special issue gastrointestinal health · 4 ©2013 natural medicine journal. all rights reserved....
TRANSCRIPT
SPECIAL ISSUE
Gastrointestinal Health
AUDIO INTERVIEW WITH EAMONN QUIGLEY, MD
The Role of the Microbiome on Scientific Research and Human Health
SEPTEMBER 2013 SUPPLEMENT
LITERATURE REVIEW
Probiotics for the Treatment of Irritable Bowel Syndrome

New ideas are taking root at Integrative TherapeuticsTM. In addition to developing innovative formulas
that help patients live stronger, healthier lives, we’re working with renewed focus to help you grow a
stronger practice. Our refreshed packaging will make product selection quick and intuitive. And you’ll
find it all on our new website, which is a burgeoning resource of product and ingredient information,
educational materials, and powerful practice-building tools. Tools that will help you work more efficiently,
giving you more time to cultivate stronger relationships with patients — and a healthier practice.
Let’s grow stronger, together. To learn more call 800.931.1709 or visit integrativepro.com.
© 2013 Integrative Therapeutics, LLC
LET’S GROWSTRONGER,TOGETHER.
| CULTIVATE HEALTHY PRACTICES |
NMJ, SEPTEMBER 2013 SUPPLEMENT—VOL 5, NO. 9 (SUPPL) ©2013 NATURAL MEDICINE JOURNAL. ALL RIGHTS RESERVED. 3
SPECIAL ISSUE GASTROINTESTINAL HEALTH
Contents
Copyright © 2013 by the Natural Medicine Journal. All rights reserved.
AUDIO INTERVIEWS
6 The Role of the Microbiome on Scientific Research and Human Health:
An Interview with Eamonn Quigley, MD
7 Clinical Applications and Current Legal Status of
Fecal Microbiota Transplantation
An Interview with Mark Davis, ND
ABSTRACTS & COMMENTARY
8 Melatonin Treats H. Pylori and Gastric Ulcers
10 Fiber, Bacteria, and Colorectal Cancer
11 Gliaden Reactivity Associated With Autism
PEER-REVIEWED ARTICLE
14 Literature Review: Probiotics for the Treatment of Irritable Bowel Syndrome
By Lise Alschuler, ND, FABNO, and Karolyn A. Gazella
BOOK REVIEW
20 Enteroimmunology Textbook by Charles Lewis, MD, MPH
Review by Teresa Silliman, ND
EXPERT Q&A
22 The Role of Digestive Enzymes in Gastrointestinal Health
A discussion with researcher M. Mamadou, PhD

4 ©2013 NATURAL MEDICINE JOURNAL. ALL RIGHTS RESERVED. NMJ, SEPTEMBER 2013 SUPPLEMENT—VOL 5, NO. 9 (SUPPL)
Lise Alschuler, NDMatthew Baral, NDBill Benda, MDRobin Bernhoft, MD, FACDonald J. Brown, NDMatthew Budoff, MDCarlo Calabrese, NDJaclyn Chasse, NDJean-Yves Dionne, RPhGeovanni Espinosa, NDAlan R. Gaby, MDPatrick Hanaway, MDCarl Hangee-Bauer, NDTori Hudson, NDMark Hyman, MDEllen Kamhi, PhD, RNMary Jo Kreitzer, PhD, RNIva Lloyd, NDDouglas MacKay, NDTracy Marsden, BSc PhmKeri Marshall, NDMorgan Martin, ND, LM, CPM Mona Morstein, NDMichael T. Murray, NDCheryl Myers, RNKasra Pournadeali, NDHarry Preuss, MD, MACN, CNSCorey Resnick, NDCathy Carlson-Rink, NDBarry W. Ritz, PhDDaniel Rubin, NDSusan Ryan, DOAlexander Schauss, PhDJacob Schor, ND, FABNODugald Seely, ND, MSc, FABNOFraser Smith, NDMichael Taylor, DC, DABCISherry Torkos, BSc PhmMichael Traub, ND, DHANP,
FABNOCatherine Ulbricht, PharmD,
MBA[c]Debi Walker, NDMarcus Webb, ND, DODecker Weiss, NMDEric Yarnell, NDHeather Zwickey, PhD
The Natural Medicine Journal is led by an esteemed group of professionals in the integrative health field representing a diverse spectrum of disciplines within medicine.
Editorial BoardLISE ALSCHULER, ND, FABNO, is a naturopathic physician with board certi-fication in naturopathic oncology and a graduate of Bastyr University where she received her naturopathic doctorate. She is the coau-
thor of two books on cancer, The Definitive Guide to Cancer and The Definitive Guide to Thriving After Cancer. She is also the cohost of the Five to Thrive Live! internet radio show featured on The Cancer Support Network. For more information visit www.FiveToThrivePlan.com or DrLise.net.
MATTHEW BARAL, ND, received his naturopathic medical degree from Bastyr University in 2000. He is chair of the Depart-ment of Pediatric Medicine at the Southwest College of Naturopathic Medicine &
Health Sciences (SCNM), where he teaches pediatrics in the classroom and supervises student clinicians on clinical rotations. Dr. Baral designed the first naturopathic pedi-atric residency program in naturopathic medicine and serves as its director at SCNM. He is also the founding and current president of the Pediatric Association of Naturopathic Physicians.
In addition to being the publisher of Natural Medi-cine Journal, KAROLYN A. GAZELLA has been writing and publishing wellness information since 1992. She is the author or coauthor of hundreds
of articles and several books including the two books that she has written with Dr. Lise Alschuler, The Definitive Guide to Cancer and The Definitive Guide to Thriving After Cancer. For more information, visit www.karolyngazella.com.
TINA KACZOR, ND, FABNO, is a naturopathic physician, board certi-fied in naturopathic oncology. She is in private practice at the Clinic of Natural Medicine in Eugene, Ore. Kaczor received her naturopathic doctorate from National College of Natural Medi-cine, and completed her residency in
naturopathic oncology at Cancer Treatment Centers of America in Tulsa, Okla. Kaczor is also the senior medical editor of Natural Medicine Journal.
HEATHER PAULSON, ND, FABNO, is a Fellow of the American Board of Naturopathic Oncology (FABNO), which represents the highest expertise in the area of naturopathic oncology. Paulson is in private practice at Arizona Natural Health Center. She provides her patients with comprehensive natural treatment
options for cancer, including dietary, botanical, and IV therapies with classical homeopathy for cancer inhibi-tion. Paulson enjoys sharing her passion for naturopathic oncology by teaching oncology courses and clinical rota-tions at Southwest College of Naturopathic Medicine.
JACOB SCHOR ND, FABNO, is a graduate of National College of Natu-ropathic Medicine and now practices in Denver. He served as president to the Colorado Association of Naturo-pathic Physicians and is on the board of directors of the Oncology Associa-tion of Naturopathic Physicians. He
is recognized as a Fellow by the American Board of Naturopathic Oncology. Schor serves as associate medical editor of NMJ.
TERESA SILLIMAN, ND, received her doctorate of Naturopathic Medi-cine, with academic honors, from National College of Naturopathic Medicine. Prior to that, she obtained her bachelor’s degree from Stanford University. She was awarded a fellow-ship from the American Heart Asso-
ciation which led to a publication of her work in the American Journal of Physiology.
This Issue’s Contributors
Lise Alschuler, ND, FABNO
Matthew Baral, ND
Karolyn A. Gazella
Teresa Silliman, ND
Jacob Schor ND, FABNO
Tina Kaczor, ND, FABNO
Heather Paulson, ND, FABNO

NMJ, SEPTEMBER 2013 SUPPLEMENT—VOL 5, NO. 9 (SUPPL) ©2013 NATURAL MEDICINE JOURNAL. ALL RIGHTS RESERVED. 5
Copyright © 2013 by the Natural Medicine Journal. All rights reserved.
SENIOR MEDICAL EDITORTina Kaczor, ND, FABNO
ASSOCIATE MEDICAL EDITORJacob Schor, ND, FABNO
PUBLISHERKarolyn A. Gazella
EDITOR-IN-CHIEFDeirdre Shevlin Bell
COMMUNICATIONS SPECIALISTTeresa M. Peterson
DESIGNKaren Sperry
PUBLISHED BYCHAT Inc.P.O. Box 17232Boulder, CO 80308
Natural Medicine Journal (ISSN 2157-6769) is published 12 times per year by CHAT Inc. Copyright © 2013 by CHAT Inc. All rights reserved. No part of this publica-tion may be reproduced in whole or in part without written permission from the publisher. The statements and opinions in the articles in this publication are the responsibility of the authors; CHAT Inc. assumes no liability for any information published herein. Advertisements in this publication do not indicate endorse-ment or approval of the products or services by the editors or authors of this publication. CHAT Inc. is not liable for any injury or harm to persons or property resulting from statements made or products or services referred to in the articles or advertisements.
MESSAGE FROM THE PUBLISHER
Please Enjoy Our Inaugural Special IssueWelcome to the first special issue of the Natural Medicine Journal. Each year we will publish two special issues on topics with broad appeal. We begin with gastro-intestinal (GI) health. Even if you don’t have specialty in this area, because of the increasing prevalence of GI disorders, this issue’s content covers topics you are likely to encounter.
The phrase “death begins in the colon” may be debatable, but certainly for millions of people worldwide, poor health can be traced back to the gastrointestinal tract. The National Digestive Diseases Information Clearinghouse reports that approxi-mately 70 million Americans are afflicted with some type of digestive disease. Of those disorders, irritable bowel syndrome (IBS) has become one of the most common, affecting 1 in 5 women and 1 in 10 men. This special issue includes a peer-reviewed literature review on the topic of probiotics and IBS, beginning on page 14. In addition, leading gastrointestinal expert Eamonn Quigley, MD, discusses probiotics and IBS in the audio interview featured on page 6. Quigley also provides listeners with an update on the Human Microbiome Project.
In an audio interview on page 7, Mark Davis, ND, discusses the fascinating and controversial topic of fecal microbiota transplantation (FMT). Davis gives an over-view of the science, procedure, and legal status of FMT. In the question and answer interview on page 22, researcher M. Mamadou, PhD, describes the use of enzymes in common digestive disorders.
As with every issue of the Natural Medicine Journal, this special issue also features our popular Abstracts & Commentary section. In this section your colleagues examine the latest published research and weigh in on the studies’ applications to clinical practice.
And finally, Teresa Silliman, ND, provides us with a review of the new textbook, Enteroimmunology: A guide to prevention and treatment of chronic disease, by Charles A. Lewis, MD, MPH. Silliman will tell you why she believes, “Every physician should have this insightful book at his or her side—especially those practitioners who follow the tenets of naturopathic medicine.”
If you are interested in contributing to the Natural Medicine Journal, please contact me at [email protected]. Also, please remind your colleagues that they can visit our website — www.naturalmedicinejournal.com — and sign up to receive the journal and all special issues absolutely free.
We hope you find this special issue of the Natural Medicine Journal interesting and informative. On behalf of the staff, editorial board, and contributors, we appreciate your support.
In good health,
Karolyn A. GazellaPublisher

