standards for newborn blood spot screening for newborn blood spot screening – august 2013 3...
TRANSCRIPT

Newborn Blood Spot
Standards for newborn blood spot screening
Version 1.0 / August 2013

Standards for newborn blood spot screening – August 2013
2
About the NHS Newborn Blood Spot
Screening Programme
The NHS Newborn Blood Spot Screening Programme has responsibility for developing,
implementing and maintaining a high quality, uniform screening programme for all newborn
babies and their parents. The UK National Screening Committee (UK NSC) recommends that
all babies in the UK are offered screening for phenylketonuria (PKU), congenital hypothyroidism
(CHT), sickle cell disease (SCD), cystic fibrosis (CF) and medium-chain acyl-CoA
dehydrogenase deficiency (MCADD). There is a service specification for the NHS Newborn
Blood Spot Screening Programme (No.19) available as part of the public health functions
exercised by NHS England (www.gov.uk/government/publications/public-health-
commissioning-in-the-nhs-from-2013).
The UK NSC and NHS Screening Programmes are operated by Public Health England.
PHE’s mission is to protect and improve the nation’s health and to address inequalities
through working with national and local government, the NHS, industry and the
voluntary and community sector. PHE is an operationally autonomous executive agency
of the Department of Health.
NHS Newborn Blood Spot Screening Programme newbornbloodspot.screening.nhs.uk
© Crown copyright 2013
You may re-use this information (excluding logos) free of charge in any format or
medium, under the terms of the Open Government Licence v2.0. To view this licence,
visit OGL or email [email protected]. Where we have identified any third
party copyright information you will need to obtain permission from the copyright holders
concerned. Any enquiries regarding this publication should be sent to
Published August 2013
PHE publications gateway number: 2013139
Uncontrolled when printed. To ensure you have the latest version of this
document, please view it online.

Standards for newborn blood spot screening – August 2013
3
Contents
About the NHS Newborn Blood Spot Screening Programme 2
Introduction 4
Summary of main changes 7
Standard 1a: Completeness of coverage (CCG responsibility at birth) 9
Standard 1b: Completeness of coverage (movers in) 11
Standard 2: Timely identification of babies with a null or incomplete result
recorded on the child health information system 13
Standard 3: Baby’s NHS number (or UK equivalent) is included on the
blood spot card 14
Standard 4: Timely sample collection 15
Standard 5: Timely receipt of a sample in the newborn screening laboratory 16
Standard 6: Quality of the blood spot sample 17
Standard 7: Timely taking of a repeat blood spot sample 19
Standard 8: CPA (screening) 20
Standard 9: Timely processing of all PKU, CHT and MCADD screen
positive samples 21
Standard 10: CPA (diagnosis) 22
Standard 11: Timely receipt into clinical care 23
Standard 12: Timeliness of results to parents 25
Abbreviations 26
Appendix 1: Glossary 27
Appendix 2: Newborn blood spot screening status codes 30

Standards for newborn blood spot screening – August 2013
4
Introduction
The UK National Screening Committee (UK NSC) recommends that all babies in the UK are
offered screening for phenylketonuria (PKU), congenital hypothyroidism (CHT), sickle cell
disease (SCD), cystic fibrosis (CF) and medium-chain acyl-CoA dehydrogenase deficiency
(MCADD). All newborn babies up to one year of age are offered screening in order that a small
number with the potential to develop disease might be diagnosed and treated and their parents
receive support and education. It is a complex programme delivered by a range of different
organisations working together.
This document presents the revised national standards for the NHS Newborn Blood Spot
Screening Programme. It should be read in conjunction with the standards for the NHS Sickle
Cell and Thalassaemia Screening Programme (www.sct.screening.nhs.uk/standards) and the
UK NSC generic standards (under development). These revised standards replace standards
1–9 in Standards and Guidelines for Newborn Blood Spot Screening (August 2008) and unless
stated in the document have an implementation date of April 2014. A summary of the main
changes is available on page 7.
Generic standards framework
The updated standards have been reviewed in keeping with the proposed generic standards
framework that has been developed for the eight English non-cancer NHS Screening
Programmes by representatives from the programmes, UK NSC Quality Assurance, regional
screening leads and antenatal and child health screening teams. The generic standards
framework is based on 10 themes:
Identify Population
Inform
Coverage/Uptake
Test
Diagnose
Intervention/Treatment
Outcome

Standards for newborn blood spot screening – August 2013
5
Minimising Harm
Staff: Education and Training
Commissioning/Governance
The aim is, where it is appropriate, to have one generic acceptable/achievable measurement
across the programmes. The themes in italics have specific newborn blood spot screening
standards. For all other themes the generic standards apply.
Format
Where appropriate, the revised standards are measured at two levels: achievable and
acceptable. As defined by the UK NSC:
The achievable threshold represents the level at which the programme is likely to be running
effectively; screening programmes should budget for and aspire towards performance at this
level. Local constraints may sometimes result in programmes failing to meet this threshold.
Service improvement plans should focus on the delivery of a balanced service with as many
standards as possible meeting the achievable threshold.
The acceptable threshold is the lowest level of performance considered safe. All programmes
are expected to exceed the acceptable threshold and to agree service improvement plans that
develop performance towards an achievable level. Programmes not meeting the acceptable
threshold are expected to implement recovery plans to ensure rapid and sustained
improvement.
The standards are accompanied by a number of best practice guidelines that should be
followed to deliver high quality screening processes and to meet the standards.
Data collection and analysis
Please note that data may need to be aggregated by a variety of denominator cohorts, eg local
authority (or UK equivalent), maternity service, clinical commissioning group (CCG) and
newborn screening/specialist laboratory. The cohort of responsibility for child health records
departments remains the same: primary care trusts (PCTs) have been mapped to CCGs.
PHE is responsible for ensuring that reports on important aspects of screening are available at
various geographies (eg local authority) to enable population-based oversight.
Please see the data dictionary for exact data requirements – this is updated each year.

