slides for enduring syncd with video · antidepressants beta blockers anticonvulsants all ......
TRANSCRIPT
12/21/16
1
Faculty
CHAIRDavid Dodick, MD, FAHS, FRCPC, FACPProfessor of NeurologyMayo ClinicPhoenix, AZ
FACULTYDeborah I. Friedman, MD, MPH, FAHSProfessor, Neurology and Neurotherapeutics and OphthalmologyUniversity of Texas Southwestern Medical CenterDallas, TX
Stewart J. Tepper, MD, FAHSGeisel School of Medicine at DartmouthProfessor of NeurologyHanover, NH

12/21/16
2
Activity Description
Target AudienceThis activity is designed for clinicians involved in the care and treatment of patients with migraine pain.
Statement of NeedPatients with frequent migraines and/or who experience functional disability need preventative migraine treatment. However, studies have shown that of the 38% of patients who stand to benefit from prophylactic therapy, only 3‐13% of them actually receive it. Calcitonin gene‐related peptide (CGRP) monoclonal antibodies are under clinical investigation and constitute a new prophylactic migraine therapy class. Increased physician attention when individualizing treatment plans to maximize therapy efficacy and minimize side effects as well as managing headache triggers and existing comorbidities continue to be vital strategies as new agents emerge and when maximizing patient function.
SupportThis activity is supported by an educational grant from Lilly. For further information concerning Lilly grant funding, visit www.lillygrantoffice.com.
BarriersintheTreatmentof ChronicMigraine
David W.Dodick, M.D.
Professor
Department of Neurology
Mayo Clinic
Phoenix, Arizona

12/21/16
3
Migraine 7th mostdisabling
MOH 20th mostdisabling
Lancet 2016; 388: 1545–602
MOH = Migraine overuse headache
Only 45% see an HCP
Only 39% diagnosed by
an HCP
Of 775patients
meeting EM criteria
Only 26% receive treatment
Only 41% see an HCP
Only 11% diagnosed by
an HCP
Of 1254patients
meeting CM criteria
Only 4.5% receive treatment
Diagnosis and Management of Migraine (episodic and chronic) in United States
Lipton RB, et al. Headache 2013;51:81-92. Dodick DW, Headache 2016;56:821-834

12/21/16
4
Migraine Still Undertreated!
Adults withMigraine¹
50% of those diagnosed get
prescription treatment
36M
Fewer than 5 in 100 persons with migraine receive prescription treatment.Many diagnosed, yet untreated patients have cardiovascular conditions orrisks, or they have stopped treatments due to lack of adequate response
Diagnosis of Migraine2 3.7M Patients
Scale: figure = 1M people
1.9MNo PrescriptionTreatment
1.8MReceive Treatment2
3 out of 4 Treated Patients Receive Triptans2
1. www.americanmigrainefoundation.org; 2. IMS Health, PharMetrics Plus, January – December 2013 Cohort Projected to U.S. Insured Patient Population, 2015
CVD=cardiovasculardisease
Kurth et al. BMJ2016;353:i2610
Cardiovascular Risk in Migraine Women’s Health Study
• A prospective cohort study of 115,541 female nurses aged 25–42 followed from 1989-2011
• Migraine was associated with increased risk of:
– Major CVD
– Myocardial infarction
– Stroke
– Angina/coronary revascularisation procedures
– Significant increased risk for CVD mortality
• Women with migraine should be evaluated for vascular risk

12/21/16
5
Serious and unexpected
• Ischemic
cardiovascular
events
• Aneurysms/dissections
• Pregnancy‐related
vascular events
Coronary artery spasm (adj ROR 21.6; 16.1–23.9)
Arterial dissection (ROR 12.24; 4.42–32.25)
Placental infarction (ROR 12.68; 3.23–42.70)
Roberto G, et al. Cephalalgia 2013
2600/7800 adverse events attributed to
triptans fell under the cardiac category
• 2H-PF = 18-50%• 24HSPF = 13-33%
Cameron C, et al. Headache2015
HR=headache relief PF=pain freeSHR=sustained headache relief SPF=sustained pain free

12/21/16
6
Optimal Treatment Strategy of CM associated with medication overuse is not known
• Survey of 95 AHS members– I think that a well‐designed clinical trial that
compares different strategies of treating chronic migraine with medication overuse is needed
– 92 clinicians
– 3 migraine researchers• 88.4% agreed that the most effective tx
strategy is unknown
Studies Evidence Class
Early discontinuation 3 III
Early discontinuation with preventive medication
19 III
Preventive medication17 II
Strongly agree Somewhat agree Somewhat disagree Disagree
9.5%
87.4%
1.1% 2.1%
Closer Look at Preventive treatment
Underutilized, adherence poor

