socm physical exam of the neurological system pfn: sompyl0m
TRANSCRIPT

1
Slide 1JSOMTC, SWMG(A)
SOCMPhysical Exam of the Neurological
SystemPFN: SOMPYL0M
Hours: 2.0
Slide 2JSOMTC, SWMG(A)
Terminal Learning Objective Action: Communicate knowledge of “Physical Exam of the Neurological System”
Condition: Given a lecture in a classroom environment
Standard: Received a minimum score of 75% IAW course standards on the formative quizzes and the Physical Exam Practical Test grade sheet
Slide 3JSOMTC, SWMG(A)
References
Bates’ Guide to Physical Examination And History Taking (11th edition; 2013; Lynn S. Bickley)

2
Slide 4JSOMTC, SWMG(A)
Reason
As a SOCM Medic/Corpsman, your ability to conduct a good neurologic exam will affect your ability to diagnose and disposition (organize a treatment plan for) your teammates with head, dive, blast, or other high‐impact injuries.
Slide 5JSOMTC, SWMG(A)
Agenda
Identify the physical exam techniques and common findings when assessing mental status
Identify the physical exam techniques and common findings when assessing cranial nerves
Identify the physical exam techniques and common findings when assessing cerebellar and motor system functions
Slide 6JSOMTC, SWMG(A)
Agenda
Identify the physical exam techniques and common findings when assessing sensation
Identify the physical exam techniques and common findings when assessing deep tendon reflexes and the Babinski reflex
Communicate the neurologic evaluation of the stuporous or comatose patient

3
Slide 7JSOMTC, SWMG(A)
Physical Exam Techniques and Common Findings when Assessing
Mental Status
Slide 8JSOMTC, SWMG(A)
Important Areas of Examination
Mental status
Cranial Nerves I through XII
Cerebellar system/Motor
Sensory system
Deep tendon, abdominal, and plantar reflexes
Slide 9JSOMTC, SWMG(A)
Nervous System
During the Exam, Solve Three Questions
Is the mental status intact?
Are the right and left finding symmetric?
If not, is the problem in the central or peripheral nervous system?

4
Slide 10JSOMTC, SWMG(A)
Common or Concerning Symptoms
Headache
Dizziness or vertigo
Generalized, proximal, or distal weakness
Numbness
Loss of consciousness
Seizures
Tremors or involuntary movements
Slide 11JSOMTC, SWMG(A)
Neurologic Examination
Mental Status
Appearance and behavior
Speech and language
Mood
Thoughts and perceptions
Cognitive function
Slide 12JSOMTC, SWMG(A)
Cognitive Function
Ability to make new memories ‐ Ball, diamond, and tree
Math ‐ Serial sevens
Ask to recall the 3 objects
Language – Recognize a written word, spell it backwards without looking
Abstract thought – “people that live in glass
houses shouldn’t throw stones”

5
Slide 13JSOMTC, SWMG(A)
Loss of Consciousness
Get a complete description
Warning signs?
What position was the patient in?
How long did it last?
Could voices be heard?
How rapidly did they recover?
Did anyone else observe the event?
Slide 14JSOMTC, SWMG(A)
Headache
Ask about severity, location, and duration
Ask about any associated symptoms
Visual changes
Weakness
Loss of sensation
Is headache affected by coughing, sneezing, or sudden movements?
Slide 15JSOMTC, SWMG(A)
Dizziness or Vertigo
Need to elicit what the patient is experiencing
Are there any associated symptoms
Diplopia (double vision)
Dysarthria (difficulty forming words)
Ataxia (difficulty with balance)
6
Slide 16JSOMTC, SWMG(A)
Stroke and TIA
Stroke – sudden neurologic deficit
Cerebrovascularischemia ( 80‐85%)
Hemorrhagic (10‐15%)
Transient Ischemic Attack (TIA) – similar to a stroke but lasting between 1 – 24hrs with no structural defects
Slide 17JSOMTC, SWMG(A)
Stroke and TIA
Most Common Signs
Sudden numbness or weakness
Sudden confusion, trouble speaking or understanding
Sudden trouble walking, dizziness, or loss of balance
Sudden trouble seeing in one or both eyes
Sudden severe headache
Slide 18JSOMTC, SWMG(A)
Stroke and TIA
Cincinnati Stroke Scale
Facial Droop
•Normal: Both sides of face move equally
• Abnormal: One side of face does not move at all
Arm Drift
• Normal: Both arms move equally or not at all
• Abnormal: One arm drifts compared to the other
Speech
•Normal: Patient uses correct words with no slurring
• Abnormal: Slurred or inappropriate words or mute

