slide deck. - neocate · slide deck. any views, opinions or recommendations expressed in the slides...
TRANSCRIPT


Nutricia Paediatric Food Allergy Expert Meeting
The speaker had sole editorial control over the content in this
slide deck.
Any views, opinions or recommendations expressed in the
slides are solely those of the speaker and do not necessarily
represent those of Nutricia.

Baked milk challenge: for whom is it appropriate?
Paediatric Food Allergy Expert Meeting
Royal College of Physicians, London UK
December 6, 2016
Anna Nowak-Węgrzyn, MD PhD Associate Professor of Pediatrics
Icahn School of Medicine at Mount Sinai
New York, NY, USA

“I am extraordinarily patient, provided I get my own way in the end.”
1) Albert Einstein
2) Donald Trump
3) Shakespear
4) Margaret Thatcher
21
53
4
39
1 2 3 4

Effect of cooking & digestion on food
proteins
1
2
Processing
M I
I M
K
L L I
M
K M
I K L
L
K
Majority of children outgrow milk or egg within first 6 years of life
- children who “outgrow” milk / egg allergy have IgE directed
primarily at conformational epitopes
High temperature affects
1) All proteins in milk equally
2) Caseins more than whey proteins
3) Whey protein more than caseins
4) No significant effect on milk proteins
42 43
35
3
1 2 3 4

