special report ajog - cdn-cms.f-static.com · antiarrhythmic drugs by direct intra ... growing risk...
TRANSCRIPT

Special Report ajog.org
Successful in utero transesophageal pacingfor severe drug-resistant tachyarrhythmia
Julien Stirnemann, MD; Alice Maltret, MD; Ayman Haydar, MD; Bertrand Stos, MD; Damien Bonnet, MD;Yves Ville, MDSustained fetal tachyarrhythmia can evolve into a life-threatening condition in 40% of cases
when hydrops develops, with a 27% risk of perinatal death. Several antiarrhythmic drugs can
be given solely or in combination to the mother to achieve therapeutic transplacental con-
centrations. Therapeutic failure could lead to progressive cardiac insufficiency and restrict
therapeutic options to either elective delivery or direct fetal administration of antiarrhythmic
drugs, which may increase the risk of death. We report for the first time successful fetal
transesophageal pacing to treat a hydropic fetus with drug-resistant tachyarrhythmia.
Key words: fetal, fetoscopy, pacing, surgery, tachyarrhythmia
28-year-old pregnant mother, at 27
A 5/7 weeks of gestation in her sec-ond pregnancy was referred after thediscovery of a fetal tachyarrhythmia thathad been discovered by fetal ausculta-tion at routine follow-up evaluation.This pregnancy had been uneventful:ultrasound examinations were normalin the first and second trimester, andfetal movements remained normal.Fetal echocardiography diagnosed atrialflutter as the cause of tachyarrhythmia,with atrial and ventricular frequenciesof 440 and 220 bpm, respectively, thatwere compatible with a 2:1 atrial flutter(Figure 1, A) and moderate mitral andtricuspid regurgitations, which wereconsidered functional in the context.From Obstetrics and Maternal Fetal Medicine(Drs Stirnemann and Ville) and the M3C-Necker,Congenital and Pediatric Cardiology Unit (DrsMaltret, Haydar, Stos, and Bonnet), HôpitalNecker Enfants Malades, Université ParisDescartes, Paris, France.
Received Jan. 24, 2018; revised July 11, 2018;accepted July 19, 2018.
The authors report no conflict of interest.
Corresponding author: Julien Stirnemann, [email protected]
0002-9378/$36.00ª 2018 Published by Elsevier Inc.https://doi.org/10.1016/j.ajog.2018.07.018
320 American Journal of Obstetrics & Gynecology
The fetus was hydropic with moderatepericardial, thoracic, and peritoneal ef-fusions. After a normal electrocardio-gram and routine blood tests, themother was hospitalized and givendigoxin and flecainide.1e3 Serial follow-up echocardiography showed wors-ening of hydrops without return to si-nus rhythm. On day 7, treatment wasswitched for amiodarone.4 Steroids(betamethasone) were also given forfetal lung maturation.After 5 days of amiodarone, at 29 3/7
weeks of gestation, hydrops had wors-ened, with associating subcutaneousedema, with persisting atrial flutter, andwith worsening tricuspid and mitralregurgitations. Given the failure of 2lines of medical treatment and pro-gressive hydrops, in utero trans-esophageal pacing (IUTP) wasconsidered as a third-line option, alongwith elective delivery and third-lineantiarrhythmic drugs by direct intra-cordal administration. The mother wascounselled based on efficacy and safetyof transesophageal pacing in newborninfants with atrial flutter5,6 and on thepossible adverse events and inefficacy ofthird-line medical therapies and thegrowing risk of intrauterine fetaldeath.2,4 Preterm elective delivery wasnot considered a choice, given the earlygestational age. Despite the associatedrisk of iatrogenic preterm prematurerupture of the membranes and the
OCTOBER 2018
recent concerns raised by fetal anes-thesia,7 this innovative treatment wasadvised by both cardiologists and peri-natologists; the patient opted for feto-scopic IUTP.
