special aspects of treating unborn babies - fpo.org.uk aspects of treating unborn babies. 2 ......
TRANSCRIPT

© Msc. Dr. Beatrix Urbanek D.O. DPO. 1
Special aspects of treating unborn babies
2
I am a specialist in obstetrics, homoeopathy and osteopathy.
In my practice, I work both as a gynaecologist and as an osteopath.
I am also a board member of the Osteopathic Centre for Children in Vienna, supervisor for child osteopathy and I teach osteopathy in obstetrics, newborns and premature babies .
I am a co-autor in the guidebook „Hilfe ich bin versteinert“ (only available in German) and the book „Osteopathie in der Frauenheilkunde“ (Osteopathy in obstetrics“) published by Elsevier Publishing.
In my profession I had the opportunity to develop a treatment of the blood flow in the A. uterine and their importance for the growing of the unborn child.
In this presentation I will show you the different aspects of it with three case reports.
After that I will present how you can influence malformations of the baby though osteopathic treatments.
© Msc. Dr. Beatrix Urbanek D.O. DPO.

© Msc. Dr. Beatrix Urbanek D.O. DPO. 3
Maria
32a Maria is a slim, very gentle woman who appears slightly shy, twin pregnancy manifested itself by way of the T-sign as monochorionic, diamnial
23rd week: The day before, during a check-up at the University Clinic the examining doctor had found a TTTS which showed that one fetus had pathological Doppler-flow measurements and a dystrophy. The other fetus was
found to have a polyhydramnion. The findings of the ultrasound tests carried out at the University Clinic showed
monochorionic twin pregnancy, significant weight discrepancy of 24%, polyhydramnion in fetus 1, fetus 2 with
pathological Doppler-flow measurements in the A. umbilicalis and the Ductus venosus. A high risk pregnancy.
The patient was advised to return to the clinic the following day for hospitalisation. Doctors at the clinic had pointed
out the high risk that the second fetus might not survive the pregnancy. They therefore wanted to induce labour.

4
The uterine artery coming from the internal iliac artery to the cervix with an acute angle going from caudal to cranial shaped arcade.

© Msc. Dr. Beatrix Urbanek D.O. DPO. 5

6
The blood flow in this angle can easily be influenced by the many anatomical connections in this area (cervix-corpus axis of the uterus, Lig. latum,.)
© Msc. Dr. Beatrix Urbanek D.O. DPO.

7
Lig. sacrouterinum with the connection to the M. piriformis and the
connection to the bony pelvis and the pelvic
floor and the
Lig. sacrorectogenito- pubealis (SRGP)
© Msc. Dr. Beatrix Urbanek D.O. DPO.

8
Osteopathic treatment:
Strong left rotation of the lower uterine segment with a confluence twist of the left artery. Work on the Lig. latum left with soft tissue techniques and balanced membranous techniques, on the left lamina SRGP and pelvic floor which shows tension of the left M. levator. This caused a better blood flow and a better angle between the cervix and the corpus uteri. Balance of increased sympathetic activity over the sacrum and the occiput with craniosacral work to calm the mothers emotional state and anxiety about her unborn children.
The next day the results of the Doppler examination are better and the patient doesn´t need to be hospitalized any more. (Fetus 1: A. umbilical PI 1,47, Ductus venous 0,74; Fetus 2: A. umbilical 1,76, Ductus venous 0,72)
The patient went to a check-up in the University Clinic every week.
The Doppler examination was stable, the dystrophy was still there but the 2nd fetus grew.
Osteopathic treatment first weekly until the 28th week, then in the 30th, 33rd and 36th week.
Delivery: Sectio caesarae of two boys: 2390g /50 cm Apgar 9/10/10 2100g/50 cm Apgar 9/10/10

© Msc. Dr. Beatrix Urbanek D.O. DPO. 9
Barbara
39 year old woman, psychologist
8th week: a small intrauterine hematoma
30th week: severe dystrophy of the baby (3rd percentile),
Doppler flow IV
Flow of the A. uterina:Before pregnancy 50ml/min At the end of pregnancy500ml/min