α-lactalbumin
β-lactoglobulin
Caseins
Lactoferrin
BSA
Immunoglobulins
Boiling
Time (min)0 5 10 15 20 30 45 60 75 90
Amount
(µg)10 10 10 10 10 10 10 10 10 10
Boiling
Time (min)0 5 10 15 20 30 45 60 75 90
Amount
(µg)10 10 10 10 10 10 10 10 10 10
Standard
+ DTT / heating
Modified
- DTT / heating
0 5 10 15 20 30 45 60 75 90
10 10 10 10 10 10 10 10 10 10
0 5 10 15 20 30 45 60 75 90
10 10 10 10 10 10 10 10 10 10
α-lactalbumin
β-lactoglobulin
caseins
Heated Milk-Reactive Heated Milk-Tolerant
Boiling time
(min)
0 5 10 15 20 25 30 60 90Boiling time
(min)
0 5 10 15 20 25 30 60 90
Negative Control
0 5 10 15 20 25 30 60 900 5 10 15 20 25 30 60 90 0 5 10 15 20 25 30 60 900 5 10 15 20 25 30 60 90
SDS-PAGE and immunoblots with boiled milk
Bloom K et al, PAI 2014
Hypothesis: Children who “outgrow” milk/egg allergy will tolerate baked milk/egg products
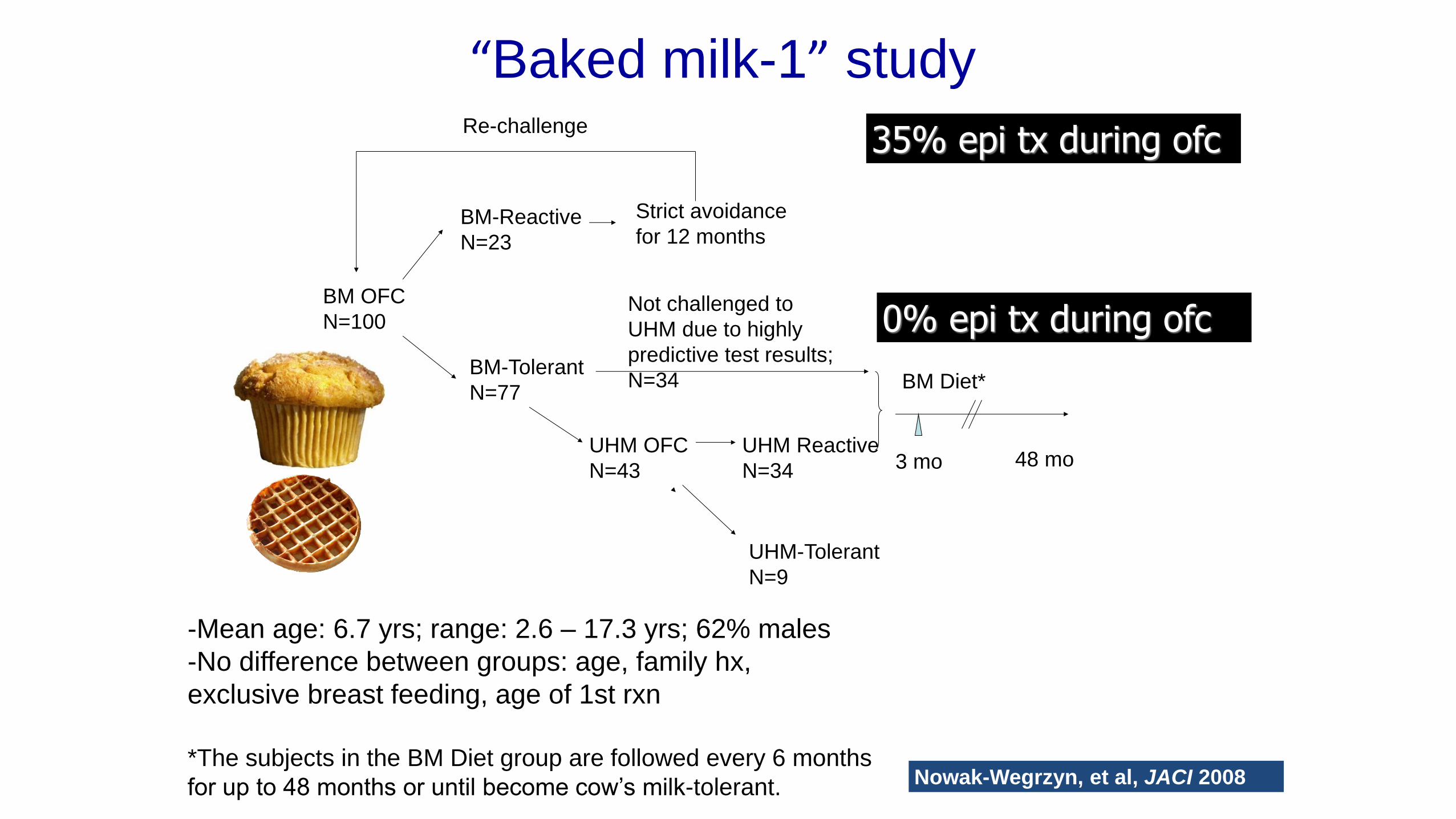
BM OFC
N=100
BM-Reactive
N=23
UHM-Tolerant
N=9
UHM OFC
N=43
Not challenged to
UHM due to highly
predictive test results;
N=34 BM-Tolerant
