state of maternal health in ghana, causes of maternal mortality, perenatal mortality, strategies for...
TRANSCRIPT

STATE OF MATERNAL HEALTH IN GHANA, CAUSES OF MATERNAL MORTALITY, PERENATAL MORTALITY, STRATEGIES FOR REDUCING MM AND NNM
Emmanuel K Srofenyoh

Outline of Presentation
Introduction Global and National Magnitude of the
Problem Strategies to reduce mortalities and
morbidities. Conclusions

The issue of the unacceptably high maternal mortality in developing countries has remained an unrelenting challenge to major world bodies and advocates over the past decades and threatened to remain so over decades to come.
In 2005, there were an estimated 536 000 maternal deaths worldwide." WHO 2009a.

Maternal Health: Scope of Problem
Current Approach to Reduction of Maternal
Mortality4
180–200 million pregnancies per year 75 million unwanted pregnancies 50 million induced abortions 20 million unsafe abortions (same as above) 600,000 maternal deaths (1 per minute) 1 maternal death = 30 maternal morbidities
99% in developing world ~ 1% in developed countries

Burden of the problem - Why all the worry? – cont.
Region Risk of Dying
Africa 1 in 16
Asia 1 in 65
Latin America & Caribbean 1 in 130
Europe 1 in 1400
North America 1 in 3700
All developing countries 1 in 48
All developed countries 1 in 1800
Ghana 1 in 35
Women's lifetime risk of dying from Pregnancy.

Neonatal Health: Scope of Problem
Current Approach to Reduction of Maternal
Mortality6
3 million neonatal deaths (first week of life)
3 million stillbirths

Why is it Necessary for Every Country to make efforts to protect Women and ensure their Survival?

Economic Reasons:1. Death of a woman in reproductive age has
clear implications for a country’s Productive capacity, labour supply, economic well being.
2. A woman’s wage earnings are critical to the family unit, community and to over all poverty reduction effort and benefist family welfare more than men’s wage earnings.
3. Also when a woman dies the children or her dependants has a diminished prospect of leaving a productive life (World Bank 1999).

Other reasons
Intrinsic value of women: protecting them is therefore an end in itself
Human right and social justice dimensions (ICPD, CEDAW).