© Msc. Dr. Beatrix Urbanek D.O. DPO. 10
Arteriografie

© Msc. Dr. Beatrix Urbanek D.O. DPO. 11
Doppler alle

© Msc. Dr. Beatrix Urbanek D.O. DPO. 12
Osteopathic treatment of the pelvis and the A. uterina
The next day Doppler II
32nd week Sectio caesarea because of contractions and dystrophy of
the baby with Doppler III
Girl 1060g/36cm Apgar 5/9/9

© Msc. Dr. Beatrix Urbanek D.O. DPO. 13
33 year old dark-haired pregnant woman with her second child, trainer. At the organ screening in the 20th week there was a notch in the A. uterina, the other parameters were okay.
Andrea
14© Msc. Dr. Beatrix Urbanek D.O. DPO.
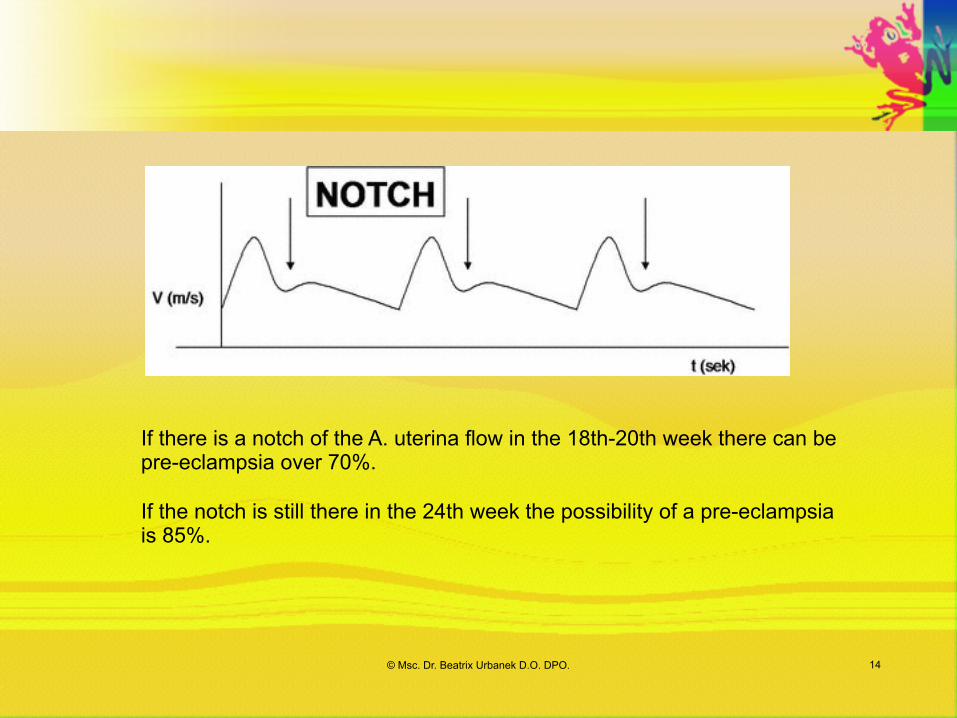
If there is a notch of the A. uterina flow in the 18th-20th week there can be pre-eclampsia over 70%.
If the notch is still there in the 24th week the possibility of a pre-eclampsia is 85%.
15© Msc. Dr. Beatrix Urbanek D.O. DPO.
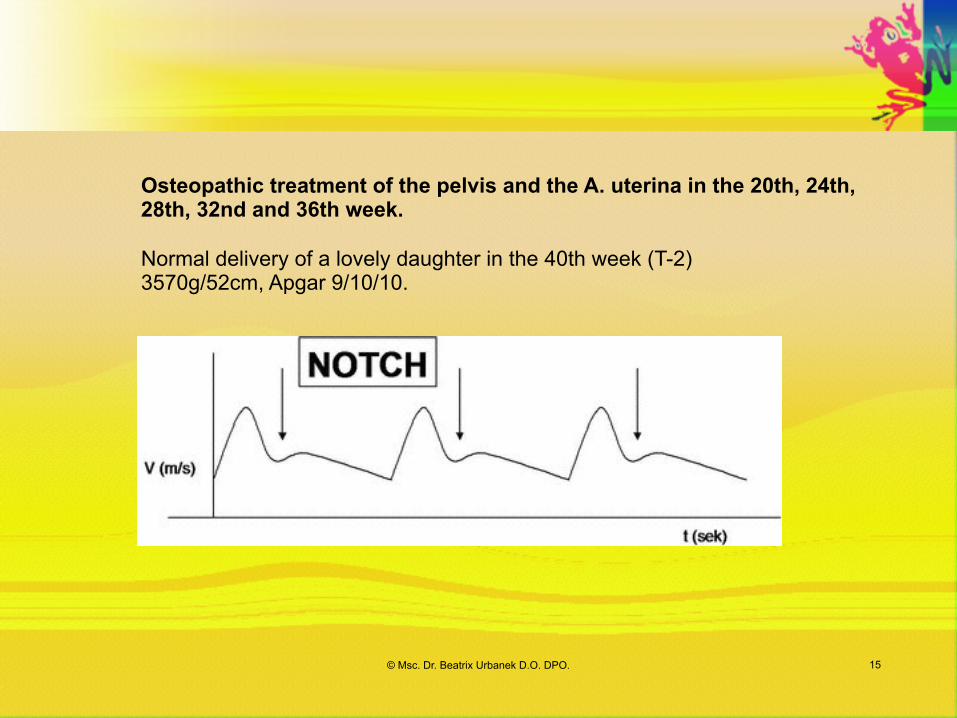
Osteopathic treatment of the pelvis and the A. uterina in the 20th, 24th, 28th, 32nd and 36th week.
Normal delivery of a lovely daughter in the 40th week (T-2) 3570g/52cm, Apgar 9/10/10.

