status epilepticus in child je workshop mks
TRANSCRIPT
STATUS EPILEPTICUS
Dr. Manoj Kumar SinghAssistant Professor
PMCH Patna

Electrical power house
Status Epilepticus
An important Medical Emergency dealt by PhysiciansPediatrician NeurologistsFamily physician
Prompt & efficient treatment
↓mortality & morbidity.
Regional differences in epidemiology

Epidemiology
• USA 102000-152000/yr
• Highest (>50% of cases <3y) in children & >60yrs ,bimodal distribution
• Burden of SE in India 2,80,000/y
• Mortality • Adults
• Children
15 to 22%
3 to 15%


Frequency of seizure in different age groups
0
5
10
15
20
No
of
pat
ien
ts
1st 2nd 3rd 4th 5th 6th >6th
Decades
frequency of status epilepticus in different age group
Kalita J et al 2009
Pathophysiology
• GLUTAMATE = the major excitatory AA neurotransmitter in brain
– Any factor increases Glutamate activity can lead to seizures
– NMDA(N-methyl-D-aspartic acid) is an AA derivative which acts as a specific agonist at the NMDA receptor mimicking the action of glutamate
• GABA = main inhibitory neurotransmitter, ; GABA antagonists can cause SE

Definition of SE :
• Definition by ILAE in 1981 :
– Seizure lasting > 30 minutes
OR
Recurrent seizures > 30 minutes during which the pt. does not regain consciousness.
Why 30 minutes ?
Animal experiments in the 1970s and 1980s had shown that ...
… neuronal injury could be demonstrated after 30 min of seizure activity, even while maintaining respiration and circulation 1985;18(3):281-90.

“Continuous seizures lasting at least 5 minutes
or two or more discrete seizures between which there is an incomplete recovery of
consciousness”
Operational Definition:

Status epilepticus 11
The longer SE persists,–the lower is the likelihood of spontaneous cessation–the harder is it to control–the higher is the risk of morbidity and mortality
Treatment for most seizures needs to be instituted after > 5 minutes of seizure activity
Bleck TP. Epilepsia 1999;40(1):S64-6

TERMINOLOGY:
• CONVULSIVE SE : characterised by prolonged tonic clonic muscle contractions, associated loss of consciousness.
• Prolonged convulsive status epilepticus can degenerate into a non convulsive state look for subtle mouth twitching, eye movements etc.
• NON-CONVULSIVE SE – absence of overt muscle activity
• has continuous or near-continuous generalized electrical seizure activity for at least 30 minutes without physical convulsions.
• Diagnosis can be difficult - physical signs: agitation or confusion, nystagmus, or bizarre behaviors such as lip smacking or picking at items in the air.
TERMINOLOGY:
• NCSE is categorized into absence or complex partial SE based on EEG criteria.
• Absence SE - benign form of SE that does not cause serious brain damage.
• Complex partial SE is associated with neuronal injury and high morbidity and mortality ~ 3 times higher.
• aggressive treatment advocated.
REFRACTORY SE: When seizure have persisted for >60 minutes and have not responded to use of 3 or more medications. Mortality 16-32%.

ETIOLOGY:
• New onset epilepsy of any type.• Drug intoxication (eg. TCA’s), drug withdrawl and
abuse.• Electrolyte imbalance,• Acute head trauma.• Encephalitis, Meningitis,Stroke.• HIE, Brain tumors.• IEM• Neurodegenerative diseases.

Causes of SE
6315
79
13Infection
Stroke
Metabolic
Drug default
Misc
Kalita J et al 2009

