special article - homepage | circulationcirc.ahajournals.org/content/33/3/474.full.pdfspecial...
TRANSCRIPT

SPECIAL ARTICLE
Interarterial Shunts in the CerebralCirculation
By JAMES F. TOOLE, M.D.
GEORGE ELGIE BROWN of the MayoClinic, one of the founders of the Coun-
cil on Circulation of the American HeartAssociation, was a physician whose particularinterest was vascular diseases, primarily thoseof the lower extremities. This lectureship wasendowed to honor his memory by helping tokeep alive the widespread interest which hekindled in the peripheral circulation. My pres-entation is the twenty-sixth in this series butthe first relating to the cerebral circulation,the most complicated vascular bed in thebody.The situation in which we find ourselves
today concerning the cerebral circulation isso reminiscent of that described for theperipheral circulation by Dr. Isaac Starr inhis introduction to the thirteenth BrownMemorial Lecture1 delivered in 1952 that Iwould like to introduce my subject by quotingit to you:
Let us recall the background under which Brownwas working in the years preceding 1928. At thetime he and I were in medical school, clinicalmedicine in the United States was dominated bvthe great pathologic school of thought whoseprimary interest was in the lesions found atnecropsy. It was under the aegis of this schoolthat the obstructive lesions of peripheral vasculardisease had been discovered and described. Asa result of such knowledge when a clinician de-tected diminution or lack of pulsation in a periph-eral vessel, he could confidently predict thatat necropsy the vessel would be found to beobstructed by something solid and tangible, by aclot perhaps, by a sclerotic lesion of the vessel's
Adapted from the Twenty-sixth George E. BrownMemorial Lecture delivered at the meeting of theAmerican Heart Association, Miami. Florida, Octo-ber 15 to 17, 1965.
walls, either alone or accompanied by a clot, orpossibly by pressure from without. This concen-tration of thought on the demonstrated arterialobstruction had led to a completely pessimistictherapeutic outlook. The vessel was obstructedand nothing could be done about it; the diseaseran its malignant course, more vessels wouldbecome involved, the part supplied would sufferincreasingly from lack of blood until eventuallygangrene was inevitable.
Since 1928, cardiology has been transformedfrom an art in which the stethoscope was theonly tool and digitalis the major therapy intoa dynamic specialty commanding the fullresources of electronics and physics, of bio-chemistry, physiology, radiology, and surgery.The tremendous advances that brought aboutthis transformation have yet to be applied, ona large scale, to the cerebral circulation andits diseases. Too many present-day physicianshave a 1928 attitude toward circulatory dis-eases of the brain, and the field continues tobe dominated to a certain extent by pathology,just as was general medicine in the 1920's.We neurologists are just now learning to usethe stethoscope, and the hemodyanics of thearteries in the thorax, neck, and head are stilla mystery to us.On the other hand, many internists have an
oversimplified concept of the aortocranialcirculation, considering it to be analogousto the coronary and peripheral vascular beds.Phrases like "cerebral angina" and "in-termittent claudication of the brain" havecrept into their vocabularies. Tempting asit is, this holistic concept is dangerous, be-cause the cerebral circulation is unique inmany ways. One of its distinctive features-interarterial shunts-is the subject of thispaper.
Cir4-ulation, Volume XXXIII, March 1966474
by guest on July 12, 2018http://circ.ahajournals.org/
Dow
nloaded from
SHUNTS IN CEREBRAL CIRCULATION
For convenience I have divided these ar-terial anastomoses into intracranial and ex-tracranial varieties, but the two do not actseparately in the body and one compensatesfor deficiencies in the other. Together theyconstitute the only means for transferring largevolumes of blood from one hemisphere orlobe of the cerebrum to another.
Intracranial ShuntsNormal shunts take place through lepto-
meningeal (surface conducting) arteries suchas the anterior, middle, and posterior cerebralarteries and their pial branches,2 3 or throughthe circle of Willis.4-6 In rare cases persistentembryonic anastomoses between the carotidand vertebral basilar systems form still anotherinterarterial shunt.7 All of these arteries andtheir anastomoses lie on the surface of thebrain where they form an interconnectingnetwork containing a pool of blood whichflows into the brain parenchyma accordingto its needs.
Systemic blood pressure is transmitted intothese arteries, and pressure differences amongbranches of the surface network equilibratewith one another. Even though mean arterialblood pressure may fluctuate widely, so longas the changes are not too abrupt total flowthrough this system remains remarkably con-stant at about 55 ml/ 100 g of tissue perminute when mean arterial pressure rangesbetween 70 and 200 mm Hg.8 Therefore,blood from this pool arrives in the capillarynetwork at constant flow and perfusion pres-sure.Most authorities attribute this remark-
able autoregulation of the cerebral cir-culation to diffuse change in the caliber ofarterioles interconnecting the surface arteriesand the capillary bed.9 A few contend that itis effected by sphincters located at the originof small arteries and large arterioles.10 What-ever its mechanism, there is ample evidencethat this autoregulatory capacity normallyresponds both to systemic stresses and toregional stimuli.