© Msc. Dr. Beatrix Urbanek D.O. DPO. 16
I became acquainted with Mrs K. in the 25th week of her pregnancy. She was a delicate, very likeable, anxious woman. Anamnestically, her pregnancy was unremarkable up until the 20th week. It was her first child and she had allowed a genetic examination to be carried out in the early stages of her pregnancy by means of the OSCAR test. This was without pathological findings.
In the 20th week of pregnancy, during organ screening carried out in a special ultrasound centre, a 2-cm pulmonary cyst was detected in the baby.
Claudia
17© Msc. Dr. Beatrix Urbanek D.O. DPO.
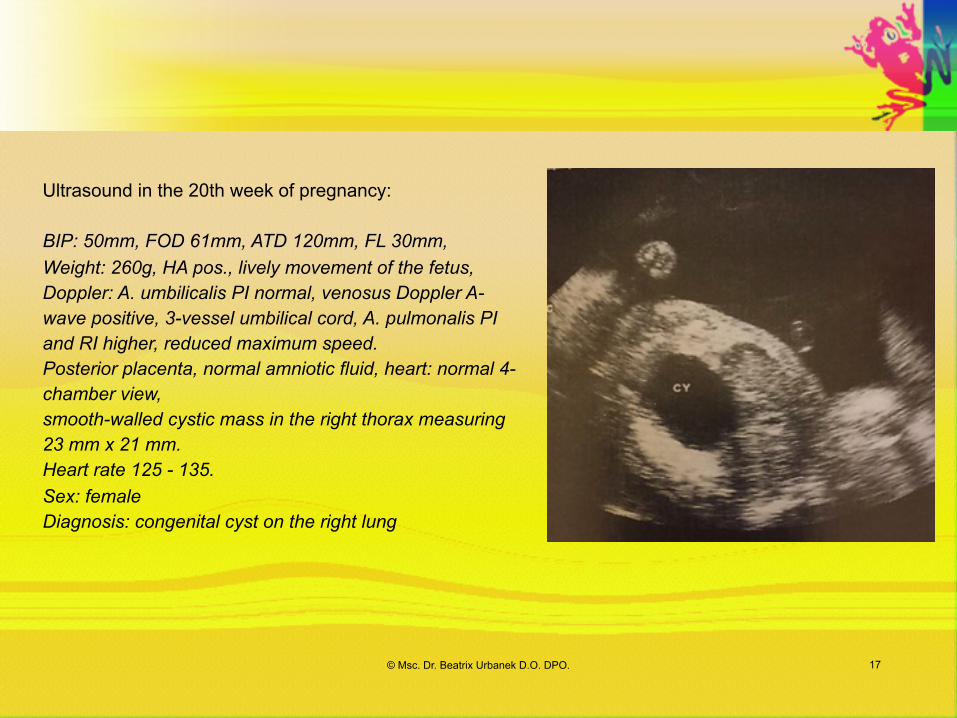
Ultrasound in the 20th week of pregnancy:
BIP: 50mm, FOD 61mm, ATD 120mm, FL 30mm, Weight: 260g, HA pos., lively movement of the fetus, Doppler: A. umbilicalis PI normal, venosus Doppler A-wave positive, 3-vessel umbilical cord, A. pulmonalis PI and