UN Millenium Development goals

GHANA’S GOAL
BY 2015
REDUCE MATERNAL MORTALITY (by 3/4) FROM THE 2000 LEVEL TO 54/100,000 LIVE BIRTHS.
REDUCE U5 MORTALITY (2/3)TO 40/1000 LIVEBIRTHS
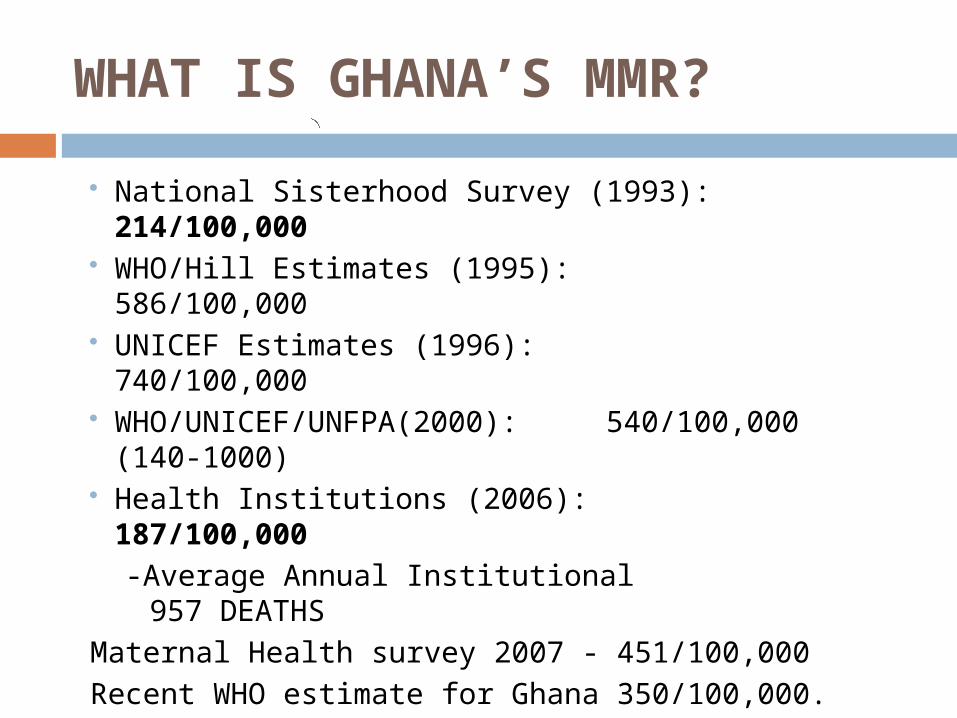
WHAT IS GHANA’S MMR?
National Sisterhood Survey (1993): 214/100,000 WHO/Hill Estimates (1995): 586/100,000 UNICEF Estimates (1996): 740/100,000 WHO/UNICEF/UNFPA(2000): 540/100,000 (140-
1000) Health Institutions (2006): 187/100,000
-Average Annual Institutional 957 DEATHS
Maternal Health survey 2007 - 451/100,000
Recent WHO estimate for Ghana 350/100,000.
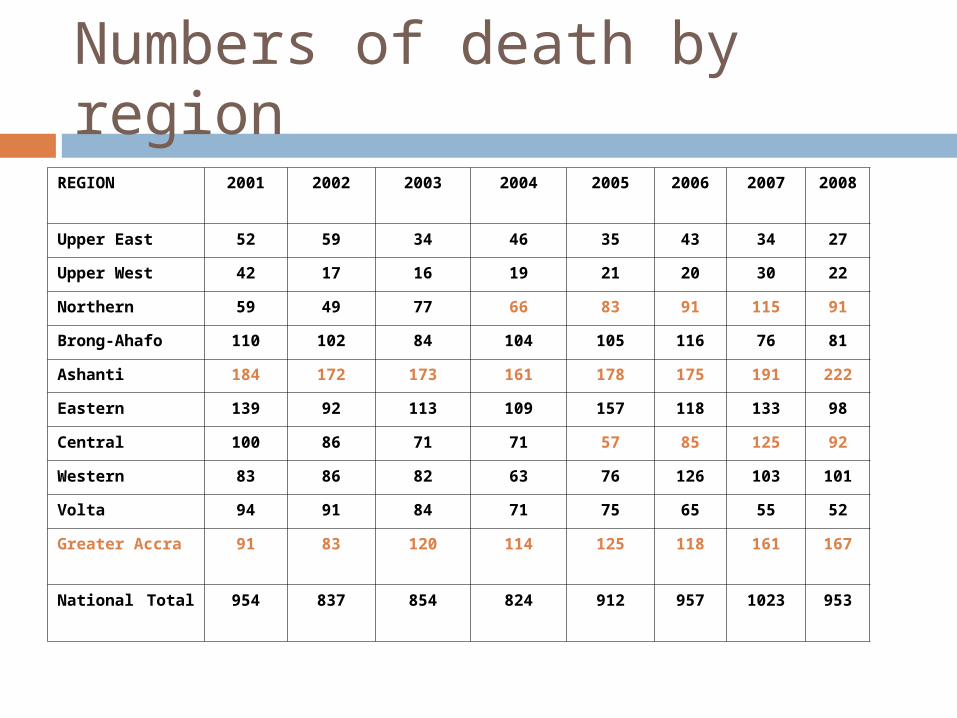
Numbers of death by region
REGION 2001 2002 2003 2004 2005 2006 2007 2008
Upper East 52 59 34 46 35 43 34 27
Upper West 42 17 16 19 21 20 30 22
Northern 59 49 77 66 83 91 115 91
Brong-Ahafo 110 102 84 104 105 116 76 81
Ashanti 184 172 173 161 178 175 191 222
Eastern 139 92 113 109 157 118 133 98
Central 100 86 71 71 57 85 125 92
Western 83 86 82 63 76 126 103 101
Volta 94 91 84 71 75 65 55 52
Greater Accra 91 83 120 114 125 118 161 167
National Total 954 837 854 824 912 957 1023 953

MATERNAL MORTALITY RATIO SCENARIOS 2005 – 2015
0
50
100
150
200
250
2005 2006 2007 2008 2009 2010 2011 2012 2013 2014 2015
Mat
erna
l de
aths
per
100
,000
liv
e bi
rths
With radical interventions
Without interventions/with current traditional interventions
214/100,000 LB
54/100,000 LB

Trend in Institutional MMR: GHANA 2002 - 2006
1.871.97
1.862.052.04
0
0.5
1
1.5
2
2.5
3
2002 2003 2004 2005 2006Year
MM
R/10
00 L
ive
Birt
hs

