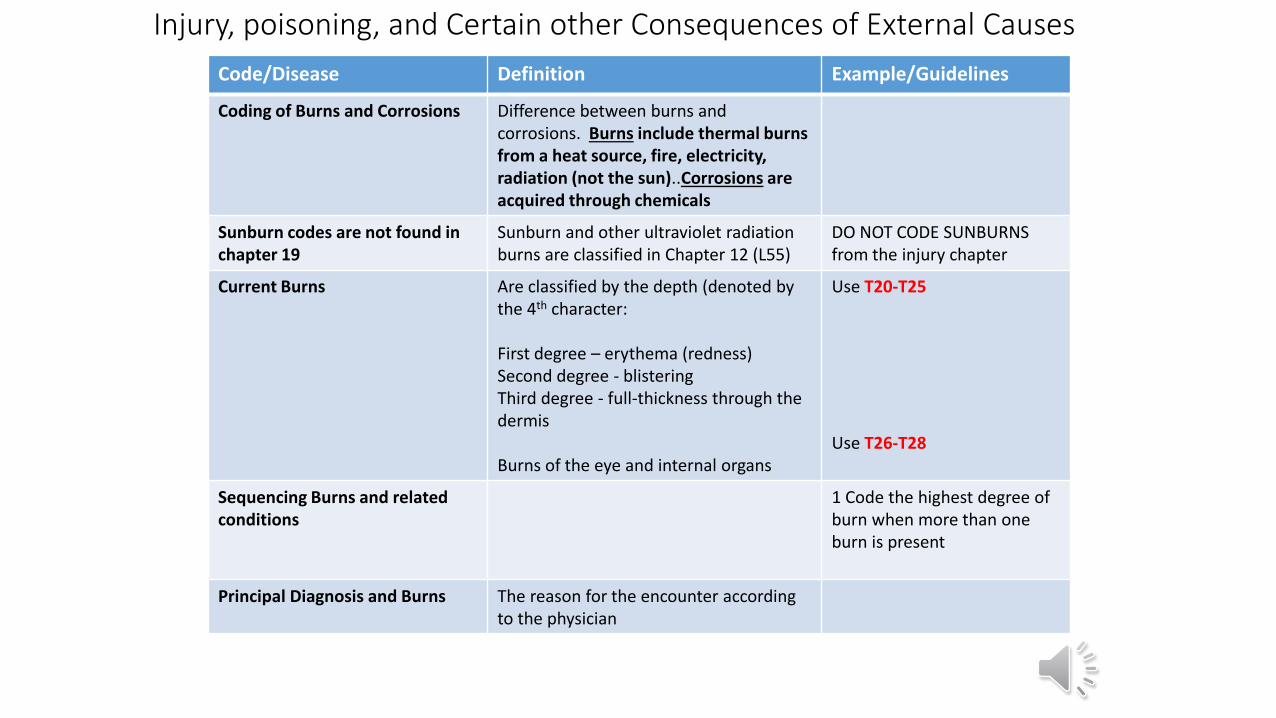
Injury, poisoning, and Certain other Consequences of External Causes
Code/Disease Definition Example/Guidelines
Coding of Burns and Corrosions Difference between burns and corrosions. Burns include thermal burns from a heat source, fire, electricity, radiation (not the sun)..Corrosions are acquired through chemicals
Sunburn codes are not found in chapter 19
Sunburn and other ultraviolet radiationburns are classified in Chapter 12 (L55)
DO NOT CODE SUNBURNS from the injury chapter
Current Burns Are classified by the depth (denoted by the 4th character:
First degree – erythema (redness)Second degree - blisteringThird degree - full-thickness through the dermis
Burns of the eye and internal organs
Use T20-T25
Use T26-T28
Sequencing Burns and relatedconditions
1 Code the highest degree of burn when more than one burn is present
Principal Diagnosis and Burns The reason for the encounter according to the physician
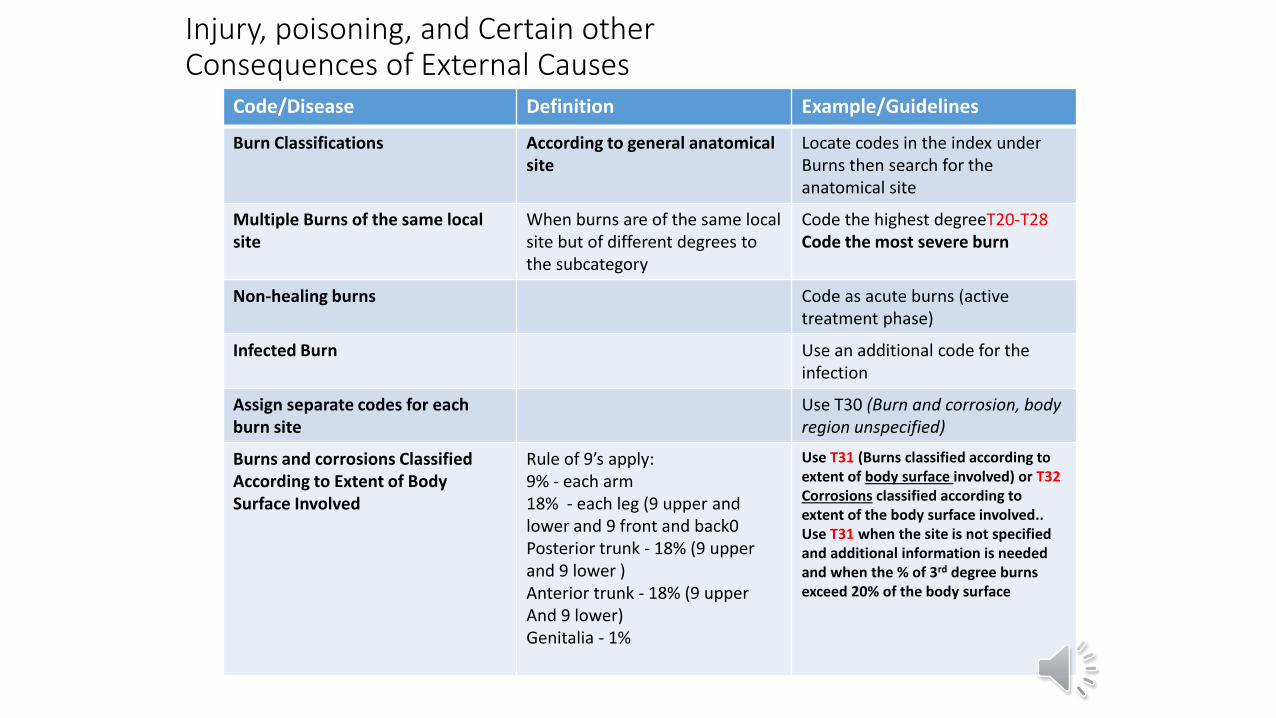
Injury, poisoning, and Certain other Consequences of External Causes
Code/Disease Definition Example/Guidelines
Burn Classifications According to general anatomicalsite
Locate codes in the index under Burns then search for the anatomical site
Multiple Burns of the same local site
When burns are of the same local site but of different degrees to the subcategory
Code the highest degreeT20-T28Code the most severe burn
Non-healing burns Code as acute burns (activetreatment phase)
Infected Burn Use an additional code for the infection
Assign separate codes for each burn site
Use T30 (Burn and corrosion, body region unspecified)
Burns and corrosions ClassifiedAccording to Extent of Body Surface Involved
Rule of 9’s apply:9% - each arm18% - each leg (9 upper and lower and 9 front and back0Posterior trunk - 18% (9 upper and 9 lower )Anterior trunk - 18% (9 upperAnd 9 lower)Genitalia - 1%