RI higher, reduced maximum speed. Posterior placenta, normal amniotic fluid, heart: normal 4-chamber view, smooth-walled cystic mass in the right thorax measuring 23 mm x 21 mm. Heart rate 125 - 135. Sex: female Diagnosis: congenital cyst on the right lung
18
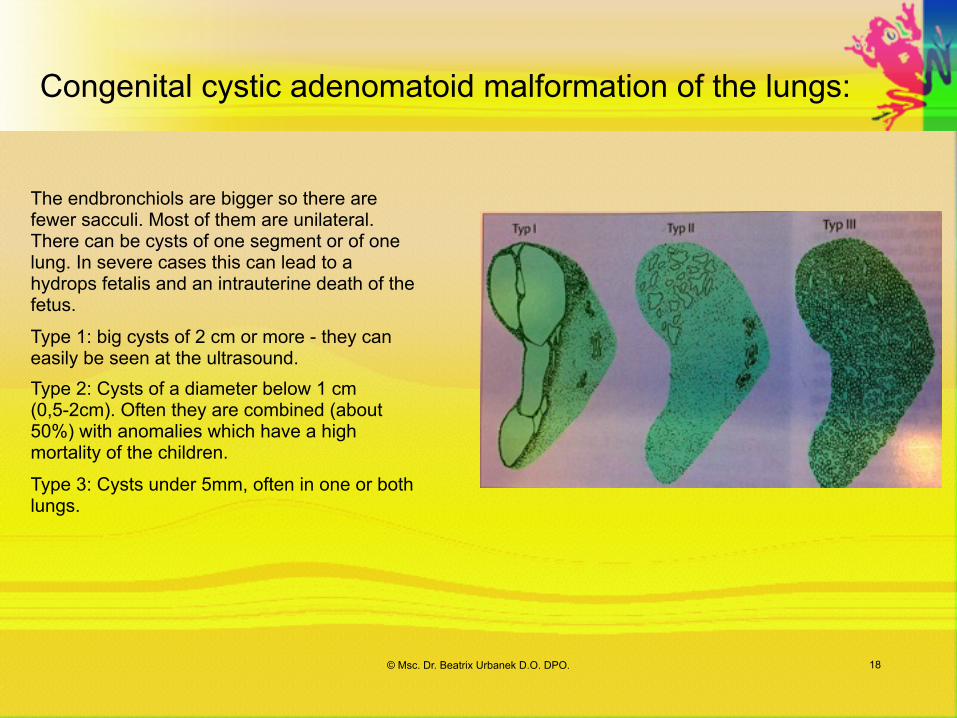
The endbronchiols are bigger so there are fewer sacculi. Most of them are unilateral. There can be cysts of one segment or of one lung. In severe cases this can lead to a hydrops fetalis and an intrauterine death of the fetus.
Type 1: big cysts of 2 cm or more - they can easily be seen at the ultrasound. Type 2: Cysts of a diameter below 1 cm (0,5-2cm). Often they are combined (about 50%) with anomalies which have a high mortality of the children.
Type 3: Cysts under 5mm, often in one or both lungs.
© Msc. Dr. Beatrix Urbanek D.O. DPO.
Congenital cystic adenomatoid malformation of the lungs:

© Msc. Dr. Beatrix Urbanek D.O. DPO. 19
Osteopathic treatment of the baby: Opening the Lymphs of the upper thorax and the lungs
The patient was presented at the University Clinic.
US University clinic 25th week:
Unstable fetal position, BIP 65mm, TH 58mm, FEM 43mm, weight: 680g. HA positive, positive fetal movements, posterior placenta,
Pulmonary cyst: right, smooth-walled 44 mm x 43mm, heart rate 100 - 105 /min, heart
displaced to the left
Diagnosis: pulmonary cyst, early stage bradycardia, high-risk pregnancy

© Msc. Dr. Beatrix Urbanek D.O. DPO. 20
I again treated the pregnant woman shortly before the Caesarean.
Claudia gave birth to a lively daughter weighing 2650g / 47cm and with an Apgar of 9/9/9 in spinal anesthesia, and was briefly able to hold little Sarah in her hands after birth and thus initiate a bonding process.
The newborn was operated on the very same day and the major operation was carried out without any difficulty. It was possible to save the upper right pulmonary lobe; the medial and inferior lobes of the right lung were reviewed and found to be almost entirely complete. The histological specimen was benign.
Considering the severity of the operation Sarah recovered very well within a period of three weeks.

© Msc. Dr. Beatrix Urbanek D.O. DPO. 21
very slim 32 a old patient with long dark hair, translator, very shy, withdrawn
I have known Mrs. B. since 2014, because she suffered from a strong dysmenorrhoe and was very sensitive to medicine because of a diverticulitis. She was sent to me from a very good osteopathic colleague.
I treated her osteopathically with intravaginal techniques because I found there was a strong tension at the left Lig. vesicouterinum and a portion between cervix and corpus uteri and a sidebendig of the uterus to the sigmoid.
The effect was that she got pregnant.
Valerie

© Msc. Dr. Beatrix Urbanek D.O. DPO. 22
US 14+6: CRL 92=15, HA+, placenta VW, inflated belly, she got Nat. carbonic C30.
20+0: She feels her fetus since 5 days, very strong pain in the belly and flatulence, osteopathic treatment of the intestine, which doesn´t have a nice and smooth movement and motilitation, the fetus feels well.
21+6: At the organ screening the fetal aortic valve was conspicuous. The mother was sent to see a cardiologist in the University Clinic.
cardiologist 22th week: 4 chambers of the heart are normal, there is a strong tendon thread in the left ventricle. Flow difference between the Aorta and the Bow of the Aorta.

© Msc. Dr. Beatrix Urbanek D.O. DPO. 23
24+1 Abdomen flatulence, treatment of the fetus, the heart of the fetus felt quite normal
25+7 osteopathic treatment of the fetus and the mother because of the strong obstipation, Lac.fellinum C 30

© Msc. Dr. Beatrix Urbanek D.O. DPO. 24
34+5 Sectio because of the obstipation of the mother and the breathing difficulties resulting from it
Fleming 2200g, 46cm, Apgar 9/9/10
29+6 Valerie felt much better, the heart of the fetus is the same
34+1 osteopathic treatment: the main focus is the belly of the mother
27the week cardiologist: Echocardiography, little flow difference between the Aorta and the AP and a strong tendon thread in the left ventricle

© Msc. Dr. Beatrix Urbanek D.O. DPO. 25
43a old small woman, 2nd partus, 2014 after IVF in the 39th week vacuum birth of Theresa, 2800g/48cm, Apgar 9/10/10
Case history: polyp removal, Factor V Leiden mutation
8+2 spontaneous pregnancy: CRL 21, HA pos, medication: Thyrex, Lovenox, Arefam, folic acid
Chorion villus biopsy because of a suspicious combined test, FISH test unsuspicious, long-term test: normal male karyotyp, placental failure is increased, 100mg Acetylsalicylacid until the 36th week 21Trisomy 1:93 (1:27) Trisomy 18 1:43 (1:64) Trisomy 13 1:13 (1: 201) free Beta-hCG, PAPP-Arisk of pre-eclampsia 1: 395, fetal growth retardation before 37th week: 1:123
Margit