6 ©2013 NATURAL MEDICINE JOURNAL. ALL RIGHTS RESERVED. NMJ, SEPTEMBER 2013 SUPPLEMENT—VOL 5, NO. 9 (SUPPL)
Yep, it really is that EASY!
We set up your FREE, personalized web storeYou send the patients We send you a monthly check
1
2
3
DNSW INC 119203 HALFpg.indd 1 9/3/13 11:05 AM
AUDIO INTERVIEW
The Role of the Microbiome in Scientific Research and Human HealthAn Interview with Eamonn Quigley, MD
Highly respected gastro-intestinal researcher and expert, Eamonn Quigley, MD, discusses the research significance of the Human Microbiome Project and what role it could play in terms of disease prevention
and treatment. Quigley also explains his view of the role that probiotics, prebiotics, and synbiotics play in the treatment of gastroin-testinal disorders and other health issues.
ABOUT THE EXPERT
Eamonn Quigley, MD, is the past president of the American College of Gastroenterology and the World Gastroenterology Organization. Presently he is the chair of the World Gastroen-terology Organization Foundation and the divi-sion head of Gastroenterology and Hepatology at The Methodist Hospital System in Houston, Texas, where he is also developing a gastroenterology fellowship program. Quigley earned his medical doctorate from National University of Ireland, Cork, Ireland. He has been published in nearly 500 different peer-reviewed publications and has been the principal investigator or co-principal investigator of many research studies involving gastrointestinal issues.

NMJ, SEPTEMBER 2013 SUPPLEMENT—VOL 5, NO. 9 (SUPPL) ©2013 NATURAL MEDICINE JOURNAL. ALL RIGHTS RESERVED. 7
AUDIO INTERVIEW
Clinical Applications and Current Legal Status of Fecal Microbiota TransplantationAn Interview with Mark Davis, ND
In this audio interview, clinician Mark Davis, ND, explains what fecal microbiota transplanta-tion (FMT) is, how to administer it safely in clinical practice, and what the present legal status is regarding administration of FMT in the clinical setting. He
also describes how FMT differs from probiotic therapy and which conditions are most likely to benefit from FMT.
ABOUT THE EXPERT
Mark Davis, ND, is the medical director at the Good Life Medicine Center in Port-land, Ore., where he focuses on gastroin-testinal health. He received his medical doctorate with honors in research from Natural College of Natural Medicine. Davis is internationally known for his expertise in microbial medicine and is currently awaiting FDA approval for his clinical trial protocol to study fecal microbiota transplantation (FMT) for colonic inflamma-tory bowel disease. You can find out more about Davis at BrightMedicineClinic.com, FecalMicrobiotaTransplantation .com, and GoodLifePDX.com.
Scientifically-Valid, Clinically-Proven Quality IngredientsBrought to you by Tomorrow’s Nutrition
For more information about these quality ingredients, contact Tomorrow’s Nutrition at 1-877-498-3228
or visit www.tomorrowsnutrition.com.
Relax, refresh, revive
Produced via a patented fermentation process, delivering 100% pure L-theanine, scientifically proven to reduce stress and improve focus, concentration and the quality of sleep.
www.suntheanine.com
Invisible fiber, visible benefits
This unique regulating soluble fiber helps reduce both constipation and diarrhea with less gas and bloating. It also lowers blood sugar, normalizes cholesterol, improves mineral absorption and promotes healthy satiety.
www.sunfiber.com
Power of green tea, naturally
This high quality green tea ingredient is produced from pesticide compliant green tea and extracted via a water infusion process and decaffeinated using only approved food grade solvents and no chloroform or other illegal solvents.
www.sunphenon.com
To receive 20% off
your product order, just type in
the code NMJGI at check out.
8 ©2013 NATURAL MEDICINE JOURNAL. ALL RIGHTS RESERVED. NMJ, SEPTEMBER 2013 SUPPLEMENT—VOL 5, NO. 9 (SUPPL)
ABSTRACT & COMMENTARY
Melatonin Treats H. Pylori and Gastric Ulcers
REFERENCEOsadchuk MA, Sibriaev AA, Kireeva NV, Kvetno�ı IM. The influence of melatonin included in the combined treatment of antichelicobaterial therapy on immunohistochemical characteristics of gastric epitheliocytes from patients with duodenal ulcer. Klin Med (Mosk). 2012;90(12):48-52.
DESIGN An open clinical trial that added melatonin to a standard protocol for treating Helicobacter pylori infection. Clinical outcomes were compared with matched controls.
PARTICIPANTS The study included 100 patients with duodenal ulcer (DU), 30 with chronic non-atrophic gastritis (CNAG), 30 with chronic atrophic gastritis (CAG), and 12 healthy subjects. All patients with DU and CNAG had morphologically confirmed H. pylori infection. The patients with DU were divided into 2 groups, each including age-matched subjects with endoscopically, morphologically, and immunohisto-chemically identical characteristics.
STUDY MEDICATION AND DOSAGEGroup 1 patients underwent a conventional 7-day course of treatment for H. pylori that included omepra-zole (20 mg BID), clarithromycin (500 mg BID), and amoxicillin (1,000 mg BID). Group 2 received the same treatment with the addition of melatonin (3 mg before bedtime). Patients in group 1 continued omeprazole and those in group 2 omeprazole plus melatonin for a total of 2 months. Healthy subjects and patients with CAG served as controls.
OUTCOME MEASURES All patients underwent fibrogastroduodenoscopy (FGDS) on weeks 2 and 4. Immunohistochemical studies were conducted for endothelin-1 and mela-tonin-positive cells. Apoptotic activity of mucosal epitheliocytes from gastric antrum was measured before and 6 weeks after the start of therapy.
KEY FINDINGSThe addition of melatonin to the standard treatment protocol for H. pylori increases efficacy of H. pylori elimination and accelerates DU healing. A 2-month therapy of omeprazole + melatonin is more effec-tive at normalizing markers of healing than treat-ment with omeprazole alone.
PRACTICE IMPLICATIONSMelatonin should now be considered in the treatment of H. pylori, gastric and duodenal ulcers, and gastrointestinal reflux disease.
Many patients are aware that melatonin may improve insomnia, but few are aware of its beneficial impact on the gastrointestinal tract. We think of melatonin only as the hormone produced in the brain by the pineal gland, yet far more melatonin is actually made by enteroendocrine cells that line the digestive tract.
Bowel habits follow clear circadian rhythms, and it is melatonin that regulates this timing. Dietary L-tryptophan increases blood levels of melatonin, even in animals that have had their pineal glands removed. L-tryptophan is converted to serotonin that in turn is converted into melatonin. The nighttime surge in melatonin comes from the pineal gland, but the gastrointestinal tract maintains baseline levels. Melatonin levels in the gut are 10 to 100 times higher than in the blood.1
This is not the first study to report melatonin has benefit in treating H. pylori. In 2 studies published in 2011, Celinski et al reported that either melatonin or L-tryptophan helps heal gastric and duodenal ulcers resulting from H. pylori infections in humans. They gave all patients omeprazole 20 mg twice a day and then added either melatonin (5 mg BID) or tryptophan (250 mg BID). Both melatonin and tryptophan sped healing compared to omeprazole alone.2,3
A number of reports suggest melatonin may be useful in treating gastro-esophageal reflux disease (GERD). This was first brought to our attention by de Souza Pereira who in a May 2006 letter to the editor of the Journal of Pineal Research described a 64-year-old woman whose GERD responded well to a formula containing melatonin (6 mg). Later the same year de Souza Pereira reported the results of a clinical trial in which 176 patients received this melatonin-containing product and 175 received omeprazole (20 mg). All the patients receiving melatonin supplements “reported a complete regression of symptoms after 40 days of treatment.” Only 65.7% of those receiving omeprazole reported similar improvement.4
Madalinski in 2011 suggested that melatonin might protect against development of “erosive esophagitis, … esophageal stricture, Barrett’s esophagus and extra-esophageal damage (including the lungs, throat, sinuses, middle ear, and teeth),” all of which are “major risk factors for esophageal carcinoma.”5
Jacob Schor, ND, FABNO

