site.iugaza.edu.pssite.iugaza.edu.ps/.../09/physiology-of-the-newborn.docx · web viewfetal...
TRANSCRIPT
Physiology of the Newborn
The neonatal or newborn period is the first 28 days of life during which the infant undergoes amazing growth and change.
Respiratory Changes :The primary function of the respiratory system is two fold: the exchange of oxygen and carbon dioxide through respiration and maintenance of the acid–base balance.The amniotic fluid plays an important role in fetal lung development. Inhalation of the amnioticfluid into the lungs helps to promote growth and differentiation of the lung tissue. Normal pulmonary functioningis dependent on two factors: the alternating in and out fetal breathing movements and the formation of intrapulmonary fluid.Fetal breathing movements from11wk.During a vaginal birth, approximately one third of the fetal lung fluid is expelled due to the “thoracic squeeze” that occurs during passage through the birth canal. Infants of cesarean births are at a higher risk for pulmonary transitional difficulties because they do not receive the lung compression benefits associated with a vaginal birth
Lung expansion after birth stimulates the release of surfactant, a slippery, detergent-like lipoprotein. Surfactantcauses a decreased surface tension within the alveoli, which allows for alveolar re-expansion after each exhalation. Under normal circumstances, by the 34th to 36th weeks of gestation, surfactant is produced in sufficient amounts to maintain alveolar stability (Bloom, 2006).
89
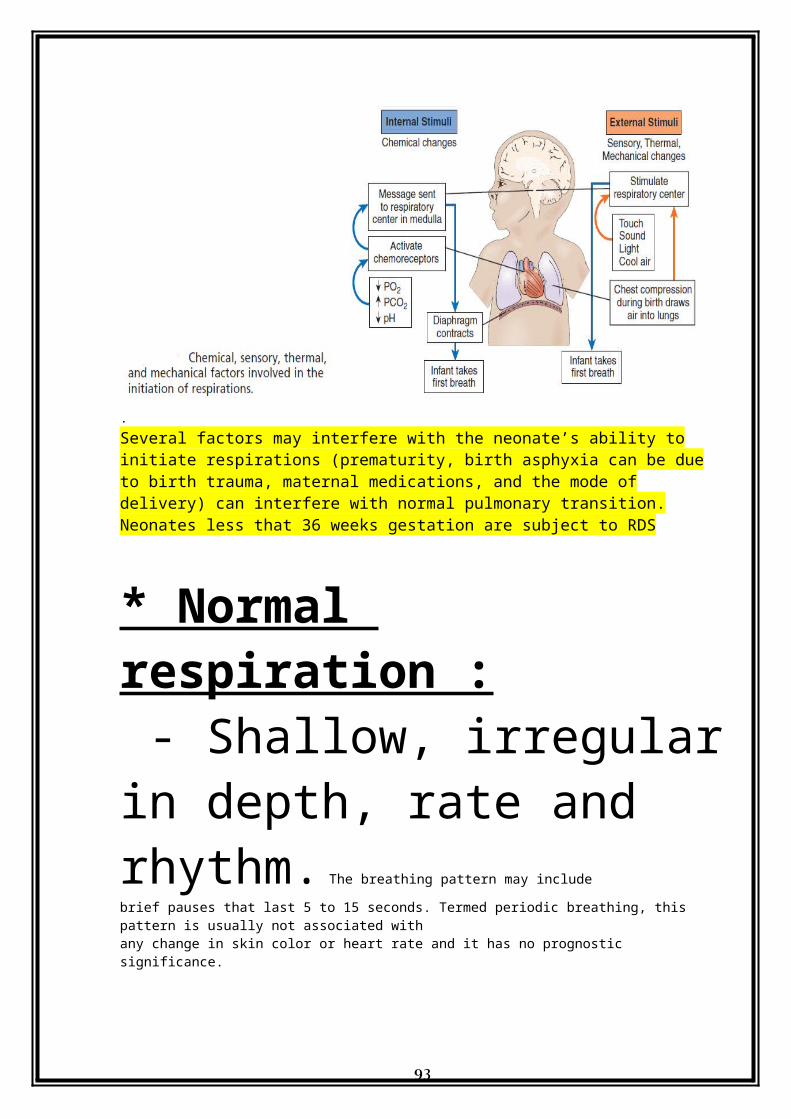
Initiation of respiration: a combination of physical, sensory, thermal, and chemical factors:1. physical : sudden change
from intrauterine life produces stimulations needed to initiate respiration.
2. Chemical :, hypercapnia ↑CO2, hypoxia ↓O2, and acidosis ↓PH level.
3. Sensory : maximum effort is required to expand the lungs and full the collapsed alveoli.
90

