smart helmet: brain and cardiac activity monitor · smart helmet: brain and cardiac activity...
TRANSCRIPT

Smart helmet: brain and cardiac activity monitor
Wilhelm von Rosenberg1, Theerasak Chanwimalueang1,Valentin Goverdovsky1, Danilo P. Mandic1
Abstract— Time of assessing the severity of the injuriesfollowing a road-traffic accident involving motorcyclists isabsolutely crucial particularly in the events with head injuries.Standard apparatus for monitoring cardiac activity is usuallyattached to the limbs or the torso, while the brain functionis routinely measured with a separate unit connected to thehead-mounted sensors. In stark contrast to these, we proposean integrated system which incorporates the two functionalitiesinside an ordinary motorcycle helmet. We have mounted mul-tiple fabric electrodes inside the helmet at positions featuringgood contact with the skin at different sections of the head. Wedemonstrate that the R-peaks (and therefore the heart rate) canbe reliably extracted from potentials measured with electrodeson the mastoids and the lower jaw, while the electrodes onthe forehead enable the observation of neural signals. Thus,we conclude that various vital sings and brain activity can bereadily recorded from the inside of a helmet in a comfortableand inconspicuous way, requiring only diminutive setup effort.
I. INTRODUCTION
Wearable devices are set to revolutionise and democratisepersonalised diagnosis and treatment, brining it to millions,if not billions of people. Monitoring health in extremesituations is essential to ensure the safety of all participantsand to provide rapid response in the event of emergencies. Itis important to get accurate vital signs and brain activitymeasurements as soon as possible even if no external orobvious signs of trauma are present. As a preventive measure,recordings of cardiac and brain activity enable the exam-ination and assessment of stress and concentration levels,which are especially important in potentially dangeroussituations such as flying a plane, riding a motorcycle orskiing. Common parameters that are considered for the eval-uation of the physiological state are body temperature, heartrate, breathing rate and blood pressure [1]. Additionally, anelectroencephalogram (EEG) can provide an indication ofthe psychological state of a person. This study focuses onperforming measurements from the sensors mounted inside ahelmet worn while executing a set of specific activities. Thiswork uses a modified motorcycle helmet, but the techniquesand approaches described are applicable to all helmets,whose inner lining is routinely in good contact with the skinat a number of locations on the head.
Some of the previous work in this area included mea-surements of the electrocardiogram (ECG) of Formula Onedrivers during races [2] employing electrodes attached tothe torso which had to be installed before every event.However, a system that can be set up off-site or does not
1Department of Electrical and Electronic Engineering, Imperial CollegeLondon, United Kingdom wv12, tc2113, goverdovsky,[email protected]
require a laborious setup process would be beneficial as itreduces the inconvenience for the person being examined[3].Obtaining a ballistocardiogram and a single lead ECG fromsensors placed behind the ear, [4] showed the possibilityto collect cardiac data non-invasively from head locations.Additionally, the ECG and electrooculogram (EOG) wererecorded from an army helmet equipped with electrodesattached to straps [5], and the ECG between both earsfrom modified earphones [6]. Another ear-based recordingtechnique is in-the-ear EEG where an EEG is obtained fromelectrodes inside the ear canals [7].
Although similar to this work none of the above ap-proaches demonstrated an integrated solution for monitor-ing both brain and body functions simultaneously. Otherimprovements of the proposed method and apparatus com-pared to the earlier work are: (i) the increased comfortand convenience since the helmet is worn in the same wayas a standard helmet; and (ii) the enhanced performanceachieved by the steady electrode-skin contact. A precursorof this study is described in [8], where cardiac data wasextracted from electrodes underneath a motorcycle helmetusing metallic gold-cap electrodes. In the current study, therigid electrodes were replaced with flexible conductive fabricand the cardiac data is supplemented with measurements ofthe brain activity. This fabric can be easily integrated withinthe helmet’s inner lining and requires only saline solution toachieve the low impedance contact. We have analysed thepotential differences between the electrodes and the optimalsensor positions were determined. The utility of the cardiacdata obtained from the helmet was corroborated with thereference signal recorded simultaneously from the limbs,while the capabilities of the proposed system to measure thebrain function were verified with standard brain responses –auditory steady state response (ASSR) and steady-state visualevoked potential (SSVEP).
