social support at age 33: the influence of gender, employment status and social class
TRANSCRIPT
Social support at age 33: the in¯uence of gender,employment status and social class
Sharon Matthewsa,*, Stephen Stansfeldb, Chris Powera
aInstitute of Child Health, Department of Epidemiology and Public Health, University College London, 30 Guilford Street,
London WC1N 1EH, UKbDepartment of Epidemiology and Public Health, University College London, 1-19 Torrington Place, London WC1 6BT, UK
Abstract
This paper investigates the conceptualisation and operationalisation of social support and it's relationship to
gender, employment status and social class. Clari®cation of these relationships is sought in order to betterunderstand associations between social support and health. We used data from the 33-year survey of the 1958British birth cohort study. Individual items and subscales of practical and emotional support were examined. In
general, men had lower support than women and social classes IV and V had lower support than classes I and II.Emotional support, either from personal (for example, from friends or family), or combined with organisationalsources of support (such as from a church or a ®nancial institution), showed consistent gender and social class
patterns. This suggests that emotional support is a robust concept across socio-demographic groups. Less consistenttrends were found for practical support, in that socio-demographic trends depended on how practical support wasmeasured. In particular, it depended on whether both personal and organisational sources of support wereexamined. Gender di�erences in social support were large and might therefore be expected to contribute to gender
di�erences in health, whereas social class di�erences in social support were modest, suggesting a minor explanatoryrole for this factor in accounting for inequalities in health. # 1999 Elsevier Science Ltd. All rights reserved.
Keywords: Social support; Gender; Employment status; British birth cohort
Introduction
Since the mid 1970s there has been increasing inter-
est in the relationship between social support and
health. Social support, as measured by social network
variables, has been shown to predict all cause mortality
among adults of all ages (Blazer, 1982; House et al.,
1982; Berkman and Breslow, 1983; Welin et al., 1985;
Schoenbach et al., 1986; Kawachi et al., 1996), and is
especially related to coronary heart disease mortality
(Orth-Gomer and Johnson, 1987; Kaplan et al., 1988;
Kawachi et al., 1996). As well as mortality, social sup-
port has been related to a wide range of health out-
comes including well-being and depression (Brown and
Harris, 1978; Aneshensel and Stone, 1982; Brown et
al., 1986; Brugha et al., 1990; Stansfeld et al., 1998b),
pregnancy outcome (Turner et al., 1990; Ho�man and
Hatch, 1996; Rogers et al., 1996), perinatal health of
mother's and children (Norbeck and Peterson Tilden,
1983; Oakley et al., 1994a,b; Kearns et al., 1997), post
traumatic distress disorder (Stephens and Long, 1997),
Social Science & Medicine 49 (1999) 133±142
0277-9536/99/$ - see front matter # 1999 Elsevier Science Ltd. All rights reserved.
PII: S0277-9536(99 )00122-7
* Corresponding author. Tel.: +44-171-813-8392; fax: +44-
171-242-2723
E-mail address: [email protected] (S. Matthews)

improved immune status following drug therapy for
cancer (Lekander et al., 1996), anorexia and bulimianervosa (Tiller et al., 1997) and various chronic con-ditions such as rheumatoid arthritis (Fitzpatrick et al.,
1988, 1991) and diabetes (Kaplan and Hartwell, 1987).Although the literature is extensive, research on
social support has tended to focus on either men orwomen. For instance, cardiovascular risk has been pre-dominantly studied in men, whereas studies of mental
health have focused on women. However, the strengthof the relationship between social support and mor-tality may di�er between men and women (Fusilier et
al., 1986): for example low scores on an index of socialconnection were signi®cantly associated with mortality
risk for men but not women (Kaplan et al., 1988).Sources of social support may di�er both qualitativelyand quantitatively, for example men may bene®t from
work based sources of support, while women may relymore on family and non-work sources (Leavy, 1983).Such di�erences may play a role in explaining sex
di�erences in mortality and morbidity rates. Similarly,social support may contribute to socio-economic
inequalities in health and mortality. There is evidencethat social support varies by social class, perceivedsupport (Turner and Marino, 1994; Stansfeld et al.,
1998b) and network size (Fischer, 1982) are greater inhigher social groups. Moreover the contribution of
social support to class di�erences in health may varyfor men and women, but such gender comparisons aregenerally overlooked (Macintyre and Hunt, 1997).
Much of the research on social support is based onsecondary data or where original studies have beenconducted sample sizes are generally small or the
samples are very specialised. Therefore clari®cation isneeded of the nature of socio-economic and gender
di�erences in social support.Future investigations of social support should take
account of methodological issues such as the conceptu-
alisation and measurement of social support. Many ofthe inconsistencies in research ®ndings on social sup-
port and health may be due to methodological pro-blems (Miller and Ingham, 1976; Fuller and Larson,1980; Barrera, 1981; Billings and Moos, 1981;
Broadhead et al., 1983). Needless to say social supporthas been conceptualised and measured in many ways.It is unlikely that a universally recognised measure will
be established, rather key concepts and dimensions ofsocial support have emerged. For example, it has been
de®ned in terms of social networks, social integration,availability of support, received social support and per-ceived support (Sarason et al., 1990). For each of these
concepts, di�erent measures have been developed.Wellman (1981) identi®es `structural dimensions' ofsupport including the number of people in a network,
density and complexity of a network. Several investi-gators make a theoretical distinction between social
support and networks, whereby support denotes`emotional, instrumental and ®nancial aid' obtained
from a social network (Kaplan et al., 1977; House,1981; Thoits, 1982; Berkman, 1984). This introducesquality of interaction as well as number of contacts. A
further distinction is now often made betweenemotional (con®ding) and practical (or instrumental)social support, with investigators focusing on either or
both dimensions (Schaefer et al., 1981; Seeman et al.,1985; Stansfeld and Marmot, 1992; Rodgers, 1994).Given these methodological considerations, our
objectives were ®rst, to establish the appropriateness ofdi�erent de®nitions of social support for di�erentsocial strata focusing in particular on emotional andpractical support, and second, to examine the relation-
ship of social support to gender, employment statusand social position. Speci®cally, we addressed ®vequestions: do women report better or worse social sup-
port than men; how are these di�erences distributedacross separate support items; does social support dif-fer by employment status; are the socio-economic gra-
dients in social support similar for men and women,and ®nally, if social gradients exist, do they varyaccording to employment status? A ®nal objective is to
discuss the implications of the results for furtherresearch on social support and health. We used datafrom the 1958 British birth cohort study, which con-tains information on social relationships and support
at age 33.
