stm functional showdeck mockup v2 w refs
TRANSCRIPT

1
HCT Nonbranded Speaker Training Sample Show Deck Functional Test Only Hotel TBA Dallas, Texas February 1, 2013

2
Access to Health Care Is Defined as Receiving Timely Cost-Effective Health Care
Definition • Cost-effective, appropriate
health care to achieve best possible outcome
• Timely performance of health care services
• Influenced by health care providers (HCPs), patients, and health care systems
Goal • Optimal health outcomes
Joshua TV, et al. Cancer. 2010;116(14):3469-3476.
© iStockphoto.com / sjlocke.
3
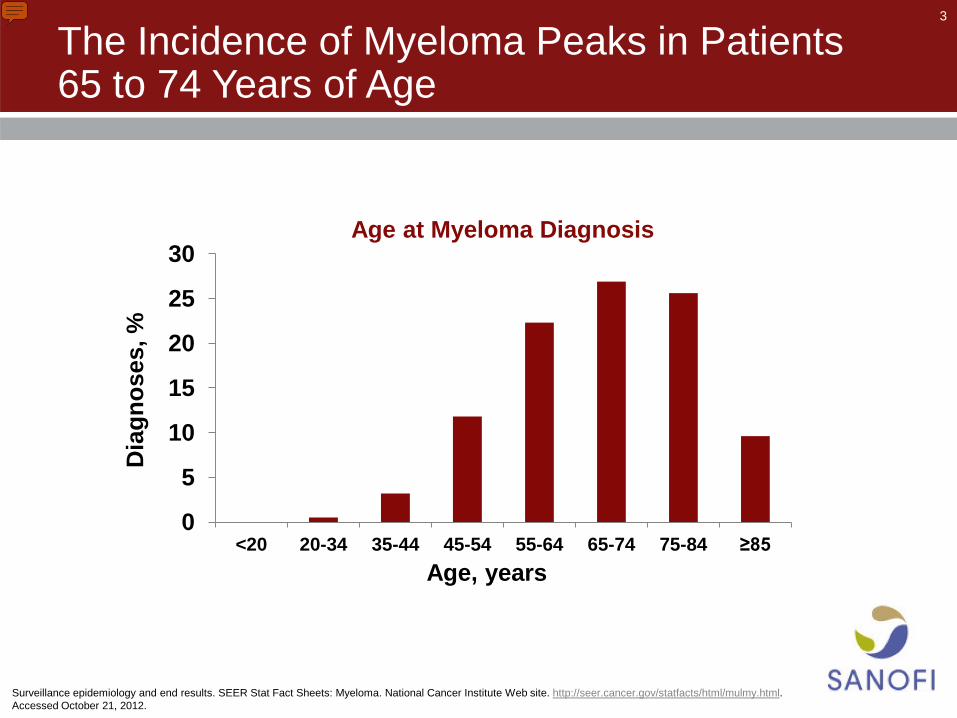
The Incidence of Myeloma Peaks in Patients 65 to 74 Years of Age
0
5
10
15
20
25
30
<20 20-34 35-44 45-54 55-64 65-74 75-84 ≥85
Dia
gnos
es, %
Age at Myeloma Diagnosis
Age, years
Surveillance epidemiology and end results. SEER Stat Fact Sheets: Myeloma. National Cancer Institute Web site. http://seer.cancer.gov/statfacts/html/mulmy.html. Accessed October 21, 2012.

4
Several Reasons for Limited Access to HCT Among Elderly Patients With MM Have Been Proposed
• Possible reasons for discrepancy – Patients ≥65 years historically not candidates for HCT1
– Elderly patients excluded from clinical trials2
– Comorbidity3
– Patient preference3
“Advanced age alone should not preclude the use of effective cancer treatment that could improve quality of
life or extend meaningful survival.”4 ‒NCCN Guidelines for Senior Adult Oncology
1. Palumbo A, Gay F. Hematology Am Soc Hematol Educ Program. 2009:566-577. 2. Kumar SK, et al. Am J Hematol. 2008;83(8):614-617. 3. Majhail NS, et al. Biol Blood Marrow Transplant. 2010;16(8):1070-1075. 4. National Comprehensive Cancer Network. NCCN Clinical Practice Guidelines in Oncology: Senior Adult Oncology. v2.2012.

5
© 2013 sanofi-aventis U.S. LLC, a Sanofi company US.PLE.12.12.001

Access to Hematopoietic Stem CellTransplantationEffect of Race and Sex
Thomas V. Joshua, MS1; J. Douglas Rizzo, MD, MS2; Mei-Jie Zhang, PhD3; Parameswaran N. Hari, MD, MS2;
Seira Kurian, MD, MS, MPH4; Marcelo Pasquini, MD, MS2; Navneet S. Majhail, MD, MS5;
Stephanie J. Lee, MD, MPH6; and Mary M. Horowitz, MD, MS2
BACKGROUND: The purpose of the current study was to determine whether the use of hematopoietic stem cell
transplantation (HCT) to treat leukemia, lymphoma, or multiple myeloma (MM) differs by race and sex. METHODS:
The annual incidence of leukemia, lymphoma, and MM was estimated in the United States in people aged <70 years
by race and sex using the Surveillance, Epidemiology, and End Results (SEER) cancer registry between 1997 and
2002 and US census reports for the year 2000. The annual incidence of autologous, human leukocyte antigen (HLA)
identical sibling, and unrelated HCT performed in these groups was estimated using Center for International Blood
and Marrow Transplant Research data from 1997 through 2002. Logistic regression analysis was used to calculate the
age-adjusted odds ratio (OR) of receiving HCT for Caucasians versus African Americans and for men versus women.
RESULTS: The likelihood of undergoing HCT was found to be higher for Caucasians than for African Americans (OR,
1.40; 95% confidence interval [95% CI], 1.34-1.46). This difference existed for each type of HCT: autologous (OR, 1.24;
95% CI, 1.19-1.30), HLA identical sibling (OR, 1.59; 95% CI, 1.46-1.74), and unrelated donor (OR, 2.02; 95% CI, 1.75-2.33).
Overall, men were more likely than women to receive HCT (OR, 1.07; 95% CI, 1.05-1.1 [P < .0001]); however, this differ-
ence was found to be significant only for autologous HCT (OR, 1.10; 95% CI, 1.07-1.13 [P < .0001]). CONCLUSIONS:
HCT is more frequently used to treat leukemia, lymphoma, and MM in Caucasians than in African American individu-
als. African Americans have lower rates of both autologous and allogeneic HCT, indicating that donor availability can-
not fully explain the differences. Women are less likely than men to receive autologous HCT for reasons unexplained
by age or disease status. Cancer 2010;116:3469–76. VC 2010 American Cancer Society.
KEYWORDS: access to care, hematopoietic stem cell transplantation, effect of race and sex, leukemia, lymphoma.
Hematopoietic stem cell transplantation (HCT) is a relatively new treatment modality. Its history began in thelate 1940s and early 1950s, when animal studies revealed the ability of donor bone marrow to restore hematopoiesis afterirradiation.1 The first successful HCTs in humans were performed in 1968.2-4 Procedure volume has increased rapidlyover the last few decades, with approximately 60,000 transplants performed worldwide in 2006.4 Although HCT has thepotential to increase survival for patients with many diseases, particularly hematologic malignancies, it is an intensive,costly, and technically sophisticated procedure with a substantial risk of early morbidity and mortality.
Access to healthcare is defined as using affordable personal health services in a timely manner to achieve the besthealth outcomes possible.5 The process of gaining access to care includes dynamic interactions between individuals withdiverse ethnic, cultural, and socioeconomic backgrounds; healthcare providers operating in a variety of practice patternswith external constraints; and healthcare systems.6 HCT is an important treatment option for patients with leukemia,lymphoma, and related disorders, offering the best chance for cure in several clinical situations.4,7,8 Limitations in accessto this procedure have substantial clinical, ethical, and policy implications.
DOI: 10.1002/cncr.25297, Received: November 10, 2009; Revised: January 20, 2010; Accepted: January 29, 2010, Published online May 24, 2010 in Wiley Inter-
Science (www.interscience.wiley.com)
Corresponding author: Thomas V. Joshua, MS, Center for Nursing Research, School of Nursing, Medical College of Georgia, 987 St. Sebastian Way, EC-4410,
Augusta, GA 30912; Fax: (706) 721-7049; [email protected]
1Center for Nursing Research, School of Nursing, Medical College of Georgia, Augusta, Georgia; 2Center for International Blood and Marrow Transplant Research,
Medical College of Wisconsin, Milwaukee, Wisconsin; 3Department of Biostatistics, Medical College of Wisconsin, Milwaukee, Wisconsin; 4Los Angeles County
Department of Public Health, Los Angeles, California; 5Department of Hematology/Oncology, University of Minnesota, Minneapolis, Minnesota; 6Department of
Hematology/Oncology, Fred Hutchinson Cancer Center, Seattle, Washington
Cancer July 15, 2010 3469
Original Article

Considerable variation exists in the distribution ofhealth and healthcare in the United States. In 2002, theInstitute ofMedicine published an authoritative report indi-cating that minorities are less likely than whites to receiveneeded routine and complex healthcare services across abroad array of diseases including cancer, cardiovascular dis-ease, human immunodeficiency virus (HIV)/acquired im-munodeficiency syndrome (AIDS), diabetes, and mentalillness.9 Since that report, the Agency for HealthcareResearch and Quality has published an annual NationalHealthcare Disparities Report (NHDR) to provide an over-view of disparities in healthcare among racial, ethnic, andsocioeconomic groups in the United States, and to trackprogress in reducing disparities.10 The 2006 NHDR sug-gested that disparities remain prevalent between men andwomen and among racial groups, including disparities incancer care.11 Several studies have indicated that menreceive more early cancer detection tests than women in thesame practices,5,12,13 and cancer treatment outcomes arepoorer in African Americans.9-14 Outcome disparities maybe correlated with more advanced stage of disease at thetime of diagnosis, a phenomenon believed to be primarilybecause of the underutilization of cancer screening. Somestudies have suggested that lower socioeconomic statusresulting in reduced access to healthcare may be a major ex-planation for racial differences in cancer mortality.15-25
The purpose of the current study was to determinewhether the use of HCT to treat leukemia, lymphoma, ormultiple myeloma (MM) differs by race and sex. Wehypothesized that women and African Americans with thesediseases are less likely to receive HCT. Although there maybe regional differences in healthcare availability,26 this studyexamined utilization rates for the country as a whole.
MATERIALS AND METHODSThe Center for International Blood and Marrow Trans-plant Research (CIBMTR) database was used to estimatethe annual number of HCTs performed in the UnitedStates between 1997 and 2002. Data from the Surveil-lance, Epidemiology, and End Results (SEER)27,28 data-base and the US Census Bureau29 were used to estimatethe annual total number of new cases of each disease inthe US population in the same time period. By using thesedata, we estimated the rates (number of transplantations/number of patients with disease) of HCT performed forleukemia, lymphoma, andMM between 1997 and 2002.
The CIBMTR is a research program formed in July2004 through an affiliation of the International Bone Mar-row Transplant Registry and Autologous Blood andMarrow
Transplant Registry of the Medical College of Wisconsinand the National Marrow Donor Program (NMDP). TheCIBMTR is a voluntary consortium involving >500 trans-plant centers in 54 countries. These transplant centers world-wide contribute data regarding consecutive allogeneic andautologous HCTs to the CIBMTR. Participating centers arerequired to report all transplants consecutively and compli-ance is monitored through on-site audits. Computerizedchecks for errors, physician review of submitted data, andon-site audits of participating centers ensure the quality ofthe data. Patients are followed longitudinally, with yearly fol-low-up. The NMDP facilitates approximately 95% of allunrelated donorHCTs in the United States.
The SEER program of the National Cancer Insti-tute27,28 is an authoritative source of information regard-ing cancer incidence and survival in the United States.The SEER program collects and publishes cancer inci-dence and survival data from 14 population-based cancerregistries and 3 supplemental registries covering approxi-mately 26% of the US population.
Study Population
The population considered for this study included USpatients aged <70 years with acute lymphoblastic leuke-mia (ALL), acute myelogenous leukemia (AML), chronicmyelogenous leukemia (CML), non-Hodgkin lymphoma(NHL), and MM who were treated between 1997 and2002; these are the most common disease indications forHCT. Patients aged >70 years were not consideredbecause few transplants are performed in older patients.
Statistical Analysis
We calculated the annual number of incident cases ofALL, AML, CML, NHL, and MM per 100,000 personsbased on the SEER population sampling frame between1997 and 2002. First, incidence estimates were calculatedfrom the SEER database separately for age group (agesbirth-19 years, 20-29 years, 30-39 years, 40-49 years,50-59 years, and 60-69 years), race (African Americanand Caucasian), and sex. This incidence rate was thenapplied to US Census Bureau (year 2000) estimates fornumbers of persons in similar age, sex, and racial groupsto derive an estimated annual number of patients witheach disease in the US. The estimated annual numbers ofautologous, human leukocyte antigen (HLA) identicalsibling, and unrelated donor HCTs performed during thesame time period, and for each sex, racial, and age group,were calculated by retrieving the number of transplantsregistered with the CIBMTR between 1997 and 2002.
Original Article
3470 Cancer July 15, 2010

During this period, the CIBMTR collected an estimated55% of autologous, 50% of HLA identical sibling, and>90% of unrelated donor HCTs performed in the US(estimation is described in more detail elsewhere).30,31
Consequently, we applied an adjustment factor of1.8 and 2.0, respectively, to the reported numbers of auto-logous and HLA identical sibling HCTs.
We then evaluated the rates of all HCTs as well asautologous, HLA identical sibling, and unrelated donorHCTs by race and sex, for all diagnoses, and for each dis-ease separately using logistic regression analysis adjustingfor age. The rates of HCTs were calculated by dividingthe number of estimated procedures by the number ofpatients diagnosed with disease in the same age range.When multiple comparisons were made, the P value ofsignificance was considered to be �.001 using Bonferroniadjustment.
In these analyses, we assumed that the sample ofpatients reported to the CIBMTR was representative ofthe total US population of HCT recipients. A sensitivityanalysis was performed to assess the potential effect ofselective under-reporting of HCT for African Americanson the results of this study. In the initial analysis, weassumed that 55% of all autologous HCTs and 50% of allallogeneic HCTs performed in the United States werereported to CIBMTR, regardless of patient race. Data werereanalyzed after increasing the number of autologous andHLA identical sibling transplants for African Americansreported to the CIBMTR by 5%, 10%, 15%, and 20%.
RESULTSA total of 27,725 patients registered with the CIBMTRmet our selection criteria. Of these, 15,363 (55%) under-went autologous HCT, 5731 (21%) underwent HLAidentical sibling HCT, and 6631 (24%) underwent unre-lated donor HCT. There were 25,068 (90%) patientsclassified as Caucasian and 2657 (10%) classified as Afri-can American. Approximately 59% were males. Pediatricpatients represented only 10% of patients who underwenttransplantation and among those, 81% of the transplantswere for acute leukemia (AML and ALL). General charac-teristics of the HCT population are presented in Table 1.By using these data and the adjustment factors describedearlier, we estimated that there were approximately45,750 HCTs performed for the eligible diseases duringthe study period. During the same period of time, therewere an estimated 273,853 patients diagnosed in the USwith the diseases considered in this analysis.
Effect of Race
Overall effect of race
Compared with African Americans, the age-adjustedodds ratio (OR) of undergoing any type of HCT for alldiseases considered was higher for Caucasians (OR, 1.40;95% confidence interval [95% CI], 1.35-1.46 [P <
.0001]). A significantly higher OR of receiving HCT wasnoted for each type of HCT: autologous (OR, 1.24; 95%CI, 1.19-1.30 [P < .0001]), HLA identical sibling (OR,1.59; 95% CI, 1.46-1.74 [P < .0001]), and unrelated do-nor (OR, 2.02; 95%CI, 1.75-2.33 [P< .0001]) (Table 2).
Table 1. Characteristics of HCT Patients
Variables CaucasianNo. (%)Evaluable
AfricanAmerican No.(%) Evaluable
Total(%)
No. of patients 25,068 (90) 2657 (10) 27,725
SexMale 14,807 (59) 1443 (54) 16,250 (59)
Female 10,261 (41) 1214 (46) 11,475 (41)
Year of transplant1997 3319 (13) 289 (11) 3608 (13)
1998 3916 (16) 403 (15) 4319 (16)
1999 4236 (17) 468 (18) 4704 (17)
2000 4427 (18) 463 (17) 4890 (18)
2001 4466 (18) 510 (19) 4976 (18)
2002 4704 (19) 524 (20) 5228 (19)
Age group at transplant, yBirth-19 2282 (9) 370 (14) 2652 (10)
20-29 1956 (8) 206 (8) 2162 (8)
30-39 3261 (13) 406 (15) 3667 (13)
40-49 5915 (24) 652 (25) 6567 (24)
50-59 7491 (30) 684 (26) 8175 (29)
60-69 4163 (17) 339 (13) 4502 (16)
Donor typeAuto HCT 13,758 (55) 1605 (60) 15,363 (55)
HLA sibling HCT 5230 (21) 501 (19) 5731 (21)
Unrelated HCT 6080 (24) 551 (21) 6631 (24)
DiseaseAML 5247 (21) 458 (17) 5705 (21)
ALL 2340 (9) 245 (9) 2585 (9)
CML 2824 (11) 341 (13) 3165 (11)
NHL 8936 (36) 546 (21) 9482 (34)
MM 5721 (23) 1067 (40) 6788 (24)
Graft typeBone marrow 7544 (30) 635 (24) 8179 (30)
Peripheral blood 16,985 (68) 1895 (71) 18,880 (68)
Cord blood 539 (2) 127 (5) 666 (2)
HCT indicates hematopoietic stem cell transplantation; Auto HCT, autolo-
gous HCT; HLA sibling HCT, human leukocyte antigen identical sibling HCT;
AML, acute myelogenous leukemia; ALL, acute lymphoblastic leukemia;
CML, chronic myelogenous leukemia; NHL, non-Hodgkin lymphoma; MM:
multiple myeloma.
Access to HCT: Effect of Race and Sex/Joshua et al
Cancer July 15, 2010 3471