It is suspected that smaller branches ofthe surface arteries change their caliber in
Circulation, Volume XXXIII, March 1966
response to neuronal activity, but there islittle to suggest that shunting of blood fromone to another branch of the same arteryoccurs under normal conditions.1" However,this possibility has not been completely ex-cluded, because precise methods for detectingregional flow in man have not yet been de-vised.Angiograms performed on the immobilized
patient with face front show that the twocarotid arteries and the vertebral-basilar sys-tem function independently despite the richinterconnections described above. Yet changein pressure relations between the two carotidarteries, or between the vertebral-basilar andthe carotid system, causes blood to shift im-mediately into the system with the lowerpressure. Because head rotation alters flowthrough the vertebral and probably thecarotid arteries, it may reasonably be suspect-ed that the areas of intracranial distributionof these arteries vary when the head isturned. Once more, however, there have beenno investigations of this possibility.When one or both carotids are occluded
by disease, remarkable intracranial shuntscan develop to protect the brain.12-14 Oneexample is illustrated by the following case.A 49-year-old man (Hospital of the University
of Pennsylvania, case no. 20 17 81) was evaluatedfor recurrent episodes of transitory neurologicaldeficit which had begun in 1951 when he was39 years old. The first manifestation was rightfacial paralysis, and after a customary neurolog-ical evaluation he was diagnosed as having mul-tiple sclerosis. Subsequent to this he experiencedepisodic right hemiparesis, dysphasia, and dys-lexia, and in 1960 episodes of left hemiparesis atwhich time his wife began to notice intellectualdeterioration.
Over the years he had been examined by sev-eral physicians all of whom concurred in thediagnosis of multiple sclerosis.On examination in the hospital he had bilat-
eral spastic hemiparesis and hesitant speech buthe was lucid and oriented. His recall of therecent and remote past was adequate to testingeven though his wife averred that his memoryhad deteriorated. Pulsation was stronger in hisleft superficial temporal artery than in the right.Pulsations in his carotid arteries in the neck, thesubelavians, and the radial arteries seemed to beintact. He had a grade III holosystolic murmur
475
by guest on July 12, 2018http://circ.ahajournals.org/
Dow
nloaded from

TOOLE
over the region of the origin of the left vertebralartery from the subelavian. This murmur wastransmitted up the left vertebral artery.
Blood pressure in the right arm was 160/100mm Hg while that in the left was 120/90.Ophthalmic artery pressures were 60/10 g in theright eye and 20/0-10 in the left. The internalcarotid artery in the pharynx could not be pal-pated.
Because of the low ophthalmic artery pres-sures, a tentative diagnosis of bilateral carotidartery disease was made, and arteriography ofthe aortic arch and great vessels was carriedout through a retrograde femoral catheter. Thisdemonstrated occlusion of both internal carotidarteries and very large vertebral arteries whichappeared to be free of atherosclerosis. The ori-gins of the innominate, left common carotid,and left subclavian arteries appeared to be nor-mal. There was no evidence of a subclaviansteal.To delineate the intracranial ramifications of the
aortocranial arteries, percutaneous puncture ofhis common carotid arteries (figs. 1 and 2), andthe left vertebral artery were carried out (figs.3 to 5).
Drs. Christian Lambertson and Harry Wol-man performed studies of the cerebral bloodflow and cerebral oxygen consumption. The re-sults are tabulated in table 1. Strangely enough,cerebral vascular resistance was low despite thebilateral carotid occlusions and cerebral bloodflow increased remarkably in response to the
inhalation of air containing 5% carbon dioxidepossibly due to increase in systemic blood pres-sure and cerebral vasodilatation.
In addition to proving that occlusion ofextracranial portions of both carotid arteriesneed not affect the capacity for normalcerebral blood flow, this case demonstrates
Figure 2Left internal carotid artery is occluded just distal toits origin.
Arteriogram of right common and external carotidarteries. Right internal carotid is occluded just distalto its origin.
Figure 3Right vertebral artery opacified. Early phase demon-strating dilated vertebral and basilar arteries. Notethe large posterior communicating arteries.
Circulation, Volume XXXIII, March 1966
476
by guest on July 12, 2018http://circ.ahajournals.org/
Dow
nloaded from

SHUNTS IN CEREBRAL CIRCULATION
the phenomenal extent to which intracranialshunts can compensate for extracranial oc-clusive disease.We have shown that in normal men under
general anesthesia each carotid artery carriesabout 300 ml of blood per minute and the twoproximal vertebrals together carry about 100ml per minute.' '16 When one internal carotidor vertebral artery is occluded in the neck,flow through the other one immediately in-creases by more than 50%-undoubtedly be-cause of intracranial arterial shuntingthrough the channels just described. Flow alsoincreases somewhat in the vertebral systemif one carotid is occluded and vice versa.However, this potential for shunting in re-sponse to arterial occlusion depends upontwo factors: (1) the pattern of the surfacenetwork of arteries laid down within 90 daysafter conception, and (2) the vagaries ofatherosclerosis which may destroy segmentsof the anastomotic system throughout the re-mainder of one's life. Variations in the circleof Willis are known to all of us.17 If theposterior communicating arteries are con-genitally small or if they are destroyed by
Figure 4
Later phase. Leptomeningeal anastomoses of posteriorcerebral to middle cerebral arteries opacified. Pos-terior communicating arteries are not seen but anteriorand middle cerebral arteries filled through them.