Standards for newborn blood spot screening – August 2013
6
Consultation
These revised standards were disseminated widely for consultation in early 2013. Following
consultation further revisions were made and the standards were presented to and approved by
the Blood Spot Advisory Group in May 2013.
Please note that an abbreviation list and glossary are provided at the end of the document. A
broken underline indicates that a term is used according to its definition in this glossary. Where
terms from the glossary are used without a broken underline, their common English meaning
can be assumed. Except where the context determines otherwise, definitions include all forms
of the defined term; so “tested” and “testing” refer to the definition of “test”. The newborn blood
spot screening status codes are reproduced in Appendix 2.

Standards for newborn blood spot screening – August 2013
7
Summary of main changes
Standard Changes Data collected by
Standard 1a: Completeness of coverage (CCG responsibility at birth)
Standard agreed in August 2011
Child health records departments
Standard 1b: Completeness of coverage (movers in)
New standard – this standard will be piloted using PKU as proxy to ensure that it is realistic
Child health records departments (to be piloted)
Standard 2: Timely identification of babies with a null or incomplete result recorded on the child health information system
Standard agreed in August 2011
Child health records departments
Standard 3: Baby’s NHS number (or UK equivalent) is included on the blood spot card
No change Newborn screening laboratories
Standard 4: Timely sample collection
Change to thresholds Newborn screening laboratories
Standard 5: Timely receipt of sample in the newborn screening laboratory
Change to thresholds Newborn screening laboratories
Standard 6: Quality of the blood spot sample
Change to avoidable repeat definition to account for pre-transfusion sample protocol
Newborn screening laboratories
Standard 7: Timely taking of a repeat blood spot sample
Changes to thresholds and definitions to account for changes in screening protocols. Please note that data collection against this standard will be deferred until implementation of the Newborn Blood Spot Failsafe Solution
Maternity services (deferred until implementation of the Newborn Blood Spot Failsafe Solution)
Standard 8: CPA standard (screening)
New standard Newborn screening laboratories
Standard 9: Timely processing of all PKU, CHT and MCADD screen positive samples
No change Newborn screening laboratories

Standards for newborn blood spot screening – August 2013
8
Standard 10: CPA standard (diagnosis)
New standard Newborn screening laboratories
Standard 11: Timely receipt into clinical care
New standard
Newborn screening laboratories and paediatric specialist centres
Standard 12: Timeliness of results to parents
New standard Child health records departments

Standards for newborn blood spot screening – August 2013
9
Standard 1a: Completeness of coverage
(CCG responsibility at birth)
Objective To maximise uptake in the eligible population who are fully informed and wish to participate in the screening programme.
Measure Tested babies expressed as a percentage Eligible babies
Thresholds
Acceptable Equal to or more than 95% of eligible babies are tested for all conditions.
Achievable Equal to or more than 99.9% of eligible babies are tested for PKU, MCADD and SCD.
Equal to or more than 98% of eligible babies are tested for CHT and CF.
Definitions
Tested babies (numerator) are the total number of eligible babies for whom a conclusive screening result for each of the five conditions was available within an effective timeframe.
Eligible babies (denominator) are the total number of babies born within the reporting period, excluding any baby who died before the age of eight days. For the purpose of this standard, the cohort includes babies for whom the CCG was responsible at birth and is still responsible on the last day of the reporting period.
The effective timeframe is that a conclusive result for each of the five conditions is recorded on the child health information system by 17 days of age.
A conclusive result is one of the following newborn screening status codes:
04 not suspected
05 carrier
06 sickle not suspected, carrier of other haemoglobin
07 not suspected, other disorders follow up
08 suspected
10 S not suspected (by DNA) No other Hb/thal excluded
Status code 02 declines are not included in the count for a conclusive result – data is collected and reported alongside coverage data to help interpretation.
Standards for newborn blood spot screening – August 2013
10
Reporting
Reported quarterly for key performance indicator (KPI) NB1 – using PKU as proxy: Deadlines: 30 September (Q1), 31 December (Q2), 31 March (Q3), 30 June (Q4)
Reported annually for babies born in the previous financial year: Deadline: 30 June
Data collected by: child health records departments
Monitoring performance of: maternity services, newborn screening laboratories and child health records departments
Aggregated by: CCG

