st. john’s, newfoundland -...
TRANSCRIPT

ST. JOHN’S, NEWFOUNDLAND


St. John’s, Newfoundland
© 2013 CAMH 3
St. John’s, Newfoundland
For more information, please contact:
Joanna Henderson, Ph.D.
Clinician Scientist
Gloria Chaim, MSW
Deputy Clinical Director
Child, Youth and Family Services
Centre for Addiction and Mental Health
80 Workman Way, Toronto, ON M6J1H4
Production of this report has been made possible through a financial contribution from Health Canada.
The views expressed herein do not necessarily represent the views of Health Canada

St. John’s, Newfoundland
4
Acknowledgments
The National Youth Screening Project Team would like to acknowledge the commitment, dedication
and hard work of the many people representing agencies in St. John’s, Newfoundland, one of ten
participating communities across Canada. Sincere thanks are due to Renee Ryan, former Addictions
Consultant, Department of Health and Community Services, Newfoundland and Labrador and Kim
Baldwin, Regional Director of Mental Health and Addiction Services, Eastern Health, both of whom
supported the project and brought it to the attention and encouraged participation of Choices for
Youth and Eastern Health respectively. Appreciation goes to Sheldon Pollett, Executive Director,
Choices for Youth, for initiating development of the youth screening network in St. John’s,
volunteering his agency to take on the “Lead Agency” role and making it possible for Cheryl Mallard to
take on the role of network lead. Sincere appreciation is also due to Cheryl for providing on-going
leadership to the network and working diligently to ensure full implementation of the project protocol;
to the agency leads who were prepared to commit to participate in a cross-sectoral collaboration,
adapt program protocols to integrate consistent administration of a screening tool and dedicate staff
time to participate in the project; to front-line service providers who were willing to take the time to
explore new practices, and to engage youth in a screening process for clinical and research purposes;
and, most of all, to the youth who participated in completing the screeners and consented to sharing
them for project purposes. We would also like to thank Health Canada for their commitment to
capacity building, data collection and knowledge exchange, demonstrated by providing the funding
support that made this project and dissemination of the findings possible.
National Youth Screening Project Partner Agencies: St. John’s, Newfoundland
The following agencies participated in one or more of the four key project activities: Capacity Building,
Network Development, Screening Implementation and Data Collection (Refer to Appendix A for
agency descriptions and Appendix B for key project activity descriptions)
Partner Agencies Agency Leads Choices for Youth Community Youth Network
o Rogers Break Thru Project o Springboard GED o Street Outreach o Youth at Promise
Kerri Collins Ellie Jones
Eastern Health o Janeway Family Centre o Central Intake o Bridges Program o Complex Case Management o Family Services Counsellors o Youth Services / Youth Corrections o Rowan Centre
Susan McLeod and Deanne Costello

St. John’s, Newfoundland
5
o Community Mental Health Counsellors o Youth Outreach Counsellors
Stella Burry Community Services o Naomi Centre
Jennifer Corrigan
Network Lead
Cheryl Mallard, Choices for Youth
Network Coordinator
Heather Quinlan
Project Team: Centre for Addiction and Mental Health
Project Leads
Joanna Henderson
Gloria Chaim
Project Coordinator
Megan Anne Tasker
Administrative Support
Stephanie Schultz
Research Analysts
Andra Ragusila
Dave Summers
Carly Clifton
GAIN SS License
Chestnut Health Systems – Copyright holder for all Global Appraisal of Individual Needs instruments,
including Global Appraisal of Individual Needs - Short Screener (GAIN SS)

St. John’s, Newfoundland
Table of Contents
List of Figures 7
National Youth Screening Project 9
Overview 9
Context 9
Objectives 12
National Youth Screening Project: St. John's, Newfoundland 13
Summary 13
Development 13
Partners 14
Roles 14
Implementation Process 15
Materials 17
Findings 21
Background Information about Youth 23
Clinical Needs of Youth Based on the GAIN SS 36
Other Clinical Needs 45
Concurrent Substance Use and Mental Health Concerns 46
Service Provider Survey 53
Feasibility and Utility of the GAIN SS 54
Summary of Findings 56
Discussion 57
Recommendations 59
Appendix A: St. John's, Newfoundland Network Member Agency Descriptions 63
Appendix B: Key Project Activity Descriptions 65
Appendix C: Agency Project Activity Participation 66
Appendix D: Project Timeline 67
Appendix E: Project Flow Chart 68
Appendix F: References 69

St. John’s, Newfoundland
7
List of Figures
Figure 1: Age Distribution of Participants 24
Figure 2: Age Distribution by Service Sector 25
Figure 3: Sex Distribution of Participants 26
Figure 4: Sex Distribution of Participants by Service Sector 27
Figure 5: Service History by Service Sector 28
Figure 6: Ethnicity Distribution of Participating Youth 29
Figure 7: Current Living Arrangements 30
Figure 8: Current Living Arrangements by Sex 31
Figure 9: Current Living Arrangements by Age Categories 32
Figure 10: Current Living Arrangements by Service Sector 33
Figure 11: Number of Concerns Endorsed by GAIN SS Domain 37
Figure 12: Recent Clinical Needs Using Moderate Threshold by Service Sector 38
Figure 13: Recent Clinical Needs Using High Threshold by Service Sector 39
Figure 14: Recent Internalizing Concerns by Age and Sex Categories 40
Figure 15: Recent Externalizing Concerns by Age and Sex Categories 41
Figure 16: Recent Substance Use Concerns by Age and Sex Categories 42
Figure 17: Recent Crime and Violence Concerns by Age and Sex Categories 43
Figure 18: Recent Suicide Concerns by Age and Sex Categories 44
Figure 19: Rates of Recent Additional Concerns by Sex Categories 45
Figure 20: Rates of Endorsement of Concurrent Disorders 46
Figure 21: Rates of Endorsement of Concurrent Disorders by Service
Sector and Sex 48
Figure 22: Rates of Endorsement of Concurrent Disorders by Age and Sex 49
Figure 23: Rates of Endorsement of Concurrent Disorders by Legal
System Involvement 50
Figure 24: Complexity of Needs 51
Figure 25: Service Provider Perceptions of GAIN SS Utility and Feasibility 54

St. John’s, Newfoundland

St. John’s, Newfoundland
9
National Youth Screening Project
Overview
The National Youth Screening Project (NYSP), Enhancing Youth-Focused, Evidence-Informed
Treatment Practices through Cross-Sectoral Collaboration, was funded under Health Canada’s Drug
Treatment Funding Program (DTFP) to work collaboratively with youth-serving agencies in seven
communities across Canada to implement a common screening tool for youth substance use and
mental health concerns. Each network was to include a range of agencies representing three or more
sectors, including substance use, mental health, justice, child welfare, education, housing, outreach
and primary health care. Each of the agencies was to participate in one or more of four key project
activities: Capacity Building, Network Development, Screening Implementation and Data Collection
(see Appendix B). Through this process, the project would have the opportunity to examine rates of
co-occurring substance use and mental health concerns (frequently referred to as concurrent or co-
occurring disorders (CD)) in different service sectors, across the adolescent and emerging adulthood
age spectrum, and to examine the extent to which rates of CD are consistent with service provider
expectations. As well, the project aimed to explore service provider perceptions of interagency
referrals, perceived interagency collaboration and youth CD attitudes, knowledge, and practices at
different time points in the project.
The overall objective of the NYSP was to enhance service provider CD capacity, increase early
intervention opportunities and improve pathways to treatment for youth aged 12-24 years with
substance use concerns and CD. This was done through building sustainable stakeholder
collaborations and providing CD-related capacity development opportunities.
Context
Background
Youth with CD experience difficulties in many areas of functioning, resulting in vulnerability to
increased risk-taking behaviour, poor academic/vocational performance, increased suicide risk, and
adverse health effects, including increased risk for substance dependency and psychiatric disorders
continuing into adulthood (Rush, Castel, & Desmond, 2009). Unfortunately, effective, developmentally-
informed interventions have yet to be established. From a public health perspective there is a
desperate need to develop integrated models of service delivery across the continuum of care to
improve outcomes and reduce the high individual and societal costs associated with CDs (Rush et al.,
2009). Evidence suggests that universal screening for mental health and/or substance use disorders

St. John’s, Newfoundland
10
should be a routine part of client care in adults (Rush et al., 2009). However, effective and efficient
screening, assessment and treatment approaches, especially for youth, are only beginning to emerge.
At the same time, concerns about co-occurring substance use and mental health issues in youth have
been identified in services across sectors including child welfare, youth justice, mental health,
addictions, education, health care, housing and other social service agencies (Chaim & Henderson,
2009). There is a strong rationale for effective, consistent screening in youth service delivery settings
(Rush et al., 2009).
In Canada, there have traditionally been separate service delivery systems for health, mental health,
substance use treatment and social services rather than integrated or collaborative models of service
delivery. With recent calls to develop integrated models of service delivery in Canada (Health Canada,
2002), some agencies are beginning to offer integrated CD services, although little information is
available about types and accessibility of these services. Emerging evidence suggests that cross-
discipline collaborations may have particular benefits for improving access and meeting youth and
family needs (McElheran, Eaton, Rupcich, Basinger, & Johnson, 2004; Murphy, Rosenheck,
Berkowitz, & Marans, 2005). There are many barriers, however, to cross-discipline approaches,
especially if the disciplines involved differ substantially in organizational culture, philosophy, values
and practices (Oliver & Dykeman, 2003; Robillard, Gallito-Zaparaniuk, Kimberly, Kennedy, Hammett,
& Braithwaite, 2003). It has been argued that these barriers can be addressed through
communication, relationship-building, joint educational opportunities and practice-based initiatives,
although the specific impacts of these strategies have not been established (McElheran et al., 2004;
Murphy et al., 2005; Oliver & Dykeman, 2003; Henderson, MacKay, & Peterson-Badali, 2010).
Although it is well known that youth presenting for service often have multiple co-occurring needs, the
fragmented system is generally not set up to address them. There are many challenges including
stigma, lack of resources, lack of knowledge and lack of attention to youth-specific needs, as well as a
frequent lack of collaboration and limited integration. The work of the Canadian Mental Health
Commission (2006) and the National Treatment Strategy Working Group (2008) highlighted these
issues and provided some fundamental principles to be considered and followed in planning new
initatives. Themes and recommendations identified across these documents including “every door is
the right door,” the need to improve access, the importance of attending to population specific needs,
the need to collaborate within and across sectors, the importance of generating solid data to inform
investments and making knowledge exchange a priority, have informed this project as well as our
previous collaborative screening network projects ( GAIN Collaborating Network, 2009; Concurrent
Disorders Support Services Screening Project, 2011).
Choosing a Screening Tool for Youth
The importance of screening for both mental health and substance use concerns across sectors has
been identified through a number of initiatives. From 2002 to 2006, the emphasis was primarily on the