Circulation, Volume XXXIII, March 1966
Figure 5Late phase vertebral arteriogram demonstrating opaci-fication of distal anterior and middle cerebralbranches from vertebral circulation.
disease, there can be no compensatory shunt-ing between carotid and vertebral basilarsystems, and blood must take a more circui-tous and probably less satisfactory routethrough the leptomeningeal system.
Extracranial-Intracranial Shunts
When the circle of Willis is incompetent,the extracranial-intracranial channels can sub-stitute to a certain degree.18 There are threeprincipal anastomotic groups:
1. External to internal carotid arteriesa. Through the orbitb. Through the remains of the rete mirab-
ile which join the meningeal arteriesof the external to the leptomeningeal(surface conducting)
2. External carotid to vertebral-basilarartery through the occipital branch ofthe external carotid
3. Subelavian-vertebral to vertebral arteriesa. Of the same side bypassing segmental
obstructionb. To the opposite side
This system develops in response to diseaseor unusual stresses. Because of a general lackof interest in these extracranial portions of
477
by guest on July 12, 2018http://circ.ahajournals.org/
Dow
nloaded from
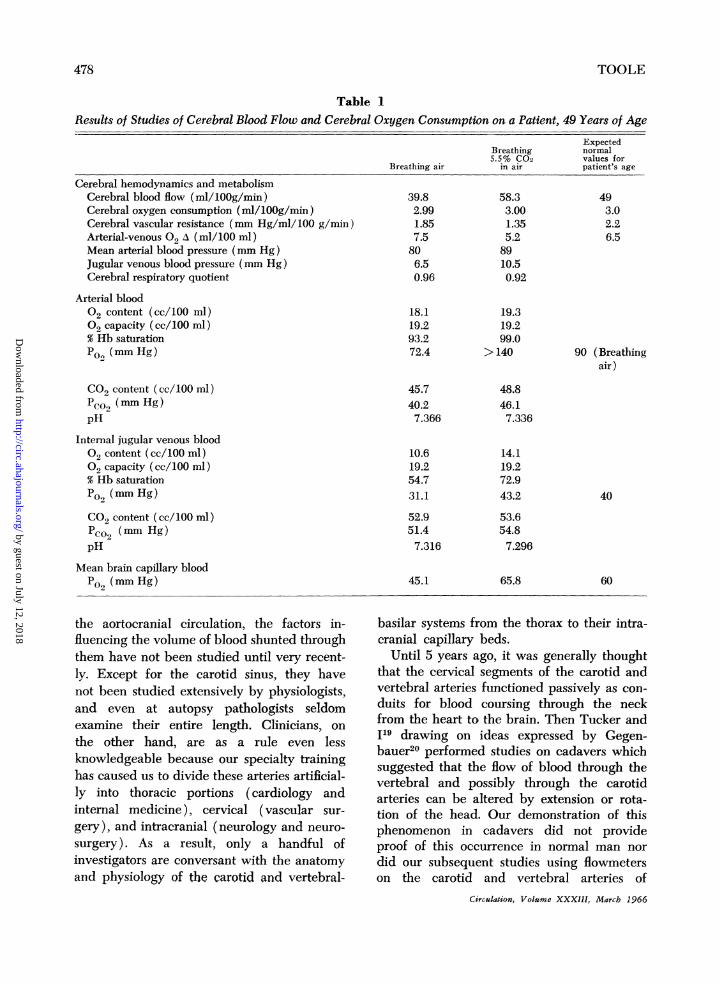
Table 1Results of Studies of Cerebral Blood Flow and Cerebral Oxygen Consumption on a Patient, 49 Years of Age
ExpectedBreathing normal5.5% C02 values for
Breathing air in air patient's age
Cerebral hemodynamics and metabolismCerebral blood flow (ml/lOOg/min)Cerebral oxygen consumption (ml/1OOg/min)Cerebral vascular resistance (mm Hg/ml/100 g/min)Arterial-venous 02 A (ml/100 ml)Mean arterial blood pressure (mm Hg)Jugular venous blood pressure (mm Hg)Cerebral respiratory quotient
Arterial blood02 content (cc/100 ml)02 capacity (cc/100 ml)% Hb saturationPo,, (mm Hg)
CO2 content (cc/100 ml)PcO0 (mm Hg)pH
Internal jugular venous blood02 content (cc/100 ml)02 capacity (cc/100 ml)% Hb saturationPO, (mm Hg)
CO2 content (cc/100 ml)Pco2 (mm Hg)pH
Mean brain capillary bloodPO, (mm Hg)
39.82.991.857.5806.50.96
18.119.293.272.4
45.740.27.366
10.619.254.731.1
52.951.47.316
45.1
58.33.001.355.28910.50.92
19.319.299.0
> 140
493.02.26.5
90 (Breathingair)
48.846.17.336
14.119.272.943.2
53.654.87.296
65.8
40
60
the aortocranial circulation, the factors in-fluencing the volume of blood shunted throughthem have not been studied until very recent-ly. Except for the carotid sinus, they havenot been studied extensively by physiologists,and even at autopsy pathologists seldomexamine their entire length. Clinicians, onthe other hand, are as a rule even lessknowledgeable because our specialty traininghas caused us to divide these arteries artificial-ly into thoracic portions (cardiology andinternal medicine), cervical (vascular sur-gery), and intracranial (neurology and neuro-surgery). As a result, only a handful ofinvestigators are conversant with the anatomyand physiology of the carotid and vertebral-
basilar systems from the thorax to their intra-cranial capillary beds.