Standards for newborn blood spot screening – August 2013
11
Standard 1b: Completeness of coverage
(movers in)
Objective To maximise uptake in the eligible population who are fully informed and wish to participate in the screening programme.
Measure Tested babies expressed as a percentage Eligible babies
Thresholds
Acceptable Equal to or more than 95% of eligible babies are tested for PKU.
Achievable Equal to or more than 99.9% of eligible babies are tested for PKU.
Please note that this new standard will be piloted using PKU as proxy to ensure that it is realistic.
Definitions
Tested babies (numerator) are the total number of eligible babies for whom a conclusive screening result for PKU is available within an effective timeframe.
Eligible babies (denominator) are the total number of babies born within the reporting period and equal to or less than 364 days old. For the purposes of this standard, the cohort includes only babies who have moved in and become the responsibility of the CCG during the reporting period and for whom the CCG remains responsible on the last day of the reporting period.
The effective timeframe is that a conclusive result for PKU is recorded on the child health information system equal to or less than 21 calendar days of movement in being recorded on the child health information system.
A conclusive result is one of the following newborn screening status codes:
04 not suspected
07 not suspected, other disorders follow up
08 suspected
Status code 02 declines are not included in the count for a conclusive result – data are collected and reported alongside coverage data to help interpretation.
Reporting
Reported quarterly for key performance indicator (KPI) NB4 – using PKU as proxy: Deadlines: 30 September (Q1), 31 December (Q2), 31 March (Q3), 30

Standards for newborn blood spot screening – August 2013
12
June (Q4) (implementation date Q1 2014)
Reported annually for babies born in the previous financial year (data to be collated between two and three months after financial year-end): Deadline: 30 June
Data collected by: child health records departments
Monitoring performance of: maternity and health visiting services, newborn screening laboratories and child health records departments
Aggregated by: CCG