4.Thermal; The drastic change in temperature helps to stimulate the initiation of respirations.Sensors in the skin respond to the temperature changes and send signals to the respiratory system in the brain. Physiological changes in the neonate’s temperature may occur and as long as the temperature remains within the normal range of 36.5 to 37.0ºC
.Several factors may interfere with the neonate’s ability to initiate respirations (prematurity, birth asphyxia can be due to birth trauma, maternal medications, and the mode of delivery) can interfere with normal pulmonary transition.Neonates less that 36 weeks gestation are subject to RDS
* Normal respiration : - Shallow, irregular in depth, rate and rhythm. The breathing pattern may include
91
brief pauses that last 5 to 15 seconds. Termed periodic breathing, this pattern is usually not associated withany change in skin color or heart rate and it has no prognostic significance.
- 30/40 - 60 breath \ minute- Affected by such things like crying.- Accomplished mainly by the diaphragm and abdominal muscles.- Dyspnea or cyanosis may indicate anomaly or pathology.
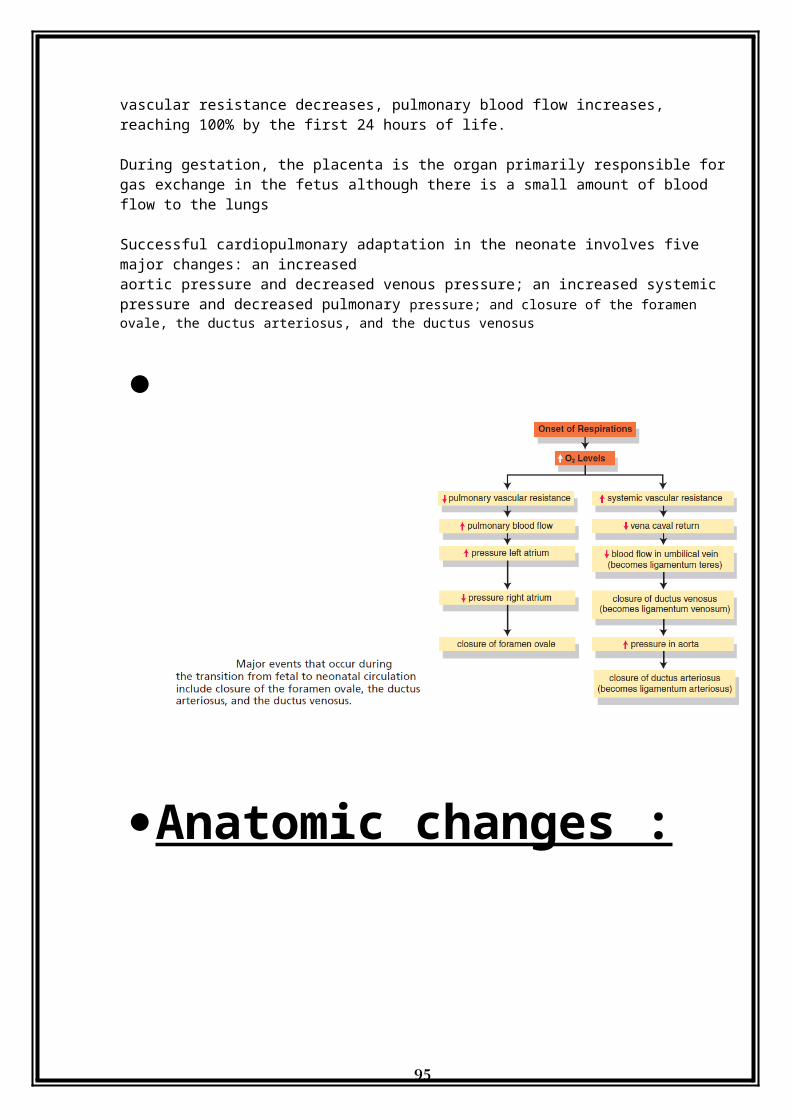
Circulatory Changes:As air enters the lungs, the PO2 rises in the alveoli. This normal physiologic response causes pulmonary artery relaxation and results in a decrease in pulmonary vascular resistance. As the pulmonary vascular resistance decreases, pulmonary blood flow increases, reaching 100% by the first 24 hours of life.
During gestation, the placenta is the organ primarily responsible for gas exchange in the fetus although there is a small amount of blood flow to the lungs
Successful cardiopulmonary adaptation in the neonate involves five major changes: an increasedaortic pressure and decreased venous pressure; an increased systemic pressure and decreased pulmonary pressure; and closure of the foramen ovale, the ductus arteriosus, and the ductus venosus
92
Anatomic changes : - Umbilical arteries and vein
contract and close.- Ductus arteriosus close
within 24/27 hours due to increased PaO2 after clamping the cord and lungs start to work. Also decreased prostaglandin E2.
93
- Ductus arteriosus (3-4wks)and ductus venosus (IVC & UV) are converted to fibrous tissue ( ligaments ) within 2 - 3 months.
- When the pressure in the left ventricle & atrium exceed than that of right atrium
Formen Ovale close. Oxygen-rich blood returning to the heart from the inferior vena cava crosses from the right atria to the left atria across the foramen ovale.
Foramen ovale closes functionally 1-2 hrs after delivery, physiologically by 1 month, anatomically by 6 months)
Blood Volume : 85 - 100 ml \ kg at birth.
The full-term infant’s average blood volume ranges from 80-90 mL/kg of body weight, as compared with a blood volume of 90 to 105 mL/kg of body weight in the preterm infant.
94
Peripheral Circulation : residual cyanosis in hands and feet (Acrocyanosis).
Pulse Rate : Immediately after birth, the newborn’s pulse rate may reach 160 to 180 beats per minute but during the first 30 minutes of life, the rate should decline to 120 to 160 beats per minute
120 - 160 beat \ minute, apical rate is more accurate.Blood Pressure : 70\40 mmhg at birth, 100\50 mmhg by the 10 day.
Blood Elements : ( Hb 16 - 22 gm ,FHb,HbF has a greater affi nity for oxygen than does HbA, the
newborn’s blood oxygen saturation is greater than that found in adults.), ( leukocytes 15,000 - 20,000 \ ml )
95
BloodCoaguation : - Coagulability is temporarily