26
Osteopathic treatment: 13+4 St. p. chorion villus biopsy: compensation of the ATN, plexus solaris osteopathic treatment by rebalancing the diaphragm, the fetus has a flexion lesion
16+3 Fetomed: Organ screening everything okay
22+1 Fetomed: ventricular septum defect, referral to a cardiologist and a psychologist
University Clinic: ventricular septum defect 3mm, ASD with R-L Shunt, normal drainage, normal pumpfunction of the heart
© Msc. Dr. Beatrix Urbanek D.O. DPO. 27
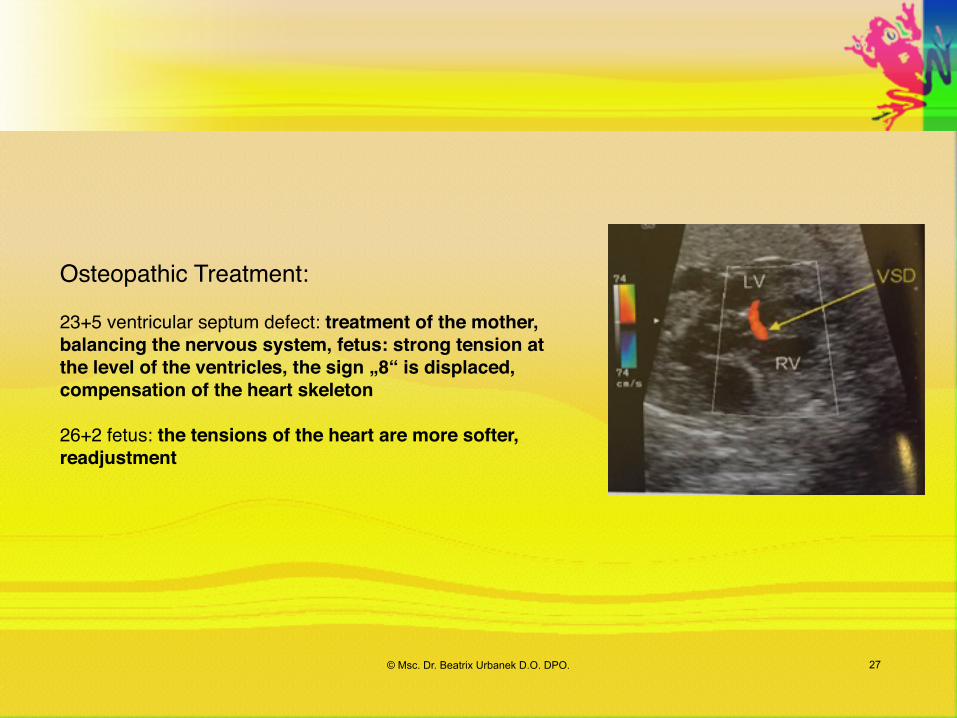
Osteopathic Treatment:
23+5 ventricular septum defect: treatment of the mother, balancing the nervous system, fetus: strong tension at the level of the ventricles, the sign „8“ is displaced, compensation of the heart skeleton
26+2 fetus: the tensions of the heart are more softer, readjustment

28
With a ventricular defect in 80% of the cases there is a hole in the pars membranacea and in 20% of the cases there is a hole in the pars muscular of the intraventricular septum.
Very often you find a perimembranous ventricle septum defect where a membranacea defect is combined with the pars muscular.
It is the most common heart defect. 30% of all congenital heart defects are single heart defects and 50% are associated with other heart defects like Fallot tetralogy, a pulmonary atresia, arterioventricular defect…..
A defect smaller than 3mm is only recognizable with colour Doppler.
Small defects can heal spontaneously also after delivery.
© Msc. Dr. Beatrix Urbanek D.O. DPO.
Ventricular defect

© Msc. Dr. Beatrix Urbanek D.O. DPO. 29
University Clinic: ventricular septum defect reduction of 50%
verified through Fetomed one week later
Osteopathic treatment:30+5 Breech position, osteopathic treatment of the uterine and fetus axes, work on M. psoas and the movement of the fetus
31+5 Fetomed: four chamber view normal
Osteopathic treatment:35+2: head position, preparation of the pelvis for the delivery and the movement of the fetus through it
39th week, spontaneous delivery of a healthy boy named Thomas, 3400g, 50cm, Apgar 9/10/10
US of the heart after the delivery was without a result

30
I showed you some special aspects of treating unborn babies and I want to ask you to listen
what the babies want from you and how you to come in contact with them.
© Msc. Dr. Beatrix Urbanek D.O. DPO.

© Msc. Dr. Beatrix Urbanek D.O. DPO. 31
Hebamme plus Kind
Thank you for your attention.Dr. Beatrix Urbanek: www.ozk.at.