sleep disturbances and weight gain: examining the evidence eileen chasens, dsn, rn assistant...
TRANSCRIPT

Sleep Disturbances and Weight Gain: Examining
the Evidence
Eileen Chasens, DSN, RNAssistant ProfessorNovember 19, 2009


1998
Obesity Trends* Among U.S. AdultsBRFSS, 1990, 1998, 2007
(*BMI 30, or about 30 lbs. overweight for 5’4” person)
2007
1990
No Data <10% 10%–14% 15%–19% 20%–24% 25%–29% ≥30%
•BRFSS, Behavioral Risk Factor Surveillance System http: //www.cdc.gov/brfss/

Obesity in Children
Enlarged Tonsil & Adenoids

A Good Night’s Sleepis when you…
A Bad Night’s Sleep is when you…

What is sleep?
State in which the individual is Unresponsive to the external environment Is accompanied by stereotypical behavior
Reversible Basic need

Mean Hours of Sleep in Adults
6.4
6.6
6.8
7
7.2
7.4
7.6
7.8
8
Hours
Week Days Week Ends
National Sleep Foundation, 2001 “Sleep in America” Poll of adults
7 to 8 hours recommended

Earth’s rotation on its axis is the fundamental orbital mechanism that underlies endogenous circadian rhythms.
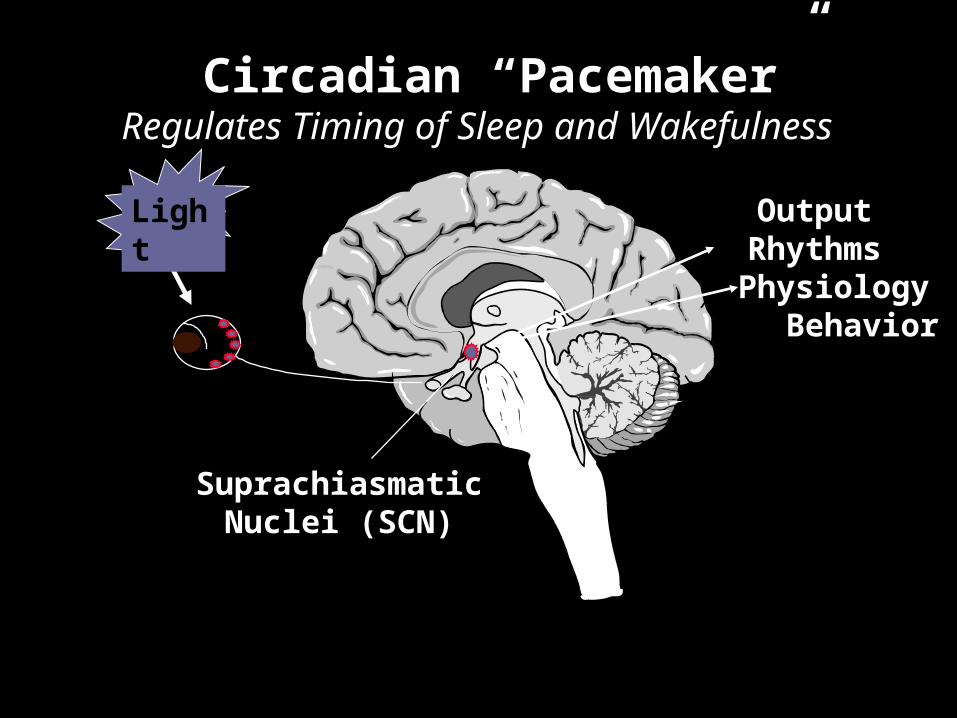
Circadian “Pacemaker”Regulates Timing of Sleep and Wakefulness
Suprachiasmatic Nuclei (SCN)
Light
Output Rhythms
Physiology Behavior

Sleep/Wake Restorative ProcessBalances Sleep and Wakefulness
Borbely, A. (1982). Neurobiology, 1; 195-204)
Awake Load

Reticular Activation System

Sleep-Promoting System

Normal Sleep Architecture

Changes in Sleep Architecture Associated with Aging

Normal Changes in Sleep With Age

EEG while Awake

EEG Sleep StagesAwake Alpha waves (if
eyes are closed)
Eyes moving together
High muscle tone