NMJ, SEPTEMBER 2013 SUPPLEMENT—VOL 5, NO. 9 (SUPPL) ©2013 NATURAL MEDICINE JOURNAL. ALL RIGHTS RESERVED. 9
ABSTRACT & COMMENTARY
REFERENCES1 Bubenik GA. Thirty-four years since the discovery of gastrointestinal melatonin. J Physiol Pharmacol. 2008;59 Suppl
2:33-51. 2 Celinski K, Konturek PC, Konturek SJ, et al. Effects of melatonin and tryptophan on healing of gastric and duodenal
ulcers with Helicobacter pylori infection in humans. J Physiol Pharmacol. 2011;62(5):521-526.3 Celinski K, Konturek SJ, Konturek PC, et al. Melatonin or L-tryptophan accelerates healing of gastroduodenal ulcers in
patients treated with omeprazole. J Pineal Res. 2011;50(4):389-394. 4 Pereira Rde S. Regression of gastroesophageal reflux disease symptoms using dietary supplementation with melatonin,
vitamins and amino acids: comparison with omeprazole. J Pineal Res. 2006;41(3):195-200.5 Madalinski MH. Does a melatonin supplement alter the course of gastro-esophageal reflux disease? World J Gastroin-
test Pharmacol Ther. 2011;2(6):50-51. 6 Jaworek J, Brzozowski T, Konturek SJ. Melatonin as an organoprotector in the stomach and the pancreas. J Pineal Res.
2005;38(2):73-83.7 Belyaev O, Herzog T, Munding J, et al. Protective role of endogenous melatonin in the early course of human acute
pancreatitis. J Pineal Res. 2011;50(1):71-77.8 Koppisetti S, Jenigiri B, Terron MP, et al. Reactive oxygen species and the hypomotility of the gall bladder as targets for
the treatment of gallstones with melatonin: a review. Dig Dis Sci. 2008;53(10):2592-2603.9 Cichoz-Lach H, Celinski K, Konturek PC, Konturek SJ, Slomka M. The effects of L-tryptophan and melatonin on selected
biochemical parameters in patients with steatohepatitis. J Physiol Pharmacol. 2010;61(5):577-580.
The benefits of melatonin aren’t limited to the esophagus and stomach but extend to the pancreas and liver. Melatonin “prevents various forms of gastritis and pancre-atitis through the activation of specific MT2-receptors and scavenges reactive oxygen species (ROS). Melatonin counteracts the increase in the ROS-induced lipid peroxi-dation and preserves, at least in part, the activity of key anti-oxidizing enzymes such as superoxide dismutase.”6 In a 2011 study of 75 patients with acute pancreatitis, high levels of endogenous melatonin played a protective role and were associated with a milder course of disease.7
Melatonin may also protect against gallstone formation. It reduces biliary levels of cholesterol by inhibiting cholesterol absorption across the intestinal epithelium and by increasing conversion of cholesterol to bile acids.8 In a study of 45 patients with steatohepatitis, melatonin produced a “statistically significant reduction in GGTP, triglycerides and proinflammatory cytokine levels.”9
The bottom line is simple: In melatonin we have a potent tool to help protect and heal the gastrointestinal tract. This study just adds further evidence to support its use.
10 ©2013 NATURAL MEDICINE JOURNAL. ALL RIGHTS RESERVED. NMJ, SEPTEMBER 2013 SUPPLEMENT—VOL 5, NO. 9 (SUPPL)
PRACTICE IMPLICATIONSThis study supports what has been reported in several cell culture and epide-miological studies: The right gut bacteria, fiber, and SCFAs may reduce colon cancer cell growth.
Fibers that initiate SCFA production from greatest to least are citrus pectin, soy fiber, sugar beet fiber, pea fiber, apple pectin, and oat fiber.1 Some of the possible protective effects of butyrate include its ability to nourish colonocytes, induce apoptosis, and increase glutathione transferases.2,3
Research has also supported the use of probiotics for reducing colon cancer cell growth in vitro and in vivo. Studies have supported the use of Lactobacillus species to decrease colorectal cell invasion.4 In patients with familial adenoma-tous polyposis, a 4-week intervention with the probiotic VSL#3, containing both Bifidobacteria and Lactobacillus strains, showed a reduction in cell prolif-eration and an increase in glutathione S-transferase (GST) enzyme, providing a protective benefit against colon cancer.5
Regarding fiber intake, human data supports the use of vegetable fiber in particular for reducing the risk of developing colon polyps. Another fiber that has been studied in animal models is inulin, which induced apoptosis in already transformed cells when used in the diet.
Although more research is needed, practitioners might suggest citrus pectin, probiotics containing Lactobacillus and Bifidobacteria, and butyrate to reduce colon cancer risk. I encourage my patients to eat a diet rich in vegetable fiber to increase the Bifidobacterium already present in their gut and thus SCFA production. These lifestyle and supplement interventions may provide the right fiber, gut bacteria, and SCFAs to reduce colon cancer cell growth and promote healthy colonocytes.
REFERENCES1 Titgemeyer EC, Bourquin LD, Fahey GC Jr, Garleb KA. Fermentability of various fiber sources by human fecal
bacteria in vitro. Am J Clin Nutr. 1991;53(6):1418-1424.2 Scharlau D, Borowicki A, Habermann N, et al. Mechanisms of primary cancer prevention by butyrate and
other products formed during gut flora-mediated fermentation of dietary fibre. Mutat Res. 2009;682(1):39-53. 3 Hinnebusch BF, Meng S, Wu JT, Archer SY, Hodin RA. The effects of short-chain fatty acids on human colon
cancer cell phenotype are associated with histone hyperacetylation. J Nutr. 2002;132(5):1012-1017.4 Escamilla J, Lane MA, Maitin V. Cell-free supernatants from probiotic Lactobacillus casei and Lactobacillus
rhamnosus GG decrease colon cancer cell invasion in vitro. Nutr Cancer. 2012;64(6):871-878.5 Friederich P, Verschuur J, van Heumen BW, et al. Effects of intervention with sulindac and inulin/VSL#3 on
mucosal and luminal factors in the pouch of patients with familial adenomatous polyposis. Int J Colorectal Dis. 2011;26(5):575-582.
ABSTRACT & COMMENTARY
Fiber, Bacteria, and Colorectal Cancer
REFERENCEChen HM, Yu YN, Wang JL, et al. Decreased dietary fiber intake and structural alteration of gut microbiota in patients with advanced colorectal adenoma. Am J Clin Nutr. 2013; 97:1044-1052.
DESIGNObservational case control, cross-sectional designed trial matching patients with a diag-nosis of advanced colorectal cancer (A-CRA) to a healthy control (HC) group
PARTICIPANTSStudy selected 5,632 consecutive patients who had undergone colonoscopy from 5 medical centers in China. Of these subjects, 688 (344 in each of the A-CRA and HC groups) eligible subjects completed the food-frequency questionnaire and provided fecal samples.
STUDY PARAMETERSDietary fiber intake, short-chain fatty acids (SCFAs), and gut microbiota in patients with advanced colorectal cancer were compared to the control group.
PRIMARY OUTCOME MEASURESSCFAs, microbiota, dietary fiber intake as related to A-CRA risk
KEY FINDINGSThis study identified several factors that were protective against A-CRA, including intake of vegetables and high amounts of fecal acetic acid and butyric acid. A high-fiber diet increased butyrate and butyrate-producing bacteria. The A-CRA group had significantly lower SCFAs in their stool. The major SCFA production in the HC group was acetate, followed by butyrate and propionate.
There was also a significant difference in the gut microbiota between the groups. Participants with A-CRA had higher levels of Enterococcus, Streptococcus, and Bacte-roidetes and lower levels of Clostridium, Roseburia, and Eubacterium spp. compared to the HC group.
Heather Paulson, ND, FABNO
NMJ, SEPTEMBER 2013 SUPPLEMENT—VOL 5, NO. 9 (SUPPL) ©2013 NATURAL MEDICINE JOURNAL. ALL RIGHTS RESERVED. 11
REFERENCELau NM, Green PH, Taylor AK, et al. Markers of celiac disease and gluten sensitivity in chil-dren with autism. PLoS One. 2013;8(6):e66155.
DESIGNPopulation study
PARTICIPANTSStudy included 140 children (37 with autism, 27 non-autistic siblings of those autistic children, and 76 healthy controls). The autistic children were diagnosed based on the Autism Diagnostic Observation Schedule (ADOS) and the Autism Diagnostic Interview, Revised (ADI-R). Serum specimens were collected from all groups and tested for reactivity to gliadin as well as celiac-specific markers.
KEY FINDINGSImmunoglobulin G (IgG) reactivity to gliadin was higher in autistics compared to unaffected siblings and healthy controls. The pres-ence of gliadin reactivity was also associated with a history of gastro-intestinal symptoms. However, celiac-specific markers were not increased in autistics compared to controls. This study helps to clarify an immunological basis for symptomology in autistic children who appear to be intolerant to the gluten-containing grains.
PRACTICE IMPLICATIONSA gluten-free, casein-free (GFCF) diet has been popular for many years among both families of children with autism and alternative-minded practitioners who treat these patients. Most of the evidence that has circulated in the past has been anecdotal in nature, but a small body of research does exist in this area. In 2008, Barcia reported a 3-fold higher prevalence of celiac disease in people with autism,1 which speaks to the importance of screening all autism patients regardless of gastrointestinal symptoms. This reactivity may have several etiologies. It is well known that there are immune aberrations in children with autism.2–4 It is not entirely clear whether these abnormalities are purely genetic in nature or if they are induced by diet and lifestyle factors. Cuchacovich and colleagues demonstrated in patients who had a myocardial infarction that streptokinase can promote autoantibodies to dipeptidyl-peptidase IV,5–7 the primary enzyme used to digest gluten and casein. Streptokinase is released in large amounts when antibiotics are used for streptococcal infections; many people with autism have extensive histories of antibiotic treatment for multiple infections, which may explain their gliadin intolerance.
The science that explains gliadin intolerance only accounts for part of this complicated picture. Specific neurological impairment may result from an immunological response to gliadin. IgG to gliadin has been shown to cross-react with cerebellar peptides and Purkinje cells.8 The cerebellum, other than aiding in balance, is also involved with cognitive abilities like attention and language, as well as regulating fear and pleasure responses. These additional cerebellar functions are quite often impaired in autistic children. Purkinje cells are GABAergic, which may explain why a larger percentage of people with autism will have some seizure activity in their lifetime than will the neuro-typical population: 1–2% of children in the general population will develop epilepsy, compared to 5–38% of children with autism spectrum disorder.9
The benefits of a GFCF diet may also be explained by a decrease in systemic inflamma-tion during dietary elimination. Milk and wheat ingestion has been shown to increase proinflammatory cytokines TNF-α, IFN-δ.10 Interestingly, autistic patients show higher serum TNF-α when compared to controls, and those patients exhibit more gastrointestinal symptoms.11 There is also a direct relationship between a GFCF diet and a decrease in colonic TNF-α compared to controls, adding validity to the diet’s use in the autistic population.12
It is important to mention the research that many conventional physicians refer to as evidence that the GFCF diet does not work. Elder and colleagues performed a double-blind, placebo-controlled study on the GFCF diet in children with autism and reported no statistically significant findings.13 However, several parents in the study did report improvement in their children’s symptoms. It is also worth noting that the participants in the study only stayed on the diet for 6 weeks, which may be too short of a duration to see significant improvement. The results of another study that was presented at the 9th
ABSTRACT & COMMENTARY
Gliaden Reactivity Associated With Autism Matthew Baral, ND

