specificities of surgery in time of armed conflict or natural disaster christos giannou advanced...
TRANSCRIPT

Specificities of Surgery inTime of Armed Conflict or
Natural Disaster
Christos Giannou
Advanced Course in the Management of Disaster Victims
Nicosia, October 2011

Understand what you are getting into
BEFORE
you go.

Natural disaster, accident, isolated explosion
One-off event:
surprise, warning
War
Successive events:
NO surprise, political build-up

1. Rights and obligations of Medical Personnel
2. Specific epidemiology of war (constant) / disaster (variable)
3. Predominance of emergency surgery (especially during early tactical field care)
4. Surgery within a limited technical environment
5. Limits of surgery: post-operative nursing + anaesthesia
6. Surgery in a hostile, violent environment

7. Mass casualties involving the principles of triage
8. Surgery and triage in successive echelons (delayed evacuation)
9. Specific wound pathology, qualitatively different from civilian wounds: ballistics & blast; all are dirty and contaminated
10. Specific techniques appropriate to the context and pathology: simplicity, security, speed
11. Importance of disease: disease is four times more common than trauma among soldiers; disaster public health approach

1. Rights and obligations of Medical Personnel
2. Specific epidemiology of war (constant) / disaster (variable)
3. Predominance of emergency surgery (especially during early tactical field care)
4. Surgery within a limited technical environment
5. Limits of surgery: post-operative nursing + anaesthesia
6. Surgery in a hostile, violent environment

Medical Ethics
Oath of Hippocrates:
International Code of Medical Ethics: WMA 1949 London, 2006 Pilanesberg S. Africa

International Humanitarian Law: laws of war
Geneva Conventions 1949
Additional Protocol I 1977
1. Rights and obligations of International Humanitarian Law: laws of war
2. Specific epidemiology of war (constant) / disaster (variable)
3. Predominance of emergency surgery
4. Surgery within a limited technical environment
5. Limits of surgery: post-operative nursing + anaesthesia
6. Surgery in a hostile, violent environment

War wounded in the field: epidemiology
First AidDressing
40-60 %No surgery
10-15% Head10-12% Chest8-10% Abdomen60-70% Limbs
90% Surgery
Small woundsParaplegiaTetraplegia
Observation
10% NO Surgery
40-60 %Hospital care
WW in the field(GSW, mine, blast)
100 wounded

War wounded: causes of death
Severe injury (brain, major vessels)
Haemorrhage: peripheral
Airway, breathing
Coagulopathy, acidosis, hypothermia / multiple system failure

Natural disaster: context
Earthquake demographic density type of construction access: rural or urban
Tsunami
Storm / flooding
Neighbourhood nuclear plant

Epidemiology of disaster wounded:collapse of 8-storey building China
80% of entrapped died immediately or early
10% survived with minor injuries
10% severe injuries
of which 70% developed crush syndrome

Earthquake Survival Rate:% survivors still alive without extraction
0102030405060708090
100
0.5h 24h 48h 72h 96h 120h

Earthquake: causes of death
Immediate: severe crush of head or thorax (organ damage + suffocation)
Early: ABC
Delayed: dehydration, hypothermia
Late: crush syndrome (acute renal failure), sepsis, multiple organ failure

1. Rights and obligations of International Humanitarian Law: laws of war
2. Specific epidemiology of war (constant) / disaster (variable)
3. Predominance of emergency surgery
4. Surgery within a limited technical environment
5. Limits of surgery: post-operative nursing + anaesthesia
6. Surgery in a hostile, violent environment