Use T31 (Burns classified according to extent of body surface involved) or T32Corrosions classified according to extent of the body surface involved.. Use T31 when the site is not specified and additional information is needed and when the % of 3rd degree burns exceed 20% of the body surface
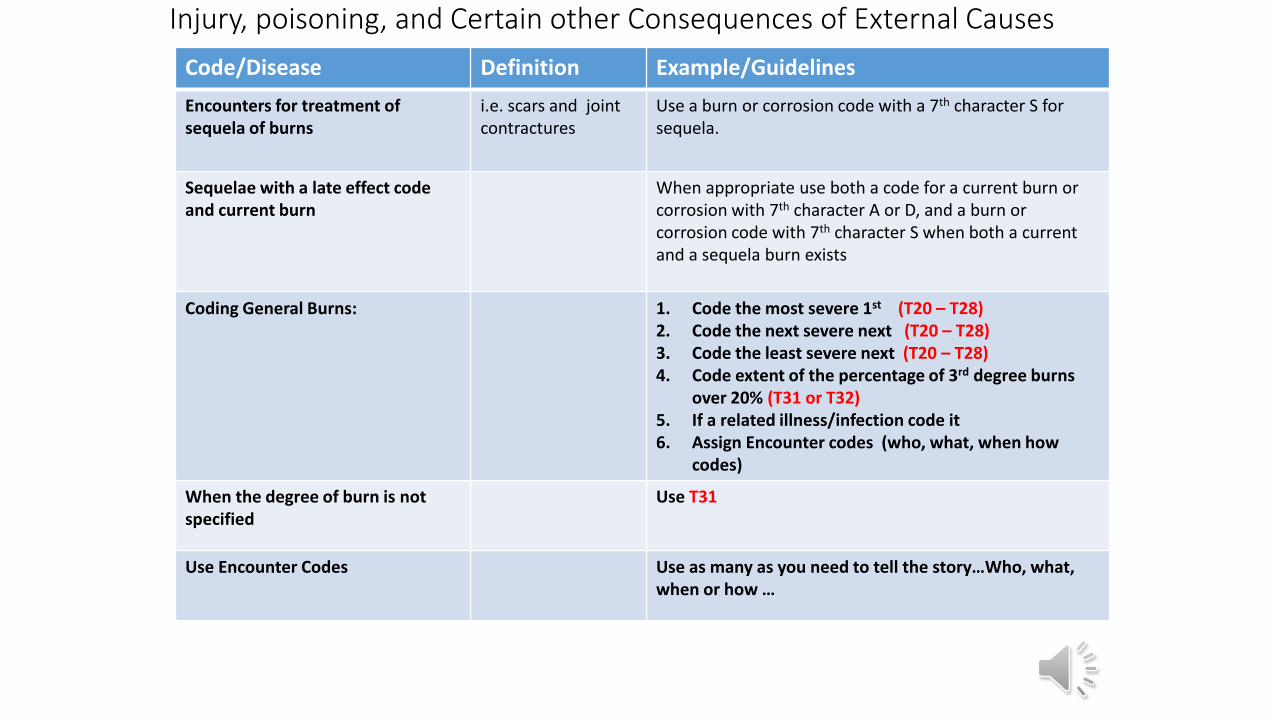
Injury, poisoning, and Certain other Consequences of External Causes
Code/Disease Definition Example/Guidelines
Encounters for treatment of sequela of burns
i.e. scars and joint contractures
Use a burn or corrosion code with a 7th character S for sequela.
Sequelae with a late effect code and current burn
When appropriate use both a code for a current burn or corrosion with 7th character A or D, and a burn or corrosion code with 7th character S when both a current and a sequela burn exists
Coding General Burns: 1. Code the most severe 1st (T20 – T28)2. Code the next severe next (T20 – T28)3. Code the least severe next (T20 – T28)4. Code extent of the percentage of 3rd degree burns
over 20% (T31 or T32)5. If a related illness/infection code it6. Assign Encounter codes (who, what, when how
codes)
When the degree of burn is not specified
Use T31
Use Encounter Codes Use as many as you need to tell the story…Who, what, when or how …
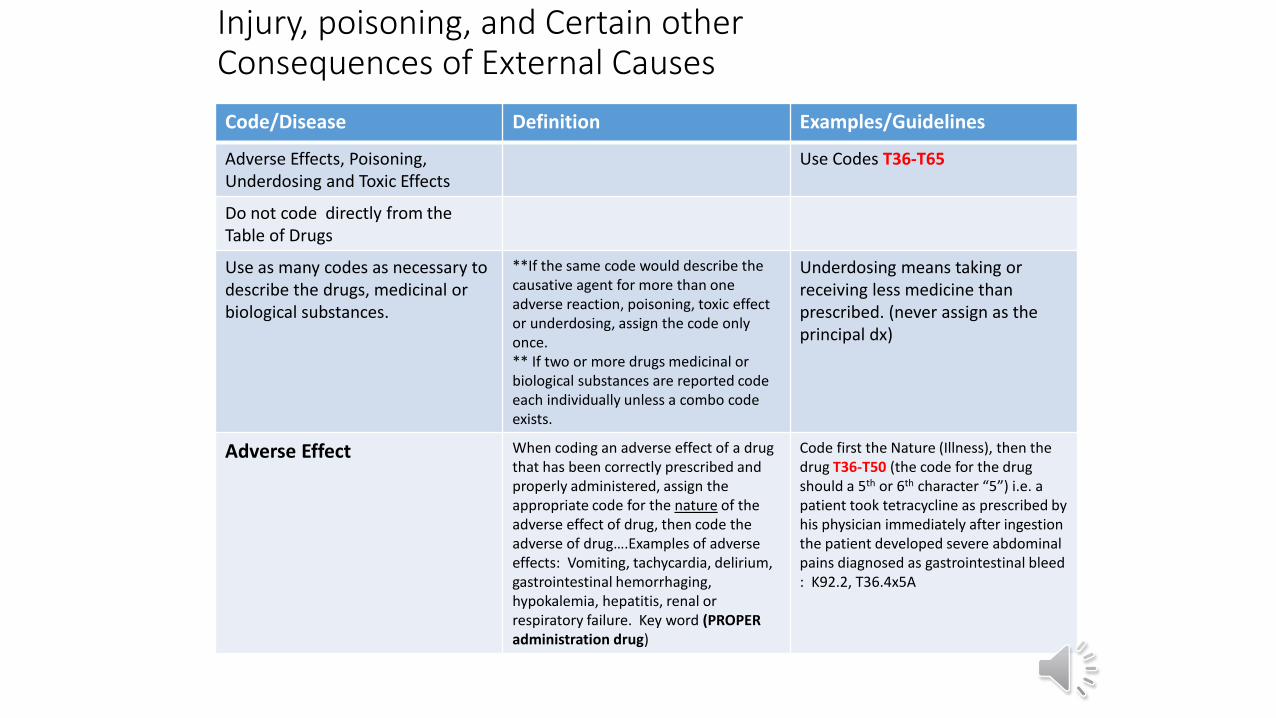
Injury, poisoning, and Certain other Consequences of External Causes
Code/Disease Definition Examples/Guidelines
Adverse Effects, Poisoning,Underdosing and Toxic Effects
Use Codes T36-T65
Do not code directly from the Table of Drugs
Use as many codes as necessary to describe the drugs, medicinal or biological substances.
**If the same code would describe the causative agent for more than one adverse reaction, poisoning, toxic effect or underdosing, assign the code only once. ** If two or more drugs medicinal or biological substances are reported code each individually unless a combo code exists.