12 ©2013 NATURAL MEDICINE JOURNAL. ALL RIGHTS RESERVED. NMJ, SEPTEMBER 2013 SUPPLEMENT—VOL 5, NO. 9 (SUPPL)
ABSTRACT & COMMENTARY
Annual International Meeting for Autism Research also suggest that the GFCF diet is not effective.14 This research made headlines and was discussed extensively in the media as the definitive answer as to whether this treatment can be helpful. The design of this study was flawed in several ways. The study only included 14 participants, and they were put on a GFCF diet for only 4 weeks, which in my experience is not enough time. Furthermore, when challenging potentially offending dairy and wheat products in the diet, participants were not on a strict GFCF diet, which would obviously skew the results. Most importantly, patients who had gastrointestinal symptoms were eliminated from the study, which seems counterintuitive. Those patients are the ones who might benefit most from this diet, so eliminating those patients would also certainly affect the results.
As for positive findings in the research, a small study (N=7) at Bastyr University did not show changes in the Gastrointestinal Symptoms Rating Scale (GSRS) or Childhood Autism Rating Scale (CARS), but parents of all children on the GFCF diet did report improvement of gastrointestinal symptoms and behaviors.15 At Pennsylvania State University, a parent-questionnaire study of 387 children with autism that have implemented the diet showed improvements in autistic behaviors, physiological symptoms, and other social behaviors.16
When considering treatments for children with autism, it is of utmost importance to consider all research on a particular therapy. However, not all safe and effective treatments have large bodies of data supporting their benefits. In such cases those who practice a biomedical approach to autism care may need to depend on information passed anecdotally. Therefore, a reasonable approach would be to weigh the benefits versus the risk of adverse effects of a therapy and proceed prudently.
REFERENCES1 Barcia G, Posar A, Santucci M, Parmeggiani A. Autism and
coeliac disease. J Autism Dev Disord. 2008;38(2):407-408.2 Warren RP, Margaretten NC, Pace NC, Foster A. Immune
abnormalities in patients with autism. J Autism Dev Disord. 1986;16(2):189-197.
3 Gupta S, Aggarwal S, Heads C. Dysregulated immune system in chil-dren with autism: beneficial effects of intravenous immune globulin on autistic characteristics. J Autism Dev Disord. 1996;26(4):439-452.
4 Singh VK, Warren RP, Odell JD, Warren WL, Cole P. Antibodies to myelin basic protein in children with autistic behavior. Brain Behav Immun. 1993;7(1):97-103.
5 Cuchacovich M, Gatica H, Vial P, Yovanovich J, Pizzo SV, Gonzalez-Gronow M. Streptokinase promotes development of dipeptidyl peptidase IV (CD26) autoantibodies after fibrino-lytic therapy in myocardial infarction patients. Clin Diagn Lab Immunol. 2002;9(6):1253-1259.
6 Vojdani A, Bazargan M, Vojdani E, et al. Heat shock protein and gliadin peptide promote development of peptidase antibodies in children with autism and patients with autoimmune disease. Clin Diagn Lab Immunol. 2004;11(3):515-524.
7 Vojdani A, Pangborn JB, Vojdani E, Cooper EL. Infections, toxic chemicals and dietary peptides binding to lymphocyte recep-tors and tissue enzymes are major instigators of autoimmunity in autism. Int J Immunopathol Pharmacol. 2003;16(3):189-199.
8 Vojdani A, O’Bryan T, Green JA, et al. Immune response to dietary proteins, gliadin and cerebellar peptides in children with autism. Nutr Neurosci. 2004;7(3):151-161.
9 Frye RE. Seizures in autism spectrum disorder. Talk About Curing
Autism. http://www.tacanow.org/family-resources/seizures. Updated December 27, 2012. Accessed August 22, 2013.
10 Jyonouchi H, Sun S, Itokazu N. Innate immunity associated with inflammatory responses and cytokine production against common dietary proteins in patients with autism spectrum disorder. Neuro-psychobiology. 2002;46(2):76-84.
11 Jyonouchi H, Geng L, Ruby A, Reddy C, Zimmerman-Bier B. Eval-uation of an association between gastrointestinal symptoms and cytokine production against common dietary proteins in children with autism spectrum disorders. J Pediatr. 2005;146(5):605-610.
12 Ashwood P, Anthony A, Torrente F, Wakefield AJ. Spontaneous mucosal lymphocyte cytokine profiles in children with autism and gastrointestinal symptoms: mucosal immune activation and reduced counter regulatory interleukin-10. J Clin Immunol. 2004;24(6):664-673.
13 Elder JH, Shankar M, Shuster J, Theriaque D, Burns S, Sherrill L. The gluten-free, casein-free diet in autism: results of a preliminary double blind clinical trial. J Autism Dev Disord. 2006;36(3):413-420.
14 Hyman S. 9th Annual International Meeting for Autism Research: Abstract 140.007. Presented May 22, 2010.
15 Harris C, Card B. A pilot study to evaluate nutritional influences on gastrointestinal symptoms and behavior patterns in chil-dren with Autism Spectrum Disorder. Complement Ther Med. 2012;20(6):437-440.
16 Pennesi CM, Klein LC. Effectiveness of the gluten-free, casein-free diet for children diagnosed with autism spectrum disorder: based on parental report. Nutr Neurosci. 2012;15(2):85-91.

It took 57 years, 130 patentsand 70 human clinical trials
to get from here to here
*These statements have not been evaluated by the Food and Drug Administration. This product is not intended to diagnose, treat, cure, or prevent any disease. Building a Better Mineral™
For 57 years, Albion has been the leading global supplier of chelated minerals. Through our decades of research, acquisition of 130 patents and results from 70 human clinical trials, we’ve learned a thing or two about how to chelate minerals. Better yet, we’ve converted this extensive body of scientific knowledge into a six-stage process for building chelated minerals that are, not only more effective, but also safer, easier to absorb, and gentle on the stomach.* If you thought chelated minerals were all the same, it’s time you discovered Albion’s six steps for building more effective, more absorbable and more easily tolerated chelated minerals.*
www.AlbionMinerals.com 1-800-222-0733
Albion builds a betterchelated mineral in six stages: 1
Start with high quality raw materials
2 3Use patented chelation and
bonding technology 4
Employ proven manufacturing
processes
6Continue
research and development5
Validatestructure using
FT-IR
Select quality organic ligands

14 ©2013 NATURAL MEDICINE JOURNAL. ALL RIGHTS RESERVED. NMJ, SEPTEMBER 2013 SUPPLEMENT—VOL 5, NO. 9 (SUPPL)
PEER-REVIEWED ARTICLE
Literature Review: Probiotics for the Treatment of Irritable Bowel SyndromeBy Lise Alschuler, ND, FABNO, and Karolyn A. Gazella
ABSTRACTInterest in the use of probiotics to treat irritable bowel syndrome (IBS) has increased considerably over the past several years. The literature now provides us with a distinct picture as to how these beneficial bacteria impact health and relieve IBS symptoms. In many cases, probiotics can be a first-line treatment choice and provide a viable alternative to existing treatments that lack efficacy and may cause side effects. While more data is needed regarding strain, dosage, and sub-type application, it is clear that multistrain probiotics can play a significant clinical role in the treatment of IBS.
INTRODUCTIONIrritable bowel syndrome (IBS) is not a disease, but rather a functional gastrointestinal disorder. It has characteristic symp-toms, the presence of which elucidate accurate diagnosis. IBS is a diagnosis of exclusion, and it is important to rule out other organic pathologies before making the final diagnosis and proceeding to treatment. Prevalence statistics vary dramati-cally, but most studies have shown that approximately 10% to 15% of the US population is affected by this disorder.1 Many experts believe prevalence may be higher, affecting up to 40% of adults in the United States.2 This prevalence range may be the result of the fact that less than 30% of people affected see their doctor for appropriate diagnosis and treatment.3 IBS can be difficult to diagnose because it is not associated with structural or tissue abnormalities. As such, physicians must rely solely on symptom presentation to make the diagnosis.
The Rome criteria were developed to classify functional gastrointestinal disorders based on clinical symptoms. The most recent revision is Rome III, in which IBS is diagnosed based on the following criteria:4
• symptom onset at least 6 months prior to diagnosis
• recurrent abdominal pain or discomfort (ie, an uncomfort-able sensation, not pain) for at least 3 days per month during the prior 3 months
• in addition to recurrent abdominal pain or discomfort, at least 2 of the following must also be present:
1. symptom improvement with defecation
2. onset associated with change in frequency of stool
3. onset associated with a change in the form or appear-ance of stool
The Rome criteria specify that in order for a person to be eligible for pathophysiological research in clinical trials, he should report pain and/or discomfort frequency of at least 2 days per week during the screening evaluation.
The National Institute of Diabetes and Digestive and Kidney Diseases (NIDDK), National Institutes of Health, has iden-tified 4 subtypes of IBS that help drive treatment decisions. The following categorizations are based on percentage of all bowel movements over a representative time period:5
1. IBS with constipation
—hard or lumpy stools at least 25%
—loose or watery stools less than 25%
2. IBS with diarrhea
—loose or watery stools at least 25%
—hard or lumpy stools less than 25%
3. Mixed IBS
—hard or lumpy stools at least 25%
—loose or watery stools at least 25%
4. Unsubtyped IBS
—hard or lumpy stools less than 25%
—loose or watery stools less than 25%
The NIDDK National Digestive Disease Information Clear-inghouse also states that secondary symptoms can include abdominal bloating, passing mucus, or feeling that the bowel movement was unproductive or incomplete.
Previously, IBS was thought to be a psychosomatic disorder; however, research has advanced our understanding of IBS to