ETIOLOGICAL CLASSIFICATION OF SE:
• CRYPTOGENIC: SE in absence of an acute precipitating CNS insult or metabolic dysfunction in a patient without a pre-existing neurologic abnormality.
• REMOTE SYMPTOMATIC: SE in a patient with a known history of a neurologic insult asociated with an increased risk of seizures(Stroke,TBI,static encephalopathy).
• FEBRILE: THE MOST COMMON TYPE IN CHILDREN. SE provoked solely by fever in a patient without a history of afebrile seizures.
• ACUTE SYMPTOMATIC: SE during an acute illness involving a known neurologic insult or metabolic dysfunction.
• PROGRESSIVE ENCEPHALOPATHY: SE in a pt. with a progressive neurologic disease.
Prolonged seizures
Duration of seizureDuration of seizure
Life Life threateningthreatening
systemicsystemicchangeschanges
DeathDeathTemporaryTemporary
systemicsystemicchangeschanges
Respiratory
• Hypoxia and hypercarbia
- ⇓ ventilation (chest rigidity from muscle spasm)
- Hypermetabolism (⇑ O2 consumption, ⇑ CO2 production)
- Poor handling of secretions- Neurogenic pulmonary edema?
Hypoxia
• Hypoxia/anoxia markedly increase the risk of mortality in SE
• Seizures (without hypoxia) are much less dangerous than seizures and hypoxia
Towne AR. Epilepsia 1994;35(1):27-34
Neurogenic pulmonary edema
•Rare complication
•Likely occurs as consequence of marked increase of pulmonary vascular pressure
Johnston SC. Postictal pulmonary edema requires pulmonary vascular pressure increases. Epilepsia 1996;37(5):428-32

Acidosis
• Respiratory
• Lactic– Impaired tissue oxygenation– Increased energy expenditure
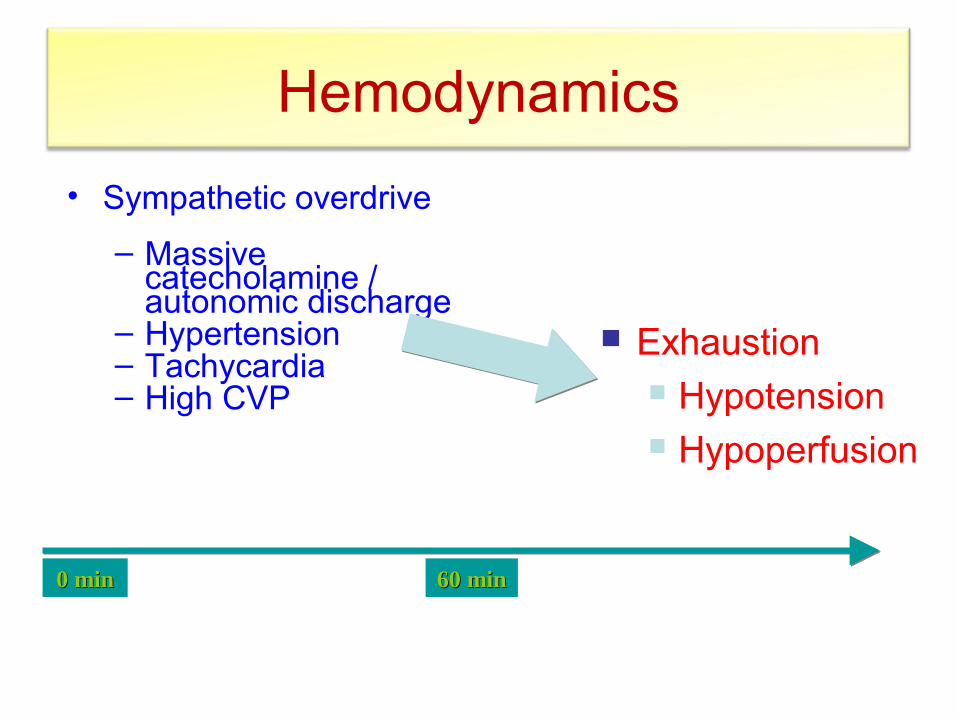
Hemodynamics
• Sympathetic overdrive – Massive
catecholamine / autonomic discharge
– Hypertension– Tachycardia– High CVP
Exhaustion Hypotension Hypoperfusion
0 min0 min 60 min60 min
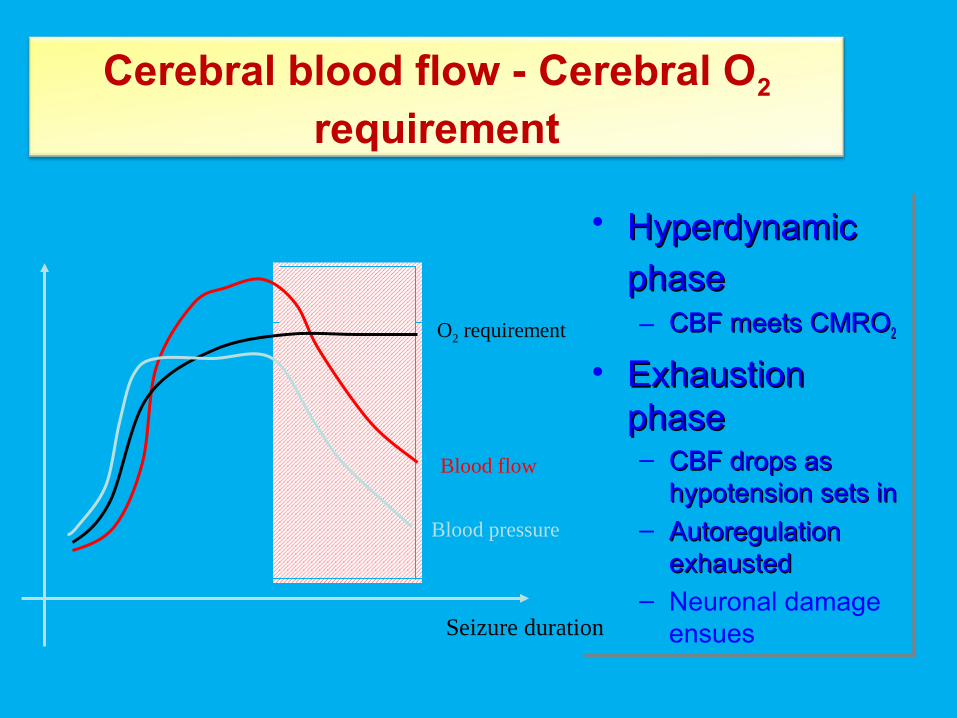
Cerebral blood flow - Cerebral O2 requirement
• HyperdynamicHyperdynamic phasephase – CBF meets CMROCBF meets CMRO22
• Exhaustion Exhaustion phasephase– CBF drops as CBF drops as
hypotension sets inhypotension sets in– Autoregulation Autoregulation
exhaustedexhausted– Neuronal damage
ensues
• HyperdynamicHyperdynamic phasephase – CBF meets CMROCBF meets CMRO22
• Exhaustion Exhaustion phasephase– CBF drops as CBF drops as
hypotension sets inhypotension sets in– Autoregulation Autoregulation
exhaustedexhausted– Neuronal damage
ensues
Blood pressure
Blood flow
O2 requirement
Seizure duration

