sle by dr sadaf b
TRANSCRIPT

By:
Dr. SADAF BUKHARI
PGR WMW

*NAME: mehwish
*AGE: 18yrs
*SEX: Female
*MARRITAL STATUS: single
*RESIDENT OF: sundar,lahore
*OCCUPATION: beautician
*D.O.A. : 13/06/14
*M.O.A. : OPD
*
*FEVER- 1yr
*JOINT PAIN- 1yr

*
My patient was in her USOH 1yr back when
she developed FEVER that was gradual in
onset,low-grade,intermittent associated
with anorexia and malaise but no
rigors/chills,no aggravating factor and
relieved by medication.

*
The pt is also complaining of JOINT PAIN since 1yr that
was gradual in onset,aching in character, symmetrical,
initially involving small joints of both hands and then
progressing to wrists, elbows and shoulders.The pain was
present throughout the day but aggravated on joint
movements and was relieved by medication.It was also
associated with redness and swelling of joints but no
numbness or tingling.The pain has worsened for the last
1M and now the patient is unable to perform her daily
chores and difficulty lifting any object,even difficulty
walking and climbing stairs.
There is no H/O morning stiffness..

** The patient is also having RASH over her face,dorsum of
both hands and extensor surfaces of arms that flares up
on sun exposure.
*There is also history of painless oral ulceration, hair
loss,bluish discolouration of her fingers on exposure to
cold and weight loss since 3months..
*There is no history of dyspnea,cough,sputum,hemoptysis
or any wheeze..
*No history of chest pain, palpitations, syncope,
orthopnea, PND or pedal edema..
*No history of abdominal pain, diarrhea, constipation,
vomitting,urinary frequency,urgency,burning micturation
or any genital ulcers..
*No history of difficulty standing from sitting posture..
*
*PAST HISTORY: history of hospital admission 5months back for
similar complaints..
*DRUG HISTORY: on and off intake of NSAIDs for fever and
joint pain..
*PERSONAL HISTORY:non diabetic,non hypertensive,non-
smoker..
*FAMILY HISTORY:insignificant
*MENSTRUAL HISTORY:Age of menarche 15yrs with regular
cycle of 4/28days..
*SOCIO-ECONOMIC: belongs to lower middle class..


1.SLE
2.DRUG INDUCED LUPUS ERYTHEMATOSUS
3.JRA
4.SYSTEMIC VASCULITIS
A young thin female sitting comfortably on bed,well
oriented in time,place and person with branula
over her right arm having following vitals:
*PULSE: 78/min
*B.P. : 120/80 mmHg
*TEMP: Afebrile
*R/R: 16/min

*
*Pallor +ve
*Jaundice –ive
*Splinter hemorrhages –ive
*Peri ungual erythema –ive
*Nail fold infarct –ive
*Joint swelling –ive
*Proximal IPJ deformity (2nd,3rd,4th digit left hand) +
*Reddish Plaques(atrophic and non blanchable)over
dorsum of hands and fingers

*Lymphadenopathy -ive
*Conjunctivitis:-ive
*Malar rash +
*Oral ulcers +
*JVP: not raised

*
MUSCULOSKELETAL SYSTEM:
*Reddish atrophic plaques over dorsum of both
hands and fingers,non blanchable
*no swelling or hypertrophic joint changes.
*Proximal IPJ deformity of 2nd,3rd and 4th digits with
painful flexion and extension of these joints.
*Rest of the joints have normal range of
movements,both flexion and extension.
*No proximal myopathy

*CNS:
GCS 15/15
HMF,CN:intact
SENSORY SYSTEM:normal
MOTOR:normal bulk,tone,power and reflexes,both upper limbs and lower limbs
FUNDOSCOPY:normal
RESP:
*No chest deformity with thoraco-abdominal breathing pattern
*Trachea central
*Chest expansion:4cm
*Normal vocal fremitus bilaterally
*Auscultation:NVB with no added sounds,normal vocal resonance,no pleural rub..
GIT:
*Soft,non-tender abdomen
*No visceromegaly
*B/S audible(2sets/min)
*CVS:
* INSPECTION:No visible pulsations,striae or scar mark
*APEX BEAT:in 5th ICS,midclavicular line.
*S1+S2:of normal intensity and character with no added sound
*No pericardial rub

*A Young Female Having 1yr History Of Fever And Joint
Pain,associated With Redness And Swelling Of
Joints.The Pain Has Worsened Over The Period Of
Time Leading To Proximal IPJ Deformity Of Her
Hands..
*There Is Also History Of Anorexia,malaise,weight
Loss,oral Ulceration And Hair Loss..
*Malar Rash,photosensitivity And Raynauds
Phenomenon +ive