St. John’s, Newfoundland
11
identification of useful adult tools and practices (Health Canada, 2002; Centre for Addiction and
Mental Health, 2006).
In 2006, Rush and colleagues initiated a process to identify youth screening tools and processes and
conducted a comprehensive review and synthesis of screening tools for substance use and mental
health disorders among children and adolescents (Rush, Castel, & Desmond, 2009).
Through these initiatives, the Global Assessment of Individual Needs Short Screener (GAIN SS) was
identified as an ideal first stage screening tool for substance use and mental health concerns for youth
and adults. In particular, it was recommended because it:
Screens for both substance use and mental health issues
Is reliable and valid
Is brief (five to seven minutes to complete)
Can be self-administered
Has been validated for individuals aged 10 years and older (including adults)
Is low cost
Can be used in different service settings (e.g., treatment, primary care, etc.)
Collaborative Screening Initiatives 2003 - 2010
In 2003, CAMH merged its children’s mental health and youth substance use services into the Child,
Youth and Family Program (CYFP) and in 2005 a project was initiated to identify and implement a
common screening tool for substance use and mental health concerns across the merged program.
Based on the work of Rush and colleagues, the GAIN SS was chosen and implemented. In addition,
substance use and mental health-related staff attitudes, knowledge and practices were measured and
staff feedback was gathered. Findings from that project demonstrated that many youth endorsed co-
occurring substance use and mental health concerns, regardless of “presenting problem” and initial
service request. As well, participating staff indicated that implementing a consistent substance use
and mental health screening tool was feasible across diverse services and provided clinically useful
information (Henderson, Chaim, & Rush, 2007; Skilling, Henderson, Root, Chaim, Bassarath, &
Ballon, 2007).
Discussion about this project at workshops, conferences and network meetings generated interest in
the Toronto-based Mental Health and Addiction Youth Network (MAYN) in replicating the project
within their own agencies. In 2008, a cross-sectoral network of 10 Toronto-based youth serving
agencies, all members of MAYN, led by Gloria Chaim and Joanna Henderson committed to
administer the GAIN SS, along with a standardised background information form to the youth (aged
12 – 24 years) seeking service at their agencies for a 6-month period. The GAIN Collaborating
Network research findings resulted in a report describing youth needs across sectors and about the
feasibility and utility of consistent screening and the GAIN SS in particular. Stakeholder discussion

St. John’s, Newfoundland
12
about the findings generated a number of service, system and research initiatives and suggested that
the GAIN SS is a feasible and useful clinical instrument (Chaim & Henderson, 2009).
Upon completion of the GAIN Collaborating Network project, findings were presented to local
stakeholders including service providers, agency leaders and policy makers as well as at multiple
international, national and local conferences, meetings, and forums, most notably the Annual
Convention of the American Psychological Association (2009) and Issues of Substance (2009).
Through these knowledge sharing opportunities, interest in implementing the GAIN SS in youth
serving agencies and in participating in collaborative research was generated in communities across
Canada. In 2009, the Health Canada, Drug Treatment Funding Program had a call for proposals.
With interest and stakeholder support from several provinces, Chaim and Henderson submitted a
proposal to engage youth-serving agencies in participating in a national youth screening project.
In 2010, while awaiting acceptance of their DTFP proposal, Chaim and Henderson, in collaboration
with the Toronto Concurrent Disorders Support Services Network, supported by the Toronto Central
Local Health Integration Network, launched another screening project, working with a cross-sectoral
group of 10 Toronto-based health and social service agencies focused on youth and adults seeking or
receiving service at their agencies. Similar to the GAIN Collaborating Network Project, service
providers’ attitudes regarding feasibility and utility of the GAIN SS were positive and stakeholders
reported that the research results were useful in identifying gaps in service and training needs for staff
(Hillman et al., 2011).
The National Youth Screening Project: Enhancing Youth-Focused, Evidence-Informed Treatment
Practices through Cross-Sectoral Collaboration was granted DTFP funding in 2010.
Objectives
Promote, facilitate and evaluate implementation of evidence-based screening procedures and tools
in cross-sectoral youth-serving agencies
Establish network protocols for referral and intervention to improve pathways to care for youth
Promote and facilitate collaboration and knowledge exchange amongst service providers through
the establishment of local cross-sectoral networks of youth-serving agencies
Increase use of reliable and valid tools across agencies and sectors
Evaluate and compare youth service needs across jurisdictions
Evaluate and compare pre-post service provider capacity re: evidence-based practices for youth
substance use with or without co-occurring mental health concerns
Promote a standardised screening protocol for youth concurrent disorders

St. John’s, Newfoundland
13
National Youth Screening Project: St. John’s, Newfoundland
Summary
Discussion about the St. John’s, Newfoundland Network collaboration began in June 2010, followed
by several meetings throughout the summer and fall, resulting in four agencies committing to
participate in the project. All necessary Research Ethics Board (REB) submissions were approved
and agreements were signed by December 2011.
Over a staggered six month period, commencing in January 2011, a cross-sectoral group of four
youth-serving agencies in and around St. John’s, Newfoundland undertook this collaborative project to
administer the GAIN SS and a demographic information form to youth aged 12 – 24 years seeking
service at their agencies. Service providers participated in training about youth substance abuse and
CD, with an emphasis on evidence-based screening practices, clinical use of the GAIN SS and
implementation of the project protocol. Service providers completed pre/post surveys about their own
knowledge, attitudes and practices related to youth substance use and mental health concerns. They
also provided feedback about their perceptions of the feasibility and utility of implementing the
screening tool in their practices and the impact of screening in particular and project participation
more generally on their referral practices. Presented in this report are the background and service
needs of youth who participated in this study as well as service provider perceptions of the screening
tool and related processes.
Development
In 2010, the Department of Health and Community Services, Mental Health and Addictions Division,
Newfoundland and Labrador expressed interest in development of a National Youth Screening Project
network in St. John’s in response to broad national dissemination of information about the project prior
to the submission of the proposal as well as following the funding announcement. Choices for Youth
expressed interest in developing and leading a cross-sectoral network ultimately comprised of four
local agencies that serve youth. Similar to the pilot screening projects described previously, the
agencies expressed interest in participating in a project to build capacity to identify and address the
complex needs of the youth who access their services as well as in having the opportunity to
document the needs of youth seeking service in their respective agencies, sectors and community.

St. John’s, Newfoundland
14
In September 2011, Choices for Youth formally agreed to take on the role of “Lead Agency” and
coordinate a local collaborative network to implement the GAIN SS[1] with youth seeking service at the
participating agencies. The project team held a one-day training workshop for service providers,
repeated on two consecutive days to allow for all agency staff to be trained, in St. John’s,
Newfoundland April 4-5, 2011. Service providers attended from all four participating agencies. Prior
to the training, the service providers were surveyed regarding their attitudes, knowledge and practices
related to youth substance use, mental health and co-occurring concerns. In January, all four
agencies launched the six-month data collection phase. Four of the Eastern Health programs
participated in all project activities. Five were unable to participate in the data collection activity. The
Complex Case Management program participated in capacity building and network development. The
Central Intake, Family Services Counsellors, Youth Services / Youth Corrections, and Youth Outreach
Counsellors participated in all project activities other than data collection, including GAIN SS
implementation.
The St. John’s, Newfoundland Network was established based on shared interests and concerns,
including interest in the opportunity to work together in a research-community collaboration.
Furthermore, the network members expressed a desire to lay the groundwork for on-going
partnerships and collaboration through their participation in the NYSP. The network was interested
and committed to ensuring that knowledge gained through this collaborative effort be shared locally,
provincially and nationally.
Partners
The St. John’s, Newfoundland Network includes representation from the addictions, family services,
housing, outreach & support, justice and mental health sectors, with both hospital and community-
based agencies and services included (see Appendix A for agency descriptions). Two thirds of the
agencies participated in all four project activities, which included: Capacity Building, Network
Development, Screening Implementation, and Data Collection. Please refer to Appendix B for a
description of key project activities and Appendix C for description of the respective agency
participation.
Roles
National Project Team:
Provide resources for and support meetings of youth-serving agencies to support all aspects of
project participation;
[1]
Chestnut Health Systems granted a license to Choices for Youth to use the GAIN SS (CAMH Version) and gave permission to Choices for Youth to include all the participating agencies in the network in its licensing agreement.

St. John’s, Newfoundland
15
Provide training to staff in identifying and addressing substance use and/or CD concerns in youth,
implementing the GAIN SS and the data collection protocol;
Provide all necessary screening and project-related materials;
Provide templates and support for developing response, resource and referral guides customised
for each community;
Obtain ethics approval through Health Canada and CAMH and support each agency to comply with
their ethics approval processes.
Lead Agency: Choices for Youth
Identify local organizations, representing a minimum of 3 sectors to participate in the project as a
participating agency;
Vet prospective participating agencies for suitability;
Act as a liaison between CAMH and participating agencies during the term of the project;
Identify and facilitate agency leads to obtain local REB approval for the project;
Obtain licenses from Chestnut Health Systems Inc. for use of the GAIN SS for participating
agencies;
Support training provided by the project leads and facilitate provision of consultation as needed
throughout the project;
Facilitate pre and post service provider surveys of staff attitudes, knowledge and practices to all
agency staff involved in the project;
Facilitate data collection by the participating agencies.
Participating Agencies:
Comply with the agreed upon protocol by obtaining participant and parental consents, administering
GAIN SS and submitting the data to the lead agency for review;
Ensure staff participation in project-related training;
Maintain and store original data from participants as per REB policies and in accordance with legal
requirements;
Ensure that as many eligible youth as possible have the opportunity to be included in the project
and that the rates of eligibility and consent are tracked.
Implementation Process
(See Appendix D for Project Timeline)
Prior to initiating project activities, two separate agreements were signed:
1. A two-party agreement between CAMH and Choices for Youth, the network lead agency.
2. A three-party agreement between CAMH, Choices for Youth and each of the respective
participating agencies.

