sob diagnosis
TRANSCRIPT

WEEK3: SHORTNESS OF BREATH
Abdulrhman Aljoher…..(62/8)

How to diagnose a patient with dyspneaassociated with chest pain?


Steps to reach the diagnosis
History of present illness
Review of systems
Past medical history
Physical examination
Interpretation of findings
Testing Diagnosis
History of present illness
It should cover the following:
• Duration
• Onset (e.g., Abrupt, insidious)
• Provoking or aggravating factors (eg, allergen exposure, cold, exertion, supine position).
• Severity by assessing the activity level required to cause dyspnea
Review of systems
In this step, you should look for symptoms of possible causes.
For example:
chest pain or pressure
suggests pulmonary embolism
[PE], myocardial
ischemia, or pneumonia
dependent edema,
orthopnea, and
paroxysmal nocturnal dyspneasuggests
heart failure
fever, chills, cough, and
sputum production
suggests pneumonia

Past medical history
Past medical history should cover disorders known to cause dyspnea, including asthma, COPD, and heart disease.
You should look for risk factors for the different etiologies (next slide).
Occupational exposures (eg, gases, smoke, asbestos) should be investigated

Risk factors for the different etiologies
• Smoking history
For cancer, COPD, and
heart disease
• Family history, hypertension, and high cholesterol levels
For coronary artery disease
• Recent immobilization , trauma or surgery, recent long-distance travel, prior or family history of clotting, pregnancy, oral contraceptive use, calf pain, leg swelling, and known deep venous thrombosis
For PE

Physical examination
Vital signs: fever, tachycardia, and tachypnea.
Lung examination
A full lung examination should be perfomed to evaluate:
• adequacy of air entry and exit
• Breathing sounds symmetry
• Presence of abnormal sounds crackles, rhonchi, stridor, and wheezing. (listen to them on YouTube)
• Signs of consolidation
• Lymphadenopathy (cervical, supraclavicular, inguinal palpation)
Physical examination
Neck veins should be inspected for distention
the legs should be palpated for pitting edema (both suggesting heart failure).
Heart sounds should be auscultated with notation of any extra heart sounds, weak heart sounds, or murmur.
Conjunctiva should be examined for pallor.

Red flags signs in PE
Dyspnea at rest during
examination
Decreased level of consciousness or
agitation or confusion
Accessory muscle use and poor air
excursion
Chest pain Crackles Weight loss
Night sweats Palpitations

Interpretation of findings
The history and physical examination often suggest a cause and guide further testing
• suggests asthma or COPD.
Wheezing
• suggests extrathoracic airway obstruction (eg, foreign body, epiglottitis, vocal cord dysfunction).
Stridor
• suggest left heart failure, interstitial lung disease, or, if accompanied by signs of consolidation, pneumonia.
Crackles

Testing
Pulse oximet
ry
CXR ECG ABG

Extra Testing
If no clear diagnosis obtained from chest x-ray and ECG and patient is at moderate or high risk of having PE, he should undergo
CT angiography
ventilation/perfusion scanning.
• Patients who are at low risk may have
d-dimer testing (a normal d-dimer level effectively rules out PE in a low-risk patient).


Now you can give your final diagnosis!
How to evaluate a patient with Dyspnea at the Emergency room?

Components of Emergency evaluation of Dyspenic patient
History
Physical examination
Ancillary studies

History at ER
It is Critical to the evaluation of the acutely dyspneic patient.
It can be difficult to obtain and it can be obtained from
• the patient
• EMS providers
• family and friends
• Pharmacists
• primary care clinicians

History at ERAsk for the following whenever possible!
General historical features
Past historyPrior
intubationTime course
Severity Chest pain Trauma Fever
Paroxysmal nocturnal
dyspnea (PND)Hemoptysis
Cough and sputum
Medications
Tobacco and drugs
Psychiatric conditions

Physical Examination at ER
Physical examination at the beginning should look for clinical danger signs (e.g. signs of significant respiratory distress in all patients with acute dyspnea.)
Respiratory arrest can be portended by:
Depressed mental status
Inability to maintain respiratory effort
Cyanosis

Physical Examination
Respiratory rate Pulse oximetry (normal SpO2 ≥ 95%) Abnormal breath sounds: stridor, wheezing,
crackles, diminished breath sounds. Cardiovascular signs:
An abnormal heart rhythm Heart murmurs S3 or S4 heart sound Muffled or distant heart sounds Elevated JVP
Pulsus paradoxus

ANCILLARY STUDIES
Ancillary testing should be performed in the context of the history and examination
findings.
Random testing without a clear differential diagnosis can mislead the clinician and
delay appropriate management.

