sport medicine centre 1 st world congress on sports injury prevention oslo, norway, june 23-25, 2005...
TRANSCRIPT

SPORT MEDICINE CENTRE
1st World Congress on Sports Injury PreventionOslo, Norway, June 23-25, 2005
Willem H. Meeuwisse, MD, PhD
Key Components of Collection and Classification of Sports Injuries

SPORT MEDICINE CENTRE
Outline –Key Components1. Collection
• Who is collecting?• Completeness / precision• Injuries and exposure
2. Use of diagnostic coding systems3. Classification methods
• By location• By type• By diagnosis• By severity

SPORT MEDICINE CENTRE
Steps in Developing Injury Prevention:
1. Identify the problem
2. seek to understand "cause" of injury
3. attempt to reduce injury• develop an intervention• introduce the intervention• evaluate the intervention

SPORT MEDICINE CENTRE
Why Surveillance?
• to identify injury problems• estimate public health
impact• identify risk/causal factors• identify possible
preventative measures

SPORT MEDICINE CENTRE
1. Collection
• Who is collecting?• Trained medical staff (therapist)• Student• Lay person (coach, parent, player)• Payment / honorarium?
• Motivation, accountability

SPORT MEDICINE CENTRE
Collection
• Validation?• how complete is reporting?• Are sources of error estimated or
unknown?
• Anticipate how this might this affect analysis plan

SPORT MEDICINE CENTRE
Injury Rates
• Numerator• Counting injuries
• Denominator• Counting exposure

SPORT MEDICINE CENTRE
Collection of Denominator
• Number of sessions vs hours• Inconsistent across literature• Consider purpose of study

SPORT MEDICINE CENTRE
Estimating Exposure
• exposure estimation (group index)• no. of athletes X no. sessions = no.
athlete exposures
• exposure measurement (individual index)• count each exposure (or partial
exposure) for each athlete

SPORT MEDICINE CENTRE
Environmental Factors• Environment
• Facilities, surfaces, equipment
• Part of the assessment of denominator and risk

SPORT MEDICINE CENTRE
Exposure in Sport Injury
• Importance for assessing risk and evaluating prevention
• a combination of:• possessing a risk factor• participating in sport with that factor

SPORT MEDICINE CENTRE
2. Diagnostic Coding Systems
• “Open source” coding systems best• Limitations with universal systems
• ICD-9 or ICD-10
• Sport-specific open systems best• Orchard codes• University of Calgary System
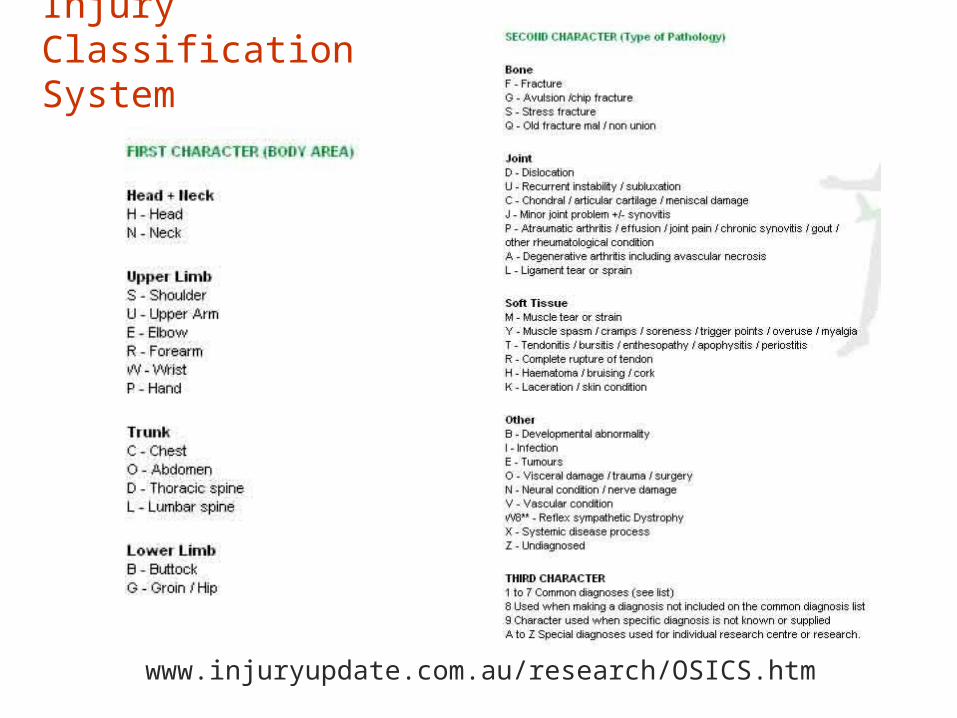
Orchard Sport Injury Classification System
www.injuryupdate.com.au/research/OSICS.htm

University of Calgary Diagnostic Coding System
SPORT MEDICINE CENTRE
Diagnostic Coding
• Diagnostic coding systems can affect how data are grouped, analyses, displayed and interpreted

SPORT MEDICINE CENTRE
3. Classification Methods
• By location• Body region
• By type• Tissue type, injury type
• By diagnosis• Specific or unique
diagnoses• By severity

Rodeo Injuries

SPORT MEDICINE CENTRE
Injury Severity
• “grading” (1st, 2nd, 3rd degree)• By time loss
• Continuous variable• Days vs sessions
• Categorical• 1, 2-7, >7 ????
• Time loss may be most “objective”

SPORT MEDICINE CENTRE
Time Loss
• Same session?• Next session?• Next day?

SPORT MEDICINE CENTRE
Return to Play
• “clearance” affects measurement of time loss• Return to full training• Return to play
• Medically cleared?• Actual return (e.g., coaching decision)?

SPORT MEDICINE CENTRE
Classification Pitfalls
• Multiple diagnoses?• Knee triad: ACL, MCL, meniscal tear
• Multiple injuries• Concussion and AC separation
• Bias for acute vs overuse?• In research, assumptions and
limitations must be clearly stated
SPORT MEDICINE CENTRE
Summary Statements1. Collection should be done by trained personnel, with
incentives (pitfalls with volunteers)2. Whenever possible, exposure should be measured
(individual), not estimated (group)3. Error should be measured (or estimated)4. Sport diagnostic coding systems that are “public”
should be used5. Assumptions and limitations should be stated6. Be comprehensive in data collection and flexible in
the analysis
SPORT MEDICINE CENTRE
Issues
1. Need consistency in denominator• Athlete exposures (sessions) vs hours
2. Need consistency in measures / categories of severity
• Time loss
3. How do we handle multiple regions / diagnoses?
4. Accurate capture of overuse injuries

SPORT MEDICINE CENTRE
Thank You!
Willem H. Meeuwisse, MD, PhD
Key Components of Collection and Classification of Sports Injuries