Standards for newborn blood spot screening – August 2013
13
Standard 2: Timely identification of babies
with a null or incomplete result recorded on
the child health information system
Objective
To maximise uptake in the eligible population who are fully informed and wish to participate in the screening programme.
The newborn screening programme relies on regular checks of the child health information system to ensure early identification of babies with a null or incomplete result, within an effective timeframe. Failsafe reports are produced and action taken to follow-up, according to local protocols.
Measure Is the child health information system capable of identifying babies with null or incomplete blood spot results within the standard?
Thresholds
Acceptable 100% of child health records departments perform regular checks (ideally daily, minimum weekly) to identify babies with null values or status codes 01 specimen received in laboratory or 03 repeat/further sample required, for any of the five conditions, for all babies equal to or more than 17 days and equal to or less than 364 days.
Achievable 100% of child health records departments perform regular checks (ideally daily, minimum weekly) to identify babies with null values or status codes 01 specimen received in laboratory or 03 repeat/further sample required, for any of the five conditions, for all babies equal to or more than 14 days and equal to or less than 364 days.
Definitions
There can be flexibility in frequency and age range of reports providing the method complies with the acceptable performance threshold – eg daily check of babies equal to or more than 17 days and equal to or less than 364 days; weekly with an age range equal to or more than 11 days and equal to or less than 364 days.
Reporting Child health records departments are asked to report annually whether they have a system in place that meets the standard: Deadline: 30 June
Standards for newborn blood spot screening – August 2013
14
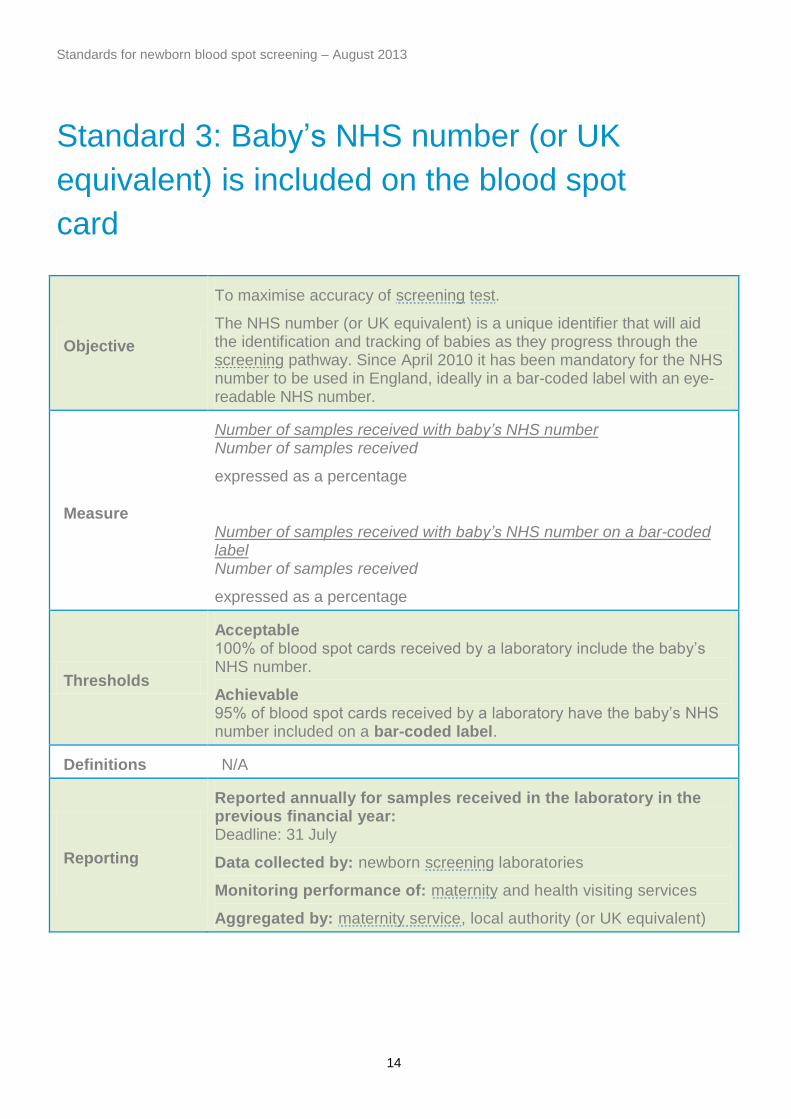
Standard 3: Baby’s NHS number (or UK
equivalent) is included on the blood spot
card
Objective
To maximise accuracy of screening test.
The NHS number (or UK equivalent) is a unique identifier that will aid the identification and tracking of babies as they progress through the screening pathway. Since April 2010 it has been mandatory for the NHS number to be used in England, ideally in a bar-coded label with an eye-readable NHS number.
Measure
Number of samples received with baby’s NHS number Number of samples received
expressed as a percentage
Number of samples received with baby’s NHS number on a bar-coded label Number of samples received
expressed as a percentage
Thresholds
Acceptable 100% of blood spot cards received by a laboratory include the baby’s NHS number.
Achievable 95% of blood spot cards received by a laboratory have the baby’s NHS number included on a bar-coded label.
Definitions N/A
Reporting
Reported annually for samples received in the laboratory in the previous financial year: Deadline: 31 July
Data collected by: newborn screening laboratories
Monitoring performance of: maternity and health visiting services
Aggregated by: maternity service, local authority (or UK equivalent)
Standards for newborn blood spot screening – August 2013
15
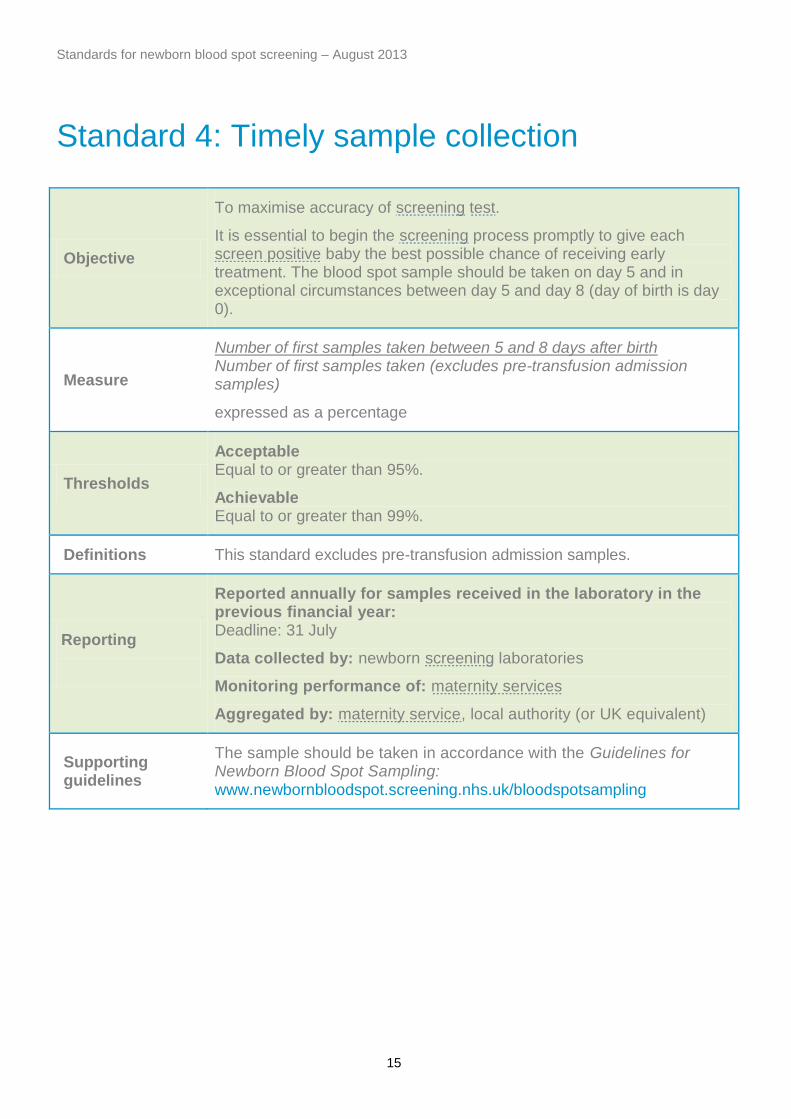
Standard 4: Timely sample collection
Objective
To maximise accuracy of screening test.
It is essential to begin the screening process promptly to give each screen positive baby the best possible chance of receiving early treatment. The blood spot sample should be taken on day 5 and in exceptional circumstances between day 5 and day 8 (day of birth is day 0).
Measure
Number of first samples taken between 5 and 8 days after birth Number of first samples taken (excludes pre-transfusion admission samples)
expressed as a percentage
Thresholds
Acceptable Equal to or greater than 95%.
Achievable Equal to or greater than 99%.
Definitions This standard excludes pre-transfusion admission samples.
Reporting
Reported annually for samples received in the laboratory in the previous financial year: Deadline: 31 July
Data collected by: newborn screening laboratories
Monitoring performance of: maternity services
Aggregated by: maternity service, local authority (or UK equivalent)
Supporting guidelines
The sample should be taken in accordance with the Guidelines for Newborn Blood Spot Sampling: www.newbornbloodspot.screening.nhs.uk/bloodspotsampling