Underdosing means taking or receiving less medicine than prescribed. (never assign as the principal dx)
Adverse Effect When coding an adverse effect of a drug that has been correctly prescribed and properly administered, assign the appropriate code for the nature of the adverse effect of drug, then code the adverse of drug….Examples of adverse effects: Vomiting, tachycardia, delirium, gastrointestinal hemorrhaging, hypokalemia, hepatitis, renal or respiratory failure. Key word (PROPER administration drug)
Code first the Nature (Illness), then the drug T36-T50 (the code for the drug should a 5th or 6th character “5”) i.e. a patient took tetracycline as prescribed by his physician immediately after ingestion the patient developed severe abdominal pains diagnosed as gastrointestinal bleed : K92.2, T36.4x5A
Injury, poisoning, and Certain other Consequences of External Causes
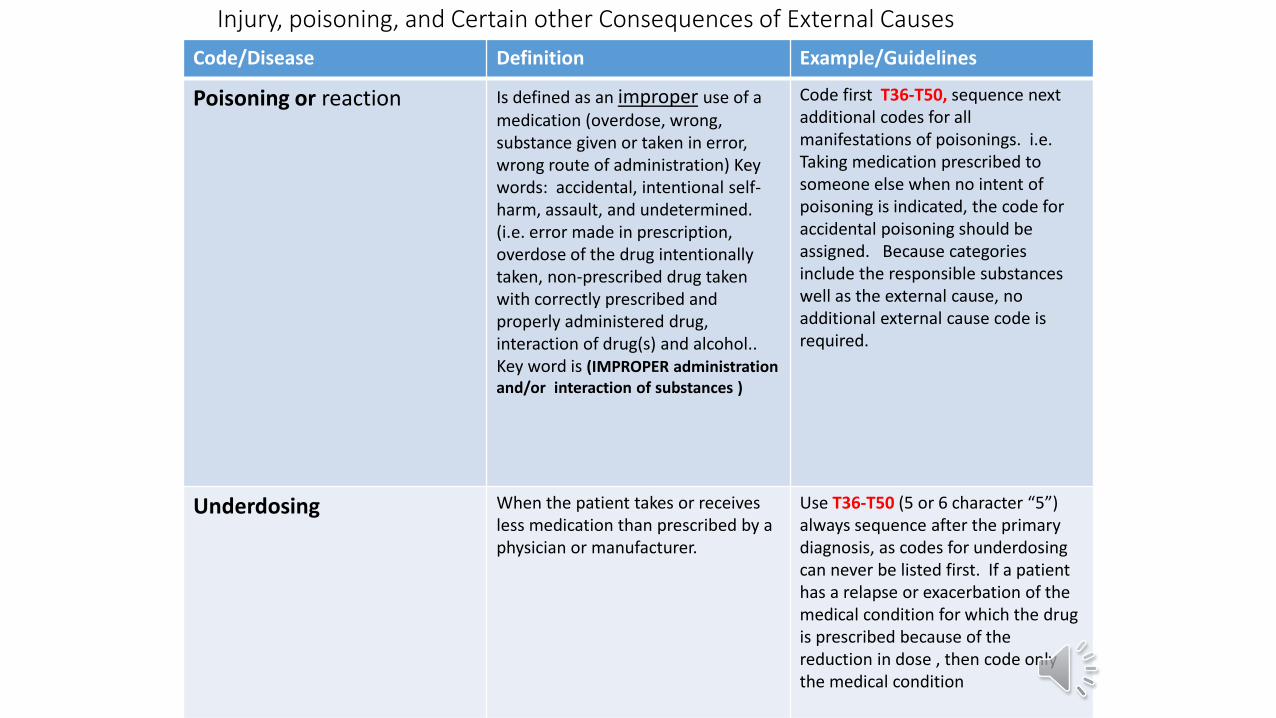
Code/Disease Definition Example/Guidelines
Poisoning or reaction Is defined as an improper use of a medication (overdose, wrong, substance given or taken in error, wrong route of administration) Key words: accidental, intentional self-harm, assault, and undetermined. (i.e. error made in prescription, overdose of the drug intentionally taken, non-prescribed drug taken with correctly prescribed and properly administered drug, interaction of drug(s) and alcohol.. Key word is (IMPROPER administration and/or interaction of substances )
Code first T36-T50, sequence nextadditional codes for all manifestations of poisonings. i.e. Taking medication prescribed to someone else when no intent of poisoning is indicated, the code for accidental poisoning should be assigned. Because categories include the responsible substances well as the external cause, no additional external cause code is required.
Underdosing When the patient takes or receives less medication than prescribed by a physician or manufacturer.
Use T36-T50 (5 or 6 character “5”) always sequence after the primary diagnosis, as codes for underdosingcan never be listed first. If a patient has a relapse or exacerbation of the medical condition for which the drug is prescribed because of the reduction in dose , then code only the medical condition
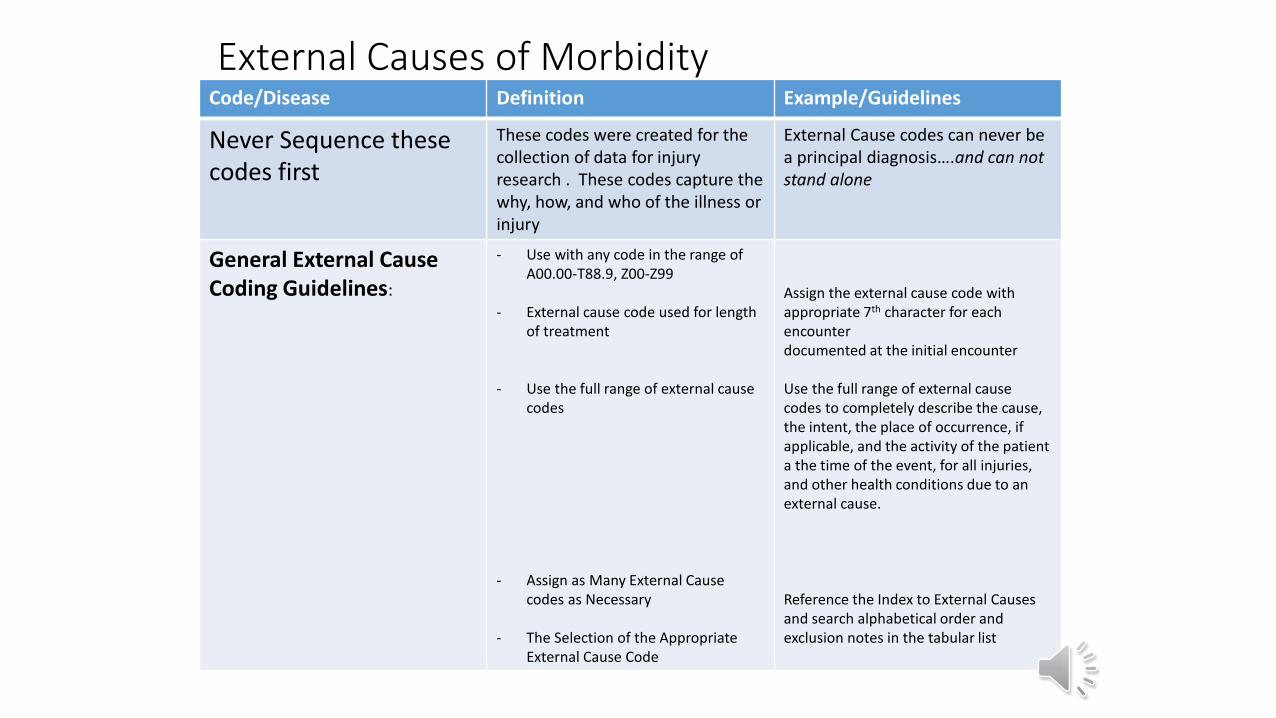
External Causes of MorbidityCode/Disease Definition Example/Guidelines
Never Sequence these codes first
These codes were created for the collection of data for injury research . These codes capture the why, how, and who of the illness or injury
External Cause codes can never be a principal diagnosis….and can not stand alone
General External Cause Coding Guidelines:
- Use with any code in the range of A00.00-T88.9, Z00-Z99
- External cause code used for length of treatment
- Use the full range of external cause codes
- Assign as Many External Cause codes as Necessary
- The Selection of the Appropriate External Cause Code
Assign the external cause code with appropriate 7th character for each encounter documented at the initial encounter
Use the full range of external cause codes to completely describe the cause, the intent, the place of occurrence, if applicable, and the activity of the patient a the time of the event, for all injuries, and other health conditions due to an external cause.