Glucose
• Hyperdynamic phase – Hyperglycemia
• Exhaustion phase– Hypoglycemia
develops– Hypoglycemia
appears earlier in presence of hypoxia
– Neuronal damage ensues
• Hyperdynamic phase – Hyperglycemia
• Exhaustion phase– Hypoglycemia
develops– Hypoglycemia
appears earlier in presence of hypoxia
– Neuronal damage ensues
Glu
cose
Seizure duration
30 min
SE
SE + hypoxia
Other alterations
• Blood leukocytosis (50% of children)
• Spinal fluid leukocytosis (15% of children)
• ⇑ K+
• ⇑ creatine kinase• Myoglobinuria

Management in the hospital
• Any patient who comes to emergency & is convulsing requires aggressive treatment.
• Aim: Maintain vitalsTermination of SE,sPrevent seizure recurrenceManagement of precipitating causesCorrect metabolic imbalanceManagement of systemic complications

Immediate general care
• Airway: Suction, avoid mandible & tongue fall• Administer 02 by nasal catheter• IV access:
– blood sugar, electrolyte, LFT, KFT, AED level, coagulation level
– Administer 2-4ml/kg 10% dextrose if hypoglycemia.• Monitor BP: Immediate ↑BP, after 2 hr ↓BP• Fluid: Avoid over hydration but maintain
euvolemia.• Acidosis: Subsides with control of SE
HCO3 therapy unnecessary• Pyrexia: Cold sponging