NMJ, SEPTEMBER 2013 SUPPLEMENT—VOL 5, NO. 9 (SUPPL) ©2013 NATURAL MEDICINE JOURNAL. ALL RIGHTS RESERVED. 15
include an organic etiology linked to altered gut microbiota and low-grade inflammation.6
Presently, conventional treatment for IBS symptoms includes the use of nutritional counseling, fiber or laxatives such as lubiprostone (Amitiza), prescription antispasmodics, or prescription antidepressants. The high treatment failure rate of current conventional management, combined with a chal-lenging side effect profile associated with the drug therapy has prompted new explorations into the etiology and treat-ments of IBS. Foremost among these new approaches is the understanding of underlying dysbiosis as a prime cause of IBS, with the attendant rationale for the use of probiotics as a leading treatment.7–9
PATHOPHYSIOLOGYWhile the specific cause of IBS remains somewhat unclear and continues to be debated, several well-established hypoth-eses exist regarding the pathophysiology of the condition. IBS is essentially a disorder of gut motility,10 characterized by hypertonic segmental contractions (spastic constipa-tion) alternating with hypomotile bowel or increased peri-staltic contractions (diarrhea). Several factors contribute to this disordered bowel motility. Food intolerance, consid-ered a major contributing factor, is estimated to affect up to 50% of all patients with IBS.11 For example, studies have shown that inadequate carbohydrate digestion can provoke IBS symptoms.12 Serotonin receptor hypersensitivity in the bowel wall resulting in abnormal peristaltic contractions has also been implicated in IBS.13 Serotonin dysregulation can be provoked by acute histamine-mediated inflammation or significant stress with resultant increased secretion of corti-cotropin releasing factor and IL-1, which in turn stimulate the intestinal release of 5-hydroxytryptophan and activation of serotonin receptors. Alterations in bowel flora and associ-ated immune dysregulation are also recognized as key factors in IBS.14 This review will focus on the pathophysiology of dysbiosis and immune dysregulation in IBS, and how probi-otics may be indicated in treating patients with IBS.
From an immunoregulation standpoint, studies demon-strate that commensal bacteria provide an environment that encourages the effective modulation of both innate and adaptive immunity.15 Immunoregulation is also intimately connected to the composition of the microbiota environment in the gut.16 Additionally, immune homeostasis is critical to the control of inflammatory processes that can exac-
erbate IBS. In 2007, Liebregts and colleagues demonstrated that IBS patients had significantly higher proinflammatory markers, specifically TNF-alpha, IL-1beta, IL-6, and LPS-induced IL-6 levels.17 Immunoregulatory dysfunction has been found in IBS patients both mucosally, as well as system-ically via a decrease of T regulatory cells.18 T regulatory cells, also known as suppressor T cells, play a critical role in gut-associated lymphoid tissue (GALT) antigen sampling and tolerance.19 Decreased intestinal T regulatory cells increase immune-mediated inflammation in response to ingested food compounds and intestinal microflora. This, in turn, alters the migratory motor complex of the intestines and contributes to the altered motility characteristics of IBS.
In large measure, due to the immune-disrupting effects from altered intestinal microflora, dysbiosis is a main etiologic factor in the development and worsening of IBS.20 Further-more, the subsequent correction of this imbalance may be an effective treatment for this condition.21
When the state of equilibrium in the large intestines is disrupted to favor an overgrowth of harmful bacteria, low-grade inflammation and immune dysregulation can result.22 Correcting large intestinal dysbiosis will in turn reverse inflammatory responses and normalize immunoregulation in the gut. A review by Hemarajata and Versalovic reinforce data showing that probiotics positively influence the compo-sition and function of internal microbial communities and can reverse large intestinal dysbiosis, thereby alleviating corre-sponding IBS symptoms.23
Dysbiosis in the form of bacterial overgrowth in the small intes-tines is referred to as small intestinal bowel overgrowth (SIBO) syndrome and has been implicated in IBS. In 2000, Pimentel and colleagues found that of their 202 patients with IBS, 78% had SIBO.24 In 2005, Nucera et al found that 65% of their 98 patients with IBS had SIBO.25 SIBO can be diagnosed via
“”
When the state of equilibrium
in the large intestines is disrupted
to favor an overgrowth of harmful
bacteria, low-grade inflammation and
immune dysregulation can result.