St. John’s, Newfoundland
16
Each agreement described the project, roles, responsibilities, activities and commitments, as well as
the data collection protocol. Five of the programs in Eastern Health were unable to participate in all 4
of the key activities of the project; however, the Complex Case Management program participated in
the Capacity Building and Network Development activities, and Central Intake, Family Services
Counsellors, Youth Services / Youth Corrections, and Youth Outreach Counsellors programs also
participated in Screening Implementation.
A collaborative process was used throughout the project to develop joint goals, materials and
processes as well as research questions and data analyses. The lead agency, Choices for Youth, was
involved with the project throughout each stage of the project from initiation to completion. Once the
agency level training was completed and data collection was underway, the lead agency, along with
the project team at CAMH, was involved in communicating with the participating agencies to maintain
engagement, momentum, and compliance with the project protocol, problem-solving of issues arising
and collaborating in the joint data analysis process.
Implementation Process
1. May - November, 2010–Networking:
a. Identified interested agencies
b. Established cross-sectoral network
2. September,2010 - December 2011–Agreements and REB:
a. Developed 2-party agreement between CAMH and Choices for Youth
b. Developed 3-party agreement between CAMH, Choices for Youth and all
participating agencies
c. Secured all required REB approvals
3. April 4-5, 2011 – Capacity building
a. Capacity building across sites was delivered using the package developed by
the project leads
b. Project leads administered service provider consents and the Service Provider
Survey at the beginning of training day
c. Each Agency identified a lead to act as a “point person” for communication with
the Network Lead, including receiving and distributing project packages to the
participating service providers in their respective agencies
4. January 2012 – Project launch:
a. Distributed project packages i.e. project instruction sheets, consent forms, GAIN
SS, Background Information forms, tracking sheets
5. January – July 2012 – Project actively underway:
a. Service providers obtained consent from youth seeking service at their

St. John’s, Newfoundland
17
agencies, administered the GAIN SS and Background Information Form
b. Anonymous copies of the completed measures and tracking sheets were
submitted to the network coordinator on a monthly basis, and delivered to
CAMH at month 1, 3 and 6
c. Consultation was provided as needed by the network coordinator and/or project
coordinator/project leads
d. Staff feedback forms were collected on completion of the data collection
e. Additional teleconference capacity building sessions were provided to train staff
who could not attend the in-person sessions in the administration of the
measures and the project protocol
6. October 4th. 2012 – Preliminary data analysis meeting:
Discussed:
a. Data analysis questions
b. Preliminary findings
c. Fit with expectations and experiences of the community
d. Lessons learned, including staff feedback provided on utility and feasibility of
administering the GAIN SS to youth in their agencies
e. Feedback from network and agency leads
f. Potential recommendations based on findings
g. Report dissemination plan
Materials
Service Provider Project Package
Service Provider Consent Form
The consent form described the project, confidentiality and plans for data management. Service
providers’ initials only were required to ensure anonymity.
Service Provider Survey
The Service Provider Survey is a self-report questionnaire that combines measures of service
providers’ 1) service-related knowledge, attitudes and practices regarding youth substance use,
mental health, co-occurring disorders, and screening; 2) perceptions of co-occurring disorders-
informed practices; 3) estimates of current use of CD-informed practices; and 4) experiences with
inter-agency referrals and collaboration.
Project Flow Chart (See Appendix E)

St. John’s, Newfoundland
18
A step-by-step project flow chart was developed for use by all service providers to facilitate
consistency across providers.
Referral Resource Guide
Customised templates listing local resources for consultation and referrals for follow-up to
endorsement of concerns on the GAIN SS were provided to each participating service provider.
GAIN SS Tracking Sheet
Tracking sheets were used to document rates of youth eligibility for project participation, consent/non-
consent, participation/reasons for non-participation, and data collection completion and submission for
each youth seeking service in each agency.
Feedback Survey
The feedback survey was designed to gather information from participating service providers
regarding their perceptions of the feasibility and utility of administering the GAIN SS to youth in their
setting and about the impact of the screening process on their practices.
Youth Project Package
Youth Consent Form
The consent form described the project, confidentiality and plans for data management. Youth initials
only were required to ensure anonymity.
Parental Consent Form
The consent form described the project, confidentiality and plans for data management. Parental
consent was required in addition to youth consent only where parental consent was required to obtain
services for youth under 16 years of age. Parent’s initials only were required to ensure anonymity.
Background Information Form
The Background Information Form is a one-page questionnaire used to gather demographic
information about the participating youth. The questions seek information about the determinants of
health frequently cited in the literature as associated with youth substance use and mental health
concerns including age, sex, education, employment, income support, housing, legal involvement,
ethno-racial identification, and language diversity.
GAIN SS (CAMH Version)
The GAIN SS is a brief screening tool validated for use with individuals aged 10 years and older to
quickly identify those who may be experiencing difficulties in one or more of four dimensions: 1)
internal mental distress (e.g., depression, anxiety); 2) behavioural complexity (externalizing
behaviours e.g., ADHD); 3) substance use problems; and 4) crime and violence (Denis, Chan, &

St. John’s, Newfoundland
19
Funk, 2006). The tool was developed by Chestnut Health Systems and copyrighted in 2005. Chestnut
Health Systems permitted CAMH’s Child, Youth and Family Program to modify the GAIN SS in 2006,
by adding seven items (not part of the original validation) at the end to screen for: eating-related
issues, trauma-related distress, disordered thinking and gambling, gaming and internet misuse
concerns.

St. John’s, Newfoundland
20

St. John’s, Newfoundland
21
Findings

St. John’s, Newfoundland
22

St. John’s, Newfoundland
23
Background Information about Youth
Who participated?
In total, 107 youth participated:
63 (59%) from housing, outreach, and support sector
44 (41%) from treatment sector
How representative is the sample of youth who participated in the project?
Service providers were asked to use tracking sheets to record each youth eligible to participate.
Information collected on the tracking sheets included sex, age, consent response, and any comments
on why individual youth may not have been approached or refused to consent. All participating
agencies used this approach to track participation rates.
According to the tracking sheets provided by the service providers 136 youth presented for service to
the participating programs and agencies over the course of the six-month project timeframe. Of these
youth 87% were eligible for the project (n = 118). Reasons for ineligibility included the GAIN SS had
already been administered (14%), immediate mental health concerns (e.g., psychosis) (43%), and
cognitive limitations (43%). In addition, for 11 cases information was not provided. Of the youth who
were eligible to participate in the project, 111 (94%) were approached for participation. Reasons for
youth not being approached included clinician-based reasons (e.g., judgment) (57%), youth was
unavailable (e.g., left, no show) (14%), and parent unavailable to provide required consent (29%). Of
the youth who were approached, 95% completed the GAIN SS. Based on the tracking sheets, 5% of
youth who were asked to complete the GAIN SS refused. Of the youth who completed the GAIN SS,
100% consented to have a copy used for the purposes of this project. Overall then, based on these
tracking sheet numbers, 90% of eligible youth contributed screeners for this report.
Please note: Based on the number of completed consents and screeners we received, we estimate
that approximately 99% of eligible youth were captured on tracking sheets.

St. John’s, Newfoundland
24
What are the demographics of the youth who participated?
AGE
FIGURE 1: AGE DISTRIBUTION OF PARTICIPANTS
The participating youth ranged in age from 14 to 24 years with an average age of 18.2 years and a
median age of 17.0 years. In Figure 1, the ages of participating youth are presented using age
categories commonly used in service provision. As can be seen, participating youth were evenly
distributed across age categories.
33%
34%
33% 12-16 years old
17-19 years old
20-24 years old

St. John’s, Newfoundland
25
FIGURE 2: AGE DISTRIBUTION BY SERVICE SECTOR
When youth are grouped by sector (see Figure 2), it can be seen that youth who participated in the
housing, outreach, and support sector were more likely to be in the older age group (20 to 24 years),
whereas the majority of participating youth presenting to the treatment sector were12 to 16 years old.
8%
70%
37%
30% 56%
0%
10%
20%
30%
40%
50%
60%
70%
80%
90%
100%
Housing, Outreach, & Support Treatment
Pro
po
tio
n o
f Y
ou
th
Sector
20-24years
17-19years
12-16years

St. John’s, Newfoundland
26
Sex
FIGURE 3: SEX DISTRIBUTION OF PARTICIPANTS
This project had 51 male participants, 54 female participants, and one participant who identified as
trans. The difference in the number of male and female participants was not significant. There was
also one individual who did not provide this information. In order to protect the privacy of participants,
only those who identified as male or female are included in subsequent analyses related to sex.
48%
50%
1% 1%
Male
Female
Trans
Missing

St. John’s, Newfoundland
27
FIGURE 4: SEX DISTRIBUTION OF PARTICIPANTS BY SERVICE SECTOR
Comparing the two sectors reveals that the male to female ratio does not differ between sectors.
51% 45%
49% 55%
0%
10%
20%
30%
40%
50%
60%
70%
80%
90%
100%
Housing, Outreach, & Support Treatment
Pro
po
rtio
n o
f Y
ou
th
Sector
Female
Male

St. John’s, Newfoundland
28
Service History
FIGURE 5: SERVICE HISTORY BY SERVICE SECTOR
More youth participating in the project endorsed being involved with the participating service for more
than a year (37%) than any other option. There was a fair amount of variability between sectors. For
example, more youth from the treatment sector completed the GAIN SS on their first visit or in their
first month (46%) of being with the service than youth from the housing, outreach, and support sector
(22%).
7%
23% 15%
23% 31%
31%
47%
23%
0%
10%
20%
30%
40%
50%
60%
70%
80%
90%
100%
Housing, Outreach, & Support Treatment
Pro
po
rtio
n o
f Y
ou
th
Sector
More thana year ago
2-12Monthsago
In the pastmonth
Today

St. John’s, Newfoundland
29
Ethnicity
FIGURE 6: ETHNICITY DISTRIBUTION OF PARTICIPATING YOUTH
Seven percent of participating youth endorsed more than one ethnicity. The most commonly endorsed
ethnicity across all youth was White/European (85%), followed by Aboriginal (9%), ‘Don’t know’ (3%),
‘Other’ (2%), and Black (1%). Five percent of youth (n = 5) did not complete this question.
Birth Country and First Language
The majority of participating youth reported being born in Canada (96%) while 2% reported being born
outside of Canada and 2% did not answer the question. Those born outside of Canada reported
having been in Canada two and 15 years respectively. The majority of participating youth also
reported that English was their first language (95%), while 2% reported a different first language and
3% left it blank. One individual indicated Inuktitut as their first language; no other languages were
reported for non-English first language.
9% 1%
85%
2%
3%
Aboriginal
Black
White / Europe
Other
Don't know