Until 5 years ago, it was generally thoughtthat the cervical segments of the carotid andvertebral arteries functioned passively as con-duits for blood coursing through the neckfrom the heart to the brain. Then Tucker and1l9 drawing on ideas expressed by Gegen-bauer20 performed studies on cadavers whichsuggested that the flow of blood through thevertebral and possibly through the carotidarteries can be altered by extension or rota-tion of the head. Our demonstration of thisphenomenon in cadavers did not provideproof of this occurrence in normal man nordid our subsequent studies using flowmeterson the carotid and vertebral arteries of
Circulation, Volume XXXIII, March 1966
TOOLE478
by guest on July 12, 2018http://circ.ahajournals.org/
Dow
nloaded from
SHUNTS IN CEREBRAL CIRCULATION
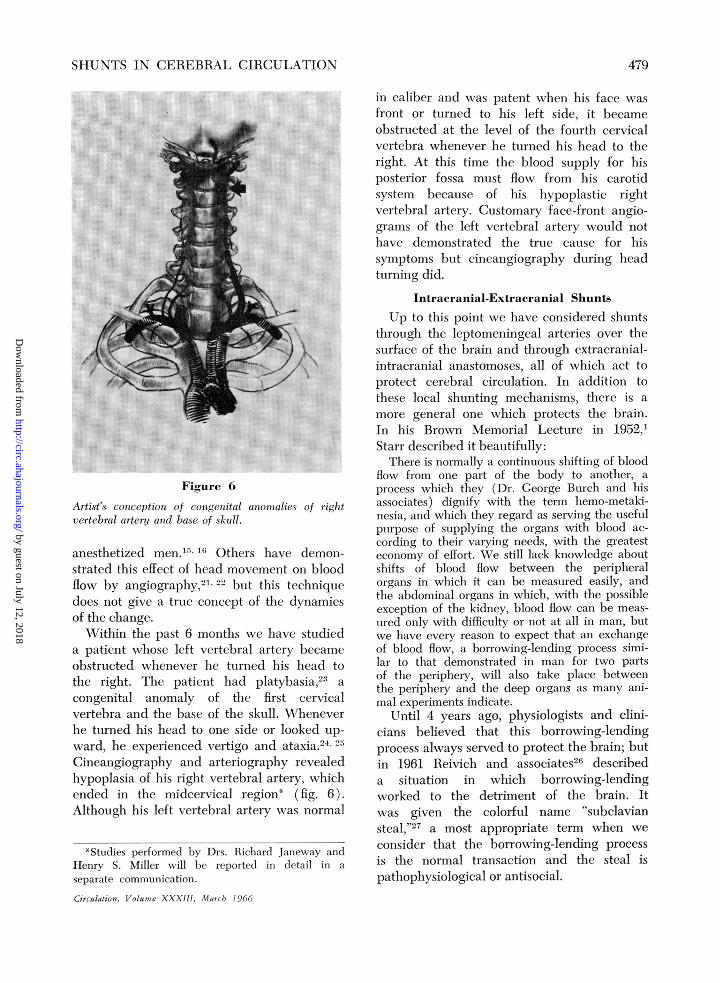
Figure 6
Artist's conception of congenital anomalies of rightvertebral artery and base of skull.
anesthetized men.15' 16 Others have demon-strated this effect of head movement on bloodflow by angiography,21'22 but this techniquedoes not give a true concept of the dynamicsof the change.Within the past 6 months we have studied
a patient whose left vertebral artery becameobstructed whenever he turned his head tothe right. The patient had platybasia,23 a
congenital anomaly of the first cervicalvertebra and the base of the skull. Wheneverhe turned his head to one side or looked up-
ward, he experienced vertigo and ataxia.24Cineangiography and arteriography revealedhypoplasia of his right vertebral artery, whichended in the midcervical region* (fig. 6).Although his left vertebral artery was normal
in caliber and was patent when his face was
front or turned to his left side, it became
obstructed at the level of the fourth cervicalvertebra whenever he turned his head to theright. At this time the blood supply for hisposterior fossa must flow from his carotidsystem because of his hypoplastic rightvertebral artery. Customary face-front angio-grams of the left vertebral artery would not
have demonstrated the true cause for hissymptoms but cineangiography during headturning did.