Trends in Antenatal Care Coverage (at least one) - GDHS

Postnatal Care Coverage 2002-200657.8% (2008)
53.4
55.7
53.3
55
53.7
52
52.5
53
53.5
54
54.5
55
55.5
56
2002 2003 2004 2005 2006Year
% C
over
age

Caesarean Section Rate, 2002 - 2006
6.9
6.1
5.75.85.6
4
4.5
5
5.5
6
6.5
7
2002 2003 2004 2005 2006
Year
Rate
(%)

Classification
Immediate Cause of Death Direct Indierct Avoidable Factors

Global Causes of Maternal Mortality
24.8
14.9
12.96.912.9
7.9
19.8
Hemorrhage 24.8%
Infection 14.9%
Eclampsia 12.9%
Obstructed Labor6.9%Unsafe Abortion12.9%Other Direct Causes7.9%Indirect Causes19.8%
Current Approach to Reduction of Maternal
Mortality21


Causes of Maternal Death in Ridge Cause Freq %tage
Direct Causes
Hypertensive disoders 9 34.6%
Obstetric Hemorrhage 6 23.1%
Septic abortion 1 3.8%
Pueperal Sepsis with Septicaemia 1 3.8 %
Ruptured Ectopic Gestation 1 3.8%
Indirect causes
HIV in Pregnancy 3 11.5 %
Malaria with severe IVH 1 3.8 %
Severe anaemia In pregnancy 1 3.8 %
SCD with VOC and Septicaemia 1 3.8 %
Others
Acute Collapse with severe respiratory Distress
2 7.7%
Total 26 100

Common Maternal Morbidities Recorded in Ghana
Fistula (leaking urine and faeces)
Infertility Anaemia Chronic Pelvic Pain

Interventions to Reduce Maternal Mortality
Current Approach to Reduction of Maternal
Mortality25
Historical Review Traditional birth attendants Antenatal care
Current Approach Family Planning Skilled attendant at delivery, Provision of Emergency obstetric care
services

Interventions: Traditional Birth Attendants
Advantages Community-
based Sought out by
women Low tech Teaches clean
delivery
Disadvantages Technical skills
limited May keep
women away from life-saving interventions due to false reassurance
26Current Approach to
Reduction of Maternal Mortality
Maternal Mortality ReductionSri Lanka 1940–1985
Current Approach to Reduction of Maternal
Mortality27
Health system improvements: Introduction of system of health facilities Expansion of midwifery skills Decreased use of home delivery and
delivery by untrained birth attendants Spread of family planning

Maternal Mortality ReductionSri Lanka 1940–1985
0
200
400
600
800
1000
1200
1400
1600
1800
1940–45 1950–55 1960–65 1970–75 1980–85Ma
tern
al
De
ath
s p
er
10
0 0
00
liv
eb
irth
s
Current Approach to Reduction of Maternal
Mortality28
85% births attended by trained personnel

Interventions: Traditional Birth Attendants
Current Approach to Reduction of Maternal
Mortality29
Conclusion: TBAs are useful in the maternal health network, but there will not be a substantial reduction in maternal mortality by TBAs delivering clinical services alone

Maternal Mortality: UK 1840–1960
050
100150200250300350400450500
MaternalDeaths
Current Approach to Reduction of Maternal
Mortality30
Improvements in nutrition, sanitation
Antibiotics, banked blood, surgical improvements
Antenatal care
Maine 1999.