At 29 4/7 weeks of gestation, after 2weeks of antiarrhythmic therapy, a fe-toscopy was performed under maternalepidural analgesia, continuous infusionof atosiban, and antibiotic prophylaxis bycefazolin. The video of the whole pro-cedure is presented in the Appendix. Fetalanesthesia and paralysis were obtained byan injection of sufentanil and atracuriumbesylate (a curare) in the umbilical veinunder ultrasound guidance. A 10F (3.3mm) introducer (Pinnacle introducer;Terumo Medical Corporation, Sommer-set, NJ) was inserted in the amnioticcavity with a Seldinger technique, undercontinuous ultrasound guidance andaiming towards the fetal mouth. A 3-mmcurved cannula receiving a 2-mm 0-degree semirigid fetoscope (Karl StorzGmbh, Tuttlingen, Germany) was inser-ted in the fetal esophagus. The position ofthe distal tip of the cannula was placedright above the heart under ultrasoundguidance (Figure 2). The fetoscope wasthen retrieved from the cannula andreplaced by a 6F (2 mm) bipolar pacingesophageal lead (FIAB Esokid 4S, Firenze,Italy) and positioned right behind the leftatrium. The lead was connected to anasynchronous esophageal pacemaker(FIAB 2007, Firenze Italy). Pacing ratewas increased incrementally until atrialcapture, monitored by continuous echo-cardiography, and then increased to 640beats/min at a pulse amplitude of 5 mAwith 2-millisecond pulse width. Two 6-second bursts with these settings were noteffective. Pacing parameters were then setat 10 mA/5 millisecond at the same cyclelength. Two bursts of 6 seconds with thesesettings converted the rhythm to atrialfibrillation along with periods of sinusrhythm (Figure 1, B). Conversion to
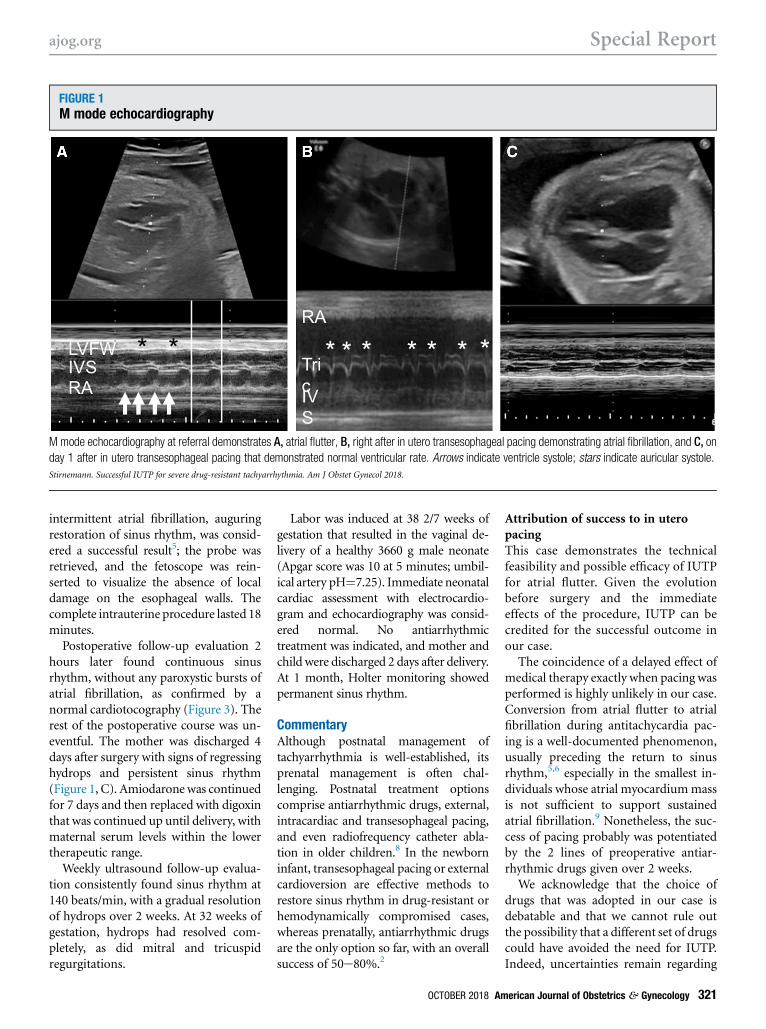
FIGURE 1M mode echocardiography
Mmode echocardiography at referral demonstrates A, atrial flutter, B, right after in utero transesophageal pacing demonstrating atrial fibrillation, and C, on
day 1 after in utero transesophageal pacing that demonstrated normal ventricular rate. Arrows indicate ventricle systole; stars indicate auricular systole.