diminished because of lack of bacteria in the intestinal tract that contribute to the synthesis of vitamin K.
- Coagulation time 3 – 4 minutes.
- Bleeding time 2 - 4 minutes.
- Prothrombin 50% decreasing to 20% - 30%.
- The normal newborn’s platelet (thrombocyte) levels range from 150,000
96
to 300,000/mm3 (as in adults). Small for gestational age (SGA) infants may have platelet counts up to 25% lower than those found in appropriate for gestational age neonates.
Temperature Regulation:The neutral thermal environment (NTE) is the range of temperature in which the newborn’s body temperature can be maintained with minimal metabolic demands and oxygen consumption.
A term infant’s core temperature can fall by approximately 0.5ºF (0.3ºC) per minute up to a total of 5.4ºF (3ºC) before ever leaving the birthing area. However, most term newborns are able to restore the initial decline in body temperature and stabilize at a normal temperature of 97.7ºF (36.5ºC) to 98.6ºF (37ºC) within 2 to 3 hours after birth
At birth temperature is as mother one. The newborn has poor ability regulate his body temperature because of :
97
He has little fat insulation; neonates
have less than half of the amount of subcutaneous fat normally present in adults..- He has large body surface.- He has a relatively poor
circulation.- He doesn't yet sweat or
shiver.- Weak muscles to maintain
flexed position.- Their skin is thin and their blood vessels are close to
body surface,
98
Basal Metabolism:
- Surface area of the infant is large in comparison with body surface.
- Basal metabolism per kg of body is higher than that of adult.
- Caloric requirements are high (117 calorise \ kg day).
Renal Funcion:In the term newborn, the following three major physiologicalfactors enable the kidneys to manage bodily fluidsand excrete urine:• The nephrons are fully functional by 34 to 36 weeksof gestation.• The glomerular filtration rate is lower than that of theadult.• There is a limited capacity for the reabsorption of
99
HCO3– and H_.
- A t birth the kidney's function 30 % - 50% of the adult capacity and are not yet mature enough to concentrate urine. - The infant usually void within 24 hours.- During the first 2 days of life, infants normally void two to six times in a 24-hour period, with a total output of 15 mL/day.During the first 24 to 48 hours, full-term newborns require 60 to 80 mL/kg of fluids to maintain an adequatefluid balance. This requirement increases to 100 to 150 mL/ kg per day after the first few days, and a urine output of 1 to 3 mL/kg per hour is indicative of adequate fluid maintenance (Hertz, 2005).
- Anurea should be reported .
100
- Increase uric acid will stain in the diaper brick dust spots.Hepatic Function :
- Limited because of decrease of GIT activity and decrease blood supply.
Decrease ability to conjugate bilirubin will lead to jaundice. Conjugation is a process that converts the yellow lipid-soluble (nonexcretable) bilirubin pigment(present in bile) into a water-soluble (excretable) pigment.
Jaundice is a condition characterized by a yellow (icteric) coloration of the skin, sclera, and oralmucous membranes. Jaundice results from the accumulation of bile pigments associated
Decrease ability to regulate glucose will lead to hypoglycemia. Glucose is utilized more rapidly in the newborn than in the fetus because of the metabolic events that occur during the normal transitional phase
-The blood glucose of a term infant should be 70% to
101

