staff development special c follow this guide to lead a
TRANSCRIPT
GENERAL PURPOSE: To provideprofessional nurses with an under-standing of the care of a patient whohas had a cerebral vascular accident.LEARNING OBJECTIVES: Afterreading the following article and tak-ing the test, you’ll be able to:1. Identify risk factors associated withcerebral vascular accidents.2. Discuss specific cerebral anatomyand physiology as it relates to cerebralvascular accidents. 3. Describe clinical manifestations ofcerebral vascular accidents. 4. Describe therapeutic interventionsfor patients who have had a cerebralvascular accident.
A. Classification and causes1. ischemic
a. thromboticb. embolic
2. hemorrhagicB. Circulation and neurofunction
1. carotid arteries2. vertebral arteries3. anatomy
a. cerebrumb. cerebellumc. brain stem
C. Clinical presentation1. location2. symptoms3. transient ischemic attacks
D. Diagnostics1. bedside neurological assessments
2. blood work3. electrocardiogram4. computerized axial tomography
scan5. magnetic resonance imaging6. electroencephalogram
E. Nursing’s response1. preservation of life2. prevention of additional brain
damage3. reduction of disability4. tissue plasminogen activator
a. indicationsb. contraindications
5. monitoringF. Financial considerations
1. length of stay2. insurance concerns
Cerebral vascular accident (CVA)—known also as “stroke” or “brainattack”—is a disruption of normal blood supply to the brain. Its suddenonset requires immediate treatment to prevent or lessen neurological deficitand lifelong disability.
www.nursingmanagement.com August 2004 Nursing Management 27
Staff Development
Teaching Guide
Follow this guide to lead a staff discussion on cerebral vascular accidents.
Countering“brain attacks”
Special

By Joan Harvey,
RN, MSN, CCRN
Abstract: Proactive nursing markedly
improves CVA patients’ outcomes. [Nurs
Manage 2004:35(8):27-33]
Every year, approximately700,000 Americans experi-ence a new or recurrentstroke.1 And every threeminutes, someone dies
from the event.2 Because the brain’smetabolic demands are high com-pared to other organs, permanentdamage can occur within minutes ifblood supply is interrupted.
The basics: classification, causesStrokes are classified according totype: ischemic and hemorrhagic.Ischemic is further delineated intothrombotic and embolic. Ischemic stokeis caused by an obstruction of cerebralblood flow, as in a vessel blockage.Ischemic stroke can also be caused byan embolus, then referred to as anembolic stroke.
Ischemic stroke causes include:♦ intracranial arteriosclerosis♦ carotid plaque with arteriogenicemboli♦ flow-reducing carotid stenosis♦ aortic arch plaque.
Cerebral vessel occlusion fromthrombosis in both large and smallarteries occurs most frequently in thepresence of atherosclerotic cerebralvascular disease. Vascular changes indeep penetrating arteries associatedwith chronic hypertension can resultin small vessel thrombosis.3
A stroke caused by a thrombus,referred to as a thrombotic stroke, isassociated with the development ofarteriosclerosis of the blood vesselwall. Plaque deposits build up on ves-sel walls and over time-—usuallyyears-—cause decreased blood flowand eventual blockage. Inflammatorydisease processes may also damagethe vessel wall and cause narrowing.With any type of narrowing, the ves-sel wall is subject to clot formationfrom platelet adhesion, aggregation,and fibrin attachments.
Embolic stroke results when anembolus travels to the brain and cutsoff blood supply. Major causes include:
♦ atrial fibrillation♦ cardiogenic emboli♦ valvular disease♦ left ventricular thrombi.
Cerebral emboli are often a compli-cation from cardiovascular disease.Cardiovascular disease, a risk factorin and of itself, further increases therisk of embolic formation when cou-pled with ventricular wall hypokine-sis or atrial arrhythmia. Emboli arereleased from the cardiovascular sys-tem and carried to the cerebral circu-lation, thus obstructing blood flowand causing stoke.
Hemorrhagic stroke results from avessel wall rupture and bleeding intothe brain or into the spaces aroundthe brain. Hemorrhagic stroke can bethe result of an aneurysm rupture,uncontrolled hypertension, a sub-arachnoid hemorrhage, infections,clotting disorders, head/neck trauma,radiation to the head/neck, and cere-bral angioplasty.