Stirnemann. Successful IUTP for severe drug-resistant tachyarrhythmia. Am J Obstet Gynecol 2018.
ajog.org Special Report
intermittent atrial fibrillation, auguringrestoration of sinus rhythm, was consid-ered a successful result5; the probe wasretrieved, and the fetoscope was rein-serted to visualize the absence of localdamage on the esophageal walls. Thecomplete intrauterine procedure lasted 18minutes.
Postoperative follow-up evaluation 2hours later found continuous sinusrhythm, without any paroxystic bursts ofatrial fibrillation, as confirmed by anormal cardiotocography (Figure 3). Therest of the postoperative course was un-eventful. The mother was discharged 4days after surgery with signs of regressinghydrops and persistent sinus rhythm(Figure 1, C). Amiodaronewas continuedfor 7 days and then replaced with digoxinthat was continued up until delivery, withmaternal serum levels within the lowertherapeutic range.
Weekly ultrasound follow-up evalua-tion consistently found sinus rhythm at140 beats/min, with a gradual resolutionof hydrops over 2 weeks. At 32 weeks ofgestation, hydrops had resolved com-pletely, as did mitral and tricuspidregurgitations.
Labor was induced at 38 2/7 weeks ofgestation that resulted in the vaginal de-livery of a healthy 3660 g male neonate(Apgar score was 10 at 5 minutes; umbil-ical artery pH¼7.25). Immediate neonatalcardiac assessment with electrocardio-gram and echocardiography was consid-ered normal. No antiarrhythmictreatment was indicated, and mother andchild were discharged 2 days after delivery.At 1 month, Holter monitoring showedpermanent sinus rhythm.
CommentaryAlthough postnatal management oftachyarrhythmia is well-established, itsprenatal management is often chal-lenging. Postnatal treatment optionscomprise antiarrhythmic drugs, external,intracardiac and transesophageal pacing,and even radiofrequency catheter abla-tion in older children.8 In the newborninfant, transesophageal pacing or externalcardioversion are effective methods torestore sinus rhythm in drug-resistant orhemodynamically compromised cases,whereas prenatally, antiarrhythmic drugsare the only option so far, with an overallsuccess of 50e80%.2
OCTOBER 2018 Am
Attribution of success to in uteropacingThis case demonstrates the technicalfeasibility and possible efficacy of IUTPfor atrial flutter. Given the evolutionbefore surgery and the immediateeffects of the procedure, IUTP can becredited for the successful outcome inour case.
The coincidence of a delayed effect ofmedical therapy exactly when pacing wasperformed is highly unlikely in our case.Conversion from atrial flutter to atrialfibrillation during antitachycardia pac-ing is a well-documented phenomenon,usually preceding the return to sinusrhythm,5,6 especially in the smallest in-dividuals whose atrial myocardiummassis not sufficient to support sustainedatrial fibrillation.9 Nonetheless, the suc-cess of pacing probably was potentiatedby the 2 lines of preoperative antiar-rhythmic drugs given over 2 weeks.
We acknowledge that the choice ofdrugs that was adopted in our case isdebatable and that we cannot rule outthe possibility that a different set of drugscould have avoided the need for IUTP.Indeed, uncertainties remain regarding
erican Journal of Obstetrics & Gynecology 321

FIGURE 2Schematic view
Schematic view of the fetoscopic approach of the fetal esophagus for in utero pacing.
Stirnemann. Successful IUTP for severe drug-resistant tachyarrhythmia. Am J Obstet Gynecol 2018.
Special Report ajog.org
322 American Journal of Obstetrics & Gynecology OCTOBER 2018

FIGURE 3Cardiotocography performed 2 hours after surgery
Baseline heart rate is 135-140 beats per minute with normal oscillations during the 25-minute recording.
Stirnemann. Successful IUTP for severe drug-resistant tachyarrhythmia. Am J Obstet Gynecol 2018.
ajog.org Special Report
the best first-line drug or combination ofdrugs and how to manage failure in thecontext of a potentially worsening fetalcondition. An ongoing trial will attemptto answer these questions but is far fromcompletion.10 Nonetheless, trans-placental sotalol has been suggested as asafe and effective treatment for atrialflutter; despite the limited evidence of itsefficacy in case of hydrops, it could havebeen a good candidate drug in first-linetherapies in our case, alone or incombination.2,11e13
Aside from sotalol, a few alternativethird-line drugs or combinations ofdrugs could have been considered beforeIUTP, including direct intracordal orintramuscular administration.14,15
However, lethal accidents have been re-ported with the use of direct fetaladministration.16
Safety of the procedureThe risks of IUTP are limited comparedwith other invasive prenatal cardiacinterventions(such as percutaneousvalvuloplasty,17 atrial septostomy,18,19 or
resection of pericardial teratomas20) orextracardiac surgeries (such as endo-scopic repair of myelomeningo-celes).21,22 The risks of IUTP are thoseof the fetoscopic surgical approach ofthe esophagus and those of cardiacpacing.