12/21/16
7
Closer look at prevention
13%
Prevention
Candidates Treated
40%
Migraine Sufferers
Lipton RB et al. Neurology 2007.Bigal et al. Neurology 2008;71:559‐66.
Treated 33%
Chronic Migraine Sufferers
Adherence to oral migraine preventive medications in patients with chronic migraine
Hepp Z., et al. Cephalalgia 2015;35:478-488

12/21/16
8
19%
2 1 %
3 1 %2 9 %
3 3 %
2 3 %
3 6 %
2 4 %
2 9 %
2 4 %
2 8 %
2 0 %
2 6 %
1 0 % 1 0 %
1 7 %
1 4 %
1 7 %
1 0 %
1 9 %
1 3 %
1 8 %
1 2 %
2 1 %
1 6 % 1 6 %
8 %
1 1 %
1 4 %
5 %
0 %
1 0 %
1 5 %
2 0 %
2 5 %
3 0 %
3 5 %
4 0 %
Amitriptyline
N=1,164
Nortriptyline
N=653
Citalopram
N=1,150
Sertraline
N=622
Fluoxetine
N=421
Paroxetine
N=190
Ven
lafaxine
N=277
Propranolol
N=699
Metoprolol
N=395
Nad
olol
N=110
Atenolol
N=195
Topiramate
N=2,604
Gabap
entin
N=860
Divalproex
N=292
Total
N=9,632
A n t i dep res s an t s Beta B lo cker s An t i convu l s an t s A l l
Cla sse s
ProportionofPatients
Persistent
Pers i s ten t A t 6 Mon t h s
3 2 %
Pers i s ten t a t 1 2 Mon t h s
86%
discontinue at 12months
Hepp Z., et al. Cephalalgia 2015;35:478-488
An even higher percentage discontinue drugs after switching
Start a Prophylactic N=9,632
Persist 14%
Discontinue86%
Switch 23% Discontinue87%
Switch 27% Discontinue90%
Reinitiate 32% Discontinue100%
Reinitiate 43% Discontinue92%
Untreated34%
2nd Prophylactic1st Prophylactic 3rd Prophylactic
Hepp Z., et al. Cephalalgia 2015;35:478-488
18
12/21/16
9
SummaryEnormous disability associated with migraine, chronic migraine and medication overuse headache
EM and CM are poorly recognized and under‐treated in clinical practice
There remains a large unmet acute treatment need with drugs that are more effective, lack safety concerns, and do not induce MOH
Prophylactic therapies for migraine are under‐utilized and lack the efficacy and tolerability to enable patients to persist
Current and Emerging TherapiesStewart J Tepper, MD, FAHS
Professor of NeurologyGeisel School of Medicine at Dartmouth
Hanover, New Hampshire

12/21/16
10
Episodic Migraine (EM) Prophylaxis: Anti‐Epilepsy Drugs• Topiramate
• FDA‐approved for migraine prevention with Level A/Class 1 evidence and 2 large RCTs (studied up to 200 mg/day)
• Commonly reported side effects: paresthesia, weight loss, cognitive dysfunction, mood change, kidney stones
• Contraindicated in pregnancy due to teratogenicity
• Multiple mechanisms include anti‐glutamate effects and inhibition of cortical spreading depression (CSD)
• Also 2 RCTS showing effectiveness in prevention of Chronic Migraine (not FDA approved for this)
• Divalproex sodium, sodium valproate• Level A/class I evidence
• 500‐1000 mg/day, significant reduction in 4‐week migraine headache rate as compared with PBO
• AEs: weight gain, alopecia, nausea, tremor, hepatotoxicity, polycystic ovaries
• Contraindicated in pregnancy due to teratogenicity
• Gabapentin• Level U evidence
• Cochrane meta‐analysis found ineffective in migraine prophylaxisSilberstein SD, et al. Neurology. 2012;78:1337-1345.
Linde M, et al. Cochrane Database Syst Rev. 2013;(6):CD010609. doi: 10.1002/14651858.CD010609.
Episodic Migraine Prophylaxis: Anti‐hypertensives• Beta Blockers
• Level A evidence: propranolol, timolol (both FDA approved), also metoprolol
• Level B evidence: atenolol, nadolol• Contraindicated in patients with asthma, COPD, emphysema, pre‐existing bradycardia, partial AV block, hypotension, and hypoglycemia associated with diabetes treatment
• Beta blockers inhibit CSD and central neuronal hyperexcitability
• The ARB candesartan now has Level A evidence and is equal to (directly compared) propranolol
Silberstein SD, et al. Neurology. 2012;78:1337-1345.Barbanti P, et al. Neurol Sci. 2011;32(suppl1):S111-115.
Stovner E, et al. Cephalalgia. 2014;34:523-532.

