sleeve en y does changing the name change the perception? mitchell roslin, md facs chief of...
TRANSCRIPT
Sleeve En YDoes Changing the Name Change the Perception?
Mitchell Roslin, MD FACS
Chief of Bariatric Surgery
Lenox Hill Hospital
Northern Westchester Hospital Center
Disclosures
• Consultant J&J, Covidien, CR Bard• Research Grant Covidien• Patent License J&J, CR Bard, Allergan• SAB ValenTx, Scientific Intake• Founder VentralFix
• Gastric bypass has been most popular stapling procedure
• Best balance between outcome and complications?
• Preferable for sweet eaters because of dumping?• Dumping is an important component for weight
loss surgery as it deters carbohydrate intake?• Tremendous amount of long term data?
“A person with a new idea is a crank until the idea succeeds.”
Mark Twain • Described RYGB• Abandoned anemia, bone
loss, micronutrient deficiencies
• 1971 VBG• Lesser curvature• 2005 International
Registry• RYGB 67 vs 59 %EBL• VBG 0 mortality vs .5%
Edward E Mason MD, PHD
Harvey SUGERman• Compared VBG to
RYGB in sweet eaters• Big difference in
outcome 37% EBL VBG• What is a sweet eater?• 69% vs 67% wt loss in
sweet eaters vs non in rygb
• Dumping caused sweet aversion?
Ann Surg 1987

Ten and more years after vertical banded gastroplasty as primary operation for
morbid obesity
• 71 patients• BMI 49 – 39• 26% 50% ebl• High amount of
emesis• High re operation rate
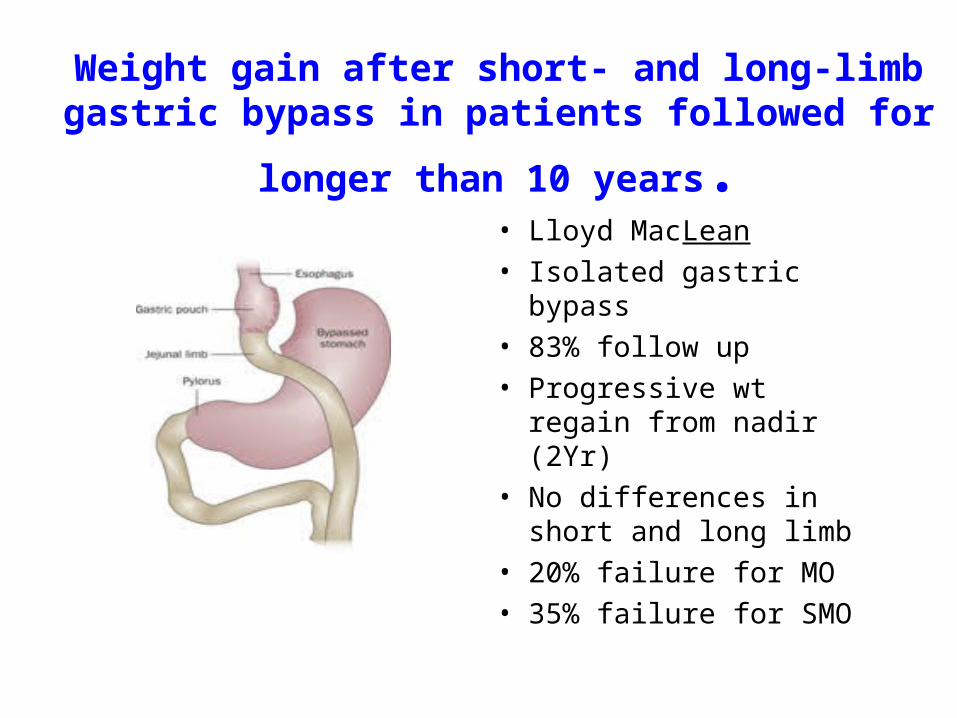
Weight gain after short- and long-limb gastric bypass in
patients followed for longer than 10 years.• Lloyd MacLean
• Isolated gastric bypass
• 83% follow up
• Progressive wt regain from nadir (2Yr)
• No differences in short and long limb
• 20% failure for MO
• 35% failure for SMO

Dumping?
• Literature contains numerous articles about hyperinsulinemic hypoglycemia
• None showing relationship between dumping and weight loss
• Mallory et al: No relationship between wt loss and dumping

OBESITY IS A CHRONIC DISEASE
• 70% of excess weight loss after one year• Much higher rate of recidivism than noted