Methods and measures
Sample
The 1958 British cohort includes all births in one
week in 1958 (3rd±9th March) in England, Scotlandand Wales. Information was collected on 98% ofbirths totalling 17,414. Subsequent follow-up of survi-
vors was undertaken at ages 7, 11, 16, 23 and mostrecently in 1991 at 33 years, when 11,405 subjects(69% of the target) were re-interviewed (Ferri, 1993).
Despite sample attrition, those remaining in the studywere found to be generally representative of the orig-inal sample (Ferri, 1993). Only data from the 33 yearsurvey were used in this analysis.
Measures
Social class: based on current (91% of men and72% of women) or most recent (the remainder) occu-pation according to the Registrar General's 1990
classi®cation. Women were classi®ed by their own oc-cupation and not by their partner's. Four categorieswere used: classes I and II (professional and manage-
S. Matthews et al. / Social Science & Medicine 49 (1999) 133±142134

rial), IIInm (skilled non-manual), IIIm (skilled man-
ual), and IV and V (semi and unskilled manual).Employment status: at age 33 respondents reported
their current main economic activity. Women were
categorised as employed (full-time, thirty hours ormore per week or part-time, less than thirty hours) or
home-workers (that is housewives). Men were cate-gorised as employed (employees or self-employed) orunemployed and seeking work. Men who were home-
workers (n=24), in full-time education (n=21), tem-porary or permanently sick or disabled (n=117), andunclassi®ed (n=38) were excluded from the analyses
due to small numbers. For women, those excludedwere unemployed (n=118), in full-time education
(n=48), temporary or permanently sick/disabled(n=64) and the unclassi®ed (n=35).Social support: six questions on social relationships,
adapted from the British Social Attitudes Survey(Finch, 1989) include:
1. ``Suppose you needed advice about an importantchange in your life, for example, about a job, or
moving to another part of the country, who wouldyou turn to for advice?'' (personal advice).
2. ``Suppose you were very upset about a problem
with your husband, wife or partner, and had notbeen able to sort it out with them. Even if you are
not married or have no partner, what would you doif you were, who would you turn to for help?'' (con-®ding support).
3. ``Suppose you felt just a bit down or depressed andyou wanted to talk about it, who would you turn tofor help?'' (distress support).
4. ``Suppose you had the `¯u' and you had to stay inbed for a few days, and needed help around the
home, with shopping and so on, who would youturn to for help?'' (domestic help).
5. ``Suppose you needed to borrow a large sum of
money, who would you turn to for help?'' (®nan-cial).
6. ``There are some household and garden jobs youreally can't do alone, for example, you may needsomeone to hold a ladder, who would you turn to
for help?'' (household DIY).
Respondents were required to nominate up to four
sources of support from personal (`spouse/partner',`parent/in-law', `other relative', `friend or neighbour',
`someone you work with') and organisational sources(`church, charity, social services etc.', `someone youpay to help'; and `other source of advice'). Initially a
scale was derived by summing the numbers of sourcesof support from across all possible eight sources (thatis, personal and organisational). Separate scales were
constructed for emotional support (items 1±3 above)and practical support (items 4±6 above). For `con®ding
support' (in the emotional scale) there was more miss-ing data than expected, especially for men, signifying
that the hypothetical situation (item 2) was particularlyproblematic for con®ding support. To overcome thisproblem, the emotional sub-scale comprised all three
items only for those who had married or cohabited,with a cut-o� of three or less indicating low support.For the never married the `con®ding support' item was
omitted, and a cut o� of two or less was used to indi-cate low support. In addition to the sub-scales foremotional and practical support, we examined the indi-
vidual questions separately, with a cut-o� of one orless indicating low support, that is, only one source ofsupport was identi®ed.
Data analysis
In the ®rst stage of analysis we examined social class
patterns for each support question separately, andcompared trends for ®ve (personal) with eight (per-sonal and organisational) sources of support; second,
we compared the social support sub-scales and individ-ual items to investigate relationships with gender,social position and employment status. Pearson's w 2
was used to test independence between social support,employment status and gender. Social class trends insocial support were examined for men and women,and for employment status groups, using the Mantel±
Haenszel w 2 test. Analysis was carried out using SPSSUnix version 6.1.
Results
Methodological ®ndings
Table 1 presents the percentages of men and women
with low support by social class, for individual ques-tions and for 5 (personal only) and 8 (personal and or-ganisational) support sources. Similar social trends
were observed for the 5 and 8 item support sourcesrepresenting emotional support: the percentage withlow support increased from classes I and II to classes
IV and V. Exclusion of organisational support had lit-tle impact on the social class trend. For practical sup-port, household DIY showed a consistent classgradient for scores based on both 5 and 8 support
sources. For `domestic help' there was no class trendfor men or women for either 5 or 8 support sources.However, for `®nancial' support the 5 and 8 support
sources showed inconsistent class distributions. A classgradient (to the detriment of lower classes) was evidentfor the 8 support sources measure but not for the 5
support sources measure. This suggests that whilst®nancial support from personal sources is similaracross social classes, support from organisational
S. Matthews et al. / Social Science & Medicine 49 (1999) 133±142 135
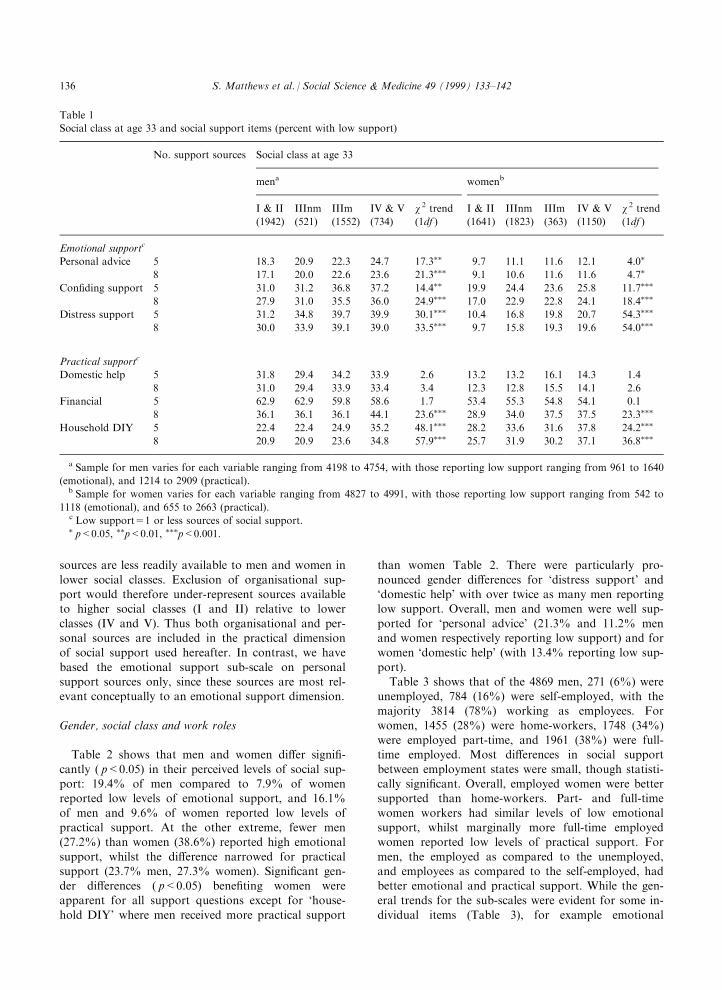
sources are less readily available to men and women in
lower social classes. Exclusion of organisational sup-port would therefore under-represent sources availableto higher social classes (I and II) relative to lower
classes (IV and V). Thus both organisational and per-sonal sources are included in the practical dimensionof social support used hereafter. In contrast, we have
based the emotional support sub-scale on personalsupport sources only, since these sources are most rel-evant conceptually to an emotional support dimension.