II. EXPERIMENTAL DETAILS
Heartbeats are triggered by electrical currents propagatingthrough the heart. From a distance, the superposition of allcurrent dipoles in the entire heart can be represented by onecurrent dipole – the heart vector, whose orientation and am-plitude change over the course of one cycle. In this study weinvestigate six electrode positions: two to monitor brain andfour to monitor cardiac activity. Comparing with standardECG electrode configurations, the setup is approximatelyakin to lead I. However, the currents produced by the heartvector travel through inhomogeneous tissues and geometriesuntil they are picked up by sensors on the head, therefore,

they may include components of other leads and are likely tobe corrupted by artefacts such as cheek and jaw movementsand other muscle activity.
The most prominent feature of the ECG cycle is the R-peak – a sharp spike with a high amplitude. Its occurrencesin time can be used to determine the heart rate. To be able toassess the quality of the recordings, the identified timings ofR-peaks are compared to reference measurements taken fromthe arms and quantified by using the established parameters:sensitivity (Se) and positive predictivity (+P ) [9]:
Se =TP
TP + FN, +P =
TP
TP + FP
where TP stands for the number of correctly identifiedR-peaks, FN for the number of missed R-peaks and FPfor the number of points incorrectly labelled as R-peaks.Furthermore, we introduce another measure of quality, thatof assessing the deviation of the estimated heart rate fromthe actual heart rate at regular instances in time.
There is a number of EEG paradigms, particularly evokedresponse potentials (ERP) which lend themselves well totesting new hardware. The two we have concentrated on inthis work are the SSVEP and the ASSR. SSVEP is the signalthat originates in the visual cortex [10] in response to a visualstimulus operating at a fixed rate of 3.5Hz to 75Hz. Theresulting brain electrical activity contains exactly the sameor multiples of the stimulation frequency. It is widely used inthe area of brain computer interfaces (BCI) due to excellentsignal-to-noise (SNR) ratio and robustness to artefacts. ASSRinvolves the hearing pathway and is the brain’s response toauditory stimuli. When presented with either white noiseor a high frequency sinusoidal signal (e.g. 1 kHz) ampli-tude modulated with another sinusoid of significantly lowerfrequency (e.g. 40Hz), the human brain ‘demodulates’ thesignal and produces the response at the modulating frequency[11]. This response is most pronounced in the temporal lobeof the brain. We have evaluated the performance of the twoforehead electrodes by analysing the recordings during theexposure of the subjects to the above stimuli. Additionally,we have also assessed the capability of the setup to measurethe alpha rhythm – periodic signal bursts in the 7.5Hz –15.5Hz frequency band, produced by the brain in a relaxedstate with eyes closed.
A. Setup
A standard motorcycle helmet was equipped with elec-trodes mounted on its inner lining (see Fig. 1 (left)). Conduc-tive fabric (MedTex130) was used to construct the electrodes,ensuring that they are unobtrusive and fit well inside thehelmet. The fabric electrodes can easily be sewed directlyinto the helmet cloth at a later stage and the results areexpected to be identical. However, the ability to freely moveelectrodes around was more important at this stage. Theelectrode positions were chosen based on the quality of thecontact with the skin and their location relative to the sourcesof the signals of interest. Out of seven electrodes, three werein contact with the forehead, the one in the centre serving as
the common ground (GND), two on the mastoids, and two onboth sides of the lower jaw, see Fig. 1 (right). They are namedafter the side on the head – Left or Right, and their position –Forehead, Mastoid or Jaw. To reduce the impedance of theelectrode-skin interface, the fabric was lightly wetted withsaline solution.