EEG Sleep Stages Stage 1 Theta waves
(3-7cycles second)
Rolling eye movements
High muscle tone

EEG Sleep StagesStage 2 Sleep spindles (12-
14 cycles/second) & K complexes
No distinctive eye movement
Lower muscle tone

EEG Sleep StagesStages 3 & 4 Delta (slow) waves
Stage 3: delta < half of epoch
Stage 4: delta >half of epoch
No distinguishing eye movement
Low muscle tone

EEG Sleep Stages
REM sleep Fast waves
Rapid eye movements (phasic REM)
Absence of muscle tone

Assessment of Sleep Direct observation Asking about sleep Diaries Use of a Sleep Questionnaire Actigraphy Sleep study

Assessment: Ask your subjects“how’s your sleep?”
Check if any of the following apply: Sleep less than 7 or more than 9 hours/night Snore loudly Stop breathing or gasp during sleep Excessive daytime sleepiness or doze off Difficulty 3 or more times a week with insomnia
symptoms Unpleasant feelings in legs when trying to sleep Interruptions to sleep

Self-Report Measures Sleep diary for bed time, wake time(s),
include daytime activities and meals/beverages

Instruments to Evaluate Sleep
Epworth Sleepiness Scale Johns MW (1991) Sleep, 14 (6),540-545)
Pittsburgh Sleep Quality Index Buysse DJ et al. (1989) Psychiatry Res, 28, 193-213
Functional Outcomes of Sleep Questionaire Weaver et al. (1997). Sleep:835-43
.

The Epworth Sleepiness Scale 1. Sitting and reading
2. Watching television
3. Sitting inactive in a public place, or example, a theater or meeting
4. As a passenger in a car for an hour without a break
5. Lying down to rest in the afternoon
6. Sitting and talking to someone
7. Sitting quietly after lunch (when you’ve had no alcohol)
8. In a car, while stopped in traffic
0 = would never doze1 = slight chance of dozing2 = moderate chance of dozing3 = high chance of dozing

Pittsburgh Sleep Quality IndexBuysse DJ et al. (1989) Psychiatry Res, 28, 193-213
19 items Generates 7 "component" scores Sum of scores from 7 components yields
one Global Score. Global PSQI >5 score distinguishes good
and poor sleepers http://www.sleep.pitt.edu

Functional Outcomes of Sleep Questionnaire
30-item questionnaire developed to evaluate areas sensitive to sleep disruption
5 Factor Design: activity level, vigilance, intimacy and sexual
relationships, general productivity, and social outcome areas
Short FOSQ 10-items

Body Movement Monitors
Wrist Actigraphy
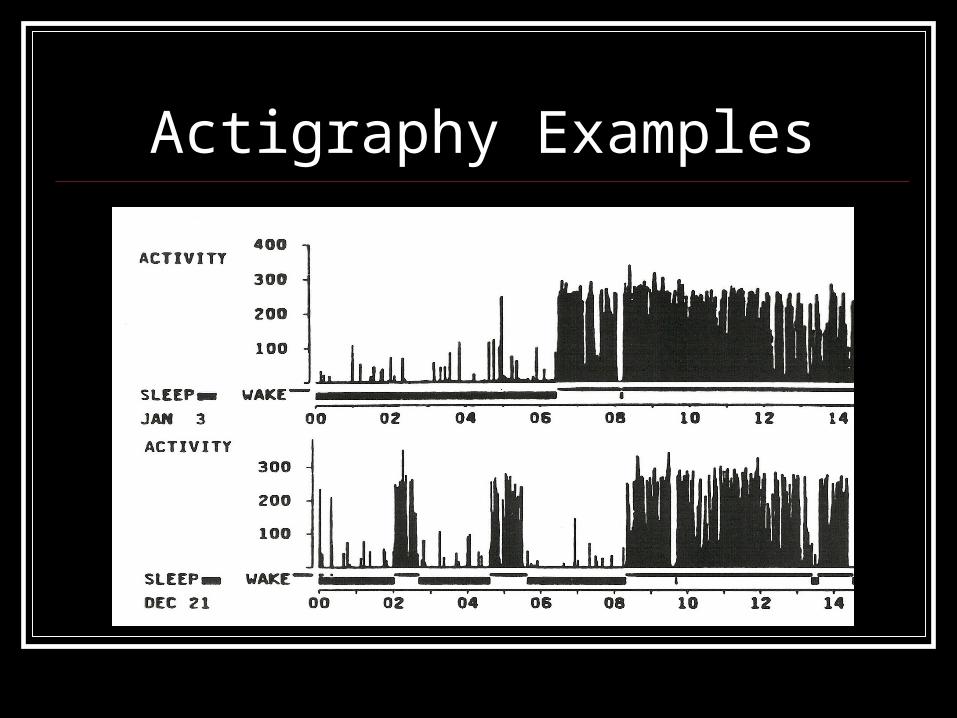
Actigraphy Examples


