stent assisted reconstruction of difficult aneurysms in acute subarachnoid hemorrhage
TRANSCRIPT

STENT ASSISTED RECONSTRUCTION OF DIFFICULT ANEURYSMS IN ACUTE SUBARACHNOID HEMORRHAGE: A SINGLE CENTER EXPERIENCE
Vipul GuptaNeurointerventional Surgery
Institute of Neurosciences
Medanta the Medicity, Gurgaon

When?
Aneurysms not amenable to standard coiling, balloon assisted coiling or surgery
Dissecting/fusiform aneurysms
Blister aneurysms
Dysplastic berry aneurysms

Stent…. Flow diversion
Intimal growth- healing
Angle of the artery

Purpose
Antiplatelet therapy External Ventricular drain
Associated intraparenchymal hematoma
Potential for infarction secondary to
vasospasm
High likelihood of future invasive
procedures.
StentSupport at neck
Avoid coil protrusion

Data
• Retrospective review of 548 intracranial aneurysms
• 35 aneurysms in 33 patients -F- 19, M-14; 30-68 yrs
• Fisher grade III SAH - 22 (66.6%)
• H& H grade- I-III - 27 (81.8%)• EVD/ Lumbar drainage - 8 (24.2%)
• <14 days of SAH - 26(78.7%)
•
• Wide Neck aneurysms - 16
• Dissecting and/or blister aneurysms - 19
• Single (28) or double overlapping (5) stents with additional coil placement in 26 aneurysms.

Anti-platelet Regime
Antiplatelets - 2 hours prior to the procedure Ecospirin -300 mg
& Clopidogrel -450mg/Prasugrel -50mg/Ticagrelor 180 mg
Systemic heparinization during procedure
EVD if required, prior to the loading dose.
• Technical complications
• 5 (15.1%) in-stent clots, resolved with I/A Reopro
• 1(2.8%) aneurysm rupture during coiling
• 2 (5.7%)- ICA dissection, placement of stent.
• 2 patients had non fatal parenchymal haemorrhage at the EVD insertion/removal site.
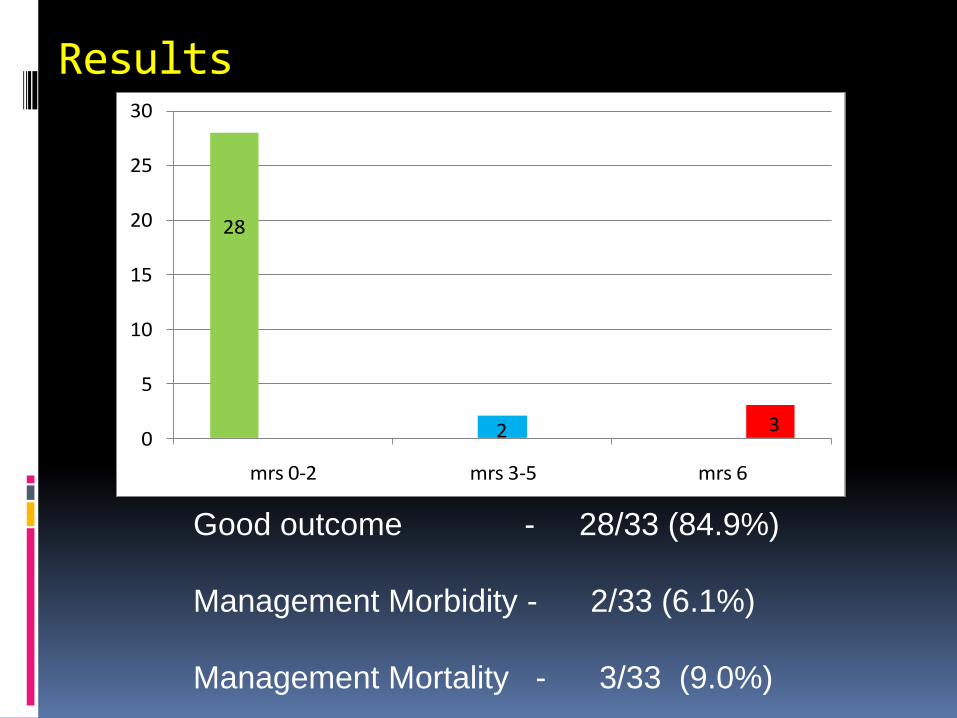
Results
28
2 30
5
10
15
20
25
30
mrs 0-2 mrs 3-5 mrs 6
Good outcome - 28/33 (84.9%)
Management Morbidity - 2/33 (6.1%)
Management Mortality - 3/33 (9.0%)

Mortality and MorbidityPatient Age H
&H
Site Stents Used
MRS at discharge
Death
Patient 1 33/F 2 Left vertebral artery dissecting aneurysm
1 6 Rupture during coiling
Patient 2 53/F 4 Right ICA blister aneurysm
3 6 Meningitis
Patient 3 65/F 3 Right ICA blister aneurysm
1 3( righthemiparesis)
Cardiac arrest while tapping pleural fluid
Patient 4 62/M 4 Basilar artery dissecting aneurysm
2 3 Vision loss due to vitreous hemorrhage
Patient 5 42/M 4 Right ICA blister aneurysm
1 5 Malignant vasospasminfarcts

Classical blister aneurysm
34-year M, SAH

2 overlapping stents
1-year follow-up

Dissecting blister aneurysm –
poor grade
EVD
2-overlapping stents
Had repeated nasal & gastric bleedings (Varices,
Cirrhosis) - Anti-platelets were reduced
Almost complete clinical recovery
Case 3
5 months

Angiogram after 10 days
Case 2




A
D E F


A

B C

Review of literature
Neurosurgery. 2012 Jun;70(6):1415-29; discussion 1429. doi: 10.1227/NEU.0b013e318246a4b1.
Stent-assisted coiling of wide-necked aneurysms in the setting of acute subarachnoid hemorrhage: experience in 65
patients.
Neurosurgery. 2013 Jun;72(6):953-9. doi: 10.1227/NEU.0b013e31828ecf69.
Treatment of ruptured intracranial aneurysms: comparison of stenting and balloon remodeling.
AJNR Am J Neuroradiol. 2011
Aug;32(7):1232-6. doi:
10.3174/ajnr.A2478. Epub 2011 May 5.
Stent-assisted coiling in acutely
ruptured intracranial aneurysms: a
qualitative, systematic review of the
literature.

Conclusion
Our findings demonstrate that stent-assisted coiling is a viable treatment option for these challenging lesions in the setting of an acute SAH.
Hemorrhagic complications secondary to antiplatelet agents, although potentially deadly or debilitating, occurred infrequently.
Thromboembloic complications can be avoided by careful management with antiplatelets.