12/21/16
11
Onabotulinumtoxin A for Prevention of Chronic Migraine (CM): Pooled Analysis of the PREEMPT Trials
• Design• Two trials that were double‐blind, randomized, 24‐week, placebo‐controlled identically designed trials of Chronic Migraine (CM) patients
• Followed by a 32‐week open label trial
• Primary endpoint• Onabot (155‐195U) injections q 12 weeks for 2 cycles (n=688), placebo n= 3,696
• At week 24, there was a significant decrease in frequency of headache days for the experimental (‐8.4 days, onabot) vs the pbo group (‐6.6 days, P<.001)
• Few treatment AEs • Only 3.8% of onabot pts discontinued due to AEs (vs 1.2% of pbo patients)
Dodick DW, et al. Headache. 2010;50:921-936.
AAN Practice Guidelines for OnabotulinumtoxinA• Class A evidence: Safe and effective for reducing the number of headache days in CM (2 Class I studies)
• Probably effective for improving QOL (1 Class I study)
• Insufficient evidence to compare onabot with oral topiramate (no direct comparison)
• Ineffective for EM and not recommended
• Probably ineffective for treating CTTH
Simpson DM et al. Neurology 2016;86:1818‐26

12/21/16
12
As we move to the many new classes, formulations, and devices in development for emerging therapies, how can we best assess their utility for our patients?
Patient‐Reported Outcomes (PROs)
• 5 questions can be condensed to one: How many days was the patient at least 50% disabled at work, home, school, or recreational activities in the last 3 months?
• The domain collected is time loss reported
• The more time lost the higher the score, intuitively understood, e.g. 20 days in the last 90 days with at least 50% disability due to migraine
• Validated for data collection Q3 months
Stewart WF, et al. Pain. 2000;88:41-52.
Migraine Disability Assessment Scale: MIDAS

12/21/16
13
The Headache Impact Test (HIT‐6)
• 6 domains, validated for monthly data collection• Social functioning• Role functioning• Vitality• Cognitive functioning• Psychological distress• Severity of headache pain
• Scores range between 36 and 78; >60 severe impact • Both MIDAS and HIT‐6 used to follow therapy effects as PROs
• HIT‐6 scale not intuitive, but 6 domains may have an advantage over one domain
• 2‐3 point change likely clinically meaningful
Yang M, et al. Cephalalgia. 2011;31:357-367.Kosinski M, et al. Qual Life Res. 2003;12:963-974.
The FDA, 2009‐ 40 pages of Requirements for a New Validated PRO:Since this Guidance, not a single validated PRO has been approved for therapy evaluation in any medical area, too bureaucratic, complicated, and costly
US Dept of HHS, FDA, CDER, CBER, CDRH. December, 2009.