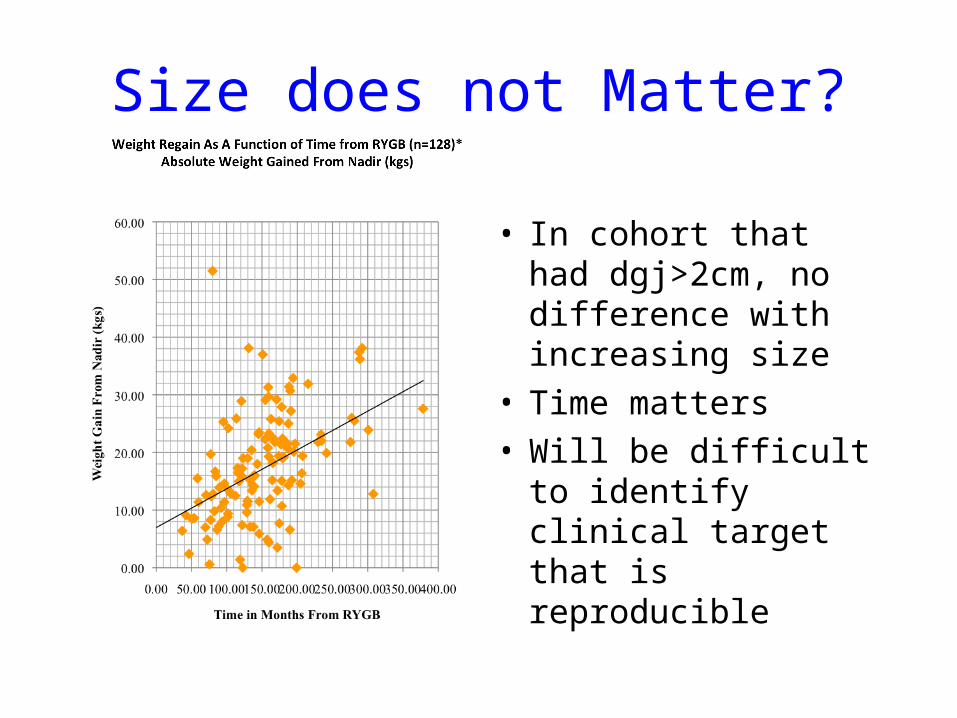
Size does not Matter?
• In cohort that had dgj>2cm, no difference with increasing size
• Time matters• Will be difficult to
identify clinical target that is reproducible