Sensitivity analyses suggested that the results of this studywere robust, even in the conditional setting of 20%under-reporting of HCTs in African Americans (OR,1.15; 95% CI, 1.10-1.20). There were some differencesobserved by disease.
Effect of race by disease and type of HCT
The OR of undergoing HCT for MM was higherfor Caucasians than for African Americans (OR, 1.75;95% CI, 1.64-1.86 [P < .0001]) (Table 2). This differ-ence was observed for autologous HCT (OR, 1.72; 95%CI, 1.62-1.83 [P < .0001]), HLA identical sibling HCT(OR, 1.55; 95% CI, 1.21-1.98 [P¼ .0006]), and unre-lated donor HCT (OR, 3.24; 95% CI, 1.24-8.50[P¼ .016]). The OR of undergoing HCT for NHL washigher for Caucasians than for African Americans (OR,2.12; 95% CI, 1.95-2.29 [P < .0001]). This differencewas noted for autologous HCT (OR, 2.03; 95%CI, 1.86-2.22 [P < .0001]), HLA identical sibling HCT (OR,
2.23; 95% CI, 1.89-2.79 [P< .0001]), and unrelated do-nor HCT (OR, 3.14; 95% CI, 1.79-5.53 [P < .0001]).The OR of undergoing HCT for CML was higher forCaucasians than for African Americans (OR, 1.42; 95%CI, 1.23-1.64 [P< .0001]). This difference was noted forHLA identical sibling HCT (OR, 1.25; 95% CI, 1.05-1.49 [P¼ .01]) and unrelated donor HCT (OR, 1.45;95% CI, 1.16-1.81 [P¼ .001]). Few patients (n¼ 22)received autologous HCT. The OR of undergoing HCTfor AML was higher for Caucasians than for AfricanAmericans (OR, 1.52; 95% CI, 1.35-1.71 [P < .0001]).This difference was noted for HLA identical sibling HCT(OR, 1.44; 95% CI, 1.23-1.69 [P < .0001]) and unre-lated donor HCT (OR, 2.29; 95% CI, 1.74-3.02 [P <
.0001]), but not for autologous HCT (OR, 1.08; 95%CI, 0.90-1.3). There was no difference noted with regardto the OR of undergoing HCT for ALL between Cauca-sians and African Americans (OR, 1.01; 95% CI, 0.81-1.25 [P¼ .97]).
Table 2. Age-Adjusted OR of Receiving HCT by Race and Sex
HCT Types andORs CaucasiansVersus AfricanAmericans
HCT Types andORs Males Versus
Females
EstimatedAnnual USIncidence
EstimatedAnnual HCTsin the US
TransplantTypes
OR (95% CI) P OR (95% CI) P
All diseases 45,643 7623 Overall HCT 1.40 (1.35-1.46) <.0001 1.07 (1.05-1.1) <.0001
4608 Autologous HCT 1.24 (1.19-1.30) <.0001 1.10 (1.06-1.13) <.0001
1910 HLA identical sibling HCT 1.59 (1.46-1.74) <.0001 1.05 (0.99-1.10) .063
1105 Unrelated donor HCT 2.02 (1.75-2.33) <.0001 0.94 (0.88-1.01) .11
ALL 3508 580 Overall HCT 1.01 (0.81-1.25) .97 1.08 (0.96-1.21) .21
40 Autologous HCT 0.74 (0.42-1.28) .28 0.7 (0.49-0.98) .04
262 HLA identical sibling HCT 0.93 (0.69-1.24) .61 1.17 (0.99-1.38) .06
278 Unrelated donor HCT 1.23 (0.87-1.73) .24 1.08 (0.90-1.28) .42
AML 5032 1459 Overall HCT 1.52 (1.35-1.71) <.0001 0.83 (0.78-0.88) <.0001
363 Autologous HCT 1.08 (0.90-1.3) .40 0.77 (0.69-0.85) <.0001
694 HLA identical sibling HCT 1.44 (1.23-1.69) <.0001 0.91 (0.83-0.99) .021
402 Unrelated donor HCT 2.29 (1.74-3.02) <.0001 0.87 (0.77-0.98) .017
CML 2231 744 Overall HCT 1.42 (1.23-1.64) <.0001 0.90 (0.82-0.98) .018
22 Autologous HCT 2.36 (0.99-5.64) .05 1.17 (0.77-1.78) .46
413 HLA identical sibling HCT 1.25 (1.05-1.49) .01 0.89 (0.80-0.99) .041
309 Unrelated donor HCT 1.45 (1.16-1.81) .001 0.92 (0.81-1.05) .21
NHL 27,960 2804 Overall HCT 2.12 (1.95-2.29) <.0001 1.22 (1.17-1.26) <.0001
2273 Autologous HCT 2.03 (1.86-2.22) <.0001 1.18 (1.13-1.23) <.0001
428 HLA identical sibling HCT 2.23 (1.89-2.79) <.0001 1.45 (1.31-1.60) <.0001
103 Unrelated donor HCT 3.14 (1.79-5.53) <.0001 1.03 (0.84-1.27) .77
MM 6912 2036 Overall HCT 1.75 (1.64-1.86) <.0001 1.1 (1.05-1.15) <.0001
1910 Autologous HCT 1.72 (1.62-1.83) <.0001 1.1 (1.05-1.15) .0001
113 HLA identical sibling HCT 1.55 (1.21-1.98) .0006 1.03 (0.86-1.23) .77
13 Unrelated donor HCT 3.24 (1.24-8.50) .016 1.64 (0.94-2.86) .08
OR indicates odds ratio; HCT, hematopoietic stem cell transplant; 95% CI, 95% confidence interval; HLA, human leukocyte antigen; ALL, acute lymphoblastic
leukemia; AML, acute myelogenous leukemia; CML, chronic myelogenous leukemia; NHL, non-Hodgkin lymphoma; MM, multiple myeloma.
Original Article
3472 Cancer July 15, 2010

Effect of Sex
Overall effect of sex
Overall, men were more likely than women toreceive HCT (OR, 1.07; 95% CI, 1.05-1.1 [P< .0001]).This difference was significant for autologous HCT (OR,1.10; 95% CI, 1.06-1.13 [P < .0001]) but not for HLAidentical sibling (OR, 1.05; 95%CI, 0.99-1.10 [P¼ .06])or unrelated donor HCT (OR, 0.94; 95% CI, 0.88-1.01[P¼ .11]), and there were significant differences by dis-ease. In particular, men were more likely than women toundergo autologous HCT for MM or NHL.
Effect of sex by disease and type of HCT
The OR of undergoing HCT for AML was lowerfor males than females; this difference was significant inall transplant types (Table 2). The OR of undergoingHCT for CML was lower for males than females; this dif-ference was significant for HLA identical sibling HCTbut not for autologous or unrelated donor HCT. The ORof undergoing HCT for NHL was higher for males thanfor females; this difference was significant for autologousand HLA identical sibling HCT but not for unrelated do-nor HCT. The OR of undergoing HCT for MM washigher for males than females; this difference was signifi-cant for autologous but not for HLA identical sibling orunrelated donor HCT. There was no difference noted inthe OR of undergoing HCT for ALL between males andfemales.
Affect of Adult Versus Pediatric Age Group
There were 2652 patients aged<20 years who were regis-tered with the CIBMTR and met our selection criteria inthe study period. The majority of these children had AMLor ALL. We estimated that there were approximately2955 HCTs performed for the eligible diseases during thestudy period. During the same period of time, there werean estimated 18,595 patients aged<20 years diagnosed inthe United States with the diseases considered in this anal-ysis. There were no significant differences by race and sexto report (data not shown) for this age group.
Interaction of Sex and Race
We tested for interactions between sex and race by com-paring the overall and disease-specific OR of undergoingHCT in males versus females adjusting for race, and bycomparing the odds of HCT in Caucasians versus AfricanAmericans, adjusting for sex. No significant interactionswere evident.
DISCUSSIONDecision-making regarding the performance of HCTinvolves a complex interplay of factors. In general, catego-ries of factors that may explain disparities in applied ther-apy include biologic factors (intrinsic variability in diseasenatural history or response to therapy), patient factors(presence of comorbidities that prevent application oftherapy and patient preferences), healthcare systems fac-tors (health insurance and availability of healthcare facili-ties), and care process or discrimination factors (providerattitudes such as bias against minorities, greater clinicaluncertainty when understanding minorities’ symptomsand severity, or preconceived beliefs regarding minoritybehavior or health). Ideally, clinical needs and appropri-ateness, biologic factors, and patient preferences shouldbe the only considerations driving the therapeutic deci-sion-making process. We assume that patient-related(other than preferences) and disease-related clinical factorsdo not vary by race and sex such that indications for HCTare not dramatically different in different racial and sexgroups. We believe this is a reasonable assumption basedon what is known about the diseases included in theseanalyses. The findings of the current study suggest a dis-parity in the rates of autologous and allogeneic HCT forAfrican Americans and females that should cause concern,with the greatest disparity observed based on race. Therates of HCT were higher in Caucasians than in AfricanAmericans in nearly all subgroups examined, with ORs>2 in some categories.
Disparity in care could represent either underutiliza-tion in African Americans or overutilization in Cauca-sians. It could also be attributed to biologic differences.For example, the greater distribution of HLA types inAfrican Americans and the smaller number of AfricanAmericans in volunteer donor registries make it more dif-ficult to find suitably matched donors for African Ameri-cans in need of unrelated donor HCT. This maycontribute to the lower rate of unrelated donor HCTsnoted in this group. However, MM is a common indica-tion for HCT. The preferred type of HCT for this diseaseis autologous, and during the 5-year time period spannedby the current study, it became the most common indica-tion for autologous HCT.31 MM is twice as common inAfrican Americans compared with Caucasians, but theORs of undergoing HCT for MM were found to be 72%higher for Caucasians. These lower rates of autologousHCT suggest that the disparity is best explained by under-utilization of HCT in African Americans and cannot bewholly attributed to donor availability.
Access to HCT: Effect of Race and Sex/Joshua et al
Cancer July 15, 2010 3473

The disparity in the use of HCT in men comparedwith women is less consistent than the disparity in use byrace, with ORs closer to 1 and an increased OR noted inmen for some diseases and in women for others. A unify-ing hypothesis for these differences is difficult to devise.
There were no significant differences in access toHCT for children noted based on sex or race. The lack ofdifferential access to HCT for children compared withadults may be attributed, in part, to better governmental(including state gap programs) and private insurance forchildren compared with adults. In addition, a larger per-centage of children, particularly those with acute leuke-mia, are referred early in their treatment course to largerpediatric medical centers and are treated on cooperativegroup trials, which may be more likely to afford themaccess to HCT.
Limitations
Several limitations of the current study should be consid-ered. This analysis takes a national perspective in consid-ering racial disparities in HCT. The CIBMTR collecteddata on approximately 55% of all autologous transplantsand 50% of related donor transplants performed annuallyin the United States during the time period included inthe current study. Although regional differences may be ofgreater interest because referral for HCT generally occurson a local/regional basis, the nature of the SEER andCIBMTR databases preclude subanalyses to present re-gional differences in HCT. It is also possible that centersthat perform more related donor or autologous HCTs inAfrican American individuals are under-represented inthe CIBMTR. We addressed this incomplete denomina-tor of transplant activity in the United States by perform-ing sensitivity analysis, the results of which suggested thatour conclusions were robust up to a moderate (20%) levelof under-reporting for specific racial groups. Because theCIBMTR captures data regarding nearly all unrelated do-nor transplants in the United States, potential biases inreporting are not an issue for that type of HCT and, infact, disparities in utilization were found to be highest forunrelated donor HCT.
An additional consideration is that attribution ofpatient race in the CIBMTR observational database isprovided by the transplant centers. Centers may not usehomogenous processes to identify and report the race ofHCT recipients; these designations may not match self-reported race and may contribute to reporting bias. How-ever, it appears likely that reporting of race within theSEER database during the same time period would be
subject to very similar biases, given the similarities inreporting methods between the 2 databases. If individualsfrom a particular race were systematically misclassified inany of these databases, it may misrepresent the true accessrate for that particular race.
We assumed that family size, and therefore the num-ber of potential sibling donors, was equal between Afri-can-American and Caucasian populations. Because theCIBMTR only collects data regarding HCT recipients,we were unable to explore whether differences existbetween sex and racial groups with regard to rates of refer-ral for consideration of HCT. Biologic-based racial differ-ences in clinical presentation or response to initial therapyfor disease may represent a partial explanation for the dis-parity in HCT rates. Unfortunately, we did not have suffi-cient data regarding disease status at the time of diagnosisor comorbidities to determine whether this may haveaffected consideration of HCT as a treatment option.Although for the purposes of these analyses we haveassumed that the clinical appropriateness of HCT is simi-lar across the groups studied as described above, otherstudies have suggested that African Americans aremore likely to be diagnosed with an advanced stage of dis-ease than whites, which would make them more likely tobe candidates for aggressive therapy.32-34 However, iftrue, such differences in stage at diagnosis should serve toincrease, not decrease, the ORs of HCT being performedamong African Americans compared with Caucasians.
To the best of our knowledge, no data are currentlyavailable regarding patient preferences for treatment, ratesof refusal of HCT, or other sociocultural factors thatcould explain the differences in HCT observed in the cur-rent study. Finally, there were insufficient data regardinghealthcare process factors such as referring provider andtransplant physician characteristics and practice patterns,geographic referral patterns, transplant center characteris-tics, or socioeconomic characteristics of the patient to beincorporated into these analyses.
Conclusions
We observed a difference in the utilization of HCT forleukemia, lymphoma, and MM by race, with Caucasiansmore likely to receive HCT than African Americans.Importantly, lower HCT rates for African Americanswere noted for autologous HCT, indicating that donoravailability cannot fully explain the differences observed.Differences by sex were less striking. We believe these dif-ferences represent substantial underutilization of HCT inAfrican Americans. The identification of disparities
Original Article
3474 Cancer July 15, 2010