*1.SLE
*2.JRA
*CBC:
*Hb 10.6 g/dl
*Hct 31.5%
*RBC 3.9x106
*MCV 80.8 fl
*MCH 27.2 pg/cell
*MCHC 33.7 g/dl
*WBC 3.8x103
*Neutros 50%
*Lymphos 45%
*PLT 17000
*ESR: 36mm/hr

LFTs:
*ALT 20.6
*AST 27.5
*ALP 126
*T.BIL 0.4
RFTs,S/E:
*UREA 61
*Cr 1.6
*Na 135
*K 3.6
*LDH: 360(225-450)
*RA Factor: -ive
*HBsAg,Anti HCV –ive
*URINE C/E:
*Sp Gr 1.015
*pH 6.0
*Pr-nil
*Glu-nil
*Pus cells 1—2
*Epi cells 3-5
*RBCs-nil
*24hrs Urinary Protein 280mg/24hrs(50-150)
*RA factor –ive
*ANA:-+ive
*ANTI DsDNA: 90 IU/ml
*USG Abd: normal

*
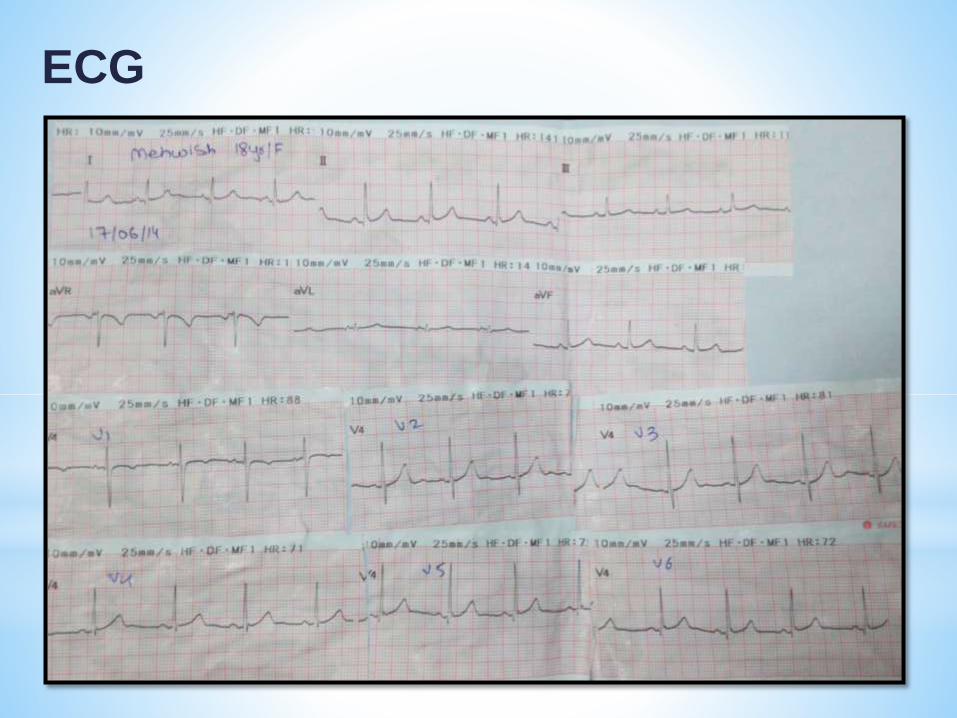
ECG


1.Cap RISEK 40mg 1 OD
2.Tab DELTACORTIL 5mg 2+0+2
3.Tab HCQ 200mg 1 BD
4.Tab QALSAN-D 1 BD
5.Tab NIMS 1 BD
*Joint X-rays:
To look for erosions, periarticular osteopenia
+ soft tissue swelling..
*CTBrain or Brain MRI ± angiography:
lupus white matter changes,vasculitis/ stroke
*CXR/CT chest:
ILD, pneumonitis, pulmonary emboli,
alveolar hemorrhage
*ECHO:
pericardial effusion, pulmonary hypertension
or Libman-Sacks endocarditis..