Interventions: Skilled Attendant at Childbirth (Can avoid 13 t0 33%)
Current Approach to Reduction of Maternal
Mortality31
Proper training, range of skills Assess risk factors Recognize onset of complications Observe woman, monitor fetus/infant Perform essential basic interventions Refer mother/baby to higher level of
care if complications arise requiring interventions outside realm of competence
Have patience and empathyWHO 1999.
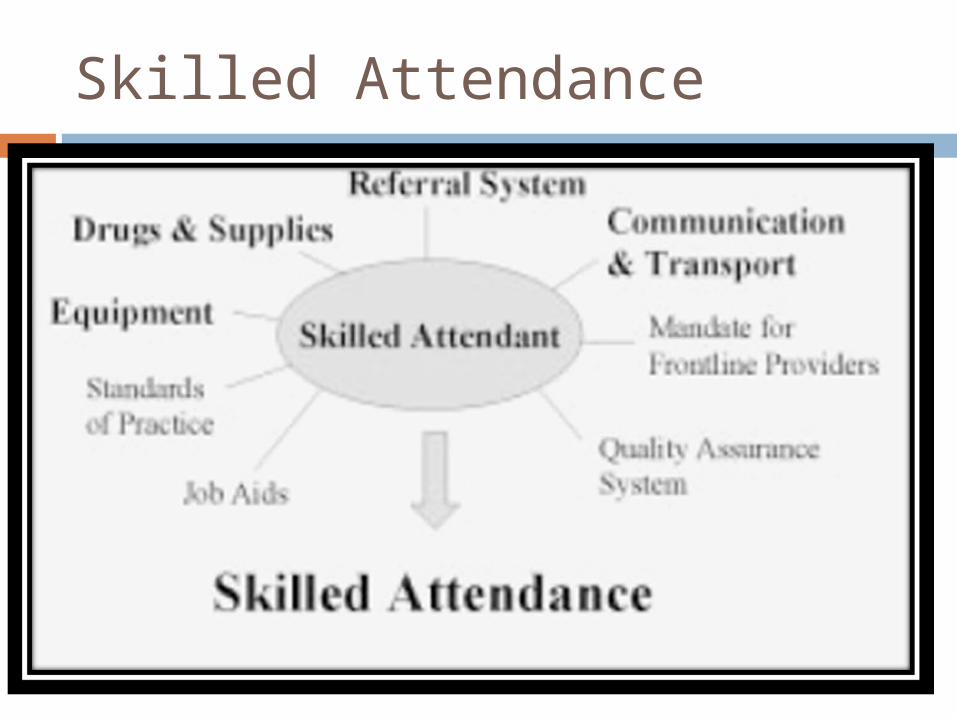
Skilled Attendance

Current Approach to Reduction of Maternal
Mortality33
R² = 0.74
0
200
400
600
800
1000
1200
1400
1600
1800
2000
0 10 20 30 40 50 60 70 80 90 100
Y Log. (Y)
The higher the proportion of deliveries attended by skilled attendant in a country, the lower the country’s maternal mortality ratio
% skilled attendant at delivery
Mat
erna
l dea
ths
per
1000
000
live
birt
hs

Signal Functions of EmOC (for every 500,000 population 1 comprehensive and 4 basic)
Basic EmOC 1. Administer parenteral antibiotics 2. Administer parenteral oxytocic drugs 3. Administer parenteral anticonvulsants for preeclampsia and eclampsia 4. Perform manual removal of placenta 5. Perform removal of retained products 6. Perform assisted vaginal deliveryComprehensive 7. Perform surgery (caesarean section) 8. Perform blood transfusion A Basic EmOC facility is one that is performing all of functions 1 to
6. A Comprehensive EmOC facility is one that is performing all of
functions 1 to 8.

Why EmONC
By far most important Intervention 15% of pregnancies develop
complications and becomes emergencies. These complications cannot be predicted
and many cannot be prevented. These emergencies can kill rapidly. Early identification and expeditious
management can avoid death in many cases

Some major questions that need be answered Are there enough facilities that provide
EmONC? Are they well distributed? Do women use these services, if not
why? Are the women using the services those
who really need them?
Some major questions that need be answered Are facilities providing critical life-saving
services? Is the quality of the services adequate? Are other interventions needed?

FACTORS INFUENCING MATERNAL DEATHSDELAY ONE:Recognizing danger signs
Simply does not know the signs and symptoms
Some signs are initially innocuous and pose serious threat in their extreme forms eg. PIH
Difficulty in assessing severity. Bleeding and Prolonged labour

DELAY TWO : Deciding to seek care
Other decision makers not available TBAs make not act on time Lack of trust for staff Fear of poor care Fear of being mistreated by staff Cost of services
DELAY THREE : Reaching Care
Poor roads Scarce vehicles Vehicles refuse to carry pregnant women
with complications for fear of soiling their vehicle or even dying in their vehicle.
Cost of transport Lack of companion
DELAY FOUR: Receiving care at Health Facility.
LACK OF EMERGENCY PREPAREDNESS INADEQUATE SKILLS AND KNOWLEDGE SHORTAGE OF STAFF. POOR STAFF ATTITUDE LACK OF EQUIPMENT AND SUPPLIES POOR INFRASTRUCTURE
Conclusion
The only ways we as a nation can achieve our vision with regards to maternal health are to ensure that:
Women do not carry pregnancy against their wishes.
Those who wish to have babies have access to skilled and professional care.
And those who develop complications have rapid access to EmONC services.