six sigma engages physicians in achieving strategic performance improvement at osf saint francis...
TRANSCRIPT
Six Sigma Engages Physicians inAchieving Strategic PerformanceImprovement at OSF Saint FrancisMedical Center
JODY THOMPSON ,T IM MILLER ,
AMY KRANTZ ,AND T OM THOMAS
Driven largely by a desire to improve the safety andquality of its healthcare services, a large medical cen-ter has achieved dramatic and sustained improve-ment in core clinical processes, in part by gettingresidents and attending physicians involved in SixSigma process improvement teams and change lead-ership. SFMC aligned the Six Sigma managementsystem with its strategy and other performance im-provement methods; implemented a 100-day planto launch the initiative; and built credibility throughsignificant sustained improvements in nonclinicalprocesses that mattered to physicians, before suc-cessfully extending the effort into the clinical andacademic arenas to support evidence-based care.© 2008 Wiley Periodicals, Inc.
Ever since the 2000 publication of the Institute ofMedicine’s To Err is Human, and its shocking con-clusions about medical errors, healthcare qualityand safety have been under intense public and regu-latory agency scrutiny.1 The bar has continued torise as hospital and physician performance is in-creasingly being made public and becoming a keycriterion for reimbursement by payers. There can beno doubt that safely and reliably providing evidence-based care to every patient served is a top concernof every healthcare executive in the United States.
Through due diligence study during 2001, OSF SaintFrancis Medical Center (SFMC) decided to committo full deployment of the Six Sigma ManagementSystem as a vehicle for transformational change andstrategic performance improvement. We were con-
vinced that our organization needed the consistentand rigorous methods offered by Six Sigma to de-velop our people and to create the alignment, ac-countability, and impact needed to enhance strategyexecution capabilities. We were also convinced thatwe must engage physicians in the Six Sigma trans-formation from the outset because they are partnersin care delivery and key stakeholders in all of ourcore processes for providing safe and reliable pa-tient care.
In the beginning of our deployment, we recognizedthe need to align Six Sigma with our culture of car-ing “without regard for the patient’s ability to pay”and our mission of “serving others with the great-est care and love.” Therefore, Six Sigma had to beunderstood as an instrument for improving patientcare rather than the bottom line. With that in mind,we established two firm requirements:
� Six Sigma will focus on strategic performance im-provement; therefore, we will consistently have aportfolio of financial and nonfinancial projects.
� Six Sigma must pay for itself with real and quan-tifiable direct-to-bottom-line net financial im-provements.
Since deployment in 2002, SFMC has achievedtremendous success with the Six Sigma ManagementSystem in clinical and operations processes, realiz-ing more than $18 million in net bottom-line ben-efits, with an average financial return of $200,000per project. In addition, we have developed better
6
c© 2008 Wiley Per iodicals , Inc .Publ ished onl ine in Wi ley InterScience (www.interscience.wi ley .com)Global Business and Organizat ional Excel lence • DOI : 10.1002/ joe .20200 • March/Apr i l 2008

measurement systems and a robust accountabilitymanagement system. Most importantly, we have im-proved problem-solving competencies at all levels ofSFMC and across our multidisciplinary communityof caregivers. We now have a habit of using effectiveinformation to help us make decisions, and we askbetter questions of each other and ourselves.
This article describes the “progress over perfection”approach we took to deploy Six Sigma; the methodswe used to achieve executive and physician com-mitment; how we integrated Six Sigma with otherclinical improvement methodologies; and the resultsof our Six Sigma efforts. We will also share leader-ship challenges, lessons learned, and next steps forthe Six Sigma effort at SFMC.
The Burning Platform for ChangeThe OSF Healthcare System includes seven acutecare facilities, two long-term care facilities, homecare, health plans, and OSF Medical Group, a 200+physician primary and subspecialty medical group.Saint Francis Medical Center, the system’s flagshiphospital in Peoria, Illinois, is a large, complex or-ganization with 570 licensed beds and more than4,500 employees. SFMC is a tertiary care providerand Magnet hospital that includes the Children’sHospital of Illinois, the Illinois Neurological Insti-tute, and the Saint Francis Heart Hospital, as well asa regional Level 1 trauma center with Life Flight ser-vices. SFMC works with 520 independent attendingphysicians and a total of 944 credentialed providers,and is affiliated with the University of IllinoisCollege of Medicine as an independent academicmedical center hosting 50 residents per year.
Like many other healthcare institutions at the turnof the millennium, SFMC was looking for a “betterway” to create and sustain significant improvementsin the time, quality, and cost of our core care deliv-ery processes. Clinical outcome data, as well as sat-isfaction data from patients, staff, and physicians,was telling us that we had many opportunities for
improvement. In addition, Caterpillar (CAT), theworld’s leading manufacturer of construction andmining equipment, with which SFMC has an ex-clusive healthcare provider relationship, was keenlyinterested in reducing costs for healthcare servicesfor their more than 12,000 Peoria-area employees.Helping CAT meet its business needs was a veryimportant consideration for SFMC.
Like many other healthcare institutions at the turn ofthe millennium, SFMC was looking for a “better way”to create and sustain significant improvements inthe time, quality, and cost of our core care deliveryprocesses.
Why Six Sigma?The due diligence team, which included two physi-cians (the assistant administrator for Quality andthe chief safety officer) and two registered nurses(the director of Clinical Performance Improvementand the director of Case Management) worked to-gether for about a year to investigate performanceimprovement methodologies. During our study, wecame to realize that within the healthcare industry,benchmarking to mediocrity was the norm. In otherwords, standard practice within healthcare was tocompare one facility’s performance to that of otherhealthcare organizations, none of which were per-forming at a level nearing perfection.
For example, when compared with other healthcareorganizations, SFMC was performing very well onthe key indicator of “average time from ‘door tostent”’ for treatment of acute myocardial infarction.However, we realized that in terms of Six Sigmaperformance levels, our overall performance fell farshort of perfection, and a significant number of ourpatients were not receiving care within the “aver-age” time.