should serve as the motivation to further understand theircause, and their elimination whenever they are inappro-priate. Further study is essential to better characterize andexplain disparities in access to HCT. Research shouldexplore whether patient or provider preferences, sociocul-tural or socioeconomic factors, or healthcare process fac-tors explain disparities in access to HCT, and whetherthese factors are modifiable. While waiting for furtherresearch to better understand disparate access to HCT,the medical community should work at all levels to elimi-nate these disparities.
CONFLICT OF INTEREST DISCLOSURESThe Center for International Blood and Marrow TransplantResearch (CIBMTR) is supported by Public Health ServiceGrant/Cooperative Agreement U24-CA76518 from theNational Cancer Institute (NCI); the National Heart, Lungand Blood Institute (NHLBI); and the National Institute ofAllergy and Infectious Diseases (NIAID); a Grant/CooperativeAgreement 5U01HL069294 from NHLBI and NCI; contractHHSH234200637015C with the Health Resources and ServicesAdministration (HRSA/DHHS); and 2 grants (N00014-06-1-0704 and N00014-08-1-0058) from the Office of NavalResearch, as well as grants from AABB; Aetna; American Societyfor Blood and Marrow Transplantation; Amgen, Inc; an anony-mous donation to the Medical College of Wisconsin; AstellasPharma US, Inc; Baxter International, Inc; Bayer HealthCarePharmaceuticals; Be the Match Foundation; Biogen IDEC; Bio-Marin Pharmaceutical, Inc; Biovitrum AB; BloodCenter of Wis-consin; Blue Cross and Blue Shield Association; Bone MarrowFoundation; Canadian Blood and Marrow Transplant Group;CaridianBCT; Celgene Corporation; CellGenix, GmbH; Centersfor Disease Control and Prevention; Children’s LeukemiaResearch Association; ClinImmune Labs; CTI Clinical Trial andConsulting Services; Cubist Pharmaceuticals; Cylex Inc; Cyto-Therm; DOR BioPharma, Inc; Dynal Biotech, an InvitrogenCompany; Eisai, Inc; Enzon Pharmaceuticals, Inc; EuropeanGroup for Blood and Marrow Transplantation; Gamida Cell,Ltd; GE Healthcare; Genentech, Inc; Genzyme Corporation;Histogenetics, Inc; HKS Medical Information Systems; Hospira,Inc; Infectious Diseases Society of America; Kiadis Pharma;Kirin Brewery Co., Ltd; The Leukemia and Lymphoma Society;Merck & Company; The Medical College of Wisconsin; MGIPharma, Inc; Michigan Community Blood Centers; MillenniumPharmaceuticals, Inc; Miller Pharmacal Group; Milliman USA,Inc; Miltenyi Biotec, Inc; National Marrow Donor Program;Nature Publishing Group; New York Blood Center; NovartisOncology; Oncology Nursing Society; Osiris Therapeutics, Inc;Otsuka America Pharmaceutical, Inc; Pall Life Sciences; PfizerInc; Saladax Biomedical, Inc; Schering Corporation; Society forHealthcare Epidemiology of America; StemCyte, Inc; StemSoftSoftware, Inc; Sysmex America, Inc; Teva Pharmaceutical Indus-tries; THERAKOS, Inc; Thermogenesis Corporation; VidacareCorporation; Vion Pharmaceuticals, Inc; ViraCor Laboratories;ViroPharma, Inc; and Wellpoint, Inc. The views expressed inthis article do not reflect the official policy or position of theNational Institute of Health, the Department of the Navy, theDepartment of Defense, or any other agency of the USGovernment.
REFERENCES
1. Serna DS, Lee SJ, Zhang MJ, et al. Trends in survival ratesafter allogeneic hematopoietic stem-cell transplantation foracute and chronic leukemia by ethnicity in the United Statesand Canada. J Clin Oncol. 2003;21:3754-3760.
2. Bach FH, Albertini RJ, Joo P, Anderson JL, Bortin MM.Bone-marrow transplantation in a patient with the Wiskott-Aldrich syndrome. Lancet. 1968;2:1364-1366.
3. Gatti RA, Meuwissen HJ, Allen HD, Hong R, Good RA.Immunological reconstitution of sex-linked lymphopenicimmunological deficiency. Lancet. 1968;2:1366-1369.
4. Center for International Blood and Marrow TransplantResearch. CIBMTR Progress Report: January-December2007. Milwaukee, WI: Center for International Blood andMarrow Transplant Research; 2007:5.
5. Mandelblatt JS, Yabroff KR, Kerner JF. Equitable access tocancer services: a review of barriers to quality care. Cancer.1999;86:2378-2390.
6. Mitchell JM, Meehan KR, Kong J, Schulman KA. Access tobone marrow transplantation for leukemia and lymphoma:the role of sociodemographic factors. J Clin Oncol.1997;15:2644-2651.
7. Copelan EA. Hematopoietic stem-cell transplantation. NEngl J Med. 2006;354:1813-1826.
8. Lennard AL, Jackson GH. Stem cell transplantation. BMJ.2000;321:433-437.
9. Smedley BD, Stith AY, Nelson AR. Unequal Treatment:Confronting Racial and Ethnic Disparities in Health Care.Washington, DC: National Academies Press; 2003.
10. Agency for Healthcare Research and Quality. NationalHealthcare Disparities Report. Rockville, MD: Agency forHealthcare Research and Quality; 2006.
11. Long JA, Chang VW, Ibrahim SA, Asch DA. Update onthe health disparities literature. Ann Intern Med. 2004;141:805-812.
12. Shavers VL, Harlan LC, Stevens JL. Racial/ethnic variationin clinical presentation, treatment, and survival amongbreast cancer patients under age 35. Cancer. 2003;97:134-147.
13. Demark-Wahnefried W, Strigo T, Catoe K, et al. Knowl-edge, beliefs, and prior screening behavior among blacksand whites reporting for prostate cancer screening. Urology.1995;46:346-351.
14. Robinson KD, Kimmel EA, Yasko JM. Reaching out to theAfrican American community through innovative strategies.Oncol Nurs Forum. 1995;22:1383-1391.
15. Vernon SW, Heckel V, Jackson GL. Medical outcomes ofcare for breast cancer among health maintenance organiza-tion and fee-for-service patients. Clin Cancer Res. 1995;1:179-184.
16. Zaloznik AJ. Breast cancer stage at diagnosis: Caucasiansversus Afro-Americans. Breast Cancer Res Treat. 1995;34:195-198.
17. Mehta P, Pollock BH, Nugent M, Horowitz M, WingardJR. Access to stem cell transplantation: do women fare aswell as men? Am J Hematol. 2003;72:99-102.
18. Liu JR, Conaway M, Rodriguez GC, Soper JT, Clarke-Pear-son DL, Berchuck A. Relationship between race and intervalto treatment in endometrial cancer. Obstet Gynecol. 1995;86(4 pt 1):486-490.
19. Schapira MM, McAuliffe TL, Nattinger AB. Treatment oflocalized prostate cancer in African-American compared
Access to HCT: Effect of Race and Sex/Joshua et al
Cancer July 15, 2010 3475
with Caucasian men. Less use of aggressive therapy for com-parable disease. Med Care. 1995;33:1079-1088.
20. King TE Jr, Brunetta P. Racial disparity in rates of surgeryfor lung cancer. N Engl J Med. 1999;341:1231-1233.
21. Bach PB, Schrag D, Brawley OW, Galaznik A, Yakren S,Begg CB. Survival of blacks and whites after a cancer diag-nosis. JAMA. 2002;287:2106-2113.
22. Demark-Wahnefried W, Schildkraut JM, Iselin CE, et al.Treatment options, selection, and satisfaction among AfricanAmerican and white men with prostate carcinoma in NorthCarolina. Cancer. 1998;83:320-330.
23. Espey D, Paisano R, Cobb N. Regional patterns and trendsin cancer mortality among American Indians and AlaskaNatives, 1990-2001. Cancer. 2005;103:1045-1053.
24. Du W, Simon MS. Racial disparities in treatment and sur-vival of women with stage I-III breast cancer at a large aca-demic medical center in metropolitan Detroit. Breast CancerRes Treat. 2005;91:243-248.
25. Shavers VL, Brown ML. Racial and ethnic disparities in thereceipt of cancer treatment. J Natl Cancer Inst. 2002;94:334-357.
26. Asch DA, Armstrong K. Aggregating and partitioning popu-lations in health care disparities research: differences in per-spective. J Clin Oncol. 2007;25:2117-2121.
27. Surveillance, Epidemiology, and End Results (SEER) Pro-gram. Cancer incidence and survival among children andadolescents: United States SEER Program 1975-1995. In:Ries LAG, Gurney JG, Linet M, Tamra T, Young JL,Bunin GR, eds. NIH Pub. No 99-4649. Bethesda, MD:National Cancer Institute; 1999.
28. Surveillance, Epidemiology, and End Results (SEER) Pro-gram. SEER*Stat (6.4) Database: Incidence-SEER 9 Regs
Public-Use, Nov 2004 Sub (1973-2002). Bethesda, MD:National Cancer Institute, Division of Cancer Controland Population Sciences, Surveillance Research Program,Cancer Statistics Branch; released April 2005, based onthe November 2004 submission. Available at: www.seer.cancer.gov.
29. US Census Bureau. Race and Gender Data. Available at:http://www.census.gov 2000. Accessed June 11, 2005.
30. Nietfeld JJ, Pasquini MC, Logan BR, Verter F, HorowitzMM. Lifetime probabilities of hematopoietic stem cell trans-plantation in the U.S. Biol Blood Marrow Transplant.2008;14:316-322.
31. Pasquini M. Current use and outcome of hematopoieticstem cell transplantation: part I – CIBMTR SummarySlides, 2005. CIBMTR Newsletter [serial online]. 2005;12:5-8.
32. U.S. Cancer Statistics Working Group. United States Can-cer Statistics: 1999-2005. Incidence and Mortality Web-based Report. Atlanta, GA: U.S. Department of Health andHuman Services, Centers for Disease Control and Preven-tion and National Cancer Institute; 2009. Available at:www.cdc.gov/uscs. Accessed June 11, 2005.
33. North American Association of Central Cancer Registries,Inc. Average-Annual Registry-Specific Cancer Incidence byRace, Ethnicity, and Sex; 2009v2. Springfield, IL: NorthAmerican Association of Central Cancer Registries, Inc;Year. Available at: http://www.naaccr.org/filesystem/pdf/CI-NA2009v2.world.pdf. Accessed January 17, 2009.
34. Parker SL, Johnston Davis K, Wingo PA, Ries LAG, HeathCW. Cancer statistics by race and ethnicity. CA Cancer J Clin.1998;48:31-48. Available at: http://caonline.amcancersoc.org/cgi/reprint/48/1/31.pdf. Accessed January 17, 2009.
Original Article
3476 Cancer July 15, 2010

From theReseasin; 2CReseaMinn4Medsachuand M7BristKingdversitTexas10A CHutch12BayRocheCentetonio,Nebra
Race and Outcomes of Autologous Hematopoietic CellTransplantation for Multiple Myeloma
Parameswaran N. Hari,1 Navneet S. Majhail,2,3 Mei-Jie Zhang,1 Anna Hassebroek,2
Fareeha Siddiqui,4 Karen Ballen,5 Asad Bashey,6 Jenny Bird,7 Cesar O. Freytes,8 John Gibson,9
Gregaory Hale,10 Leona Holmberg,11 Ram Kamble,12 Robert A. Kyle,13 Hillard M. Lazarus,14
Charles F. LeMaistre,15 Fausto Loberiza,16 Angelo Maiolino,17 Philip L. McCarthy,18
Gustavo Milone,19 Nancy Omondi,20 Donna E. Reece,21 Matthew Seftel,22 Michael Trigg,23
David Vesole,24 Brendan Weiss,25 Peter Wiernik,26 Stephanie J. Lee,1 J. Douglas Rizzo,1
Paulette Mehta27
Blacks are twice as likely to develop and die from multiple myeloma (MM), and are less likely to receive anautologous hematopoietic-cell transplant (AHCT) for MM compared to Whites. The influence of race onoutcomes of AHCT for MM is not well described. We compared the probability of overall survival (OS), pro-gression-free survival (PFS), disease progression, and nonrelapse mortality (NRM) among Black (N 5 303)and White (N 5 1892) recipients of AHCT for MM, who were reported to the Center for InternationalBlood and Marrow Transplant Research (CIBMTR) from 1995 to 2005. The Black cohort was more likelyto be female, and had better Karnofsky performance scores, but lower hemoglobin and albumin levels at di-agnosis. Black recipients were younger and more likely to be transplanted later in their disease course. Dis-ease stage and treatment characteristics prior to AHCTwere similar between the 2 groups. Black and Whiterecipients had similar probabilities of 5-year OS (52% versus 47%, P 5.19) and PFS (19% versus 21%, P 5.64)as well as cumulative incidences of disease progression (72% versus 72%, P 5.97) and NRM (9% versus 8%,P 5.52). In multivariate analyses, race was not associated with any of these endpoints. Black recipients ofAHCT for MM have similar outcomes compared to Whites, suggesting that the reasons underlying lowerrates of AHCT in Blacks need to be studied further to ensure equal access to effective therapy.
Biol Blood Marrow Transplant 16: 395-402 (2010) � 2010 American Society for Blood and Marrow Transplantation
KEY WORDS: Autologous hematopoietic cell tran
splantation, Multiple myeloma, Race, Survival, Progres-sion-free survival1Center for International Blood and Marrow Transplantrch, Medical College of Wisconsin, Milwaukee, Wiscon-
enter for International Blood and Marrow Transplantrch, National Marrow Donor Program, Minneapolis,esota; 3University of Minnesota, Minneapolis Minnesota;ical College of Wisconsin, Milwaukee, Wisconsin; 5Mas-setts General Hospital, Boston, Massachusetts; 6Bloodarrow Transplant Group of Georgia, Atlanta, Georgia;
ol Haematology and Oncology Centre, Bristol, Unitedom; 8South Texas Veterans Health Care System and Uni-
y of Texas Health Center at San Antonio, San Antonio,; 9Royal Prince Alfred Hospital, Camperdown, Australia;hildren’s Hospital, Saint Petersburg, Florida; 11Fredinson Cancer Research Center, Seattle, Washington;
lor College of Medicine, Houston, Texas; 13Mayo Clinic,ster Minnesota; 14University Hospitals Case Medicalr, Cleveland, Ohio; 15Texas Transplant Institute, San An-Texas; 16University of Nebraska Medical Center, Omaha,ska; 17Hospital Univarstario Clementino Frago Filho,
Rio de Janeiro, Brazil; 18Roswell Park Cancer Institute, BuffaloNew York; 19Angelica Ocampo-Hospital and Research Center,Fundaleu Buenos Aires, Argentina; 20National Marrow DonorProgram, Minneapolis, Minnesota; 21University of Toronto,Toronto, Ontario, Canada; 22CancerCare Manitoba, Manitoba,Canada; 23Merck & Co. Inc., Wilmington, Delaware; 24LoyolaUniversity Health System, Maywood, Illinois; 25Walter ReedArmy Medical Center, Washington, DC; 26New York MedicalCollege, Bronx, New York; and 27University of Arkansas, LittleRock, Arkansas.
Financial disclosure: See Acknowledgments on page 401.Correspondence and reprint requests: Parameswaran Hari, MD,
MS, CIBMTR, Medical College of Wisconsin, P.O. Box26509, 8701 Watertown Plank Road, Milwaukee, WI 53226(e-mail: [email protected]).
Received September 11, 2009; accepted November 8, 2009� 2010 American Society for Blood and Marrow Transplantation1083-8791/10/163-0012$36.00/0doi:10.1016/j.bbmt.2009.11.007
395

396 Biol Blood Marrow Transplant 16:395-402, 2010P. N. Hari et al.
BACKGROUND
Multiple myeloma (MM) remains an incurable dis-ease, although prognosis has improved in the pastdecade [1,2]. It is the most common hematologic ma-lignancy among Blacks, and is the only hematologicmalignancy that is more frequent in this racial groupcompared with Whites. In the United States, MMand its precursor disease monoclonal gammopathy ofundetermined significance (MGUS) are twice as com-mon in Blacks (annual incidence of 14.4/100,000 inmen and 9.8/100,000 in women compared with 6.6/100,000 in White men and 4.1/100,000 in Whitewomen) [1,3-7]. Proposed factors to explain theincreased incidence among Blacks include socioeco-nomic factors, greater exposure to hazardous materials,genetic predisposition, greater degree of backgroundantigenic stimulation, and a greater prevalence of obe-sity [8-10]. Mortality rates from MM in the UnitedStates are twice as high for Blacks compared to Whites(8.3/100,000 for men and 6.0/100,000 for women com-pared to 4.3/100,000 and 2.8/100,000 for White menand women, respectively) [11].
Socioeconomic factors that may have an impact onaccess to cancer therapy and therapeutic choices in-clude place of residence, distance from care centers, un-employment, availability and quality of healthinsurance, poor nutrition, exposure to infectiousagents, lower educational level, and annual income[12,13]. Prior comparisons have drawn conflicting con-clusions on treatment outcomes among Blacks com-pared with White patients with MM. Savage et al.[13,14] found that Black patients had shorter survivaltimes following similar therapy for MM. Presentationat later stages of disease, socioeconomic factors, or dif-ferential access to care were thought to explain this dis-parity. Other investigators have suggested that thesedisparities in outcomes are primarily because of biolog-ical characteristics [15,16].
Randomized clinical trials support the use of autol-ogous hematopoietic-cell transplant (AHCT) as a stan-dard therapy for MM [17,18]. We have previouslyshown that Blacks are less likely to receive AHCT forMM compared with their age- and sex-matched Whitecounterparts [19]. In the current study, we comparedoutcomes between Black and White patients receivingAHCT for MM to determine if disparate post trans-plant outcomes validate lower AHCT use in Blacks.
PATIENTS AND METHODS
The Center for International Blood and MarrowTransplant Research (CIBMTR) consists of a volun-tary working group of more than 450 transplantcenters worldwide. Centers contribute detailed dataon consecutive allogeneic and autologous transplantsto a statistical center at either the Medical College of
Wisconsin in Milwaukee or the National MarrowDonor Program (NMDP) Coordinating Center inMinneapolis. Subjects are followed longitudinally,with yearly follow-up. Computerized checks forerrors, physicians’ review of submitted data, and on-site audits of participating centers ensure data quality.Observational studies conducted by the CIBMTR aredone with a waiver of informed consent and in compli-ance with HIPAA regulations as determined by theInstitutional Review Board and the Privacy Officer ofthe Medical College of Wisconsin.
Patients
The study included 2195 (303 Black and 1892White) adult (aged $18 years) recipients of AHCTfor MM who were transplanted between January 1995and June 2005 (Table 1). Only recipients of peripheralblood (PB) AHCT were included in this study; patientswho had received planned tandem AHCT (N 5 582)were excluded. Centers obtained information aboutpatient race and then reported it to the CIBMTR.
Statistical Methods
Patient-, disease-, and treatment-related factorswere compared between the Black and White cohorts,using a chi-square test for categorical and a Kruskal-Wallis test for continuous variables. Outcomes analyzedincluded nonrelapse mortality (NRM), relapse/pro-gression, progression-free survival (PFS), and overallsurvival (OS). NRM was defined as death occurring inthe absence of relapse or progression of MM followingAHCT. Relapse/progression was defined according tostandard criteria [20]. Chemotherapy sensitivity was de-fined as achievement of a partial or complete response(PR, CR) to pretransplant therapy. PFS was defined assurvival without disease progression or relapse. Patientsalive and with no evidence of disease progression or re-lapse were censored at the time of last follow-up. Thesurvival interval variable was defined as time from thedate of transplant to the date of death or last contactand summarized by a survival curve. Probabilities ofOS and PFS were calculated using the Kaplan-Meier es-timator [21,22]. NRM and relapse/progression werecalculated using cumulative incidence estimates. Thelog-rank test was used for univariate comparisons.
Multivariate Cox proportional hazards regressionwas used to examine the outcomes between Blackand White patient cohorts and to identify risk factorsassociated with outcomes [23]. A stepwise forwardselection multivariate model was built to identifycovariates that influenced outcomes. Any covariatewith a value of P \ .05 was considered significant.The proportionality assumption for Cox regressionwas tested by adding a time-dependent covariate foreach risk factor and each outcome. Tests indicatedthat all variables met the proportional hazards