Risks of fetoscopy. Technically, this sur-gical procedure is comparable with pre-natal fetoscopic endoluminal trachealocclusion for congenital diaphragmatichernia;23e26 iatrogenic preterm prema-ture rupture of the membranes and itsassociated morbidity are the main sur-gical complication, which occurs in 17%of cases. Given that the introducer’sdiameter, gestational age, and surgicalroute are close to the setting of fetoscopicendoluminal tracheal occlusion, asimilar rate of preterm prematurerupture of the membranes is to beanticipated with IUTP.
Specific risks of transesophageal pacing inthe fetus. Postnatally, transesophagealpacing carries potential risks not only
OCTOBER 2018 Am
of ventricular fibrillation, if theventricle is captured instead of theatrium, but also of sinus nodedepression after reduction because ofprevious antiarrhythmic therapy.Therefore, postnatally, transesophagealpacing is performed under continuouselectrocardiogram and with immediateaccess to an external defibrillator andexternal pacemaker. In our case, atrialcapture was secured by ultrasound-guided placement of the pacing leadand continuous echocardiographicmonitoring. The same lead offers thepossibility of atrial escape pacing in theevent of a prolonged pause afterreduction, along with rescue intra-cordal injection of adrenalin.
Place of IUTP in the management offetal tachyarrhythmiaThe place of IUTP in the management offetal tachyarrhythmia is to be balancedwith the risks of medical therapy, theseverity of the condition (ie, hydrops andcardiac failure),27 and the cause oftachyarrhythmia.
erican Journal of Obstetrics & Gynecology 323

Special Report ajog.org
Antiarrhythmic drugs can lead toincreased morbidity. Despite their un-disputed efficacy, antiarrhythmic drugscan lead to increased morbidity for themother, fetus, and neonate. Among allpotential antiarrhythmic drugs that canbe used in fetal tachyarrhythmia, amio-darone carries the highest risk, given itspotential impact on both the maternaland fetal thyroid functions. Althoughtransplacental pharmacokinetics ofantiarrhythmic drugs have been stud-ied,28 the resulting fetal concentrationscan vary widely, especially in case ofhydrops that reduces transplacental drugtransfer.15,29,30 Furthermore, in case ofatrial flutter specifically, medicallyslowing the atrial cycle can increase theventricular response when 1:1 atrioven-tricular conduction occurs and lead tointractable ventricular dysfunction.
Transplacental antiarrhythmic drugs. Theefficacy of transplacental antiarrhythmicdrugs is delayed, sometimes requiring upto 3 subsequent lines of treatment,although the growing risks of cardiacfailure, hydrops, and fetal death increasewith time. Therefore, IUTP, whichaims to restore sinus rhythm promptly,is a legitimate option in severe cases, inaddition to transplacental antiarrhythmictherapy.
Two main causes of fetal tachyar-rhythmia. The 2 main causes of fetaltachyarrhythmia are atrial flutter in20e30% of cases and reentrant tachy-cardia that is mediated by an accessorypathway (atrioventricular reentranttachycardia) in >60% of cases.31,32 Inatrial flutter, the macro-reentrant circuitcan be terminated easily by pacing, andrecurrence is uncommon, which allowsthe withdraw of antiarrhythmic therapyafter reduction.33 Although atrial flutteris the ideal candidate for IUTP, atrio-ventricular reentrant tachycardia is alsoamenable to pacing. In those cases, IUTPcould be considered a rescue therapy inyoung fetuses or as an alternative to earlydelivery, along with transplacental drugtherapy in order to minimize the risk ofrecurrence.
However, some rare fetal arrhythmiasare not candidates for IUTP.34 Ectopic
324 American Journal of Obstetrics & Gynecology
atrial tachycardia cannot be corrected bypacing, and permanent junctionalreciprocating tachycardia that is medi-ated by decremental accessory pathway istoo prompt to recur to be a goodcandidate for IUTP. Apart from fetaltachyarrhythmia, several rarer condi-tions could also benefit from IUTP: notonly arrhythmia in long QT syndrometype 2 but also complete atrioventricularblock35 with very low escaping heartrate, where IUTP before delivery couldfacilitate perinatal management thatoften is facing profound hemodynamicinstability.