At that point, we realized how inadequate “average”was as a measure of performance. Not only is it a
Global Business and Organizat ional Excel lence March/Apr i l 2008 7DOI : 10.1002/ joe

Exhibit 1. Fundamental Attributes of a Six Sigma Culture
• Relentless quest for perfection• Customer-focused• Data-driven, fact-based decision making• Rigorous alignment of actions with strategy• Develops people and enhances teamwork• Consistent, scientific approach to problem solving• Measurable success and bottom-line financial impact• Sustainability through process management
poor measure for assessment of total process perfor-mance but also it clearly misses the point from theperspective of those we serve. It was suddenly appar-ent that we must shift our focus from performanceaverages to performance variations.
Six Sigma philosophy began to transform our think-ing. As another example, whereas in the past wewould have proudly touted our 87 percent perfor-mance on appropriate use of beta-blockers at dis-charge for acute myocardial infarction—consideredvery good performance for the time—we now beganto ask why 13 percent of our patients did not receivethis care standard.
As members of the investigation team, we were in-trigued by the change in our own thinking that re-sulted simply from our study of the Six Sigma ap-proach. We also saw the value in Six Sigma’s focuson quality as defined by the customer, data-drivendecision making, and development of competencywith sophisticated statistical analysis tools, as wellas the value in developing our people and using theircollective wisdom for solving SFMC’s most difficultperformance problems. These and other fundamen-tal characteristics of a Six Sigma culture, shown inExhibit 1, were a perfect fit with the mission, vision,and values of our organization.
In addition, process management, which in our in-vestigation was unique to the Six Sigma method-ology, provided a robust method for developingaccountability management systems and sustainingimprovements. We felt this aspect of improvement
was indispensable for creating process ownership atthe point of service.
By the end of our investigation, we were confidentthat SFMC leaders, physicians, and care providers atall levels across the care continuum could buy in tothe Six Sigma Management System as a way to im-prove care for our patients while engaging the caredelivery team in developing new skills and compe-tencies. We believed we could honestly promote SixSigma as a means for strengthening our ability to liveour mission of “serving others with the greatest careand love.” While there were few demonstrated suc-cessful deployments of Six Sigma in healthcare, wewere convinced that Six Sigma was the comprehen-sive framework and rigorous approach we neededto achieve our strategic performance improvementgoals.
Transformational Change via Six SigmaIn the mid-1990s, SFMC had initiated a transfor-mational change to “Live Our Values Every Day.”Around that same time, we implemented the PDSA(Plan, Do, Study, Act) model for quality improve-ment, and became involved in a number of projectswith the Institute for Healthcare Improvement. Inaddition, many of our clinical departments were en-gaged in collaborative quality improvement effortssuch as Vermont Oxford for Neonatal Care and theSociety of Thoracic Surgeons (STS) for improvementof adult outcomes in cardiac surgery. While we didsee some improvements, it was a patchwork of ef-forts only marginally linked to strategy, and the im-provements were difficult to sustain.
Given the mix of improvement methods and activ-ities going on across SFMC, we needed physicians,executives, and staff to understand Six Sigma as
� The next natural step in our transformation� Different but complementary to improvement
methods already employed� The way we would do our work—rather than
more work
8 March/Apr i l 2008 Global Business and Organizat ional Excel lenceDOI : 10.1002/ joe

� A long-term investment in a comprehensiveframework for improvement
SFMC found a unique method of assistance for ourSix Sigma deployment: Caterpillar, whose worldheadquarters is in Peoria. CAT had deployed SixSigma across its global operations in the year 2000,and in late 2001, they invited SFMC to participatein the Six Sigma training programs being offering totheir extended enterprise of suppliers and dealers.With their invitation and the demonstrated successof Six Sigma at CAT, SFMC’s chief operating officerdecided to accept the invitation and deploy the SixSigma Management System, with the support andguidance of CAT’s Six Sigma team.
Best Practice Deployment RecipeWith the chief executive officer’s full support, thechief operating officer, the assistant administratorfor Quality Management, and the director of SixSigma spearheaded the SFMC deployment, with theinitial guidelines that Six Sigma will—
� Change the way we think about work and do ourwork
� Create a direct line of sight from strategy toprojects
� Create sustainable improvement in areas thatmatter most
� Leverage and develop our people� Pay for itself
With high hopes, excitement, and more than a bit oftrepidation, the deployment team attended a week-long workshop for Deployment Champions (DC),where they received the comprehensive training re-quired to deploy Six Sigma using a “best practicedeployment recipe” in a “progress over perfection”approach, which included a 100-day implementa-tion plan. The success recipe shared with us by GlenBarton, then CEO of Caterpillar, was quite simple:
� Lead with clarity, consistency, and commitment.
Exhibit 2. Seven Critical Success Factors for Six SigmaDeployment
• Committed leadership• Full-time Six Sigma Deployment Champions and
Black Belts• Strategy integration• Customer and market focus• Business process framework• Alignment of incentives and accountability• Quantifiable measures and results
� Embrace the Seven Critical Success Factors forSix Sigma Deployment (see Exhibit 2).
� Be accretive (benefits exceed cost in 12 months).
Implementation planning that started at the DCworkshop continued with the immediate formationof a Six Sigma steering team—the initial Six Sigmadeployment team expanded to include the assistantadministrator of Human Resources, the chief finan-cial officer, the director of Public Relations, and thedirector of Decision Support—to plan and executethe 100-day plan. Key aspects of the implementationplan focused on communications, targeted training,and processes for selecting the right people for theSix Sigma Black Belt role and the right projects forour initial improvement efforts.