7
Slide 19JSOMTC, SWMG(A)
Stroke Risk Factors
Primary prevention targets “modifiable risk factors”
Hypertension
Smoking
Hyperlipidemia
Diabetes
Excess weight
Lack of exercise
Heavy alcohol use
Slide 20JSOMTC, SWMG(A)
Physical Exam Techniques and Common Findings when Assessing
Cranial Nerves
Slide 21JSOMTC, SWMG(A)
Neurologic Examination
Cranial Nerve I –Olfactory – Sense of Smell
Patient should close both eyes
Occlude one nostril
Present a familiar non‐noxious odor; e.g., coffee
Ask patient to identify
Test other nostril

8
Slide 22JSOMTC, SWMG(A)
Neurologic Examination
Cranial Nerve II – Optic ‐ Vision
Test visual acuity (Snellen Chart)
Test visual fields
Inspect optic fundi
Slide 23JSOMTC, SWMG(A)
Neurologic Examination
Cranial Nerve II and III –Optic and Oculomotor
Inspect the size and shape of the pupils
Reactions to light
Convergence
Accommodation
Slide 24JSOMTC, SWMG(A)
Neurologic Examination
CN III – Oculomotor – innervates superior rectus, inferior oblique, medial rectus, and inferior rectus
CN IV – Trochlear – innervates superior oblique
CN VI – Abducens – innervates lateral rectus

9
Slide 25JSOMTC, SWMG(A)
Neurologic Examination
Cranial nerves III, IV, and VI – Oculomotor, Trochlear, and Abducens
Test extraocular movements – LR6, SO4, R3
Identify nystagmus (involuntary jerking movement)
Look for ptosis (drooping of the upper eyelids) CNIII lesion
Slide 26JSOMTC, SWMG(A)
Neurologic Examination
Cranial Nerve V – Trigeminal
Motor ‐ Palpating the temporal and massetermuscles, note the strength of muscle contraction
Sensory – Forehead, cheeks, and chin
• Pain sensation – Sharp/dull
• Temperature sensation – Hot/cold
• Light touch – Cotton wisp
Corneal Reflex –Touch cornea with a fine wisp of cotton (Have patient remove contact lenses)
Slide 27JSOMTC, SWMG(A)
Neurologic Examination
Cranial Nerve VII – Facial expression
Note any asymmetry or abnormal movements
Ask patient to
• Raise both eyebrows
• Frown
• Close both eyes tightly (test strength by trying to open them)
• Show upper and lower teeth
• Smile

10
Slide 28JSOMTC, SWMG(A)
Neurologic Examination
Cranial Nerve VIII – Vestibulocochlear ‐Hearing
Use whispered voice to assess hearing. If there is a deficit, determine if damage is:
• Conductive (air through ear)
• Sensorineural (damage to cochlear branch)
Weber test (lateralization)
Rhinne test (air and bone conduction)
Slide 29JSOMTC, SWMG(A)
Neurologic Examination
Cranial Nerves IX and X – Glossopharyngeal and Vagus
Listen to the patient’s voice
Ask about difficulty swallowing
Have patient say “Ahhh”
•Movements of the soft palate and pharynx should be symmetrical
Slide 30JSOMTC, SWMG(A)
Neurologic Examination
Cranial Nerve XI –Spinal Accessory
Look for muscular atrophy or fasciculation's
Ask patient to shrug shoulder against resistance
Turn head against resistance

11
Slide 31JSOMTC, SWMG(A)
Meningeal Signs
Important if you suspect meningeal inflammation or subarachnoid hemorrhage
Slide 32JSOMTC, SWMG(A)
Neck Mobility
Make sure there is no c‐spine injury
Ask the patient to touch their chin to their chest
If they can’t, place your hands behind their head and flex their neck forward
If this causes pain, consider it a Positive Meningeal sign
Slide 33JSOMTC, SWMG(A)
Meningeal Signs
Brudzinski’s Sign
Flex the neck forward
A normal reaction is to remain relaxed
Watch for the hips and knees to flex
Kernig’s Sign
Flex the legs then straighten the knee
This should not produce pain

12
Slide 34JSOMTC, SWMG(A)
Neurologic Examination
Cranial Nerve XII – Hypoglossal
Listen to how well the patient speaks
Look at the patient’s tongue
• Does it lay symmetrically in lower jaw?
• Look for atrophy or fasciculations
• Stick tongue straight out and move in a circle
• Puff out cheeks
Slide 35JSOMTC, SWMG(A)
Physical Exam Techniques and Common Findings when Assessing
Cerebellar and Motor System Functions
Slide 36JSOMTC, SWMG(A)
Cerebellar/Coordination
Movement requires the nervous system to function in an integrated way
Motor system – muscle strength
Cerebellar system – rhythmic movements and steady posture
Vestibular system – balance and coordinating eye, head, and body movements
Sensory system – sense of position and proprioception