A closer look at circulation andneurofunctionBecause stroke manifestations dependon the affected vessel or area, clini-cians should clearly understand thecirculation of the brain. The carotidarteries supply 80% of cerebral bloodflow, with the vertebral arteries sup-plying the remaining 20%. The inter-nal carotid arteries supply the anteri-or and middle parts of the cerebralhemispheres. The vertebral arteriesjoin to form the basilar artery.
The vertebral-basilar arteries sup-ply the posterior parts of the cerebral
Countering“brain attacks”Cerebral vascular
accident (CVA)—known
also as “stroke” or
“brain attack”—is a
disruption of normal
blood supply to the
brain. Its sudden onset
requires immediate
treatment to prevent or
lessen neurological
deficit and lifelong
disability.
www.nursingmanagement.com August 2004 Nursing Management 29
1.5ANCC/AACN CONTACT HOURS
CE 0.5
PHARMACOLOGYCREDIT
��
hemispheres, the brainstem, and thecerebellum. Blood flows from theinternal carotid and vertebral-basilararteries into a ring of vessels joinedtogether known as the Circle of Willis,which sits at the base of the brain. Itconsists of the anterior communicat-ing artery and the paired anterior cere-bral, internal carotid, posterior com-municating, and posterior cerebralarteries. Each of the arteries suppliesblood flow to a different region of thebrain. Specifically, the anterior cerebralartery supplies the medial surface ofthe frontal and parietal lobes. Themiddle cerebral arteries supply the lat-eral surfaces of the cerebral hemi-spheres and smaller branch penetrat-ing arteries, bringing blood flow deep-er into the brain’s structure. The poste-rior cerebral arteries supply the medi-al and inferior surfaces of the occipitaland temporal lobes.
The brain’s vascular system automat-ically changes the diameter of its ves-sels to maintain a constant cerebralblood flow during blood pressure fluc-tuations—a process known as autoreg-ulation. The brain can effectivelyautoregulate when systolic blood pres-sure is 60 to 100 mm/Hg. But whenautoregulation fails, cerebral blood flowdiminishes, resulting in ischemia.4
To understand the clinical presenta-tion of stroke, you should have a basicunderstanding of neuroanatomy andfunction. The brain is divided intothree main components: the cerebrum,the cerebellum, and the brain stem.The cerebrum is the largest and mostadvanced part, responsible for severalfunctions, including higher intellect,speech, emotion, integration of senso-ry stimuli of all types, initiation of thefinal common pathways for move-ment, and fine control of movement.The cerebellum, the second largestarea, is responsible for maintainingbalance and assists in the control ofmovement and coordination. Thebrain stem is responsible for a varietyof automatic functions, such as controlof respiration, heart rate, and bloodpressure, and wakefulness, arousal,
and attention.The cerebrum is divided into a right
and a left hemisphere, each of whichhas a frontal, parietal, temporal, andoccipital lobe. The right side of thebrain controls the function of the leftside of the body and vice versa. Thisoccurs because the nerves cross in thebrain stem.
Clinical presentationClinical presentation of stroke variesaccording to the location of actual bloodsupply deficit. Symptoms are sudden inonset and can range from deep coma tolocal manifestations on one side of thebody. If the right cerebral hemisphere isaffected, subsequent weakness on theleft side of the body will occur, includ-ing left arm or leg weakness, numb-ness, or even neglect. The patient’s facewill be asymmetrical on the left, he orshe may have a loss of visual left fieldof both eyes, and a gaze that’s promi-nent to the right.
A left cerebral hemisphere stroke
results in weakness, numbness, orneglect on the body’s right side. If thespeech-controlling Broca’s area is af-fected, the patient will have aphasia(expressive, receptive, or mixed). His orher face will be asymmetrical on theright, and a loss of vision to the rightvisual field in both eyes may occur,with a preference to gaze to the left.
If the patient’s brainstem and cere-bellum are affected, he or she mayexperience hemi/quadriparesis,hemisensory loss and ataxia, abnormaleye movements, oralphayrngealweakness, nausea, vomiting, hiccups,vertigo, tinnitus, abnormal respira-tions, and decreased level of con-sciousness. An affected thalamic arearesults in sensory alterations (touch,pain, vibration, and temperature).