Status epilepticus 28
Other investigations
• Lumbar puncture Always defer LP in unstable patient, but never delay
antibiotic/antiviral rx if indicated
• Neuroimaging – Do if doubt of intracranial pathology,raised ICT,
history of trauma or presence of lateralising sign. If etiology is uknown (only after SE is controlled and
Pt. is stabilised) .MRI is more sensitive than CT.
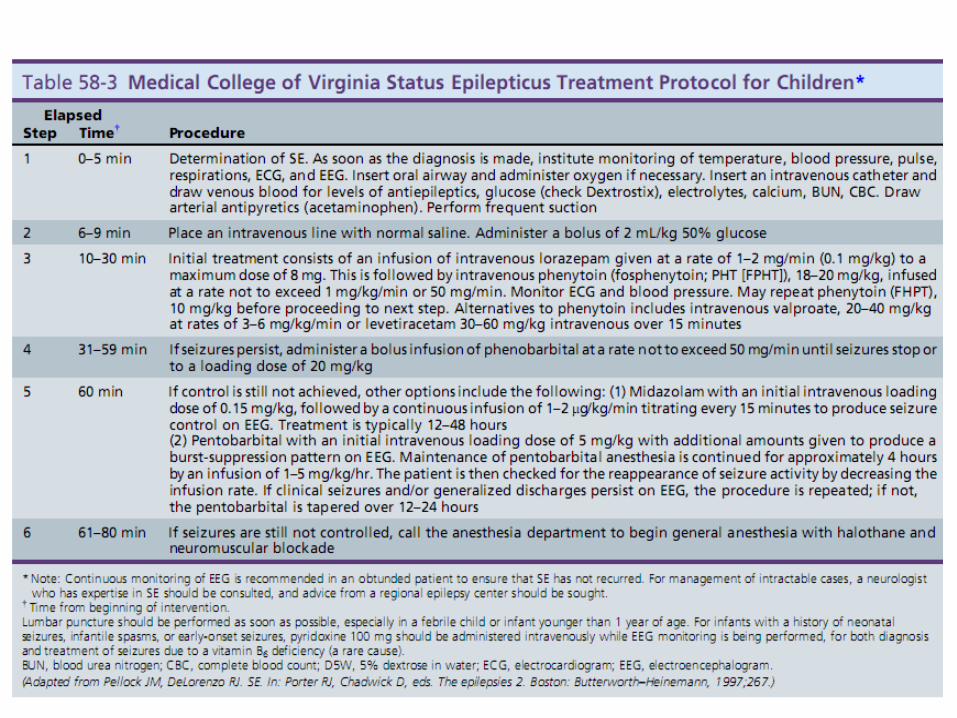

Benzodiazepines
• Diazepam– High lipid solubility– Thus very rapid onset – Redistributes rapidly– Thus rapid loss of
anticonvulsant effect– Adverse effects are
persistent:• Hypotension• Resp. depression
• Lorazepam– Low lipid solubility– Action delayed 2 minutes– Anticonvulsant effect 6-12
hrs– Less respiratory depression
than diazepam
Midazolamfor brief seizures May be given i.m. to treat refractory SE

Phenytoin Fosphenytoin
• 15-20 mg/kg i.v. @50mg/min• 100 mg phenytoin =
• 20 mg PE/kg i.v @ 150mg/min Fosphenytoin 150 mg
pH 12Extravasation causessevere tissue injury
pH 8.6Extravasation welltolerated
• Onset 10-30 min • Onset 5-10 min
•May cause hypotension, dysrhythmia(may be because of rapid administration and propylene glycol which is used as diluent)
• less cardiac complications as it is water soluble and propylene glycol is not used as diluent.
• Cheap • Expensive

Anticonvulsants - Long acting
PHENOBARBITONE:• First line agent in neonatal seizures.• A potent AED, acts by enhancing GABA-A
activity.• Dose- 20 mg/kg infused at no more than 30
mg/min.• Unacceptably high incidence of sedation and
respiratory depression and it may be difficult to perform neurological assesment upto 24-36 hrs.

Anticonvulsants - Long acting
LEVETIRACETAM:• New broad spectrum anticonvulsant, recently
been used with success in acute seizures and SE.
• Renal excretion, free from any significant drug interactions, neuroprotective effects demonstrated.
• Multiple sites of action- Ca, glutamate receptors and GABA modulation.
• LD- 30-60 mg/kg @ 5 mg/kg/min.