Gender, social class and work roles
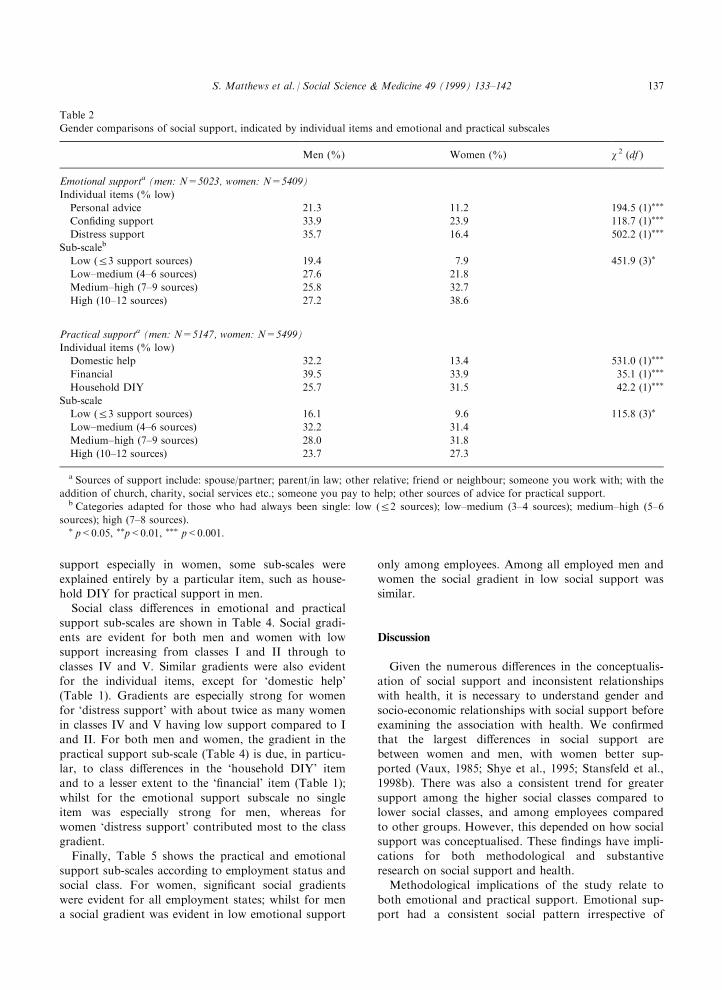
Table 2 shows that men and women di�er signi®-
cantly ( p<0.05) in their perceived levels of social sup-port: 19.4% of men compared to 7.9% of womenreported low levels of emotional support, and 16.1%
of men and 9.6% of women reported low levels ofpractical support. At the other extreme, fewer men(27.2%) than women (38.6%) reported high emotional
support, whilst the di�erence narrowed for practicalsupport (23.7% men, 27.3% women). Signi®cant gen-der di�erences ( p<0.05) bene®ting women wereapparent for all support questions except for `house-
hold DIY' where men received more practical support
than women Table 2. There were particularly pro-
nounced gender di�erences for `distress support' and`domestic help' with over twice as many men reportinglow support. Overall, men and women were well sup-
ported for `personal advice' (21.3% and 11.2% menand women respectively reporting low support) and forwomen `domestic help' (with 13.4% reporting low sup-
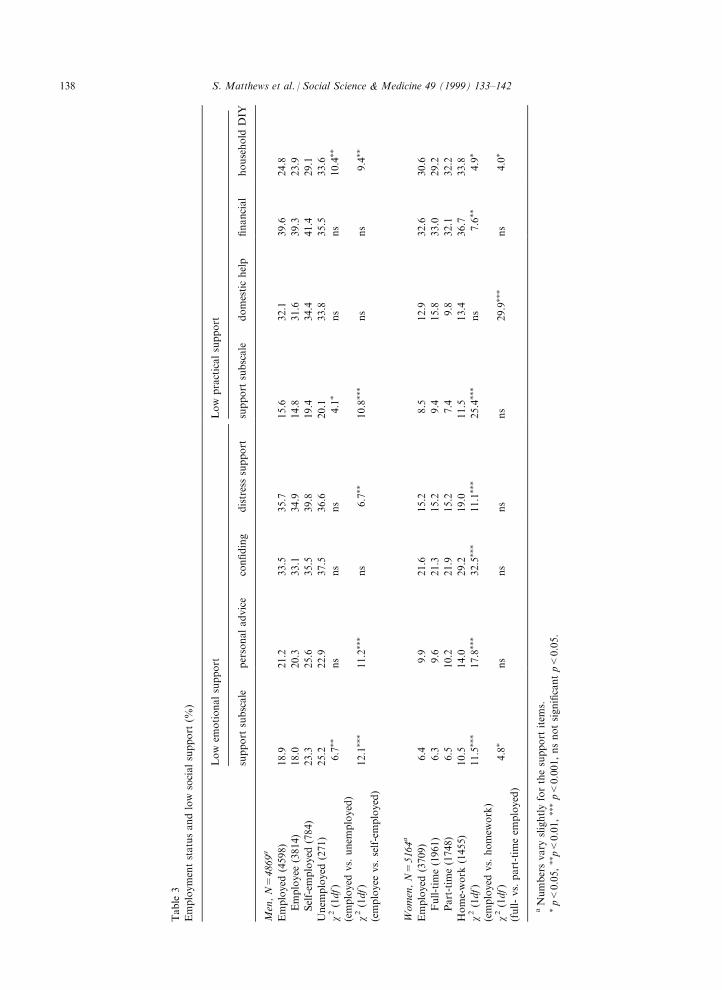
port).Table 3 shows that of the 4869 men, 271 (6%) were
unemployed, 784 (16%) were self-employed, with themajority 3814 (78%) working as employees. For
women, 1455 (28%) were home-workers, 1748 (34%)were employed part-time, and 1961 (38%) were full-time employed. Most di�erences in social support
between employment states were small, though statisti-cally signi®cant. Overall, employed women were bettersupported than home-workers. Part- and full-time
women workers had similar levels of low emotionalsupport, whilst marginally more full-time employedwomen reported low levels of practical support. For
men, the employed as compared to the unemployed,and employees as compared to the self-employed, hadbetter emotional and practical support. While the gen-eral trends for the sub-scales were evident for some in-
dividual items (Table 3), for example emotional
Table 1
Social class at age 33 and social support items (percent with low support)
No. support sources Social class at age 33
mena womenb
I & II
(1942)
IIInm
(521)
IIIm
(1552)
IV & V
(734)
w 2 trend
(1df )
I & II
(1641)
IIInm
(1823)
IIIm
(363)
IV & V
(1150)
w 2 trend
(1df )
Emotional supportc
Personal advice 5 18.3 20.9 22.3 24.7 17.3�� 9.7 11.1 11.6 12.1 4.0�
8 17.1 20.0 22.6 23.6 21.3��� 9.1 10.6 11.6 11.6 4.7�
Con®ding support 5 31.0 31.2 36.8 37.2 14.4�� 19.9 24.4 23.6 25.8 11.7���
8 27.9 31.0 35.5 36.0 24.9��� 17.0 22.9 22.8 24.1 18.4���
Distress support 5 31.2 34.8 39.7 39.9 30.1��� 10.4 16.8 19.8 20.7 54.3���
8 30.0 33.9 39.1 39.0 33.5��� 9.7 15.8 19.3 19.6 54.0���
Practical supportc
Domestic help 5 31.8 29.4 34.2 33.9 2.6 13.2 13.2 16.1 14.3 1.4
8 31.0 29.4 33.9 33.4 3.4 12.3 12.8 15.5 14.1 2.6
Financial 5 62.9 62.9 59.8 58.6 1.7 53.4 55.3 54.8 54.1 0.1
8 36.1 36.1 36.1 44.1 23.6��� 28.9 34.0 37.5 37.5 23.3���
Household DIY 5 22.4 22.4 24.9 35.2 48.1��� 28.2 33.6 31.6 37.8 24.2���
8 20.9 20.9 23.6 34.8 57.9��� 25.7 31.9 30.2 37.1 36.8���
a Sample for men varies for each variable ranging from 4198 to 4754, with those reporting low support ranging from 961 to 1640
(emotional), and 1214 to 2909 (practical).b Sample for women varies for each variable ranging from 4827 to 4991, with those reporting low support ranging from 542 to
1118 (emotional), and 655 to 2663 (practical).c Low support=1 or less sources of social support.� p<0.05, ��p<0.01, ���p<0.001.
S. Matthews et al. / Social Science & Medicine 49 (1999) 133±142136