While taking a patient’s medical his-tory, you may find that he or she hasencountered a temporary disruption ofblood flow to the brain, which results ina brief loss of function that resolveswithin 24 hours. This is known as a
www.nursingmanagement.com30 Nursing Management August 2004
Brain attacksContraindications and additional t-PA considerations
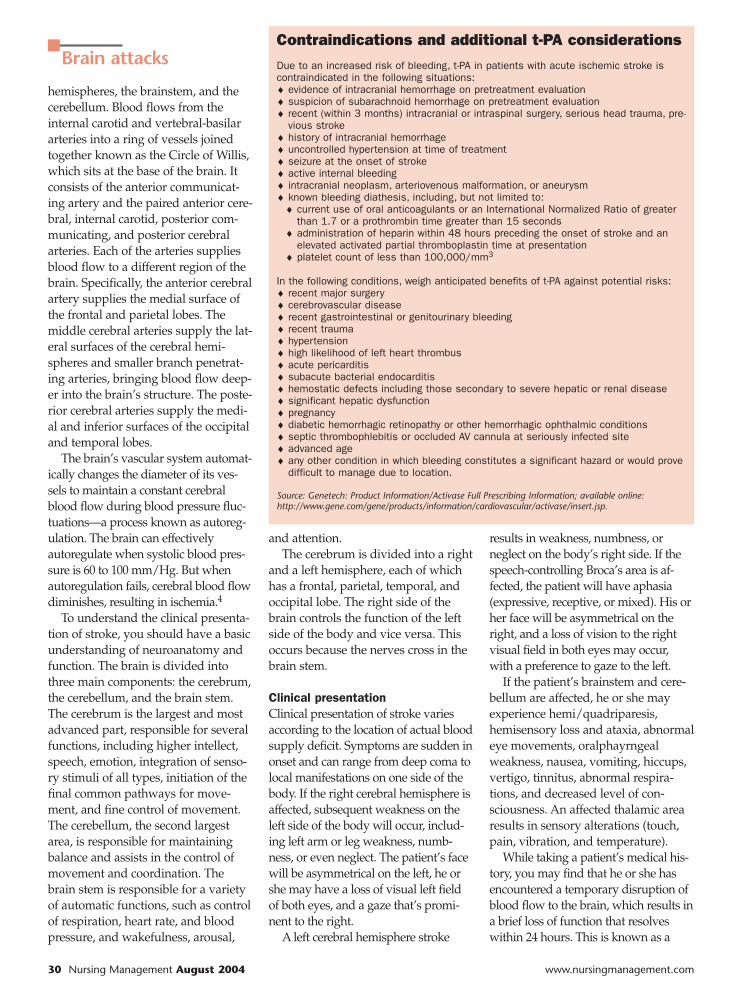
Due to an increased risk of bleeding, t-PA in patients with acute ischemic stroke iscontraindicated in the following situations:♦ evidence of intracranial hemorrhage on pretreatment evaluation♦ suspicion of subarachnoid hemorrhage on pretreatment evaluation♦ recent (within 3 months) intracranial or intraspinal surgery, serious head trauma, pre-
vious stroke♦ history of intracranial hemorrhage♦ uncontrolled hypertension at time of treatment♦ seizure at the onset of stroke♦ active internal bleeding♦ intracranial neoplasm, arteriovenous malformation, or aneurysm♦ known bleeding diathesis, including, but not limited to:
♦ current use of oral anticoagulants or an International Normalized Ratio of greaterthan 1.7 or a prothrombin time greater than 15 seconds
♦ administration of heparin within 48 hours preceding the onset of stroke and anelevated activated partial thromboplastin time at presentation
♦ platelet count of less than 100,000/mm3
In the following conditions, weigh anticipated benefits of t-PA against potential risks:♦ recent major surgery♦ cerebrovascular disease♦ recent gastrointestinal or genitourinary bleeding♦ recent trauma♦ hypertension♦ high likelihood of left heart thrombus♦ acute pericarditis♦ subacute bacterial endocarditis♦ hemostatic defects including those secondary to severe hepatic or renal disease♦ significant hepatic dysfunction♦ pregnancy♦ diabetic hemorrhagic retinopathy or other hemorrhagic ophthalmic conditions♦ septic thrombophlebitis or occluded AV cannula at seriously infected site♦ advanced age♦ any other condition in which bleeding constitutes a significant hazard or would prove
difficult to manage due to location.
