small bowel enteroscopy dr cc foo queen mary hospital joint hospital surgical grand round 24-10-2009
TRANSCRIPT

SMALL BOWEL ENTEROSCOPY
Dr CC FooQueen Mary HospitalJoint Hospital Surgical Grand Round24-10-2009

SMALL BOWEL ENTEROSCOPY Small bowel represent the last frontier to be
explored with endoscopic means Difficulties caused by its relatively long length
and tortuosity

SMALL BOWEL ENTEROSCOPY 5% of all GI bleeding occurs between the
ligament of Treitz and ileocaecal valve
DiSario J et al. Enteroscopes - technology status evaluation report. Gastrointest Endosc 2007; 66(5): 872–80
SMALL BOWEL ENTEROSCOPY Small bowel pathologies
AngiodysplasiaMeckel’s diverticulaNSAID related enteropathyBenign or malignant tumour
SMALL BOWEL ENTEROSCOPY Push enteroscopy Double balloon enteroscopy (DBE) Single balloon enteroscopy (SBE) Spiral enteroscopy Capsule endoscopy

SMALL BOWEL ENTEROSCOPY Indications:
GI bleeding of obscure origin Chronic diarrhoea Malabsorptive syndrome Chronic abdominal pain
Therapeutic application: Foreign body removal Mucosal resection Insertion of SEMS Dilatation of stricture in Crohn’s disease ERCP after Billroth II or Roux-en-Y reconstruction or after bariatric
surgery

1807Bozzini :‘Lichtleiter’Comprised of wax candle, reflecting mirror and inspection tube
1957Hirshowitz: First flexible fiber endoscope
1970sClinical use of colonoscopy and upper endoscopy
1987Push enteroscocpy
2000Capsule endoscopy
1977Tada :Sonde enteroscope
2001Yamamoto:Double balloon enteroscopy
2006Otsuka:Single balloon enteroscopy
2007Akerman:Spiral endoscopy
ENDOSCOPY TIMELINE

SONDE ENTEROSCOPY
Described by Tada in 1977 Sonde enteroscopy Working length of 250-400cm Propelled by small bowel peristalsis Lack of working channel and prolonged
examination time
PUSH ENTEROSCOPY
Performed with a dedicated enteroscope with an overtube
Method:Overtube loaded onto the enteroscopeEnteroscope enter the proximal jejunumOvertube pushed into the 3rd part of duodenum and
held by assistantEnteroscope proceed to advance into the jejunum
Depth of insertion: 40 to 100cm past ligament of Treitz

DOUBLE BALLOON ENTEROSCOPY (DBE) Developed by Yamamoto in
2001 Manufactured by the Fujinon,
Inc, Saitama, Japan
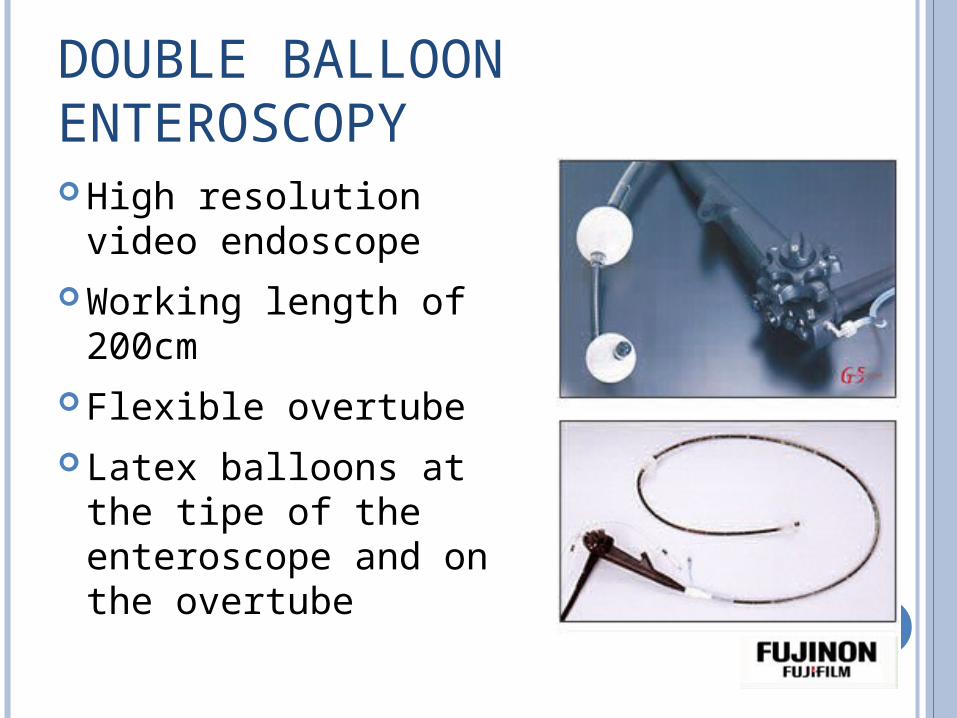
DOUBLE BALLOON ENTEROSCOPY High resolution video
endoscope Working length of 200cm Flexible overtube Latex balloons at the tipe
of the enteroscope and on the overtube