CommentIUTP is a potentially life-saving pro-cedure that should be considered in themanagement of drug-resistant tachyar-rhythmia, particularly atrial flutter, incombination with antiarrhythmic drugs.It is important that this message reachesthe maternal-fetal medicine communityto increase the awareness of the feasi-bility of this procedure. Indeed, thesecases could be addressed to superspe-cialized centers instead of planning asemielective preterm delivery in a criticalcardiac condition without consideringthis novel approach. -
REFERENCES
1. Jaeggi ET, Carvalho JS, Groot ED, et al.Comparison of transplacental treatment of fetalsupraventricular tachyarrhythmias with digoxin,flecainide, and sotalol clinical perspective: re-sults of a nonrandomized multicenter study.Circulation 2011;124:1747–54.2. Donofrio MT, Moon-Grady AJ,Hornberger LK, et al. Diagnosis and treatment offetal cardiac disease: a scientific statement fromthe American Heart Association. Circulation2014;129:2183–242.3. Strizek B, Berg C, Gottschalk I, Herberg U,GeipelA,GembruchU.High-dose flecainide is themost effective treatment of fetal supraventriculartachycardia. Heart Rhythm 2016;13:1283–8.4. Strasburger JF. Amiodarone therapy fordrug-refractory fetal tachycardia. Circulation2004;109(3):375–9.5. Rhodes LA, Walsh EP, Saul JP. Conversion ofatrial flutter inpediatricpatientsby transesophagealatrial pacing: a safe, effective, minimally invasiveprocedure. Am Heart J 1995;130:323–7.6. Watson RM, Josephson ME. Atrial flutter: I,electrophysiologic substrates and modes ofinitiation and termination. Am J Cardiol 1980;45:732–41.
OCTOBER 2018
7. Olutoye OA, Baker BW, Belfort MA,Olutoye OO. Food and Drug Administrationwarning on anesthesia and brain development:implications for obstetric and fetal surgery. Am JObstet Gynecol 2018;218:98–102.8. Philip Saul J, Kanter RJ, Writing Committee,et al. PACES/HRS expert consensus statementon the use of catheter ablation in children andpatients with congenital heart disease: devel-oped in partnership with the Pediatric andCongenital Electrophysiology Society (PACES)and the Heart Rhythm Society (HRS). Endorsedby the governing bodies of PACES, HRS, theAmerican Academy of Pediatrics (AAP), theAmerican Heart Association (AHA), and the As-sociation for European Pediatric and CongenitalCardiology (AEPC). Heart Rhythm 2016;13:e251–89.9. Simpson RJ, Foster JR, Mulrow JP,Gettes LS. The electrophysiological substrate ofatrial fibrillation. Pacing Clin Electrophysiol1983;6:1166–70.10. FAST Therapy Trial of Fetal Tachyarrhythmia-Full Text View-ClinicalTrials.gov [Internet]. [cited2017Aug 26]. Available at: https://clinicaltrials.gov/ct2/show/NCT02624765?term¼fetalþtachycardia&rank¼6. Accessed August 1, 2018.11. Oudijk MA, Ruskamp JM, Ververs FFT, et al.Treatment of fetal tachycardia with sotalol:transplacental pharmacokinetics and pharma-codynamics. J Am Coll Cardiol 2003;42:765–70.12. Hill GD, Kovach JR, Saudek DE, Singh AK,Wehrheim K, Frommelt MA. Transplacentaltreatment of fetal tachycardia: a systematic re-view and meta-analysis. Prenat Diagn 2017;37:1076–83.13. Shah A, Moon-Grady A, Bhogal N, et al.Effectiveness of sotalol as first-line therapy forfetal supraventricular tachyarrhythmias. Am JCardiol 2012;109:1614–8.14. Cuneo BF, Strasburger JF. Managementstrategy for fetal tachycardia. Obstet Gynecol2000;96:575–81.15. Parilla BV, Strasburger JF, Socol ML.Fetal supraventricular tachycardia complicatedby hydrops fetalis: a role for direct fetal intra-muscular therapy. Am J Perinatol 1996;13:483–6.16. Hansmann M, Gembruch U, Bald