support especially in women, some sub-scales wereexplained entirely by a particular item, such as house-hold DIY for practical support in men.
Social class di�erences in emotional and practicalsupport sub-scales are shown in Table 4. Social gradi-ents are evident for both men and women with lowsupport increasing from classes I and II through to
classes IV and V. Similar gradients were also evidentfor the individual items, except for `domestic help'(Table 1). Gradients are especially strong for women
for `distress support' with about twice as many womenin classes IV and V having low support compared to Iand II. For both men and women, the gradient in the
practical support sub-scale (Table 4) is due, in particu-lar, to class di�erences in the `household DIY' itemand to a lesser extent to the `®nancial' item (Table 1);
whilst for the emotional support subscale no singleitem was especially strong for men, whereas forwomen `distress support' contributed most to the classgradient.
Finally, Table 5 shows the practical and emotionalsupport sub-scales according to employment status andsocial class. For women, signi®cant social gradients
were evident for all employment states; whilst for mena social gradient was evident in low emotional support
only among employees. Among all employed men andwomen the social gradient in low social support wassimilar.
Discussion
Given the numerous di�erences in the conceptualis-ation of social support and inconsistent relationshipswith health, it is necessary to understand gender and
socio-economic relationships with social support beforeexamining the association with health. We con®rmedthat the largest di�erences in social support are
between women and men, with women better sup-ported (Vaux, 1985; Shye et al., 1995; Stansfeld et al.,1998b). There was also a consistent trend for greater
support among the higher social classes compared tolower social classes, and among employees comparedto other groups. However, this depended on how socialsupport was conceptualised. These ®ndings have impli-
cations for both methodological and substantiveresearch on social support and health.Methodological implications of the study relate to
both emotional and practical support. Emotional sup-port had a consistent social pattern irrespective of
Table 2
Gender comparisons of social support, indicated by individual items and emotional and practical subscales
Men (%) Women (%) w 2 (df )
Emotional supporta (men: N=5023, women: N=5409)
Individual items (% low)
Personal advice 21.3 11.2 194.5 (1)���
Con®ding support 33.9 23.9 118.7 (1)���
Distress support 35.7 16.4 502.2 (1)���
Sub-scaleb
Low (R3 support sources) 19.4 7.9 451.9 (3)�
Low±medium (4±6 sources) 27.6 21.8
Medium±high (7±9 sources) 25.8 32.7
High (10±12 sources) 27.2 38.6
Practical supporta (men: N=5147, women: N=5499)
Individual items (% low)
Domestic help 32.2 13.4 531.0 (1)���
Financial 39.5 33.9 35.1 (1)���
Household DIY 25.7 31.5 42.2 (1)���
Sub-scale
Low (R3 support sources) 16.1 9.6 115.8 (3)�
Low±medium (4±6 sources) 32.2 31.4
Medium±high (7±9 sources) 28.0 31.8
High (10±12 sources) 23.7 27.3
a Sources of support include: spouse/partner; parent/in law; other relative; friend or neighbour; someone you work with; with the
addition of church, charity, social services etc.; someone you pay to help; other sources of advice for practical support.b Categories adapted for those who had always been single: low (R2 sources); low±medium (3±4 sources); medium±high (5±6
sources); high (7±8 sources).� p<0.05, ��p<0.01, ��� p<0.001.