DOUBLE BALLOON ENTEROSCOPY Serial inflation and
deflation of balloons with air by the pressure-controlled pump
Alternating pushing and pulling maneuvers
Allowing the small bowel to be threaded onto the overtube
Matsumoto et al. Am J Roentgenol 2008

DOUBLE BALLOON ENTEROSCOPY
The Wolfson Unit for EndoscopySt Mark's Hospital, UK

DOUBLE BALLOON ENTEROSCOPY Antegrade (oral) and
retrograde (anal) approach could achieve total small bowel examination
Fluoroscopy can be used as an aid

SINGLE BALLOON ENTEROSCOPY (SBE) Developed by Ohtsuka in
2007 Manufactured by Olympus,
Inc, Tokyo, Japan
Working length of 200cm Outer diamter of 9.2mm Working channel 2.8mm Overtube overall length
140cm Latex free balloon

SINGLE BALLOON ENTEROSCOPY In contrast to DBE, balloon
is not attached to the tip of the enteroscope
Stable positioning in the small bowel is achieved during withdrawal of the scope by angling the tip of the endoscope

SINGLE BALLOON ENTEROSCOPY

SPIRAL ENTEROSCOPY
Described by Dr Akerman First performed in 2006 Applies the mechanical advantage of a screw to
convert rotational force into linear one Currently more than 2000 cases have been
performed worldwide

SPIRAL ENTEROSCOPY
Device: Discovery SB overtube Spirus CorporationOverall length 118cmOuter diameter 14.5mmAccomodates endoscope
<9.4mm diameter

SPIRAL ENTEROSCOPY Method
Overtube is backloaded on the enteroscopeAdvanced slowly with gentle clockwise rotation of the
overtube Spiral passes beyond the ligament of TreitzSpiral threads engage in the jejunum and mobile small
bowel can be rapidly pleated onto the enteroscope
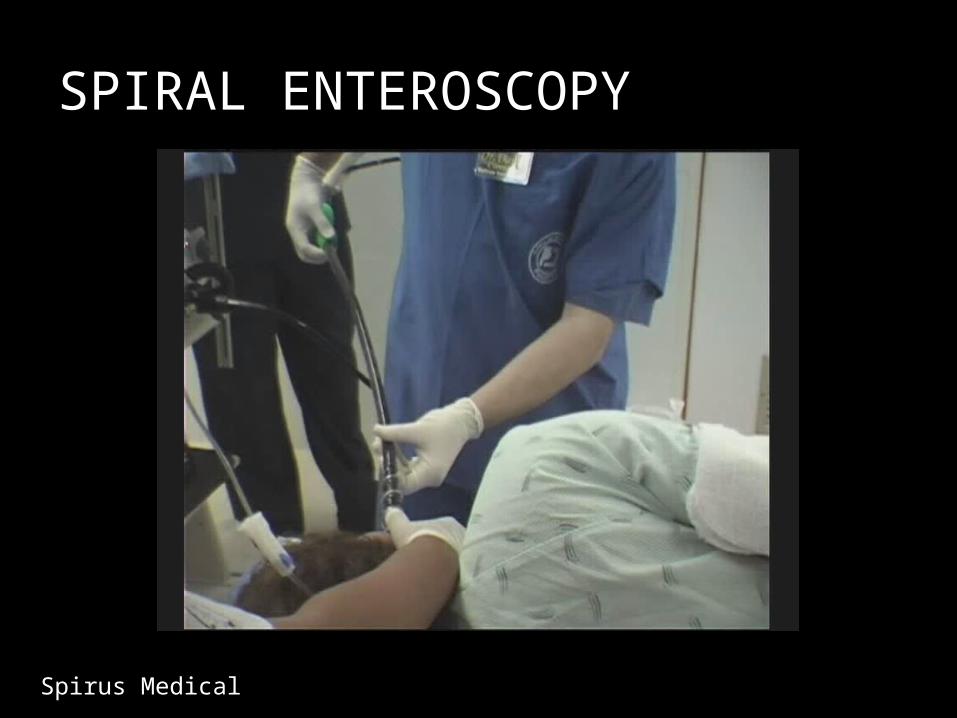
SPIRAL ENTEROSCOPY
Spirus Medical

COMPLICATIONS OF SMALL BOWEL ENTEROSCOPY Mucosal stripping Pancreatitis Aspirations Bleeding Gastric, duodenal and jejunal perforations
Complication rate generally <1%