13
Slide 37JSOMTC, SWMG(A)
Cerebellar/Coordination
To test coordination
Rapid alternating movements
Point to point movements
Gait and other body movements
Standing in specific ways
Note: Patients with obvious disability should not be asked to do standing or walking tests!
Slide 38JSOMTC, SWMG(A)
Cerebellar/Coordination
Rapid alternating movements
Arms – Observe speed, rhythm, and smoothness of the movements of bothhands
Legs – Note any slowness or awkwardness
Slide 39JSOMTC, SWMG(A)
Cerebellar/Coordination
Point to point movements
Arms – Finger to nose test, observe for accuracy and smoothness of movements
Legs – Heel to shin test, note smoothness and accuracy, repeat with patient’s eyes closed

14
Slide 40JSOMTC, SWMG(A)
Cerebellar/Coordination
Gait
Walk across the room and return
Walk heel to toe
Walk on toes, then on heels
Hop in place on one foot then the other
Shallow knee bend with one leg then the other
Rise from a seated position without arm support
Slide 41JSOMTC, SWMG(A)
Cerebellar/Coordination
Stance
Romberg test
Stand feet together
Eyes closed
30 to 60 sec without support
Be ready to catch the patient
Slide 42JSOMTC, SWMG(A)
Cerebellar/Coordination
Stance
Test for Pronator drift
Have patient stand for 20‐30 sec.
Eyes closed
Arms straight out
Palms up
If the patient cannot stand allow them to sit
Tap arms down – they should return to horizontal position

15
Slide 43JSOMTC, SWMG(A)
Seizures
Sudden excessive electrical discharge in the cerebral cortex
Get a complete description
Precipitating events
Warning signs (Aura)
Age of onset
Frequency
Medications
History of head injury
Slide 44JSOMTC, SWMG(A)
Motor System
Focus on
Body position
Involuntary movements
Characteristics of the muscles (bulk, tone, and strength)
Coordination
Slide 45JSOMTC, SWMG(A)
Motor System
Body Position – Look at the patient’s position during movement and at rest
Involuntary Movements
Tremors, tics, and fasciculation's
Fibrillations: Pt will sense them, but are not visible to medic
Note their location, rate, rhythm, and quality

16
Slide 46JSOMTC, SWMG(A)
Motor System
Muscle Bulk
Inspect size and contour of muscles
Atrophy?
Bilateral
Unilateral
Proximal
Distal
Slide 47JSOMTC, SWMG(A)
Motor System
Muscle Tone
Tested by feeling the muscle’s natural resistance to passive movement
Note any variances in resistance or jerkiness during the range of motion
Slide 48JSOMTC, SWMG(A)
Motor System
Muscle Strength
Have patient actively move against your resistance or resist your movements
Not a competition
If unable to, test them against gravity, or with gravity eliminated
If unable to do that watch or feel for muscular contraction

17
Slide 49JSOMTC, SWMG(A)
Scale for Grading Muscle Strength
Muscle strength is graded on a 0 to 5 scale:
0—No muscular contraction detected
1—A barely detectable flicker or trace of contraction
2—Active movement of the body part with gravity eliminated
3—Active movement against gravity only
4—Active movement against gravity and some resistance
5—Active movement against full resistance without evident fatigue (This is normal muscle strength)
Slide 50JSOMTC, SWMG(A)
Muscle StrengthTest flexion (C5, C6 – Biceps) Test extension (C6, C7, C8 –
triceps)
Slide 51JSOMTC, SWMG(A)
Muscle Strength
Test extension at the wrist (C6, C7, C8, radial nerve )
Test grip (C7, C8, T1)

18
Slide 52JSOMTC, SWMG(A)
Muscle StrengthTest finger abduction and adduction (C8, T1, ulnar nerve)
Test opposition of the thumb (C8, T1, median nerve)
Slide 53JSOMTC, SWMG(A)
Muscle Strength
Muscle strength of the trunk
Flexion, extension, and lateral bending of the spine
Thoracic expansion and excursion during respiration
Slide 54JSOMTC, SWMG(A)
Muscle Strength
Test flexion at the hip (L2, L3, L4 – iliopsoas)
Test extension at the hips (S1‐gluteus maximus)

19
Slide 55JSOMTC, SWMG(A)
Muscle Strength
Test adduction at the hips (L2, L3, L4 –adductors)
Test abduction at the hips ( L4, L5, S1 –gluteus medius and minimus)
Slide 56JSOMTC, SWMG(A)
Muscle Strength
Test extension at the knee (L2, L3, L4 – quadriceps)
Test flexion at the knee (L4, L5, S1, S2 – hamstrings)
Slide 57JSOMTC, SWMG(A)
Muscle Strength
Test dorsiflexion at the ankle (L4, L5 – tibialis anterior)
Test plantar flexion (S1 –gastrocnemius, soleus)

20
Slide 58JSOMTC, SWMG(A)
Weakness
Paresis: incomplete paralysis
Generalized
Localized
Rapid or slow onset
What areas are involved?
Slide 59JSOMTC, SWMG(A)
Tremors
May occur with or without neurological manifestations
Ask about any body movements they seem unable to control
e.g., Parkinson’s disease
Slide 60JSOMTC, SWMG(A)
Physical Exam Techniques and Common Findings when Assessing
Sensation