From the outset, the deployment team knew thatwe needed to make a clear and bold statement ofour expectations for Six Sigma to both leadershipand physicians. One of the key deployment tacticswe learned from CAT was to orchestrate an offi-cial launch of Six Sigma that would clearly com-municate to the executive level “This is different!”We did exactly that through a two-hour awarenesstraining that ended with an executive commitmentsession. Each executive was required to commit tothe CEO, both verbally and in writing, how he orshe would support the Six Sigma deployment overthe next year. Through the project selection process,the steering team ensured that all executives, includ-ing our CEO, were involved in a Six Sigma projectin the initial launch.
Global Business and Organizat ional Excel lence March/Apr i l 2008 9DOI : 10.1002/ joe

CommunicationAt the outset, the SFMC Deployment Championswere confident that the Six Sigma methodologywould work well in operations such as materialsmanagement, patient logistics, and the revenue cy-cle, but were less confident that it would be suc-cessful in clinical process improvement. We knew akey deployment hurdle would be getting our entirecommunity of caregivers, including physicians, tounderstand that Six Sigma was not a “flavor of themonth” but rather the SFMC framework for strat-egy execution and model for process improvement.
With the assistance of the CAT guidelines, the SixSigma steering team created a 12-month communi-cation plan. Key messages were developed for thefirst 100 days as well as the first year of Six Sigmadeployment:
� The first 100 days: The key messages includedwhat was changing; why we were changing; howwe were going to accomplish the change; andwhat we expected to achieve as a result of thechange. The principle behind the key messageswas to provide concise statements that would rep-resent “teachable points of view” (see Exhibit 3).
� The first year: We focused all internal commu-nication activities on projects and Six Sigmaprinciples, with the goals of creating aware-ness, establishing expectations, and communicat-ing progress of the Six Sigma deployment.
Exhibit 3. Key Communication Messages in Six Sigma Launch
• Six Sigma is about success• Engaging our best and brightest to solve our toughest
problems• It’s more about the people than the tools• Direct line of sight from strategy to action• Our patients, our staff, and our physicians deserve it• Progress over perfection• The learning is in the doing
Our communication activities with physicians cen-tered on Six Sigma being different than past effortsin quality improvement. To our delight, we foundthe data-driven, process-focused DMAIC improve-ment methodology of Six Sigma had great appeal toour staff, and particularly to physicians.2
In the past, physicians tended to be skeptical of man-agement initiatives, and so we knew that the mostimportant message for our physicians would be thesuccess of projects that made their work more effi-cient and effective. Because it would take some timeto produce definitive results, our initial commitmentto physicians was that we would not expect them tochange their processes until the medical center coulddemonstrate significant improvement in its own pro-cesses. We clearly focused on the physician as ourcustomer in the first year.
Initial Training and Project Selection ProcessTraining is a fundamental and critical element in de-ploying the Six Sigma Management System to cre-ate transformational change. In the first year, weinvested in a number of focused training sessions,shown in Exhibit 4, to help people at all levelsof the organization understand why we were de-ploying Six Sigma, what Six Sigma is, and how SixSigma would impact their jobs. Key messages fromour communication plan were given great impor-tance as SFMC’s CEO and Deployment Championsprovided key portions of the initial training for the
Exhibit 4. Six Sigma Training Programs
Type of Program DurationDeployment Champion Training 4 daysExecutive Awareness Training
& Commitment Session 2 hoursBusiness Leader and Project
Sponsor Training 4 daysProcess Owner Training 3 daysBlack Belt Training 4 weeksGreen Belt Training 10 hoursStaff Awareness Training 2 hours
10 March/Apr i l 2008 Global Business and Organizat ional Excel lenceDOI : 10.1002/ joe

management team. The amount of focused trainingand communication we provided sent a strong mes-sage to the organization that, indeed, Six Sigma wassomething different.
It is imperative that the organization select “excel-lent” people to fill the role of Six Sigma Black Belt,most obviously because the Black Belts will be lead-ing teams to solve some of the organization’s mostdifficult problems using a rigorous methodology thatincludes statistical analysis. Less obviously, the se-lection process and the resulting choices send a mes-sage to the organization about the importance of theinitiative. Interviews for “Wave I” Black Belts wereconducted by SFMC executives, and eleven excellentpeople were selected for the training.
Our goal was to select strategic projects that wouldimprove physician and staff efficiency, as well asprojects to improve patient safety.
The initial Six Sigma projects were selected duringthe Business Leader and Project Sponsor Trainingevent. With the assistance of our CAT facilitators,we employed a very structured approach for projectselection that helped us align and quantify the strate-gic impact of our project ideas. Our goal was toselect strategic projects that would improve physi-cian and staff efficiency, as well as projects to im-prove patient safety. In addition, we wanted to haveprojects that would penetrate all areas of the medi-cal center, and involve all administrators in at leastone project. The initial projects, and the many thathave since followed, were directed at five categoriesof strategic focus for SFMC:
� Clinical Quality/Safety� Patient Satisfaction� Community of Caregivers (including RN attrac-
tion/retention)� Financial Integrity� Capacity/Strategic Growth
Selecting the right projects and the right peoplefor Black Belts, investing in comprehensive train-ing, and having committed leadership at the topall contributed to the success of the initial projects.Wide communication of those successes created ex-citement and forward momentum for the Six Sigmadeployment. However, demonstrating that the im-provements could be sustained over time has beenthe most important factor in garnering physician,staff, and executive commitment to the Six SigmaManagement System at SFMC. As with all perfor-mance improvement efforts, the challenge of sustain-ability is the true test of an organization’s readinessand ability to change. Through rigorous implemen-tation of process management at project turnover,Six Sigma helped us to not only sustain initial gainsbut also integrate ongoing performance improve-ment and Six Sigma with our daily work.