Physiological Measures
Polysomnography (PSG)
Multiple Sleep Latency Test (MSLT)

What are the links between sleep and obesity?... inadequate sleep duration because of lifestyle factors or insomnia??
Insomnia
Obesity
LifestyleFactorsSleep

INSUFFICENT SLEEP DURATION 2nd to Lifestyle Factors
Caffeine, alcohol and nicotine Exercise, too close to
bedtime Excessive naps Irregular sleep schedules Too many demands of daily
life!

INSOMNIA
What is it? Difficulty getting to
sleep Difficulty staying
asleep Awakening too early
from sleep Hyper-vigilant at
night/ Tired & fatigued during the day?
Insomnia Transient - less than 2 weeks Chronic - continuing difficulty with sleep for at
least 6 months Etiology:
Medical Psychiatric Pharmacologic Primary Sleep Disorder Genetic Tobacco / Alcohol

Adjusted BMI
(adj. for age, gender)
Taheri S, et al. PLoS Med. 2004
Short Sleep Duration & BMI In the Wisconsin Sleep Cohort
Average Nightly Sleep (Hrs.)
6 7 8 930
31
32
33
(N=1,024)

Abundant data indicates that we live in a sleep-restricted society
5.256.216.25
6.666.13
012345678
All Cauc.Women
Cauc.Men
BlackWomen
Black Men
Hrs
. S
lep
t /
Day
(in
cl.
Nap
s)
Lauderdale DS, et al. Am. J. Epi. 2006
Ancillary study of the CARDIA Study (n=668; age: 38-50)

Percentage of adults with < 6 hrs sleep per night
Guo, et al. (2002). American J. Clinical Nutrition: 76: 653-8.)
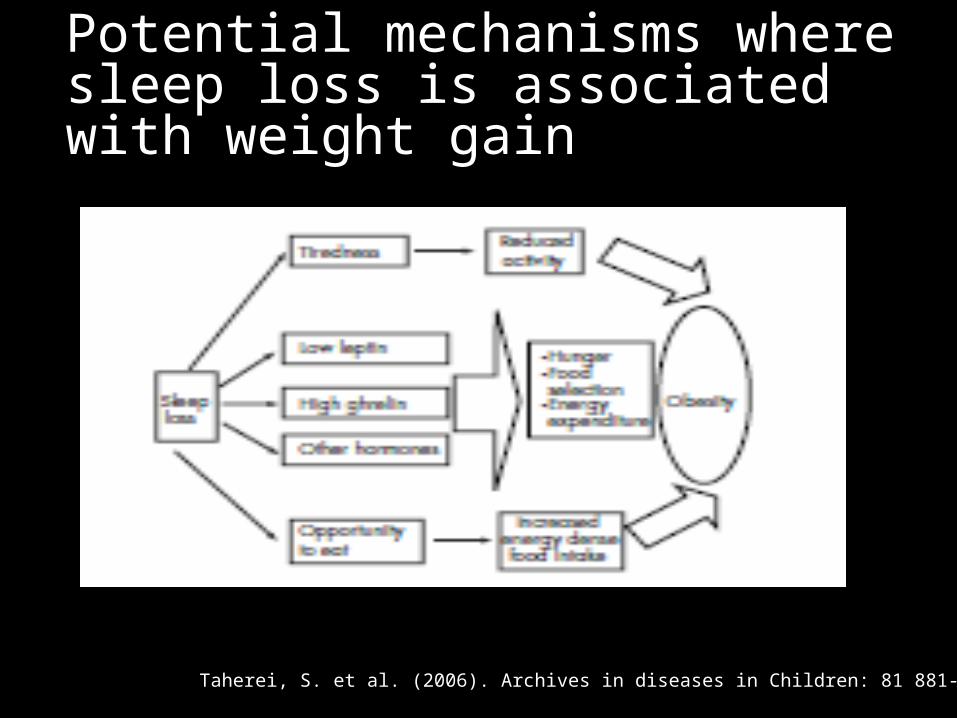
Potential mechanisms where sleep loss is associated with weight gain
Taherei, S. et al. (2006). Archives in diseases in Children: 81 881-884)