N=77
UHM Reactive
N=34
Strict avoidance
for 12 months
Re-challenge
BM Diet*
3 mo 48 mo
“Baked milk-1” study
-Mean age: 6.7 yrs; range: 2.6 – 17.3 yrs; 62% males
-No difference between groups: age, family hx,
exclusive breast feeding, age of 1st rxn
*The subjects in the BM Diet group are followed every 6 months
for up to 48 months or until become cow’s milk-tolerant. Nowak-Wegrzyn, et al, JACI 2008
35% epi tx during ofc
0% epi tx during ofc

Changes in milk-specific PST, IgE &
IgG4 in baked milk –tolerant subjects
Median Skin Prick Test (wheal diameter, mm)
in BM-tolerant Group over Time
0
5
10
15
20
0 months 3 months
P = <0.001
Median Casein-Specific IgG4 (ug/L)
in BM-tolerant Group over Time
0
3
6
9
12
15
0 months 3 months
P = 0.001
Median Milk-Specific IgE (kUA/L)
in BM-tolerant Group over Time
0
5
10
15
20
0 months 3 months
P = 0.183
Median B Lactoglobulin-Specific IgG4 (ug/L)
in Baked Milk Group over Time
0
1
2
3
4
0 months 3 months
P = 0.592
Milk PST ↓; casein-IgG4 ↑
Nowak-Wegrzyn, et al, JACI 2008