Reference the Index to External Causes and search alphabetical order and exclusion notes in the tabular list
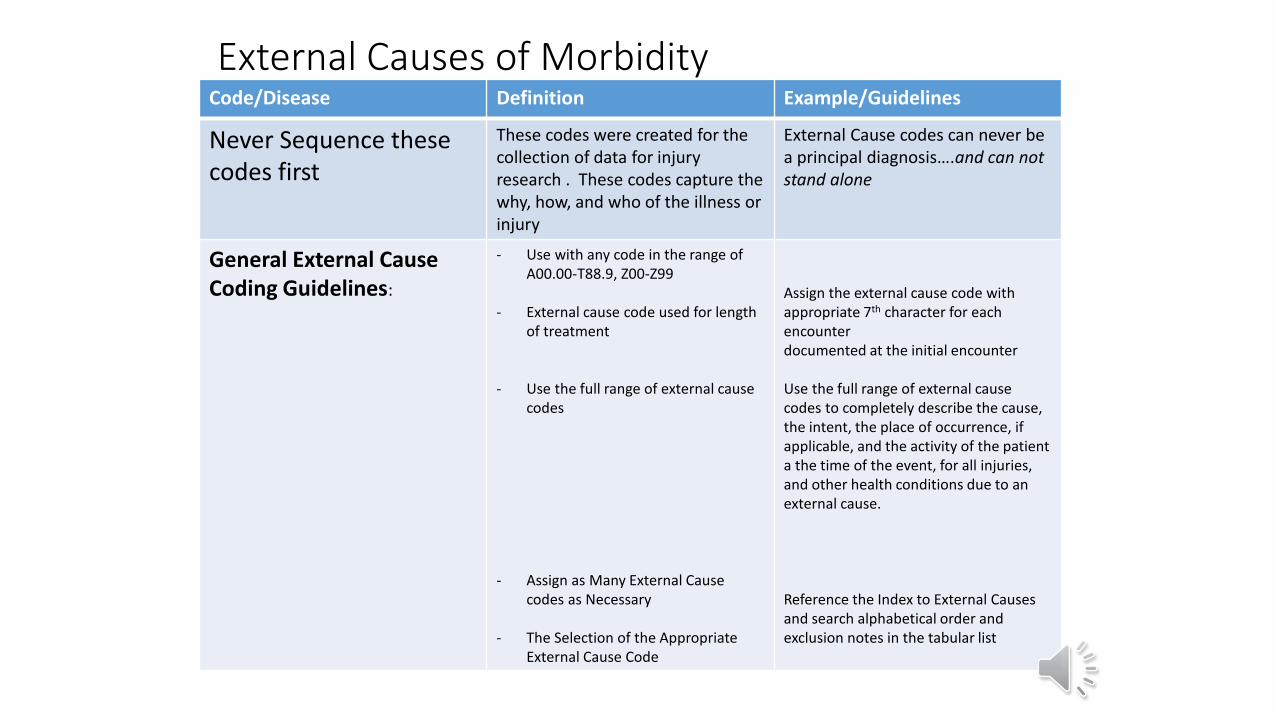
External Causes of MorbidityCode/Disease Definition Example/Guidelines
Never Sequence these codes first
These codes were created for the collection of data for injury research . These codes capture the why, how, and who of the illness or injury
External Cause codes can never be a principal diagnosis….and can not stand alone
General External Cause Coding Guidelines:
- Use with any code in the range of A00.00-T88.9, Z00-Z99
- External cause code used for length of treatment
- Use the full range of external cause codes
- Assign as Many External Cause codes as Necessary
- The Selection of the Appropriate External Cause Code
Assign the external cause code with appropriate 7th character for each encounter documented at the initial encounter
Use the full range of external cause codes to completely describe the cause, the intent, the place of occurrence, if applicable, and the activity of the patient a the time of the event, for all injuries, and other health conditions due to an external cause.
Reference the Index to External Causes and search alphabetical order and exclusion notes in the tabular list
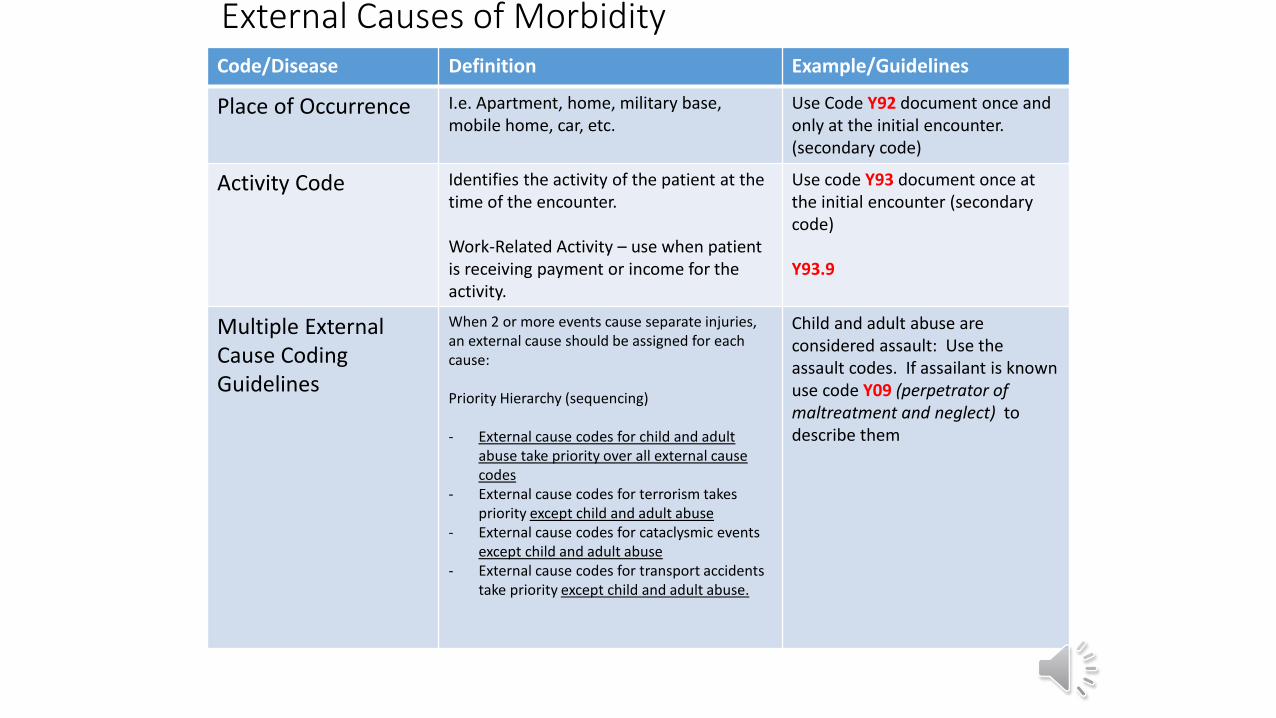
External Causes of MorbidityCode/Disease Definition Example/Guidelines
Place of Occurrence I.e. Apartment, home, military base, mobile home, car, etc.
Use Code Y92 document once and only at the initial encounter. (secondary code)
Activity Code Identifies the activity of the patient at the time of the encounter.
Work-Related Activity – use when patient is receiving payment or income for the activity.
Use code Y93 document once at the initial encounter (secondary code)
Y93.9
Multiple External Cause Coding Guidelines
When 2 or more events cause separate injuries, an external cause should be assigned for each cause:
Priority Hierarchy (sequencing)
- External cause codes for child and adult abuse take priority over all external cause codes
- External cause codes for terrorism takes priority except child and adult abuse
- External cause codes for cataclysmic events except child and adult abuse
- External cause codes for transport accidents take priority except child and adult abuse.
Child and adult abuse are considered assault: Use the assault codes. If assailant is known use code Y09 (perpetrator of maltreatment and neglect) to describe them
External Causes of MorbidityCode/Disease Definition Example/Guidelines
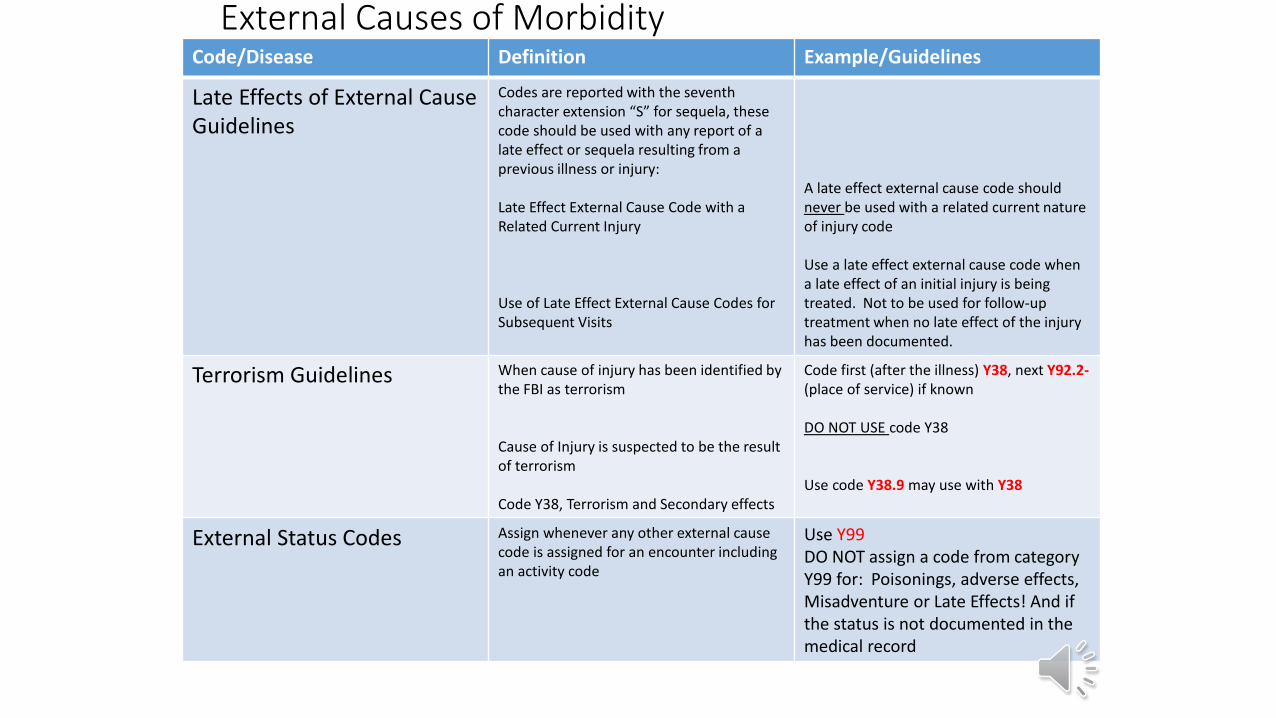
Late Effects of External Cause Guidelines
Codes are reported with the seventh character extension “S” for sequela, thesecode should be used with any report of a late effect or sequela resulting from a previous illness or injury:
Late Effect External Cause Code with a Related Current Injury
Use of Late Effect External Cause Codes for Subsequent Visits
A late effect external cause code should never be used with a related current nature of injury code
Use a late effect external cause code when a late effect of an initial injury is being treated. Not to be used for follow-up treatment when no late effect of the injury has been documented.