12/21/16
14
Current and Future Acute Therapies
• Triptans and Ergots• Migraine‐specific (also work for some TACs)• Usage at 10 days or more per month associated with chronification• Vasoconstrictive
• Non‐vasoactive migraine‐specific acute medications in development:• 5HT1F receptor agonists: Lasmiditan• Phase 3 study completed & presented at EHMTIC meeting Sept 2016, Glasgow
• Established efficacy of 2 hour pain freedom and elimination of “most bothersome symptom”• Centrally acting, no vasoconstriction• Phase 3 adverse event profile: dizziness and fatigue at approximately the same rates as rizatriptan (not directly compared)
• CGRP receptor antagonists (“Small molecules”), gepants: Ubrogepant‐ more later• Prevent vasodilation, don’t vasoconstrict
Tfelt-Hansen PC, Olesen J. J Headache Pain. 2012;13:271-275.EHMTIC presentations. Glasgow, Scotland. Sept 2016.
Neuromodulation
• Targets: occipital cortex, occipital nerves, vestibular nerves, supraorbital nerves, vagus nerve, and sphenopalatine ganglion
Proposed Mechanisms of Action
• Transcranial magnetic stimulation inhibits cortical spreading depression
• Some neuromodulation devices may modulate central pathways such as thalamocortical pathways to gradually down‐regulate pain systems
12/21/16
15
• Delivers an electric current to supraorbital and supratrochlear nerves1
• Sham controlled, randomized trial for the prevention of EM (n=67)
• Worn 20 mins/day, above the procerus, for 3 months
• Poor adherence in this study
• Patients had at least 2 migraine attacks/month (n=67)
• Only one of two primary endpoints were positive:
• Change in monthly migraine days negative vs placebo
• 50% responder rate was significantly greater in the active vs the sham group (38.1% vs 12.1%, p=0.23)
• AEs: Dysphoric paresthesias/dysesthesias, drowsiness2
• FDA approved for prevention of EM as a minimal risk device 1. Schoenen J. Neurology. 2013;80:1-8. 2. Magis D, et al. The Journal of Headache and Pain.
2013;14:95.
FDA Approved Devices:Transcutaneous Supraorbital Neurostimulator (tSNS)
FDA Approved Devices: Single Pulse Transcortical Magnetic Stimulation• sTMS1‐2
• Sham controlled trial to evaluate if 2 pulses could terminate a migraine in patients with aura
• Inhibits rat cortical spreading depression
1. Lipton RB, et al. Lancet Neurol. 2010;9(4):373-80.2. Bhola R, et al. J Headache Pain. 2015;16:51.
12/21/16
16
• N=449 (140 analyzed), 9000 attacks, women in 2nd trimester of pregnancy included
• Mean baseline frequency 15 attacks per month
• PRN instructions: • 2 consecutive pulses at onset of migraine attack• Continue with 2 pulses every 15min for 1-2h or pain relief
• Evaluate after 1st month, increase the number of pulses if needed: • Increase to 3 pulses every 15min for 1-2h or pain relief
• Evaluate after 2nd month, increase the number of pulses if needed: • Increase to 4 pulses every 15min for 1-2 hours or pain relief
• For frequent migraine attack pattern: Daily treatment, 4 pulses BID
Bhola R, et al. J Headache Pain. 2015;16:51.
sTMS for Episodic Migraine: UK Post Market Pilot Program
• Pain relief (62%) in >9,000 attacks
• EM: reduction in headache days/month
• 12 (median, 8-13 IQR) to 9 (4-12 IQR)
• CM: reduction headache days/month
• 24 (median, 16-30 IQR) to 16 (10-30 IQR)
• Nausea, photophobia, phonophobia relief
• Decreased use of acute medication use in 119
(Average 8.5 day reduction)
• AEs: Lightheadedness (20%)
• Discontinuation rate: 55% (n=105)• Ineffective, inconvenient, cost
Bhola R, et al. J Headache Pain. 2015;16:51.
UK Post Market Pilot Program: Results

12/21/16
17
• US Open Label ESPOUSE Study
• 8 U.S. Headache Centers, N=132 migraine patients with 5‐25 headache days/month
• 4 pulses BID + prn up to 17 pulses/day
• average 9 headache days/month at baseline to 6 days/month at 3 months of treatment
• No serious adverse events
Presented EHMTIC meeting, Glasgow, Scotland 9/7/16.
sTMS US ESPOUSE Study : Acute & Preventive, MO & MA, EM & CM
• Tested under acute and preventive conditions for
• Episodic and Chronic Cluster, Episodic and Chronic Migraine, acute and preventive
• 5 RCTs not all published or presented
• ACT1 study: Showed acute effectiveness to provide relief by 15 minutes in episodic cluster headaches but not chronic cluster headaches
• Acute regimen: 2 pulses lasting 2 mins each; used at the beginning of a cluster attack
• Preventive regimen: Two 90‐120 second pulses, TID for prevention of cluster and migraine
• Handheld device delivers electrical stimulation to the vagus nerve
• Evidence for effectiveness
• Approved for use in Europe
• Approved and available in Canada but not used much
• Before the FDA for acute treatment of cluster headache
Gaul C, et al. Cephalalgia 2016;36:534‐46.Clinicaltrials.gov. NCT01792817.Clinicaltrials.gov. NCT02378844.
Silberstein SD, et al. Headache. 2016;56:1317‐1332. https://www.nice.org.uk/guidance/ipg552, accessed 4-14-16.
Devices in Development: Non‐invasive Vagal Nerve Stimulator (nVNS)

12/21/16
18
• Delivers controlled time‐varying thermal waveforms• Heats and cools the vestibular system• 3rd mechanism of centrally modulating migraine
• Pilot study to treat Episodic Migraine• 6 wks of treatment, 4 weeks of follow‐up• Per protocol: active (n = 28); placebo (n = 18)
• Used 2x daily; sessions 18 min in length• Primary endpoint +:migraine days/ 3rd mo
• 2°: RR, acute meds, mood, cognition, balance
• Will likely be submitted to the FDA soon for prevention of EM
Black RD, et al. IEEE J Transl Eng HealthMed. 2016;4:2000310.
Devices in Development: Caloric Vestibular Stimulation
• Implantable microstimulator for SPG neuromodulation of cluster headache
• Implanted through the mouth in <15 minutes
• EU RCT for Chronic Cluster, Sham‐controlled, n=28• Acute treatment of chronic cluster attacks: Pain relief at 15 mins following SPG stimulation
• 55% of attacks with pain relief 15 minutes vs 6% sham
• 89% reduction of attack preventive response seen in 40% of patients
• Transient, mild‐moderate loss of sensation within distinct maxillary nerve regions
• 65% of events resolved within 3 months
Schoenen J, et al. Cephalalgia. 2013;33:816-830.
Devices in Development: Implanted Sphenopalatine Ganglion (SPG) Stimulation