Integrating Six Sigma with ClinicalQuality ImprovementTo achieve the goal of standardizing SFMC’sproblem-solving approach, including the languageof performance improvement projects, we imple-mented the Six Sigma Management System through-out the organization as a framework for strategicperformance improvement, and DMAIC as the par-ticular methodology for problem solving. We werecareful in our initial communications with physicianleaders and clinical improvement project teams tomake the following distinctions between Six Sigmaimprovements and evidence-based practice improve-ments in the clinical areas:
1. Six Sigma does not “create” evidence-based prac-tice; it removes system and process barriers toimplementing evidence-based practice.
2. Six Sigma is not a clinical research project, butinvestigating the clinical research is part of clini-cal process improvement projects.
3. Six Sigma does not replace improvement effortssuch as IHI and Vermont Oxford Collabora-tives; rather it augments them with a strategic
Global Business and Organizat ional Excel lence March/Apr i l 2008 11DOI : 10.1002/ joe

framework, rigorous methodology, and a com-prehensive set of tools.
It is also important for us to explain to the clinicalstaff that Six Sigma deployment at SFMC is not lim-ited to a specific set of statistical tools, but ratherit incorporates improvement tools from a varietyof methodologies, including Lean Manufacturing,project management, and change management. Us-ing DMAIC with a comprehensive toolkit helps us“keep it simple” for the staff, use standard languagefor improvement, and prevent “methodology wars”that waste time and confuse stakeholders.
Using DMAIC with a comprehensive toolkit helps us“keep it simple” for the staff, use standard languagefor improvement, and prevent “methodology wars”that waste time and confuse stakeholders.
Three clinical quality improvement projects that re-sulted in significant and sustainable improvementswere pivotal in establishing Six Sigma’s credibil-ity with the Medical Staff—a point that cannot beemphasized enough. These projects clearly demon-strated the applicability and benefits of Six Sigmain a clinical environment; the commitment of themedical center to improve patient care outcomes;and the breakthrough performance improvementthat can be achieved through committed physicianparticipation. The projects—which focused on re-duction of pressure ulcers, ventilator-acquired pneu-monia, and blood stream infections—are describedbelow.
Pressure Ulcer ReductionPressure ulcers are wounds that result from reducedblood flow to pressure points on the skin, and fre-quently occur as a clinical complication in the careof very ill, hospitalized patients. One of the first SixSigma projects at SFMC targeted the reduction ofthe incidence of hospital-acquired pressure ulcers.
While not all hospital-acquired pressure ulcers canbe prevented, many can be through evidence-basednursing care processes, including identification ofhigh-risk patients; daily skin assessment; and turn-ing or repositioning the patient frequently. Althoughthe nursing staff understood the evidence-based carestandards, a number of barriers prevented themfrom consistently applying the evidence in their dailywork. The Six Sigma project team identified the rootcauses of the barriers and then implemented solu-tions that decreased the incidence of pressure ulcersper 1,000 patient days from the September 2001baseline rate of 9.4 to 7.3 in July 2002, the end ofPhase I implementation. Not only were the improve-ments sustained over time but also results have con-tinued to improve, with an average incidence rate of2.5 for 2006–2007, as shown in Exhibit 5.
In addition to the convincing clinical results, thisproject demonstrated the power of a clinical teamand the synergy between Six Sigma and evidence-based care. The entire effort stimulated great ex-citement and real commitment within the nursingstaff in the general care units, while making a boldstatement to the physicians and leadership at SFMC.In addition to the clinical and cultural benefits, theproject prevented the additional length of stay asso-ciated with the complication and, in so doing, real-ized more than $3 million in direct-to-bottom-linesavings.
Ventilator-Acquired PneumoniaVentilator-acquired pneumonia (VAP) is a compli-cation of care that frequently occurs in critically illpatients who require ventilator care. According toone study, it carries a mortality rate of 31.9 percent.3
Like pressure ulcers, not all VAPs can be prevented,but many can be through the reliable delivery ofevidence-based care.
During the Business Leader and Project Sponsortraining event, SFMC’s chief trauma surgeon recom-mended that reduction of ventilator-acquired pneu-monia be an early Six Sigma priority. While we did
12 March/Apr i l 2008 Global Business and Organizat ional Excel lenceDOI : 10.1002/ joe

Exhibit 5. Pressure Ulcer Incidence (per 1,000 Patient Days)
not have the data to clearly validate the baseline per-formance, we leveraged the chief’s passion to take aprogress-over-perfection approach and selected thisproject, with him as physician champion.