Terrorism Guidelines When cause of injury has been identified by the FBI as terrorism
Cause of Injury is suspected to be the result of terrorism
Code Y38, Terrorism and Secondary effects
Code first (after the illness) Y38, next Y92.2-(place of service) if known
DO NOT USE code Y38
Use code Y38.9 may use with Y38
External Status Codes Assign whenever any other external cause code is assigned for an encounter including an activity code
Use Y99DO NOT assign a code from category Y99 for: Poisonings, adverse effects, Misadventure or Late Effects! And if the status is not documented in the medical record
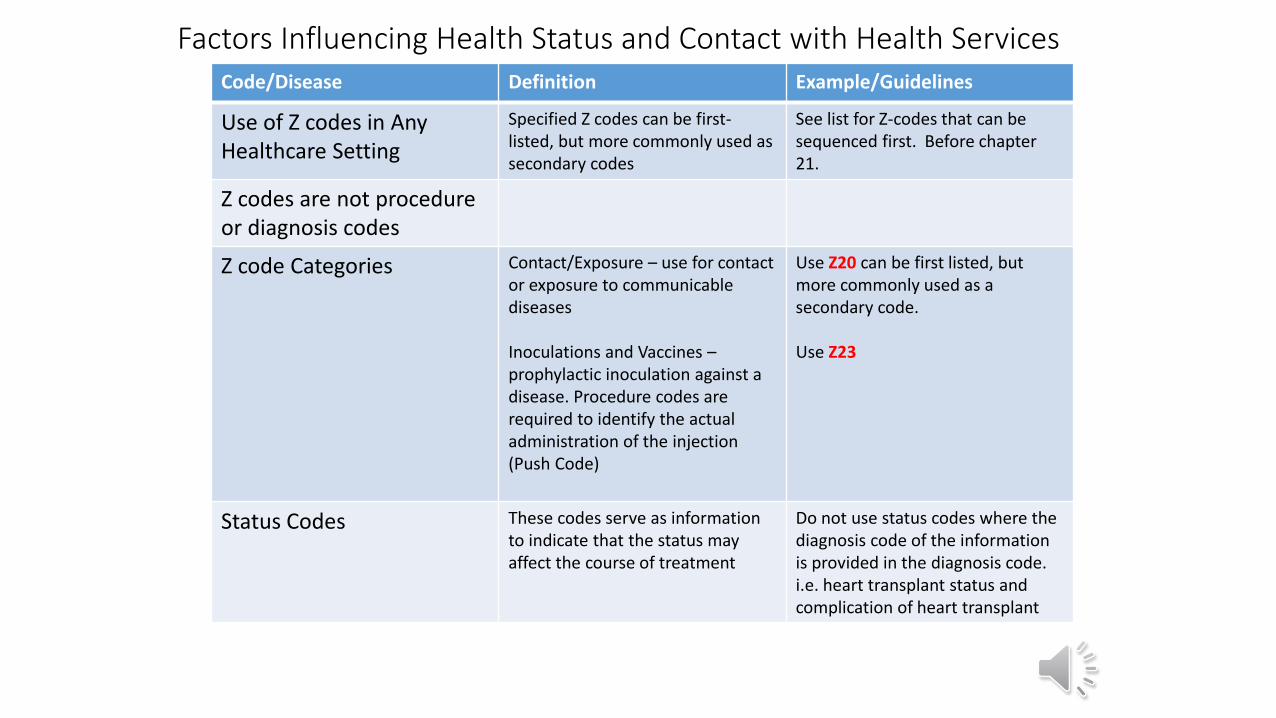
Factors Influencing Health Status and Contact with Health Services Code/Disease Definition Example/Guidelines
Use of Z codes in AnyHealthcare Setting
Specified Z codes can be first-listed, but more commonly used as secondary codes
See list for Z-codes that can be sequenced first. Before chapter 21.
Z codes are not procedure or diagnosis codes
Z code Categories Contact/Exposure – use for contact or exposure to communicable diseases
Inoculations and Vaccines –prophylactic inoculation against a disease. Procedure codes are required to identify the actual administration of the injection (Push Code)
Use Z20 can be first listed, but more commonly used as a secondary code.
Use Z23
Status Codes These codes serve as information to indicate that the status may affect the course of treatment
Do not use status codes where the diagnosis code of the information is provided in the diagnosis code. i.e. heart transplant status and complication of heart transplant
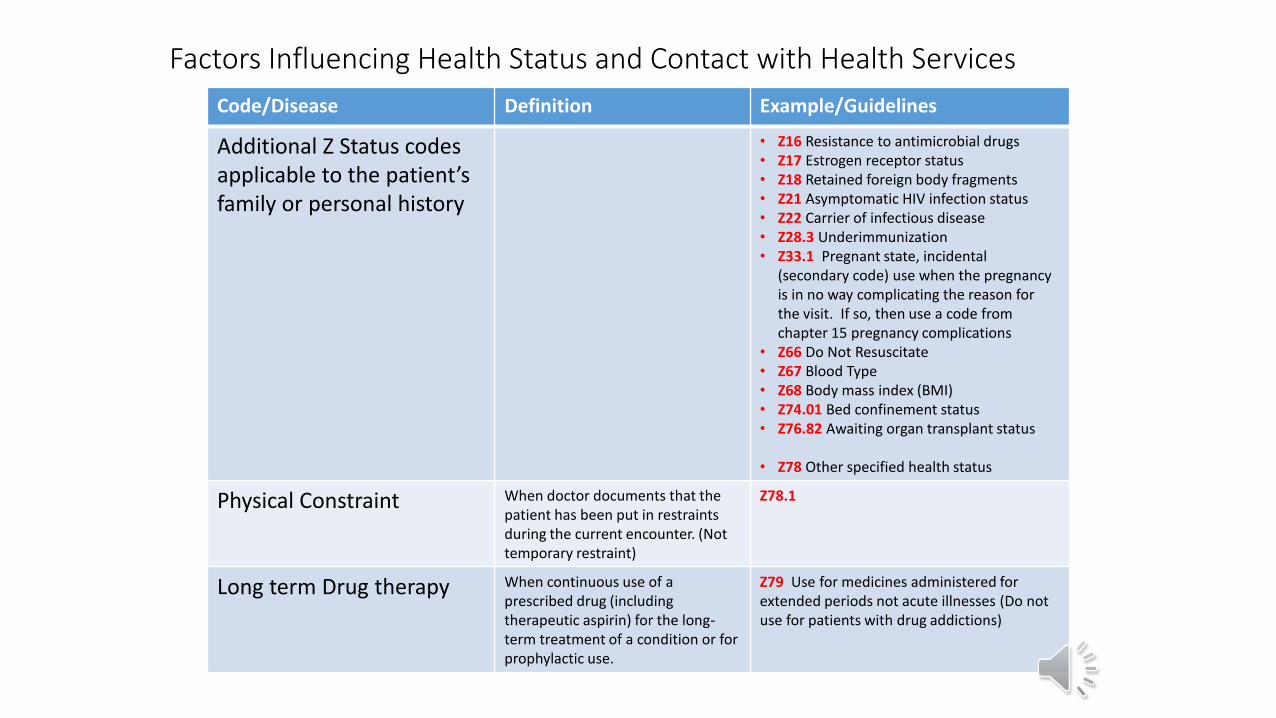
Code/Disease Definition Example/Guidelines
Additional Z Status codes applicable to the patient’s family or personal history
• Z16 Resistance to antimicrobial drugs• Z17 Estrogen receptor status• Z18 Retained foreign body fragments• Z21 Asymptomatic HIV infection status• Z22 Carrier of infectious disease• Z28.3 Underimmunization• Z33.1 Pregnant state, incidental
(secondary code) use when the pregnancy is in no way complicating the reason for the visit. If so, then use a code from chapter 15 pregnancy complications
• Z66 Do Not Resuscitate• Z67 Blood Type• Z68 Body mass index (BMI)• Z74.01 Bed confinement status• Z76.82 Awaiting organ transplant status
• Z78 Other specified health status
Physical Constraint When doctor documents that the patient has been put in restraints during the current encounter. (Not temporary restraint)
Z78.1
Long term Drug therapy When continuous use of a prescribed drug (including therapeutic aspirin) for the long-term treatment of a condition or for prophylactic use.