Standards for newborn blood spot screening – August 2013
16
Standard 5: Timely receipt of a sample in
the newborn screening laboratory
Objective
To maximise accuracy of screening test.
All samples must arrive within the screening laboratory as soon as possible after the sample has been taken. This enables the laboratory to analyse the sample at the earliest opportunity and also reduces the risk of sample deterioration due to prolonged despatch.
Measure
All samples received within 4 working days of sample collection All samples received in laboratory
expressed as a percentage
All samples received within 3 working days of sample collection All samples received in laboratory
expressed as a percentage
Thresholds
Acceptable Equal to or greater than 99% of all samples received within 4 working days.
Achievable Equal to or greater than 99% of all samples received within three working days.
Definitions The day the sample is taken is day 0 for this standard.
Reporting
Reported annually for samples received in the laboratory in the previous financial year: Deadline: 31 July
Data collected by: newborn screening laboratories
Monitoring performance of: maternity and health visiting services
Aggregated by: maternity service, local authority (or UK equivalent)
Supporting guidelines
The sample should be taken in accordance with the Guidelines for Newborn Blood Spot Sampling: www.newbornbloodspot.screening.nhs.uk/bloodspotsampling

Standards for newborn blood spot screening – August 2013
17
Standard 6: Quality of the blood spot
sample
Objective
To maximise accuracy of screening test.
To obtain a good quality sample first time.
Measure
Number of avoidable repeat requests Total number of first blood spot samples received in laboratory
expressed as a percentage
Thresholds
Acceptable The avoidable rate is less than or equal to 2%.
Achievable The avoidable rate is less than or equal to 0.5%.
Definitions
A good quality blood spot sample is one that: is taken at the right time; has all data fields completed on the blood spot card; contains sufficient blood to perform all tests; has not been contaminated; and arrives in the laboratory in a timely manner.
Avoidable repeat requests (numerator) is the total number of repeat (second or subsequent) samples requested by the laboratory during the reporting period because the previous sample was:
Taken when the baby was too young (on or before day 4, where day of birth is day 0) (excluding pre-transfusion admission samples)
Insufficient blood
Unsuitable sample/card (eg on an expired blood spot card, contaminated, in transit for more than 14 days, anti-coagulated sample, baby’s NHS number and/or other details not accurately recorded on the blood spot card)
Blood samples received in laboratory (denominator) are the total number of first blood spot samples received in the laboratory during the reporting period as part of the newborn blood spot screening programme.
Reporting
Reported quarterly for key performance indicator (KPI) NB2: Deadlines: 30 September (Q1), 31 December (Q2), 31 March (Q3), 30 June (Q4)
Reported annually for samples received in the laboratory in the previous financial year: Deadline: 31 July

Standards for newborn blood spot screening – August 2013
18
Data collected by: newborn screening laboratories
Monitoring performance of: maternity and health visiting services
Aggregated by: maternity service, local authority (or UK equivalent)
Supporting guidelines
The sample should be taken in accordance with the Guidelines for Newborn Blood Spot Sampling: www.newbornbloodspot.screening.nhs.uk/bloodspotsampling

Standards for newborn blood spot screening – August 2013
19
Standard 7: Timely taking of a repeat blood
spot sample
Objective
To maximise accuracy of screening test.
In order that treatment and clinical referral targets are met the timely receipt of a repeat/second blood spot sample is imperative.
Measure
For each category defined:
Number of repeat samples taken as defined for individual tests Number of repeat samples requested
expressed as a percentage
Thresholds
Acceptable Equal to or greater than 95% of repeat samples taken as defined.
Achievable Equal to or greater than 99% of repeat samples taken as defined.
Definitions
A repeat sample from the avoidable repeat category must be taken within three calendar days of receipt of request
A second blood spot sample for raised IRT should be taken ideally on day 21 (between day 21 and 28)
A second blood spot sample for borderline TSH should be taken between seven and 10 days after the initial borderline sample
A second blood spot sample for TSH should be taken from babies born at less than 32 weeks gestation (less than or equal to 31 weeks + six days) when they reach 28 days of age, or day of discharge home whichever is the sooner (day of birth is day 0)
Reporting
Reported annually for babies born in the previous financial year: Deadline: deferred until 30 June 2014
Data collected by: maternity services (following implementation of the Newborn Blood Spot Failsafe Solution)
Monitoring performance of: maternity and health visiting services
Aggregated by: maternity service, local authority (or UK equivalent)