21
Slide 61JSOMTC, SWMG(A)
Sensory System
Types of sensations you will be testing
Pain
Temperature
Position
Vibration
Light touch
Discrimination
Note: If gross sensations are not intact, the results of other sensation tests are unreliable
Slide 62JSOMTC, SWMG(A)
Sensory System
Patterns of testing
Compare symmetric areas
Compare proximal and distal areas
Vary the pace of testing
When you detect an abnormality, map out boundaries
Slide 63JSOMTC, SWMG(A)
Pain
Use something with a sharp and dull side
Without the patient looking, demonstrate both sharp and dull
Move along the areas asking “Is this sharp or dull?”
Do not draw blood
Never reuse on another patient

22
Slide 64JSOMTC, SWMG(A)
Temperature
Often omitted if pain reception is normal
Use one heated object and one cooled object
Similar to the pain sensation test; ask the patient to identify hot or cold
Slide 65JSOMTC, SWMG(A)
Light Touch
Touch the patient lightly
Avoid any pressure
Ask the patient to respond whenever a touch is felt
Slide 66JSOMTC, SWMG(A)
Vibration
Vibration
Use a low frequency tuning fork (128Hz)
Tap on the heel of your hand
Place on the patient’s fleshy areas (e.g., fingertips)
Ask the patient to tell you when the vibration stops
If vibration sense is impaired, move proximally and try again
23
Slide 67JSOMTC, SWMG(A)
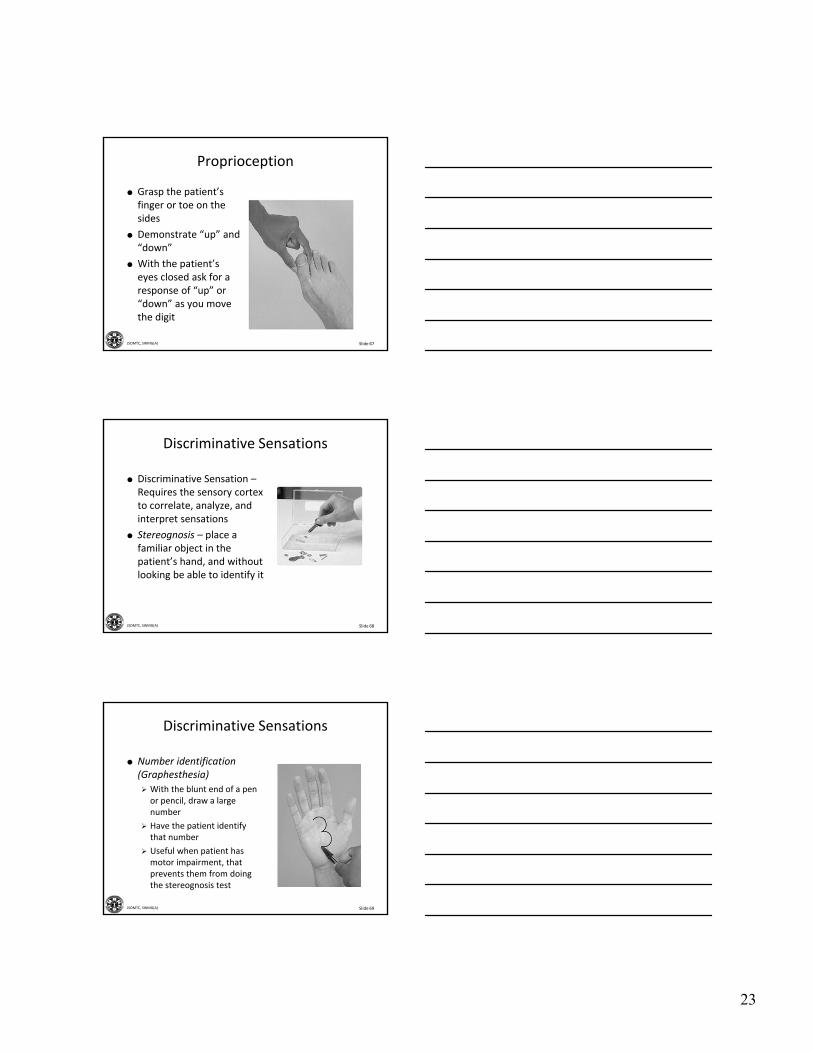
Proprioception
Grasp the patient’s finger or toe on the sides
Demonstrate “up” and “down”
With the patient’s eyes closed ask for a response of “up” or “down” as you move the digit
Slide 68JSOMTC, SWMG(A)
Discriminative Sensations
Discriminative Sensation –Requires the sensory cortex to correlate, analyze, and interpret sensations
Stereognosis – place a familiar object in the patient’s hand, and without looking be able to identify it
Slide 69JSOMTC, SWMG(A)
Discriminative Sensations
Number identification (Graphesthesia)
With the blunt end of a pen or pencil, draw a large number
Have the patient identify that number
Useful when patient has motor impairment, that prevents them from doing the stereognosis test