Active ITT group, n=88
Failed initial BM challenge, n=23
Passed initial BM challenge, n=65
Passed subsequent BM challenge, n=5
Active PP group, n=70
Comparison group, n=60
59% developed UHM tolerance
22% developed UHM tolerance Natural history
60% developed UHM tolerance
9% developed UHM tolerance
Kim J et al. JACI 2011
Median age 6.6 yrs
[2.1-17.3]
Follow-up median 37 mo (range 8-75 mo)
ITT - ACTIVE VS. COMPARISON SURVIVAL ANALYSIS
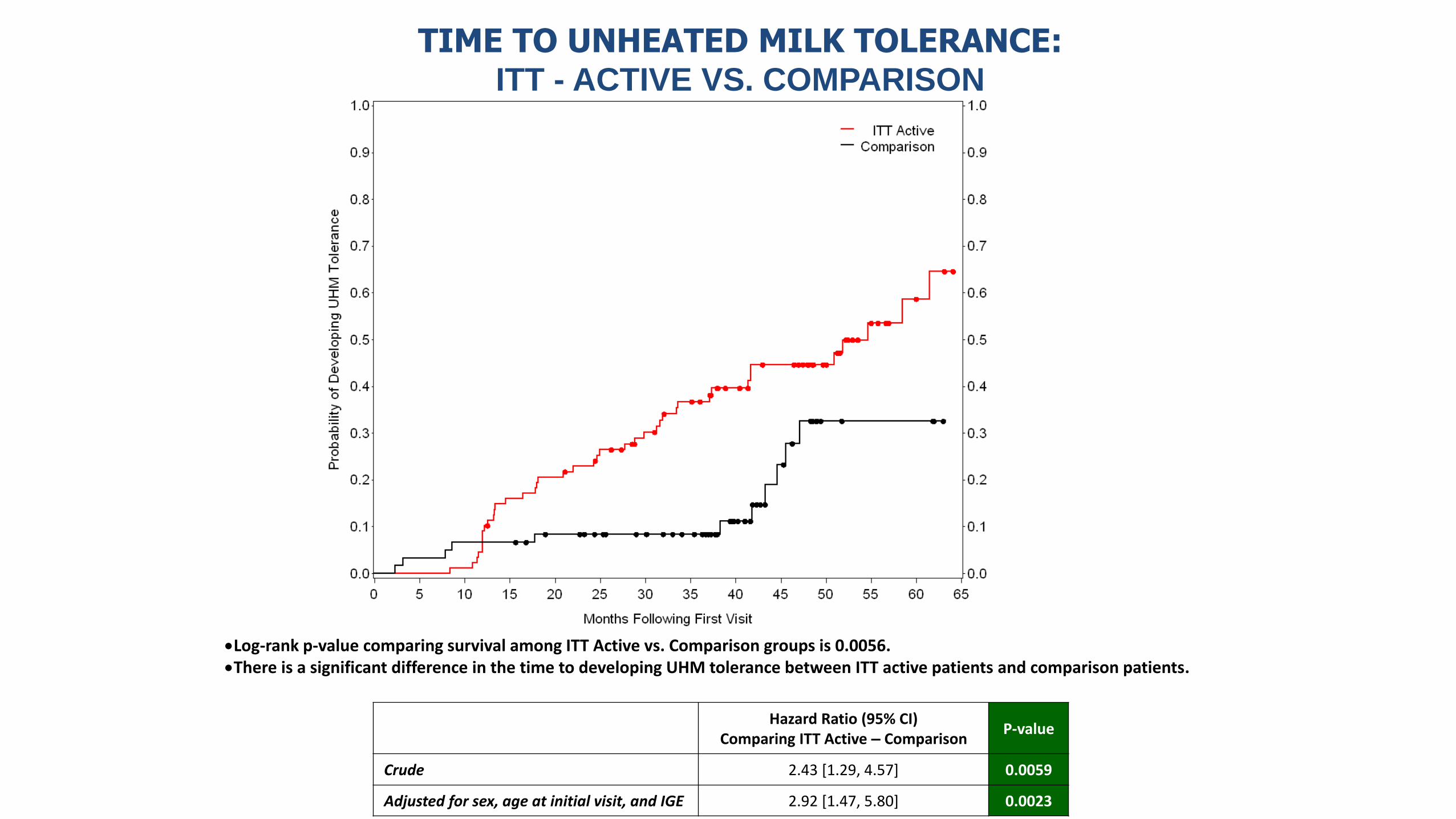
Log-rank p-value comparing survival among ITT Active vs. Comparison groups is 0.0056. There is a significant difference in the time to developing UHM tolerance between ITT active patients and comparison patients.
Hazard Ratio (95% CI)
Comparing ITT Active – Comparison P-value
Crude 2.43 [1.29, 4.57] 0.0059
Adjusted for sex, age at initial visit, and IGE 2.92 [1.47, 5.80] 0.0023
Patients in the ITT active group are 2.92 times more likely to develop UHM tolerance than patients in the Comparison group. This increased risk is statistically significant; HR=2.92 [1.47, 5.80] p=0.0023.
TIME TO UNHEATED MILK TOLERANCE: ITT - ACTIVE VS. COMPARISON