Intracranial-Extracranial Shunts
Up to this point we have considered shuntsthrough the leptomeningeal arteries over thesurface of the brain and through extracranial-intracranial anastomoses, all of which act to
protect cerebral circulation. In addition to
these local shunting mechanisms, there is a
more general one which protects the brain.In his Brown Memorial Lecture in 1952,Starr described it beautifully:
There is normally a continuous shifting of bloodflow from one part of the body to another, a
process which they (Dr. George Burch and hisassociates) dignify with the term hemo-metaki-nesia, and which they regard as serving the usefulpurpose of supplying the organs with blood ac-
cording to their varying needs, with the greatesteconomy of effort. We still lack knowledge aboutshifts of blood flow between the peripheralorgans in which it can be measured easily, andthe abdominal organs in which, with the possibleexception of the kidney, blood flow can be meas-
ured only with difficulty or not at all in man, butwe have every reason to expect that an exchangeof blood flow, a borrowing-lending process simi-lar to that demonstrated in man for two partsof the periphery, will also take place betweenthe periphery and the deep organs as many ani-mal experiments indicate.
Until 4 years ago, physiologists and clini-cians believed that this borrowing-lendingprocess always served to protect the brain; butin 1961 Reivich and associates26 describeda situation in which borrowing-lendingworked to the detriment of the brain. Itwas given the colorful name "subclaviansteal,"27 a most appropriate term when we
consider that the borrowing-lending processis the normal transaction and the steal ispathophysiological or antisocial.
*Studies performed by Drs. Richard Janeway andHenry S. Miller will be reported in detail in aseparate communication.
Circulation, Volume XXXIII, March 1966
479
by guest on July 12, 2018http://circ.ahajournals.org/
Dow
nloaded from

TOOLE
Subelavian steal occurs in patients whoseanatomic configuration permits a reversal offlow through one vertebral artery when theproximal portion of the subclavian artery isstenosed or occluded (fig. 7). In addition toinstances of such one-sided reversal, path-ological siphons down both vertebral arter-ies28 and also through the right carotid arteryhave been documented. Of the more than 200reported examples of this disorder, most haveresulted from atherosclerosis, but some arecongenital or caused by trauma or surgery.29Once again, it is the anatomic configuration
of the arteries laid down within the first 90days after conception that determines whethera steal can develop. If the innominate artery,for example, is extremely short or nonexistent,30so that the right subelavian and commoncarotid arteries arise independently from thearch, no caroticosubelavian shunt can develop.If the left vertebral artery arises from the archrather than from the subelavian artery, as itdoles in approximately 1% of individuals,3'obstruction in the right subelavian or the in-nominate artery can cause reversal of flow,
Figure 7Diagram of subclavian steal. Stenosis or occlusion ofsubclavian artery proximal to the origin of thevertebral may result in reversal of vertebral artery
fiow.
but occlusion of the left subelavian arterycannot.When reversal of flow does develop, the
vascular reserve of the brain determineswhether or not it produces symptoms. If thenormal intracranial shunting mechanisms pre-viously described are adequate, a pathologicalsiphon causes no symptoms. Obstruction lo-cated in the proximal subelavian artery iseasily tolerated if the opposite vertebral arteryis patent, because diversion of blood downthe vertebral artery is accompanied by in-creased cephalic flow on the other side.With increasing age, however, the deposi-
tion of atheromatous plaques in many loca-tions usually results in varying degrees ofreduction in cerebral vascular reserve. Letus consider the vertebral-basilar circulationas an example. In an adult, approximately100 ml of blood per minute normally flowsthrough the two proximal vertebral arteriesto supply muscles of the neck, portions ofthe spinal cord, the entire brain stem, thecerebellum, and portions of the temporal lobe,as well as the entire occipital lobe, of eachcerebral hemisphere. If these arteries areatherosclerotic and compressed in their fora-mina by osteoarthritic spurs, the blood flow-ing through them will be under decreasedpressure and may be decreased in volume.If, in addition, the posterior communicatingarteries are congenitally small, the alreadycompromised vertebral-basilar system is iso-lated from the carotid circulation and willbe unusually susceptible to factors (such ashypotension) which diminish cerebral bloodflow. Compensatory dilatation of the carotidbed, no matter how great, cannot preventhypovolemia and hypotension in the isolatedvertebral-basilar system.