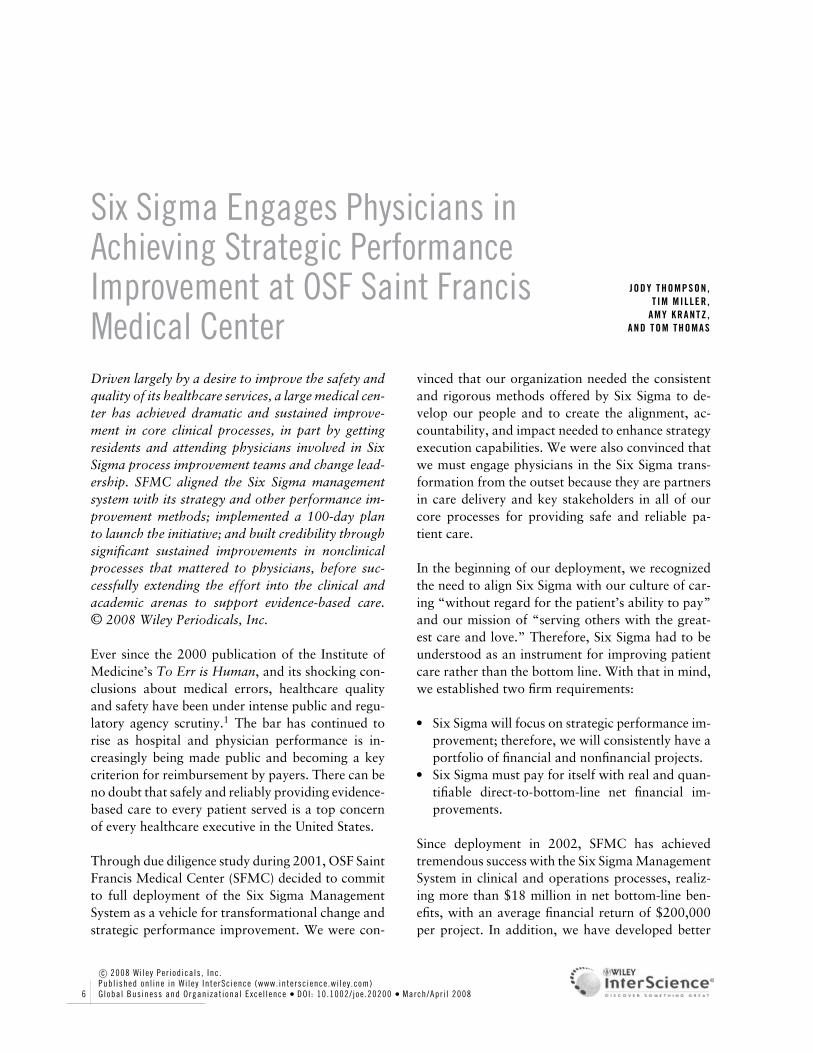
The VAP project became the defining Six Sigmaproject for the nursing staff on the intensive andintermediate care units. Through the VAP team’swork, and the work of the process owners afterturnover, SFMC has lowered the VAP rate, mea-sured as the number of ventilator-acquired pneumo-nias per 1,000 patient days, as shown in Exhibit 6a.It is notable that even as the number of ventila-tor days has trended steadily upward since 2005,the incidence of ventilator-acquired pneumonias hastrended downward, as shown in Exhibit 6b. Theproject results helped transform our understandingand vision of what the SFMC community of care-givers could achieve through the Six Sigma Man-
agement System, and along with the pressure ulcerproject, demonstrated the power of process owner-ship at the bedside.
Blood Stream InfectionsBlood stream infection (BSI), which occurs mostoften as a result of central line insertion, is a seriouscomplication that carries a high mortality rate, andat SFMC increased the patient’s length of stay by anaverage of 40 days. Unlike the pressure ulcer project,reducing BSI would require improvement of bothnursing and physician care processes. Given the levelof physician buy-in that resulted from the sustainedsuccess of the pressure ulcer and VAP projects, in2004 SFMC launched the BSI reduction project.
Once again, the evidence-based care standards wereknown, but the root causes of failure to applythe care standard were system barriers. The initial
Global Business and Organizat ional Excel lence March/Apr i l 2008 13DOI : 10.1002/ joe
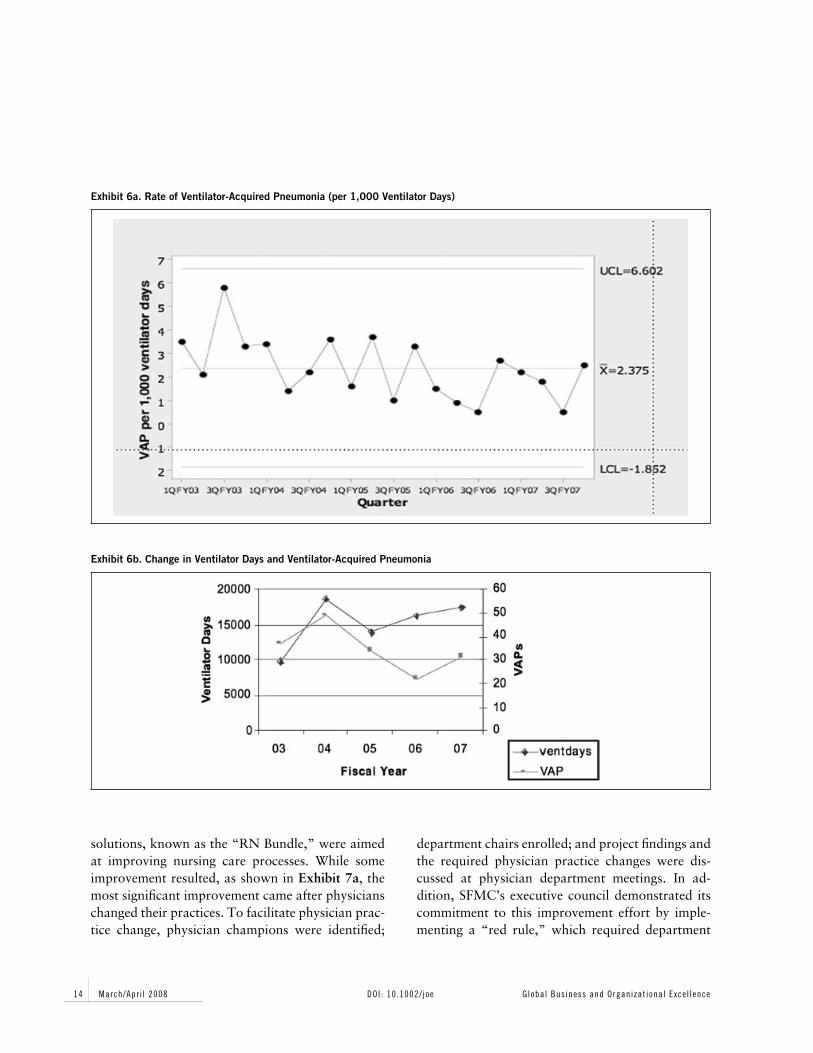
Exhibit 6a. Rate of Ventilator-Acquired Pneumonia (per 1,000 Ventilator Days)
Exhibit 6b. Change in Ventilator Days and Ventilator-Acquired Pneumonia
solutions, known as the “RN Bundle,” were aimedat improving nursing care processes. While someimprovement resulted, as shown in Exhibit 7a, themost significant improvement came after physicianschanged their practices. To facilitate physician prac-tice change, physician champions were identified;
department chairs enrolled; and project findings andthe required physician practice changes were dis-cussed at physician department meetings. In ad-dition, SFMC’s executive council demonstrated itscommitment to this improvement effort by imple-menting a “red rule,” which required department
14 March/Apr i l 2008 Global Business and Organizat ional Excel lenceDOI : 10.1002/ joe

Exhibit 7a. Rate of Blood Stream Infections (per 1,000 Central Line Days)
Exhibit 7b. Change in Central Line Days and Blood Stream Infections
chairs to counsel any physician who failed to im-plement required practice changes. As can be seenin Exhibit 7a, dramatic improvements followed the“red rule” implementation. BSI rates, measured asinfections per 1,000 central line days, were in ex-cess of 6 at the time of project kick-off in 2004,and have since declined by two-thirds, to an average
of 2 during 2007. Although the number of centralline days increased dramatically at about the timeof project kick-off and has remained high, as shownin Exhibit 7b, the number of blood stream infec-tions has trended steeply downward, another indi-cation of continuing improvement in response to thechanges associated with the Six Sigma project.