Standards for newborn blood spot screening – August 2013
20
Standard 8: CPA (screening)
Objective
To maximise accuracy of screening test.
Laboratories undertaking newborn blood spot screening shall be accredited by Clinical Pathology Accreditation (UK) Ltd (CPA), now formally part of the United Kingdom Accreditation Service (UKAS). This shall include the NBS specialist assessment.
DNA laboratories shall be a member of the UK Genetic Testing Network (UK GTN) and comply with the quality criteria laid down by the UK GTN Steering Group.
Measure The laboratory is CPA accredited.
Thresholds Acceptable The laboratory is CPA accredited (with the specialist assessment of NBS screening by the next full visit).
Definitions
CPA accredits pathology laboratories against a set of defined standards. These standards are allied to international standards for competence in medical laboratories – ISO 15189. During the newborn screening specialist assessment CPA looks at both the ISO standards and the UK screening specific laboratory standards, as an integrated process. Read more information on the newborn screening laboratory standards included in the CPA assessment at: www.newbornbloodspot.screening.nhs.uk/standards-consultation-2012-13.
Reporting
The assessment comprises a main visit to the laboratory by a team of independent assessors at intervals of every four years, with a surveillance visit by a regional assessor within two years of the main visit. Other visits may be undertaken to assess resolved non-compliances as part of continuing surveillance of enrolled laboratories.
Laboratories must make available reports from accreditation services to screening programmes, the national team and commissioners.
Laboratory accreditation can be checked at www.cpa-uk.co.uk.

Standards for newborn blood spot screening – August 2013
21
Standard 9: Timely processing of all PKU,
CHT and MCADD screen positive samples
Objective To facilitate high quality and timely intervention in those who wish to participate.
Measure
For each condition:
Number of positive screening results available and clinical referral initiated within three or four working days Total number of positive screening results available
expressed as a percentage
Thresholds
Acceptable 100% of babies with a positive screening result have a clinical referral initiated within four working days of sample receipt by screening laboratory.
Achievable 100% of babies with a positive screening result have a clinical referral initiated within three working days of sample receipt by screening laboratory.
Definitions
Applies to PKU, CHT and MCADD – laboratories shall notify positive screening results in accordance with the Initial Clinical Referral Guidelines and Standards for each condition. This notification initiates the clinical referral of screen positive cases.
Reporting
Reported annually for samples received in the laboratory in the previous financial year: Deadline: 31 July
Data collected by: newborn screening laboratories
Monitoring performance of: newborn screening laboratories
Aggregated by: newborn screening laboratory

Standards for newborn blood spot screening – August 2013
22
Standard 10: CPA (diagnosis)
Objective
To maximise accuracy of diagnostic test.
Follow up screening and diagnostic tests shall be undertaken in line with the diagnostic protocols.
Measure The laboratory is CPA accredited.
Thresholds Acceptable The laboratory is CPA accredited.
Definitions CPA accredits pathology laboratories against a set of defined standards. These standards are allied to international standards for competence in medical laboratories – ISO 15189.
Reporting
The assessment comprises a main visit to the laboratory by a team of independent assessors at intervals of every four years, with a surveillance visit by a regional assessor within two years of the main visit. Other visits may be undertaken to assess resolved non-compliances as part of continuing surveillance of enrolled laboratories. Read more information on the newborn screening and diagnostic laboratory standards included the CPA assessment at www.newbornbloodspot.screening.nhs.uk/standards-consultation-2012-13.
Laboratory accreditation can be checked at www.cpa-uk.co.uk.

Standards for newborn blood spot screening – August 2013
23
Standard 11: Timely receipt into clinical
care
Objective To facilitate high quality and timely intervention in those who wish to participate.
Measure
Babies referred to specialist services are seen by condition-specific standard Total number of screen positive babies referred per condition
expressed as a percentage
Thresholds
A baby in whom PKU, CHT (on first sample) or MCADD is suspected should attend their first clinical appointment by:
Acceptable 100% by 17 days of age
Achievable 100% by 14 days of age
A baby in whom CHT is suspected on a repeat blood spot sample that follows a borderline TSH should have their first clinical appointment by:
Acceptable 100% by 24 days of age
Achievable 100% by 21 days of age
A baby in whom CF is suspected should have their first clinical appointment by:
CF suspected: two CFTR mutations detected:
Acceptable 95% of babies seen by 28 days of age
Achievable 100% of babies seen by 28 days of age
CF suspected: none or one CFTR mutation detected:
Acceptable 80% of babies seen by 35 days of age
Achievable 100% of babies seen by 35 days of age
A baby in whom SCD is suspected should be referred and registered with designated healthcare professional by:
Acceptable 90% of babies by 8 weeks of age
Achievable 95% of babies by 8 weeks of age
A baby in whom SCD is suspected should attend local clinic by 3 months of age:
Acceptable 90% of babies

Standards for newborn blood spot screening – August 2013
24
Achievable 95% of babies
Screen positive babies should be offered and prescribed penicillin V (or alternative) by 3 months of age:
Acceptable 90% of babies
Achievable 99% of babies
Definitions N/A
Reporting
Reported annually for babies born in the previous financial year: Deadline: 31 July
Data collected by: newborn screening laboratories (anonymised baby level data on all babies in whom a condition is suspected) and paediatric specialist centres
Monitoring performance of: all service providers
Aggregated by: newborn screening laboratory for PKU, CHT, CF and MCADD and by specialist centre for SCD