St. John’s, Newfoundland
30
Living Arrangements
FIGURE 7: CURRENT LIVING ARRANGEMENTS
The largest group of participating youth (45%) reported that they were living with parents, while 27%
reported living in unstable housing (e.g. “shelter”, “on street”, “couch surfing”), 11% were living on
their own or with friends, 8% reported living in supportive housing (e.g. “group home”, “treatment
facility”) and 4% were living with other family members.
45%
11% 4%
8%
27%
1%
4%
Parental/Family Home
Own/With Friends
Other Family/Relative
Supportive Housing
Unstable
Other
Missing

St. John’s, Newfoundland
31
FIGURE 8: CURRENT LIVING ARRANGEMENTS BY SEX
Examination of sex differences in living arrangements revealed that the living arrangements of male
and female youth did not differ significantly.
46% 45%
10% 13%
6% 2%
10% 8%
25%
32% 2%
0%
10%
20%
30%
40%
50%
60%
70%
80%
90%
100%
Male Female
Pro
po
rtio
n o
f Y
ou
th
Sex
Other
Unstable
Supportive Housing
Other Family/Relative
Own/With Friends
Parental/Family Home
St. John’s, Newfoundland
32
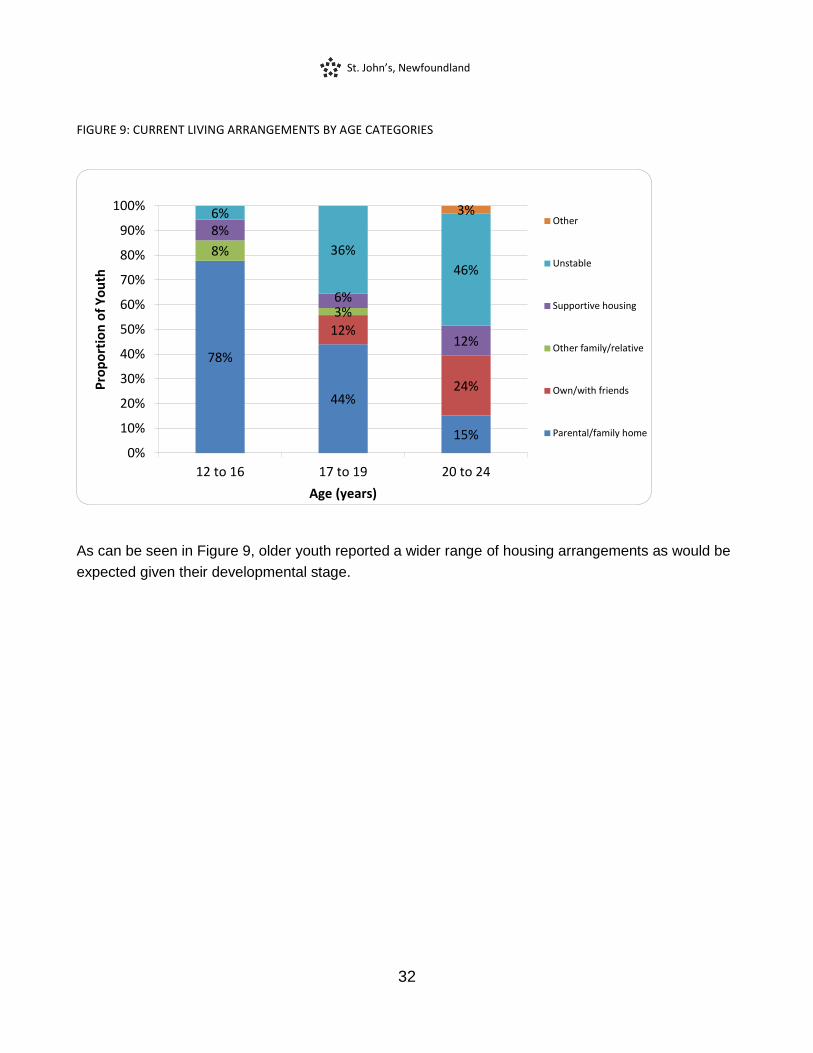
FIGURE 9: CURRENT LIVING ARRANGEMENTS BY AGE CATEGORIES
As can be seen in Figure 9, older youth reported a wider range of housing arrangements as would be
expected given their developmental stage.
78%
44%
15%
12%
24%
8%
3%
8%
6%
12%
6%
36%
46%
3%
0%
10%
20%
30%
40%
50%
60%
70%
80%
90%
100%
12 to 16 17 to 19 20 to 24
Pro
po
rtio
n o
f Y
ou
th
Age (years)
Other
Unstable
Supportive housing
Other family/relative
Own/with friends
Parental/family home

St. John’s, Newfoundland
33
FIGURE 10: CURRENT LIVING ARRANGEMENTS BY SERVICE SECTOR
As would be expected given the services provided by the housing, outreach, and support sector, there
is more variability in living arrangement than in the treatment sector which predominantly serves youth
who live in parental/family homes.
17%
86% 3%
5%
8%
9%
49%
2%
0%
10%
20%
30%
40%
50%
60%
70%
80%
90%
100%
Housing, Outreach, & Support Treatment
Pro
po
rtio
n o
f Y
ou
th
Sector
Other
Unstable
Supportive Housing
Other Family/Relative
Own/With Friends
Parental/Family Home
St. John’s, Newfoundland
34
Legal Involvement
The majority of participating youth reported never having any legal involvement (54%), while the
remaining youth reported legal involvement in the past 12 months (27%), more than a year ago
(14%), or did not answer the question (5%).
Education, Employment and Income
Overall 37% of participating youth identified as students. Of those who did not identify as students,
79% indicated that they were unemployed, 11% indicated part-time employment, 5% indicated they
had full-time employment, 3% indicated involvement in an apprenticeship program, and 2% indicated
self-employment.
Age was related to educational, employment and income status. Youth aged 18 years and older (n =
53), indicated that their employment situations were as follows: unemployed (75%), attending school
(12%), working part-time (10%), working full-time (6%), and in an apprenticeship program (4%), (not
mutually exclusive). In contrast youth aged 17 years or younger (n = 54) indicated that they were
students (63%), unemployed (33%), working part-time (9%), volunteering (4%), and in an
apprenticeship program (2%). Similarly, the most commonly reported income sources for youth aged
18 and older were as follows: welfare (62%), no income (17%), employment (9%), family benefits
(4%) parents/spouse (4%), and disability (4%) while youth 17 years and younger reported their
income sources to be parents/spouse (22%), no income (39%), Choices for Youth/CYFS (15%);
family benefits (9%), welfare (9%), and employment (7%).
For youth aged 18 years and older, educational attainment was also examined revealing a broad
range of educational achievements, including 10% of youth participants reporting grade 8 completion
or less as their highest educational achievement, 65% indicating grades 9-11 as their highest
achievement, 8% reporting achievement of high school completion without diploma, 14% indicating
completion of high school with diploma, 2% obtaining a trade or vocational certificate, and 2%
completing some non-university post-secondary education.