Global Business and Organizat ional Excel lence March/Apr i l 2008 15DOI : 10.1002/ joe
Medical Staff InvolvementFrom its inception, Six Sigma was received withskepticism at all levels of the medical staff—theorganized Medical Staff, the Executive LeadershipCommittee, and the Residents-in-training from theeducational side of our Regional Academic MedicalCenter—for three primary reasons:
� The perceived failure of previous quality initia-tives (TQM and others) at SFMC to change theway care was delivered in today’s complex med-ical environment.
� Their natural reluctance to see how pro-cess/system change applied to care delivery inthe complex patho-physiology world of acute andchronic illness could be compared with and ex-trapolated from the industrial world of improvingassembly line “widgets.”
� Most importantly, the inherent lack of train-ing in many medical education systems in theimportance of “system-based” and “team-based”
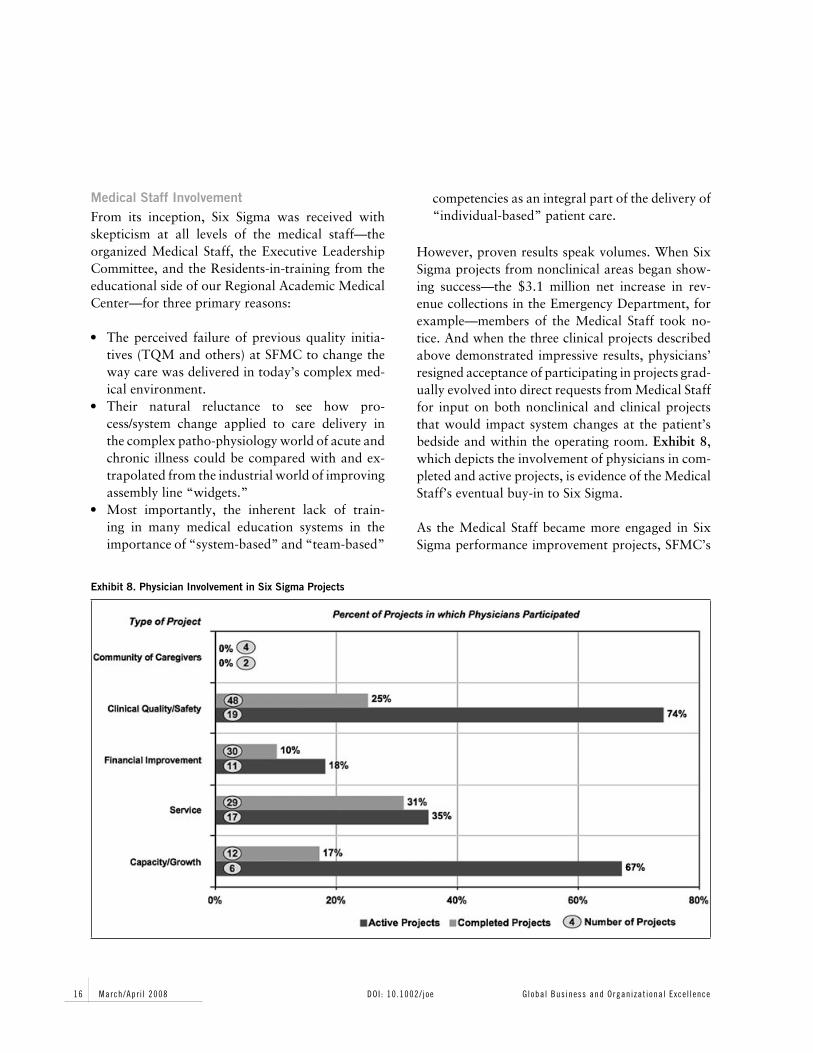
Exhibit 8. Physician Involvement in Six Sigma Projects
competencies as an integral part of the delivery of“individual-based” patient care.
However, proven results speak volumes. When SixSigma projects from nonclinical areas began show-ing success—the $3.1 million net increase in rev-enue collections in the Emergency Department, forexample—members of the Medical Staff took no-tice. And when the three clinical projects describedabove demonstrated impressive results, physicians’resigned acceptance of participating in projects grad-ually evolved into direct requests from Medical Stafffor input on both nonclinical and clinical projectsthat would impact system changes at the patient’sbedside and within the operating room. Exhibit 8,which depicts the involvement of physicians in com-pleted and active projects, is evidence of the MedicalStaff’s eventual buy-in to Six Sigma.
As the Medical Staff became more engaged in SixSigma performance improvement projects, SFMC’s
16 March/Apr i l 2008 Global Business and Organizat ional Excel lenceDOI : 10.1002/ joe

director of Medical and Academic Affairs (chiefmedical officer) challenged the leaders of the ten ap-proved Residency Programs to join the effort. Theleaders, in turn, initiated the first-of-its-kind “allphysician” Six Sigma project and encouraged seniorresidents from each of the ten programs to becometeam members.