Specificities of austere environments
Damaged infrastructure (water, electricity)
Lack of experienced human resources: competency, fatigue, fear
Lack of equipment and supplies: appropriate
Lack of blood for transfusion
"Humanitarian circus" and military-civilian cooperation
Culture shock
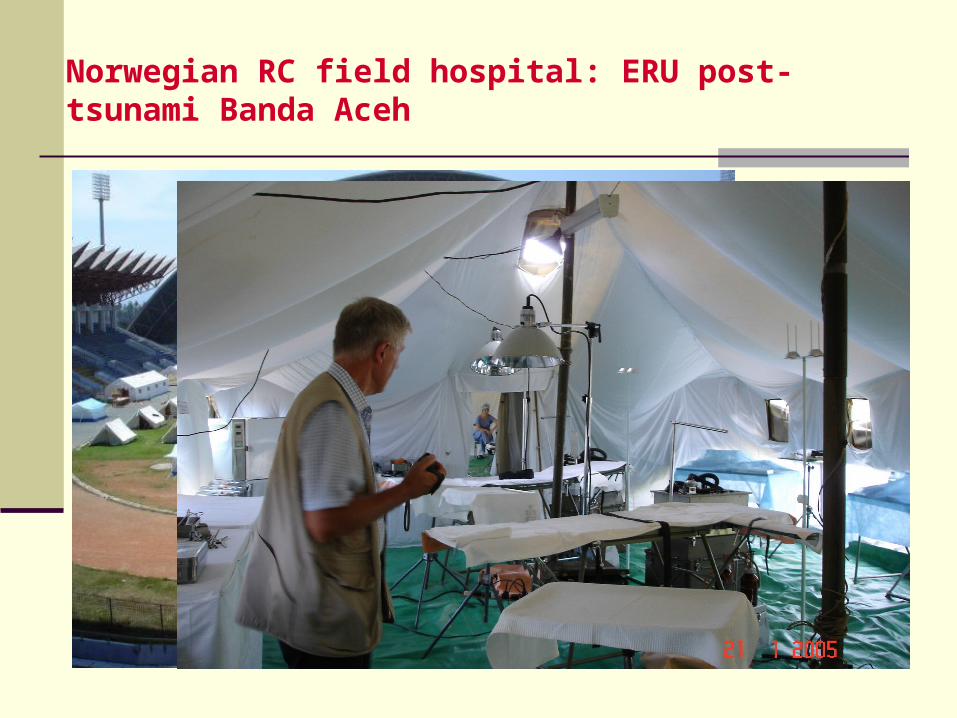
Norwegian RC field hospital: ERU post-tsunami Banda Aceh

Field Surgical Team Darfur

Recycling of a prison


Somali Red Crescent Society: No State
Shatilla refugee camp 1987

Understanding the limits
simplicity of diagnostic means available
laboratory: Hb/Hct, blood grouping & screening
anaesthesia (local, regional, ketamine)
availability of blood (no components): autotransfusion
patient monitoring (BP, P, O2 saturation)
post-operative nursing care
Heroic surgery will never replace good surgery.

Clinical skills
• Lucky if you have X-rays
• Chest tube & laparotomy on clinical basis alone (no DPL)
• No place for CPR, ER thoracotomy
• Limited- or non- use of endotracheal intubation, no mechanical ventilation
• Proper indications and use of damage control techniques• Will you see your patient again?• Category IV? supportive treatment

Always plan for alternatives:
infrastructure
equipment
communications
supplies, logistics
human resources

1. Rights and obligations of International Humanitarian Law: laws of war
2. Specific epidemiology of war (constant) / disaster (variable)
3. Predominance of emergency surgery
4. Surgery within a limited technical environment
5. Limits of surgery: post-operative nursing + anaesthesia
6. Surgery in a hostile, violent environment

Hostile, violent environment


7. Mass casualties involving the principles of triage
8. Surgery and triage in successive echelons (delayed evacuation)
9. Specific wound pathology, qualitatively different from civilian wounds: ballistics & blast; all are dirty and contaminated
10. Specific techniques appropriate to the context and pathology: simplicity, security, speed
11. Importance of disease: disease is four times more common than trauma among soldiers; disaster public health approach

Everyday work
MCI
MAD
Triage

7. Mass casualties involving the principles of triage
8. Surgery and triage in successive echelons (delayed evacuation)
9. Specific wound pathology, qualitatively different from civilian wounds: ballistics & blast; all are dirty and contaminated
10. Specific techniques appropriate to the context and pathology: simplicity, security, speed
11. Importance of disease: disease is four times more common than trauma among soldiers; disaster public health approach

Old lessons for new surgeons
War / disaster wounds are dirty and contaminated, from the moment of injury.
The rules of septic surgery apply.

Principles of septic surgery
The best antibiotic is good surgery.

7. Mass casualties involving the principles of triage
8. Surgery and triage in successive echelons (delayed evacuation)
9. Specific wound pathology, qualitatively different from civilian wounds: ballistics & blast; all are dirty and contaminated
10. Specific techniques appropriate to the context and pathology: simplicity, security, speed
11. Importance of disease: disease is four times more common than trauma among soldiers; disaster public health approach