Source: Genetech: Product Information/Activase Full Prescribing Information; available online:http://www.gene.com/gene/products/information/cardiovascular/activase/insert.jsp.

transient ischemic attack (TIA). Patientswho have a TIA must be evaluatedpromptly for stroke risk. According tothe National Institute of NeurologicalDisorders and Stroke, approximatelyone-third of Americans who experienceTIAs will have a stroke.5
DiagnosticsTo effectively treat stroke, you mustact quickly, as time is essential to braintissue and function preservation.Upon patient arrival to the emergencydepartment, the health care team willask him or her a series of questions,the most important of which is whensymptoms first occurred and whatthey are, specifically. It’s crucial toknow when the symptoms began, asthis will help tailor patient treatment.A series of bedside neurologicalassessments and a specific examdeveloped to determine the severity ofstroke will ensue. (To view theNational Institutes of Health StrokeScale, visit http://www.strokecenter.org/trials/scales/nihss.pdf.)
Also, the clinician will order com-mon blood tests such as a CBC,platelet count, PT, PTT, a metabolicpanel, and a urinalysis. Carefullyreview blood glucose results, as bloodsugar disturbances often mimic stroke.Additionally, an electrocardiogram isdone to rule out arrhythmia.
The single most effective tool todiagnose a stroke is a computerizedaxial tomography (CT) scan. To devisean effective treatment plan, a radiolo-gist will determine if the stroke isischemic or hemorrhagic. In additionto a CT scan, the clinician may orderan MRI to help determine the exactlocation and size of injury. MRIs,which can find evidence of a strokewithin minutes of its occurrence,prove especially beneficial for assess-ing smaller strokes located deep inbrain tissue.
The clinician may also order anelectroencephalogram, which revealsthe brain’s electrical activity and helpsscreen for any seizure activity result-ing from brain injury. In addition,
carotid Doppler studies help evaluatethe patency of the carotid arteries.
Nursing’s responseThe focus of therapeutic managementfor the stroke patient is the preserva-tion of life, prevention of additionalbrain damage, and reduction of dis-ability. Care of the acute stroke patientproves challenging, as brain cells diewithin minutes. The longer thepatient’s brain is deprived of oxygenand blood, the more likely that he orshe will suffer permanent damage.
Lifestyle changes may helpdecrease stroke risk factors. Encouragepatients to lead a healthy lifestyle—one that includes a balanced diet; aer-obic exercise for at least 30 minutesmost days of the week; monitor andcontrol blood pressure, blood glucose,and lipid levels; and smoking cessa-tion, if appropriate.
Although nothing will stop a strokefrom occurring, one drug— tissueplasminogen activator (t-PA)—canminimize the size of the infarcted areaby opening blocked vessels that areoccluded with clot. The drug worksby converting plasminogen to plas-min, which in turn dissolves the clot.Patients eligible to receive t-PA,according to National Institutes ofHealth criteria, include those whosesymptom onset is less than 3 hours,those older than 18 years of age, andthose whose CT scan shows no evi-dence of intracerebral bleeding.
Although expectations of positiveoutcomes are reduced and sympto-matic intracranial hemorrhage ratesare higher in severe stroke population,treatment with t-PA improves out-comes, but overall success ratesremain low.6 T-PA isn’t recommendedfor patients with isolated mild neurodeficits, such as ataxia alone, sensoryloss alone, dysarthria alone, or traceweakness.7 (See “Contraindicationsand other t-PA considerations.”)
If t-PA is used, the recommendedadministered dose is 0.9mg/kg; maxi-mum dose is 90 mg given over 60minutes, with 10% of the total dose
given as a bolus over one minute.Nurses should acquire all baseline lab-oratory data and ensure several work-ing intravenous lines.
Nurses also remain responsible forfrequent vital sign monitoring, moni-toring of neurological status, monitor-ing for bleeding complications, andlimiting invasive procedures for atleast 24 hours. In addition, no antico-agulants or antiplatelets may be usedfor 24 hours post t-PA. A CT scan isusually done within 24 hours. A fol-low-up CT rules out any type ofbleeding post t-PA.
If t-PA isn’t used, the focus of treat-ment lies with the symptoms thepatient exhibits and the potential causeof the stroke event. If the patient has acardiac history and clinicians discoveratrial fibrillation, he or she shouldreceive anticoagulants, once a hemor-rhagic stroke is ruled out by CT scan.