Table 1. Patient Characteristics
White Black
Variable N (%) N (%) P-value
Number of patients 1892 303Age median (range), years 57 (27-80) 55 (27-74) <.001Age group at transplant, years .002
<50 396 (21) 88 (29)50-64 1111 (59) 172 (57)$ 65 385 (20) 43 (14)
Male sex 1136 (60) 164 (54) .05Karnofsky score pretransplant .005
$90 1153 (61) 210 (69)Hypertension <.001
Yes 471 (25) 143 (47)Diabetes <.001
Yes 169 (9) 50 (17)Body Mass Index .01
Underweight/normal (<25) 557 (29) 67 (22)Overweight (25-29.9) 741 (39) 120 (40)Obese/morbidly obese ($30) 594 (31) 116 (38)
Disease relatedDurie-Salmon stage at diagnosis .25
I 203 (11) 25 (8)II 562 (30) 101 (33)III 1127 (60) 177 (58)
Immunochemical subtype of myeloma .34IgG 1003 (53) 173 (57)IgA 359 (19) 45 (15)Light chain 329 (17) 54 (18)Others/unknown 125 (11) 16 (10)
Albumin level at diagnosis .05>3.5 g/dL 732 (39) 101 (33)
Hemoglobin at diagnosis <10 g/dL <.001<10 g/dL 552 (29) 135 (45)
Creatinine at diagnosis .09>1.5 mg/dL 361 (19) 74 (24)
B-2 microglobulin level at diagnosis .83$5.5 mg/L 195 (10) 31 (10)
Prior chemotherapy regimens .78MP ± others 334 (18) 50 (17)VAD ± others (not MP) 1104 (58) 182 (60)Cy ± others 300 (16) 52 (17)Corticosteroids ± others 154 (8) 19 (6)
Number of lines of chemotherapy§ .291 1125 (59) 167 (55)2 536 (28) 99 (33)>2 231 (12) 37 (12)
Sensitive to chemotherapy prior to transplant .83Sensitive 1434 (76) 228 (75)
Disease status at time of transplant .67Complete remission/partial remission 1396 (74) 231 (76)
Treatment relatedTime from diagnosis to transplant median (range), months 8 (<1-249) 9 (2-217) <.001Time from diagnosis to transplant <.001
<12 months 1364 (72) 190 (63)$12 months 528 (28) 113 (37)
Conditioning regimen .7Melphalan only 1417 (75) 223 (74)Melphalan + TBI ± others 204 (11) 35 (12)Bu-Cy ± others (not TBI, not melphalan) 271 (15) 45 (15)
Median follow-up of survivors, median (range) 61 (<1-145) 51 (<1-132)
MP indicates Melphalan + Prednisone; VAD, vincristine + dexamethasone + adriamycin; Cy, cyclophosphamide; Bu, busulfan; TBI, total body irradiation;Eval, evaluable.§ Excludes stem cell priming.
Biol Blood Marrow Transplant 16:395-402, 2010 397Race and Outcomes of AHCT for MM
assumption. Results were expressed as relative risks(RR). Any risk factors found to be significant were ad-justed in the final Cox model. The main effect tested(ie, Black versus White) was included in all models.
The variables considered in multivariate analyses aresummarized in Table 2. Analyses were performed us-ing SAS software, version 9.1 (SAS Institute, Cary,NC).
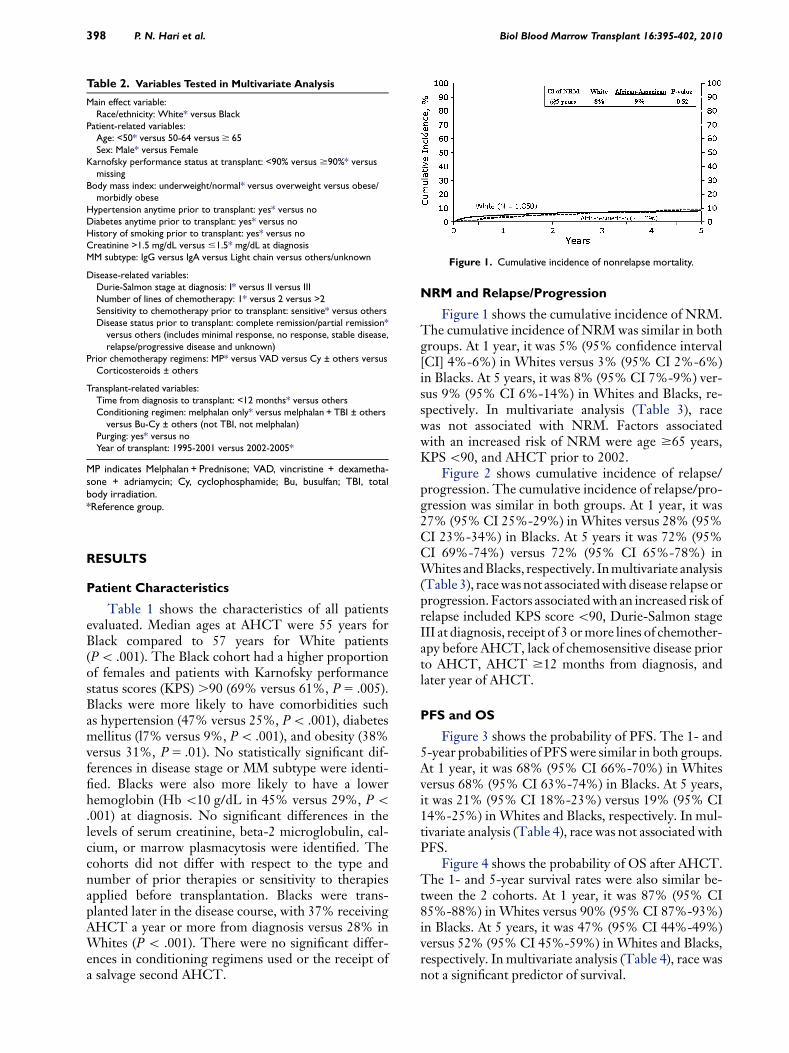
Table 2. Variables Tested in Multivariate Analysis
Main effect variable:Race/ethnicity: White* versus Black
Patient-related variables:Age: <50* versus 50-64 versus $ 65Sex: Male* versus Female
Karnofsky performance status at transplant: <90% versus $90%* versusmissing
Body mass index: underweight/normal* versus overweight versus obese/morbidly obese
Hypertension anytime prior to transplant: yes* versus noDiabetes anytime prior to transplant: yes* versus noHistory of smoking prior to transplant: yes* versus noCreatinine >1.5 mg/dL versus #1.5* mg/dL at diagnosisMM subtype: IgG versus IgA versus Light chain versus others/unknown
Disease-related variables:Durie-Salmon stage at diagnosis: I* versus II versus IIINumber of lines of chemotherapy: 1* versus 2 versus >2Sensitivity to chemotherapy prior to transplant: sensitive* versus othersDisease status prior to transplant: complete remission/partial remission*
versus others (includes minimal response, no response, stable disease,relapse/progressive disease and unknown)
Prior chemotherapy regimens: MP* versus VAD versus Cy ± others versusCorticosteroids ± others
Transplant-related variables:Time from diagnosis to transplant: <12 months* versus othersConditioning regimen: melphalan only* versus melphalan + TBI ± others
versus Bu-Cy ± others (not TBI, not melphalan)Purging: yes* versus noYear of transplant: 1995-2001 versus 2002-2005*
MP indicates Melphalan + Prednisone; VAD, vincristine + dexametha-sone + adriamycin; Cy, cyclophosphamide; Bu, busulfan; TBI, totalbody irradiation.*Reference group.
Figure 1. Cumulative incidence of nonrelapse mortality.
398 Biol Blood Marrow Transplant 16:395-402, 2010P. N. Hari et al.
RESULTS
Patient Characteristics
Table 1 shows the characteristics of all patientsevaluated. Median ages at AHCT were 55 years forBlack compared to 57 years for White patients(P \ .001). The Black cohort had a higher proportionof females and patients with Karnofsky performancestatus scores (KPS) .90 (69% versus 61%, P 5 .005).Blacks were more likely to have comorbidities suchas hypertension (47% versus 25%, P \ .001), diabetesmellitus (l7% versus 9%, P \ .001), and obesity (38%versus 31%, P 5 .01). No statistically significant dif-ferences in disease stage or MM subtype were identi-fied. Blacks were also more likely to have a lowerhemoglobin (Hb \10 g/dL in 45% versus 29%, P \.001) at diagnosis. No significant differences in thelevels of serum creatinine, beta-2 microglobulin, cal-cium, or marrow plasmacytosis were identified. Thecohorts did not differ with respect to the type andnumber of prior therapies or sensitivity to therapiesapplied before transplantation. Blacks were trans-planted later in the disease course, with 37% receivingAHCT a year or more from diagnosis versus 28% inWhites (P \ .001). There were no significant differ-ences in conditioning regimens used or the receipt ofa salvage second AHCT.
NRM and Relapse/Progression
Figure 1 shows the cumulative incidence of NRM.The cumulative incidence of NRM was similar in bothgroups. At 1 year, it was 5% (95% confidence interval[CI] 4%-6%) in Whites versus 3% (95% CI 2%-6%)in Blacks. At 5 years, it was 8% (95% CI 7%-9%) ver-sus 9% (95% CI 6%-14%) in Whites and Blacks, re-spectively. In multivariate analysis (Table 3), racewas not associated with NRM. Factors associatedwith an increased risk of NRM were age $65 years,KPS \90, and AHCT prior to 2002.
Figure 2 shows cumulative incidence of relapse/progression. The cumulative incidence of relapse/pro-gression was similar in both groups. At 1 year, it was27% (95% CI 25%-29%) in Whites versus 28% (95%CI 23%-34%) in Blacks. At 5 years it was 72% (95%CI 69%-74%) versus 72% (95% CI 65%-78%) inWhites and Blacks, respectively. In multivariate analysis(Table 3), race was not associated with disease relapse orprogression. Factors associated with an increased risk ofrelapse included KPS score \90, Durie-Salmon stageIII at diagnosis, receipt of 3 or more lines of chemother-apy before AHCT, lack of chemosensitive disease priorto AHCT, AHCT $12 months from diagnosis, andlater year of AHCT.
PFS and OS
Figure 3 shows the probability of PFS. The 1- and5-year probabilities of PFS were similar in both groups.At 1 year, it was 68% (95% CI 66%-70%) in Whitesversus 68% (95% CI 63%-74%) in Blacks. At 5 years,it was 21% (95% CI 18%-23%) versus 19% (95% CI14%-25%) in Whites and Blacks, respectively. In mul-tivariate analysis (Table 4), race was not associated withPFS.
Figure 4 shows the probability of OS after AHCT.The 1- and 5-year survival rates were also similar be-tween the 2 cohorts. At 1 year, it was 87% (95% CI85%-88%) in Whites versus 90% (95% CI 87%-93%)in Blacks. At 5 years, it was 47% (95% CI 44%-49%)versus 52% (95% CI 45%-59%) in Whites and Blacks,respectively. In multivariate analysis (Table 4), race wasnot a significant predictor of survival.

Table 3. Multivariate Analysis for Relapse and Nonrelapse Mortality
Relapse Nonrelapse mortality
Variable N RR P-Value N RR P-Value
RaceWhite 1850 1.00 1850 1.00Black 296 0.92 (0.78-1.08) P 5.28 296 1.16 (0.75-1.80) P 5.51
Patient age, years<50 475 1.00 P < .00150-64 1253 1.55 (1.01-2.39) P 5.05$65 418 3.50 (2.17-5.65) P < .001
Karnofsky Score prior to conditioning<90 815 1.00 815 1.00$90 1331 0.88 (0.79-0.98) P 5.02 1331 0.72 (0.53-0.98) P 5.03
Durie-Salmon stage at diagnosisI 222 1.00 P < .001 222 1.00 P 5.004II 652 1.23 (1.00-1.51) P 5.05 652 0.61 (0.35-1.06) P 5.08III 1272 1.54 (1.27-1.87) P < .001 1272 1.16 (0.71-1.88) P 5.56
Number of lines of chemotherapy‡1 1256 1.00 P 5.0012 628 1.12 (0.99-1.27) P 5.07>2 262 1.39 (1.16-1.66) P < .001
Sensitivity to chemotherapy priorto transplantOther 522 1.00Sensitive 1624 0.76 (0.67-0.85) P < .001
Time from diagnosis to transplant<12 months 1519 1.00$12 months 627 1.19 (1.04-1.35) P 5.009
Year of transplant1995-2001 1331 1.00 1331 1.002002-2005 815 1.17 (1.04-1.31) P 5.008 815 0.56 (0.39-0.81) P 5.002
RR indicates relative risk.‡Excludes stem cell priming.
Biol Blood Marrow Transplant 16:395-402, 2010 399Race and Outcomes of AHCT for MM
PFS and OS were worse in patients with older ageat AHCT (.50 years), KPS score \90, higher Durie-Salmon stage, those who received 2 or more lines oftherapy prior to AHCT, AHCT $12 months from di-agnosis, and chemotherapy resistant disease (Table 4).OS was also lower in patients who underwent AHCTprior to 2002.
The major cause of mortality in both cohorts wasrelapse or progression of MM that accounted for72% of all deaths.
DISCUSSION
Our analysis establishes that Black and Whiteshave very similar outcomes after AHCT for MM.
Figure 2. Cumulative incidence of disease relapse and progression.
These results concur with observations in other studiesof nontransplant therapy that the disparity in out-comes for MM disappears when Blacks receive identi-cal therapy [24].
Several investigators have shown that Blacks haveoutcomes similar to Whites when given the same non-transplant treatment for MM. Rohatgi et al. [25]showed that Blacks were less likely to receive chemo-therapy, but they responded with similar outcomeswhen given similar nontransplant therapy for MM.In the pretransplant era, Modiano et al. [26] retrospec-tively evaluated the impact of race in the results of theSWOG 8829 study of conventional chemotherapy forMM. From 99 study sites in the United States, 116Black and 467 White patients were shown to have
Figure 3. Probability of progression-free survival.

Table 4. Multivariate Analysis for Overall Survival and Progression-Free Survival
Overall Survival Progression-Free Survival
Variable N RR P-Value N RR P-Value
RaceWhite 1892 1.00 1850 1.00Black 303 0.94 (0.78-1.13) P 5.50 296 0.94 (0.81-1.09) P 5.39
Patient age, years<50 484 1.00 P < .0001 475 1.00 P 5.0350-64 1283 1.26 (1.09-1.46) P 5.002 1253 1.12 (0.99-1.27) P 5.08$65 428 1.52 (1.26-1.83) P < .0001 418 1.24 (1.06-1.46) P 5.007
Karnofsky Score prior to conditioning<90 832 1.00 815 1.00$90 1363 0.74 (0.66-0.83) P < .0001 1331 0.87 (0.79-0.97) P 5.009
Durie-Salmon stage at diagnosisI 228 1.00 P < .0001 222 1.00 P < .0001II 663 1.13 (0.89-1.44) P 5.32 652 1.12 (0.93-1.36) P 5.23III 1304 1.67 (1.34-2.09) P < .0001 1272 1.49 (1.25-1.79) P < .0001
Number of lines of chemotherapy‡1 1292 1.00 P < .0001 1256 1.00 P 5.00022 635 1.10 (0.96-1.27) P 5.17 628 1.13 (1.00-1.27) P 5.04>2 268 1.66 (1.37-2.01) P < .0001 262 1.41 (1.19-1.67) P < .0001
Sensitivity to chemotherapy prior to transplantOther 533 1.00 522 1.00Sensitive 1662 0.82 (0.72-0.94) P 5.003 1624 0.76 (0.68-0.85) P < .0001
Time from diagnosis to transplant<12 months 1554 1.00 1519 1.00$12 months 641 1.16 (1.01-1.34) P 5.04 627 1.16 (1.03-1.31) P 5.01
RR indicates relative risk.‡Excludes stem cell priming.
400 Biol Blood Marrow Transplant 16:395-402, 2010P. N. Hari et al.
similar median survival (32 and 30 months, respec-tively). There were no differences by stage or MM sub-type. A smaller study from the Department of Defenseequal access health care system, reported on the out-comes of 36 Black and 55 White newly diagnosed pa-tients receiving AHCT for MM and observedcomparable outcomes between the 2 groups [27]. Intheir study, there were no differences in the stage, he-moglobin, calcium, or creatinine levels, althoughBlacks did have higher C-reactive protein (CRP) levelsand a trend for less skeletal involvement. The authorsrecommended a larger retrospective study such as thecurrent one. Other single center analyses comparingBlack and White recipients of AHCT for MM havedrawn conflicting conclusions. Khaled et al. [28] ana-lyzed 101 Black patients and concluded that theywere likely to relapse earlier after AHCT. Survivalwas not compared in this study. Saraf et al. [24] in their
Figure 4. Probability of overall survival.
comparative study that included 38 Black and 32White AHCT recipients, found that Black patientshad more prolonged responses and greater event-freesurvival (EFS).
Unfortunately, there is ample evidence that Blacksare less likely to receive chemotherapy for MM as wellas AHCT. Rohatgi et al. [25] reviewed patterns ofchemotherapy use for patients with MM outside theclinical trial setting. From a population-based retro-spective cohort of 49,021 patients aged 65 years orolder with stage II or III MM, they found that only52% received chemotherapy. Blacks were less likely toreceive chemotherapy compared to Whites (47.6%versus 52.8%) despite evidence that use of chemother-apy decreased all cause mortality, myeloma specificmortality, and increased survival [25]. The reasonsfor the disparate access are unclear, because control-ling for socioeconomic status did not eliminate the dis-parity in the receipt of chemotherapy.
These disparities in the receipt of therapy occur inthe transplant setting as well. Joshua et al. [19], in aprevious study from the CIBMTR, demonstrate thatWhites are more likely to receive AHCT for newlydiagnosed MM compared to an age- and sex-adjustedBlack population. Using data from the SEER andCIBMTR registries, the study showed that age- andsex-adjusted odds of receiving AHCT for MM is 1.72times greater in Whites compared to Blacks. Althoughour study cannot address the reasons for this underuti-lization of AHCT in Blacks, interesting conclusions canbe drawn regarding AHCT for MM in Black patients.

Biol Blood Marrow Transplant 16:395-402, 2010 401Race and Outcomes of AHCT for MM
It has been proposed that reduced access to treat-ment for MM may be related to actual or perceivedworse outcomes in Black patients. Our study clearlyshows that outcomes are not different between Blacksand Whites receiving AHCT for MM, suggesting thistreatment modality should be offered to all patientswhen medically appropriate. These results are in ac-cordance with a meta-analysis of patients treated for14 different cancers, where survival in the majority ofcancers was similar between races when comparabletreatment was given [29].
The pretransplant characteristics of Black recipi-ents of AHCT are interesting. The Black cohort wasyounger and had better performance status than theWhite cohort, despite higher rates of anemia and othercomorbidities at diagnosis. These differences likelyindicate a selection bias operating against older Blackpatients with lower KPS scores with regard to referralfor consideration of AHCT. Black patients were alsolikely to have had a longer time between diagnosisand transplantation compared to Whites, while receiv-ing a similar number of chemotherapy regimens andhaving similar responses. This suggests delayed refer-ral for consideration of AHCT. A referral bias favoringonly the healthiest Black patients for transplant may bein effect, whereas patients with less favorable clinicalfeatures may only be offered nontransplant or evennontreatment options.
The major strength of our study is the broad rep-resentation of transplant centers making it very likelythat these results are applicable to the transplant com-munity as a whole. In this analysis, we are unable todraw any conclusions about factors associated withnonreceipt of transplant in Blacks because a nontrans-plant population is not represented. The characteris-tics of the population of black MM patients notreceiving AHCT need to be analyzed to identify thecauses of a under utilization of AHCT. It is possiblethat many Blacks who are not receiving stem cell trans-plantation for myeloma are forgoing the transplant bychoice. However, it is also possible that referral bias,unequal access to tertiary care, compliance gap, reluc-tance to enter clinical trials, and socioeconomic dispar-ities account for some of the differences in utilizationof AHCT for patients with MM. With the demonstra-tion of equal outcomes for Blacks with MM, furtherstudy and definitive action to ensure better awarenessand delivery of transplant options for the Black popu-lation is warranted.
ACKNOWLEDGMENTS
Financial disclosure: The CIBMTR is supported byPublic Health Service Grant/Cooperative AgreementU24-CA76518 from the National Cancer Institute(NCI), the National Heart, Lung and Blood Institute(NHLBI), and the National Institute of Allergy and
Infectious Diseases (NIAID); a Grant/CooperativeAgreement 5U01HL069294 from NHLBI and NCI;a contract HHSH234200637015C with HealthResources and Services Administration (HRSA/DHHS); 2 Grants N00014-06-1-0704 and N00014-08-1-0058 from the Office of Naval Research; andgrants from AABB; Aetna; American Society for Bloodand Marrow Transplantation; Amgen, Inc.; anony-mous donation to the Medical College of Wisconsin;Association of Medical Microbiology and InfectiousDisease Canada; Astellas Pharma US, Inc.; BaxterInternational, Inc.; Bayer HealthCare Pharmaceuti-cals; Blood Center of Wisconsin; Blue Cross andBlue Shield Association; Bone Marrow Foundation;Canadian Blood and Marrow Transplant Group; Cel-gene Corporation; CellGenix, GmbH; Centers forDisease Control and Prevention; ClinImmune Labs;CTI Clinical Trial and Consulting Services; CubistPharmaceuticals; Cylex Inc.; CytoTherm; DOR Bio-Pharma, Inc.; Dynal Biotech, an Invitrogen Company;Enzon Pharmaceuticals, Inc.; European Group forBlood and Marrow Transplantation; Gambro BCT,Inc.; Gamida Cell, Ltd.; Genzyme Corporation; His-togenetics, Inc.; HKS Medical Information Systems;Hospira, Inc.; Infectious Diseases Society of America;Kiadis Pharma; Kirin Brewery Co., Ltd.; Merck &Company; The Medical College of Wisconsin; MGIPharma, Inc.; Michigan Community Blood Centers;Millennium Pharmaceuticals, Inc.; Miller PharmacalGroup; Milliman USA, Inc.; Miltenyi Biotec, Inc.;National Marrow Donor Program; Nature PublishingGroup; New York Blood Center; Novartis Oncology;Oncology Nursing Society; Osiris Therapeutics, Inc.;Otsuka Pharmaceutical Development & Commercial-ization, Inc.; Pall Life Sciences; PDL BioPharma,Inc; Pfizer Inc; Pharmion Corporation; SaladaxBiomedical, Inc.; Schering Plough Corporation; Soci-ety for Healthcare Epidemiology of America; Stem-Cyte, Inc.; StemSoft Software, Inc.; Sysmex; TevaPharmaceutical Industries; The Marrow Foundation;THERAKOS, Inc.; Vidacare Corporation; Vion Phar-maceuticals, Inc.; ViraCor Laboratories; ViroPharma,Inc.; and Wellpoint, Inc.
The views expressed in this article do not reflectthe official policy or position of the National Institutesof Health, the Department of the Navy, the Depart-ment of Defense, or any other agency of the U.S.Government.
REFERENCES
1. Kyle RA, Rajkumar SV. Epidemiology of the plasma-cell disor-ders. Best Pract Res Clin Haematol. 2007;20:637-664.
2. Kumar SK, Rajkumar SV, Dispenzieri A, et al. Improved survivalin multiple myeloma and the impact of novel therapies. Blood.2008;111:2516-2520.
3. Brown LM, Gridley G, Check D, Landgren O. Risk of multiplemyeloma and monoclonal gammopathy of undetermined signif-icance among white and black male United States veterans with