S. Matthews et al. / Social Science & Medicine 49 (1999) 133±142 137
Table
3
Employmentstatusandlow
socialsupport
(%)
Low
emotionalsupport
Low
practicalsupport
support
subscale
personaladvice
con®ding
distresssupport
support
subscale
domestichelp
®nancial
household
DIY
Men,N=
4869a
Employed
(4598)
18.9
21.2
33.5
35.7
15.6
32.1
39.6
24.8
Employee
(3814)
18.0
20.3
33.1
34.9
14.8
31.6
39.3
23.9
Self-em
ployed
(784)
23.3
25.6
35.5
39.8
19.4
34.4
41.4
29.1
Unem
ployed
(271)
25.2
22.9
37.5
36.6
20.1
33.8
35.5
33.6
w2(1df)
(employed
vs.unem
ployed)
6.7��
ns
ns
ns
4.1�
ns
ns
10.4��
w2(1df)
(employee
vs.self-employed)
12.1���
11.2���
ns
6.7��
10.8���
ns
ns
9.4��
Women,N=
5164a
Employed
(3709)
6.4
9.9
21.6
15.2
8.5
12.9
32.6
30.6
Full-tim
e(1961)
6.3
9.6
21.3
15.2
9.4
15.8
33.0
29.2
Part-tim
e(1748)
6.5
10.2
21.9
15.2
7.4
9.8
32.1
32.2
Home-work
(1455)
10.5
14.0
29.2
19.0
11.5
13.4
36.7
33.8
w2(1df)
(employed
vs.homew
ork)
11.5���
17.8���
32.5���
11.1���
25.4���
ns
7.6��
4.9�
w2(1df)
(full-vs.part-tim
eem
ployed)
4.8�
ns
ns
ns
ns
29.9���
ns
4.0�
aNumbersvary
slightlyforthesupport
item
s.�p<
0.05,��p<
0.01,���p<
0.001,nsnotsigni®cantp<
0.05.
S. Matthews et al. / Social Science & Medicine 49 (1999) 133±142138
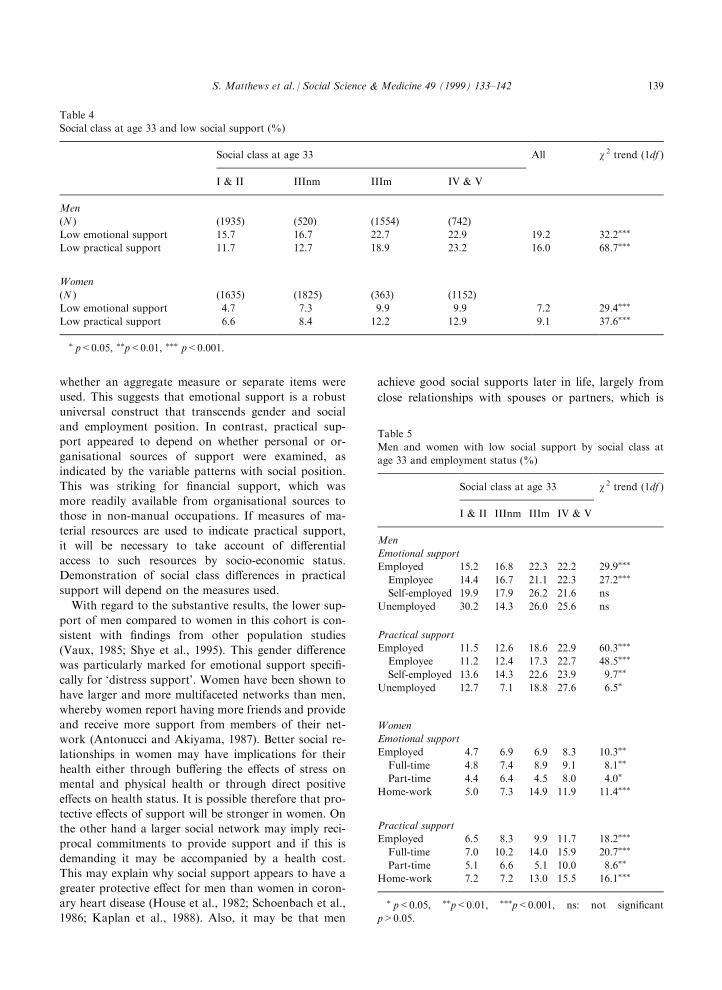
whether an aggregate measure or separate items were
used. This suggests that emotional support is a robust
universal construct that transcends gender and social
and employment position. In contrast, practical sup-
port appeared to depend on whether personal or or-
ganisational sources of support were examined, as
indicated by the variable patterns with social position.
This was striking for ®nancial support, which was
more readily available from organisational sources to
those in non-manual occupations. If measures of ma-
terial resources are used to indicate practical support,
it will be necessary to take account of di�erential
access to such resources by socio-economic status.
Demonstration of social class di�erences in practical
support will depend on the measures used.
With regard to the substantive results, the lower sup-
port of men compared to women in this cohort is con-
sistent with ®ndings from other population studies
(Vaux, 1985; Shye et al., 1995). This gender di�erence
was particularly marked for emotional support speci®-
cally for `distress support'. Women have been shown to
have larger and more multifaceted networks than men,
whereby women report having more friends and provide
and receive more support from members of their net-
work (Antonucci and Akiyama, 1987). Better social re-
lationships in women may have implications for their
health either through bu�ering the e�ects of stress on
mental and physical health or through direct positive
e�ects on health status. It is possible therefore that pro-
tective e�ects of support will be stronger in women. On
the other hand a larger social network may imply reci-
procal commitments to provide support and if this is
demanding it may be accompanied by a health cost.