EXAMINATION TIMEStudy Patient no. Mean exam
time(min)
Type
Yamamoto Japan 2004 123 123 DBE
Di Caro Europe 2005 62 160 DBE
Heine Netherland 2006 275 200 DBE
Mehdizadeh US 2006 188 197 DBE
Gross and Stark US 2008 137 197 DBE
Tsujikawa Japan 2008 41 (78 procedures) 133 SBE
Ramchandani India 2009 106 (131 procedures)
137 SBE
Akerman US 2008 101 17 Spiral
Esmail US 2009 57 28 Spiral
Morgan US 2009 148 34 Spiral
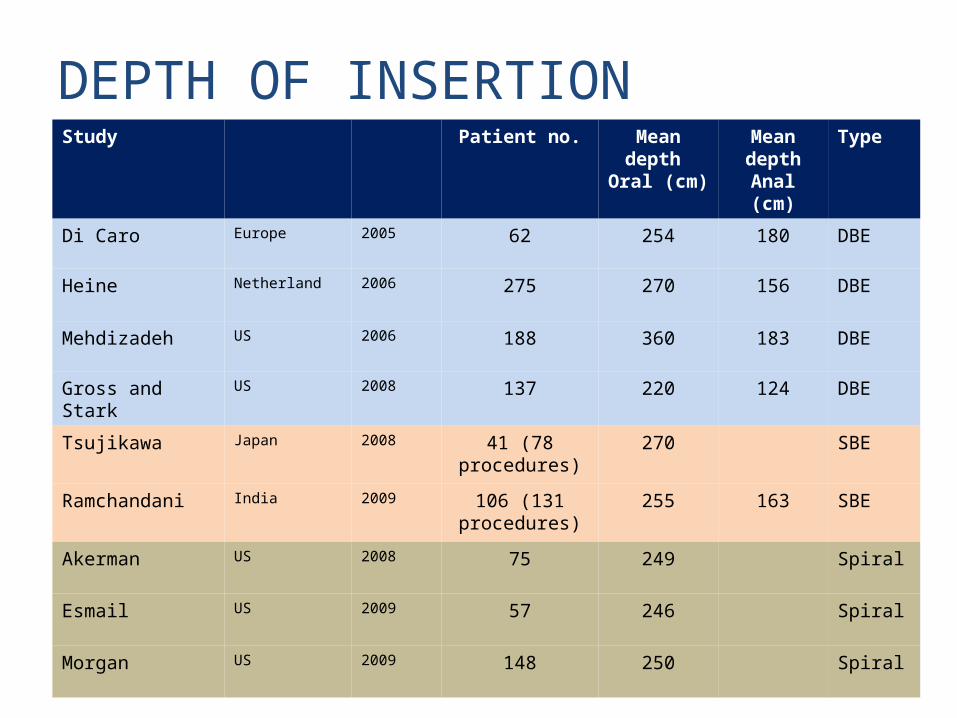
DEPTH OF INSERTIONStudy Patient no. Mean
depth Oral (cm)
Mean depthAnal (cm)
Type
Di Caro Europe 2005 62 254 180 DBE
Heine Netherland 2006 275 270 156 DBE
Mehdizadeh US 2006 188 360 183 DBE
Gross and Stark US 2008 137 220 124 DBE
Tsujikawa Japan 2008 41 (78 procedures)
270 SBE
Ramchandani India 2009 106 (131 procedures)
255 163 SBE
Akerman US 2008 75 249 Spiral
Esmail US 2009 57 246 Spiral
Morgan US 2009 148 250 Spiral

DIAGNOSTIC YIELDStudy Patient no. Yield
(%)Therap
y(%)
Type
Yamamoto Japan 2004 123 76 18 DBE
Di Caro Europe 2005 62 80 42 DBE
Heine Netherland 2006 275 73 55 DBE
Mehdizadeh US 2006 188 43 27 DBE
Gross and Stark US 2008 137 80 45 DBE
Tsujikawa Japan 2008 41 (78 procedures)
54 SBE
Ramchandani India 2009 106 (131 procedures)
61 8.4 SBE
Akerman US 2008 75 24 13 Spiral
Esmail US 2009 57 51 Spiral

COMPLETE SMALL BOWEL EXAMINATIONStudy Patient no. Complete
examination%
Type
Yamamoto Japan 2004 123 86 DBE
Di Caro Europe 2005 62 16 DBE
Heine Netherland
2006 275 42 DBE
Mehdizadeh US 2006 188 4 DBE
Gross and Stark US 2008 137 20 DBE
Tsujikawa Japan 2008 24 25 SBE
Ramchandani India 2009 20 25 SBE

CONCLUSION
Advances in small bowel enteroscopy facilitate diagnosis and management of small bowel lesions
Histological sampling and therapeutic endoscopies are made possible
Results of different enteroscopies are yet to be revealed by future clinical trials