spleen spleen injury - orthopaedic research and education · injuries in football course april 29,...
TRANSCRIPT

5/8/2017
1
Abdominal Injuries
Andrews Institute:
Injuries in Football Course
April 29, 2017
Brett J Kindle, MD, CAQSM, RMSK
Abdominal Injuries
• Rare
• Potentially life-threatening
• Spleen
• Liver
• Abdominal wall
• Kidney
• Stomach
• Pancreas
• Gall Bladder
• Intestines
Spleen
• LUQ, enclosed ant. & lat. by rib cage
• Most vascular organ in body
– Splenic artery – 5 non-anastamosing
branches, damage to 1 branch � segmental infarction
• Function
– Mechanically filters RBCs
– Active in immune system
Spleen Injury
• Blunt trauma (helmet to abdomen)
– Most commonly injured – 25% BAT
• Associated with L 10-12th rib fractures
• Laceration is life-threatening
Spleen Injury
• LUQ & flank pain
• +/- L shoulder pain (Kehr’s sign)
• Exam:
– TTP LUQ, distention (50% cases)
– Hypotension (20-30% cases)
– Guarding & rebound
– Younger athletes � more subtle presentation
Spleen Injury
• Diagnosis & Treatment
– Sideline – US Grade 1 Grade 2
Grade 3
Grade 4 Grade 5

5/8/2017
2
LUQ: Free Fluid
sonoguide.com
Spleen Injury
• Diagnosis & Treatment
– Sideline – US
– CT with IV contrast
– Inpatient – serial h/h
– Surgery – splenectomy vs ligation
– Post-splenectomy precautions
• H influenza type B, pneumococcal,
meningococcal vaccines (encapsulated)
• SSD, Thalassemia, Cancer � daily
PCN ppx for pneumococcal infection
Grade 1 Grade 2
Grade 3
Grade 4 Grade 5
Spleen Injury
• Return to play – controversial
– Nonoperative tx: 2-6 months (based on severity)
– Surgical tx: ≥ 6 weeks postop
– Infectious mononucleosis
• Splenic rupture reported at 4-21 days post-infection
• Asymptomatic athletes w/ normal spleen size –gradual RTP at 21 days post-infection
Liver
• RUQ, enclosed ant. & lat. by rib cage
• Largest solid organ in body • Relatively fixed position, friable parenchyma,
& thin capsule � prone to injury
• Function– Glycogen storage
– Plasma protein synthesis– Decomposition of RBCs– Bile production– Detoxification
Liver Injury
• Blunt trauma (helmet to abdomen)
– 2nd most commonly injured – 15-20% BAT
– 50% deaths related to BAT
• Shearing injury (rapid deceleration)
• Associated with R 8-12th rib fractures
• More common in children
– Increased rib flexibility, less developed
framework of liver parenchyma
Liver Injury
• RUQ pain
• +/- R shoulder pain
• Nausea & vomiting
• Exam:– TTP RUQ � diffuse
– Guarding & rebound
– Cannot stand upright ( abd pressure)
– Pulse, BP (hypovolemic shock)
5/8/2017
3
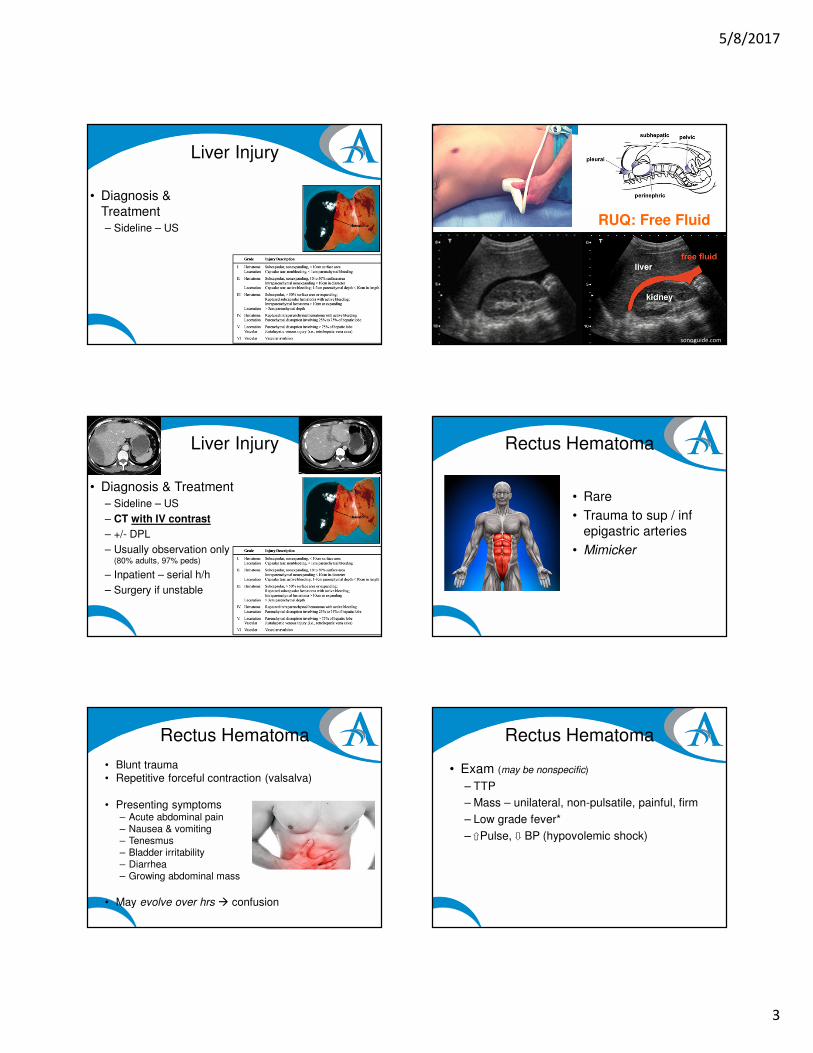
Liver Injury
• Diagnosis &
Treatment
– Sideline – US RUQ: Free Fluid
sonoguide.com
Liver Injury
• Diagnosis & Treatment
– Sideline – US
– CT with IV contrast
– +/- DPL
– Usually observation only (80% adults, 97% peds)
– Inpatient – serial h/h
– Surgery if unstable
Rectus Hematoma
• Rare
• Trauma to sup / inf
epigastric arteries
• Mimicker
Rectus Hematoma
• Blunt trauma
• Repetitive forceful contraction (valsalva)
• Presenting symptoms– Acute abdominal pain– Nausea & vomiting– Tenesmus– Bladder irritability– Diarrhea – Growing abdominal mass
• May evolve over hrs � confusion
Rectus Hematoma
• Exam (may be nonspecific)
– TTP
– Mass – unilateral, non-pulsatile, painful, firm
– Low grade fever*
– Pulse, BP (hypovolemic shock)