Standards for newborn blood spot screening – August 2013
25
Standard 12: Timeliness of results to
parents Objective
To report newborn blood spot screening results which are screen negative for each of the five conditions in a timely manner to parents.
Measure
Number of screen negative results letters despatched direct to parents from the child health records department by six weeks of age Number of babies that have newborn blood spot screening results which are screen negative for each of the five conditions recorded on the child health records department system within six weeks of birth
expressed as a percentage
Thresholds Acceptable 100%
Definitions
A template for the screen negative results letter is available: www.newbornbloodspot.screening.nhs.uk/statuscodes.
Where normal results letters are not sent by child health records departments, area teams should provide evidence that the health visitors have given the results to parents and documented this in the PCHR. This could be achieved through local audit.
Reporting
Reported annually for babies born in the previous financial year: Deadline: 31 July
Data collected by: child health records departments
Monitoring performance of: all service providers
Aggregated by: CCG

Standards for newborn blood spot screening – August 2013
26
Abbreviations
CCG clinical commissioning group
CF cystic fibrosis
CFTR cystic fibrosis transmembrane conductance regulator
CHT congenital hypothyroidism
CPA Clinical Pathology Accreditation (UK) Ltd
DNA deoxyribonucleic acid
IRT immunoreactive trypsinogen
ISO International Organization for Standardization
KPI key performance indicator
MCADD medium-chain acyl-CoA dehydrogenase deficiency
NBS newborn blood spot
NHS National Health Service
PCHR personal child health record
PCT primary care trust
PHE Public Health England
PKU phenylketonuria
SCD sickle cell disease
TSH thyroid stimulating hormone
UKAS United Kingdom Accreditation Service
UK GTN UK Genetic Testing Network
UK NSC UK National Screening Committee

Standards for newborn blood spot screening – August 2013
27
Appendix 1: Glossary
This glossary is reproduced in part from the glossary in the UK NSC’s Key Performance
Indicators for Screening 2013/14 Version 1.12 (© Crown Copyright, 2013) (available at
www.screening.nhs.uk/kpi/data-collection). The UK NSC glossary defines terms that are
consistent across the Quality Assurance standards/service objectives of all screening
programmes.
coverage
The proportion of those eligible for screening who are tested. Coverage is a measure of the delivery of timely screening to an eligible population. Low coverage might indicate that:
1. not all eligible people have been offered screening
2. those offered screening are not accepting the test
3. those accepting the test are not being tested
decline A response to an offer which indicates that a screening subject does not wish to proceed with a screening encounter
diagnosis A diagnostic process following a screen positive result to determine whether the subject is an affected case
effective timeframe
The period of time within which a screening test can be delivered such that a reliable result is most likely to be obtained. The effective timeframe for a test is usually specified in the policy / guidance for the relevant screening programme
eligible
The population that is entitled to an offer of screening. The criteria for eligibility may be administrative, demographic, clinical, or any combination of these, and may take into account individual circumstances such as time of presentation to the screening service
maternity service
A co-ordinated network of healthcare professionals contracted to or working under the policies and procedures agreed with a single acute Trust, with collective responsibility for the provision of antenatal, intrapartum and postpartum care. A single maternity service may include:
obstetric-led maternity units
midwifery-led maternity units
units responsible for the management of home births
newborn intensive care units
special care baby units
paediatric intensive care units

Standards for newborn blood spot screening – August 2013
28
offer
A formal communication made by the screening service, giving a specific subject a realisable opportunity to be tested within an effective timeframe. An offer or invitation will only count as an offer if:
1. it reaches the subject
2. the subject is capable of understanding and acting upon it
3. the screening service has the capacity to realise it
4. it offers an opportunity of testing within an effective timeframe
In the case of newborn screening programmes, the offer of screening is made to a responsible parent/guardian rather than the subject baby
refer
The process of securing further diagnosis/specialist assessment following a screen positive test. The date of referral is the first realisable assessment date offered by an appropriate specialist unit to a screening subject following a screen positive result. Allocation to a pending list or a referral subsequently cancelled by the specialist unit is not a referral
reporting period
The defined time period over which activities should be included in an aggregate audit or performance return. A reporting period can relate to any specified period but for routine reports is usually quarterly or annual. Most screening processes occur over a period of days or weeks, to allow a scan or sample to be assessed. In such cases, a single point in the process (such as the screening encounter) should be used to determine whether the process falls within a particular reporting period
result
A formal and completed assessment of the risk of a condition being screened for in a subject, following a screening encounter. Usually a result will be screen positive or screen negative. Insufficient and unassessable indicate a failure to obtain a result, and are not themselves results
screen negative An indication following a test that the condition being screened for is low-risk / not suspected in a subject
screen positive An indication following a test that the condition being screened is high-risk/suspected in a subject
screening
Testing people who do not have or have not recognised the signs or symptoms of the condition being tested for, either with the aim of reducing risk of an adverse outcome, or with the aim of giving information about risk
test A screening encounter leading to the determination of a conclusive result
total population The population that meets the general criteria for inclusion within a screening programme. The criteria for inclusion within a screening programme may be administrative, demographic, clinical, or any

Standards for newborn blood spot screening – August 2013
29
combination of these. Not everyone in the total population is likely to be eligible for screening (for example, those who present later than it would be possible to test)
uptake
The proportion of those offered screening who are tested. Uptake is a measure of the delivery of screening in the population to which it is offered. Low uptake might indicate that:
1. those offered screening are not accepting the test
2. those accepting the test are not being tested