St. John’s, Newfoundland
35
How do the demographics of males and females compare?
TABLE 1: DEMOGRAPHIC COMPARISON OF MALE AND FEMALE PARTICIPANTS
Male Female
Average Age 18.3 18.2
White / European
Aboriginal
88%
6%
82%
14%
Born in Canada 98% 98%
English First Language 100% 96%
Unstable Housing 25% 32%
Legal Involvement 58% 31%*
*p<.05
Examination of potential differences in background characteristics between male and female youth
revealed that they only differed significantly in their histories of legal involvement, with male youth
reporting significantly higher rates of current and previous legal involvement.
St. John’s, Newfoundland
36
Clinical Needs of Youth Based on the GAIN SS
The GAIN SS is a well-validated and reliable screener for mental health and substance use concerns
in youth and adults. It has four 5-item subscreeners embedded within the overall measure to screen
across four domains: Internalizing (INT) disorders (e.g., mood, anxiety disorders), Externalizing (EXT)
disorders (e.g., attention deficit/hyperactivity disorder), Substance Use disorders (SUB), and
engagement in Crime/Violence (CV). In order to fully understand the findings presented in this report,
it is important to understand the scoring decisions that informed the analyses. The GAIN SS has been
shown to have excellent sensitivity and specificity. These rates change, however, depending on how
the GAIN SS is scored and analyzed.
Within each subscreener using a moderate threshold of at least one recent (2-12 months ago) or
current (past month) concern has excellent sensitivity (94-98%) for identifying youth who will meet
diagnostic criteria for disorder, but lower (71-76%) specificity, i.e. lower accuracy in ruling out youth
who will not meet diagnostic criteria for disorder. Using a high threshold of three or more recent or
current concerns within one domain improves the specificity to 96-100%, but results in decreases in
sensitivity (49-68%). Using a threshold of three or more current or recent concerns endorsed across
all domains (total) will identify 91% of youth who will meet diagnostic criteria for a disorder and will
rule out 90% of youth who will not have a disorder (Dennis, Chan, & Funk, 2006).
Depending on the service setting, use of each threshold may be more appropriate. For example, in
settings where the rates of clinically significant mental health and substance use problems are
expected to be low (e.g. primary care), use of the moderate threshold may be most appropriate. In
settings where individuals are seeking service for mental health and substance use concerns, use of
the high threshold may be more informative.
For this project, a modified version of the GAIN SS was used (GAIN SS CAMH Modified Version)
which includes 7 additional items following the original subscreeners. These additional items provide
information about eating behavior, thinking-related issues, traumatic distress, and gambling, gaming
and internet overuse. Sensitivity and specificity data for these items are not yet available and these
items are not scored.
St. John’s, Newfoundland
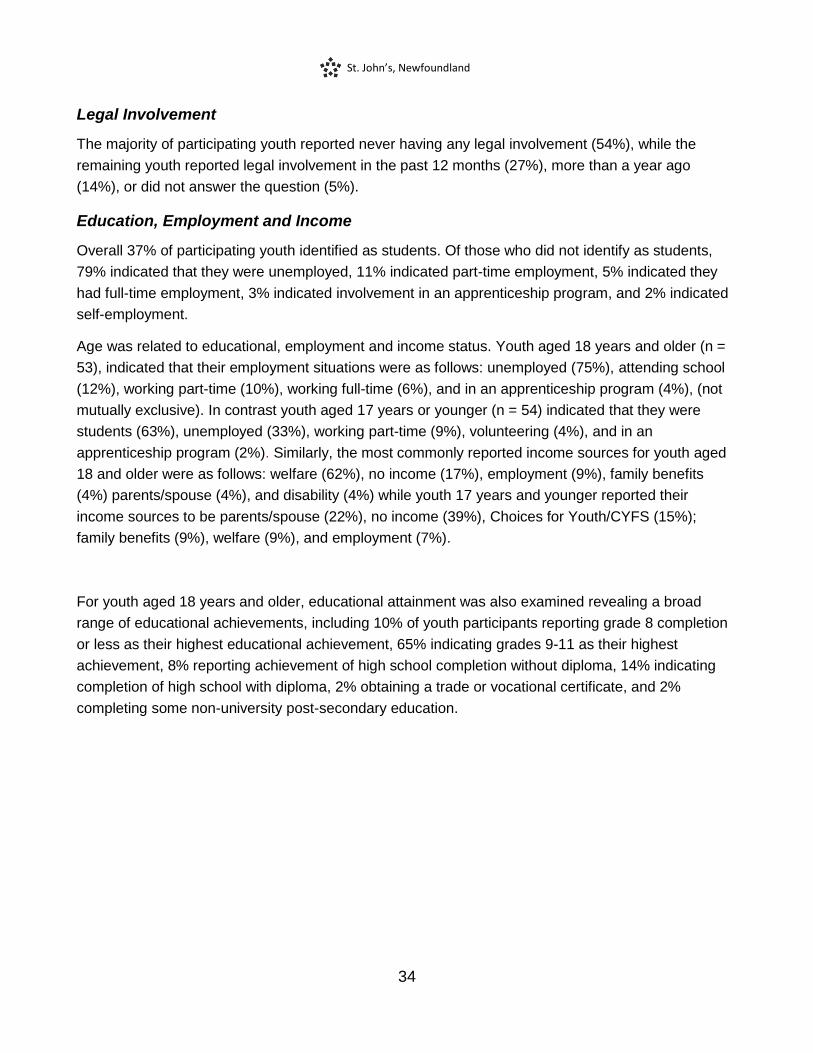
37
FIGURE 11: NUMBER OF CONCERNS ENDORSED BY GAIN SS DOMAIN
As can be seen in Figure 11, more than two thirds of participating youth endorsed 3 or more recent
internalizing concerns, suggesting that with a full diagnostic assessment they may meet criteria for a
diagnosis in the internalizing domain (e.g. mood disorder, anxiety disorder, etc.). Similarly, in the
externalizing domain more than half of youth endorsed 3 or more recent externalizing concerns.
Endorsement of 3 or more concerns on the substance disorder subscreener was less common, but
nevertheless, almost half of participating youth reported 3 or more recent indications of problematic
substance use. In the area of crime and violence, almost a quarter of youth reported 3 or more
crime/violence concerns. Overall, 94% of participating youth endorsed 3 or more issues across the 4
subscales, suggesting that most participating youth would receive a diagnosis with a full diagnostic
assessment.
7% 12%
30% 36% 24%
29%
21%
42%
6%
69% 59%
49%
22%
94%
0%
10%
20%
30%
40%
50%
60%
70%
80%
90%
100%
INT EXT SUB CV Total
Pro
po
rtio
n o
f Y
ou
th
GAIN SS Domain
3+ recentconcerns
1-2 recentconcerns
No recentconcerns

St. John’s, Newfoundland
38
How do the needs of youth differ across sectors?
FIGURE 12: RECENT CLINICAL NEEDS USING MODERATE THRESHOLD (1+ ENDORSEMENTS) BY SERVICE SECTOR
In Figure 12, the needs of youth by service sector are presented. Using the threshold of 1
endorsement to identify youth who screen positive, more than 90% of youth regardless of sector,
screened positive for internalizing concerns. Similarly, more than 80% of youth across sectors
screened positive for externalizing concerns. Within the substance use and crime and violence
domains, rates of endorsement ranged from 59%-77% across sectors. Youth presenting to the
treatment sector were more likely to screen positive for externalizing difficulties than youth presenting
to housing, outreach and support, while youth presenting to housing, outreach and support were more
likely than youth presenting to the treatment sector to screen positive for substance use problems.
92%
84% 77%
68%
96% 95%
59% 59%
0%
10%
20%
30%
40%
50%
60%
70%
80%
90%
100%
INT EXT SUB CV
Pro
po
rtio
n o
f Y
ou
th
GAIN SS Domain
Housing,Outreach,and Support
Treatment

St. John’s, Newfoundland
39
FIGURE 13: RECENT CLINICAL NEEDS USING HIGH THRESHOLD (3+ ENDORSEMENTS) BY SERVICE SECTOR
Using a threshold of three or more recent or current concerns within one domain improves the
specificity (i.e. fewer false positives) of the GAIN SS screener and allows identification of youth with
higher severity of needs.
As can be seen in Figure 13, the majority of youth presenting for service across sectors have high
internalizing concerns. In addition, over 80% of youth presenting to the treatment sector reported
experiencing high severity externalizing difficulties.
In the substance use domain, approximately half of youth endorsed experiencing 3 or more symptoms
of problematic substance use in the past year.
In the area of crime and violence, rates of endorsement were substantially lower than other domains,
although approximately one quarter of youth endorsed 3 or more crime and violence problems.
67%
44% 52%
18%
73%
81%
46%
30%
0%
10%
20%
30%
40%
50%
60%
70%
80%
90%
100%
INT EXT SUB CV
Pro
po
rtio
n o
f Y
ou
th
GAIN SS Domain
Housing,Outreach, andSupport
Treatment

St. John’s, Newfoundland
40
How do the needs of youth differ across age and sex categories?
FIGURE 14: RECENT INTERNALIZING CONCERNS BY AGE AND SEX CATEGORIES
Overall, female youth were more likely to endorse internalizing concerns than male youth, although as
can be seen in Figure 14 this is true for younger youth only. In the older age group male and female
youth did not differ in their rates of endorsement.
48% 50%
67%
93% 91%
63%
0%
10%
20%
30%
40%
50%
60%
70%
80%
90%
100%
12 to 16 17 to 19 20 to 24
Pro
po
rtio
n o
f Y
ou
th
Age
Male
Female

St. John’s, Newfoundland
41
FIGURE 15: RECENT EXTERNALIZING CONCERNS BY AGE AND SEX CATEGORIES
As shown in Figure 15, younger youth were more likely to endorse externalizing concerns than older
youth.
86%
45% 53%
80%
59%
31%
0%
10%
20%
30%
40%
50%
60%
70%
80%
90%
100%
12 to 16 17 to 19 20 to 24
Pro
po
rtio
n o
f Y
ou
th
Age
Male
Female

St. John’s, Newfoundland
42
FIGURE 16: RECENT SUBSTANCE USE CONCERNS BY AGE AND SEX CATEGORIES
Male youth overall were more likely to endorse problematic substance use concerns than female
youth.
62%
45%
67%
47%
35%
44%
0%
10%
20%
30%
40%
50%
60%
70%
80%
90%
100%
12 to 16 17 to 19 20 to 24
Pro
po
rtio
n o
f Y
ou
th
Age
Male
Female

St. John’s, Newfoundland
43
FIGURE 17: RECENT CRIME AND VIOLENCE CONCERNS BY AGE AND SEX CATEGORIES
Crime and violence problems were more commonly endorsed by male than female youth, especially
male youth in the oldest age category.
38%
27% 28% 27%
13%
0% 0%
10%
20%
30%
40%
50%
60%
70%
80%
90%
100%
12 to 16 17 to 19 20 to 24
Pro
po
rtio
n o
f Y
ou
th
Age
Male
Female

St. John’s, Newfoundland
44
FIGURE 18: RECENT SUICIDE CONCERNS BY AGE AND SEX CATEGORIES
Given the clinical importance of suicide-related concerns, the single item related to suicide-related
thinking and behavior from the internalizing subscreener was examined. Overall, 15% of participating
youth indicated that they had thought about suicide in the past month, with an additional 19%
reporting having thought about suicide in the past 2 to 12 months and 25% reporting concerns more
than 12 months ago. Forty-one percent of youth indicated they had never thought about suicide.
When we examined rates of endorsement by sex and age category it was revealed that female youth
were more likely than male youth to endorse suicide concerns, especially in the younger age
categories.
14% 9%
22%
67%
48%
38%
0%
10%
20%
30%
40%
50%
60%
70%
80%
90%
100%
12 to 16 17 to 19 20 to 24
Pro
po
rtio
n o
f Y
ou
th
Age
Male
Female

St. John’s, Newfoundland
45
Other Clinical Needs
How many youth endorsed additional areas of concern?
As part of the process of meeting the needs of service sector stakeholders, and with the permission of
Chestnut Health Systems, the copyright holders of the GAIN SS, we added 7 items to the end of the
GAIN SS. The items that were added were not part of the original GAIN SS nor the validation study
(Dennis et al., 2006), and as a result their reliability, validity, and utility are unknown. Nevertheless, it
was identified by stakeholders that it would be important to ask about other areas of concern expected
to be important for the youth participants so that these areas could be explored further if youth
indicated any concerns. The items were from the areas of eating concerns (2 items), traumatic stress
(1 item), disordered thinking concerns (2 items), gambling concerns (1 item) and gaming/internet
concerns (1 item).
FIGURE 19: RATES OF RECENT ADDITIONAL CONCERNS BY SEX CATEGORIES
As can be seen, the distressing memories/dreams (traumatic distress) item was endorsed by
approximately half of youth and was the most commonly endorsed additional item. Youth were least
likely to endorse concerns about gambling. Female youth were significantly more likely than male
youth to endorse eating concerns and thoughts of persecution, while male youth were more likely than
female youth to endorse videogame overuse.
0%10%20%30%40%50%60%70%80%90%
100%
Pro
po
rtio
n o
f Y
ou
th
Additional Concerns
Male
Female

St. John’s, Newfoundland
46
Concurrent Substance Use and Mental Health Concerns
This project used the GAIN SS to identify youth who are likely to have concurrent disorders (i.e., co-
occurring substance use and mental health concerns). Youth who endorsed at least three recent
concerns in the substance use domain as well as at least three recent concerns in either the
internalizing or externalizing domain were identified as endorsing a concurrent disorder.
How many youth endorsed both substance use and mental health concerns?
FIGURE 20: RATES OF ENDORSEMENT OF CONCURRENT DISORDERS
INT
SUD
14%
6% 5%
5%
6%
34%
15% Did not screen positive for INT, EXT, or SUD
13%
EXT

St. John’s, Newfoundland
47
Overall, 59% of youth screened positive for more than one area of concern, and 45% of participating
youth screened positive for possible concurrent (substance and mental health) disorders. As can be
seen in the Figure 20, 34% of all participating youth screened positive for co-occurring internalizing,
externalizing and substance use concerns, 6% endorsed concurrent internalizing and substance use
concerns, and 5% indicated concurrent externalizing and substance use concerns.