Spiegel K, et al. J. Clin. Endocr. Metab. 2004
Effects of Sleep Restriction (6 d) vs. Extension: Young, Healthy Men
Glucose(mg/dl)
Insulin(mlU/L)
HOMA(Io x Go/22.5)
(BMI: ~23)
3h 48’ Sleep 9h 03’ Sleep CHO Breakfast

Spiegel K, et. al. Ann. Int. Med. 2004
Sleep Duration: Leptin, Ghrelin, Hunger and Appetite in Healthy Young Men
After 2 days of 4 hrs.
sleep
After 2 days
of 10 hrs. sleep

What are the links between sleep and obesity?... sleep fragmentation 2o to Circadian Rhythm Disturbances
Sleep
Type 2 Diabetes
LifestyleFactors
Insomnia
Circadian Rhythm Disturbances

Shift Work Sleep Disorder Sleep disorder that affects people who
frequently rotate shifts or work at night The most common symptoms of SWSD
are insomnia and excessive sleepiness. Other symptoms of SWSD include:
Difficulty concentrating Headaches Lack of energy

What are the consequences of SWSD?
Increased accidents Increased work-related errors Increased sick leave Increased irritability, mood problems,
etc. WEIGHT GAIN!

Work-shift period and Weight Gain (Geliebter, A. (2000). Nutrition )
Survey about weight gain since starting shift work
85 Respondents, 36 on Days, 49 on Late shift

A longitudinal study on the effect of shift work on weight gain in male Japanese workers. Suwazono Y. (2008) Obesity: 18877-1893.

What are the links between sleep and type 2 diabetes?... sleep fragmentation 2o to Restless Leg Syndrome
Sleep
Type 2 Diabetes
LifestyleFactors
Insomnia
Circadian Rhythm Disturbances
Restless LegSyndrome

Restless Legs Syndrome & Sleep Fragmentation
Unpleasant, creeping feeling in legs
Irresistible urge to move
Associated with other medical conditions
Periodic Leg Movements during sleep require evaluation

Odds Ratio (OR, 95% CI) of RLS according to BMI from Nurses Health Study & Health Professionals Follow-Up Study
Gao, X. et al. (2009) Neurology, 72: 1255-61.

What are the links between sleep and obesity?... Obstructive Sleep Apnea
Sleep
Type 2 Diabetes
LifestyleFactors
Insomnia
Circadian Rhythm Disturbances
Restless LegSyndrome
OSA

Obstructive Sleep Apnea Repetitive episodes of complete (apnea) or partial (hypopnea) upper airway obstruction during sleep
This interruption in breathing can take place just a few times or up to hundreds of times over the course of a night
Airflow cessations or reductions produce: Arousals Fragmented sleep Reductions in blood oxygen saturation Fluctuations in blood pressure and heart rate

Obstructive Sleep Apnea
Anatomy of a blocked airwayPossible obstruction sites
The upper airway excess tissue, large tonsils, a large tongue, and usually includes the airway muscles relaxing and collapsing when asleep
The nasal passagesStructure of the jaw and airway can be a factor in sleep apnea

Risk Factors for OSA
Risk Factors Male gender Increased
age Obesity Recessed
mandible Comorbid
Medical Conditions

Outcomes Associated with Untreated OSA
DIABETES Increased Mortality
Hypertension Stroke Heart Attack Atrial fibrillation Depression Functional
Impairments Performance
Impairments