Furthermore, the vertebral-basilar circula-tion is in competition with the vascular bedof the upper extremities for blood pressureand flow. These two beds, one cerebral andthe other musculoskeletal, are regulated in-dependently and sometimes in reverse direc-tions. When the muscular bed dilates inresponse to heat, emotional experience, andexercise of the limbs, flow to the posterior
Circulation, Volume XXXIII, March 1966
480
by guest on July 12, 2018http://circ.ahajournals.org/
Dow
nloaded from

SHUNTS IN CEREBRAL CIRCULATION
fossa is kept constant, under physiologicalconditions, by regional vasodilatation. In pa-tients with atherosclerosis, however, thisvasodilatation may not occur and factors thatincrease the flow of blood to the limbs maydecrease that to the basilar artery and itsbranches, precipitating symptoms of ischemia.Only a hint of the dynamics of this inter-
play has been provided by rapid serial angi-ography. Cineangiography, using selectivecatheter technique, once again provides amethod for seeing the dynamic situation. Therapid transit of contrast material up onevertebral artery, down the opposite artery,and out into the arm is dramatic, but less sothan situations in which proximal portionsof both subclavian arteries are stenosed. Insuch cases, the bolus traverses the carotidcirculation of the two sides, flows through theposterior communicating arteries, and passesin reverse direction down the basilar artery,down both vertebral arteries, and out into thetwo arms (fig. 8). The entire brain then be-comes dependent upon the upper limbs forits circulation. When the arms are exercised,
the volume of reversed flow increases, and if,because of disease, the cerebral arteriolescannot dilate quickly, cerebral perfusion pres-sure falls and the patient has symptoms causedby ischemia in the cerebrum, the brain stem,or both.
DiscussionIn this survey I have attempted to develop
the concept that the production of symptomsin patients with occlusive forms of cerebralvascular disease depends to a large extentupon the matrix of vessels laid down withinthe first 90 days of intra-uterine life and uponthe atheromatous material deposited in thesevessels during the next ensuing years. I haveillustrated anomalies of the aortic arch andhave shown what happens in the cerebralcirculation of a patient with a hypoplasticright vertebral artery who obstructs his leftvertebral artery by turning his head. Finally,I have mentioned the frequent variations inthe circle of Willis which can prevent cross-circulation in the cranium.
Unfortunately, there have been no studies
,, Anterior communicoting
Anterior cerebrol"I Middle cerebrol
,#' Posterior communicatingI .,
,-~Posterior cerebral
- Bosilor
, Internal ouditory
Internol corotid-
--,Left vertebralRt. common carotid--
,,Left subclovion
' STENOSIS/
'Aorta
Figure 8
Bilateral subclavian steal.
Circulation, Volume XXXIII, March 1966
Rt vertebral - - - --
Rt subclavion _
lnnominote-~./
STENOSIS /
481
by guest on July 12, 2018http://circ.ahajournals.org/
Dow
nloaded from

TOOLE
in which anomalies of the aortic arch, thecervical segments, and the circle of Willishave been considered as a unit. Hence, Imust ask you a question which I have askedmyself: Are anomalies of one area frequentlyassociated with vascular anomalies elsewhere?Since the whole circulatory system is laiddown during the same period of embryo-genesis, one might suspect that they wouldbe. If they are, do any of the teratogenicagents recognized for other organ systemsaffect the cerebral arterial system, and do weinherit our parents' vascular anatomy jtist aswe inherit their facial characteristics?
In order to consider in specific terms some ofthe multitude of factors affecting the cerebralcirculation, let us study a hypothetical case.The patient, a vigorous 65-year-old man, has
moderate atherosclerosis and diabetes. The bloodpressure in his right arm is 200/100 mm Hg,while that in his left is reduced to 140/90 be-cause of a plaque in the proximal portion of hisleft subclavian artery which causes reversed ver-tebral flow.
After a good night's sleep in a prone positionwith his head turned sharply to the left (a pos-ture which may diminish blood flow through hisright vertebral and carotid arteries), our pa-tient is awakened by his alarm clock and openshis eyes. The sudden sound and light cause anincreased flow of blood to his auditory and visualpathways.32 With customary gusto, he arises tostart the new day. Because his mild diabetes hasproduced neuropathy of the lower extremities,however, his vasomotor reflexes are lost, and thenormal borrowing-lending process does not occur;hence, blood pressure and cerebral blood flowfall somewhat when he stands Up.33 At the sametime the blood pressure difference between thetwo arms is increased, so that the volume ofreversed flow is augmented.34 The resultant reduc-tion to cerebral blood flow, superimposed on hiscerebral atherosclerosis, causes our patient tostagger and lose his vision momentarily and hedecides to sit on the bed until he recovers him-self.