24
Slide 70JSOMTC, SWMG(A)
Discriminative Sensations
Two point discrimination
Use an opened paper clip
Alternate between single and double stimulus
Do not cause pain
Find minimal distance the patient can still discriminate one from two points
Slide 71JSOMTC, SWMG(A)
Discriminative Sensations
Point localization – Briefly touch the patient, then ask the patient to open their eyes and point to where they where touched
Extinction – Simultaneously touch corresponding areas on both sides of the body
Slide 72JSOMTC, SWMG(A)
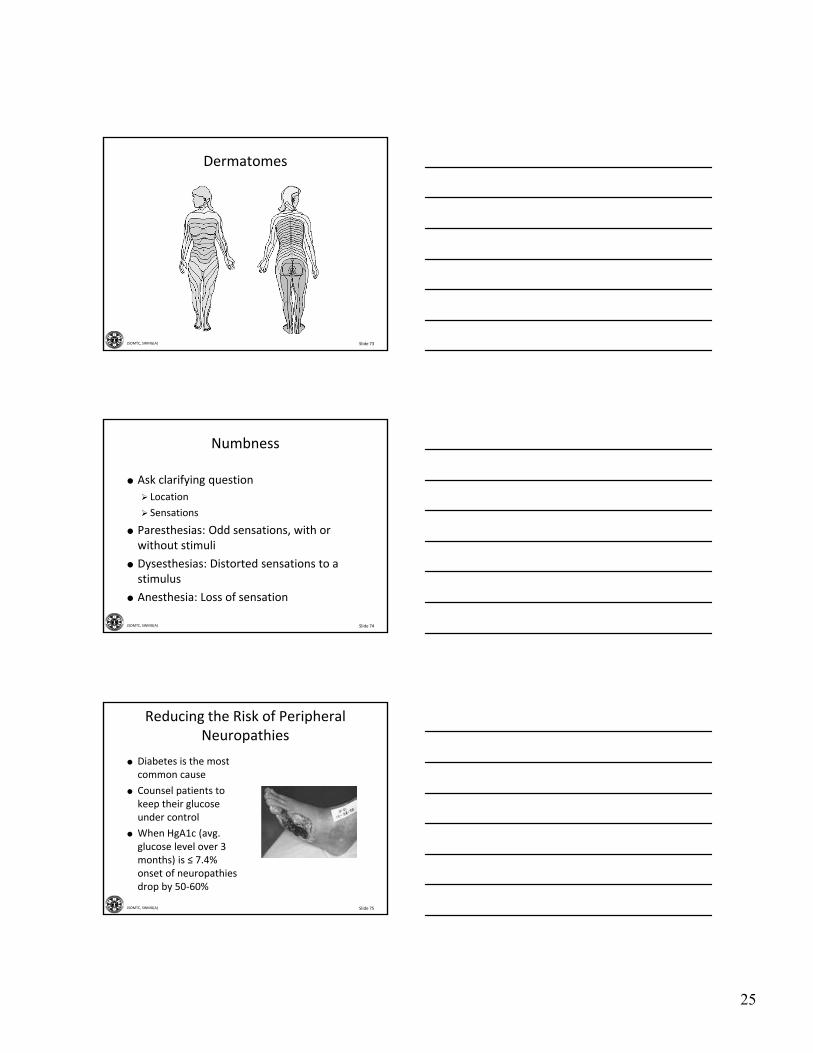
Dermatomes
A dermatome is a band of skin innervated by the sensory root of a single spinal nerve
Each spinal nerve (except C1) has a specific cutaneous sensory distribution; C1 is motor only
Do not memorize all the dermatomes
25
Slide 73JSOMTC, SWMG(A)
Dermatomes
Slide 74JSOMTC, SWMG(A)
Numbness
Ask clarifying question
Location
Sensations
Paresthesias: Odd sensations, with or without stimuli
Dysesthesias: Distorted sensations to a stimulus
Anesthesia: Loss of sensation
Slide 75JSOMTC, SWMG(A)
Reducing the Risk of Peripheral Neuropathies
Diabetes is the most common cause
Counsel patients to keep their glucose under control
When HgA1c (avg. glucose level over 3 months) is ≤ 7.4% onset of neuropathies drop by 50‐60%

26
Slide 76JSOMTC, SWMG(A)
Physical Exam Techniques and Common Findings when Assessing Deep Tendon Reflexes and the
Babinski Reflex
Slide 77JSOMTC, SWMG(A)
Deep Tendon Reflexes
Get your patient to relax
Talking to your patient distracts their mind and give you a more accurate assessment.
With your wrist relaxed, strike the tendon with a quick and direct blow
Slide 78JSOMTC, SWMG(A)
Scale for Grading Reflexes
0 ‐ No response
1+ ‐ Somewhat diminished; low normal
2+ ‐ Average; normal
3+ ‐ Brisker than average; possibly but not necessarily indicative of disease
4+ ‐ Very brisk, hyperactive, with clonus(rhythmic oscillations between flexion and extension)