Z79 Use for medicines administered for extended periods not acute illnesses (Do not use for patients with drug addictions)
Factors Influencing Health Status and Contact with Health Services
Factors Influencing Health Status and Contact with Health Services
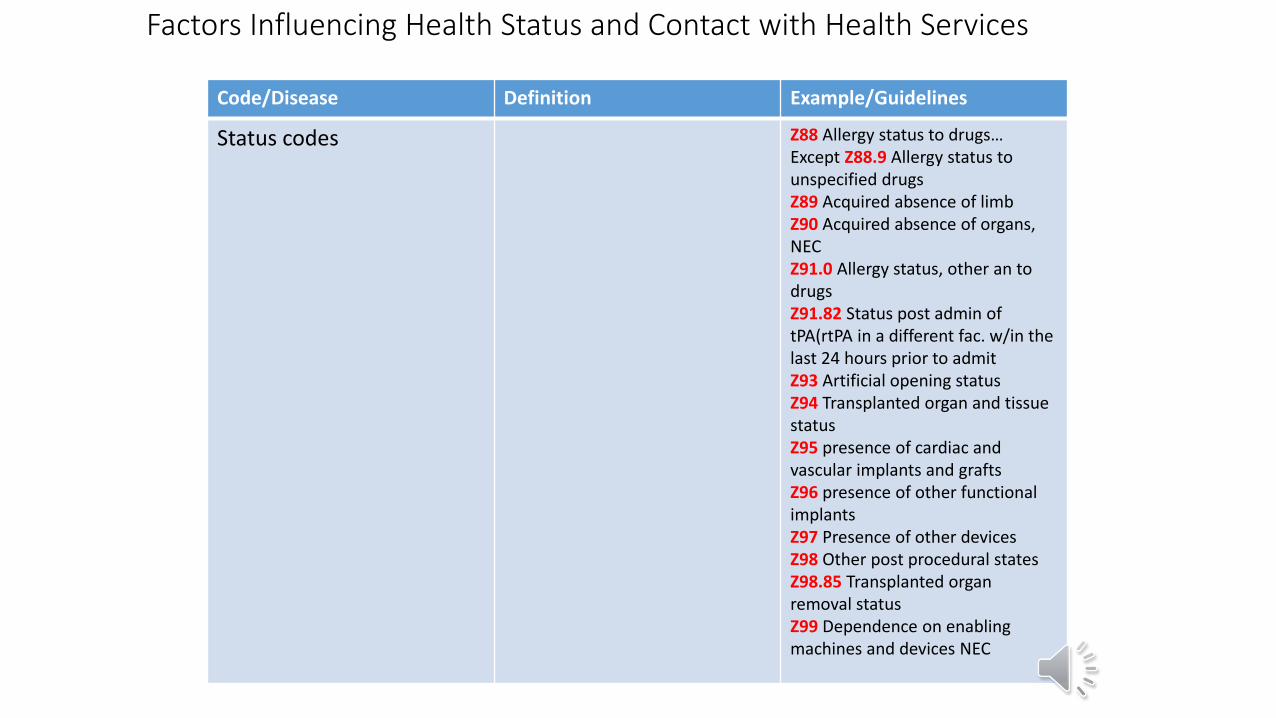
Code/Disease Definition Example/Guidelines
Status codes Z88 Allergy status to drugs…Except Z88.9 Allergy status to unspecified drugsZ89 Acquired absence of limbZ90 Acquired absence of organs, NECZ91.0 Allergy status, other an to drugsZ91.82 Status post admin of tPA(rtPA in a different fac. w/in the last 24 hours prior to admit Z93 Artificial opening statusZ94 Transplanted organ and tissue statusZ95 presence of cardiac and vascular implants and graftsZ96 presence of other functional implantsZ97 Presence of other devicesZ98 Other post procedural statesZ98.85 Transplanted organ removal statusZ99 Dependence on enabling machines and devices NEC
Factors Influencing Health Status and Contact with Health Services
Code/Disease Definition Example/Guidelines
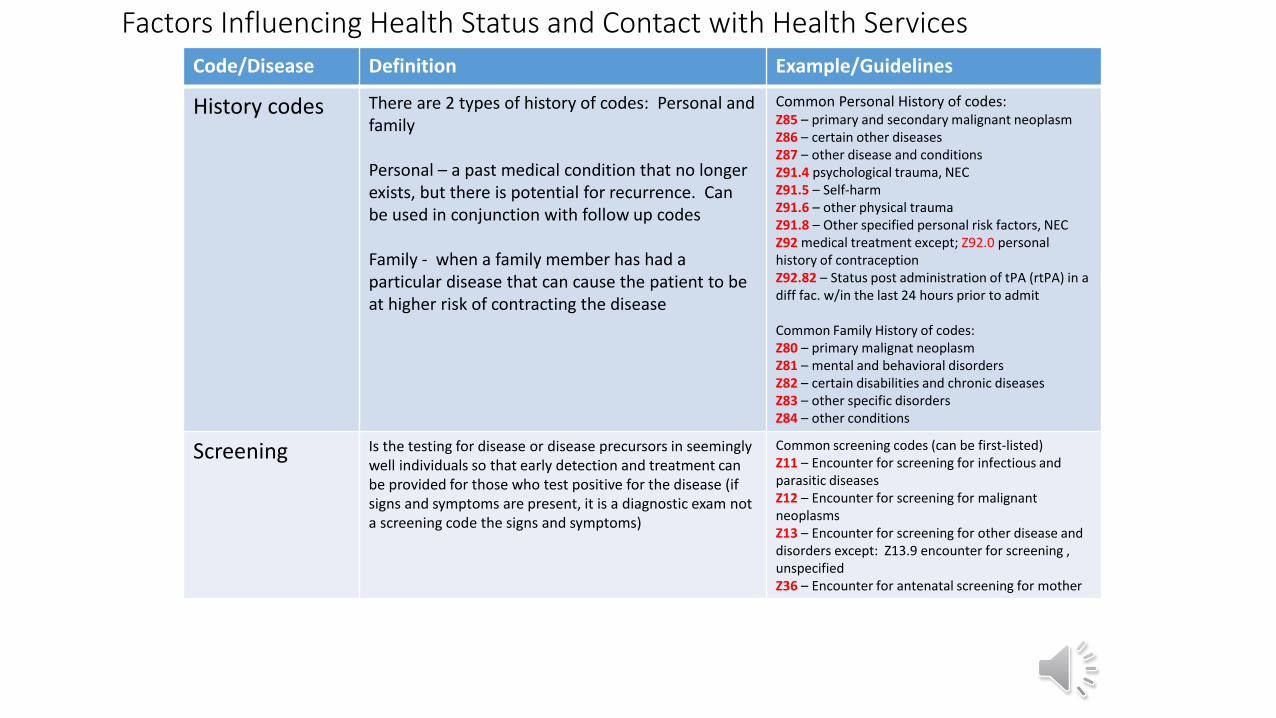
History codes There are 2 types of history of codes: Personal and family
Personal – a past medical condition that no longer exists, but there is potential for recurrence. Can be used in conjunction with follow up codes
Family - when a family member has had a particular disease that can cause the patient to be at higher risk of contracting the disease
Common Personal History of codes:Z85 – primary and secondary malignant neoplasmZ86 – certain other diseasesZ87 – other disease and conditionsZ91.4 psychological trauma, NECZ91.5 – Self-harmZ91.6 – other physical traumaZ91.8 – Other specified personal risk factors, NECZ92 medical treatment except; Z92.0 personal history of contraceptionZ92.82 – Status post administration of tPA (rtPA) in a diff fac. w/in the last 24 hours prior to admit
Common Family History of codes:Z80 – primary malignat neoplasmZ81 – mental and behavioral disordersZ82 – certain disabilities and chronic diseasesZ83 – other specific disordersZ84 – other conditions
Screening Is the testing for disease or disease precursors in seemingly well individuals so that early detection and treatment can be provided for those who test positive for the disease (if signs and symptoms are present, it is a diagnostic exam not a screening code the signs and symptoms)