The two electrodes on the sides of the forehead (LF andRF) recorded brain activity and the potentials were measuredrelative to the LJ electrode. LF acted as a reference forpotential measurements at the other four locations (LM,RM, LJ and RJ). Impedances between GND and the signalchannels ranged from 4 kΩ to 16 kΩ for subject 1 and from9 kΩ to 32 kΩ for subject 2. The unipolar setup enabled themeasurement of potential differences between any two chan-nels which is useful in the analysis of ECG recordings. Toestablish the ground truth, ECG was also recorded betweenthe two arms. Data was acquired from two different subjectsfor 60 s to 300 s at a sampling rate of 1200S/s using thebio-signal amplifier – g.USBamp, manufactured by g.tec.
For both ECG and EEG measurements the subjects wereput through three different scenarios while sitting at rest:(i) awake with eyes close – alpha rhythm measurement; (ii)listening to a 1 kHz sinusoid, amplitude-modulated with a40Hz sinusoid – ASSR measurement; and (iii) attending anLED blinking at a rate of 15Hz – SSVEP measurement.
III. DATA PREPROCESSING
A. ECG channels
As mentioned before, the heart can be represented as adipole and the potential differences are the largest when thetwo measurement points are on the opposite ends of thedipole. However, the geometry of the human body is notregular and the orientation of the heart vector changes overtime, therefore, the potential differences of all six channelcombinations of LM, RM, LJ and RJ were considered andanalysed to identify the most suitable ones.
This study concentrates on the accuracy of the heart rate,thus only the timings of the R-peaks were important and theselection of the filter parameters did not take into account
Fig. 1. Setup of the helmet (left) and the positions of the electrodes onthe head (right).

the need to conserve any of the other characteristics ofthe ECG waveform. Generally established methods whichidentify particular characteristics of the ECG-cycle do notseem to be optimised for signals with consistently highlevels of noise. For example, the algorithm developed in [12]accomplishes very good values for Se (as defined above),but due to a large number of false positives, the values for+P are low for most channels. In [8] R-peak identificationsuccess rates were compared after applying various bandpassfilters to ECG signals with very low SNR. Experimentallyit was found that 3rd order Butterworth bandpass filterswith cut-off frequencies around 8Hz and 25Hz lead tothe best results. This filter configuration corresponds tothe frequencies necessary to represent the R-peak having aduration of 0.04 s (minimum period where the amplitude ofthe R-peak is above the baseline) to 0.12 s (maximum lengthof the QRS complex)[13]). Meanwhile, other details of theECG-cycle (such as the P- and T-peak) are lost after suchfiltering. Subsequently, the resulting signals were scannedfor R-peaks and the identified timings were compared to theactual occurrences as per ground truth recordings from thearms, which have high SNR, thus R-peak locations can beeasily validated visually. The R-peak search in the signalswas performed by determining local peaks separated bya minimum time and with an amplitude above a certainthreshold.
B. EEG channels
The potentials measured at the forehead electrodes, LFand RF, were preprocessed according to the brain responseof interest. In scenario (i) – alpha rhythm measurement, a 4th
order Butterworth filter with a bandpass range between 1Hzand 30Hz was applied. For scenarios (ii) and (iii), the lowercut-off of the bandpass filter was kept constant at 1 Hz andthe upper cut-off was set to 45Hz and 25Hz, respectively.