16 ©2013 NATURAL MEDICINE JOURNAL. ALL RIGHTS RESERVED. NMJ, SEPTEMBER 2013 SUPPLEMENT—VOL 5, NO. 9 (SUPPL)
breath trace-gas analysis. Hydrogen/methane breath tests have been shown to have good sensitivity and specificity and are less invasive than intubation and culture of intestinal aspirates.26 Both the Pimentel and Nucera studies utilized the breath trace-gas analysis. Most GI experts agree that SIBO plays a role in either the development or exacerbation of IBS symptoms.
Because correcting dysbiosis and SIBO plays a significant role in alleviation of IBS symptoms, proper diagnosis is important. Signs of dysbiosis can be detected in both stool and urine. One example of dysbiosis stool analysis is the Comprehen-sive Digestive Stool Analysis 2.0, which tests various aspects of digestion, absorption, microbiology, and metabolic markers.27
Normalizing the gut microbial environment and associated GALT immunity can improve symptoms and severity of IBS. Probiotics influence both mechanisms of action.
SYSTEMATIC REVIEWSMounting evidence demonstrates that probiotics can be a clinically valid tool in the treatment of IBS. Based on existing data, as well as probiotics’ safety profile, it is prudent to consider probiotics as a potential first-line treatment choice for many patients with IBS.
Within the past few years, several systematic reviews have been published on the topic of probiotics and the treatment of IBS. In 2009, Brenner and colleagues looked at 16 trials that met the following selection criteria:
• randomized clinical trial
• adults with IBS using Rome II criteria
• single or combination probiotic versus placebo
• improvement in IBS symptoms and/or decrease in frequency of adverse events reported
The analysis clearly reflected the lack of research rigor in this field up to that point. Eleven of the 16 trials evaluated had suboptimal study design and did not have adequate data about tolerability and adverse events. The review did show that in 2 of the well-designed studies, Bifidobacterium infantis 35624 demonstrated significant benefit in improving abdominal pain and discomfort, bloating and distention, and/or constipation when compared to placebo.28
A meta-analysis in 2009 reviewed 14 randomized placebo-controlled trials in which the trials also varied in terms of length of treatment, dose, strains, and strengths of the probi-
otics. Their combined data, however, did show modest improvement in overall symptoms.29
A 2010 review looked at 19 random clinical trials. In this review, Moayyedi P et al found that overall the trial quality was good and that “probiotics were statistically significantly better than placebo.”30
The most extensive review done to date was completed and published in 2012 and looked at 42 trials. Clarke and colleagues found that 34 of the 42 trials reported beneficial effects in at least one of the symptom endpoints established.31 However, these researchers also pointed out deficits in trial design that included inconsistencies in strain and dosage. The researchers conclude: “Recent incremental advances suggest these areas are being addressed and that the future holds much promise for the use of lactic acid bacteria in the treatment of irritable bowel syndrome.”
Of note, there was minor overlap between the 2010 and 2012 systematic reviews with Clarke et al presenting the most comprehensive information available to date.
RECENT RANDOMIZED CLINICAL TRIALSA 2010 randomized, double-blind, placebo-controlled trial using a multistrain probiotic for 6 months found improve-ment in dysbiosis (P=0.02) and overall GI microbiota.32 The intervention in this study included 4 different strains, including Lactobacillus rhamnosus GG, Lactobacillus rham-nosus Lc705, Propionibacterium freudenreichii ssp. Shermanii JS, and Bifidobacterium breve Bb99. The researchers note that this same combination of strains had been shown previ-ously to alleviate IBS symptoms; their study confirms the mechanism of action.
A study published in 2012 used “adequate relief (AR) of overall IBS symptoms” as its primary outcome measure for the 50 IBS patients they assessed weekly for a 10-week period. The treatment consisted of 7 species (Lactobacillus acidoph-ilus, Lactobacillus plantarum, Lactobacillus rhamnosus, Bifi-
“”
Over the past several years, the
number of studies involving
probiotics for the treatment of IBS
has been growing.
NMJ, SEPTEMBER 2013 SUPPLEMENT—VOL 5, NO. 9 (SUPPL) ©2013 NATURAL MEDICINE JOURNAL. ALL RIGHTS RESERVED. 17
dobacterium breve, Bifidobacterium lactis, Bifidobacterium longum, and Streptococcus thermophiles). Reported AR was consistently higher in the probiotic group versus placebo (P<0.05).33 Profiles of fecal flora taken before and after the study also demonstrated that the probiotic mixture stabi-lized intestinal microbiota. The researchers concluded that the stabilization of the intestinal microbiota helped explain the therapeutic effects of the probiotic intervention.
Capello and colleagues published their randomized clinical trial in 2013 showing that a multistrain probiotic (Lacto-bacillus plantarum, Lactobacillus reuteri, Lactobacillus casei, Lactobacillus rhamnosus, Bifidobacterium infantis, Bifido-bacterium longum, Lactobacillus salivarius, Lactobacillus acidophilus, Streptococcus thermophilus, and Lactobacillus sporogenes) decreased the severity of flatulence in the 64 IBS patients they studied (P<0.05).34 However, the study did not find “improvement in global satisfactory relief of abdominal flatulence and bloating.”
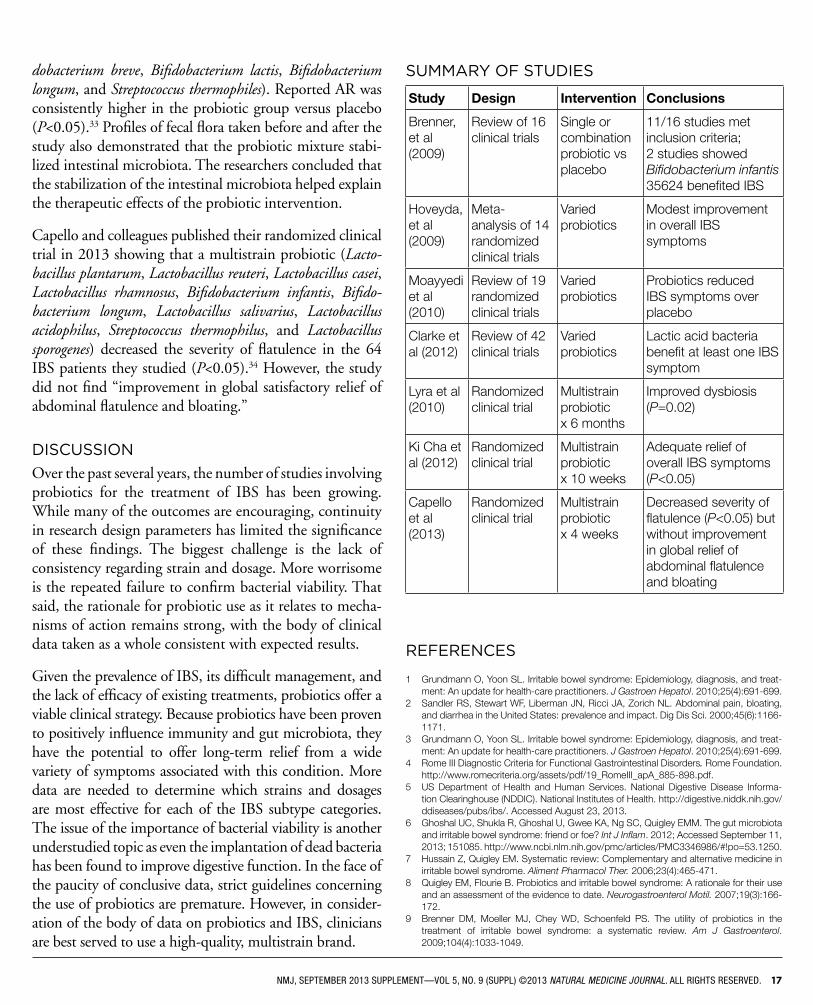
DISCUSSIONOver the past several years, the number of studies involving probiotics for the treatment of IBS has been growing. While many of the outcomes are encouraging, continuity in research design parameters has limited the significance of these findings. The biggest challenge is the lack of consistency regarding strain and dosage. More worrisome is the repeated failure to confirm bacterial viability. That said, the rationale for probiotic use as it relates to mecha-nisms of action remains strong, with the body of clinical data taken as a whole consistent with expected results.
Given the prevalence of IBS, its difficult management, and the lack of efficacy of existing treatments, probiotics offer a viable clinical strategy. Because probiotics have been proven to positively influence immunity and gut microbiota, they have the potential to offer long-term relief from a wide variety of symptoms associated with this condition. More data are needed to determine which strains and dosages are most effective for each of the IBS subtype categories. The issue of the importance of bacterial viability is another understudied topic as even the implantation of dead bacteria has been found to improve digestive function. In the face of the paucity of conclusive data, strict guidelines concerning the use of probiotics are premature. However, in consider-ation of the body of data on probiotics and IBS, clinicians are best served to use a high-quality, multistrain brand.
SUMMARY OF STUDIES
Study Design Intervention Conclusions
Brenner, et al (2009)
Review of 16 clinical trials
Single or combination probiotic vs placebo
11/16 studies met inclusion criteria; 2 studies showed Bifidobacterium infantis 35624 benefited IBS
Hoveyda, et al (2009)
Meta-analysis of 14 randomized clinical trials
Varied probiotics
Modest improvement in overall IBS symptoms
Moayyedi et al (2010)
Review of 19 randomized clinical trials
Varied probiotics
Probiotics reduced IBS symptoms over placebo
Clarke et al (2012)
Review of 42 clinical trials
Varied probiotics
Lactic acid bacteria benefit at least one IBS symptom
Lyra et al (2010)
Randomized clinical trial
Multistrain probiotic x 6 months
Improved dysbiosis (P=0.02)
Ki Cha et al (2012)
Randomized clinical trial
Multistrain probiotic x 10 weeks
Adequate relief of overall IBS symptoms (P<0.05)
Capello et al (2013)
Randomized clinical trial
Multistrain probiotic x 4 weeks
Decreased severity of flatulence (P<0.05) but without improvement in global relief of abdominal flatulence and bloating
REFERENCES
1 Grundmann O, Yoon SL. Irritable bowel syndrome: Epidemiology, diagnosis, and treat-ment: An update for health-care practitioners. J Gastroen Hepatol. 2010;25(4):691-699.
2 Sandler RS, Stewart WF, Liberman JN, Ricci JA, Zorich NL. Abdominal pain, bloating, and diarrhea in the United States: prevalence and impact. Dig Dis Sci. 2000;45(6):1166-1171.
3 Grundmann O, Yoon SL. Irritable bowel syndrome: Epidemiology, diagnosis, and treat-ment: An update for health-care practitioners. J Gastroen Hepatol. 2010;25(4):691-699.
4 Rome III Diagnostic Criteria for Functional Gastrointestinal Disorders. Rome Foundation. http://www.romecriteria.org/assets/pdf/19_RomeIII_apA_885-898.pdf.
5 US Department of Health and Human Services. National Digestive Disease Informa-tion Clearinghouse (NDDIC). National Institutes of Health. http://digestive.niddk.nih.gov/ddiseases/pubs/ibs/. Accessed August 23, 2013.
6 Ghoshal UC, Shukla R, Ghoshal U, Gwee KA, Ng SC, Quigley EMM. The gut microbiota and irritable bowel syndrome: friend or foe? Int J Inflam. 2012; Accessed September 11, 2013; 151085. http://www.ncbi.nlm.nih.gov/pmc/articles/PMC3346986/#!po=53.1250.
7 Hussain Z, Quigley EM. Systematic review: Complementary and alternative medicine in irritable bowel syndrome. Aliment Pharmacol Ther. 2006;23(4):465-471.
8 Quigley EM, Flourie B. Probiotics and irritable bowel syndrome: A rationale for their use and an assessment of the evidence to date. Neurogastroenterol Motil. 2007;19(3):166-172.
9 Brenner DM, Moeller MJ, Chey WD, Schoenfeld PS. The utility of probiotics in the treatment of irritable bowel syndrome: a systematic review. Am J Gastroenterol. 2009;104(4):1033-1049.