Standards for newborn blood spot screening – August 2013
30
Appendix 2: Newborn blood spot screening
status codes
This table of newborn blood spot screening status codes is reproduced from Newborn Status
Codes v2.0 (available at www.newbornbloodspot.screening.nhs.uk/statuscodes).
Screening status code
Suggested term displayed in child health system
Comment
01 Specimen received in laboratory
Same value applies to all screening tests (ie relates to the blood spot card)
Additional data items to be provided with this status code and entered into child health systems electronically or by manual means:
date sample taken
date sample received in laboratory
laboratory identifier
02 (Condition screened for) Declined
Applies to each screening test individually
03 (Condition screened for) Repeat/further sample required
Applies to each screening test individually. It is important for uses of the child health system to understand that this status code indicates that there is not a screening outcome associated with the condition screened for on this sample
Two additional data items:
“Reason for repeat test” and “Repeat test comment” are required where status code 03 applies”
“Reason for repeat test” will include the following pick list for all conditions screened for:
too young for reliable screening
too soon after transfusion (<72 hours)
unsuitable sample
insufficient sample

Standards for newborn blood spot screening – August 2013
31
unsatisfactory analysis
In addition “Reason for repeat test” will also include the following additional options for:
Sickle:
transfused, repeat four months after last transfusion
too premature for testing
CHT:
pre-term
borderline result
CF:
inconclusive
“Repeat test comment”
Free text field
04 (Condition screened for) Not suspected
Applies to each screening test individually
05 (Condition screened for) Carrier
Applies to sickle cell and cystic fibrosis screening tests
A free text comments field is required in association with this status code:
“(Condition screening for) Carrier comment”
This text field is required to enable additional information to be provided to Child Health if necessary
06 Sickle not suspected, carrier of other haemoglobin
Applies to sickle cell disease screening test only
07 (Condition screened for) Not suspected; Other disorders follow up
Applies to each screening test individually
08 (Condition screened for) Suspected
Applies to each screening test individually
09 (Condition screened for) Applies to each screening test individually
Standards for newborn blood spot screening – August 2013
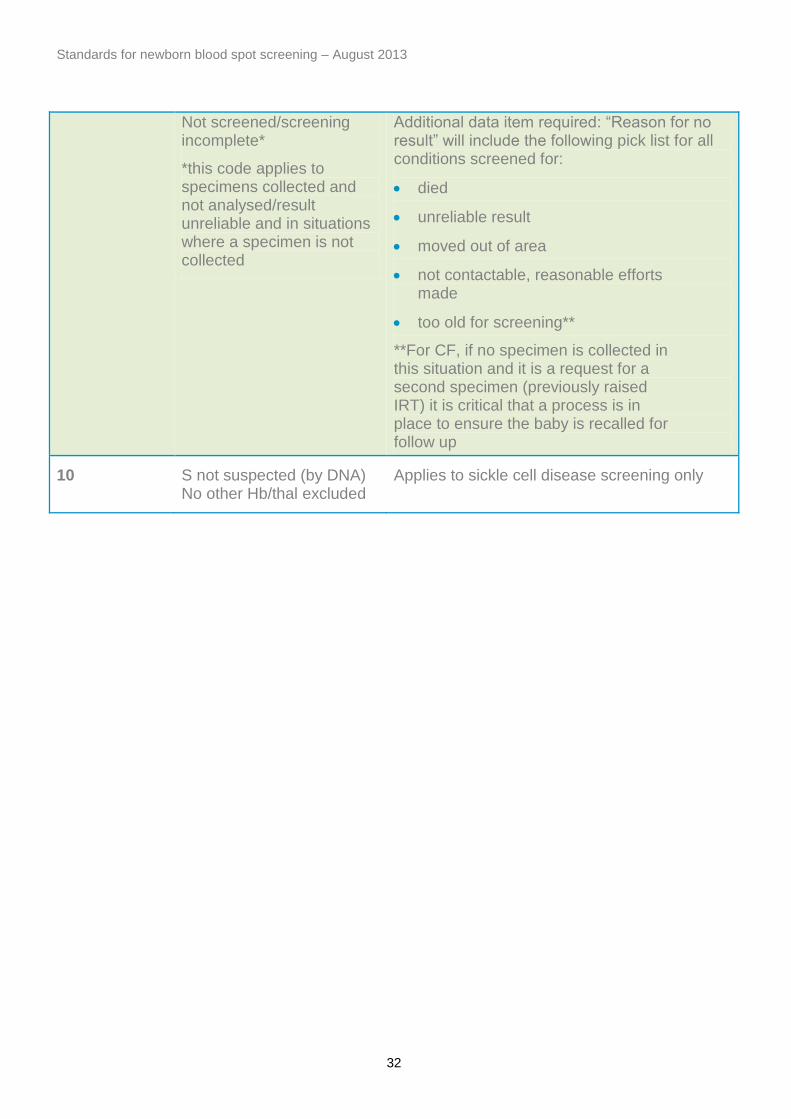
32
Not screened/screening incomplete*
*this code applies to specimens collected and not analysed/result unreliable and in situations where a specimen is not collected
Additional data item required: “Reason for no result” will include the following pick list for all conditions screened for:
died
unreliable result
moved out of area
not contactable, reasonable efforts made
too old for screening**
**For CF, if no specimen is collected in this situation and it is a request for a second specimen (previously raised IRT) it is critical that a process is in place to ensure the baby is recalled for follow up
10 S not suspected (by DNA) No other Hb/thal excluded
Applies to sickle cell disease screening only