IV. DISCUSSION
A. Cardiac activity
The accuracy of the R-peak detection was quantified byapplying two different methods, using the parameters Seand +P as outlined in Section II and by calculating thedeviation of the estimated heart rate from the real heartrate as per signals measured from the arms. An R-peak isclassified as correctly identified if it occurs within [tR −∆t, tR +∆t] where tR is the time of the actual R-peak and∆t = 0.02 × ∆tRR, with ∆tRR being the average timebetween two adjacent R-peaks. Depending on the positionof the sensors and therefore the angle between the vectorconnecting the two points and the heart vector, the mostsignificant peak in the ECG cycle can occur with a slighttime offset to the standard measurement from the arms. Toavoid classifying identified peaks as incorrect even thoughthey exhibit a constant positive or negative delay, anotherparameter is introduced – the heart rate measure obtainedfrom the inverse of the duration of five full ECG cycles.We quantify the accuracy of this measure as the root-mean-square error (RMSE) of the heart rate deviation (HRD) –
Time (s)4 6 8 10 12 14
Pot
entia
l Diff
eren
ce ∆
V a
nd R
-pea
ks
Arm - peaksArm - ECGLJ-RJ - peaksLJ-RJ - ∆VLM-RM - peaksLM-RM - ∆VLM-LJ - peaksLM-LJ - ∆VLM-RJ - peaksLM-RJ - ∆VRM-RJ - peaksRM-RJ - ∆VLJ-RM - peaksLJ-RM - ∆V
farm_low: 0.5farm_high: 40farm_order: 3fsig_low: 8
fsig_high: 25fsig_order: 3
Fig. 2. Potentials differences measured between electrodes on the face(lines) and identified R-peaks (crosses) compared to a reference ECG fromthe Arms (top trace).
the difference between the deduced and the real heart rateat every second with time series of the heart rates wasinterpolated. The results are shown in TABLE I where thetotal number of R-peaks across multiple subjects and trialswas 1290 and the HRD is measured in beats per minute(bpm).
For subject 1, the sensor combinations LJ-RJ, LM-LJ,LM-RJ, and RM-RJ produced very reliable signals acrossall trials. The values for Se and +P are close to 100%and the HRD is less than 1. The LM-LJ, the LM-RJ andin most trials the LJ-RJ as well show approximately thesame results for the 2nd subject. However, the quality ofthe other channels is much lower. This is also reflected inTABLE I which summarises the results across all subjectsand trials with LM-LJ and LM-RJ featuring the best perfor-mance parameters. Varying outcomes for certain electrodecombinations across trials can be explained by a disturbedconnection between at least one of the electrodes and theskin, e.g. in one of the trials for subject 2 all measurementswhich include RM do not result in reliable extractions ofR-peaks. A poor performance of a particular electrode pairin general can indicate that the two electrodes involved arepositioned on lines with very similar electric potentials for
TABLE IQUALITY OF THE RECORDINGS ASSESSED IN SENSITIVITY (SE),
POSITIVE PREDICTIVITY (+P) AND HEART RATE DEVIATION (HRD).
Setup TP FN FP Se +P HRD(bpm)
LJ-RJ 1211 79 72 93.9% 94.4% 2.28LM-RM 791 499 605 61.3% 56.7% 11.26LM-LJ 1275 15 15 98.8% 98.8% 0.66LM-RJ 1278 12 12 99.1% 99.1% 0.80RM-RJ 1071 219 253 83.0% 80.9% 6.41LJ-RM 516 774 977 40.0% 34.6% 17.02
a significant part of the ECG cycle. To further improve theresults, particularly in low SNR scenarios, the detection of R-peaks can be enhanced by combining multiple signals duringthe R-peak search.