The Patient Handoff Communication ProjectSafely “handing off” patient care from one careprovider to another at work shift changes requires anear-perfect process for sharing accurate and com-prehensive information regarding the patient’s sta-tus and plan of care. As such, each handoff entails acertain degree of risk. The Joint Commission hasidentified process improvement in this area as anational patient safety improvement opportunity.4
Spurred by the national patient safety initiatives andregulatory requirements from both the Joint Com-mission and the Accreditation Council for GraduateMedical Education (ACGME), the academic chairsand program directors at SFMC supported a SixSigma project for residents to improve the qualityand safety of patient handoffs.
One of the key factors the resident team had toclosely examine was the “80-hour workweek” re-quirement placed on residents during training. Thisschedule resulted in more structured resident workshifts and consequently increased the number of pa-tient handoffs occurring between residents.
One of the key factors the resident team had to closelyexamine was the “80-hour workweek” requirementplaced on residents during training.
The team of ten residents, facilitated by a Six SigmaBlack Belt, met once a week for a one-hour lunch.They outlined the scope of their work in a Six Sigmacharter, which would entail using the DMAIC pro-
cess to improve the resident handoffs by identifyingand eliminating the root cause of process problems.
Define and Measure Phases. As with all new Six Sigmaefforts, team members are naturally impatient andusually come into the Define phase of the projectwith a solution in mind. This team, being no dif-ferent, initially suggested a quick fix to the prob-lem: creation of a standard physician handoff re-port to be generated from SFMC’s electronic med-ical record (EMR) with the click of a button. Asmany of us know, EMR changes are rarely simpleand rarely offer comprehensive solutions for pro-cess problems. As a skilled facilitator, the Black Beltrecognized that the solution needed to be acknowl-edged, captured, and moved aside so that the teamcould work through the DMAIC process. To do this,the Black Belt documented the potential solution ofan EMR Handoff Report in the “idea box,” a toolused to capture and organize solution ideas sug-gested throughout all phases and especially in theImprove phase of a Six Sigma project.
With the quick fix safely captured for future ex-ploration, the Black Belt helped the team mapthe current resident handoff process and measureits process performance. As the residents learnedthat the handoff process included multiple “knowl-edge” steps that could not be “fixed” with an EMRhandoff report, they quickly dismissed their initial“quick-fix” solution.
Like many new teams, as the residents worked to-gether through the Define and Measure phases anduncovered previously unrecognized process prob-lems, they began to buy in to the Six Sigma problem-solving methodology. Shared learning is a great dy-namic for creating cohesive teamwork in all groups,but especially in a knowledge-worker team such asthis one.
Analyze Phase. In the Analyze phase of the project,the team used the data and process knowledge theyhad developed to identify problem statements, as
Global Business and Organizat ional Excel lence March/Apr i l 2008 17DOI : 10.1002/ joe

well as a fishbone (Ishikawa) diagram to conducta root cause analysis. As a result, they identifiedthe following key factors that negatively impact thehandoff process:
� Language differences posed a barrier when eitheror both residents do not have English as theirprimary language.
� There was a lack of handoff communication stan-dards, knowledge of relevant information to pro-vide at handoff, and handoff experience:
Eighty-seven percent of attending physicianswho provide direct supervision to residentsadmitted they did not provide formal hand-off communication training but would bewilling to do so.Eighty-six percent of residents reported theyhad personally experienced at least one inci-dent wherein they failed to receive relevantpatient care information from a cohort atthe point of handoff.Process mapping revealed the lack of a stan-dard handoff communication process withinor between resident programs.
� The existing handoff process involved a four-hour gap between resident shifts, which required“interim” coverage by a resident who may neverhave actually seen the patient or have compre-hensive knowledge of the patient’s care plan.
� The existing communication tool took too longto update patient information.
� Numerous environmental distractions werepresent (e.g., a high volume of simultaneoushandoffs; noise from pagers, phones, people, etc.;and presence of nonessential staff).
� Patient lists were inaccurate due to manual track-ing of a very high volume of patient transfers,admissions, and discharges.
Root cause analysis is always one of the mosteye-opening experiences of the Six Sigma DMAICmethod as it often reveals unexpected and surprisingcauses of process problems. This was never more ev-ident than in the Handoff Communications project,
in which several root causes of process failure un-covered by the team were in the fundamental careand resident education systems. Few medical schoolcurricula include communication and handoff pro-cess competencies as part of resident education andtraining.
Root cause analysis is always one of the most eye-opening experiences of the Six Sigma DMAIC methodas it often reveals unexpected and surprising causesof process problems.
Improve Phase. Based on the root cause analysis, theteam devised the following improvements:
� Eliminate the “interim” coverage requirementsby revising shift hours.
� Improve communication flow and eliminate pro-cess variation by implementing a standard, sys-tematic, team-based process for handoff prepara-tion and communication.
� Eliminate distractions by implementing a consis-tent resident handoff communication room.
� Create a process management system to monitorprocess performance and take corrective actionwhen necessary.
� Initiate a new project to create a resident handoffreport generated by the EMR.
Control Phase. Utilizing the Six Sigma methodologyof “sustaining the gain” achieved through processimprovement, the residency program directors arenow involved in creating evaluation systems, basedon “core competencies,” that will be implementedto evaluate residents’ handoff skills as a part of com-pletion of residency requirements.
As of the date of this writing, the first three so-lutions developed in the Improve phase have beensuccessfully implemented and are receiving highlypositive response. Even more challenging will be the
18 March/Apr i l 2008 Global Business and Organizat ional Excel lenceDOI : 10.1002/ joe

spinoff project to create an electronic tool to assistwith patient list management and resident handoffcommunications.