80% of the maternal blood glucose level.-The serum blood glucose leveldrops during the first 3 hours of life and then graduallyrises over the next 3 to 4 hours to reach a steady state of40 to 80 mg/dL.
- Decrease production of prothrombin will lead to hemorrhage.
Endocrine Function:Disturbances are most often related to maternally provided
102

hormones which can cause the following:
- Vaginal discharge \ bleeding in famale infant.
- Enlargement of mammary glands in both sexes.
- Disturbance related to maternal endocrine pathology ( D. M )
103
Physical Findings:
Posture :
- Full term newborn assumes symmetric posture, face turned to side, flexed extremities, hands tightly fisted with thumb covered by fingers.
- Asymmetric posture may be caused by fracture of clavicle or humerus or never injury.
104
● Length: 45-54/5, 46 - 56 cmBirth weight : (2.3-4.3) 2.9 - 4.1 kg
Skin :- Hair distribution, lanugo hair over the back.- Color : ( cyanosis -
acrocyanosis ), ( pallor - cold, anemia or heart failure)
, ( jaundice - physiologic )- Turgor : full term should
have good skin turgor.
105
- Dryness feeling : sign of post term.
- Vernix : in skin folds.Milia : small white papules or sebaceous cysts on the infant’s face that resemblepimples
- . enlarged sebaceous glands on face, decreased by 2 weeks.
Mangolian spots : are areas that appear gray,dark blue, or purple and are most commonly located on the back and buttocks, although
they may also be found the shoulders, wrists, forearms, and ankles blue pigmentation on lower back, decreased by 4 years.
- Petechiae : pinpoint hemorrhage, decreased within 24 - 48 hours.
106
- Edema : around eyes, face, legs, scrotum, labia and hands.
Head : - Caput succedaneum :
swelling of soft tissue of the scalp.
- Cephalhematoma : subperiosteal hemorrhage .
- Molding: overlapping of skull bones.
- Examine symmetry of facial movement.
107

- Head circumference : 33 - 35/38 cm (2 cm larger than chest ).
- Fontanels : ( enlarged - increased intracranial pressure), ( sunken – dehydration).
- Size of fontanels : ( posterior 2 – 3 months \ molding ), ( anterior 12- 18 months ).
Face :
108
- Eyes : color, hemorrhage, lid edema, conjunctivitis, jaundice, pupils. - Nose : patency and discharge ( nasal breathing )> - Ears : hearing, position, cartilage. - Mouth : size, palate, size of the tongue, teeth, Epstein’s pearls (whitish hardened nodules on thegums or roof of the mouth, may be visualized or palpated . These pearl-like inclusion cysts are not anunusual fi nding and disappear within a few weeks
white nodules ), frenulum linguae, oral thrust.
Neck : 109
- Mobility, lymph nodes,
fractures.- Skin folds : increased in
trisomy 21.- Stiffness : trauma or
infection.
● Chest :
- Circumference : 30 - 33 cm.
- Breast enlargment.
● Abdomen :
110
- protrude slightly, move with chest in respiration.
- Examine umbilical cord for number of vessels, signs of infection, umbilical hernia, usually falls within 7 - 10 days.
Genitalia:
- Female genitalia : vaginal discharge, labia majora cover labia minora.
- Male genitalia : testes in scrotsl sace, examine glans penis for urethral open
111
( open ventrally - hypospadias ), ( open dorsally - epispadias)
Back :
- Spinal column for normal curvature and closure.
- Anal area.
Muscloskletal:
- Extremities for fractures.- Fingers and toes for number
( if extra digit : polydactyly) ( if fused digit : syndactyly).
112

- Hips or dislocation : clicking sounds.
* Neurologic : muscle tone, head control and reflexes.
113