Intermittent Hypoxia Induces Insulin Resistance in Obese Mice
Adapted from: Polotsky VY, et al. J. Physiol. 2003
HOMA
(mean ± SEM)
65.9
204.7
58.944.9
0
50
100
150
200
250
300
Intermittent Hypoxia Intermittent Air
Day 0
Day 5

Adapted from: Gottlieb DJ, et al. Arch. Int. Med. 2005
Odds Ratio for Diabetes Mellitus & Impaired Glucose Tolerance By Self-
Report Usual Sleep Time in Older Population {SHHS} (age: 53-93 yrs.)
Adj. for: age, gender, race/ethnicity, AHI, waist circ., field site
Adj. Odds Ratio(referent to 7- 8 hrs. sleep)

<5 6 7 8 >8
Age-adj. relative risk
2.6(1.28–5.27)
1.93 (1.06–3.5)
1 1.40(0.78-2.53)
3.63 (1.79–7.38)
Multivariate model *
1.95 (0.95–4.01)
1.95 (1.06–3.58)
1 1.41(0.78-2.55)
3.12 (1.53–6.37)
Sleep Duration & Relative Risk for Incident Diabetes: Massachusetts Male
Aging Cohort
Yaggi HK, et al. Diab. Care 2006
Self-Report Hours of Sleep/Day
*Adjusted for 10-year age-group, hypertension, current smoking, self-rated health status, waist circumference, education (all covariates measured at baseline).

5 6 7 8 9+
n 122 576 731 422 118
Age-adjusted relative risk
1.57 (1.28–1.92)
1.27 (1.12–1.44)
0.98 (0.87–1.11)
1 1.47 (1.19–1.80)
Multivar. model incl BMI *
1.18 (0.96–1.44)
1.10 (0.97–1.25)
1.02 (0.91–1.16)
1 1.29 (1.05–1.59)
Sleep Duration & Relative Risk for Incident DM: Nurse’s Health Study
Ayas NT, et al. Diab. Care 2002
Hours of sleep per day
*Adj.: shift work, hypercholesterolemia, HTN, smoking, snoring, exercise, alcohol, depression, postmenopausal hormone, family hx diabetes

OSA Associated with DM in Hypertensive Men
OSA Associated with DM in Hypertensive Men
N=2,668; Obese = BMI >27; OSA = AHI >20 N=2,668; Obese = BMI >27; OSA = AHI >20 Elmasry A, et al., J. Int. Med 2001Elmasry A, et al., J. Int. Med 2001Elmasry A, et al., J. Int. Med 2001Elmasry A, et al., J. Int. Med 2001
PrevalenceOf
Diabetes
PrevalenceOf
DiabetesNon-OSA
Non-Obese
Non-OSAObese
OSANon-Obese
OSAObese

What is the evidence that sleep disturbances are associated with type 2 diabetes? Sleep AHEAD study recruited from Look AHEAD Exclusion criteria for Sleep AHEAD were previous
treatment for OSA. Efforts were made to enroll individuals
with undiagnosed OSA using a symptom questionnaire Because almost all of the first 80 participants had
OSA upon PSG, the symptom
screen was dropped

Data from Sleep AHEAD StudyPresence and Severity of OSA in Patients with
T2DM
None14%
Mild32%
Moderate31%
Severe23%
None
Mild
Moderate
Severe
Foster et al. (2009). Diabetes Care, 1017-1-19.
(N=305)
Conclusions from Sleep AHEAD Exceedingly high prevalence of undiagnosed OSA
among obese patients with type 2 diabetes Unequivocally high prevalence of moderate-to-
severe OSA Results do not appear to be secondary to a
selection bias Possibility that some of the morbidity and
mortality associated with type 2 diabetes may be attributable to undiagnosed OSA?!