This may explain why social support appears to have a
greater protective e�ect for men than women in coron-
ary heart disease (House et al., 1982; Schoenbach et al.,
1986; Kaplan et al., 1988). Also, it may be that men
achieve good social supports later in life, largely from
close relationships with spouses or partners, which is
Table 4
Social class at age 33 and low social support (%)
Social class at age 33 All w 2 trend (1df )
I & II IIInm IIIm IV & V
Men
(N ) (1935) (520) (1554) (742)
Low emotional support 15.7 16.7 22.7 22.9 19.2 32.2���
Low practical support 11.7 12.7 18.9 23.2 16.0 68.7���
Women
(N ) (1635) (1825) (363) (1152)
Low emotional support 4.7 7.3 9.9 9.9 7.2 29.4���
Low practical support 6.6 8.4 12.2 12.9 9.1 37.6���
� p<0.05, ��p<0.01, ��� p<0.001.
Table 5
Men and women with low social support by social class at
age 33 and employment status (%)
Social class at age 33 w 2 trend (1df )
I & II IIInm IIIm IV & V
Men
Emotional support
Employed 15.2 16.8 22.3 22.2 29.9���
Employee 14.4 16.7 21.1 22.3 27.2���
Self-employed 19.9 17.9 26.2 21.6 ns
Unemployed 30.2 14.3 26.0 25.6 ns
Practical support
Employed 11.5 12.6 18.6 22.9 60.3���
Employee 11.2 12.4 17.3 22.7 48.5���
Self-employed 13.6 14.3 22.6 23.9 9.7��
Unemployed 12.7 7.1 18.8 27.6 6.5�
Women
Emotional support
Employed 4.7 6.9 6.9 8.3 10.3��
Full-time 4.8 7.4 8.9 9.1 8.1��
Part-time 4.4 6.4 4.5 8.0 4.0�
Home-work 5.0 7.3 14.9 11.9 11.4���
Practical support
Employed 6.5 8.3 9.9 11.7 18.2���
Full-time 7.0 10.2 14.0 15.9 20.7���
Part-time 5.1 6.6 5.1 10.0 8.6��
Home-work 7.2 7.2 13.0 15.5 16.1���
� p<0.05, ��p<0.01, ���p<0.001, ns: not signi®cant
p>0.05.
S. Matthews et al. / Social Science & Medicine 49 (1999) 133±142 139

not necessarily the case for women, who are socialised
to develop a wider circle of support from an earlier age.This is illustrated in a middle aged cohort study, thatbetter mental health was predicted by support from the
closest person for men (Stansfeld et al., 1998b) butwomen bene®ted more from a combination of supportsources (Fuhrer et al., 1999).
Whilst there is a fairly extensive literature on genderand social support, the evidence on social support and
social position is less well documented. The data fromthe 1958 birth cohort show lower support in lowersocial classes, based on the emotional and practical
support subscales and the separate items, except for`domestic help'. As the social class trends were modest,
perceived availability of social support is unlikely toprovide a major explanation for socio-economicinequalities in health. This was demonstrated in further
analysis of the cohort, in which social support hadonly a minor impact on social class di�erences in self-rated health at age 33 for both sexes (Power et al.,
1998), although it's contribution to social class di�er-ences in other health measures has not yet been estab-
lished. Elsewhere, social support provided only amodest explanation of employment grade di�erences inpsychiatric sickness absence (Rael et al., 1995),
although it explains somewhat more of the gradient indepression among male middle aged civil servants(Stansfeld et al., 1998b). Likewise, social network
measures showed only a small e�ect in explainingsocial class gradients in mental illness in a Swedish
general population (Lundberg, 1991).Di�erences in social support by employment status
were modest. As expected, unemployed and self-
employed men and home-working women had lowerlevels of both emotional and practical support (Brownand Harris, 1978; Burke et al., 1979; Billings and
Moos, 1981; Vanfossen, 1981; Bartley, 1994;Bromberger and Matthews, 1994; Roberts et al., 1997).
This is likely to re¯ect limited social networks outsidethe household. Interestingly, di�erences in support forwomen working full- or part-time were minor. This
suggests that participation in the paid labour marketfor women is su�cient to provide opportunities forsupport regardless of the number of hours worked.
Whereas, in another investigation based on this cohort,social gradients in negative psychosocial work charac-
teristics were stronger for part-time than for full-timeworkers (Matthews et al., 1998). Women involved inpart-time employment had less opportunity for learn-
ing and greater monotony than full-time workers.Interestingly, there was no social class trend in lowemotional support among unemployed men, suggesting
that unemployment reduces the availability of socialsupport irrespective of social class background.
It is important to bear in mind that the six supportitems included in our analyses are hypothetical, aiming
to measure availability of perceived social support. Oneconsequence of the hypothetical constructs is that we
are unable to identify individuals with no support andindividual assessments of support may be in¯uenced bymood and personality. Whilst hypothetical constructs
may be important, they represent only one dimension ofsocial support. Other dimensions may prove to be morein¯uential for health, especially for men. For instance,
marital status and satisfaction, organisational member-ship including church involvement and leisure activitieshave not been considered so far in our analysis.
Furthermore, a limitation of social network measures isthat they fail to consider quality of social support. Inparticular, one person may provide much moreemotional and practical support than several more dis-
tant contacts. An issue to consider in future would bethe importance attached to each dimension of support.For instance, should each dimension of emotional sup-
port be weighted equally in deriving an aggregate vari-able? Another area to consider is that of negativeaspects of close relationships which have more of an
impact on health than positive social relations and maybe more important in contributing to social inequalitiesin health (Stansfeld et al., 1998a).
In order to advance the study of social support andhealth it will be necessary to identify more preciselywhat it is about support that is bene®cial for health.Part of this endeavour requires a better understanding
of the distribution of di�erent aspects of supportacross social groups to identify those most and least atrisk. This paper contributes to the understanding of
social support in early adulthood.