12/21/16
19
Sphenopalatine Ganglion Stimulation (cont)
• Long‐term device benefit1
• n=33
• 45% of patients demonstrated an acute response
• Approved in Europe, reimbursable; >400 patients now implanted world‐wide
• Long‐term responder rate (acute and preventive) 61% at 2 years
• Registration study in the US underway
• Safety data2
• n=96
• Perioperative surgical sequelae: sensory disturbances, pain, swelling
• Follow‐up: placement of a second stimulator on the opposite side, adjustment of lead location, replacement after initial, unsuccessful placement, or removal
• 25/29 patients indicated that surgical effects were tolerable• 90% of them would make the same decision again
1. Jürgens TP, et al. Cephalalgia. 2016;May 9.2. Assaf AT, et al. Int J Oral Maxillofacial Surg.
2016;45:245-254.
Not Everything Works: Negative Data
• Orexin 1 and 2 (receptor) antagonist1
• Filorexant (MK‐6096), 10 mg nightly for 3 months vs PBO
• Patients with 4‐14 days of migraine/month
• Nitric oxide synthase nitric oxide• NO is a gaseous vasodilator that may activate trigeminovascular fibers triggering the release of CGRP
• Nitric oxide synthase inhibitor, GW274150, given daily for 12 weeks was no different than PBO with respect to migraine prophylaxis2
1. Chabi A, et al. Cephalalgia. 2015;35:379-388. 2. Høivik HO, et al. Cephalalgia. 2010;30:1458-
1467.

12/21/16
20
A Focus on CGRP Monoclonal Antibodies
Deborah I. Friedman, MD, MPH, FAHS
University of Texas Southwestern Medical Center
Dallas, Texas
Calcitonin Gene‐Related Peptide
• CGRP is a 37 amino acid peptide
• Vasodilator and key mediator of neurogenic inflammation
• Regulates immune and inflammatory cells within the skin (psoriasis)
• Derived from mouse (100%), chimeric (65% human), humanized (90% human) or humanized (100% human)
Russell FA et al. Physiol Rev 2014:1099-1142Granstein RD et al. Acta Physiol (Oxf) 2015;213:586-94