Common screening codes (can be first-listed)Z11 – Encounter for screening for infectious and parasitic diseasesZ12 – Encounter for screening for malignant neoplasmsZ13 – Encounter for screening for other disease and disorders except: Z13.9 encounter for screening , unspecifiedZ36 – Encounter for antenatal screening for mother
Factors Influencing Health Status and Contact with Health Services Code/Disease Definition Example/Guidelines
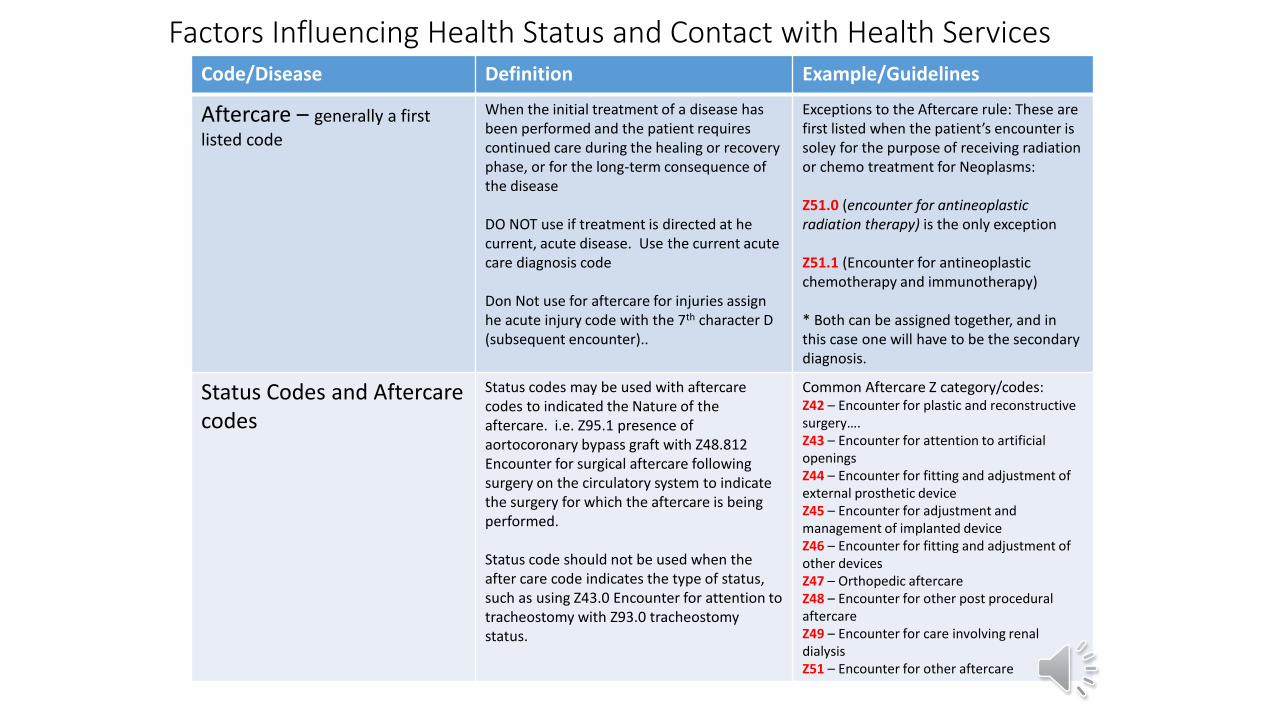
Aftercare – generally a first
listed code
When the initial treatment of a disease has been performed and the patient requires continued care during the healing or recovery phase, or for the long-term consequence of the disease
DO NOT use if treatment is directed at he current, acute disease. Use the current acute care diagnosis code
Don Not use for aftercare for injuries assign he acute injury code with the 7th character D (subsequent encounter)..
Exceptions to the Aftercare rule: These are first listed when the patient’s encounter is soley for the purpose of receiving radiation or chemo treatment for Neoplasms:
Z51.0 (encounter for antineoplastic radiation therapy) is the only exception
Z51.1 (Encounter for antineoplastic chemotherapy and immunotherapy)
* Both can be assigned together, and in this case one will have to be the secondary diagnosis.
Status Codes and Aftercare codes
Status codes may be used with aftercare codes to indicated the Nature of the aftercare. i.e. Z95.1 presence of aortocoronary bypass graft with Z48.812 Encounter for surgical aftercare following surgery on the circulatory system to indicate the surgery for which the aftercare is being performed.
Status code should not be used when the after care code indicates the type of status, such as using Z43.0 Encounter for attention to tracheostomy with Z93.0 tracheostomy status.
Common Aftercare Z category/codes:Z42 – Encounter for plastic and reconstructive surgery….Z43 – Encounter for attention to artificial openingsZ44 – Encounter for fitting and adjustment of external prosthetic deviceZ45 – Encounter for adjustment andmanagement of implanted deviceZ46 – Encounter for fitting and adjustment of other devicesZ47 – Orthopedic aftercareZ48 – Encounter for other post procedural aftercareZ49 – Encounter for care involving renal dialysisZ51 – Encounter for other aftercare
Factors Influencing Health Status and Contact with Health Services
Code/Disease Definition Example/Guidelines
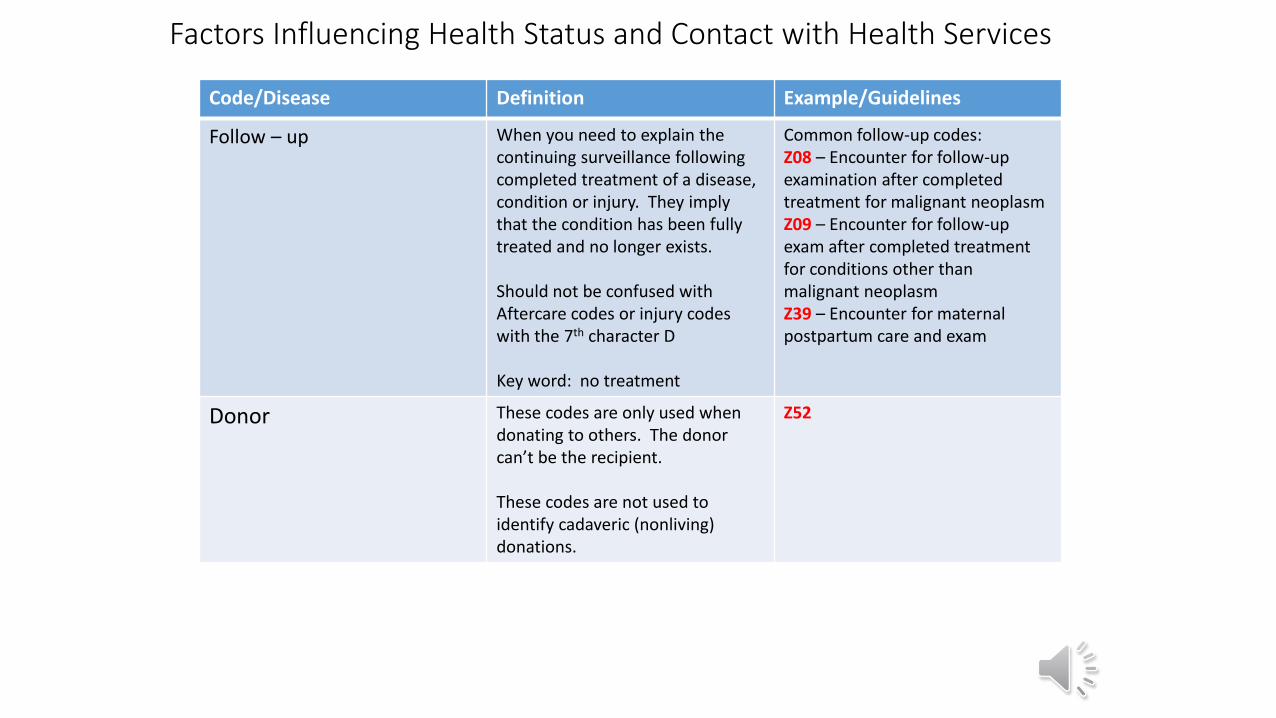
Follow – up When you need to explain thecontinuing surveillance following completed treatment of a disease, condition or injury. They imply that the condition has been fully treated and no longer exists.