Acknowledgements
This research was supported by a grant from the(UK) Economic and Social Research Council underthe Health Variations Programme (L128251021) to
Chris Power, Sharon Matthews, Stephen Stansfeld andOrly Manor. CP (Weston Fellow) is a fellow with theCanadian Institute for Advanced Research. Data
acknowledgement: Centre for Longitudinal Studies,Institute of Education, National Child DevelopmentStudy Composite File including selected Perinatal Dataand sweeps one to ®ve (computer ®le). National
Birthday Trust Fund, National Children's Bureau,Centre for Longitudinal Studies, Institute of Education(original data producers). Colchester Essex: The Data
Archive (distributor), 21 June 1994. SN: 3148.
References
Aneshensel, C.S., Stone, J.D., 1982. Stress and depression: A
S. Matthews et al. / Social Science & Medicine 49 (1999) 133±142140
test of the bu�ering model of social support. Archives of
General Psychiatry 39, 1392±1396.
Antonucci, T.C., Akiyama, H., 1987. An examination of sex
di�erences in social support among older men and women.
Sex Roles 17 (11/12), 737±749.
Barrera, M., 1981. Social support in the adjustment of preg-
nant adolescents: assessment issues. In: Gottlieb, B.H.
(Ed.), Social Networks and Social Support. Sage
Publications, Beverley Hills, CA, pp. 69±96.
Bartley, M., 1994. Unemployment and ill health: understand-
ing the relationship. Journal of Epidemiology and
Community Health 48, 333±337.
Berkman, L.F., 1984. Assessing the physical health e�ects of
social networks and social support. Annual Review of
Public Health 5, 413±432.
Berkman, L., Breslow, L., 1983. Health and Ways of Living.
The Alameda County Study. Oxford University Press,
New York.
Billings, A.G., Moos, R.H., 1981. The role of coping re-
sponses and social resources in attenuating the stress of
life events. Journal of Behavioural Medicine 4 (2), 139±
157.
Blazer, D., 1982. Social support and mortality in an elderly
community population. American Journal of
Epidemiology 115, 684±694.
Broadhead, W.E., Kaplan, B.H., James, B.H., Wagner, E.H.,
Schoenbach, V.J., Grimson, R., Heydon, S., Tibblin, G.,
Gehlbach, S.H., 1983. The epidemiologic evidence for a re-
lationship between social support and health. American
Journal of Epidemiology 117 (5), 521±537.
Bromberger, J.T., Matthews, K.A., 1994. Employment status
and depressive symptoms in middle-aged women: a longi-
tudinal investigation. American Journal of Public Health
84 (2), 202±206.
Brown, G.W., Harris, T.O., 1978. Social Origins of
Depression: A Study of Psychiatric Disorder in Women.
Tavistock, London.
Brown, G.W., Andrews, B., Harris, T., Adler, Z., Bridge, L.,
1986. Social support, self esteem and depression.
Psychological Medicine 16, 813±831.
Brugha, T.S., Bebbington, P.E., MacCarthy, B., Sturt, E.,
Wykes, T., Potter, J., 1990. Gender, social support and
recovery from depressive disorders: a prospective clinical
study. Psychological Medicine 20, 147±156.
Burke, R.J., Weir, T., DuWors, R.E., 1979. Type A behaviour
of administrators and wives' reports of material satisfac-
tion and well being. Journal of Applied Psychology 64 (1),
57±65.
Ferri, E., 1993. Life at 33: the Fifth Follow-up of the
National Child Development Study. National Children's
Bureau, London.
Finch, J., 1989. Kinship and friendship. In: Jowell, R.,
Witherspoon, S., Brook, L. (Eds.), British Social
Attitudes: Special International Report. Gower Publishing,
Aldershot, pp. 87±103.
Fischer, C.S., 1982. To Dwell Among Friends. University of
Chicago Press, Chicago.
Fitzpatrick, R., Newman, S., Lamb, R., Shipley, M., 1988.
Social relationships and psychological well-being in rheu-
matoid arthritis. Social Science & Medicine 27 (4), 399±
403.
Fitzpatrick, R., Newman, S., Archer, R., Shipley, M., 1991.
Social support disability and depression: a longitudinal
study of rheumatoid arthritis. Social Science & Medicine
33 (5), 605±611.
Fuhrer, R., Stansfeld, S.A., Hudry-Chemali, J., Shipley, M.J.,
1999. Gender, social relations and mental health: prospec-
tive ®ndings from an occupational cohort (Whitehall II
Study). Social Science & Medicine 48 (1), 77±87.
Fuller, S.S., Larson, S.B., 1980. Life events, emotional sup-
port, and health of older people. Research in Nursing and
Health 3, 81±89.
Fusilier, M.R., Ganster, D.C., Mayes, B.T., 1986. The
social support and health relationship ± Is there a gender
di�erence. Journal of Occupational Psychology 59, 145±
153.
Ho�man, S., Hatch, M.C., 1996. Stress, social support and
pregnancy outcome: a reassessment based on recent
research. Paediatric and Perinatal Epidemiology 10, 380±
405.
House, J.S., 1981. Work Stress and Social Support. Addison
Wesley, Reading, MA.
House, J.S., Robbins, C., Metzner, H., 1982. The association
of social relationships and activities with mortality:
Prospective evidence from the Tecumseh Community
health study. American Journal of Epidemiology 116, 123±
140.
Kaplan, R.M., Hartwell, S.L., 1987. Di�erential e�ects of
social support and social network on physiological and
social outcomes in men and women with type II diabetes
mellitus. Health Psychology 6 (5), 387±398.
Kaplan, B.H., Cassel, J.C., Gore, S., 1977. Social support and
health. Medical Care 15, 47±58.
Kaplan, G.A., Salonen, J.T., Cohen, R.D., Brand, R.J.,
Syme, S.L., Puska, P., 1988. Social connections and mor-
tality from all causes and from cardiovascular disease: pro-
spective evidence from eastern Finland. American Journal
of Epidemiology 128 (2), 370±380.
Kawachi, I., Colditz, G.A., Ascherio, A., Rimm, E.B.,
Giovannucci, E., Stampfer, M.J., Willett, W.C., 1996. A
prospective study of social networks in relation to total
mortality and cardiovascular disease in men in the USA.
Journal of Epidemiology and Community Health 50, 245±
251.
Kearns, R., Neuwelt, P.M., Hitchman, B., Lennan, M., 1997.
Social support and psychological distress before and after
childbirth. Health and Social Care in the Community 5
(5), 296±308.
Leavy, R., 1983. Social support and psychological disorder: a
review. Journal of Community Psychology 11, 3±21.