12/21/16
21
Targets of Monoclonal Antibodies Dictate On and Off‐Target Toxicities~50 mAbs currently on the market, most for oncology and rheumatology
• CD20 – modulates immune system (rituximab)• Increased risk of opportunistic infection
• VEGF –inhibits angiogenesis and reduces tumor growth (bevacizumab)• Can do so in healthy tissue leading to GI perforation and poor wound healing
• CGRP ‐‐ inhibits vasodilator effect• May potentially cause ulcers or diarrhea
Monoclonal Antibodies Against CGRP
• Block CGRP, a vasodilator, without causing vasoconstriction
• CGRP mAbs have very low CNS penetration
• Reduce the bioavailability of CGRP; high receptor specificity
• Eliminated through reticuloendothelial system, similarly to endogenous antibodies (not liver or kidney)
• Monoclonal antibodies against the CGRP ligand• Galcanezumab (LY‐2951742)• ALD‐403• Fremanezumab (LBR‐101/TEV‐48125)
• Monoclonal antibodies against the receptor• Erenumab (AMG334)
12/21/16
22
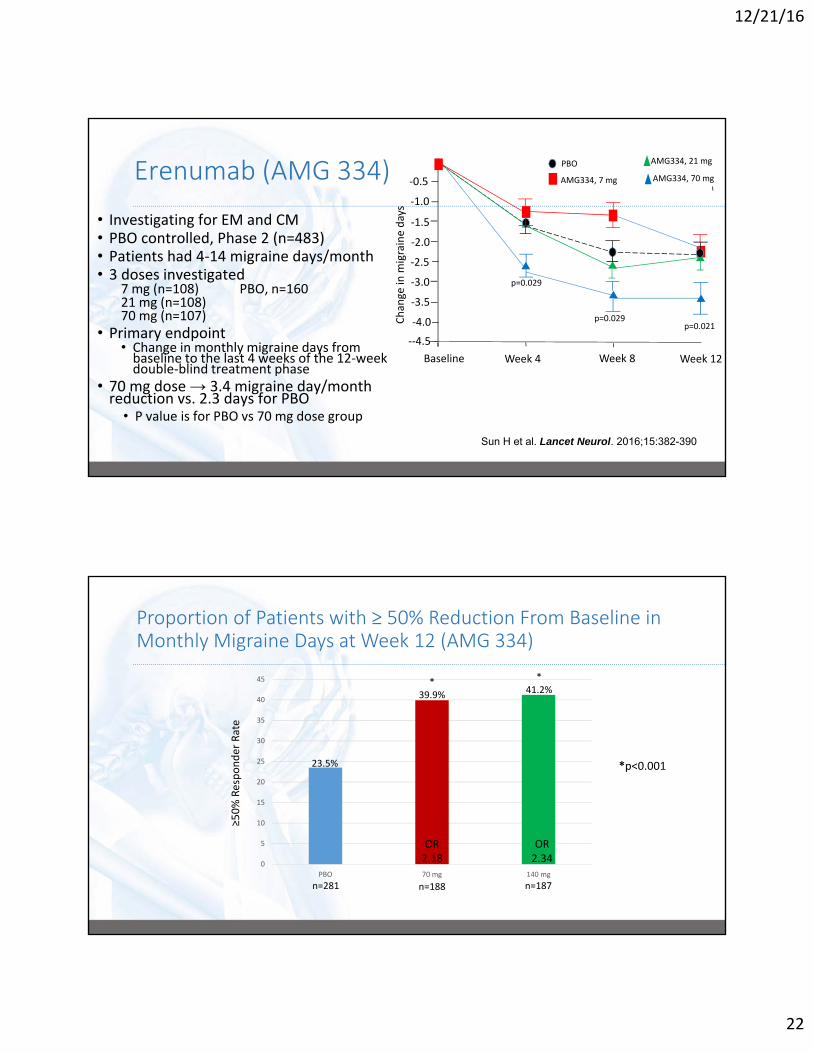
Erenumab (AMG 334)
• Investigating for EM and CM• PBO controlled, Phase 2 (n=483)• Patients had 4‐14 migraine days/month• 3 doses investigated
7 mg (n=108) PBO, n=16021 mg (n=108)70 mg (n=107)
• Primary endpoint• Change in monthly migraine days from baseline to the last 4 weeks of the 12‐week double‐blind treatment phase
• 70 mg dose → 3.4 migraine day/month reduction vs. 2.3 days for PBO
• P value is for PBO vs 70 mg dose group
Sun H et al. Lancet Neurol. 2016;15:382-390
‐0.5
‐1.0
‐1.5
‐2.0
‐2.5
‐3.0
‐3.5
‐4.0
‐‐4.5
Baseline Week 4 Week 8 Week 12
PBO
AMG334, 7 mg
AMG334, 21 mg
AMG334, 70 mg