Nursing Care of Newborn
In some hospitals the newborn infant is transferred from delivery room to transitional nursery for intensive observation. When stabilized the infant Infants is admitted to a regular nursery or mother's room. Infants designated as high risk are admitted to an ICU. The immediate care of the newborn infant after arrived in the nursery room:
114
1. Cleansing and assessment:
- Baby's hair is frequently matted with dried blood, the body may have areas with a heavy deposits of vernix caseosa.
- Just remove the excess of vernix and sponge away the dried blood to delicate skin.
- General assessment beside axillary temperature, respiration and pulse are measured at this time.
- Prevent undue exposure, provide warn environment.
115
2. Weighing and measuring:
- The newborn is weighed after arrival to nursery.
- The scales are balanced with a protective paper on which the naked infant is placed.
- Great care is taken to protect the infant from falling of the scales.
- Accuracy is vital since is a part of the baseline date.
116
- 5% - 10% weight loss is normal.
- After 3 – 5 days the baby begins to gain weight and reach their birth weight after 2 weeks.
- Measurement of the head and chest circumferences and length.
3. Estimation gestational age:
- Ability to survive is affected by the maturity of the infant.
117
- Accurate assessment of gestational age is vital to effective care planning.
- Gestational age is determined by standardized measurements of physical growth as : ( preterm, term, post term), ( SGA, AGA, LGA ).
4. Cord care:
- About 2 inches ( 5cm ) of umbilical cord usually is extending from the
118
abdomen with some type of clamp....
- In few days ( 7 - 10 days) the cord shrinks and falls off.
- Observe for signs of hemorrhage, other clamp may be used.
- Protect from infection.- As a precaution against
such an infection, the area around the umbilicus stump is scrubbed and 70% alcohol may be applied.
119
5 .Clothing and cover:
- It is not desirable to constrict their movement with heavy clothes or blankets.
6. Positioning and environment ;
- The baby is placed in a preheated incubator usually on the side with head slightly lower than the rest
120

of the body, this help drains any remaining amniotic fluid or mucus from the stomach and nasopharynx.
- Provide warm environment 24 – 27C◦.
- Never leave the infant alone.
Extra oxygen is not administered unless indicated because retrolental fibroplasias a formation of fibrous tissue behind the lens of the eye, resulting in blindness. 2 a severe form of retinopathy in premature infants associated with complete retinal detachment. It can be prevented by timely administration of retinal laser therapy
, a condition producing blindness may result from excessively high oxygen concentration.
121
7. Recording and identifying:
- All the observation, measurements and care given to the newborn should be carefully recorded on the chart.
- It is the important to label the incubator with a clearly marked card having the mother's name, room number, baby's sex, birth time and date and the physician name.
122
- It is customary to give the card to the mother when she takes her baby home.
8. Feeding and rest:
- After birth the primary need is for rest, so infant is kept NPO for 4 – 6 hours.
- Test blood glucose, infant may be hypoglycemia and require feeding sooner than usual.
9. Discharge planning:
123
- The nurse takes the baby to the mother bedside.
- The mother watches the nurse – cut off the baby's Id. Band and together they check against the mother's band.
- Give instructions about : ● Cord care. ● Follow up. ● Bathing, diapering. ● Breast and formula feeding. ● Measuring body temperature.
124
● Recognizing reportable signs and symptoms " pallor, cyanosis, vomiting, diarrhea, abdominal respiration, fever, hypothermia….".
- Encourage the parents to ask questions and participate in discussion.
-
125

126
127

128
129
130

131
132
Complications of pregnancy
133
Pregnancy is a normal funtion of the body, not a disease several factors can complicate pregnancy. However including preexisting conditions and those that develop during pregnancy. Pregnancy ( S ) that threaten the health of the fetus ot the mother need special care before, during and after delivery.
High Risk pregnancies :
□ Complications of previous pregnancies:
134
- Prolonged labor. - Cesarean birth -PIH - Bleeding - Abnormal fetal position. □ Anatomical abnormalities:- Small pelvis. - Incompetent cervix. □ Metabolic and endocrinological disorders:- Diabetes. - Thyroid disorders.
□ Cardiovascular disorders:
135
- Hypertension - Congenital heart disease. □ Kidney disorders:- Acute pyelonephritis. - Acute cystitis.
□ Hemoatological disorders:- Anemia. - Sick cell anemia.
□ other factors :- Age: under 16 or over 35 years.
136

- Weight : less than 45 kg or over 90 kg.- Syphilis.- Tuberculosis.- Smoking.- Drug addiction.
137