If the patient is hypertensive andthe stroke is caused by hemorrhage,surgical intervention may be requiredto evacuate the bleed. The patient mayreceive an antiseizure medication as aprophylactic measure. If the patient ishypertensive, blood pressure is low-ered slowly with medications toensure adequate cerebral perfusion. Ifthe patient has hyperlipidemia, anti-cholesterol medications like statinswill be instituted, once liver functionis determined to be normal. To treatcerebral vasospasm, the calcium chan-nel blocker nimodipine (Nimotop)may be given, which relaxes smoothmuscles of the vessel wall and reducesthe incidence and severity of thespasm, thus improving cerebral bloodflow and neurologic function.
Proactive nursing will help strokepatients avoid or successfully recoverfrom complications such as pneumo-nia, aspiration, deep vein thrombosis,pulmonary embolism, pressure ulcers,malnutrition, and contractures. Targeteducation to the patient, significantothers, and additional caregivers.
Keep the patient’s airway patentand encourage deep breathing andcoughing exercises, incentive spirome-
www.nursingmanagement.com August 2004 Nursing Management 31
try, early mobility, and frequent posi-tion changes to help prevent atelecta-sis. Always monitor vital signs andobserve closely for symptoms ofdeveloping pneumonia, which includefever, chills, elevated white blood cellcount, and changes in breath sounds.Alert the clinician to any of thesechanges and anticipate orders forblood cultures, sputum culture, chestx-ray, and antibiotic therapy.
Evaluate swallowing early in thepatient’s admission to avoid aspira-tion. If the patient has trouble swal-lowing, keep him or her NPO untilyou receive a speech therapy evalua-tion, which should occur within 24hours. Alert involved patient care staffand family members of the risk ofaspiration. Conduct nutritional con-sultations to ensure that the patientmeets his or her caloric needs eitherorally or via an alternate route.
Evaluate deep-vein-thrombosis riskand take measures to prevent itsoccurrence, including the use ofsequential compression devices, anti-embolic hose, or low-molecular-weight heparin, when appropriate.Movement of extremities will helpprevent blood stasis and pressureulcers.
Other considerationsStroke patients’ lengths of stay greatlyimpact hospital finances. Quite frankly,stroke is expensive. The estimateddirect and indirect cost of stroke in 2004is $53.6 billion.8 Nurses and case man-agers who follow patients closely andconsult with clinicians daily can helpdecrease costs. To that end, considerusing care maps as a guide to best prac-tice regarding diagnostic tests, speechevaluations, physical therapy, occupa-tional therapy, and dietary instructions.These maps will encourage staff mem-bers to ask the right questions andprompt clinicians to order appropriatetreatment.
Thrombolytic therapy proves costlyto hospitals, but decreases globalhealth care costs, in general. For 1,000patients receiving t-PA, hospitalizationcosts total $1.7 million more than non-t-PA patients, rehabilitation costs $1.4million less, and nursing home costs$4.8 million less—resulting in 564quality-adjusted life-years saved.9
Insurance companies also play apivotal role in the care of strokepatients. Despite the presence of clini-cal symptoms, some companies man-date certain studies to make a diagno-sis. Delays in obtaining these studies
will increase patient length of stay.Hospital administrators need to exam-ine current reimbursement schedulesand review delayed costs, weighingpatient need and financial impact.
References1. The American Stroke Association: Stroke
Facts 2004: All Americans; availableonline: http://www.strokeassociation.org.
2. Ibid.3. Braddom, R.: Physical Medicine and
Rehab, 2nd ed., p.1117. WB Saunders:Philadelphia, 2000.
4. Smeltzer, S., and Brenda, G.: BareBrunner and Suddarth’s Textbook ofMedical Surgical Nursing, 9th ed.Lippincott: Philadelphia, 2000.
5. National Institute of NeurologicalDisorders and Stroke; available online:http://www.ninds.nih.gov.
6. UMDJ and Millennium: Acute StrokeExpress Report—Providing the Latest inEvidenced Based Medicine—A CMECertified Monograph. Critical decisionsin the emergency management of acutestroke. Release date March 30, 2004.