TIME TO UNHEATED MILK TOLERANCE:
ITT – INITIAL BM TOLERANCE VS. INITIAL BM REACTION
Log-rank p-value comparing survival among ITT initial HM tolerance vs. Initial HM reaction groups is <0.0001. There is a significant difference in the time to developing UHM tolerance between patients who were initially HM-tolerant and HM-reactive.
Hazard Ratio (95% CI) Comparing ITT HM Tolerant – HM
Reactive
P-value
Crude 10.95 [2.63, 45.53] 0.0010
Adjusted for sex, age at initial visit, and IGE 7.62 [1.75, 33.14] 0.0068

Reactions to baked milk:
1) Are always mild
2) Are never treated with epinephrine
3) May be severe
4) Usually occur within more than 4 hours of eating
8 4
104
10
1 2 3 4

Subjects
Total (n=88)
Initially baked-
milk tolerant
(n=65)
Initially baked-
milk reactive
(n=23)
P value
# Challenges
performed
172 154 (90%) 18 (10%) <0.001
# Failed (%) 58 (34%) 47 (31%) 11 (61%) 0.009
# Treated with
epinephrine
(%)
8 (4.7%) 5 (3.2%) 3 (17%) 0.04
Severity of reactions
during OFC to baked milk
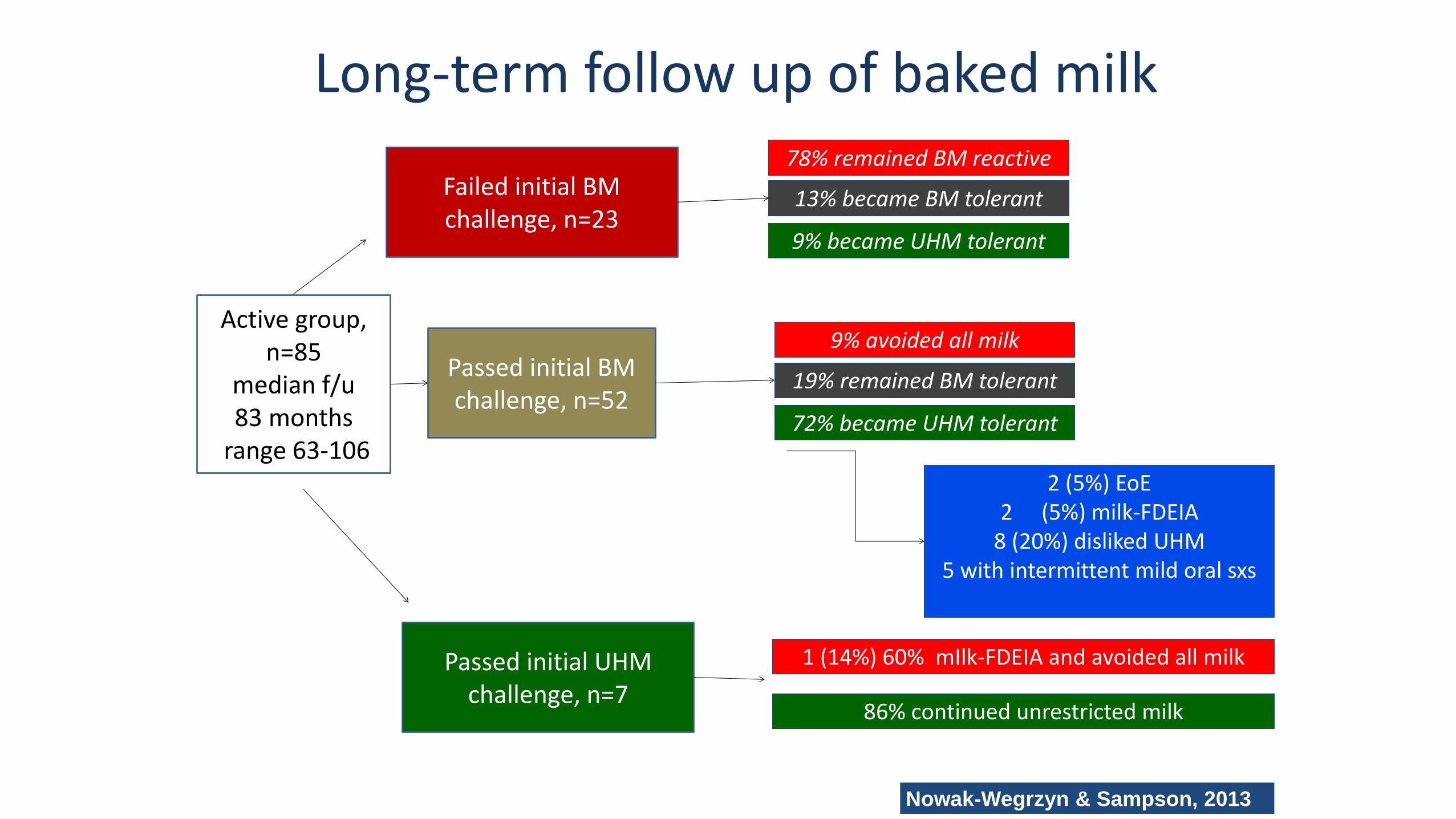
Long-term follow up of baked milk
Active group,
n=85 median f/u 83 months
range 63-106
Failed initial BM challenge, n=23
Passed initial BM challenge, n=52
1 (14%) 60% mIlk-FDEIA and avoided all milk
Nowak-Wegrzyn & Sampson, 2013
13% became BM tolerant
78% remained BM reactive
9% became UHM tolerant
Passed initial UHM challenge, n=7
86% continued unrestricted milk
19% remained BM tolerant
9% avoided all milk
72% became UHM tolerant
2 (5%) EoE 2 (5%) milk-FDEIA
8 (20%) disliked UHM 5 with intermittent mild oral sxs