Lekander, M., Fuerst, C.J., Rotstein, S., Blomgren, H.,
Fredrikson, M., 1996. Social support and immune status
during and after chemotherapy for breast cancer. Acta
Oncologica 35 (1), 31±37.
Lundberg, O., 1991. Causal explanations for class inequality
in health ± an empirical analysis. Social Science &
Medicine 32 (4), 385±393.
Macintyre, S., Hunt, K., 1997. Socio-economic position, gen-
der and health. Journal of Health Psychology 2 (3), 315±
334.
Matthews, S., Hertzman, C., Ostry, A., Power, C., 1998.
Gender, work roles and psychosocial work characteristics
S. Matthews et al. / Social Science & Medicine 49 (1999) 133±142 141
as determinants of health. Social Science & Medicine 46
(11), 1417±1424.
Miller, P.M., Ingham, J.G., 1976. Friends, con®dants and
symptoms. Social Psychiatry 11, 51±58.
Norbeck, J.S., Peterson Tilden, V., 1983. Life stress, social
support, and emotional disequilibrium in complications of
pregnancy: a prospective, multivariate study. Journal of
Health and Social Behavior 24, 30±46.
Oakley, A., Hickey, D., Rigby, A.S., 1994a. Love or money?
Social support, class inequality and the health of women
and children. European Journal of Public Health 4, 265±
273.
Oakley, A., Rigby, A.S., Hickey, D., 1994b. Life stress, sup-
port and class inequality: Explaining the health of women
and children. European Journal of Public Health 4, 81±91.
Orth-Gomer, K., Johnson, J.V., 1987. Social network inter-
action and mortality. Journal of Chronic Disease 40 (10),
949±957.
Power, C., Matthews, S., Manor, O., 1998. Inequalities in
self-rated health: explanations from di�erent stages of life.
Lancet 351, 1009±1014.
Rael, E.G.S., Stansfeld, S.A., Shipley, M., Head, J., Feeney,
A., Marmot, M., 1995. Sickness absence in the Whitehall
II study, London: the role of social support and material
problems. Journal of Epidemiology and Community
Health 49, 474±481.
Roberts, H., Pearson, J.C.G., Madeley, R.J., Hanford, S.,
Magowan, R., 1997. Unemployment and health: the qual-
ity of social support among residents in the Trent region
of England. Journal of Epidemiology and Community
Health 51, 41±45.
Rodgers, B., 1994. Pathways between parental divorce and
adult depression. Journal of Child Psychology and
Psychiatry and Allied Disciplines 35 (7), 1289±1308.
Rogers, M.M., Peoples-Sheps, M.D., Suchindran, C., 1996.
Impact of a social support program on teenage prenatal
care use and pregnancy outcomes. Journal of Adolescent
Health 19, 132±140.
Sarason, B.R., Sarason, I.G., Pierce, G.R., 1990. Traditional
views of social support and their impact on assessment. In:
Sarason, B.R., Sarason, I.G., Pierce, G.R. (Eds.), Social
Support: An Interactional View. John Wiley and Sons,
New York, pp. 9±25.
Schaefer, C., Coyne, J.C., Lazarus, R.S., 1981. The health-re-
lated functions of social support. Journal of Behavioural
Medicine 4 (4), 381±406.
Schoenbach, V.J., Kaplan, B.H., Fredman, L., Kleinbaum,
D.G., 1986. Social ties and mortality in Evans county
Georgia. American Journal of Epidemiology 123 (4), 577±
591.
Seeman, M., Seeman, T., Sayles, M., 1985. Social networks
and health status: A longitudinal analysis. Social
Psychology Quarterly 48 (3), 237±248.
Shye, D., Mullooly, J.P., Freeborn, D.K., Pope, C.R., 1995.
Gender di�erences in the relationship between social net-
work support and mortality: A longitudinal study of an
elderly cohort. Social Science & Medicine 41 (7), 935±947.
Stansfeld, S., Marmot, M., 1992. Deriving a survey measure
of social support: The reliability and validity of the close
persons questionnaire. Social Science & Medicine 35 (8),
1027±1035.
Stansfeld, S.A., Fuhrer, R., Shipley, M., 1998a. Types of
social support as predictors of psychiatric morbidity in a
cohort of British civil servants (Whitehall II Study).
Psychological Medicine 28, 881±892.
Stansfeld, S.A., Rael, E.G.S., Head, J., Shipley, M., Marmot,
M., 1998b. Social support and psychiatric sickness
absence: a prospective study of British civil servants.
Psychological Medicine 27, 35±48.
Stephens, C., Long, N., 1997. The impact of trauma and
social support on post traumatic stress disorder: A study
of New Zealand police o�cers. Journal of Criminal Justice
25 (4), 303±314.
Thoits, P., 1982. Conceptual, methodological and theoretical
problems in studying social support as a bu�er against life
stress. Journal of Health and Social Behaviour 23, 145±
159.
Tiller, J.M., Sloane, G., Schmidt, U., Troop, N., Power, M.,
Treasure, J.L., 1997. Social support in patients with anor-
exia nervosa and bulimia nervosa. International Journal of
Eating Disorders 21 (1), 31±38.
Turner, R.J., Marino, F., 1994. Social support and social
structure: a descriptive epidemiology. Journal of Health
and Social Behavior 35 (3), 193±212.
Turner, R.J., Grindsta�, C.F., Phillips, N., 1990. Social sup-
port and outcome in teenage pregnancy. Journal of Health
and Social Behavior 31, 43±57.
Vanfossen, B.E., 1981. Sex di�erences in the mental health
e�ects of spouse support and equity. Journal of Health
and Social Behaviour 22 (2), 130±143.
Vaux, A., 1985. Variations in social support associated with
gender, ethnicity and age. Journal of Social Issues 41 (1),
89±110.
Welin, L., Svardsudd, K., Ander-Peciva, S., Tibblin, G.,
Tibblin, B., Larsson, B., Wilhelmsen, L., 1985. Prospective
study of social in¯uences on mortality. Lancet 20 April,
915±918.
Wellman, B., 1981. Applying network analyses to the study of
support. In: Gottlieb, B.H. (Ed.), Social Networks and
Social Support. Sage, Beverley Hills, pp. 171±200.
S. Matthews et al. / Social Science & Medicine 49 (1999) 133±142142