R,Manz M, Redel DA. Fetal tachyarrhythmias:transplacental and direct treatment of the fetus-a report of 60 cases. UltrasoundObstet Gynecol1991;1:162–8.17. Freud LR, McElhinney DB, Marshall AC,et al. Fetal aortic valvuloplasty for evolving hy-poplastic left heart syndrome: postnatal out-comes of the first 100 patients. Circulation2014;130:638–45.18. Marshall AC, Levine J, Morash D, et al. Re-sults of in utero atrial septoplasty in fetuses withhypoplastic left heart syndrome. Prenat Diagn2008;28:1023–8.19. Quintero RA, Huhta J, Suh E, Chmait R,Romero R, Angel J. In utero cardiac fetal sur-gery: laser atrial septotomy in the treatment ofhypoplastic left heart syndromewith intact atrial

ajog.org Special Report
septum. Am J Obstet Gynecol 2005;193:1424–8.20. Rychik J, Khalek N, Gaynor JW, et al.Fetal intrapericardial teratoma: natural historyand management including successful inutero surgery. Am J Obstet Gynecol2016;215:780.e1–7.21. Pedreira DAL, Zanon N, Nishikuni K, et al.Endoscopic surgery for the antenatal treatmentof myelomeningocele: the CECAM trial. Am JObstet Gynecol 2016;214:111.e1–11.22. Belfort MA, Whitehead WE,Shamshirsaz AA, et al. Fetoscopic open neuraltube defect repair: development and refine-ment of a two-port, carbon dioxide insufflationtechnique. Obstet Gynecol 2017;129:734–43.23. Jani JC, Nicolaides KH, Gratacós E, et al.Severe diaphragmatic hernia treated by fetalendoscopic tracheal occlusion. UltrasoundObstet Gynecol 2009;34:304–10.24. Belfort MA, Olutoye OO, Cass DL, et al.Feasibility and outcomes of fetoscopic trachealocclusion for severe left diaphragmatic hernia.Obstet Gynecol 2017;129:20–9.
25. Deprest J, Brady P, Nicolaides K, et al.Prenatal management of the fetus with isolatedcongenital diaphragmatic hernia in the era of theTOTAL trial. Semin Fetal Neonatal Med 2014;19:338–48.26. Jiménez JA, Eixarch E, DeKoninck P, et al.Balloon removal after fetoscopic endoluminaltracheal occlusion for congenital diaphragmatichernia. Am J Obstet Gynecol 2017;217:78.e1–11.27. Society for Maternal-Fetal Medicine(SMFM), Norton ME, Chauhan SP, et al. Societyfor Maternal-Fetal Medicine (SMFM) clinicalguideline #7: nonimmune hydrops fetalis. Am JObstet Gynecol 2015;212:127–39.28. Schmolling J, Renke K, Richter O, Pfeiffer K,Schlebusch H, Höller T. Digoxin, flecainide, andamiodarone transfer across the placenta and theeffects of an elevated umbilical venous pressureon the transfer rate. Ther Drug Monit 2000;22:582–8.29. Younis JS, Granat M. Insufficient trans-placental digoxin transfer in severe hydropsfetalis. Am J Obstet Gynecol 1987;157:1268–9.
OCTOBER 2018 Am
30. Gembruch U, Manz M, Bald R, et al.Repeated intravascular treatment with amio-darone in a fetus with refractory supraventriculartachycardia and hydrops fetalis. Am Heart J1989;118:1335–8.31. Simpson J, Sharland G. Fetal tachycardias:management and outcome of 127 consecutivecases. Heart 1998;79:576–81.32. Strasburger JF, Wakai RT. Fetal cardiacarrhythmia detection and in utero therapy. NatRev Cardiol 2010;7:277–90.33. Texter KM, Kertesz NJ, Friedman RA,Fenrich AL. Atrial flutter in infants. J Am CollCardiol 2006;48:1040–6.34. Chien WW, Cohen TJ, Lee MA, et al.Electrophysiological findings and long-termfollow-up of patients with the permanentform of junctional reciprocating tachycardiatreated by catheter ablation. Circulation1992;85:1329–36.35. Cuneo BF, Ambrose SE, Tworetzky W.Detection and successful treatment of emergentanti-SSA-mediated fetal atrioventricular block.Am J Obstet Gynecol 2016;215:527–8.
erican Journal of Obstetrics & Gynecology 325