18 ©2013 NATURAL MEDICINE JOURNAL. ALL RIGHTS RESERVED. NMJ, SEPTEMBER 2013 SUPPLEMENT—VOL 5, NO. 9 (SUPPL)
10 Bassotti G, Crowell MD, Cheskin LJ, Chami TN, Schuster MM, Whitehead WE. Physiological correlates of colonic motility in patients with irritable bowel syndrome. Z Gastroenterol. 1998;36(9):811-817.
11 Simren M, Mansson A, Langkilde AM, et al. Food-related gastrointestinal symptoms in the irritable bowel syndrome. Digestion. 2001;63(2):108-115.
12 Nanda R, James R, Smith H, Dudley CR, Jewell DP. Food intolerance and the irritable bowel syndrome. Gut. 1989;30(8):1099-1104.
13 Sanger GJ. Hypersensitivity and hyperreactivity in the irritable bowel syndrome: An opportunity for drug discovery. Dig Dis. 1999;17(2):90-99.
14 King TS, Elia M, Hunter JO. Abnormal colonic fermentation in irritable bowel syndrome. Lancet. 1998;352(9135):1187-1189.
15 Chow J, Lee SM, Shen Y, Khosravi A, Mazmanian SK. Host-bacterial symbiosis in health and disease. Adv Immunol. 2010;107:243–274.
16 Schiffrin EJ, Blum S. Interactions between the microbiota and the intestinal mucosa. Eur J Clin Nutr. 2002;56(supplement 3):S60–S64.
17 Liebregts T, Adam B, Bredack C, et al. Immune activation in patients with Irritable Bowel syndrome. Gastroenterol. 2007;132(3):913–920.
18 Konieczna P, Akdis CA, Quigley EM, Shanahan F, O’Mahony L. Portrait of an immu-noregulatory bifidobacterium. Gut Microbes. 2012;3(3):261-266.
19 Keren DF. Intestinal mucosal immune defense mechanisms. Am J Surg Pathol. 1988;12 Suppl 1:100-105.
20 Quigley EM. Do patients with functional gastrointestinal disorders have an altered gut flora? Therap Adv Gastroenterol. 2009;2(4 Suppl):23–30.
21 Lee BJ, Bak YT. Irritable bowel syndrome, gut microbiota and probiotics. J Neurogas-troenterol Motil. 2011;17(3):252–266.
22 Hemarajata P, Versalovic J. Effects of probiotics on gut microbiota: mechanisms of intestinal immunomodulation and neuromodulation. Ther Adv in Gastroenterol. 2013;6(1)39-51.
23 Ibid
24 Pimentell M, chow EJ, Lin HC. Eradication of small intestinal bacterial over-growth reduces symptoms of irritable bowel syndrome. Am J Gastroenterol. 2000;95(12):3503-3506.
25 Nucera G, Gabrielli M, Lupascu A, et al. Abnormal breath tests to lactose, fructose and sorbitol in irritable bowel syndrome may be explained by small intestinal bacterial overgrowth. Alimentary Pharmacology & Therapeutics. 2005;21(11):1391-1395.
26 Bacterial Overgrowth of the Small Intestine Breath Test. Asheville, North Carolina: Genova Diagnostics; 2009: 1-8. http://www.gdx.net/core/application-guides/Bacte-rial-Overgrowth-Application-Guide.pdf.
27 Genova Diagnostics. Genova Diagnostics Testing. http://www.gdx.net. Accessed July 14, 2013.
28 Brenner DM, Moeller MJ, Chey WD, Schoenfeld PS. The utility of probiotics in the treatment of irritable bowel syndrome: a systematic review. Am J Gastroenterol. 2009;104(4):1033-1049.
29 Hoveyda N, Heneghan C, Mahtani KR, Perera R, Roberts N, Glasziou P. A systematic review and meta-analysis: probiotics in the treatment of irritable bowel syndrome. BMC Gastroenterology. 2009;9(15).
30 Moayyedi P, Ford AC, Talley NJ, et al. The efficacy of probiotics in the treatment of irritable bowel syndrome: a systematic review. Gut. 2010;59(3):325-332.
31 Clarke G, Cryan JF, Dinan TG, Quigley EM. Review Article: Probiotics for the treat-ment of irritable bowel syndrome. Aliment Pharmacol Ther. 2012;35(4):403-413.
32 Lyra A, Krogius-Kurikka L, Nikkilä, et al. Effect of a multispecies probiotic supplement on quantity of irritable bowel syndrome-related intestinal microbial phylotypes. BMC Gastroenterology. 2010;10:110.
33 Ki Cha B, Mun Jung S, Hwan Choi C, et al. The effect of a multispecies probiotic mixture on the symptoms and fecal microbiota in diarrhea-dominant irritable bowel syndrome: a randomized, double-blind, placebo-controlled trial. J Clin Gastroenterol. 2012;46(3):220-227.
34 Cappello C, Tremolaterra F, Pascariello A, Ciacci C, Iovino P. A randomised clinical trial (RCT) of a symbiotic mixture in patients with irritable bowel syndrome (IBS): Effects on symptoms, colonic transit and quality of life. Int J Colorectal Dis. 2013;28:349-358.
Looking for an easy way to
diagnose SIBO?Hydrogen/Methane Breath Testing from Commonwealth Labs, Inc., provides a fast, reliable and
convenient diagnostic tool for identifying Small Intestinal Bacterial Overgrowth (SIBO), a leading cause of the symptoms associated with Irritable Bowel Syndrome (IBS).
We make it easy for you and your patient!
TesT menu: Small Intestinal Bacterial Overgrowth (SIBO) • Lactose Intolerance • Fructose Intolerance • Sucrose Intolerance • H.Pylori
39 Norman Street • Salem, MA 01970Tel: 800.292.9019 • Fax: 781.659.0705
www.hydrogenbreathtesting.com
• Easy to use take-home test kit: After specimen collection, ship back to lab for analysis via UPS at no charge.
• 24-hour turnaround time: Results within 12-24 hours of receipt of test. Available via secure fax, email or online portal.
Breathe a little easier.

20 ©2013 NATURAL MEDICINE JOURNAL. ALL RIGHTS RESERVED. NMJ, SEPTEMBER 2013 SUPPLEMENT—VOL 5, NO. 9 (SUPPL)
BOOK REVIEW
Enteroimmunology: A guide to prevention and treatment of chronic disease, by Charles Lewis, MD, MPHReview by Teresa Silliman, ND
A book’s table of contents is often a telling first glimpse of what to expect from the book—not just in terms of content, as the name would imply, but also in terms of style, tone, and personality. So when I opened Enteroimmunology: A guide to prevention and treatment of chronic disease, by Charles A. Lewis, MD, MPH, my interest was piqued immediately. With chapter titles like Meteorism, Trots and Foul Winds; Appetite, Satiation and Satiety; and Obesity, Syndrome X and the Company it Keeps, how could it not be?
Enteroimmunology is a field of medicine that focuses on how the enteric immune system’s response to bacteria, toxins (parasitic or food metabolites), and foreign proteins elicits inflammation and influences all other body systems. This book covers enteroimmunology as it relates to such diverse topics as acne, rage, biofilms, interstitial cystitis, diabetes, obesity, cancer, migraines, depression, sleep, osteoporosis, and autoimmune disease. It also covers stan-dard gastrointestinal (GI) conditions: small intestinal bacte-rial overgrowth (SIBO), dysbiosis, gluten disease, leaky gut, inflammatory bowel disease, and irritable bowel syndrome. The first 7 chapters cover the basics: GI function overview, proteins, fats, carbohydrates, sugar malabsorption (the aforementioned “Meteorism, Trots and Foul Winds”), and the colon and its inhabitants. I enjoyed the overview and learned quite a few more details that are applicable in my daily practice of naturopathic medicine. For example, the thorough table outlining the hormones that affect the GI tract will become a quick, easy reference in my practice. I also appreciate that each chapter is only a few pages but does not lack for depth of information. After the quick overview, the author delves into the nitty gritty of more complicated issues—hyperammonia, enteroimmune depression, leptin resistance, mast cell activation disorder, and leukotriene-associated hypersensitivity.
Naturopathic doctors are trained to have a very good base of knowledge when it comes to the digestive system and how it affects health. We are thoroughly educated in nutrition and how the foods we eat or don’t eat can cause or perpetuate
disease states. However, details and intricacies unique to each individual can be very difficult to tease out. As one example, I have a mother and daughter who react to every-thing. They react to certain foods, most supplements, some herbs, and most synthetic agents. For the mom, her issue is chronic sinus and bronchial issues. Her daughter gets skin reactions from acne to perioral dermatitis. After many years and trying every assessment and treatment I could think of, we’ve achieved a degree of success, but their symptoms still recur intermittently. I felt like I had run out of ways to help them before reading this textbook, which contains at least 8 chapters on immune hypersensitivity. In a brief aside, “Histamine in Pregnancy,” Lewis explains that the placenta creates an increased amount of diamine oxidase (DAO), which is the enzyme that catabolyzes/inactivates histamine. He writes, “High DAO levels may explain why some women feel so much better during pregnancy and also explain the reduction in the frequency of migraines and other histamine reactions during pregnancy. High DAO levels lower histamine reactions through much of the preg-nancy and protect pregnant women from biogenic amines that otherwise have them not feel so well.”
With the mother and daughter I was treating, the daughter had just given birth, and she had not experienced any of her

NMJ, SEPTEMBER 2013 SUPPLEMENT—VOL 5, NO. 9 (SUPPL) ©2013 NATURAL MEDICINE JOURNAL. ALL RIGHTS RESERVED. 21
usual hypersensitivities during her entire pregnancy. Perhaps the daughter benefited from the placental DAO, I thought. This idea solidified as I read the very detailed chapter on Mast Cell Activation Disorder. After reading and rereading this chapter, I have a few leads on where to go next to address my complicated hyperreactive patients.
This textbook is full of factoids and details that can be applied to daily practice. I found information on carbohydrates that was useful—especially if you utilize the fermentable oligosaccha-rides, disaccharides, monosaccharides, and polyols (FODMAP) or SIBO diets in your practice. Each chapter is short and to the point and includes tables summarizing necessary details and references to other chapters to garner further clarification on difficult points. I also like that the author summarizes every chapter; at the end of the Leaky Gut chapter is a 20-point list on treating leaky gut, and only a few of the points are about a supplement. Lewis’s book is not a primer on what supple-ment to recommend but on what the possible causes or main-taining stressors are that perpetuate a state of disease. This is not another book on green pharmacy, but a book that follows the tenets of naturopathic medicine—treat the whole person, find the cause, and use food as your medicine.
FROM THE AUTHORS OF The Definitive Guide to Cancer
NOW AVAILABLE
The Definitive Guide to Thriving After Cancer by Lise Alschuler, ND, FABNO,and Karolyn A. Gazella
This book is a completely revised and updated edition of the previously titled Five to Thrive. Featuring the Five to Thrive® Plan, The Definitive Guide to Thriving After Cancer is written for people who are motivated to prevent cancer or its recurrence.
Order online at or book stores throughout North America. Quantity discounts are available by calling Random House at 1-800-733-3000. For more information visit www.FivetoThrivePlan.com.
In summary, I thoroughly enjoyed this textbook. I look forward to reading it more as I pick up some new tidbits that I can apply to my practice. I also enjoy Lewis’ writing style: He is clear and straightforward, and I can sense that he has plenty of experience behind what he is saying. I enjoy the sense of humor sprinkled throughout the book. This textbook does have its share of typo-graphical errors and forgotten prepositions, but that seems a silly demerit when the content is so exceptional. Every physician should have this insightful book at his or her side—especially those practitioners who follow the tenets of naturopathic medicine.
ABOUT THE AUTHORCharles A. Lewis, MD, MPH, is a independent consul-tant to biomedial and technology companies. He also has more than 20 years in family practice medicine. He received his medical doctorate from Universidad de Tech-nologia de Santiago in the Dominican Republic and his master of public health from the University of Alabama at Birmingham.