SLE
*Auto-immune disorder
*Multisystem microvascularinflammation
*Formation of autoantibodies
*Mostly occurs in women of childbearing age
*Chronic with relapsing and remitting course

PATHOPHYSIOLOGY
*Proposed mechanism for autoantibodies:
*Defect in apoptosis
*↑cell death → disturbance in immune tolerance
*Plasma + nuclear antigens displayed on cell surface
*Dysregulated lymphocytes target Ag (normally
intracellular)
*Immune complexes form in microvasculature →
complement activation + inflammation
*Ag-Ab complexes deposit in basement membranes of
skin and kidneys
*Constitutional – fatigue, fever, weight loss
*Skin – malar rash, photosensitive, discoid rash, alopecia, Raynaud phenomenon,peri-ungualerythema,nail fold infarct,splinter hemorrhages.
*Joint symptoms- with or without active synovitis
*Ocular manifestations- conjunctivitis,photophobia,blurring of vision
*Musculoskeletal – arthralgia, myalgia, arthritis

*Neuropsychiatric – headache, mood disorders, cognitive disorders, psychosis, seizures, TIA/ stroke, movement disorders, mononeuritis
*Pulmonary – chest pain, dyspnoea
*Gastrointestinal – Abdominal pain, jaundice
*Cardiac – heart failure(d/t myocarditis or HTN)/chest pain
*Haematological – multiple ‘cytopenias’
*Other – miscarriages, family history of autoimmune disease

American College of Rheumatology
4/11 criteria (sens 85%, specif 95%)
“SOAP BRAIN MD”
* Serositis – heart, lung, peritoneum
* Oral ulcers – painless esp palate
* Arthritis – non-erosive
* Photosensitivity

*Blood disorders :hemolytic anemia,leukopenia(<4000),lymphopenia(<1500),thrombocytopenia (<100,000)
*Renal involvement :proteinuria(>0.5g/day),>3+dipstick proteinuria /±casts
*ANA – titer > 1:160
*Immunologic phenomena – LE cells, anti-dsDNA Ab, anti-Sm Ab, antiphospholipid Ab, false +test for syphilis
*Neurological disorders – seizures/ psychosis
*Malar rash : cheeks + nasal bridge
*Discoid rash : rimmed with scaling, follicular plugging

*Depends on disease severity
*Fever, skin, musculoskeletal and serositis = milder disease
*CNS and renal involvement – aggressive Rx
*Emergencies: -
- severe CNS involvement - systemic vasculitis- profound thrombocytopenia
(TTP-like syndrome)- rapidly progressive nephritis - diffuse alveolar hemorrhage
NSAIDS: 400-800 mg PO q6-8hr; not to exceed 3.2 g/day
Hydroxychloroquine:it inhibits chemotaxis of eosinophils
and locomotion of neutrophils and impairs complement-dependent
antigen-antibody reactions.
* DOSAGE:400 mg (310 mg base) PO once or twice daily; maintenance: 200-
400 mg (155-310 mg base) PO daily
*With prolonged therapy, obtain CBCs periodically

Steroids(Prednisone)
5-60 mg/day PO in single daily dose or divided q6-12hr
Cyclophosphamide:used for immunosuppression in cases of serious SLE organ involvement, especially CNS involvement, vasculitis, and lupus nephritis
10 mg/kg IV every 2 weeks
Mycophenolate:
Induction: 1 g PO q12hr with a glucocorticoid or 2-3 g for 6 months
with glucocorticoids
Maintenance: 0.5-3 mg/day or 1 g PO q12hr or 1-2 g daily

Azathioprine: an immunosuppressant and a less toxic alternative to cyclophosphamide.
Dosage: 2 mg/kg/day PO with or without low-dose corticosteroids
Plasma exchange
IVIG:
used for immunosuppression in serious SLE flares. It neutralizes circulating myelin antibodies through anti-idiotypic antibodies

Belimumab(Benlysta):
It inhibits the biologic activity of B-lymphocyte stimulator
(BLyS); BLyS is a naturally occurring protein required for
survival and for development of B-lymphocyte cells into
mature plasma B cells that produce antibodies. In
autoimmune diseases, elevated BLyS levels are thought to
contribute to production of autoantibodies.
This agent is indicated for active, autoantibody-positive SLE
in patients in whom standard therapy(including
corticosteroids, antimalarials, immunosuppressives, and
nonsteroidal anti-inflammatory drugs)is failing.
LP – nonspecific ↑cells + protein, ↓ glucose
Skin biopsy
Renal Biopsy-prognosis and Rx


*A 15yr old female presented in OPD with presenting
complaints of high grade fever for 2months,associated with
painful joint movement of the small joints of hands,
wrist,elbow,ankle and knee..there is also history of limping
when she wakes up in morning.what is the most probable
diagnosis?
*1.SLE
*2.Scleroderma
*3.JRA
*4.Systemic vasculitis
*5.Septic Arthritis
Which of the following drug is most likely to cause drug
induced lupus erythematosus?
1.NSAIDs
2.Probenecid
3.Methotrexate
4.Chlorpromazine
5.Penicillin

Which of the following antibodies are most specific for
Drug induced lupus?
1.Anti-Ds DNA AB
2.Anti-smith AB
3.Anti-Ro AB
4.ANA
5.Anti histone AB