After a few minutes' rest has restored hissluggish circulation, the patient walks to thebathroom and, because of mild prostatism, strainssomewhat to void. This Valsalva maneuverabruptly diminishes his cardiac output and per-haps precipitates momentary cerebral ischemia.35Recovering from this, he begins to shave withhis electric razor, massaging his carotid sinuswhile turning his head far to one side. Themassage may initiate a cardio-inhibtory or vaso-
depressor reflex, while at the same time headturning reduces flow through the vertebral andcarotid arteries.36 I dare not allow our patient todo his usual push-ups after shaving, because Ifear that the tremendous increase in reversedflow through his vertebral siphon might againproduce symptoms of vertebral-basal ischemia.37Nor will I have him take a hot shower, whichwould cause cutaneous vasodilation and initiatehemometakinesis. These stresses occurring in thefirst half hour of his day are but a few of theenormous number for which our patient's cere-bral circulation must compensate minute by min-ute during his life.Even the common situations described in
this hypothetical case are so complex that noone can master all the variables. Like theblind men describing the elephant, each ofus specialists-internist, neurologist, physiol-ogist, surgeon-describes accurately his ownsegment of this magnificently complicatedcirculatory bed. The image that each of ushas, however, is only a fragment of the whole.To map out the complete picture, we mustdo with the cerebral circulation what it is saidthat Dr. George Brown did with the periph-eral:
Recognizing his limitations in certain direc-tions, he enlisted the aid of physiologists, phys-icists, pathologists, surgeons and clinicians whocould contribute to the process of enlightenmentin the field of peripheral vascular diseases. Atthe same time while he was working as a studentand investigator of peripheral vascular dis-eases, he continued to be active as a clinicianin the broader field of Internal Medicine.38
References1. STARR, I.: Physiological considerations concerned
with the pathogenesis and treatment of ob-structive vascular disease. Circulation 6: 643,1952.
2. VANDER EECKEN, H.: Anastomoses Between theLeptomeningeal Arteries of the Brain. Spring-field, Illinois, Charles C Thomas, Publisher,1959.
3. ISHIKAWA, S., HANDA, J., MEYER, J. S., ANDHUBER, P.: Hemodynamics of the circle ofWillis and leptomeningeal anastomoses: Elec-tromagnetic flowmeter study of intracranialarterial occlusion in the monkey. J NeurolNeurosurg Psychiat 28: 124, 1965.
4. SYMONDS, C.: The circle of Willis. Brit Med J1: 119, 1955.
5. BRAIN, R.: Order and disorder in the cerebralcirculation. Lancet 2: 857, 1957.
Circulation, Volume XXXIII, March 1966
482
by guest on July 12, 2018http://circ.ahajournals.org/
Dow
nloaded from

SHUNTS IN CEREBRAL CIRCULATION
6. MCDONALD, D. A., AND POTTER, J. NI.: Distribu-tion of blood to the brain. J Physiol (London)114: 356, 1951.
7. PERRYMAN, C. R., GRAY, G. H., BRUST, R. WV.,AND CONLON, P. C.: Interesting aspects ofcerebral angiography with emphasis on some
unusual congenital variations. Amer J Roent-gen 89: 372, 1963.
8. SOKOLOFF, L., AND KETY, S. S.: Regulation ofcerebral circulation. Physiol Rev 40: 38, 1960.
9. LASSEN, N. A.: Autoregulation of the cerebralblood flow. Circulation Research 15: (suppl.1) 201, 1964.
10. ROWBOTHAM, G. F., AND LITTLE, E.: The circu-lations and reservoir of the brain. Brit J Surg50: 244, 1962.
11. MEYER, J. S., AND DENNY-BROWN, D.: The cere-
bral collateral circulation: Factors influencingcollateral blood flow. Neurology (Minneap)7: 447, 1957.
12. WIENER, L. M., BERRY, R. G., AND KUNDIN, J.:Intracranial circulation in carotid occlusion.Arch Neurol (Chicago) 11: 554, 1964.
13. ALPERS, B. J.: Compensatory mechanisms in oc-
clusive vascular disease of the brain. AMAArch Neurol (Chicago) 1: 531, 1959.
14. LOWE, R. D.: Adaptation of the circle of Willisto occlusion of the carotid or vertebral artery:Its implications in carotico-vertebral stenosis.Lancet 1: 395, 1962.
15. HARDESTY, W. H., ROBERTS, B., TOOLE, J. F.,AND ROYSTER, H. B.: Studies on carotid arteryblood flow in man. New Eng J Med 263:944, 1960.
16. HARDESTY, W. H., WHITACRE, W. B., TOOLE,J. R., RANDALL, P., AND ROYSTER, H. B.:Studies on vertebral artery blood flow in man.
Surg Gynec Obstet 116: 662, 1963.17. FISHER, C. M.: The circle of Willis: Anatomical
variations. Vascular Diseases 2: 99, 1965.18. BOSNIAK, M. A.: Cervical arterial pathways as-
sociated with brachiocephalic occlusive dis-ease. Amer J Roentgen 91: 1232, 1964.
19. TOOLE, J. F., AN-D TUCKER, S. H.: Influence ofhead position on cerebral circulation. AMAArch Neurol (Chicago) 2: 616, 1960.