22 ©2013 NATURAL MEDICINE JOURNAL. ALL RIGHTS RESERVED. NMJ, SEPTEMBER 2013 SUPPLEMENT—VOL 5, NO. 9 (SUPPL)
EXPERT Q & A
The Role of Digestive Enzymes in Gastrointestinal HealthA discussion with researcher M. Mamadou, PhD
Q. What role does poor digestion play in digestive discomfort and digestive disorders?
A. Digestion is a complex process that starts in the mouth and continues throughout the alimentary canal. First, the foods must be processed. This processing must be done progressively as the foods move from one section of the digestive system to the next. Any impairment in the process at any one segment can, over time, lead to complications ranging from discom-fort to major disorders. Heartburn, colic, bloating, flatulence, and various bowel inflammations are all examples of condi-tions resulting from an impaired digestive system. Proper diet followed by an adequate and timely digestive process consti-tutes the first and last line of defense not only in maintaining gut health, but also in promoting overall general health.
Q. Conventional medicine often looks at diges-tive issues as an overproduction of acid. What is your view of this approach?
A. In many cases, the overproduction of acid is an attempt by the stomach (the organ responsible for producing the hydrochloric acid) to enhance the digestion of the proteins. This acid plays an important role in helping the digestion of proteins, and also in facilitating the absorption of minerals and some vitamins. However, as in most cases, the gut is no exception. The excess of anything could create problems. Thus, excess acid production must be avoided, and a good digestive function can do that.
When acid production is in excess, a healthy alternative approach is to improve the diet to make it more digestible, and to improve the digestive process so foods do not stay in the stomach too long and continue to stimulate acid production. Supplemental digestive enzymes that are proven effective in the conditions prevailing in the stomach and other segments of the alimentary canal can enhance the digestive process.
Q. What are the main enzymes used as supple-mental digestive enzymes?
• Proteases help break down proteins, which are very difficult to digest. No single protease can digest all proteins efficiently.
In digestive enzyme formulations, it is recommended to use a blend of proteases, also called proteolytic enzymes. Pepti-dases are also in this group. When proteins are not properly digested, they could create systemic health problems such as inflammation and behavior issues. They could also promote formation of foul-smelling gases when they are fermented by the microorganisms in the large intestine.
• Lipase helps digest fats. In the area of supplemental diges-tive enzymes, there are various lipases used, mostly based on their fungal sources. Improper digestion of fats could lead to diarrhea and deficiency of the fat-soluble vitamins A, D, E, and K.
• Amylase helps digest starch. Improperly digested starch could reach the large intestine and cause major gas formation.
• Cellulase helps break down the big molecules of cellu-lose found in plant foods. Cellulose is a fibrous molecule that also serves to cement many other health-promoting molecules in the plant-derived foods, so it is important to digest it. However, no human cell produces the enzyme cellulase necessary to break down cellulose. By incorpo-rating the enzyme cellulase in digestive enzyme formula-tions, we can digest cellulose molecules totally or partially to help free the various molecules in the plant-derived foods, but also to enhance the toxin-binding ability of the cellulose.
ABOUT THE EXPERT
M. Mamadou, PhD, is the chief science officer of Phytomedic Labs. He earned his doctorate from the University of Cincin-nati and has been actively involved in enzyme-based formulations for health and wellness. His present research activi-ties focus on isolating new phytochemicals and enzymes for dietary supplements. He has taught and conducted research at several universities and has provided consulting and research services for many health and nutrition companies, including EnzymeScience, Inc, a key sponsor of the Natural Medicine Journal.

NMJ, SEPTEMBER 2013 SUPPLEMENT—VOL 5, NO. 9 (SUPPL) ©2013 NATURAL MEDICINE JOURNAL. ALL RIGHTS RESERVED. 23
• Lactase breaks down lactose. Many people have lactose intol-erance because lactase is lacking or not working properly. A supplemental enzyme product containing lactase helps prevent the symptoms associated with lactose intolerance.
• Alpha galactosidase helps people tolerate beans and prevent the excess gas they can cause.
Q. How can supplemental digestive enzymes support overall digestive health?
A. By enhancing the breakdown of food molecules, supple-mental digestive enzymes reduce the digestive organs’ workload. Moreover, if foods are not digested in a timely manner, they tend to accumulate and promote potentially damaging local inflammations. If the walls of the intes-tines become damaged, intestinal permeability (ie, leaky gut syndrome) may occur. This condition can lead to the passage of relatively large food molecules into the general blood circulation.
The digestive system is very complex. It has a large surface area, and all the cells lining the alimentary canal are alive and continuously functional. While some of the molecules in the foods and beverages we consume are beneficial, others could be harmful. The cells of the intestinal lining have a replacement rate of 3–5 days. This high turnover rate implies a very active DNA metabolism, including DNA replica-tion to ensure continuity of the genetic make-up within the cells. Such continuous duplication and renewal of cells, with constant exposure to all types of outside molecules, makes the cells vulnerable to injury, including DNA mutations. A good way to maintain digestive health is to introduce healthy foods and ensure their digestibility.
It is important to remember that what goes on in the gut does not stay in the gut. This is critically important, because the gastrointestinal tract
• has its “own” nervous system that could function indepen-dently of the central nervous system.
• produces more serotonin than the rest of the body.
• has an intricate immune system that is continuously in contact with the rest of the immune system. An estimated 75% of the immune system in the body transits through the gastrointestinal tract.
A healthy diet, free of harmful components, supplemented with effective digestive enzymes, helps ensure digestive struc-tural and functional integrity, and thus its health.
Q. Are there any contraindications healthcare providers should keep in mind when using diges-tive enzymes in clinical practice?
A. For general digestive support, there are no known contra-indications against taking supplemental digestive enzymes. In some cases dealing with health challenges such as improper blood flow, inflammatory processes, and other systemic conditions beyond the gastrointestinal tract, check that the patient does not have blood-clotting disorders, as enzymes tend to thin the blood. Additionally, if a patient is taking other blood-thinning medications, there could be some synergistic effect that must be avoided.
Q. What should practitioners look for when choosing digestive enzymes to recommend to their patients?
A. The main points I recommend in selecting supplemental enzyme products are that the products should be made from effective enzymes that can sustain the conditions in the digestive system, and that they should be produced by reputable companies with good manufacturing practices and sound quality control protocols.
Over the years, I have visited and worked with enzyme producers, dietary supplement manufacturers, and enzyme product distributors that are very strong in every aspect of safety and quality and using standards and norms as in the pharmaceutical industry. Additionally, innovative approaches continue to be developed for selecting organisms that produce effective enzymes for use in the digestive process, inflamma-tion control, and even in cases of emergency dealing with stroke or heart attack.
These are some key points to consider when selecting an enzyme for gastrointestinal health:
• pH stability within the digestive system
• Effectiveness within the alimentary canal
• Lack of allergenicity or toxicity
Some of the key and reliable supplemental enzyme compa-nies have scientific, safety, and quality control staff that can address specific questions a practitioner may have to help in using the products.
For Dr M. Mamadou’s round-up of specific conditions that respond to digestive enzymes, visit Natural Medicine Journal
Naturopathic Physicians: Natural Medicine. Real Solutions.
S T A N D W I T H Y O U R N A T I O N A L A S S O C I A T I O N T O D A Y !
Americans’ demand for “natural medicine” is greater than ever before. This presents unlimited opportunities and significant challenges. While others provide care in natural medicine, NDs bring a profound, comprehensive, and unique quality to the table. We owe it to our patients and community to stand up for our profession to make clear that we are the experts in natural medicine.
A strong American Association of Naturopathic Physicians offers the best hope for continued growth and prosperity of the naturopathic profession. AANP’s support for the profession takes many forms. We produce a variety of tools and resources to help you build a successful practice. Our online “Find an ND” tool is a prime source of new patients for AANP members, with over 50,000 page views per month! (This number is sure to grow as AANP ramps up an aggressive public awareness campaign.) We are proud to report that our public policy efforts are achieving enormous successes. Our state licensure efforts are paying off (hooray Colorado!), and we are working tirelessly to enable licensed NDs to participate in health insurance if they so desire.
For these efforts to be successful, we need the entire naturopathic physician community to stand in support of these efforts. Please become an AANP member today. Use promotional code NMJ50 to receive $50 off your membership fee. Offer ends 10/15/2013.
We are mighty, as professionals, but we are too small in number to guarantee our inclusion in the future of impacting the world with our medicine. We must position ourselves as leaders. Together, we can create a future in which naturopathic medicine flourishes and our naturopathic whole is greater than the sum of our parts. Support your profession, and help us support you.
W W W . N A T U R O P A T H I C . O R G 818 18th Street NW, Washington, DC 20006 Tel 866.538.2267 Fax 202.237.8152
M E M B E R B E N E F I T S
ADVOCACY
Support state licensure and insurance coverage
NATURAL STANDARD ACCESS
Members receive a free subscription
ANNUAL CONFERENCE DISCOUNT
NDs can save $200 on registration
PRACTICE DEVELOPMENT LIBRARY
Stay up-to-date with the latest in marketing,
business management, HIPPA, and more
JOB BOARD
Access a national database of job opportunities AANP Board of Directors