402 Biol Blood Marrow Transplant 16:395-402, 2010P. N. Hari et al.
prior autoimmune, infectious, inflammatory, and allergic disor-ders. Blood. 2008;111:3388-3394.
4. Landgren O, Gridley G, Turesson I, et al. Risk of monoclonalgammopathy of undetermined significance (MGUS) and subse-quent multiple myeloma among black and white veterans in theUnited States. Blood. 2006;107:904-906.
5. Ries L, Melbert D, Krapcho M, et al. SEER Cancer StatisticsReview, 1975-2005, National Cancer Institute. Bethesda,MD. http://seer.cancer.gov/csr/1975_2005, based on Novem-ber 2007 SEER data submission, posted to the SEER web site,2008. last accessed January 2009.
6. Singh J, Dudley AW Jr., Kulig KA. Increased incidence ofmonoclonal gammopathy of undetermined significance in blacksand its age-related differences with whites on the basis of a studyof 397 men and one woman in a hospital setting. J Lab Clin Med.1990;116:785-789.
7. Landgren O, Katzmann JA, Hsing AW, et al. Prevalence ofmonoclonal gammopathy of undetermined significance amongmen in Ghana. Mayo Clin Proc. 2007;82:1468-1473.
8. Samanic C, Gridley G, Chow WH, Lubin J, Hoover RN,Fraumeni JF Jr. Obesity and cancer risk among white and blackUnited States veterans. Cancer Causes Control. 2004;15:35-43.
9. Benjamin M, Reddy S, Brawley OW. Myeloma and race: a reviewof the literature. Cancer Metastasis Rev. 2003;22:87-93.
10. Friedman GD, Herrinton LJ. Obesity and multiple myeloma.Cancer Causes Control. 1994;5:479-483.
11. http://seer.cancer.gov/statfacts/html/mulmy.html. last accessedJanuary 2009.
12. Abou-Jawde RM, Baz R, Walker E, et al. The role of race, socio-economic status, and distance traveled on the outcome of blackpa-tients with multiple myeloma. Haematologica. 2006;91:1410-1413.
13. Savage D, Lindenbaum J, Van Ryzin J, Struening E, Garrett TJ.Race, poverty, and survival in multiple myeloma. Cancer. 1984;54:3085-3094.
14. Cella DF, Orav EJ, Kornblith AB, et al. Socioeconomic statusand cancer survival. J Clin Oncol. 1991;9:1500-1509.
15. Lyn D, Cherney BW, Lalande M, et al. A duplicated region isresponsible for the poly(ADP-ribose) polymerase polymor-phism, on chromosome 13, associated with a predisposition tocancer. Am J Hum Genet. 1993;52:124-134.
16. Cao J, Hong CH, Rosen L, et al. Deletion of genetic materialfrom a poly(ADP-ribose) polymerase-like gene on chromosome13 occurs frequently in patients with monoclonal gammopa-thies. Cancer Epidemiol Biomarkers Prev. 1995;4:759-763.
17. Attal M, Harousseau JL, Stoppa AM, et al. A prospective, ran-domized trial of autologous bone marrow transplantation andchemotherapy in multiple myeloma. Intergroupe Francais duMyelome. N Engl J Med. 1996;335:91-97.
18. Child JA, Morgan GJ, Davies FE, et al. High-dose chemother-apy with hematopoietic stem-cell rescue for multiple myeloma.N Engl J Med. 2003;348:1875-1883.
19. Joshua TV, Rizzo JD, Zhang MJ, Horowitz MM. Access to he-matopoietic stem cell transplantation: effect of race and gender.Biol Blood Marrow Transplant. 2007;13(Suppl):22.
20. Blade J, Samson D, Reece D, et al. Criteria for evaluating diseaseresponse and progression in patients with multiple myelomatreated by high-dose therapy and haemopoietic stem cell trans-plantation. Myeloma Subcommittee of the EBMT. EuropeanGroup for Blood and Marrow Transplant. Br J Haematol.1998;102:1115-1123.
21. Kaplan EL, Meier P. Nonparametric estimation from incom-plete observations. J Am Stat Assoc. 1958;53:457-481.
22. Klein JP, Moeschberger ML. Survival Analysis: Techniquesfor Censored and Truncated Data, 2nd ed. New York: SpringerVerlag; 2003.
23. Cox DR. Regression models and life tables. J R Stat Soc B. 1972;34:187-220.
24. Saraf S, Chen YH, Dobogai LC, et al. Prolonged responsesafter autologous stem cell transplantation in black patientswith multiple myeloma. Bone Marrow Transplant. 2006;37:1099-1102.
25. Rohatgi N, Du XL, Coker AL, Moye LA, Wang M, Fang S.Chemotherapy and survival for patients with multiple myeloma:findings from a large nationwide and population-based cohort.Am J Clin Oncol. 2007;30:540-548.
26. Modiano MR, Villar-Werstler P, Crowley J, Salmon SE. Evalu-ation of race as a prognostic factor in multiple myeloma. An an-cillary of Southwest Oncology Group Study 8229. J Clin Oncol.1996;14:974-977.
27. Verma PS, Howard RS, Weiss BM. The impact of race on out-comes of autologous transplantation in patients with multiplemyeloma. Am J Hematol. 2008;83:355-358.
28. Khaled Y, Abidi MH, Janakiraman N, et al. Outcomes afterauto-SCT in blacks with multiple myeloma. Bone Marrow Trans-plant. 2009;43:845-851.
29. Bach PB, Schrag D, Brawley OW, Galaznik A, Yakren S,Begg CB. Survival of blacks and whites after a cancer diagnosis.JAMA. 2002;287:2106-2113.

Home > Cancer Statistics > Cancer Stat Fact Sheets > Myeloma
SEER Stat Fact Sheets: Myeloma
Cancer:
It is estimated that 21,700 men and women (12,190 men and 9,510 women) will be diagnosed with and 10,710 men andwomen will die of myeloma in 2012 1 .
The following information is based on NCI’s SEER Cancer Statistics Review 2 .Use the links on this page to learn moreabout each statistic type:
Incidence & MortalitySurvival & StageLifetime RiskPrevalenceReferences
Incidence & Mortality
SEER Incidence
From 2005-2009, the median age at diagnosis for myeloma was 69 years of age 3 . Approximately 0.0% were diagnosedunder age 20; 0.5% between 20 and 34; 3.2% between 35 and 44; 11.8% between 45 and 54; 22.3% between 55 and 64;26.9% between 65 and 74; 25.6% between 75 and 84; and 9.6% 85+ years of age.
The age-adjusted incidence rate was 5.8 per 100,000 men and women per year. These rates are based on cases diagnosedin 2005-2009 from 18 SEER geographic areas.
Incidence Rates by Race
Race/Ethnicity Male Female
All Races 7.4 per 100,000 men 4.7 per 100,000 women
White 6.9 per 100,000 men 4.1 per 100,000 women
Black 14.3 per 100,000 men 10.1 per 100,000 women
Asian/Pacific Islander 4.2 per 100,000 men 2.9 per 100,000 women
American Indian/Alaska Native a 4.9 per 100,000 men 4.2 per 100,000 women
Hispanic b 6.3 per 100,000 men 4.7 per 100,000 women
US Mortality
From 2005-2009, the median age at death for myeloma was 74 years of age 4 . Approximately 0.0% died under age 20;0.1% between 20 and 34; 1.2% between 35 and 44; 6.3% between 45 and 54; 16.3% between 55 and 64; 26.3% between65 and 74; 33.7% between 75 and 84; and 16.2% 85+ years of age.
The age-adjusted death rate was 3.4 per 100,000 men and women per year. These rates are based on patients who died in2005-2009 in the US.
Myeloma - SEER Stat Fact Sheets http://seer.cancer.gov/statfacts/html/mulmy.html
1 of 4 10/21/2012 6:10 PM

Death Rates by Race
Race/Ethnicity Male Female
All Races 4.4 per 100,000 men 2.7 per 100,000 women
White 4.1 per 100,000 men 2.5 per 100,000 women
Black 8.0 per 100,000 men 5.4 per 100,000 women
Asian/Pacific Islander 2.1 per 100,000 men 1.4 per 100,000 women
American Indian/Alaska Native a 3.8 per 100,000 men 2.5 per 100,000 women
Hispanic b 3.3 per 100,000 men 2.3 per 100,000 women
Trends in Rates
Trends in rates can be described in many ways. Information for trends over a fixed period of time, for example 1996-2009,can be evaluated by the annual percentage change (APC) . If there is a negative sign before the number, the trend is adecrease; otherwise it is an increase. If there is an asterisk after the APC then the trend was significant, that is, one believesthat it is beyond chance, i.e. 95% sure, that the increase or decrease is real over the period 1996-2009. If the trend is notsignificant, the trend is usually reported as stable or level. Joinpoint analyses can be used over a long period of time toevaluate when changes in the trend have occurred along with the APC which shows how much the trend has changedbetween each of the joinpoints.
The joinpoint trend in SEER cancer incidence withassociated APC(%) for myeloma between 1975-2009, All
Races
Male and Female Male Female
Trend Period Trend Period Trend Period
1.2* 1975-1991 0.6* 1975-2009 1.1* 1975-1992
0.2 1991-2009 0.0 1992-2009
The joinpoint trend in US cancer mortality with associatedAPC(%) for myeloma between 1975-2009, All Races
Male and Female Male Female
Trend Period Trend Period Trend Period
1.4* 1975-1994 1.5* 1975-1994 1.5* 1975-1993
-0.7* 1994-2002 -1.1* 1994-2009 -0.5* 1993-2002
-1.9* 2002-2009 -2.9* 2002-2009
Survival & Stage
Survival can be calculated by different methods for different purposes. The survival statistics presented here are based onrelative survival, which measures the survival of the cancer patients in comparison to the general population to estimate theeffect of cancer. The overall 5-year relative survival for 2002-2008 from 18 SEER geographic areas was 41.1%. Five-yearrelative survival by race and sex was: 42.6% for white men; 38.8% for white women; 39.5% for black men; 42.4% for blackwomen.
Stage Distribution and 5-year Relative Survival by Stage at Diagnosis for2002-2008, All Races, Both Sexes
Stage at Diagnosis StageDistribution (%)
5-yearRelative Survival (%)
Localized (confined to primary site) 5 67.0
Regional (spread to regional lymphnodes) 0 0.0
Myeloma - SEER Stat Fact Sheets http://seer.cancer.gov/statfacts/html/mulmy.html
2 of 4 10/21/2012 6:10 PM

Distant (cancer has metastasized) 95 39.8
Unknown (unstaged) 0 0.0
The stage distribution is based on Summary Stage 2000.
Lifetime Risk
Based on rates from 2007-2009, 0.67% of men and women born today will be diagnosed with myeloma at some time duringtheir lifetime. This number can also be expressed as 1 in 150 men and women will be diagnosed with myeloma during theirlifetime. These statistics are called the lifetime risk of developing cancer. Sometimes it is more useful to look at theprobability of developing myeloma between two age groups. For example, 0.30% of men will develop myeloma betweentheir 50th and 70th birthdays compared to 0.21% for women.
Prevalence
On January 1, 2009, in the United States there were approximately 71,213 men and women alive who had a history ofmyeloma -- 38,414 men and 32,799 women. This includes any person alive on January 1, 2009 who had been diagnosedwith myeloma at any point prior to January 1, 2009 and includes persons with active disease and those who are cured of theirdisease. Prevalence can also be expressed as a percentage and it can also be calculated for a specific amount of timeprior to January 1, 2009 such as diagnosed within 5 years of January 1, 2009.
References
All statistics in this report are based on SEER incidence and NCHS mortality statistics. Most can be found within:
Howlader N, Noone AM, Krapcho M, Neyman N, Aminou R, Altekruse SF, Kosary CL, Ruhl J, Tatalovich Z, ChoH, Mariotto A, Eisner MP, Lewis DR, Chen HS, Feuer EJ, Cronin KA (eds). SEER Cancer Statistics Review,1975-2009 (Vintage 2009 Populations), National Cancer Institute. Bethesda, MD, http://seer.cancer.gov/csr/1975_2009_pops09/, based on November 2011 SEER data submission, posted to the SEER web site,2012.
Footnotes
1 Table I-1 (http://seer.cancer.gov/csr/1975_2009_pops09/results_single/sect_01_table.01.pdf)2 Myeloma Section (http://seer.cancer.gov/csr/ 1975_2009_pops09/results_merged/ sect_18_myeloma.pdf)3 Table I-11 (http://seer.cancer.gov/csr/1975_2009_pops09/results_single/sect_01_table.11_2pgs.pdf)4 Table I-13 (http://seer.cancer.gov/csr/1975_2009_pops09/results_single/sect_01_table.13_2pgs.pdf)* The APC is significantly different from zero (p<.05).a Incidence data for Hispanics is based on NHIA and excludes cases from Alaska Native Registry. Hispanic death ratesexclude deaths from the District of Columbia, North Dakota and South Carolina.b Incidence and mortality data for American Indians/Alaska Natives is based on the CHSDA (Contract Health Service DeliveryArea) counties.
Definitions
Annual percent change (APC)The average annual percent change over several years. The APC is used to measure trends or the change in ratesover time. For information on how this is calculated, go to Trend Algortihms in the SEER*Stat Help system. Thecalculation involves fitting a straight line to the natural logarithm of the data when it is displayed by calendar year.
Joinpoint analysesA statistical model for characterizing cancer trends which uses statistical criteria to determine how many times andwhen the trends in incidence or mortality rates have changed. The results of joinpoint are given as calendar yearranges, and the annual percent change (APC) in the rates over each period.
SurvivalSurvival examines how long after diagnosis people live. Cancer survival is measured in a number of different waysdepending on the intended purpose.
Relative survivalA measure of net survival that is calculated by comparing observed (overall) survival with expected survival from a
Myeloma - SEER Stat Fact Sheets http://seer.cancer.gov/statfacts/html/mulmy.html
3 of 4 10/21/2012 6:10 PM

comparable set of people that do not have cancer to measure the excess mortality that is associated with a cancerdiagnosis.
Stage distributionStage provides a measure of disease progression, detailing the degree to which the cancer has advanced. Twomethods commonly used to determine stage are AJCC and SEER Summary Stage. The AJCC method (seeCollaborative Staging Method) is more commonly used in the clinical settings, while SEER has strived to provideconsistent definitions over time with their Local/Regional/Distant staging.
Lifetime riskThe probability of developing cancer in the course of one's lifespan. Lifetime risk may also be discussed in terms ofthe probability of developing or of dying from cancer. Based on cancer rates from 2007 to 2009, it was estimated thatmen had about a 45 percent chance of developing cancer in their lifetimes, while women had about a 38 percentchance.
Probability of developing cancerThe chance that a person will develop cancer in his/her lifetime.
PrevalenceThe number of people who have received a diagnosis of cancer during a defined time period, and who are alive onthe last day of that period. Most prevalence data in SEER is for limited duration because information on casesdiagnosed before 1973 is not generally available.
Myeloma - SEER Stat Fact Sheets http://seer.cancer.gov/statfacts/html/mulmy.html
4 of 4 10/21/2012 6:10 PM

566 American Society of Hematology
How to treat elderly patients with multiplemyeloma: combination of therapy or sequencing
Antonio Palumbo1 and Francesca Gay1
1Divisione di Ematologia dell’Università di Torino, Azienda Ospedaliera Universitaria S. Giovanni Battista,Torino, Italy
Patients with multiple myeloma aged older than 65 years have traditionally received an oral regimencombining melphalan and prednisone (MP). The introduction of novel agents, such as immunomodulatorydrugs and proteasome inhibitors, has substantially changed the treatment paradigm of this disease. Fiverandomized phase III studies, comparing MP plus thalidomide (MPT) versus MP, have shown that MPTincreased time to progression (TTP); however, only two of these five studies showed improvement inoverall survival (OS). One randomized study has shown that MP plus bortezomib (MPV) increases bothTTP and OS compared with MP. Both MPT and MPV are now regarded as the new standards of care forelderly patients. Other promising results have been reported with MP plus lenalidomide or lenalidomideplus dexamethasone, or the combination of cyclophosphamide, thalidomide, and dexamethasone.Reduced-intensity transplantation can be an option for some patients, especially when novel agents areincorporated into pre-transplant induction and post-transplant consolidation. For patients aged older than75 years a gentler approach should be used, and doses of standard MPT or MPV should be reduced. Anaccurate management of treatment-related adverse events with prompt dose-reduction can greatlyreduce the rate of early discontinuation and significantly improve treatment efficacy. The choice of treat-ment should be tailored according to the patient’s biologic age and co-morbidities, and the expectedtoxicity profile of the regimen.
Epidemiology
M ultiple myeloma (MM) is an incurable plasmacell disorder that comprises 1% of all cancer and10% of hematologic neoplasms. MM was
estimated to account for 19,920 new cancer cases in theUSA in 2008, including 11,190 cases in men, 8,730 casesin women, and 10,690 deaths overall.1 Incidence increasesgreatly with age: the median age at diagnosis is 70 years,with 35% of patients younger than 65 years, 28% aged 65to 74 years, and 37% older than 75 years.2,3 The number ofgeriatric patients is expected to rise over time because ofthe increased life-expectancy of the normal population.
Diagnosis and Treatment StrategyRecognition of organ damage and its correlation with MMis the first step to correctly identify either a) symptomaticMM or b) evolution of monoclonal gammopathy ofundetermined significance (MGUS) or smoldering MM tosymptomatic MM. Appropriate therapy should then bestarted (Table 1). Early intervention has shown no benefitin the treatment of asymptomatic MM.4 Patients withsymptomatic MM should be treated immediately. Multiple
myeloma is defined by serum and/or urine monoclonal (M)protein (in patients with no detectable M-protein, anabnormal serum free light-chain [FLC] ratio) and bone-marrow plasma cells greater than 10%.
Symptomatic MM is defined by the evidence of end-organdamage attributable to plasma cell proliferation accordingto the CRAB criteria: C: hypercalcemia (> 11.5 mg/dL); R:renal failure (serum creatinine > 1.73 mmol/L); A: anemia(hemoglobin < 10 g/dL or > 2 g/dL below the lower limit ofnormal); and B: bone disease (lytic lesions, severeosteopenia or pathologic fractures).5
The criteria for retreatment at relapse are the same as thoseused at diagnosis, except that retreatment should be done inpatients without organ damage if the M-protein has doubledin less than 2 months.
Treatment choice should be based on scientific evidence(randomized phase III studies) and patient’s characteristics(age and presence of comorbidities). Patients older than 65years of age are generally not considered candidates fortransplantation, although an age cut off for autologous
MULTIPLE MYELOMA _____________________________________________________________________________________