Next StepsSuccess is self-perpetuating. Can we actually achievethe Six Sigma level and deliver 99.997 percenterror-free performance in clinical processes? Whileonly time will tell, the SFMC community of care-givers is motivated and capable of applying theSix Sigma methods to keep pushing performanceto higher levels. Our physician leaders have gainedtremendous experience with change and processmanagement, and the resident physicians at SFMCare fully engaged in the Six Sigma project to improveone of their most critical processes.
While only time will tell, the SFMC community ofcaregivers is motivated and capable of applying theSix Sigma methods to keep pushing performance tohigher levels.
Over the next year, SFMC’s Six Sigma effort willfocus on the following goals:
� Augment performance improvement capabilitiesby developing advanced project managementskills and change leadership competencies
� Enhance accountability management by furtherdeveloping the medical center’s Dashboard andScorecards for tracking improvements in keymetrics
� Strengthen performance improvement partner-ship with physicians by working with them todevelop clinical scorecards and support evidence-based practice improvements within clinicaldepartments
� Work with the Graduate Medical Education lead-ership to develop Performance Improvement andChange Leadership education to be incorporatedin the Leadership curricula for senior residents
Working Effectively with Medical Staff and FacultyIn implementing the Six Sigma Management Sys-tem to improve processes in both the clinical andacademic arenas, we have learned success hinges ontwo key requirements:
� Medical Staff and physician academic facultyleaders must support the effort by professing be-lief in the system’s credibility; sponsoring change;and participating in ongoing measurement of theprocess changes implemented.
� To gain their support, the medical center’s lead-ership must demonstrate successful and sustain-able improvements in processes that matter tophysicians, such as basic care processes to pre-vent patient complications, timely access to di-agnostic imaging, and communication of criticaltest results.
Another important learning is that to successfullyengage physicians in performance improvement ef-forts, we must consistently demonstrate respect forthe extremely busy schedules of clinicians and aca-demicians. When we ask for physician participation,we must be consistent, effective, and efficient in ourmeetings, in our communication to team membersand project leadership, and especially in our projectmanagement, so as to ensure projects are completedin a timely manner to maintain commitment andmomentum for change.
To accomplish this, the Black Belt must be very or-ganized and prepared to facilitate the strong per-sonalities found within physician teams, as well ascreative to make effective participation easy. For ex-ample, the Black Belt must:
1. Accurately and precisely identify the physicianinput required.
2. Request the input in a clear and concise manner.3. Employ user-friendly feedback systems.4. Judiciously use the team meeting time to accom-
plish activities that require group process.
Global Business and Organizat ional Excel lence March/Apr i l 2008 19DOI : 10.1002/ joe

In addition, the Black Belt must be a very skilledcommunicator, negotiator, and facilitator to lead theteam through the problem-solving process, and tobuild consensus for solutions and the monitoringsystems that measure solution performance.
A third important lesson is the entire team must con-tinually insist on “evidence-based” data to supportthe quest for system-based, rather than individual-based, improvement. Bad processes will win out overgood people every time.
ClosingOne of the biggest lessons we have learned with thedeployment of the Six Sigma Management System atSFMC is that “the learning is in the doing.” Despitethe tendency in healthcare to want to study and planuntil we can ensure perfect implementation, trans-formational change comes from doing, learning, andthen doing some more.
Six Sigma is not for the faint of heart. It requires se-nior leadership vision, commitment, diligence, andperseverance, as well as the ability to celebratelearning—even if the learning comes through mak-ing mistakes—coupled with a team of committeddeployment leaders, including Master Black Belts,to make the vision reality.
As our method for strategy execution, Six Sigmahas produced transformational change in the waywe think about our work and the way we do ourwork at OSF Saint Francis Medical Center. It hasgiven us a consistent method for strategic perfor-mance improvement that has yielded tremendousand sustainable improvements in clinical processesand outcomes.
Notes1. Committee on Quality of Health Care in America & In-stitute of Medicine, To err is human: Building a safer healthsystem, ed. L. T. Kohn, J. M. Corrigan, & M. S. Donaldson(Washington, DC: National Academy Press, 2000).
2. DMAIC is the acronym for the improvement phases of aSix Sigma project: (D) define the opportunity for improve-ment; (M) measure current process performance relative tocustomer requirements; (A) analyze the process and the per-formance data for root causes that drive process defectsand waste; (I) improve the process through finding solu-tions that eliminate root causes; and (C) control the pro-cess through ongoing measurement and corrective action asneeded.
3. The Joint Commission, an independent, not-for-profit or-ganization, is the nation’s predominant standards-setting andaccrediting body in health care.
4. The Pennsylvania Health Care Cost Containment Coun-cil, PHC4 Research Briefs (5), July 2005. Downloaded fromthe Internet at http://www.phc4.org/reports/researchbriefs/071205/docs/researchbrief2005report hospacqinfections.pdf.
Jody Thompson, RN, is the director of Six Sigma and amaster black belt at OSF Saint Francis Medical Center inPeoria, Illinois, where she provides leadership for deploy-ment of Six Sigma across the OSF Healthcare System. Sheplayed a key role in planning and implementing the medicalcenter’s Six Sigma Management System, and can be reachedat [email protected]. Tim Miller, MD,is chief medical officer and director of Academic Affairs atOSF Saint Francis Medical Center. He played a key role inengaging physician participation in Six Sigma efforts and wasresponsible for incorporating Six Sigma into the GraduateMedical Education program. Amy Krantz, MSW, is the mas-ter black belt for Operative and Invasive Services and Am-bulatory Services at OSF Saint Francis Medical Center. TomThomas, MA, NCC, is a black belt at OSF Saint Francis Med-ical Center, where he led the first Six Sigma resident team inthe patient handoff communication project.
20 March/Apr i l 2008 Global Business and Organizat ional Excel lenceDOI : 10.1002/ joe