Physiologic Cause
• Lesser curvature• Restrictive anastomosis• No valve• Rapid emptying• Recidivism maybe based
on anatomy, not return of old habits
• Low glycemic index diet• Many eat refined carbs
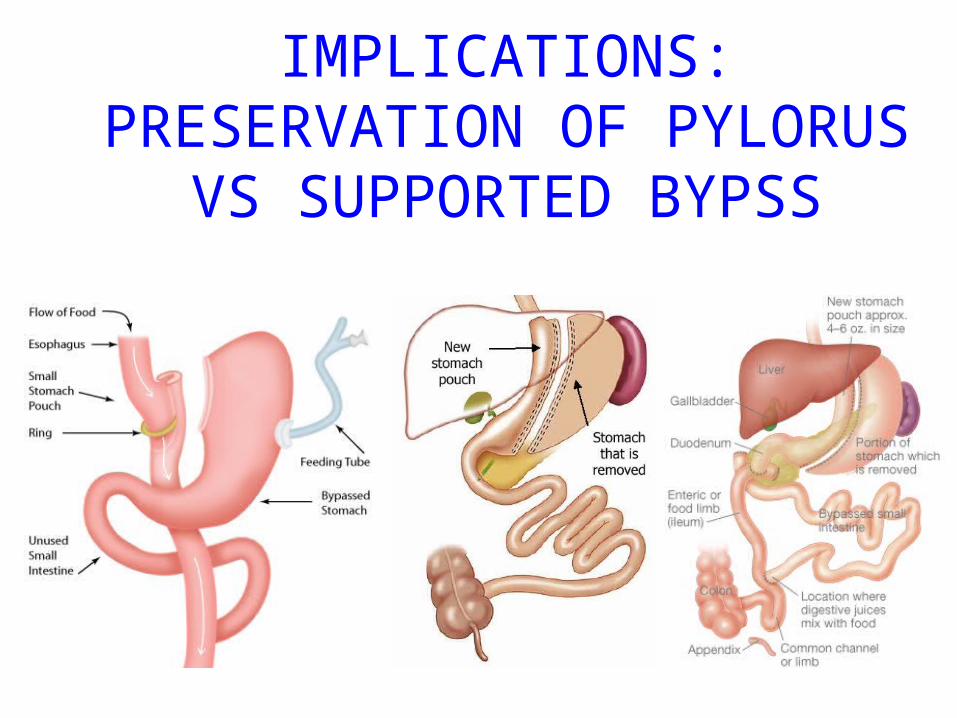
IMPLICATIONS:PRESERVATION OF PYLORUS
VS SUPPORTED BYPSS
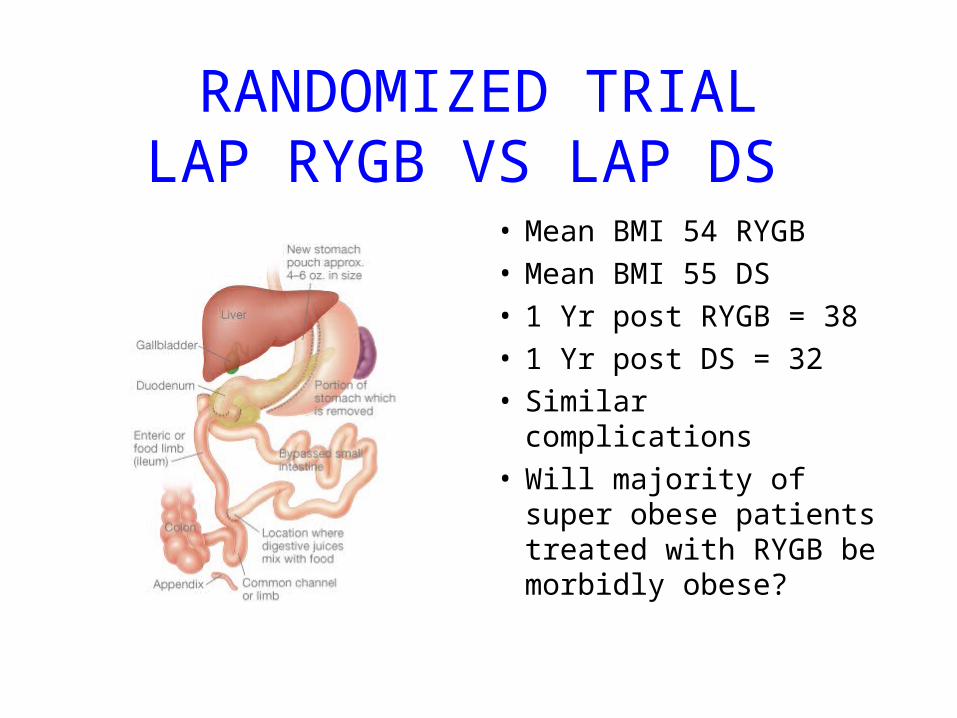
RANDOMIZED TRIALLAP RYGB VS LAP DS
• Mean BMI 54 RYGB• Mean BMI 55 DS• 1 Yr post RYGB = 38• 1 Yr post DS = 32• Similar complications• Will majority of super
obese patients treated with RYGB be morbidly obese?

The Duodenal Switch Operation for the Treatment of Morbid Obesity: A
10 Year Experience• 701 patients BMI 52• 22% BMI >60 58% BMI >50• 75% >50% excess wt at five
years• 67% EBL maintained• 40 patients with revision for
increased limb length• Similar data Hess and
Marceau

Pyloric Preservation?
• Bypass with rapid emptying causing inter meal hunger
• Instead of artificial fixed valve use biologic smart valve
• Duodenal Switch has most weight loss
• Sleeve preserves options
Introducing the Sleeve En Y
• Effectiveness of sleeve shows the value of long narrow pouch with pylorus intact
• Combination of narrow pouch and pylorus limit intake and diarrhea
• Intestinal bypass plays metabolic role
• Can lengthen common channel to avoid oily stools and frequent bowel movements

Responder Analysis• BMI > 50 Nadir response > 1 year
• 50% EWL, BMI < 40, BMI < 35, BMI <30
• 13/120 Bands less than 40
• 270 of 346 RYGB less than 40
• 10 of 30 VSG
• 22 of 23 lap DS (majority have not reached nadir
• Lowest variability in response
• Does treatment of super morbid obesity require intestinal bypass?