p=0.029
p=0.029p=0.021
Change in
migraine days
Proportion of Patients with ≥ 50% Reduction From Baseline in Monthly Migraine Days at Week 12 (AMG 334)
*p<0.001
0
5
10
15
20
25
30
35
40
45
PBO 70 mg 140 mg
OR2.18
OR2.34
23.5%
*39.9%
*41.2%
≥50% Responder Rate
n=281 n=188 n=187
12/21/16
23
-5
-4
-3
-2
-1
0
PBO LY2951742
1 32
Months
Mea
n ch
ange
from
bas
elin
e in
the
num
ber
of m
igra
ine
days
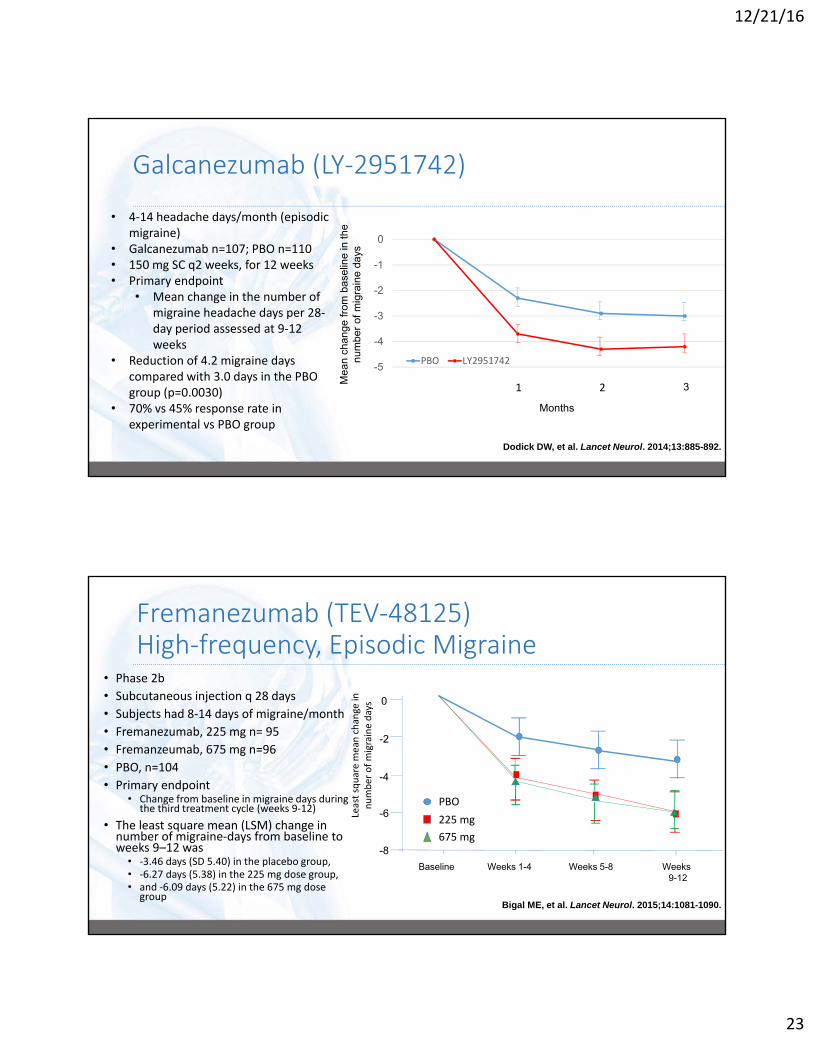
Galcanezumab (LY‐2951742)
• 4‐14 headache days/month (episodic migraine)
• Galcanezumab n=107; PBO n=110• 150 mg SC q2 weeks, for 12 weeks• Primary endpoint
• Mean change in the number of migraine headache days per 28‐day period assessed at 9‐12 weeks
• Reduction of 4.2 migraine days compared with 3.0 days in the PBO group (p=0.0030)
• 70% vs 45% response rate in experimental vs PBO group
Dodick DW, et al. Lancet Neurol. 2014;13:885-892.
Fremanezumab (TEV‐48125)High‐frequency, Episodic Migraine
• Phase 2b
• Subcutaneous injection q 28 days
• Subjects had 8‐14 days of migraine/month
• Fremanezumab, 225 mg n= 95
• Fremanzeumab, 675 mg n=96
• PBO, n=104
• Primary endpoint• Change from baseline in migraine days during
the third treatment cycle (weeks 9‐12)
• The least square mean (LSM) change in number of migraine‐days from baseline to weeks 9–12 was
• ‐3.46 days (SD 5.40) in the placebo group,• ‐6.27 days (5.38) in the 225 mg dose group, • and ‐6.09 days (5.22) in the 675 mg dose
groupBigal ME, et al. Lancet Neurol. 2015;14:1081-1090.
0
-2
-4
-6
-8
Least square mean change in
number of migraine days
Baseline Weeks 1-4 Weeks 5-8 Weeks9-12
PBO
225 mg
675 mg