27
Slide 79JSOMTC, SWMG(A)
Deep Tendon Reflexes
Biceps Reflex (C5, C6)
Patient’s arm should be partially flexed at the elbow, palm down
Place your thumb firmly over the biceps tendon
Strike your thumb so the force goes through your thumb into the biceps tendon
Slide 80JSOMTC, SWMG(A)
Deep Tendon Reflexes
Triceps Reflex (C6, C7)
Flex the patient’s arm at the elbow, palm toward the body
Strike the triceps tendon above the elbow
Use a direct blow from directly behind it
Watch for triceps contraction and elbow extension
Slide 81JSOMTC, SWMG(A)
Deep Tendon Reflexes
Supinator or brachioradialis (C5, C6)
Patient’s arm rested on abdomen or lap, forearm partially pronated
Strike the radius, 1‐2 in. above the wrist
Watch for flexion and supination of the forearm

28
Slide 82JSOMTC, SWMG(A)
Deep Tendon Reflexes
Knee Reflex (L2, L3, L4)
Patient sitting or lying down, with knee flexed
Strike the patellar tendon just below the patella
Watch for quadriceps contraction and knee extension
Slide 83JSOMTC, SWMG(A)
Deep Tendon Reflexes
Ankle Reflex (primarily S1)
Patient sitting with foot dorsiflexed
Strike the Achilles tendon
Watch for plantar flexion
Also watch for the speed of relaxation after contraction
Slide 84JSOMTC, SWMG(A)
Clonus
When reflexes seem hyperactive
Support knee in a partly flexed position
Dorsiflex and plantarflexthe foot, reminding the patient to relax
Rapidly dorsiflex the foot
Look and feel for rhythmic oscillations
29
Slide 85JSOMTC, SWMG(A)
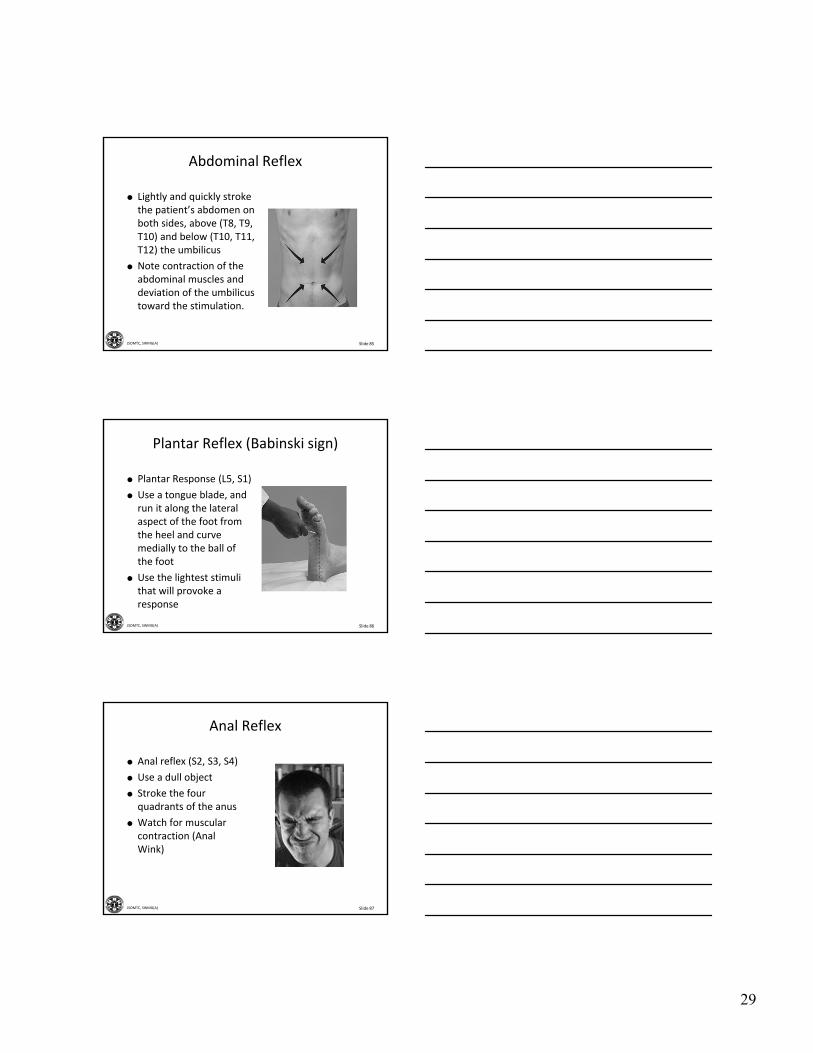