Ancillary studies list
Chest x-ray (CXR) ECGCardiac
biomarkersBrain natriuretic
peptide
D-Dimer ABGCarbon dioxide
monitoringChest CT and VQ
scan
Peak flow and pulmonary
function tests (PFTs)
Negative inspiratory force
Differential diagnosis in this patient after the clinical assessment
The probable Differential diagnosis of dyspnea with acute
onset
Pulmonary embolism
Abrupt onset of sharp chest pain, tachypnea, and
tachycardia
Often risk factors for pulmonary embolism
• cancer,
• immobilization
• DVT
• pregnancy,
• use of oral contraceptives
• recent surgery or trauma
CT angiography
V/Q scanning
pulmonary arteriography

The probable Differential diagnosis of dyspnea with acute
onsetAnxiety disorder causing hyperventilation
Situational dyspnea often
accompanied by psychomotor agitation and
paresthesias in the fingers or
around the mouth
Normal examination
findings and pulse oximetry
measurements
Diagnosis of exclusion

Case suggestive findings for the diagnosis
Patient chief complaints
Suggestive findings from the patient's history
6 months inpatient for severe depression and psychosis. Patient was bed ridden most of the
time
Right fibula fracture 15 days back
Smoker, 40 cigarettes/day
Development of hemoptysis

Additional information from the patient’s history
Patient is on regular medication for DM &
HTN
No orthopnea or leg swelling
No Family history of IHD, dyslipidemia, asthma, or chronic
lung disease
JVP is not raised No
hepatosplenomegalyNo pitting edema
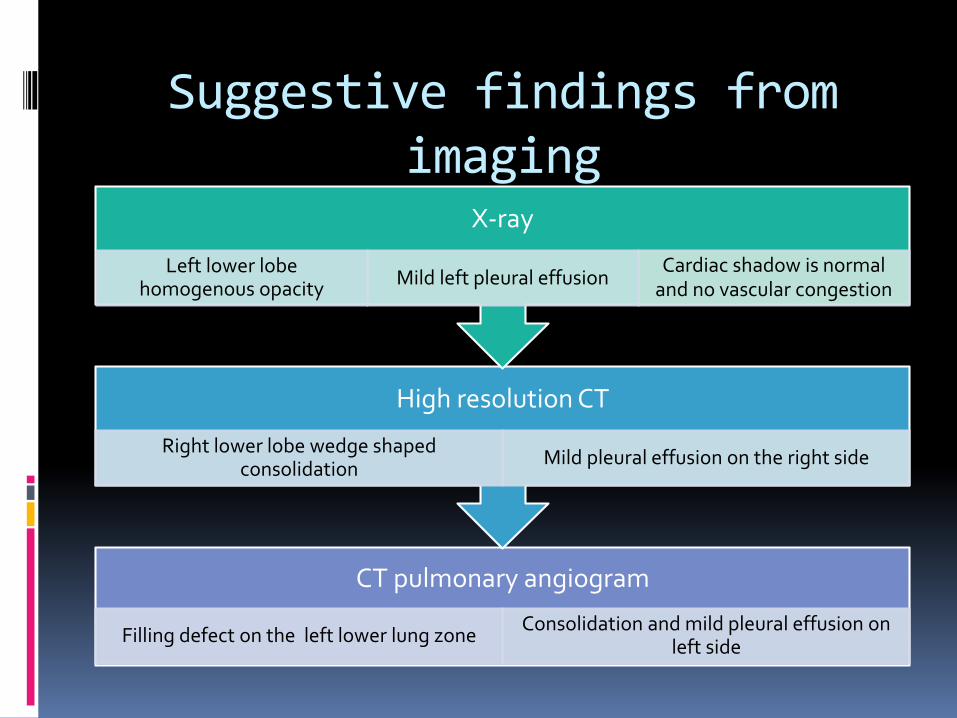
Suggestive findings from imaging
CT pulmonary angiogram
Filling defect on the left lower lung zone Consolidation and mild pleural effusion on
left side
High resolution CT
Right lower lobe wedge shaped consolidation
Mild pleural effusion on the right side
X-ray
Left lower lobe homogenous opacity
Mild left pleural effusion Cardiac shadow is normal
and no vascular congestion

References
http://www.uptodate.com/contents/evaluation-of-the-adult-with-dyspnea-in-the-emergency-department#H12
http://www.merckmanuals.com/professional/pulmonary_disorders/symptoms_of_pulmonary_disorders/dyspnea.html
http://www.uptodate.com/contents/evaluation-of-the-adult-with-dyspnea-in-the-emergency-department#H12

THANK YOU