12/21/16
24
Fremanezumab (TEV‐48125): Chronic Migraine• Phase 2b, SC injection every 28 days
• Treatment groups: • Fremanizumab 675/225 mg (n=88)
• Fremanizumab 900 mg (n=87)
• PBO (n=89)
• Primary endpoints: change in baseline in headache hours during 3rd treatment cycle; safety and tolerability
Bigal ME, et al. Lancet Neurol. 2015;14:1091-1100.
Fremanezumab for Chronic Migraine (Post‐hoc Analysis)
• High (900 mg, n=86) and low doses (675/225 mg, n=88) studied.
• PBO, n=89• Injections taken once a month, for 3 months
• Patients had a history of CM• Primary endpoint: Change from baseline in the number of headache hours in month 3• Three‐seven days post‐injection (ie, within one week of use), the number of headache hours decreased (early timepoint efficacy)
• These results endured throughout the study (month 3)
Bigal ME, et al. Neurology. 2016;87:41-48.
*
**
*
**
***
***
0
10
20
30
40
Baseline Week 1 Week 2 Week 3
PBO
675/225 mg
900 mg
Decrease in
hours from baseline

12/21/16
25
ALD403 Chronic Migraine
• Phase 2b 15‐28 headache days monthly (> 8 migraine days)
• Dose finding study with single IV dose ALD403
• 300 mg, 100 mg, 30 mg, 10 mg, PBO (n=120 per group)
• Primary outcome: 75% responder rate weeks 1‐12 reduction in migraine days)
Time Period Reduction in MMD per
month
300 mg IVN=114
100 mg IVN=118
30 mg IVN=117
10 mg IVN=123
PBO IVN=116
Weeks 1-12
50% decrease 65 (57%)** 64 (54%)* 64 (55%)* 54 (44%) 47 (41%)
75% decrease 38 (33%)* 37 (31%)* 33 (28%) 33 (27%) 24 (21%)
100% decrease 9 (8%) 6 (5%) 5 (4%) 10 (8%) 3 (3%)
1-sided p value vs. PBO: *p<0.05; **p<0.01 Dodick et al. EHMTIC 2016
ALD‐403
• Phase 2 trial
• Included patients who experienced 5‐14 migraine days every 28 day period (episodic)
• IV formulation: 1000 mg
• ALD‐403, n=81; PBO, n=82
• Primary endpoint: Change from baseline to weeks 5‐8 in the frequency of migraine days as recorded in patient electronic diaries
• Mean change in migraine days between baseline and weeks 5‐8:
• ‐5.6 days (SD 3.0) for ALD403 compared with ‐4.6 (SD 3.6) for PBO (p=0.0306)
Dodick DW, et al. Lancet Neurol. 2014;13:1100-1107.
ALD‐403
PBO
Time (weeks) 4 8 120
0
‐2
‐4
‐6
‐8
‐10
Mean change from baseline

12/21/16
26
Common Adverse Events Reported in Clinical Trials with CGRP mAbs• Injection site pain• Upper respiratory tract infection• Nausea• Erythema
• Arthralgia• UTI• Some reports of abdominal, back pain
• All treatment‐emergent adverse events were not different than those occurring with the placebo injections
• All adverse events appeared to be tolerability, not safety issues
Key Challenges to Introduction of CGRP mAbs• Long biological half-life
– Risk in patients who experience adverse events (e.g. hypertension)
– Pregnancy (planned and unplanned)
• Uncertainty in patients with atherosclerotic and vasospastic (e.g.
Raynauds) vascular disease, multiple vascular risk factors, hypertension.
• Patient access and physician burden related to ‘step-edits’ and prior
authorization
• Reserved for OnabotulinumtoxinA failures
• Small molecule CGRP receptor antagonists for prevention
– Upside: short half-life
– Downside: Daily oral medication

12/21/16
27
Small Molecule vs. Monoclonal Antibodies
Small Molecules Monoclonal Antibodies
Target specificity lower Target specificity high
Clearance (Liver, kidney) Clearance RES
Size < 1kD Size ~150kD
Oral Parenteral
Many enter cells and cross BBB Do not enter cells or cross BBB**
Half-life minutes to hours Half-life 1-4 weeks
Immunogenicity (No) Immunogenicity (yes)
CGRP Small Molecules May Offer Relief When Used Acutely
1. Voss T, et al. Cephalalgia. June 6, 2016.
• Ubrogepant (MK‐1602)
• CGRP receptor antagonist
• Phase IIb study
• Primary endpoint: pain freedom and headache response at 2 hrs
• N=527
• 100 mg of ubrogepant was significantly superior to PBO for 2‐hr pain freedom but not 2‐hr headache response

12/21/16
28
Atogepant (AGN‐241689, MK‐8031)
• Oral, small molecule CGRP receptor antagonist
• Currently in double‐blind, Phase 2, PBO‐controlled trials examining efficacy in episodicmigraine
• Characterization of the dose‐response relationship• 10 mg QD• 30 mg QD• 30 mg BID• 60 mg QD• 60 mg BID
• Primary outcome: change from baseline in the mean number of migraine/probable migraine headache days at month 3 (ie, last 28 days of the treatment period ending with week 12)
Clinicaltrials.gov. NCT02848326.
Summary
• Current preventive therapies are effective for many patients with migraine, but adverse events and lack of efficacy create a need for other options
• CGRP has a demonstrated role in the generation of migraine
• Targeted therapies against CGRP • Are promising thus far in clinical trials for migraine prevention
• Do not cause vasoconstriction
• Appear safe regarding side effect profile
• Do not require daily administration (vs. oral preventives)
• Offer treatment alternatives for EM and CM patients

12/21/16
29
Thank Youfor Your Participation!
To obtain CME/CE, please completeyour post‐test and evaluation.