Abdominal Reflex
Lightly and quickly stroke the patient’s abdomen on both sides, above (T8, T9, T10) and below (T10, T11, T12) the umbilicus
Note contraction of the abdominal muscles and deviation of the umbilicus toward the stimulation.
Slide 86JSOMTC, SWMG(A)
Plantar Reflex (Babinski sign)
Plantar Response (L5, S1)
Use a tongue blade, and run it along the lateral aspect of the foot from the heel and curve medially to the ball of the foot
Use the lightest stimuli that will provoke a response
Slide 87JSOMTC, SWMG(A)
Anal Reflex
Anal reflex (S2, S3, S4)
Use a dull object
Stroke the four quadrants of the anus
Watch for muscular contraction (Anal Wink)
30
Slide 88JSOMTC, SWMG(A)
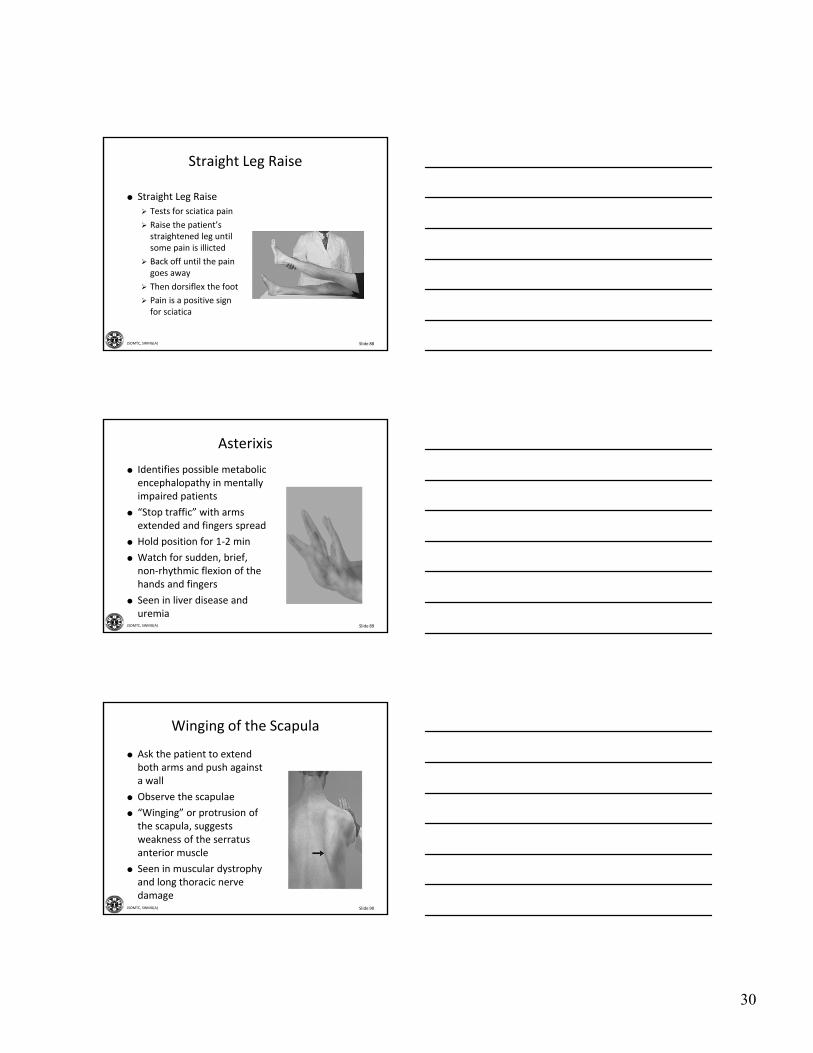
Straight Leg Raise
Straight Leg Raise
Tests for sciatica pain
Raise the patient’s straightened leg until some pain is illicted
Back off until the pain goes away
Then dorsiflex the foot
Pain is a positive sign for sciatica
Slide 89JSOMTC, SWMG(A)
Asterixis
Identifies possible metabolic encephalopathy in mentally impaired patients
“Stop traffic” with arms extended and fingers spread
Hold position for 1‐2 min
Watch for sudden, brief, non‐rhythmic flexion of the hands and fingers
Seen in liver disease and uremia
Slide 90JSOMTC, SWMG(A)
Winging of the Scapula
Ask the patient to extend both arms and push against a wall
Observe the scapulae
“Winging” or protrusion of the scapula, suggests weakness of the serratus anterior muscle
Seen in muscular dystrophy and long thoracic nerve damage