B. Brain activity
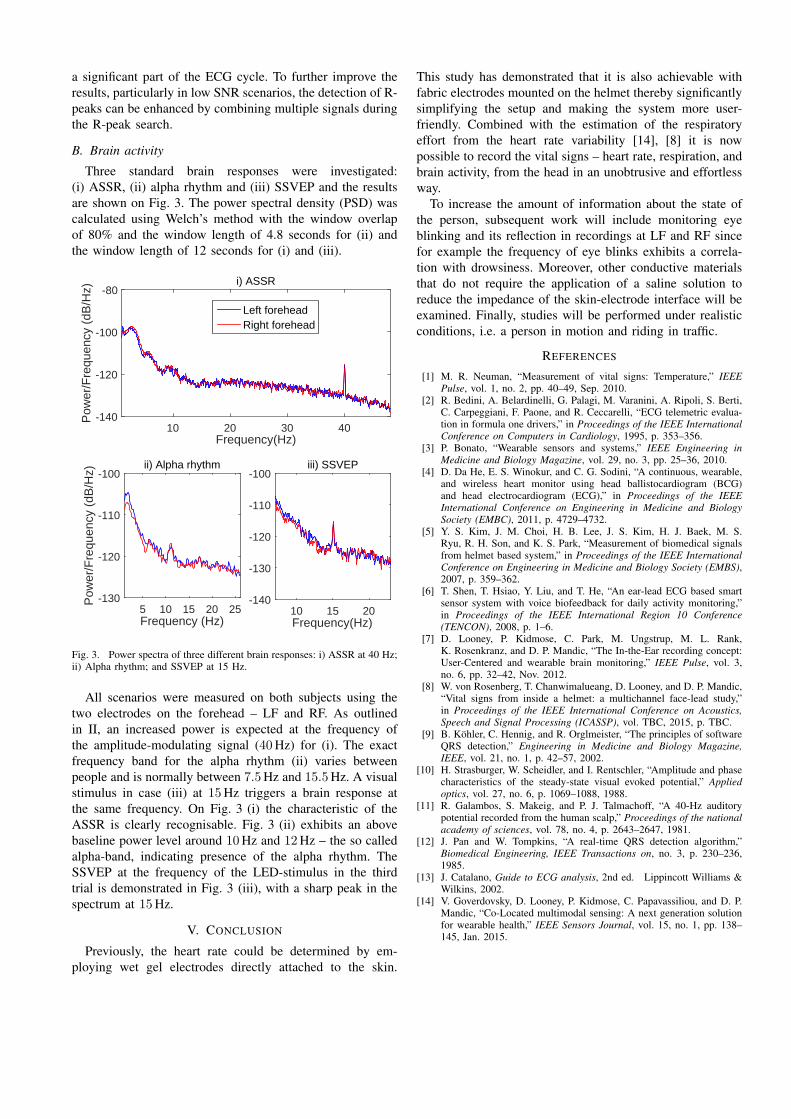
Three standard brain responses were investigated:(i) ASSR, (ii) alpha rhythm and (iii) SSVEP and the resultsare shown on Fig. 3. The power spectral density (PSD) wascalculated using Welch’s method with the window overlapof 80% and the window length of 4.8 seconds for (ii) andthe window length of 12 seconds for (i) and (iii).
Frequency(Hz)10 20 30 40
Pow
er/F
requ
ency
(dB
/Hz)
-140
-120
-100
-80i) ASSR
Left foreheadRight forehead
Frequency (Hz)5 10 15 20 25
Pow
er/F
requ
ency
(dB
/Hz)
-130
-120
-110
-100ii) Alpha rhythm
Frequency(Hz)10 15 20
-140
-130
-120
-110
-100iii) SSVEP
Fig. 3. Power spectra of three different brain responses: i) ASSR at 40 Hz;ii) Alpha rhythm; and SSVEP at 15 Hz.
All scenarios were measured on both subjects using thetwo electrodes on the forehead – LF and RF. As outlinedin II, an increased power is expected at the frequency ofthe amplitude-modulating signal (40Hz) for (i). The exactfrequency band for the alpha rhythm (ii) varies betweenpeople and is normally between 7.5Hz and 15.5Hz. A visualstimulus in case (iii) at 15Hz triggers a brain response atthe same frequency. On Fig. 3 (i) the characteristic of theASSR is clearly recognisable. Fig. 3 (ii) exhibits an abovebaseline power level around 10Hz and 12Hz – the so calledalpha-band, indicating presence of the alpha rhythm. TheSSVEP at the frequency of the LED-stimulus in the thirdtrial is demonstrated in Fig. 3 (iii), with a sharp peak in thespectrum at 15Hz.
V. CONCLUSION
Previously, the heart rate could be determined by em-ploying wet gel electrodes directly attached to the skin.
This study has demonstrated that it is also achievable withfabric electrodes mounted on the helmet thereby significantlysimplifying the setup and making the system more user-friendly. Combined with the estimation of the respiratoryeffort from the heart rate variability [14], [8] it is nowpossible to record the vital signs – heart rate, respiration, andbrain activity, from the head in an unobtrusive and effortlessway.