Hematology 2009 567
transplantation at 65 years does not reflect standard practicethroughout the world. Since biologic age can differ fromchronologic age, biologic age should be taken into accountwhen determining whether a patient is suitable for trans-plantation. Furthermore, selected patients in good clinicalconditions can be considered for reduced-dose intensitytransplantation (melphalan 100 mg/m2, Mel100). Forpatients aged 65 to 75 years, full-dose conventional therapyis recommended, whereas a gentler approach should be usedfor patients older than 75 years or those who are youngerbut with significant comorbidities (serious heart, lung,renal, or liver dysfunction), with appropriate dose reduc-tions. Adverse events should always be graded according tothe National Cancer Institute Common Toxicity Criteria(NCI-CTC).6 Treatment should be promptly interruptedwhen serious adverse events arise (grade 4 or higherhematologic toxicities or grade 3 or higher non-hemato-logic toxicities). When serious adverse events resolvecompletely or at least to grade 1, treatment should berestarted with an appropriate reduction in dose (see sectionon “Management of adverse events” for details). Physiciansshould always consider the expected treatment-related side-
effects in choosing the appropriate treatment, especially inelderly patients with multiple comorbidities.
The role of prognostic factors in the choice of therapy isstill controversial. Patients with symptomatic myeloma arecategorized according to disease stage, on the basis of theInternational Staging System (ISS) that defines three riskgroups: stage I with median survival of 62 months (serumβ2-microglobulin < 3.5 mg/L and serum albumin ≥ 35 g/L),stage II with median survival of 44 months (serum β2-microglobulin > 3.5 mg/L and serum albumin < 35 g/L orserum β2-microglobulin 3.5-5.5 mg/L), and stage III withmedian survival of 29 months (serum β2-microglobulin ≥5.5 mg/L).7 Serum FLC ratio incorporated into the ISS canimprove the risk stratification.8,9 Cytogenetics and fluores-cent in-situ hybridization (FISH) can be used to detectchromosomal abnormalities. Of FISH-based abnormalities,patients with isolated deletion 13 (del13) do not have a worseoutcome, although del13 associated with 17p deletion (del17)or t(4;14) are associated with poorer outcomes. With use ofFISH, del17 or t(4;14) or t(14;16) are associated with pooreroutcome, t(11;14) does not have negative outcome, and
Table 1. Plasma cell–related disorder diagnostic criteria.
Diagnostic criteria: all three required
Symptomatic multiple myeloma (MM) 1) Monoclonal plasma cells in the bone marrow ≥ 10% and/or presence of a biopsy-provenplasmacytoma
2) Monoclonal protein present in the serum and/or urine*3) Myeloma-related organ dysfunction (≥ 1)†
[C] Calcium elevation in the blood (serum calcium >10.5 mg/L or upper limit of normal)[R] Renal insufficiency (serum creatinine >2 mg/dL)[A] Anemia (hemoglobin <10 g/dL or 2 g <normal)[B] Lytic bone lesions or osteoporosis‡
Monoclonal gammopathy of undetermined 1) Serum monoclonal IgG <3.0 g/dL, or serum IgA <2.0 g/dL, or urine monoclonal kappasignificance (MGUS) or lambda <1.0 g/24 hours
2) Monoclonal bone marrow plasma cells <10%3) Normal serum calcium, hemoglobin concentration, and serum creatinine
No bone lesions on full skeletal radiograph survey and/or other imaging if doneNo clinical or laboratory features of amyloidosis or light-chain deposition disease
Smouldering or indolent myeloma 1) Monoclonal protein present in the serum and/or urine2) Monoclonal plasma cells present in the bone marrow and/or a tissue biopsy3) Not meeting criteria for MGUS, MM, or solitary plasmacytoma of bone or soft tissue
Solitary plasmacytoma of bone 1) Biopsy-proven plasmacytoma of bone in one site only. Radiographs and MRI and/orFDG PET imaging (if done) must be negative outside the primary site. The primary lesionmay be associated with a low§ serum and/or urine M-component
2) The bone marrow contains <10% monoclonal plasma cells3) No other myeloma-related organ dysfunction
*If no monoclonal protein is detected (non-secretory disease), then ≥ 30% monoclonal bone marrow plasma cells and/or a biopsy-provenplasmacytoma required.†A variety of other types of end-organ dysfunctions can occasionally occur and lead to a need for therapy. Such dysfunction is sufficient tosupport classifications myeloma if proven to be myeloma related.‡If a solitary (biopsy-proven) plasmacytoma or osteoporosis alone (without fractures) is the sole defining criteria, then ≥ 30% plasma cells arerequired in the bone marrow.§Low is defined as serum IgG < 3.0 g/dL, serum IgA < 2.0 g/dL, and urine monoclonal kappa or lambda <1.0 g/24 hoursMRI indicates magnetic resonance imaging; FDG: fludeoxyglucose; PET: positron emission tomography.

568 American Society of Hematology
hyperdiploid is associated with good outcome.10,11 Prelimi-nary evidence shows that targeted therapy with bortezomib,and possibly lenalidomide, can be used to overcome theeffects of cytogenetic abnormal changes; however, since thisevidence is from a small cohort of patients, no specifictherapy should be routinely recommended on the basis ofchromosomal abnormal changes at present.
Therapeutic Options
Novel Agent-based TherapyFor many years, conventional treatment for elderly patients(older than 65 years) or young patients who are ineligiblefor high-dose therapy has been the combination of oralmelphalan and prednisone (MP). In a randomized trial, MPhas been compared with melphalan plus dexamethasone(MD), or high-dose dexamethasone or high-dose dexam-ethasone plus interferon-α. Improvement in progression-freesurvival (PFS) was reported in patients receiving melphalanas part of the induction treatment (both MP and MD) butnot in those receiving high-dose dexamethasone only.12
These findings suggest the need to incorporate an alkylat-ing agent in combination regimens including new drugs. Arandomized study comparing MP with thalidomide plusdexamethasone (TD) in patients with a median age of 72years found that TD resulted in a higher proportion of atleast very good partial response (VGPR) (26% vs 13%; P =.006) and partial response (PR) (68% vs 50%; P = .002) thandid MP. Time to progression (TTP) (21.2 vs 29.1 months; P= .2) and PFS were similar (16.7 vs 20.7 months; P = .1), butoverall survival (OS) was significantly shorter in the TDgroup than in the MP group (41.5 vs 49.4 months; P =.024). Toxicity was higher with TD, especially in patientsolder than 75 years with poor performance status. Duringthe first 12 months of therapy, the number of patients whodied from non-myeloma–related causes was twice as high inthe TD group compared with those given MP.13 In anotherstudy undertaken in younger patients (median age 64years), TD showed clear benefit in terms of both PR rate(63% vs 46%, P < .001) and TTP (22.6 vs 6.5 months, P <.001) compared with high-dose dexamethasone alone.Grade 3-4 adverse events were most frequent with TD(79.5% vs 74.2%, P < .001).14 Thalidomide improves theclinical efficacy of dexamethasone, but high-dose dexam-ethasone is too toxic in elderly patients. Although TD wasbetter than was high-dose dexamethasone alone, the lack ofbenefit when compared with MP (in terms of PFS and OS)suggests that this combination is not the best approach forpatients with newly diagnosed MM who are ineligible forhigh-dose therapy and autologous transplantation (ASCT).
Lenalidomide plus high-dose dexamethasone (RD) resultedin a higher complete response (CR) rate (22.1% vs 3.8%)
and 1-year PFS (77% vs 55%, P = .002) than did high-dosedexamethasone alone;15,16 the combination of lenalidomideplus low-dose dexamethasone (Rd) showed further benefitin terms of OS at 2 years (87% vs 75%, P < .001) andadverse events were reduced compared with RD.17 Sincethese differences were even more pronounced in patientsolder than 65 years, Rd can be regarded as a reasonableoption, although a formal comparison with MP has still notbeen done.
In elderly patients with newly diagnosed MM, five random-ized studies have compared the combination of MP plusthalidomide (MPT) with MP. In all studies MPT resulted inhigher PR (42%-76% vs 28%-48%), higher at least VGPR ornear-CR (nCR) rate (15%-47% vs 6%-8%), and longer PFS(14-27.5 vs 10-19 months) than did MP.18-23 However, onlytwo studies reported improved OS with MPT (45.3-51.6 vs27.7-32.2 months).21,22 These data lend support to the use ofMPT as the standard of care. Thalidomide therapy wasgenerally well tolerated, even in patients aged 75 years andolder,22 although the MPT regimen was associated with asignificantly higher incidence of grade 3–4 non-hemato-logic adverse events, including neurologic adverse events,infections, cardiac toxicity, and deep-venous thrombosis(DVT). After the introduction of prophylactic enoxaparin,the incidence of DVT was substantially lowered from 20%to 3%.19 Antithrombotic prophylaxis is recommended whenMPT is used, although which is the best thrombo-prophylaxis to use in these patients is debated. To addressthis issue, the Italian Myeloma Network GIMEMA designeda phase III study to prospectively investigate the efficacyand safety of low-molecular-weight heparin (LMWH), low-fixed-dose warfarin (1.25 mg per day), or low-dose aspirinas prophylaxis for venous thromboembolism (VTE) innewly diagnosed patients with MM, who were randomlyassigned to receive primary induction therapy with thalido-mide-containing regimens. Patients at risk of VTE wereexcluded from the study. The risk of VTE was 3.9% withlow-fixed-dose warfarin, 4.5% with LMWH, and 5.5% withaspirin. No significant relation was recorded between thefrequency of VTE and thromboprophylaxis, inductiontreatments, or age of patients. In patients at standard risk ofVTE, LMWH, warfarin, and aspirin are likely to be aneffective thromboprophylaxis.24 The duration of MPtreatment should be limited to 6 to 9 cycles; prolongedexposure to melphalan induces thrombocytopenia thathinders the delivery of subsequent effective salvage regimens.
A randomized trial comparing the combination ofbortezomib plus MP (VMP) with standard MP reported asignificant improvement in PR (71% vs 35%), CR rate (30%vs 4%; P < .001), TTP (24 months vs 16.6 months, P <.001), and OS at 3 years (72% vs 59%, P = .0032) with the

Hematology 2009 569
VMP regimen. This superiority was also recorded inpatients older than 75 years. The incidence of peripheralneuropathy (13% vs 0%), gastrointestinal complications(20% vs 5%), and fatigue (8% vs <1%) was higher withVMP than with MP. The number of patients with herpeszoster infection was also higher in patients given VMP thanin those given MP (14% vs 4%), but the frequency droppedto 3% in those who received acyclovir prophylaxis.25, 26
In a study comparing VMP with the regimen of bortezomib,thalidomide, and prednisone (VTP), PR, TTP, and OS didnot differ significantly, but VTP had more grade 3-4 non-hematologic adverse events than did VMP, including cardiactoxicity (8.5% vs 0%, P < .001), thromboembolic events (4%vs <1%, P = not significant [NS]), and peripheral neuropa-thy (9% vs 5%, P = NS), resulting in a higher rate oftreatment discontinuation (17% vs 8%, P = .03). Patientsgiven VMP had a higher rate of neutropenia (37% vs 21%,P = .003), thrombocytopenia (22% vs 12%, P = .03), andinfections (7% vs <1%, P = .01) than did those given VTP. 27
Although equally effective, VMP was better tolerated thanwas VTP.
The first randomized study comparing a four-drug combina-tion including MP plus bortezomib and thalidomide(VMPT) with VMP reported higher rates of VGPR (55% vs45%, P < .001) and CR (39% vs 21%, P < .001) withVMPT; however, longer follow-up is needed to assess theeffects of both regimens on PFS and OS. The incidence ofthe most common adverse events (neutropenia, thrombocy-topenia, peripheral neuropathy, and infections) was similarin both groups. When the standard twice-weekly infusion ofbortezomib (1.3 mg/m2 on days 1, 4, 8, and 11) was reducedto a weekly schedule (1.3 mg/m2 on days 1, 8, 15, 22), theincidence of grade 3-4 peripheral neuropathy was signifi-cantly reduced from 24% to 6% in the VMPT group andfrom 14% to 2% in the VMP group; the incidence of CRwas reduced from 27% to 20% in the VMP group but not inthe VMPT group (36% vs 39%).28 If longer follow-upproves no decrease in survival despite dose reduction, theonce-weekly infusion may be considered an option forpatients older than 75 years and in younger patients whohave grade 1 or higher peripheral neuropathy.
Cyclophosphamide, another alkylating agent, has beenassessed in combination with thalidomide. In the MedicalResearch Council (MRC) Myeloma IX trial, the combina-tion of cyclophosphamide (500 mg on day 1, 8, and 15every 3 weeks) plus TD (CTD) was compared with standardMP in 900 patients. Patients given CTD showed higher ratesof PR (82% vs 49%) and CR (23% vs 6%) than did thosegiven MP. Unfortunately, data for PFS duration are not yetavailable because of the short follow-up of the trial. If PFS is
better with CTD than with MP, CTD should be regarded as analternative standard of care for elderly patients.29
The combination of melphalan, prednisone, andlenalidomide (MPR) has been investigated in a phase I/IIstudy. Patients given the maximum tolerated dose (MTD:0.18 mg/kg melphalan, 2 mg/kg prednisone, and 10 mglenalidomide) achieved a PR rate of 81%, including 47.6%at least VGPR and 24% CR; median TTP and PFS were 28.5months, and 2-year OS was 90.5%.30,31 Grade 3 or 4 neutro-penia was reported in 52.4% of patients, and 42.3% ofpatients required administration of granulocyte-colonystimulating factor (G-CSF). Grade 3 and 4 non-hematologicadverse effects were mild and included febrile neutropenia(9.5%), skin rash (9.5%), and thromboembolism (4.8%).This combination is being assessed in an internationalrandomized trial comparing MPR with MP. If this studyreports improvement in PFS, another standard of care willbe available for elderly patients.
Table 2 summarizes the efficacy of the main treatmentregimens, and Table 3 summarizes the most frequentadverse events.
Reduced-intensity Transplantation in ElderlyPatientsElderly patients or patients with significant comorbiditiesare generally not eligible for standard melphalan 200 mg/m2 followed by ASCT. Two randomized studies comparedintermediate Mel100 plus reduced-intensity ASCT withMP. In one study including patients aged 65 to 70 years,ASCT was better than was MP in terms of both event-freesurvival (EFS) and OS.32 In another study, includingpatients aged 65 to 75 years, reduced-intensity ASCTinduced a response rate better than MP and fairly similar toMPT, with no difference for PFS and OS. MPT was associ-ated with a significant improvement in survival and asignificantly lower extra-hematologic toxicity than wasASCT.21 These data suggest that patients aged 65 to 70years can successfully be treated with Mel100, but thisregimen is too toxic for those aged 70 to 75 years and MPTwould be more effective.
The efficacy of bortezomib, pegylated liposomal doxorubi-cin, and dexamethasone (PAD) induction therapy beforereduced-intensity ASCT, followed by consolidation withlenalidomide and prednisone (LP), and maintenance withlenalidomide alone (L) was assessed in patients aged 65 to75 years. The CR rate was 13% after PAD, 43% afterMel100, and 73% after LP-L consolidation-maintenancetherapy. These data suggest that this approach, incorporat-ing bortezomib as induction and lenalidomide as consoli-dation-maintenance treatment, improves response rate by

570 American Society of Hematology
Table 2. Efficacy of regimens used as front-line treatment in elderly patients with multiple myeloma.
≥ PR, PFS/EFS/Regimen N CR, % % TTP, % OS, % Study
MPT Mel: 4 mg/m2 days 1–7 129 16 76 50 at 22 mo 50 at 45 mo Palumbo et al19,20
Pdn: 40 mg/m2 days 1–7for six 4-week cyclesThal: 100 mg/day until PD
MPT Mel: 0.25 mg/kg days 1–4 125 13 76 50 at 28 mo 50 at 52 mo Facon et al21
Pdn: 2 mg/kg days 1–4Thal: 400 mg/dayfor 12 6-week cycles
MPT Mel: 0.25 mg/kg days 1–4 113 7 62 50 at 24 mo 50 at 45 mo Hulin et al22
Pdn: 2 mg/kg days 1–4Thal: 100 mg/dayfor 12 6-week cycles
MPT Mel: 0.25 mg/kg days 1–4 182 6 42 50 at 20 mo 50 at 29 mo Gulbrandsen et al18†Pdn: 100 mg days 1–4Thal: 200-400 mg/dayin a 6-week cycle until plateauThal: 200 mg/day until diseaseprogression
MPT Mel: 0.25 mg/kg 165 2 66 50 at 14 mo 50 at 37 mo Wijermans et al23†Pdn: 1 mg/kg days 1–5Thal: 200 mg/day for eight4-week cycles, followed byThal: 50 mg/day until diseaseprogression
VMP Mel: 9 mg/m2 days 1–4 344 30 71 50 at 24 mo 72 at 36 mo S Miguel et al25,26†Pdn: 60 mg/m2 days 1–4Bor: 1.3 mg/m2 days1,4,8,11,22,25,29,32 for thefirst four 6-week cycles; days1,8,15, 22 for the subsequentfive 6-week cycles
VMP Mel: 9 mg/m2 days 1–4 177 20 82 70 at 36 mo 87 at 36 mo Palumbo et al28†Pdn: 60 mg/m2 days 1–4Bor: 1.3 mg/m2 days 1,8,15,22Thal: 50 mg days 1–42for nine 5-week cycles
VMP Mel: 9 mg/m2 days 1-4 130 22 81 72 at 24 mo 88 at 24 mo Mateos et al27†Pdn: 60 mg/m2 days 1-4Bor: 1.3 mg/m2 twice weekly(days 1, 4, 8, 11; 22, 25, 29 and 32)for one 6-week cycle, followed byonce weekly (days 1, 8, 15 and 22)for five 5-week cycles
VTP Thal: 100 mg/day 130 27 81 65 at 24 mo 93 at 24 mo Mateos et al27†Pdn: 60 mg/m2 days 1–4Bor: 1.3 mg/m2 twice weekly(days 1, 4, 8, 11; 22, 25, 29, and 32)for one 6-week cycle, followed by onceweekly (days 1, 8, 15, and 22)for five 5-week cycles
CTD Ctx: 500 mg days 1,8,15 450 23 82 ND ND Morgan et al29
Thal: 100-200 mg/dayDex: 40 mg days 1–4, 12–15in a 3-week cycles
Table continues on next page