Initial choice of long acting anticonvulsants in SE
Is patient an infant?Is patient an infant?Is patient already receiving Is patient already receiving
phenytoin?phenytoin?
Is patient an infant?Is patient an infant?Is patient already receiving Is patient already receiving
phenytoin?phenytoin?
YesYesNoNo
At high risk for At high risk for extravasation ?extravasation ?
(small vein, difficult access etc.)?(small vein, difficult access etc.)?
PhenobarbitalPhenobarbital
YesYesNoNo
PhenytoinPhenytoin FosphenytoinFosphenytoin

Refractory SE
SE persisted for >60 min & have not respond to use of 3 or more drugs.
• Drugs: – Midazolam, thiopental, diazepam drip or
propofol drip, pentobarbital.
• Regular medication in optimal dose
• Tertiary care centre should be consulted
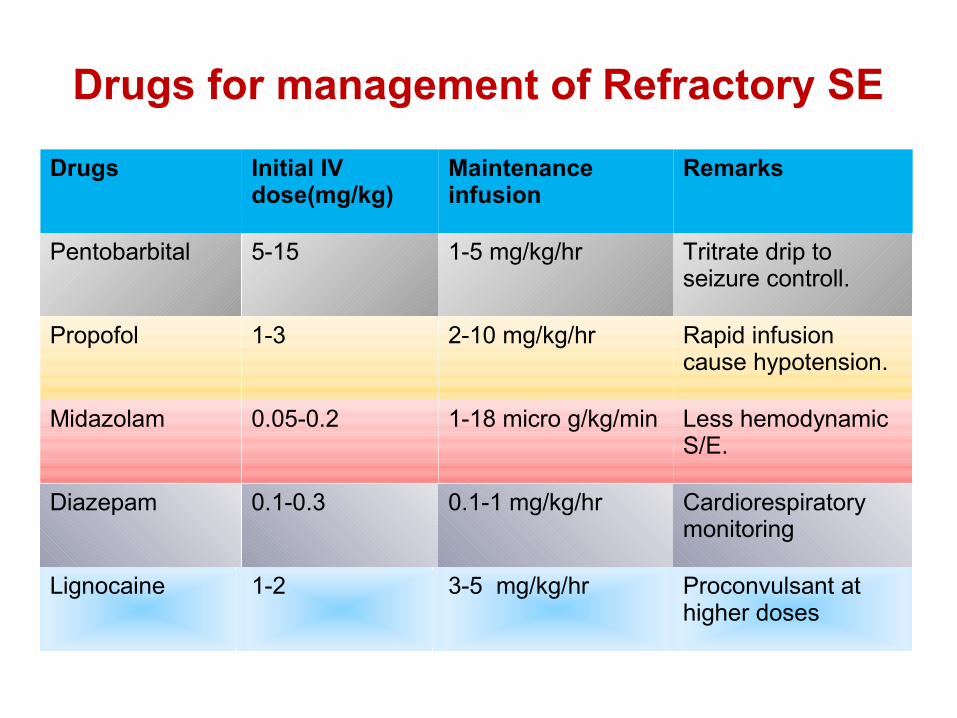
Drugs for management of Refractory SE
Drugs Initial IV dose(mg/kg)
Maintenance infusion
Remarks
Pentobarbital 5-15 1-5 mg/kg/hr Tritrate drip to seizure controll.
Propofol 1-3 2-10 mg/kg/hr Rapid infusion cause hypotension.
Midazolam 0.05-0.2 1-18 micro g/kg/min Less hemodynamic S/E.
Diazepam 0.1-0.3 0.1-1 mg/kg/hr Cardiorespiratory monitoring
Lignocaine 1-2 3-5 mg/kg/hr Proconvulsant at higher doses

Refractory SE
• Recent meta-analysis showed midazolam infusion is good choice for initial T/t of REF SE. Fewer hemodyanamic consequences and lesser need for invasive monitoring and mechanical ventilation.
• Propofol less effective than barbiturate• Propofol ↑mortality than midazolam
– Gilbert et al 1999; Niemeijer et al 2003

Emerging Therapies
• Inhalational Anaesthetic agents (isoflurane & desflurane)
Attractive features include efficacy, rapid onset of action, ability to titrate according to EEG.
Both drugs in end tidal concentrations of 1.2-5%achieved an EEG burst suppression and termination of seizure activity within minutes.
However further studies are needed in this field.

KETAMINE - An NMDA receptor antagonist
• Experimental studies have demonstrated synergistic action of diazepam and ketamine in termination SE.
• Efficacy in extremely refractory SE has been documented in both children and adults.
• No cardiac depressant properties, hence does not cause hypotension.
• Caution in patients with increased ICP. Ketamine increases ICP. Rule out SOL.