Should not be confused with Aftercare codes or injury codes with the 7th character D
Key word: no treatment
Common follow-up codes:Z08 – Encounter for follow-up examination after completed treatment for malignant neoplasmZ09 – Encounter for follow-up exam after completed treatment for conditions other than malignant neoplasmZ39 – Encounter for maternal postpartum care and exam
Donor These codes are only used when donating to others. The donor can’t be the recipient.
These codes are not used to identify cadaveric (nonliving) donations.
Z52
Factors Influencing Health Status and Contact with Health Services
Code/Disease Definition Example/Guidelines
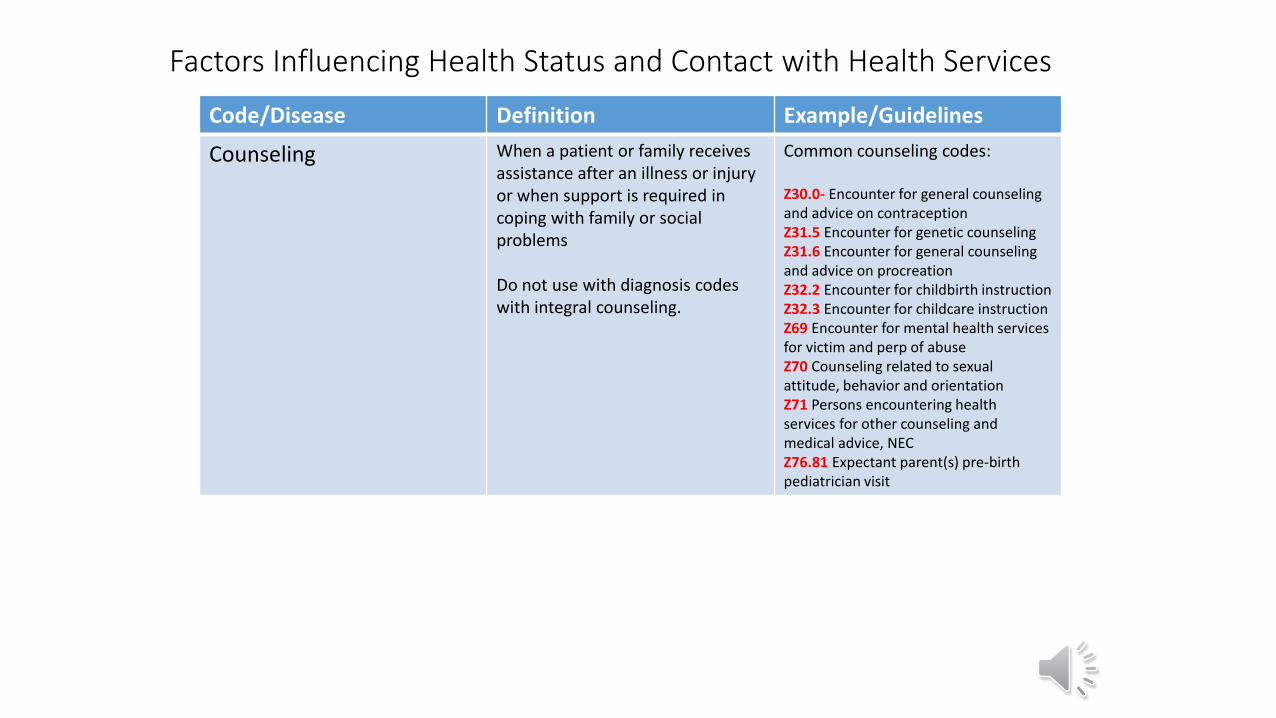
Counseling When a patient or family receives assistance after an illness or injury or when support is required in coping with family or social problems
Do not use with diagnosis codes with integral counseling.
Common counseling codes:
Z30.0- Encounter for general counseling and advice on contraception Z31.5 Encounter for genetic counselingZ31.6 Encounter for general counseling and advice on procreationZ32.2 Encounter for childbirth instructionZ32.3 Encounter for childcare instructionZ69 Encounter for mental health services for victim and perp of abuseZ70 Counseling related to sexual attitude, behavior and orientation Z71 Persons encountering health services for other counseling and medical advice, NECZ76.81 Expectant parent(s) pre-birth pediatrician visit
Factors Influencing Health Status and Contact with Health Services
Code/Disease Definition Example/Guidelines
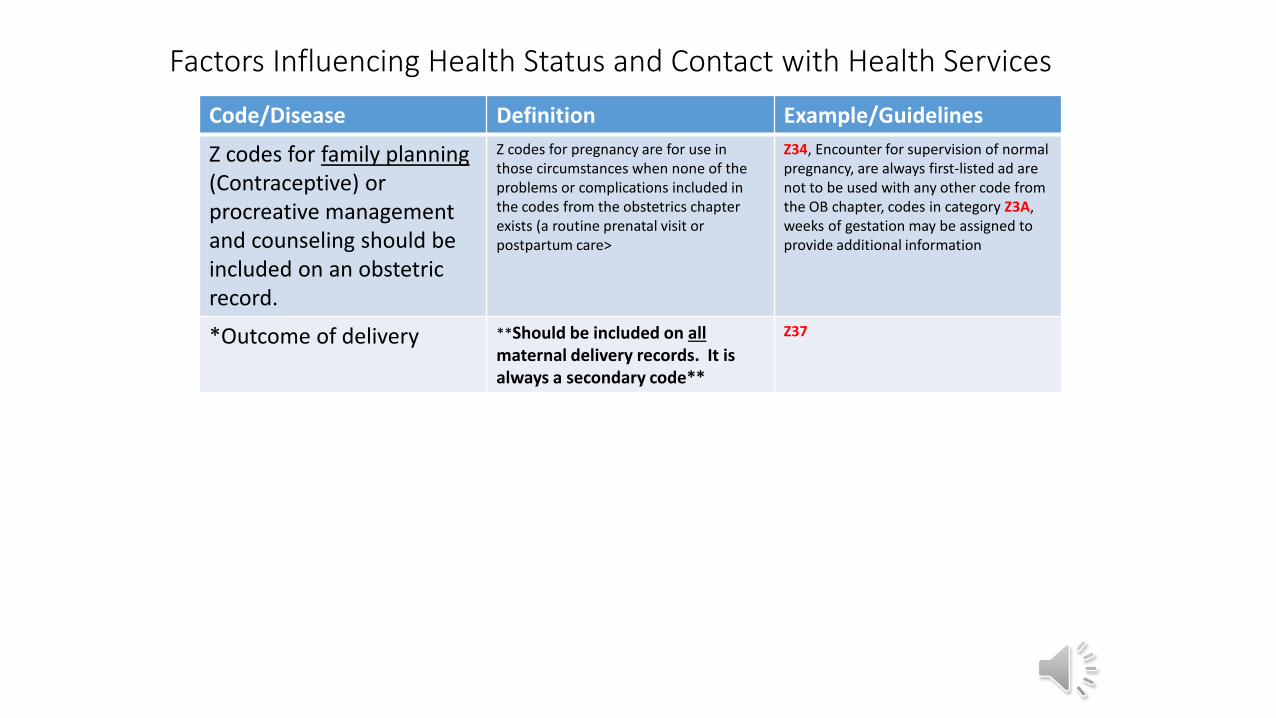
Z codes for family planning(Contraceptive) or procreative management and counseling should be included on an obstetric record.
Z codes for pregnancy are for use in those circumstances when none of the problems or complications included in the codes from the obstetrics chapter exists (a routine prenatal visit or postpartum care>
Z34, Encounter for supervision of normal pregnancy, are always first-listed ad are not to be used with any other code from the OB chapter, codes in category Z3A, weeks of gestation may be assigned to provide additional information
*Outcome of delivery **Should be included on all maternal delivery records. It is always a secondary code**
Z37
References• ICD 10 CM and ICD10 PCS Handbook, 2016 Nelly Leon-Chisen, RHIA
• AHA Coding Clinic Guidelines for ICD 10 CM and ICD 10 PCS, May 2015
• ICD 10CM – Manual
• AAPC public, supplemental manuals and publications 2015