Hematology 2009 571
Table 2. Continued from previous page.
≥≥≥≥≥ PR, PFS/EFS/Regimen N CR, % % TTP, % OS, % Study
VMPT Mel: 9 mg/m2 days 1–4 152 39 87 74 at 36 mo 88 at 36 mo Palumbo et al28†Pdn: 60 mg/m2 days 1–4Bor: 1.3 mg/m2 days 1,8,15,22Thal: 50 mg days 1–42for nine 5-week cyclesfollowed by Bor: 1.3 mg/m2
every 15 days and Thal: 50mg/day as maintenance
MPR Mel: 0.18-0.25 mg/kg days 1–4 54 24 81 80 at 24 mo 91 at 24 mo Palumbo et al30,31†Pdn: 2 mg/kg days 1–4for nine 4-week cyclesLen: 5-10 mg days 1–21 untilrelapse or progressive disease
Rd Len: 25 mg days 1–21 220 ND 70 ND 87 at 24 mp Rajkumar et al17
Dex: 40 mg days 1, 8, 15, 22in a 4-week cycles
†Updated information was presented at the meetings of the American Society of Clinical Oncology, European Haematology Association andAmerican Society of Hematology congress.N indicates number of patients; CR, complete response; PR, partial response; PFS, progression-free survival; EFS, event-free survival; TTP, timeto progression; OS, overall survival; Mel, melphalan; Pdn, prednisone; Thal, thalidomide; Bor, bortezomib; Len, lenalidomide; Ctx,cyclophosphamide; MPT, melphalan-prednisone-thalidomide; VMP, bortezomib-melphalan-prednisone; VTP, bortezomib-thalidomide-prednisone; VMPT, bortezomib-melphalan-prednisone-thalidomide; CTD, cyclophosphamide-thalidomide-dexamethasone; MPR, melphalan-prednisone-lenalidomide; Rd, lenalidomide- low-dose dexamethasone; ND, not determined.
Table 3. Safety (grade 3-4 adverse events) of regimens used as front-line treatment in elderly patients withmultiple myeloma.
Thrombo- PeripheralRegimen N Neutropenia, % cytopenia, % Infection, % neuropathy, % VTE, % Study
MPT 129 16 3 10 8 9 Palumbo et al19,20
MPT 125 48 14 13 6 12 Facon et al21
MPT 113 23* ND ND 20* 6 Hulin et al22
MPT 165 ND ND 14 9 3 Wijermans et al23†
VMP 344 40 38 11 13 1 S Miguel et al25,26†
VMP 177 28 17 9 2 2 Palumbo et al28†
VMP 130 37 22 7 5 <1 Mateos et al27†
VTP 130 21 12 <1 9 4 Mateos et al27†
VMPT 152 32 21 13 6 3 Palumbo et al28†
CTD 450 ND ND ND ND ND Morgan et al29
MPR 54 52 23 10 0 5 Palumbo et al30,31†
*Grade 2-4.†Updated information was presented at the meeting (American Society of Clinical Oncology, European Haematology Association and AmericanSociety of Hematology congress).....N indicates number of patients; MPT, melphalan-prednisone-thalidomide; VMP, bortezomib-melphalan-prednisone; VTP, bortezomib-thalidomide-prednisone: VMPT, bortezomib-melphalan-prednisone-thalidomide; CTD, cyclophosphamide-thalidomide-dexamethasone; MPR,melphalan-prednisone-lenalidomide; ND, not determined.

572 American Society of Hematology
taking advantage of a sequential exposure to differentdrugs. Infections were the most frequent non-hematologicadverse event, occurring mainly during PAD induction(16.6%) and Mel100 transplantation (27.1%).Lenalidomide consolidation and maintenance was welltolerated, and the absence of cumulative or persistentneutropenia and/or cumulative thrombocytopenia togetherwith the absence of peripheral neuropathy, further lendssupport to its use as maintenance agent.33
MaintenanceMaintenance therapy has the potential to provide newtreatment options for patients with MM. Four differentrandomized studies explored the role of thalidomidemaintenance after ASCT and all showed improvement inPFS in patients who received thalidomide; OS advantagewas reported in three of the four studies.34-37 The mainreason for thalidomide discontinuation was the occurrenceof peripheral neuropathy that restricted the long-term use ofthis drug. Thus thalidomide is regarded as a more suitableagent for consolidation treatment rather than maintenancetherapy. Because of its lack of neuropathy, lenalidomideseems the ideal candidate for an effective maintenanceapproach. No studies have investigated the efficacy ofmaintenance therapy in elderly patients, and the use ofmaintenance therapy after induction with MP or anotherregimen is unknown. Ongoing randomized trials will definethe role of maintenance therapy with novel agents.
Treatment StrategyDifferent treatment options are now available for elderlypatients, and physicians have the opportunity to choosetreatment regimens according to patient characteristics. Theefficacy of these new regimens should be balanced againsttheir higher toxicity. For example, for patients with a highrisk of thromboembolism, MPV should be the preferredoption; in those with pre-existing peripheral neuropathy,MPR should be considered; whereas in those with renalfailure, MPV or MPT are safer and well tolerated, althoughlenalidomide can be used with appropriate dose reduction.In a fragile population of very elderly patients (≥ 75 years)or younger patients with significant comorbidities, such aslung, heart, liver, or kidney disfunction, all these regimenscan be used but lower doses of thalidomide (100 mg or even50 mg every other day), bortezomib (weekly schedule), andlenalidomide (15-10 mg or even 5 mg) would be recom-mended on the basis of clinical experience of respectedauthorities38 (Table 4). MPT should be considered whencosts are a concern. Furthermore, compliance is an impor-tant factor to consider, especially for elderly patients, andthe advantages of oral treatment should be balanced againstthose of intravenous treatment. Oral treatment can be moreconvenient and easy, but the patient must be able to carefully
follow the prescription; intravenous treatment is moreinvasive and often requires several admissions to hospital.
Although no randomized clinical trials have shown theadvantage of a tailored treatment approach that considersgenetic risk when treatment is decided, clinically appli-cable tests need to be developed to identify patients withmore aggressive disease. The Mayo Clinic Group proposeda cytogenetic-based risk classification system: patients withdel17p, t(14;16), t(4;14), del13, hypodiploidy by karyo-type, or a high plasma cell labeling index (> 3%) areregarded as at high risk; and those with t(11;14), t(6;14), orhyperdiploid karyotype are regarded as at standard risk. Onthe basis of this algorithm, a regimen such as MPT shouldbe considered in patients who are not eligible for transplan-tation but who have low-risk disease, whereas MPV shouldbe considered for those at high risk.39 Since these regimenshave not yet been directly compared, randomized trials areneeded to lend support to these recommendations beforethese can be applied to standard clinical practice.
Management of Side Effects
Hematologic ToxicityA common symptom of MM is myelosuppression, espe-cially anemia, whereas thrombocytopenia tends to appear inend-stage disease. Neutropenia is a common side effect oflenalidomide and alkylating agents, as well as thrombocy-topenia, which is also fairly common in patients treatedwith bortezomib. Supportive care and dose modificationsare needed to manage myelosuppression.
Table 4. Age-adjusted dose reduction.
Furtherdose
65–75 years >75 years reduction
Dexamethasone 40 mg 20 mg 10 mgweekly
Melphalan 0.25 mg/kg 0.18 mg/kg 0.13 mg/kgdays 1–4
Thalidomide per day 200 mg 100 mg 50 mg
Lenalidomide 25 mg 15 mg 10 mg(in combinationwith dexamethasone)days 1–21
Lenalidomide 10 mg 5 mg 5 mg every(in combination other daywith melphalanplus prednisone)days 1–21
Bortezomib 1.3 mg/m2 1.3 mg/m2 1.0 mg/m2
twice-weekly weekly weekly

Hematology 2009 573
NeutropeniaThe greatest concern with neutropenia is the occurrence ofinfections. The use of G-CSF is a safe and effective methodto decrease or prevent the occurrence or severity of neutro-penia. Treatment should be withheld in case of grade 4neutropenia (neutrophilic count < 500/mm3) despite G-CSFadministration. When the adverse event resolves to grade 2(neutrophilic count ≥ 1000/mm3), treatment can be reintro-duced with dose reduction at the start of the next cycle.Prophylaxis with G-CSF is also recommended for theprevention of febrile neutropenia in patients at high risk onthe basis of their age, medical history, and disease character-istics, and the myelotoxicity of the chemotherapy regimen.
AnemiaMyeloma-related anemia generally improves with diseaseresponse to therapy. Erythropoiesis-stimulating agents(ESAs; epoetin and darbepoetin) can be used to treatchemotherapy-associated anemia, and iron supplements canimprove the effectiveness of treatment. ESA treatment isgenerally recommended when the hemoglobin concentra-tion is less than 9 g/dL; however, treatment can beginearlier (hemoglobin 10 to 12 g/dL) for patients with heartdisease or those who have difficulties undertaking regulardaily activities. The ESA dose should be adjusted tomaintain a hemoglobin concentration of 11 to 12 g/dL toavoid blood transfusion and anemia-related symptoms.Hemoglobin concentration greater than 12 g/dL in patientswith cancer can create serious health problems, with anincreased risk of thrombosis. For patients at high risk fordeveloping blood clots, the risks of these drugs need to beweighed against the benefits.
ThrombocytopeniaTreatment should be withheld in case of grade 4 thromb-ocytopenia (platelet count < 25,000/mm3). When theadverse event resolves to at least grade 2 (platelet count ≥50,000/mm3) treatment can be reintroduced, but dose of themyelotoxic drug needs to be appropriately reduced.
Renal FailureRenal impairment is common in patients with MM. Factorsinvolved in the pathogenesis of renal failure include thecapacity of the light-chain component of the immunoglo-bulin to cause proximal tubular damage, dehydration,hypercalcemia, hyperuricemia, infections, and use ofnephrotoxic drugs. Doses of agents such as thalidomide andbortezomib need no modification in the context of renaldysfunction. Lenalidomide can be used, but hematologicfunction should be monitored closely, especially in theearly cycles. Dose reductions are mandatory on the basis ofcreatinine clearance (CLcr): if CLcr is between 30 and 60mL/min, the recommended dose is 10 mg per day; if CLcr is
less than 30 mL/min but the patient does not requiredialysis, the recommended dose is 15 mg every other day;and if CLcr is less than 30 mL/min and the patient requiresdialysis, the dose is 5 mg per day administered after dialysisonly on dialysis days.
Peripheral NeuropathyPeripheral neuropathy is a common adverse event withbortezomib and thalidomide therapy. Since no pharmaco-logic drugs are available at present to effectively relieveneuropathic symptoms, prompt dose reductions andmodifications to the treatment schedule are the mosteffective means to treat peripheral neuropathy. Forbortezomib, a dose reduction to 1.0 mg/m2 is recommendedfor grade 1 with pain or grade 2 peripheral neuropathy; doseinterruption until peripheral neuropathy resolves withrestart at 0.7 mg/m2 is recommended for grade 2 with pain orgrade 3 peripheral neuropathy; and treatment discontinua-tion is recommended for grade 4 peripheral neuropathy.40
For thalidomide, patients should be taught to recognizeperipheral neuropathy and to immediately decrease thedose or to discontinue the drug when sensory paresthesia iscomplicated by pain, motor deficiency, or an interferencewith daily function. A practical rule is to maintain theassigned dose if neuropathy is grade 1, to decrease by 50%if neuropathy is grade 2, to discontinue if neuropathy isgrade 3, and to eventually resume thalidomide at a de-creased dose if neuropathy improves to grade 1.41
DVTThe choice of thromboprophylaxis in patients treated withimmunomodulatory agents depends on the risk of VTEassociated with a specific regimen. The following riskfactors should be considered when determining the form ofthromboprophylaxis: individual risk factors (age, obesity,history of VTE, central-venous catheter, comorbidities suchas cardiac disease, chronic renal disease, diabetes, infec-tions, immobilization, surgical procedures, and inheritedthrombophilia), myeloma-related risk factors (diagnosis andhyperviscosity), and therapy-related risk factors (high-dosedexamethasone, doxorubicin, or multiagent chemothera-pies). Aspirin is recommended for patients with no riskfactors or those with one individual or myeloma-related riskfactor. LMWH or full-dose warfarin are recommended forpatients with at least two individual or myeloma-relatedrisk factors and should be considered in all patientsreceiving high-dose dexamethasone or doxorubicin ormultiagent chemotherapy, independently from the presenceof additional risk factors.42 Table 5 summarizes recommen-dations for the most frequent adverse events related to theuse of novel agents.

574 American Society of Hematology
Table 5. Management of adverse events in patients with multiple myeloma treated with novel agents.
Suspectedantimyeloma agent Management Dose modification
Hematologic toxicityHematologic toxicityHematologic toxicityHematologic toxicityHematologic toxicity
Neutropenia Lenalidomide and G-CSF until neutrophil recovery in case 25%-50% reductioncombinations of uncomplicated grade 4 toxicity or
grade 2-3 adverse events complicatedby infection
Thrombocytopenia Bortezomib, lenalidomide, Platelet transfusion if grade 4 adverse 25%-50% reduction in case ofand combinations events grade 3-4 adverse event
Anemia Bortezomib, lenalidomide, Erythropoietin or darbepoietin in case of 25%-50% reduction in case ofand combinations hemoglobin concentration ≤ 10 g/dL grade 3-4 adverse event
Extra-hematologic toxicityExtra-hematologic toxicityExtra-hematologic toxicityExtra-hematologic toxicityExtra-hematologic toxicity
Infection All the agents Trimetoprin-cotrimoxazole for Pneumocystis 25%-50% reduction in case ofcarinii prophylaxis during high-dose grade 3-4 adverse eventdexamethasone. Acyclovir or valacyclovirfor HVZ prophylaxis during bortezomib-based therapy
Neurotoxicity Bortezomib, thalidomide, Neurological assessment before and Bortezomib: 25%-50% reduction for gradeand combinations during treatment. Consider symptomatic 1 with pain or grade 2 peripheral
treatment with gabapentin, pregabalin, neuropathy; dose interruption untilvitamin B complex compounds, amitryptilin peripheral neuropathy resolves to grade 1or L-carnitina (uncontrolled trials) or better with restart at 50% dose reduction
for grade 2 with pain or grade 3 peripheralneuropathy; treatment discontinuation forgrade 4 peripheral neuropathy. Thalidomide:50% reduction for grade 2 neuropathy;discontinuation for grade 3; resumeThalidomide at a decreased dose ifneuropathy improves to grade 1
Cutaneous toxicity Thalidomide, lenalidomide Steroids and antihistamines Interruption in case of grade 3-4 adverseand combinations events.
50% reduction in case of grade 2adverse events.
Gastrointestinal Thalidomide, bortezomib, Appropriate diet, laxatives, exercise, Interruption in case of grade 3-4 adversetoxicity and combinations hydration, antidiarrheic drugs events.
50% reduction in case of grade 2adverse events.
Thrombosis Thalidomide, lenalidomide, Aspirin 100-325 mg if no or one Drug temporary interruption and fulland combinations individual/myeloma thrombotic risk factor is anticoagulation, then resume treatment.
present. LMWH or full-dose warfarin if twoor more individual/myeloma risk factors arepresent and in all patients who receivehigh-dose dexamethasone or doxorubicinor multiagent chemotherapy
Renal toxicity Lenalidomide Correct precipitant factors (dehydration, Reduce dose according to creatininehypercalcemia, hyperuricemia, urinary clearance:infections, and concomitant use of if 30-60 mL/min: 10 mg/day,nephrotoxic drugs) if < 30 mL/min without dialysis needing:
15 mg every other day;if < 30 mL/min and dialysis: 5 mg/dayafter dialysis on dialysis day
G-CSF indicates granulocyte colony-stimulating factor; HVZ, herpes-varicella-zooster; LMWH, low-molecular-weight heparin.
Hematology 2009 575
ConclusionsThe combination of conventional chemotherapy or low-dose dexamethasone with new drugs has substantiallychanged the treatment paradigm of patients with MM.Randomized studies have shown that MPT and MPV areboth better than MP and can now be regarded as thestandard of care for elderly patients. Preliminary resultssuggest that Rd, CTD, or MPR could be valid alternativeoptions. The choice of the best treatment strategy for eachpatient should be based on scientific randomized studiesand tailored to account for the patient’s biologic age,comorbidities, and the expected toxicity profile of differentregimens.
DisclosuresConflict-of-interest disclosure: AP received honoraria fromCelgene and Janssen-Cilag. FG declares no competingfinancial interests.Off-label drug use: Thalidomide, lenalidomide, bortezomib.
CorrespondenceAntonio Palumbo, MD, Divisione di Ematologiadell’Università di Torino, Azienda Ospedaliera S. GiovanniBattista, Via Genova 3, 10126 Torino, Italy; Phone:+390116635814; Fax: +390116963737; e-mail:[email protected]
References1. Jemal A, Siegel R, Ward E, et al. Cancer statistics. CA
Cancer J Clin. 2008;58:71-96.2. Ferlay J, Bray F, Pisani P, et al. GLOBOCAN 2002
Cancer Incidence, Mortality and Prevalence World-wide. IARC CancerBase No. 5 Version 2.0. Lyon: IARCPress; 2004.
3. Ries LAG, Eisener MP, Kosary CL, et al. NationalCancer Institute. SEER Cancer Statistics Review, 1975-2001 http://seer.cancer.gov//csr/1975_2001. Accessedon 7 September 2004.
4. Riccardi A, Mora O, Tinelli C, et al. Long-term survivalof stage I multiple myeloma given chemotherapy justafter diagnosis or at progression of disease: amulticentre randomized study. Br J Cancer.2000;82:1254-1260.
5. Kyle RA, Rajkumar SV. Criteria for diagnosis, staging,risk stratification and response assessment of multiplemyeloma. Leukemia. 2009;23:3-9.
6. National Cancer Institute. Common TerminologyCriteria for Adverse Events, v3.0, (CTCAE) http://ctep.cancer.gov/protocolDevelopment/electronic_applications/ctc.htm#ctc_v30
7. Greipp PR, San Miguel J, Durie BG, et al. Internationalstaging system for multiple myeloma. J Clin Oncol.2005;23:3412-3420.
8. Jakob C, Sterz J, Liebisch P, et al. Incorporation of thebone marker carboxy-terminal telopeptide of type-1collagen improves prognostic information of theInternational Staging System in newly diagnosedsymptomatic multiple myeloma. Leukemia.2008;22:1767-1772.
9. Snozek CL, Katzmann JA, Kyle RA, et al. Prognosticvalue of the serum free light chain ratio in newlydiagnosed myeloma: proposed incorporation into theinternational staging system. Leukemia.2008;22:1933-1937.
10. Fonseca R, Barlogie B, Bataille R, et al. Genetics andcytogenetics of multiple myeloma: a workshop report.Cancer Res. 2004;64:1546-1558.
11. Dewald GW, Therneau T, Larson D, et al. Relationshipof patient survival and chromosome anomaliesdetected in metaphase and/or interphase cells atdiagnosis in myeloma. Blood. 2005;106:3553-3558.
12. Facon T, Mary JY, Pégourie B, et al. Dexamethasone-based regimens versus melphalan-prednisone forelderly multiple myeloma patients ineligible for high-dose therapy. Blood. 2006;107:1292-1298.
13. Ludwig H, Hajek R, Tóthová E, et al. Thalidomide-dexamethasone compared with melphalan-predniso-lone in elderly patients with multiple myeloma. Blood.2009;113:3435-3442.
14. Rajkumar SV, Rosiñol L, Hussein M, et al. Multicenter,randomized, double-blind, placebo-controlled study ofthalidomide plus dexamethasone compared withdexamethasone as initial therapy for newly diagnosedmultiple myeloma. Clin Oncol. 2008;26:2171-2177.
15. Zonder JA, Crowley JJ, Bolejack V, et al. A randomizedSouthwest Oncology Group study comparing dexam-ethasone (D) to lenalidomide + dexamethasone (LD) astreatment of newly-diagnosed multiple myeloma(NDMM): impact of cytogenetic abnormalities onefficacy of LD, and updated overall study results[abstract]. J Clin Oncol. 2008;26:8521.
16. Zonder JA, Crowley J, Hussein MA, et al. Superiority oflenalidomide (Len) plus high-dose dexamethasone(HD) compared to HD alone as treatment of newly-diagnosed multiple myeloma (NDMM): results of therandomized, double-blinded, placebo-controlledSWOG trial S0232 [abstract]. Blood. 2007;110:77.
17. Rajkumar SV, Jacobus S, Callander N, et al. Random-ized trial of lenalidomide plus high-dose dexametha-sone versus lenalidomide plus low-dose dexametha-sone in newly diagnosed myeloma (E4A03), a trialcoordinated by the Eastern Cooperative OncologyGroup: analysis of response, survival, and outcome wi[abstract]. J Clin Oncol. 2008;26:8504.
18. Gulbrandsen N, Waage A, Gimsing P, et al. Arandomised placebo controlled study with melphalan/