St. John’s, Newfoundland
48
How similar were rates of Concurrent Disorder endorsement across service sectors?
FIGURE 21: RATES OF ENDORSEMENT OF CONCURRENT DISORDERS BY SERVICE SECTOR AND SEX
Overall, 45% of youth across sectors screened positive for concurrent disorders, with the rates
between sectors being equivalent. There was also a trend for male youth to be more likely to screen
positive for concurrent disorders than female youth across service sectors.
52% 58%
39% 35%
0%
10%
20%
30%
40%
50%
60%
70%
80%
90%
100%
Housing, Outreach, & Support Treatment
Pro
po
rtio
n
of
Yo
uth
Sector
Male
Female

St. John’s, Newfoundland
49
What factors are related to endorsing both mental health and substance use concerns?
Age and Sex
FIGURE 22: RATES OF ENDORSEMENT OF CONCURRENT DISORDERS BY AGE AND SEX
Overall 54% of male youth and 37% of female youth endorsed co-occurring mental health and
problematic substance use. When rates of endorsement were examined by age categories, 50% of
the youngest age group, 35% of the middle age group, and 50% of the oldest age group screened
positive for concurrent disorders. There was a trend for male youth to be slightly more likely to
endorse concurrent disorders than female youth, but no significant age differences.
Living Arrangements
For the purposes of the following analyses living arrangements were reduced to two categories: 1)
parental/family home and 2) living outside of the parental/family home. Rates of endorsement of
concurrent disorders, however, did not differ significantly between youth who live outside of the
parental/family home (50%) and youth living in the parental/family home (41%).
57%
36%
61%
40% 35%
38%
0%
10%
20%
30%
40%
50%
60%
70%
80%
90%
100%
12 to 16 17 to 19 20 to 24
Pro
po
rtio
n o
f Y
ou
th
Age
Male
Female

St. John’s, Newfoundland
50
Legal Involvement
FIGURE 23: RATES OF ENDORSEMENT OF CONCURRENT DISORDERS BY LEGAL SYSTEM INVOLVEMENT
For the purposes of the following analyses, legal involvement was reduced to two categories: 1) no
legal involvement and 2) previous legal involvement. Youth who reported past legal involvement were
more likely to endorse concurrent disorders (59%) than youth who reported no previous involvement
with the legal system (34%). This was especially true for female youth. In addition, more than half of
youth (58%) who screened positive for concurrent disorders reported previous legal involvement.
Educational Status
When we compared youth who identified as students to those who did not, it was revealed that 44%
of students and 45% of non-students endorsed concurrent substance use and mental health
concerns, indicating that educational status was not related screening positive for concurrent
disorders.
45%
57%
28%
63%
0%
10%
20%
30%
40%
50%
60%
70%
80%
90%
100%
No legal involvement Previous legal involvement
Pro
po
rtio
n o
f Y
ou
th
Legal Involvement
Male
Female

St. John’s, Newfoundland
51
Which factors are most important in understanding the Concurrent Disorder needs of youth presenting for service in St. John’s, Newfoundland?
Given that both sex and legal involvement were found to be related to endorsing both problematic
substance use and mental health concerns, and that these factors are related to each other, we
examined these factors together in one analysis to understand which factor(s) are most important in
understanding who screens positive for concurrent disorders. When sex and legal involvement were
examined together, legal involvement was shown to be most important in understanding which youth
are more likely to endorse both substance use and mental health concerns. More specifically, youth
with legal involvement were more likely to endorse both substance use and mental health concerns,
even after the effects of sex were taken into consideration.
How many participants endorsed multiple areas of concern in their lives?
FIGURE 24: COMPLEXITY OF NEEDS
In order to understand how many participants experience multiple areas of concern we also examined
the following social determinants of health, along with mental health and substance use concerns: 1)
housing (unstable or supportive), 2) education/occupation (under 18 and not a student or 18 and older
and not a student and not employed), 3) legal involvement (past or current legal involvement), 4)
28%
52%
20%
44% 41%
15%
0%
10%
20%
30%
40%
50%
60%
70%
80%
90%
100%
0-2 3-4 5-6
Pro
po
rtio
n o
f Y
ou
th
Number of Significant Needs
Male
Female

St. John’s, Newfoundland
52
internalizing concerns (high severity), 5) externalizing concerns (high severity), and 6) substance use
problems (high severity). Overall, 62% of participants reported having 3 or more factors and almost a
fifth (17%) of participants reported experiencing 5 or more of the 6 factors. Results did not differ for
male and female youth. These findings highlight the complexity of the needs of the individuals who
are presenting for service and participated in this project.

St. John’s, Newfoundland
53
Service Provider Survey
This project included a survey about service providers’ attitudes, knowledge, and practices regarding
youth substance use, mental health, and concurrent disorders. Questions about interagency
collaboration and interagency referral practices were also included in the survey. In addition, the
project included a feedback survey that gathered information regarding the feasibility, utility, and
impact of using the GAIN SS.
Service providers in the St. John’s, Newfoundland Region (n = 53) completed the service provider
survey prior to participating in the project’s capacity building training event and then again with the
feedback survey (n = 19) approximately one year after training took place. Detailed results for the
service provider survey can be found in the National Youth Screening Project national report. The
results from the feedback survey of St. John’s, Newfoundland service providers are presented
following.

St. John’s, Newfoundland
54
Feasibility and Utility of the GAIN SS
FIGURE 25: SERVICE PROVIDER PERCEPTIONS OF GAIN SS UTILITY AND FEASIBILITY
Service providers who provided feedback reported that generally the GAIN SS was useful, impacted
treatment decisions, and facilitated referrals. The majority of service providers recommended using
the GAIN SS despite some also reporting a perceived disruption from its use. Notably, those service
providers who perceived the training to be more helpful reported the measure to impact service and
recommendations more frequently and to facilitate the referral process more often than service
providers who rated the training as less helpful.
87%
47%
87% 80%
93%
0%
10%
20%
30%
40%
50%
60%
70%
80%
90%
100%
Usefulinformation
at least someof the time
Notdisruptive
Impactedservice at
least some ofthe time
Facilitatereferral at
least some oftime
Recommenduse at leastsome of the
time
End
ors
em
en
t R
ate
GAIN SS Utility and Feasibility

St. John’s, Newfoundland
55
Service provider comments about the feasibility and utility of the GAIN SS in their
practices
“We are more attentive to making sure mental health is immediately addressed as
well as substance abuse.”
“I found this instrument difficult to administer and inappropriate to administer in a first
session.”
“It is a co-occurring screener which we don’t have currently which can be used easily
and effectively.”
“It has resulted in some additional partnership among network members who are
now delivering some programs together to at-risk youth.”
“Choices for Youth is a partner in the National Youth Screening Project. The use of
GAIN-SS was an appropriate fit for the work of our Outreach and Youth Engagement
program, and in particular, 3 key program areas also being funded by DTFP.
Addictions Community Support (focused on engaging youth with addictions issues
and connecting them to appropriate supports and service by building meaningful
relationships with them); Jumpstart (a pre-employment program for youth facing
many employment barriers including addictions); and Momma Moments (a group for
our young moms who are also experiencing isolation and multiple other barriers
while offering a supportive environment for young parents to seek appropriate
support i.e. Mental Health and Addictions).
“Through use of GAIN-SS, we have established a screening and assessment
process that allows us to develop individual support plans for the youth we are
working with. For some youth, it has helped identify issues they may be struggling
with that were difficult to disclose or discuss, or at times were unaware of the root of
their struggles. Completion of the GAIN-SS often results in starting conversations
about concerns youth had and supports they really needed.”

St. John’s, Newfoundland
56
Summary of Findings
Approximately 90% of eligible youth presenting to participating services and agencies contributed to
this report.
100% of youth who completed the GAIN SS gave consent for it to be included in this report.
Youth presenting for services from addictions, mental health, and outreach, housing and support
service sectors contributed information to this report.
Youth aged 14 to 24 years participated, with differences in age being apparent across service
sectors.
Participants were evenly split between male and female participants.
The majority of participants identified their ethnicity as white/European, reported being born in
Canada and having English as their first language.
As would be expected older youth and youth presenting for service to the outreach, housing and
support services sector endorsed a wider variety of current living arrangements and were less likely
to live in the parental/family home.
Over half of male youth (58%) and almost a third of female youth (31%) indicated that they had
experienced legal involvement.
The majority of participating youth screened positive for significant internalizing or externalizing
mental health concerns and/or problematic substance use. Moreover, substantial numbers of youth
from each sector endorsed significant difficulties.
Age and sex are related to rates of endorsement across domains.
Over one third (34%) of participating youth reported significant suicide-related concerns in the past
year and more than half reported suicide-related concerns in their lifetimes (59%).
More than half of participating youth (59%) screened positive for more than one disorder and 45% of
youth screened positive for co-occurring mental health and substance use concerns.
Factors found to be significantly related to experiencing co-occurring mental health and substance
use concerns for youth participating in the project include sex and legal involvement. Of these the
most important appear to be legal involvement, especially female youth with legal involvement.
Complexity of the needs of the participating youth was evident in the high number (62%) reporting 3
or more concerns out of 6 that include social determinants of health along with mental health and
substance use.
The majority of service providers reported that they found the GAIN SS provided useful information,
impacted service delivery and facilitated referrals. Higher ratings in some areas were associated
with service provider perceptions of the capacity building activities.