5/8/2017
4
Rectus Hematoma
• Diagnosis & Treatment
– Fothergill sign
• Differentiate abd wall vs intra-abdominal mass
• Voluntary contraction (lift head or legs while supine)
• Fixed, �TTP, �size = rectus sheath hematoma
• TTP, size = intraabdominal mass
– Sideline – US
Rectus Hematoma
Rectus Hematoma
• Diagnosis & Treatment
– Fothergill sign helps differentiate abd wall vsintra-abdominal mass
• Voluntary contraction (lift head or legs while supine)
• Fixed, �TTP, �size = rectus sheath hematoma
• TTP, size = intraabdominal mass
– Sideline – US
– CT
– Usually benign, observation only
Renal
• Kidneys, ureters, bladder, urethra
• Retroperitoneal
• Function– Eliminate waste
– Regulate blood volume & BP
– Regulate blood pH
– Control lyte & metabolite levels
Renal Injury
• Kidney > Bladder > Urethra
• Blunt trauma (helmet to flank)
– 10% BAT
• Rapid deceleration
• More common in children*
– Increased rib flexibility, less developed framework of kidney parenchyma
Renal Injury
• Important indicators (absence of all 3 = very unlikely renal injury)
– Hematuria• Not correlative with severity
• Not present initially in 25-50% cases
– Hypotension
– MOI (blunt trauma / rapid deceleration)
• Moderate indicators– Flank hematoma or tenderness
– Rib fractures
– Penetrating injury

5/8/2017
5
Renal Injury
• Diagnosis
– Sideline – US
RUQ: Free Fluid
sonoguide.com
LUQ: Free Fluid
sonoguide.com
Renal Injury
• Diagnosis
– Sideline – US
– Labs – UA, CBC, Lytes, LFTs, Cr, Glc, Amylase, Lipase, HCG
– Chest X-ray (? rib fracture)
– CT with IV contrast
Renal Injury
• Treatment (based on grade)
– I-II: usually observation
– III-V: surgery - repair vs nephrectomy
• Return to play– Wait for complete resolution of hematuria
– I-II: usually 2-6 weeks
– III-V: 6-12 months
1Grades: 2 3
4 5
Take Home Points
• Abdominal injuries are rare, but potentially
life-threatening
• If concerned on sideline � send to ED for
CT & further management