Outcomes of 114 consecutive challenges to baked milk in the allergy office
• Jan 2008-Dec 2015
• Excluded from analysis b/c did not ingest the full dose: muffin-15, pizza-2
• 72% tolerated muffin OFC (50/69)
• 82% (22/28) tolerated pizza OFC
• Muffin reactors:
• n=10
• Median cumulative dose=1/4 muffin=325 mg of milk protein=0.33 oz milk
• Pizza reactors:
• n=5
Agyemang A, et al, manuscript submitted

Outcomes of 114 consecutive challenges to baked milk in the allergy office
Agyemang A, et al, manuscript submitted G) H)
3.3 3.3 3.1
p = 0.99
B)
3.5 2.8 5.2
p = 0.003*
A)
E) F)
4.1 4.1 2.4
p = 0.61
D)
2.6 1.4
9.5
p = 0.03* C)
9 9 9
p = 0.44
9 8.5 8
p = 0.73

Outcomes of 114 consecutive challenges to baked milk in the allergy office
Agyemang A, et al, manuscript submitted

Severity of reactions to baked milk:
1. Can be predicted by large skin prick test wheal
2. Cannot be reliably predicted
3. Can be predicted by higher level of serum sIgE
to cow’s milk
4. Can be predicted by prior history
5
60
3127
1 2 3 4

Severe vs. mild reactions to baked milk
Agyemang A, et al, manuscript submitted
Clinical Characteristics
Required epi Did not require epi
P value OR
Age, years 10.6 (3.03-14.8)
7.1 ( 3.17-9.84 )
0.37 -
CM IgE (kIU/L) 4.3 (3.1-11.7) 6.17 (3.4-10) 0.88 -
SPT (mm) 7.5 (3.6- 13.6) 9 (8-13) 0.37
Anaphylaxis to milk in the past
10.5% 15.8% * >0.99 1.67 (0.22-10.7)
+Asthma 21.1% 36.8% * >0.99 1.7 (0.23-11)
+Atopic Dermatitis
10.5% 57.9% *** 0.046 0.09 ( 0.01-0.9)
+Allergic Rhinitis 21.1% 47.4% * >0.99 0.89 (0.1-6.3)

Clinical phenotypes of milk allergy
• Baked-milk reactivity ~20%
• Less likely to “outgrow” milk allergy
• More severe reactions
• Most in need of effective therapy
• Majority of those with CM-IgE>35 kIU/L react to baked milk
• Baked milk tolerance ~80%
• Excellent chances of outgrowing milk allergy
• Mild reactions
• Introduction of baked-milk products into the diet changes similar to immunotherapy; PST, IgE & IgG4 [“natural OIT”?]
• Strict avoidance may account for delay in tolerance in children who have mild / transient milk allergy
Persistent / Severe Mild / Transient

Practical tips for introducing baked milk: the US approach
• Non-IgE mediated CMA, non-FPIES: introduce baked milk and regular milk at home gradually
• FPIES: physician-supervised challenge
• IgE-CMA:
-CM-IgE>35 kIU/L: defer challenge
-CM-IgE <35 kIU/L: consider physician-supervised challenge
-CM-IgE and casein-IgE < 1 kIU/L more than 95% likely to tolerate

Conclusions-1 • Heating reduces allergenicity of milk proteins
• Majority of milk and egg allergic children do not react to baked milk
• Baked milk diets are well tolerated
• Introduction of baked milk into diet is associated with increasing sIgG4 and
decreasing basophil reactivity and skin prick test wheal size suggesting an
immunomodulatory effect
• Children who incorporate baked milk to their diet appear to progress to tolerating
unheated milk at an accelerated pace compared to the children who maintain strict
avoidance
Conclusions-2 • Reactivity to baked milk is a marker of a more severe and more persistent milk
allergy
• Children with higher cow milk and casein-sIgE are more likely to react to baked milk
• sIgE and SPT do not discriminate between severe and mild baked milk-reactors (Epi
vs. no Epi)
• We need a biomarker to identify those at risk for more severe reactions and those
who are not at risk to recommend home introduction of baked milk

THANK YOU