Treatment at home or PHC
• Seizure >5min or 3 seizures in 1hr
• Rectal diazepam 0.2-0.5mg/kg– Children: Onset→2nd dose 4hrs later– Adults: Onset →4 →12hrs
• No respiratory suppression
• ↓Seizure recurrence & ↑Global outcome

Pre-hospital treatment of SE
• Midazolam :– Buccal (Lancet, Scott et al 1999)– intranasal (BMJ,Lahat et al 2000)– IM (Emerg Med,Towne et al 1999)
• Paraldehyde PR 0.3-0.5mg/kg
NONPHARMACOLOGICAL TREATMENTS
• Resective surgery• Vagal nerve stimulation• KETOGENIC DIET- Diet high in fat and low in
carbohydrates. Induces ketosis in body and thought to suppress seizures by release of Leptin.Exact mechanism remains unknown.
• Hypothermia- decrease brain metabolism which is neuroprotective.
• Electroconvulsive therapy - ECT-dose-1 session daily for 3-8 days. Mechanism-not known

Mortality & morbidity of GCSE
• Mortality: – 3-30%– Children< adults
• If GCSE last >30min– Respiratory compromise→Hypoxia →Acidosis – Hypoglycemia
Hypotension

Prognosis of SE
• Type: GCSE worse than Partial complex partial & NCSE
• Etiology: Anoxia, encephalitis, stroke worse than drug default SE• Duration: >1hr has worse than shorter
duration of SE • Recurrence: Neurological deficit
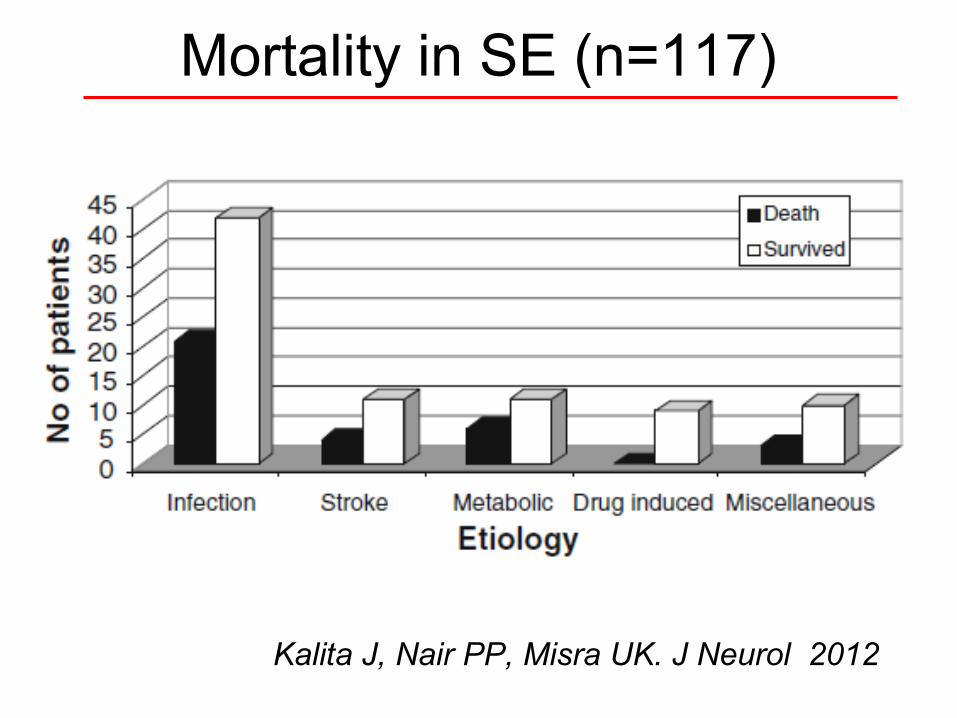
Mortality in SE (n=117)
Kalita J, Nair PP, Misra UK. J Neurol 2012
Conclusion• GCSE >5 min should be considered for operational
def of SE• ABC, general care, fluid, electrolyte & nursing • Urgent pre hospital Rx by rectal Diazepam, nasal,
buccal or im Midazolam ?• Hospital Rx: lorazepam, Fosphenytoin, PB,
midazolam, propofol, VPA, inhalation anesthetics• EEG monitoring not a must• ICU care ideal but don’t leave the patients in
absence of ventilator

Thank You & Good Luck