St. John’s, Newfoundland
57
Discussion
Youth Needs
The findings of this project in St. John’s, Newfoundland suggest that many youth presenting for
service, regardless of which sector they present to, are experiencing significant substance use and/or
mental health concerns. Moreover, almost half of participating youth endorsed significant concerns in
more than one domain, and one quarter of youth screened positive for co-occurring substance and
mental health concerns. These findings suggest that recent efforts to improve capacity to address co-
occurring substance use and mental health problem are warranted.
The findings of this report also support the need for gender-sensitive and developmentally-informed
approaches with youth. The concerns and needs of male and female youth differed, as did the needs
and concerns of younger and older youth. For example, girls in the youngest age categories were
more likely to report suicide-related concerns than boys, but in the older age category male and
female youth did not differ significantly. Also, female youth with legal involvement were much more
likely to have screened positive for concurrent disorders than female youth without legal involvement.
These, and other findings from the project, have implications for service delivery, both in terms of
thinking about issues such as access, but also in terms of what services might be most applicable at
different ages and for male and female youth. Unfortunately the number of youth who identify as trans
who participated was too small to allow for meaningful analyses. Future projects should aim to better
understand the needs of this often overlooked group of youth.
Project and Implementation Processes
As described in this report there were several essential steps required to initiate, carry out and
complete this project. First and foremost, local leadership was required to build a network through
identifying, engaging and supporting partners from various youth service sectors. In Newfoundland,
the efforts of representatives from the Department of Health and Community Services, Newfoundland
and Labrador and Mental Health and Addiction Services, Eastern Health, who had learned about the
project through their involvement in national committees, including the Federal Provincial Territorial
(FPT) Committee, to identify local leadership and interested agencies in St. John’s facilitated
community engagement in the project. The enthusiasm and sustained hard work of the Choices for
Youth lead resulted in the St. John’s, Newfoundland service community’s active engagement in the
project. They exceeded their initial agreement to enlist partners representing four service sectors;
rather, enlisting six (addictions, mental health, family services, health, outreach, housing and support
and youth justice). It should be noted that the sectors were represented in the broad spectrum of

St. John’s, Newfoundland
58
programming available across four agencies. Service providers from all six sectors participated in the
network development and capacity building activities. Ultimately all of the sectors were represented in
all aspects of the project, however not all of the participating programs engaged in the data collection
component of the project (See Appendix C).
Providing more than one capacity building event, including teleconference training options for those
who could not attend the “live” events, provided greater opportunity for all agency staff to receive
training directly from the project leads. This helped to ensure that all aspects of the protocol were
clearly and consistently communicated. Agencies decided to send staff who would participate in the
full project as well as staff who might use the screening tool with populations that were not part of this
project (e.g., adults older than 24 years), and staff who would not be administering the screener, given
their role in the agency but might receive youth who had been screened. As such, the capacity
building component of the project had a broader reach than initially anticipated.
Staff concerns about potential challenges in engaging youth in screening and research processes are
a common barrier to engaging service providers and community-based agencies in projects such as
this one. The project findings in St. John’s indicate that 100% of the youth who completed the
screener, also agreed to participate in the research component of the project. This is very
encouraging with respect to the feasibility of such initiatives and the potential of projects such as this
to learn more about youth needs.
Following completion of data collection the project team learned that GAIN SS administration was
continuing in at least one agency beyond the six month project data collection phase. This suggests
that in some situations this project has the potential to prompt sustained changes in practice.
Limitations
The findings of this project are limited by factors related to the screening tool as well as extent and
type of engagement of the participating service providers. The screening tool is a high level screening
tool intended to identify youth who would be likely to have a diagnosis with a full assessment and who
thus would benefit from assessment and service planning. As a result, it does not provide detailed
information about the areas of concern that are identified. Service providers and services engaged
with the project to differing extents which may have impacted the findings in unknown and/or ways
that may not be obvious.

St. John’s, Newfoundland
59
Recommendations
Gender-informed and gender-specific services should be considered to ensure that links to all
necessary services are available to both male and female youth given that, although they are
equally likely to present for services across agencies, it is important to ensure that the services that
are delivered are designed to address the different types of difficulties male and female youth
experience. For example, male youth were more likely to endorse substance use and crime and
violence related concerns than female youth, the latter in the oldest age category; female youth
were more likely than male youth to endorse internalizing and suicide concerns, especially in the
younger age categories and male youth were more likely than female youth to endorse co-occurring
mental health and problematic substance use. Further research is needed to address the needs of
youth who identify as trans or other youth who do not identify as solely male or female.
Developmentally informed and responsive services are indicated in order to meet the needs of
transitionally aged youth (19 to 24 years), especially those who are seeking and/or receiving
services in the adult service sector.
Continued capacity building regarding concurrent disorders across sectors is warranted given that
the majority of participants endorsed significant concerns in two or more domains. It is notable that
youth presenting to housing, outreach and support were more likely to screen positive for substance
use problems. This project aimed to improve early identification and pathways to care through
evidence-based practice in the form of screening using a standardized tool. Subsequent projects
should consider the importance of capacity building regarding interventions to address substance
use and concurrent disorders.
Building capacity for trauma-informed care across sectors is also suggested, given that half the
youth endorsed concerns related to traumatic distress.
The finding that one of the strongest predictors of screening positive for concurrent disorders was
previous legal involvement highlights the importance of early screening and follow-up for youth who
come in contact with the justice sector, particularly female youth. Consideration of strategies such
as screening youth who have early police contact for emerging substance use and/or mental health
difficulties may identify opportunities for earlier intervention, rather than waiting for serious legal
problems and/or for serious substance use and/or mental health problems to develop. This
reinforces the need for gender informed and specific approaches across sectors, including the
justice sector.
Given the high rate of endorsement of concurrent concerns across the participating sectors, to
increase opportunities for early identification, consideration should be given to gathering similar
information as was gathered through this project in other health care settings such as community
based primary care and hospital emergency rooms and/or in other highly accessible settings such
as educational settings.

St. John’s, Newfoundland
60
While this project examined youth needs at one point in time in service delivery, consideration
should be given to the potential utility of repeating administration of the screening tool at subsequent
points in the service delivery process for the purposes of monitoring within treatment progress and
post-treatment outcomes.
Further study is also recommended to examine the relative impacts of training, agency policy,
protocols, monitoring, supervision and administrative support on implementation of new practices,
such as the implementation of a consistent screening tool and process, as was examined in this
project.

St. John’s, Newfoundland
61
Appendices

St. John’s, Newfoundland
62

St. John’s, Newfoundland
63
Appendix A: St. John’s, Newfoundland Network Member Agency Descriptions
Choices For Youth – Choices is a non-profit, charitable, community-based agency that provides
housing and lifestyle development supports to youth in the St. John’s metro area. Choices for Youth’s
main focus is to provide young people with adequate, stable, and age-appropriate support systems
during a transition period in their lives. Part of what guides Choices for Youth’s programming is the
operating principles. Based on an empowerment philosophy, they strive to develop programming that
meets the needs of young people, promotes flexibility and innovative responses, and be designed and
evaluated in partnership with them. This includes: helping youth access financial support to stabilize
their immediate situation, mediate family issues and issues with landlords, counseling youth through
day-to-day issues and conflict resolution, providing youth with referrals for services such as drug
treatment or healthcare services, attending appointments with youth for treatment or healthcare
services and supporting their efforts to make healthier life choices, helping young people find stable,
safe housing, providing youth with basic necessities, providing emergency shelter to young men (and
referrals for shelter to young women), assisting young people obtain proper I.D. to access financial
support and healthcare services, create and encourage employment and educational opportunities
that work for youth. Another key aspect to helping youth is building a solid relationship of trust and
empowering them to make healthy life choices. At Choices, this involves employing a “Harm
Reduction” philosophy where youth are met and accepted regardless of what choices they are
currently making. Staff at Choices create a supportive, safe environment where youth can increasingly
become more involved and build trusting relationships, gradually making changes when they are
ready.
Community Youth Network (Thrive) – Thrive is an umbrella organization that works with the
community to address gaps in services, build community partnerships, increase awareness of existing
programs and services, and to conduct outreach to our most marginalized youth. The organization’s
vision statement is meeting youth where they are, helping youth go where they want to go, and
supporting youth to be who they want to be. The organization assists youth, primarily 12 -18 years,
who live in poverty and have limited access to mainstream programs and services. Thrive aims to
help youth to achieve their full potential and enhance the capacity of youth serving agencies.
Eastern Health:
Bridges Program – Is an outpatient mental health service for youth and their families who are
experiencing a serious, urgent mental illness/health problem or crisis. Bridges is a brief intervention/
outpatient mental health service. Bridges has an interdisciplinary team comprised of psychology,
social work, and occupational therapy. Assistance is available to young clients with problems such as
depression, suicidal and self-harm behaviors, eating disorders, sexuality concerns, mental illnesses

St. John’s, Newfoundland
64
and family conflict. Key service areas are: individual therapy, family therapy, psychiatric consultation
and treatment, parent education and supportive counseling, post hospital follow-up to inpatient mental
health treatment, and referral to other agencies.
Community Mental Health Counselors - Community Mental Health counselors are located
throughout the region. They provide therapeutic counseling to individuals of all ages in the areas of
mental health and addictions. Counseling is provided on an individual, couple, or family basis, with
groups offered as needed and opportunity arises. The Mental Health Counselors are also available for
consultations, presentations, and provision of information to any local community/professional group,
or school, upon request.
Complex Case Management-A service designed to ensure that individuals with complex mental
illness receive appropriate and integrated level of care, treatment and support. This program provides
individual group and family therapy; or service coordination coupled with individual and family support;
consultation with psychiatry and other relevant services and community agencies, with possible
referral as appropriate.
Janeway Family Center - Is an outpatient mental health service offering a coordinated and
comprehensive service for children and youth facing a wide range of mental health issues including
emotional, social or behavioral challenges. Janeway Family Centre is comprised of six teams, each
consisting of social workers, psychologists and staff using a combination of individual, family or group
interventions and varied therapeutic approaches according to their area of expertise.
Rowan Center - The Rowan Centre is a day treatment program for adolescents between the ages of
12 and 18 whose involvement with substance use and/or gambling is having a negative impact on
their lives. Youth will move into less intensive follow up services upon completion of the day treatment
program.
Youth Outreach -This program provides effective outreach to youth ages 12-17. Youth Outreach
Workers provide services and support to youth in the community in partnership with community based
organizations. Youth outreach involves rapport building in an attempt to connect youth to community
programs, services and supports. Youth outreach activities include mental health promotion,
addictions/prevention, education and program/project delivery, as well as supportive counseling,
screening, referral and advocacy in relation to mental health and addictions concerns.
Stella Burry Community Services:
Naomi Centre - Naomi Centre is an emergency shelter and short-term residence for young women
between the ages of 16 -30 who are in need of safe, supportive and temporary housing. Young
women who are residents at Naomi Centre receive support that encourages making informed choices
and decisions, potentially leading to greater stability in regards to personal relationships, finances,
emotional well being and housing so she can return to her family or community. A social worker is
available to provide counseling and assistance to the young woman and her family if necessary. Staff
assist residents with educational and employment needs, life skills instruction and housing.