Obstructive Sleep ApneaPrevalence
At least 15–18 million with OSA1 in 5 adults has at least mild OSA1 in 15 adults has at least moderate OSA80–90% OSA cases undiagnosedDoctors usually can't detect the condition during routine office visitsNo blood tests for the condition


Treatment OptionsMild OSA Losing weight
Positional therapy Avoidance of central nervous system (CNS) depressants
Oral mouth devices (keep the airway open) Can bring the jaw forward, elevate the soft palate, and retain the tongue
(from falling back in the airway and blocking breathing) Possibly requires continuous positive airway pressure (CPAP)
Moderate to severe OSA First-line treatment for the underlying obstruction is typically
continuous positive airway pressure (CPAP) Surgery of the airway may be required in certain cases

Obstructive Sleep Apnea Overview
69
Normal Airway
CPAP Airway

Treatment of Sleep Apnea CPAP (Continuous
Positive Airway Pressure) Need for increased
adherence to all night/every night
Need to bring to hospital if admitted, especially if surgical patient

CPAP only works if it is worn all night, every night. OSA: Residual Sleepiness and Functional Impairment With CPAP with suboptimal use*
*Average CPAP use over 3 months was 4.7 hours per night, which is consistent with other studies of CPAP adherence. Data presented as mean.
29. Weaver TE. Sleep. 2007;30:711-719.
After Three Months of CPAP Treatment*
34%
65%
Pati
en
ts W
ith
ES
(%
)
43%
0
10
20
30
40
50
60
70
Objective Sleepiness
(MSLT <7.5)n=85
Subjective Sleepiness (ESS >10)
n=106
Functional Impairment(FOSQ <17.9)
n=120P
ati
en
ts W
ith
Im
pair
men
t
(%)
0
10
20
30
40
50
60
70

Hours of CPAP use and Outcomes on FOSQ, ESS, and MSLT
Weaver et al. (2007) Sleep. 30: 711-719.

Babu AR, et al. Arch. Intern. Med. 2005Babu AR, et al. Arch. Intern. Med. 2005
p = 0.02
p = 0.06
CPAP Treatment & Glucose Control
(N=25/ 17 with A1c>7%)
83 +/- 50 days

Babu AR, et al. Arch. Intern. Med. 2005
Patients Using PAP Avg. >4 Hrs./Day
Patients Using PAP Avg. <4 Hrs./Day
Adherence to CPAP Determines its Efficacy

CPAP Therapy Improves Insulin SensitivityCPAP Therapy Improves Insulin Sensitivity
Harsch IA, et al. AJRCCM 2004
Harsch IA, et al. AJRCCM 2004
0
24
68
1012
1416
18
BMI <30 BMI >30
Ins
uli
n S
en
sit
ivit
y I
nd
ex
BL
2 Days CPAP
3 Mon. CPAPp = 0.001p = 0.001
p = 0.001p = 0.001
p = 0.003p = 0.003
(n = 13) (n = 18)
Not a RCT
(No BMI)

Vigilance and Sleep Restriction
Van Dongen H., et al:.
Sleep 2003;26:117-126.)

Cognitive abilities and mood are affected by sleep deprivation.
Memory is impaired when sleep is not consolidated Paying attention to and completing tasks is
compromised Mood is impaired Over ½ of adults report that sleepiness makes it hard
to concentrate, solve problems and make decisions at work
Diabetes and Depression Research linking depression and diabetes
is compelling Bi-directional association between sleep
disorders and depression Results in people having a difficult time
following a diabetes treatment plan, which in turn places them at risk for otherwise avoidable complications of diabetes

Symptom of depression, of a sleep disorder, or of both?

Incidence of Clinical Depression with Insomnia
Chang, P., et al. (1997). Am J. Epidemiol; 146: 105-114)

The Experience Of Being Sleepy While Managing Type 2 Diabetes. Sleepiness described as a burden that one must
force oneself to combat Difficulty in going beyond the minimum required to
manage one’s life A lack of structure exacerbates difficulties Expressed feeling lazy, crazy and misunderstood
because of chronic sleepinessChasens ER, Olshansky E.
JAPNA (2006);12(5):272-8.

Summary
Sleep is a physiological necessity.
Sleep disruption is due to either Insufficient sleep and lifestyle issues, or Fragmented sleep and health problems Primary sleep disorders such as OSA, RLS, or
insomnia
Sleep loss can have serious physical, personal and social consequences.

Is sleep important for improving health outcomes in persons at risk for weight gain or who are overweight or obese, you be the judge!