To increase the amount of information about the state ofthe person, subsequent work will include monitoring eyeblinking and its reflection in recordings at LF and RF sincefor example the frequency of eye blinks exhibits a correla-tion with drowsiness. Moreover, other conductive materialsthat do not require the application of a saline solution toreduce the impedance of the skin-electrode interface will beexamined. Finally, studies will be performed under realisticconditions, i.e. a person in motion and riding in traffic.
REFERENCES
[1] M. R. Neuman, “Measurement of vital signs: Temperature,” IEEEPulse, vol. 1, no. 2, pp. 40–49, Sep. 2010.
[2] R. Bedini, A. Belardinelli, G. Palagi, M. Varanini, A. Ripoli, S. Berti,C. Carpeggiani, F. Paone, and R. Ceccarelli, “ECG telemetric evalua-tion in formula one drivers,” in Proceedings of the IEEE InternationalConference on Computers in Cardiology, 1995, p. 353–356.
[3] P. Bonato, “Wearable sensors and systems,” IEEE Engineering inMedicine and Biology Magazine, vol. 29, no. 3, pp. 25–36, 2010.
[4] D. Da He, E. S. Winokur, and C. G. Sodini, “A continuous, wearable,and wireless heart monitor using head ballistocardiogram (BCG)and head electrocardiogram (ECG),” in Proceedings of the IEEEInternational Conference on Engineering in Medicine and BiologySociety (EMBC), 2011, p. 4729–4732.
[5] Y. S. Kim, J. M. Choi, H. B. Lee, J. S. Kim, H. J. Baek, M. S.Ryu, R. H. Son, and K. S. Park, “Measurement of biomedical signalsfrom helmet based system,” in Proceedings of the IEEE InternationalConference on Engineering in Medicine and Biology Society (EMBS),2007, p. 359–362.
[6] T. Shen, T. Hsiao, Y. Liu, and T. He, “An ear-lead ECG based smartsensor system with voice biofeedback for daily activity monitoring,”in Proceedings of the IEEE International Region 10 Conference(TENCON), 2008, p. 1–6.
[7] D. Looney, P. Kidmose, C. Park, M. Ungstrup, M. L. Rank,K. Rosenkranz, and D. P. Mandic, “The In-the-Ear recording concept:User-Centered and wearable brain monitoring,” IEEE Pulse, vol. 3,no. 6, pp. 32–42, Nov. 2012.
[8] W. von Rosenberg, T. Chanwimalueang, D. Looney, and D. P. Mandic,“Vital signs from inside a helmet: a multichannel face-lead study,”in Proceedings of the IEEE International Conference on Acoustics,Speech and Signal Processing (ICASSP), vol. TBC, 2015, p. TBC.
[9] B. Kohler, C. Hennig, and R. Orglmeister, “The principles of softwareQRS detection,” Engineering in Medicine and Biology Magazine,IEEE, vol. 21, no. 1, p. 42–57, 2002.
[10] H. Strasburger, W. Scheidler, and I. Rentschler, “Amplitude and phasecharacteristics of the steady-state visual evoked potential,” Appliedoptics, vol. 27, no. 6, p. 1069–1088, 1988.
[11] R. Galambos, S. Makeig, and P. J. Talmachoff, “A 40-Hz auditorypotential recorded from the human scalp,” Proceedings of the nationalacademy of sciences, vol. 78, no. 4, p. 2643–2647, 1981.
[12] J. Pan and W. Tompkins, “A real-time QRS detection algorithm,”Biomedical Engineering, IEEE Transactions on, no. 3, p. 230–236,1985.
[13] J. Catalano, Guide to ECG analysis, 2nd ed. Lippincott Williams &Wilkins, 2002.
[14] V. Goverdovsky, D. Looney, P. Kidmose, C. Papavassiliou, and D. P.Mandic, “Co-Located multimodal sensing: A next generation solutionfor wearable health,” IEEE Sensors Journal, vol. 15, no. 1, pp. 138–145, Jan. 2015.