31
Slide 91JSOMTC, SWMG(A)
The Neurologic Evaluation of the Stuporous or Comatose Patient
Slide 92JSOMTC, SWMG(A)
Evaluation of the Stuporous or Comatose Patient
Coma signals a potentially life‐threatening event
First assess for life threats
Establish the patient’s level of consciousness
Examine the patient neurologically
Slide 93JSOMTC, SWMG(A)
“Don’ts” When Assessing a Comatose Patient
Don’t dilate the pupils, this takes away the single most important clue to the cause of the coma (Structural vs. Metabolic)
Don’t flex the neck, if there is any question of head or neck trauma
Immobilize the neck
Rule out any injury with an x‐ray

32
Slide 94JSOMTC, SWMG(A)
Level of Consciousness
Alert – Patient looks at you and responds appropriately
Verbal – Responds to loud voice (lethargy) or responds to a gentle shake (obtunded)
Pain – Responds to painful stimulus (stupor)
Unresponsive – no response to any stimuli (coma)
Slide 95JSOMTC, SWMG(A)
Neurologic Evaluation
Respirations ‐ Observe rate, rhythm, and pattern of respirations
Pupils – Compare size, equality, and their reaction to light
Ocular movement – Observe the position of the eyes and eyelids at rest, check for deviation of the eyes to one side
Slide 96JSOMTC, SWMG(A)
Neurologic Evaluation
Oculocephalic Reflex
This tests for brainstem function
Hold open the patient’s upper eyelids
Turn the patient’s head rapidly
If the patient’s brainstem is intact, the eyes will move to the opposite side (opposite to the movement)

33
Slide 97JSOMTC, SWMG(A)
Neurologic Evaluation
Oculovestibular reflex
Make sure tympanic membrane is intact and ear canals are clear
Elevate the patient’s head to 30°
With a large syringe through a small catheter, inject ice water into the ear canal
Watch for deviation of the eyes toward the stimuli
Slide 98JSOMTC, SWMG(A)
Posture and Muscle Tone
If no spontaneous movement, may need to apply painful stimuli
Classify the resulting pattern
Normal – Pt. withdraws or pushes away
Stereotypic – Abnormal postural response
Flaccid – No response
Slide 99JSOMTC, SWMG(A)
Reading an Radiographic Image
Follow a systematic approach
Know your anatomy
Look for asymmetry
Go from broad observations to specific detail

34
Slide 100JSOMTC, SWMG(A)
Reading an Radiographic Image
Slide 101JSOMTC, SWMG(A)
Three Phases of a Subdural Hematoma
Slide 102JSOMTC, SWMG(A)
Normal X‐ray of the C‐spine

35
Slide 103JSOMTC, SWMG(A)
Burst Fracture – High energy axial loading injury; majority result in neurologic deficit
Slide 104JSOMTC, SWMG(A)
Recording Your Findings
Document your findings in each of the five components of the neuro exam
Mental Status
Cranial Nerves I‐XII
Motor System
Sensory System
Deep tendon, abdominal, and plantar reflexes
Slide 105JSOMTC, SWMG(A)
Recording Your Findings
“Mental Status: Alert, relaxed, and cooperative. Thought process coherent. Oriented to person, place, and time. Cranial Nerves: I—not tested; II through XII intact. Motor: Good muscle bulk and tone. Strength 5/5 throughout. Cerebellar—Rapid alternating movements (RAMs), finger‐to‐nose (F→N), heel‐to‐shin (H→S) intact. Gait with normal base. Romberg—maintains balance with eyes closed. No pronator drift. Sensory: Pinprick, light touch, position, and vibration intact. Reflexes: 2+ and symmetric with normal plantar reflexes.”

36
Slide 106JSOMTC, SWMG(A)
Questions?
Slide 107JSOMTC, SWMG(A)
Terminal Learning Objective
Action: Communicate knowledge of “Physical Exam of the Neurological System”
Condition: Given a lecture in a classroom environment
Standard: Received a minimum score of 75% on the written exam IAW course standards
Slide 108JSOMTC, SWMG(A)
References
Bates’ Guide to Physical Examination and History Taking, 10th ed., Lynn S. Bickley2009
Learning Radiology: Recognizing the Basics, 2nd ed., William Herring, 2012

37
Slide 109JSOMTC, SWMG(A)
Agenda
Identify the physical exam techniques and common findings when assessing mental status
Identify the physical exam techniques and common findings when assessing cranial nerves
Identify the physical exam techniques and common findings when assessing cerebellar and motor system functions
Slide 110JSOMTC, SWMG(A)
Agenda
Identify the physical exam techniques and common findings when assessing sensation
Identify the physical exam techniques and common findings when assessing deep tendon reflexes and the Babinski reflex
Communicate the neurologic evaluation of the stuporous or comatose patient
Slide 111JSOMTC, SWMG(A)
Reason
As a SOCM Medic/Corpsman, your ability to conduct a good neurologic exam will affect your ability to diagnose and disposition (organize a treatment plan for) your teammates with head, dive, blast, or other high‐impact injuries.

38
Slide 112JSOMTC, SWMG(A)
Break