7. Fowler, S.: Acute Stroke, unpublishedhandouts, American Association ofNeuroscience Nurses. May 20, 2004.
8. The American Stroke Association: loc cit.9. Fagan, S., et al.: “Cost-effectiveness of
tissue plasminogen activator for acuteischemic stroke,” Neurology. 50(4):883-890, 1998.
About the authorJoan Harvey is a clinical educator at OceanMedical Center, Brick, N.J.
www.nursingmanagement.com32 Nursing Management August 2004
Brain attacks
CE TestCountering “brain attacks”
Instructions:• Read the article beginning on page 27.• Take the test, recording your answers in the test answers section(Section B) of the CE enrollment form. Each question has only onecorrect answer.• Complete registration information (Section A) and courseevaluation (Section C).• Mail completed test with registration fee to: Lippincott Williams &Wilkins, CE Group, 333 7th Ave., 19th Floor, New York, N.Y. 10001.• Within 3 to 4 weeks after your CE enrollment form is received,you will be notified of your test results.• If you pass, you will receive a certificate of earned contact hoursand an answer key. If you fail, you have the option of taking the testagain at no additional cost.• A passing score for this test is 11 correct answers.• Need CE STAT? Visit http://www.nursingcenter.com for imme-diate results, other CE activities, and your personalized CE plannertool. • No Internet access? Call 1-800-933-6525 for other rush serviceoptions.• Questions? Contact Lippincott Williams & Wilkins: 646-674-6617or 646-674-6621.
Registration Deadline: August 31, 2006
Provider Accreditation:This Continuing Nursing Education (CNE) activity for 1.5 contact hours is pro-vided by Lippincott Williams & Wilkins, which is accredited as a provider ofcontinuing education in nursing by the American Nurses Credentialing Center’sCommission on Accreditation and by the American Association of Critical-CareNurses (AACN 00012278, CERP Category A). This activity is also providerapproved by the California Board of Registered Nursing, Provider Number CEP11749 for 1.5 contact hours. LWW is also an approved provider of CNE inAlabama, Florida, and Iowa and holds the following provider numbers: AL#ABNP0114, FL #FBN2454, IA #75. All of its home study activities areclassified for Texas nursing continuing education requirements as Type I.This activity has been assigned 0.5 pharmacology credit.
Your certificate is valid in all states. This means that your certificate of earnedcontact hours is valid no matter where you live.
Payment and Discounts:• The registration fee for this test is $12.95.• If you take two or more tests in any nursing journal published by LWW andsend in your CE enrollment forms together, you may deduct $0.75 from theprice of each test.• We offer special discounts for as few as six tests and institutional bulk dis-counts for multiple tests. Call 1-800-933-6525 for more information.

1.5 ANCC/AACN CONTACT HOURSC E
ENROLLMENT FORM: Nursing Management, August 2004, Countering “brain attacks”
A. Registration Information:
Last name ____________________________ First name ________________________ MI _____
Address _______________________________________________________________________________
City _______________________________________ State _________________ ZIP ______________
Telephone ____________________ Fax ____________________ E-mail ____________________
Registration Deadline: August 31, 2006Contact hours: 1.5 Pharmacology hours: 0.5 Fee: $12.95
❑ LPN ❑ RN ❑ CNS ❑ NP ❑ CRNA ❑ CNM ❑ other ___________________
Job title __________________________________ Specialty _________________________________
Type of facility ____________________________________ Are you certified? ❑ Yes ❑ No
Certified by ___________________________________________________________________________
State of license (1) __________________________ License # ___________________________
State of license (2) __________________________ License # ___________________________
Social Security # _____________________________________________________________________❑ From time to time, we make our mailing list available to outside organizations to announce special
offers. Please check here if you do not wish us to release your name and address.
B. Test Answers: Darken one circle for your answer to each question.
a b c d1. ❍ ❍ ❍ ❍2. ❍ ❍ ❍ ❍3. ❍ ❍ ❍ ❍
a b c d4. ❍ ❍ ❍ ❍5. ❍ ❍ ❍ ❍6. ❍ ❍ ❍ ❍
a b c d7. ❍ ❍ ❍ ❍8. ❍ ❍ ❍ ❍9. ❍ ❍ ❍ ❍
a b c d10. ❍ ❍ ❍ ❍11. ❍ ❍ ❍ ❍12. ❍ ❍ ❍ ❍
a b c d13. ❍ ❍ ❍ ❍14. ❍ ❍ ❍ ❍15. ❍ ❍ ❍ ❍
1. Thrombotic strokes may develop as aresult ofa. chronic hypertension.b. long-term use of aspirin.c. head trauma.d. acute renal failure.