20. GEGENBAUER, C.: Lehrbuch der Anatomie desMenschen, ed. 7, vol. 2. Leipzig, W. Engel-mann, 1899, p. 255.
21. SHEEHAN, S., BAUER, R. B., AND MEYER, J. S.:Vertebral artery compression in cervical spon-
dylosis: Arteriographic demonstration duringlife of the vertebral artery insufficiency due torotation and extension of the neck. Neurology(Minneap) 10: 968,1960.
22. LEWIs, R. C., AND COBURN, D. F.: The verte-bral artery: Its role in upper cervical andhead pains. Missouri Med 53: 1059, 1956.
23. SPILLANE, J. D., PALLIS, C., AND JONES, A. M.:Developmental abnormalities in the region ofthe foramen magnum. Brain 80: 11, 1957.
24. FORD, F. R.: Syncope, vertigo and disturbancesof vision resulting from intermittent obstructionof the vertebral arteries due to defect in theodontoid process and excessive mobility of thesecond cervical vertebra. Bull Hopkins Hosp91: 168, 1952.
25. COGAN, D. G., AND BARROWS, L. J.: Platybasiaand the Amold-Chiari malformation. AMAArch Ophthal (Chicago) 52: 13, 1954.
26. REIVICH, M., HOLLING, H. E., ROBERTS, B., AND
TOOLE, J. F.: Reversal of blood flow throughthe vertebral artery and its effect on cerebralcirculation. New Eng J Med 265: 878, 1961.
27. Editorial: A New Vascular Syndrome-"The Sub-clavian Steal." New Eng J Med 265: 912, 1961.
28. CODER, D. M., FRYE, R. L., BERNATZ, P. E., AND
SHEPS, S. G.: Bilateral subclavian steal. ProcMayo Clin 40: 473, 1965.
29. PATEL, A., AND TOOLE, J. F.: Subclavian stealsyndrome: Reversal of cephalic blood flow.Medicine 44: 289, 1965.
30. BOSNIAK, M. A.: Analysis of some anatomic roent-genologic aspects of the brachiocephalic ves-
sels. Amer J Roentgen 9: 1222, 1964.31. DASELER, W. H., AND ANSON, B. J.: Surgical
anatomy of the subclavian artery and itsbranches. Surg Gynec Obstet 108: 149, 1959.
32. ROSENBLUM, W. I.: Cerebral microcirculation: Areview emphasizing the interpretation of localblood flow and neuronal function. Angiology16: 485, 1965.
33. SHENKIN, H. A., SCHEUERMAN, W. G., SPITZ,E. B., AND GROFF, R. A.: Effect of change ofposition of the cerebral circulation of man.
J Appl Physiol 2: 317, 1949.34. CONOGHER, W. D. H., AND HUNTON, R. B.:
Ipsilateral reversed vertebral artery flow insubclavian artery stenosis or occlusion. Lancet2: 244, 1965.
35. JUDSON, W. E., HATCHER, J. D., AND WILKINS,R. W.: Blood pressure responses to the Val-salva maneuver in cardiac patients with andwithout congestive failure. Circulation 11:889, 1955.
36. TOOLE, J. F.: Stimulation of the carotid sinusin man: Cerebral response and significanceof head positioning. Amer J Med 27: 952,1959.
37. CONRAD, M. G., TOOLE, J. F., AND JANEWAY,R.: Hemodynamics of upper extremities insubclavian steal syndrome. Circulation 32:346, 1965.
38. ALLEN, E. V., BARKER, N. W., AND HINES, E.
A., JR.: Peripheral Vascular Diseases. Philadel-phia, W. B. Saunders Co., 1962, p. 6.
Circulation, Volume XXXIII, March 1966
483
by guest on July 12, 2018http://circ.ahajournals.org/
Dow
nloaded from

JAMES F. TOOLEInterarterial Shunts in the Cerebral Circulation
Print ISSN: 0009-7322. Online ISSN: 1524-4539 Copyright © 1966 American Heart Association, Inc. All rights reserved.
is published by the American Heart Association, 7272 Greenville Avenue, Dallas, TX 75231Circulation doi: 10.1161/01.CIR.33.3.474
1966;33:474-483Circulation.
http://circ.ahajournals.org/content/33/3/474.citationlocated on the World Wide Web at:
The online version of this article, along with updated information and services, is
http://circ.ahajournals.org//subscriptions/
is online at: Circulation Information about subscribing to Subscriptions:
http://www.lww.com/reprints Information about reprints can be found online at: Reprints:
document. and Rights Question and Answer
Permissionsthe Web page under Services. Further information about this process is available in thewhich permission is being requested is located, click Request Permissions in the middle column ofClearance Center, not the Editorial Office. Once the online version of the published article for
can be obtained via RightsLink, a service of the CopyrightCirculationoriginally published in Requests for permissions to reproduce figures, tables, or portions of articlesPermissions:
by guest on July 12, 2018http://circ.ahajournals.org/
Dow
nloaded from