St. John’s, Newfoundland
65
Appendix B: Key Project Activity Descriptions
Network Development
Member agencies that participated in the Network Development activity played a foundational role in
building a collaborative network, starting with preliminary discussions regarding project participation.
These agencies participated in several meetings with the project team, in addition to network specific
meetings and training. The agency leads and broader network membership also collaborated with the
project team to carry out the project.
Capacity Building
Service providers and agency leads from interested agencies participated in a half-day evidence-
based youth co-occurring disorders capacity building session and a half-day screening and
intervention protocol training session. During this session, where agencies had committed to full
project participation and had obtained research ethics approval, service providers also completed the
Service Provider Survey. Some agencies that participated in the Capacity Building activities were
interested in participating in the full project but were not able to due to resource or administrative
challenges, such as difficulties completing legal and/or ethics processes in the required network
timeframe.
Screening Implementation
Member agencies that participated in the full project implemented the GAIN SS with youth seeking
services at their agencies. Some agencies chose to implement the GAIN SS with the youth seeking
service for clinical purposes, but did not participate in the full data collection component of the project
(see below).
Data Collection
Member agencies that participated in the full project participated in a six month data collection period.
During this time, the GAIN SS and Background Information Form were administered to consenting
youth seeking service at their agencies and a copy was sent to the project team. The data was
prepared by the project team and a local community report was generated through a collaborative
process between the project team and the participating agencies.

St. John’s, Newfoundland
66
Appendix C: Agency Project Activity Participation
SECTOR Agency name
Project activity
Network Development
Capacity Building
GAIN SS Implementation
Data Collection
Addictions Eastern Health • Rowan Centre ● ● ● ●
Family services
Eastern Health • Family Services Counselors ● ●
Health services
Eastern Health • Central Intake ● ●
Housing, outreach &
support
Choices for Youth ● ● ● ● Community Youth Network ● ● ● ● Naomi Centre ● ● ● ● Eastern Health Youth Outreach Counselors ● ●
Justice Eastern Health • Services / Youth Corrections ● ●
Mental health
Eastern Health Complex Case Management ● ●
Eastern Health Bridges Program ● ● ● ● Eastern Health Janeway Family Centre ● ● ● ●
Eastern Health Central Intake ● ●
Eastern Health Community Mental Health Counselors ● ● ● ●

St. John’s, Newfoundland
67
Appendix D: Project Timeline
Year 1 Year 2 Year 3
2010 2011 2012 2013
Apr - Jun
July - Sept
Oct - Dec
Jan - Mar
Apr - Jun
July - Sept
Oct - Dec
Jan - Mar
Apr - Jun
July - Sept
Oct - Dec
Jan - Mar
Networking: Introduce project to
potential participating agencies
Establish cross-sectoral network:
REB Approval & Signing of MOU
Training for participating agencies
Project launch
Project actively underway
Preliminary findings presented
Report to stakeholders
Legend
St. John’s, Newfoundland Timeline
National Youth Screening Project Timeline
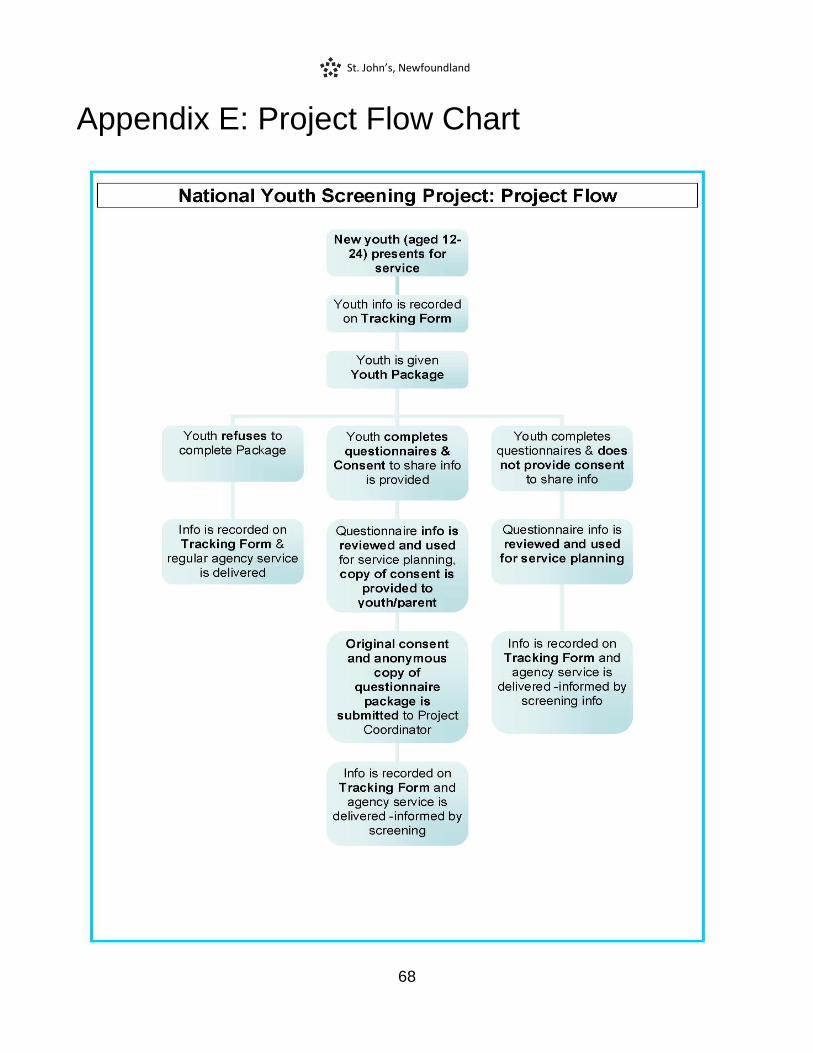
St. John’s, Newfoundland
68
Appendix E: Project Flow Chart

St. John’s, Newfoundland
69
Appendix F: References
Centre for Addiction and Mental Health. (2006). Navigating screening options for concurrent disorders.
Toronto, ON: Author.
Chaim, G. & Henderson, J. (2009). Innovations in collaboration: Findings from the GAIN Collaborating
Network Project. Toronto, ON: Centre for Addiction and Mental Health.
Dennis, M.L., Chan, Y.F., & Funk, R.R. (2006). Development and validation of the GAIN Short Screener
(GSS) for internalizing, externalizing and substance use disorders and crime/violence problems
among adolescents and adults. American Journal on Addictions, 15, 80-91.
Health Canada (2002). Best practices: Concurrent mental health and substance use disorders. Ottawa,
ON: Author.
Henderson, J., Chaim, G., & Rush, B. (2007). Knowledge, skills and tools: Addressing the mental health
and addiction needs of youth. Symposium presentation, Issues of Substance 2007 Conference,
Edmonton, AB.
Henderson, J., Chaim, G., & Goodman, I. (2009, August). Evaluating youth concurrent disorders across
youth-serving agencies in Toronto, Canada. Paper presentation, 117th Annual Convention of the
American Psychological Association, Toronto, ON.
Henderson, J., MacKay, S., & Peterson-Badali, M. (2010). Interdisciplinary knowledge translation: Lessons
learned from a mental health - fire service collaboration. American Journal of Community
Psychology, 46, 277-288.
Hillman, L., Chaim, G., & Henderson, J. (2011). Cross-sector collaboration in action: Findings from the
Concurrent Disorders Support Services Screening Project. Toronto, ON: Authors
McElheran, W., Eaton, P., Rupcich, C., Basinger, M., & Johnston, D. (2004). Shared mental health care:
The Calgary model. Families, Systems & Health. 22(4), 424–438.
Murphy, R. A., Rosenheck, R. A., Berkowitz, S. J., & Marans, S. R. (2005). Acute service delivery in a
police-mental health program for children exposed to violence and trauma. Psychiatric Quarterly,
76(2), 107-201.
National Treatment Strategy Working Group (2008). A systems approach to substance use in Canada:
Recommendations for a National Treatment Strategy. Ottawa, ON: National Framework for Actions
to Reduce the Harms Associated with Alcohol and Other Drugs and Substances in Canada.
Oliver, C., & Dykeman, M. (2003). Challenges to HIV service provision: The commonalities for nurses and
social workers. AIDS Care, 15(5), 649-663.

St. John’s, Newfoundland
70
Reid, G.J., Evans, B., Brown, J.B., Cunningham, C.E., Lent, B., Neufeld, R., Vingilis, E., Zaric, G., &
Shanley, D. (2006). Help – I need somebody: The experiences of families seeking treatment for
children with psychosocial problems and the impact of delayed or deferred treatment. Ottawa, ON:
Canadian Health Services Research Foundation.
Robillard, A.G., Gallito-Zaparaniuk, P., Arriola, K. J., Kennedy, S., Hammett, T., & Braithwaite, R. L.
(2003). Partners and processes in HIV services for inmates and ex-offenders. Facilitating
collaboration and service delivery. Evaluation Review, 27, 535-562.
Rush, B., Castel, S., & Desmond, R. (2009). Screening for concurrent substance use and mental health
problems in youth. Toronto, ON: Centre for Addiction and Mental Health.
Skilling, T., Henderson, J., Root, C., Chaim, G., Bassarath, L., & Ballon, B., (2007). Who are our clients?
Comparing the mental and addiction needs of adolescent clients across two CAMH programs.
Poster Presentation, Annual Convention of the Canadian Psychological Association, Ottawa, ON.