2. Patients at risk for embolic strokesinclude those who havea. deep vein thrombosis.b. uncontrolled hypertension.c. diabetes mellitus.d. atrial fibrillation.
3. A hemorrhagic stroke may develop as aresult of a. a cerebral angioplasty.b. diabetes mellitus.c. elevated cholesterol.d. cardiac dysrhythmias.
4. The carotid arteries provide what per-centage of the blood supply to the brain?a. 40%b. 60%c. 80%d. 100%
5. The middle cerebral arteries provideblood flow to which area of the brain?a. medial surface of the parietal lobesb. lateral surface of the cerebral hemi-spheresc. inferior surface of the occipital lobesd. posterior surface of the temporal lobe
6. Which statement is true about theblood supply in the brain?a. The internal carotid artery providesblood to the posterior regions of the brain.
b. The purpose of autoregulation is tomaintain adequate oxygenation to thebrain.c. The vertebral-basilar arteries supply 60%of the blood that reaches the Circle ofWillis.d. Ischemia may develop if the systolicblood pressure is less than 70 mm Hg.
7. One function of the cerebrum is to a. integrate sensory input.b. maintain balance.c. control wakefulness.d. regulate blood pressure.
8. A patient who has had a right cerebralvascular accident may havea. a gaze that’s prominent to the left.b. expressive aphasia.c. a loss of the visual field in both eyes.d. neglect.
9. A patient who has had a left cerebralvascular accident may havea. a loss of the left visual field.b. asymmetry of the facial muscles on theleft side.c. mixed aphasia.d. a gaze that’s prominent to the right.
10. Cerebral vascular accidents in thethalamic area producea. nausea.b. abnormal eye movements.c. tinnitus.d. sensory alterations.
11. Transient ischemic attacksa. usually last 48 hours.b. may result in residual disabilities.
c. lead to the development of strokes 50%of the time.d. are a temporary disruption in cerebralblood flow.
12. Which of the following diagnostictests is used to determine the exactlocation of a brain injury?a. CT scanb. MRIc. carotid Dopplerd. EEG
13. Which statement is true regarding thenursing care of patients who receive t-PA?a. Additional invasive procedures may beperformed 2 hours after administration.b. Vital signs should be taken q shift.c. Frequent neurological assessmentsmust be carried out.d. The entire dose should be administeredas a bolus.
14. T-PA is indicated fora. mild neurologic deficits.b. sensory loss alone.c. trace weakness.d. thrombotic stroke.
15. When is it appropriate to useanticoagulants in a patient who has hada stroke?a. as an adjuvant therapy to t-PAb. if the stroke is due to a subduralhematomac. if the patient has had an ischemicstroke and has atrial fibrillationd. if a history of hypertension is noted
Countering “brain attacks”GENERAL PURPOSE: To provide professional nurses with an understanding of the care of a patient who has had a cerebral vascular accident.LEARNING OBJECTIVES: After reading the preceding article and taking the following test, you’ll be able to: 1. Identify risk factors associatedwith cerebral vascular accidents. 2. Discuss specific cerebral anatomy and physiology as it relates to cerebral vascular accidents.3. Describe clinical manifestations of cerebral vascular accidents. 4. Describe therapeutic interventions for patients who have had acerebral vascular accident.
0804
C. Course Evaluation*1. Did this CE activity's learning objectives relate to its general purpose? ❑ Yes ❑ No2. Was the journal home study format an effective way to present the material? ❑ Yes ❑ No3. Was the content relevant to your nursing practice? ❑ Yes ❑ No4. How long did it take you to complete this CE activity?___ hours___minutes5. Suggestion for future topics __________________________________________________________
D. Two Easy Ways to Pay:❑ Check or money order enclosed (Payable to Lippincott Williams & Wilkins)❑ Charge my ❑ Mastercard ❑ Visa ❑ American Express
Card # _____________________________________________ Exp. date __________________
Signature _______________________________________________________________________
*In accordance with the Iowa Board of Nursing administrative rules governing grievances, a copy of your evaluation of the CE offering may be submitted directly to the Iowa Board of Nursing.
✄
0.5PHARMACOLOGY CREDIT
��