576 American Society of Hematology
prednisone vs melphalan/prednisone/thalidomide:quality of life and toxicity [abstract]. Haematologica.2008;93: 0209.
19. Palumbo A, Bringhen S, Caravita T, et al. Oralmelphalan and prednisone chemotherapy plus thalido-mide compared with melphalan and prednisone alonein elderly patients with multiple myeloma: randomisedcontrolled trial. Lancet. 2006;367:825-831.
20. Palumbo A, Bringhen S, Liberati AM, et al. Oralmelphalan, prednisone, and thalidomide in elderlypatients with multiple myeloma: updated results of arandomized controlled trial. Blood. 2008;112:3107-3114.
21. Facon T, Mary JY, Hulin C, et al. Melphalan andprednisone plus thalidomide versus melphalan andprednisone alone or reduced-intensity autologous stemcell transplantation in elderly patients with multiplemyeloma (IFM 99-06): a randomised trial. Lancet.2007;370:1209-1218.
22. Hulin C, Facon T, Rodon P, et al. Melphalan-pred-nisone-thalidomide (MP-T) demonstrates a significantsurvival advantage in elderly patients 75 years withmultiple myeloma compared with melphalan-pred-nisone (MP) in a randomized, double-blind, placebo-controlled trial, IFM 01/01 [abstract]. Blood.2007;110:75.
23. Wijermans P, Schaafsma M, van Norden Y, et al.Melphalan + prednisone versus melphalan + pred-nisone + thalidomide in induction therapy for multiplemyeloma in elderly patients: final analysis of theDutch cooperative group HOVON 49 study [abstract].Blood. 2008;112:649.
24. Cavo M, Palumbo A, Brighen S, et al. A phase III studyof enoxaparin versus low-dose warfarin versus aspirinas thromboprophylaxis for patients with newlydiagnosed multiple myeloma treated up-front withthalidomide-containing regimens [abstract]. Blood.2008;112:3017.
25. San Miguel JF, Schlag R, Khuageva NK, et al. Updatedfollow-up and results of subsequent therapy in thephase III VISTA Trial: bortezomib plus melphalan-prednisone versus melphalan-prednisone in newlydiagnosed multiple myeloma [abstract]. Blood.2008;112:650.
26. San Miguel JF, Schlag R, Khuageva NK, et al.Bortezomib plus melphalan and prednisone for initialtreatment of multiple myeloma. N Eng J Med.2008;359:906-917.
27. Mateos MV, Oriol A, Martinez J, et al. Bortezomib(Velcade)-melphalan-prednisone (VMP) versusvelcade-thalidomide-prednisone (VTP) in elderlyuntreated multiple myeloma patients: which is the bestpartner for Velcade: an alkylating or an
immunomodulator agent? [abstract]. Blood.2008;112:651.
28. Palumbo A, Bringhen S, Rossi D, et al. A prospective,randomized, phase III study of bortezomib, melphalan,prednisone and thalidomide (VMPT) versusbortezomib, melphalan and prednisone (VMP) inelderly newly diagnosed myeloma patients [abstract].Blood. 2008;112: 652.
29. Morgan GJ, Davies FE, Owen RG, et al. Thalidomidecombinations improve response rates: results from theMRC IX Study [abstract]. Blood. 2007;110:3593.
30. Palumbo A, Falco P, Corradini P, et al. Melphalan,prednisone, and lenalidomide treatment for newlydiagnosed myeloma: a report from the GIMEMA –Italian Multiple Myeloma Network. J Clin Oncol.2007;25:4459-4465.
31. Palumbo A, Falco P, Gay F, et al. Oral melphalan,prednisone, and lenalidomide for newly diagnosedmultiple myeloma patients: kinetics of neutropenia/thrombocytopenia and time to event results [abstract].Blood. 2008;112:2768.
32. Palumbo A, Bringhen S, Petrucci MT, et al. Intermedi-ate-dose melphalan improves survival of myelomapatients aged 50 to 70: results of a randomizedcontrolled trial. Blood. 2004;104:3052-3057.
33. Palumbo A, Falco P, Gay F, et al. Bortezomib-doxorubi-cin-dexamethasone as induction prior to reducedintensity autologous transplantation followed bylenalidomide as consolidation/maintenance in elderlyuntreated myeloma patients [abstract]. Blood.2008;112:159.
34. Attal M, Harousseau JL, Leyvraz S, et al. Mainte-nance therapy with thalidomide improves survivalin patients with multiple myeloma. Blood.2006;108:3289-3294.
35. Spencer A, Prince HM, Roberts A, et al. Thalidomideimproves survivals when used after ASCT [abstract].Haematologica. 2007;92:S7b.
36. Abdelkefi A, Ladeb S, Torjman L, et al. Single autolo-gous stem-cell transplantation followed by mainte-nance therapy with thalidomide is superior to doubleautologous transplantation in multiple myeloma:results of a multicenter randomized clinical trial.Blood. 2008;111:1805-1810.
37. Barlogie B, Tricot G, Anaissie E, et al. Thalidomideand hematopoietic-cell transplantation for multiplemyeloma. N Engl J Med. 2006;354:1021-1030.
38. San-Miguel J, Harousseau J-L, Joshua D, Anderson KC.Individualizing treatment of patients with myeloma inthe era of novel agents. J Clin Oncol. 2008;26:2761-2766.
39. Dispenzieri A, Rajkumar SV, Gertz MA, et al. Treatmentof newly diagnosed multiple myeloma based on Mayo

Hematology 2009 577
Stratification of Myeloma and Risk-adapted Therapy(mSMART): consensus statement. Mayo Clin Proc.2007;82:323-341.
40. Argyriou AA, Iconomou G, Kalofonos HP. Bortezomib-induced peripheral neuropathy in multiple myeloma: acomprehensive review of the literature. Blood.2008;112:1593-1599.
41. Palumbo A, Facon T, Sonneveld P, et al. Thalidomidefor treatment of multiple myeloma: 10 years later.Blood. 2008;111:3968-3977.
42. Palumbo A, Rajkumar SV, Dimopoulos MA. Preventionof thalidomide- and lenalidomide-associated thrombo-sis in myeloma. International Myeloma WorkingGroup. Leukemia. 2008;22:414-423.

Autologous stem cell transplantation in patients of 70 years and olderwith multiple myeloma: Results from a matched pair analysis
Shaji K. Kumar,* David Dingli, Martha Q. Lacy, Angela Dispenzieri, Suzanne R. Hayman, Francis K. Buadi,S. Vincent Rajkumar, Mark R. Litzow, and Morie A. Gertz
High-dose therapy and autologous stem cell transplant (HDT) have been shown to prolong survival in multi-ple myeloma (MM) in randomized trials, but only included patients of 65 years or younger. Given the medianage at diagnosis of 66 years, it is important to have a better understanding of the outcome of transplanta-tion in the older patients. We identified 33 patients with MM, who were ‡70 years at the time of their HDT.We matched them to a group of 60 patients, 65 years or younger, (two controls for each patient), based ontime to transplant, disease status at transplant, Durie-Salmon stage, labeling index, presence of cytogeneticabnormalities, and presence of circulating plasma cells. The median age of the two groups were 55.6(range, 37.3–64.9) and 71.7 (range 70–75.8) years at transplant. Although more of the older patients receiveddose reduced melphalan, the overall response rate was similar (97% vs. 98%) as was the median time toprogression (28.5 months vs. 17.8 months, P 5 0.7) for the elderly group compared to the younger patients.The median overall survival from transplant was not reached for the elderly patient group compared to 53.2months for the younger patients, P 5 0.7. HDT is feasible in selected patients with multiple myeloma over70 years. The toxicity of transplant as well as the outcome appears comparable to younger patients.Patients with MM should not be excluded from HDT solely on the basis of their chronological age. Am. J.Hematol. 83:614–617, 2008. VVC 2008 Wiley-Liss, Inc.
IntroductionMultiple myeloma is a clonal plasma cell proliferative dis-
order that accounts for nearly 10% of all hematologicalneoplasms and 1% of all malignancies [1]. It is estimatedthat there will be 19,900 new cases of multiple myeloma inthis country in 2007 and 10,790 will die of the disease [2].The median age of onset is in the early sixties and the me-dian survival with conventional chemotherapy is 3–4 years[1,3]. The introduction of different combination chemothera-pies have not resulted in improved survival compared tomelphalan and prednisone, which was introduced morethan 30 years ago [4]. Dose intensification using high-dosechemotherapy with autologous stem cell rescue (HDT) hasshown improved response rates and survival in randomizedtrials compared to conventional therapy [5,6]. Subsequentstudies have also demonstrated a quality of life advantagefor patients undergoing stem cell transplant early in theirdisease course compared with transplant performed as sal-vage therapy at first relapse [7]. Indeed HDT has becomethe standard approach for patients with myeloma who arethought to be able to tolerate the procedure.The large clinical trials that have evaluated the role of
HDT in myeloma mostly included patients under the age of65, and it is clear from these studies that HDT confers sur-vival advantage for these patients [5,6]. However, oneneeds to take into account that the median age of patientsdiagnosed with symptomatic myeloma is around 66 years,thus precluding the ability to extend these observations foralmost half of the patients. Several studies have retrospec-tively looked at the role of HDT in patients older than 65with myeloma, however, most of these studies had fewpatients 70 years and older [8–13]. The benefits and toxic-ity of HDT in the older patients, especially those over70 years, remains unclear in comparison with their youngercounterparts who have been well studied in the prospectivetrials. Here we examine the outcome of HDT for myelomaamong patients older than 70 years of age in a case
controlled study, comparing the results to a matched groupof patients under age 65 at the time of transplant.
ResultsThe study population consisted of 93 patients who had
undergone stem cell transplant at our institution between2000 and 2005 for multiple myeloma; 33 patients were 70years or older and a matched group of 60 patients 65 yearsor younger at the time of transplant. Table I lists and com-pares the clinical and laboratory features that were used forselecting the control group of younger patients.
Baseline clinical and laboratory featuresThe baseline features of the two groups, excluding those
used for matching, are compared in Table II. There was nodifference in the gender distribution between the groups.Measure of disease burden at transplant including bonemarrow plasma cell percentage, M protein level, as well asother laboratory features such as LDH and CRP were com-parable between the two groups. Serum creatinine washigher in the elderly group, as expected given the age dis-tribution. Proportion of patients with high b2M was similarin the two groups despite the difference seen in the renal
Department of Internal Medicine, Division of Hematology, Mayo Clinic, Roch-ester, Minnesota
Contract grant sponsors: Hematologic Malignancies Program, Mayo ClinicCR20 program, ASCO Young Investigator Award, and Amgen OncologyInstitute Junior Faculty Award.
*Correspondence to: Shaji Kumar; Associate Professor of Medicine, MayoClinic, 200 First Street SW, Rochester, MN 55905.E-mail: [email protected]
Received for publication 23 August 2007; Revised 26 February 2008; Accepted3 March 2008
Am. J. Hematol. 83:614–617, 2008.
Published online 10 March 2008 in Wiley InterScience (www.interscience.wiley.com).DOI: 10.1002/ajh.21191
VVC 2008 Wiley-Liss, Inc.
American Journal of Hematology 614 http://www3.interscience.wiley.com/cgi-bin/jhome/35105

function. There was no difference between the groups interms of bone disease or in the involved immunoglobulinisotope or proportion of patients with light chain myeloma.The response to initial chemotherapy was similar in bothgroups, with the response status at transplant being similarin the two groups. The number of CD34 cells collected wasslightly lower in the elderly group, a difference that was notstatistically significant and likely a reflection of a higher tar-get for storage for future transplants in the youngerpatients. There was a difference in the type of conditioningregimens used between the two groups. Ten of the 35(30%) of the elderly group had dose reduction in their mel-phalan conditioning compared with only 5% in the youngergroup, likely reflecting a concern for age and possiblyreduced renal function.
Toxicity and engraftmentThe most common adverse reactions to stem cell infu-
sion were nausea and vomiting, hypertension or tachycar-dia and were not different between the groups. There was
a trend toward longer post-transplant hospital stay for theelderly group (8 days) compared with the younger group (3days); a difference that was not statistically significant; P 50.06 (Table III). The proportion of patients attaining WBCengraftment (as indicated by an ANC >500 for three con-secutive days) by day 15 was 94% for the elderly groupcompared to 78% for the control group; P 5 0.08. Similarly,the proportion of patients achieving a non-transfused plate-let count of over 50,000 by day 30 was similar for bothgroups (81% and 80% respectively). The most commonpost-transplant toxicities that were encountered includednausea, mucositis, diarrhea and neutropenic fever. Posttransplant bacteremia was documented in 14 (42%)patients among the elderly group compared to 27 (45%) inthe control group; P 5 0.8. The common organisms re-sponsible for bacteremia in this population included coagu-lase negative staphylococci, Streptococcus Viridans, Pseu-domonas and E. coli. One patient in the elderly group (3%)and none in the control group died of transplant relatedcauses by day 100; P 5 NS.
Disease response and survivalThe overall response rate for the entire group was 97%
for the elderly group compared to 98% for the control group(P 5 NS). Fourteen patients in the elderly group (42%) and17 patients (28%) of the control group achieved a CR; P 5NS. Twenty-two of the older patients (67%) and 40 (67%)of the matched younger patients have had disease progres-sion. Twenty-five of the older patients (76%) and 39 (65%)of the younger patients were alive at the time of currentanalysis. The estimated median follow up of the patientsfrom transplant was 27.2 months for the elderly comparedwith 38.3 months for the younger patient group. The me-dian time to progression after transplant was equivalentbetween the two groups; 28.5 months (95% CI; 13.3, 43.8)for the elderly compared with 17.8 months (95% CI; 15.1,20.6) for the younger patients (P 5 0.7, log rank test)(Fig. 1). The median overall survival from transplant wasnot reached for the elderly patient group compared with53.3 months (95% CI; 35.3, 71.3) for the younger patients,P 5 0.7 (Fig. 2). The median overall survival from diagno-sis for the elderly patients was comparable with theyounger patient group, 80.5 months vs. 87.5 months; P 50.8. No difference in the time to progression or overall sur-vival was seen between patients receiving reduced dosemelphalan for conditioning and those receiving conventionaldose of melphalan.
DiscussionThe past decade has seen significant advances in the
care of the patient with myeloma; especially the introduc-
TABLE I. Matched Baseline and Grouping Factors
Characteristics
Elderly (�70)
(n 5 33)
Median (range)
Control (�65)
(n 5 60)
Median (range) P-value
Time to transplant
(months) 6.4 (3.7–50.2) 6.3 (3.3–61.9) NS
n (%) n (%)
Durie Salmon stage
2 17 (52) 31 (52) NS
3 16 (48) 29 (48)
PCLI �1 10 (29) 20 (33) NS
Abnormal cytogenetics 8 (25) 14 (23) NS
Circulating plasma cells 17 (52) 19 (32) NS
CTX for mobilization 17 (52) 34 (57) NS
TABLE II. Baseline Features at Transplant
Characteristics
Elderly (�70)
(n 5 33)
Median (range)
Control (�65)
(n 5 60)
Median (range) P-value
Age at diagnosis (years) 71.2 (66.7–75.3) 54.3 (36.9–64.3) <0.01
Age at transplant (years) 71.7 (70–75.8) 55.6 (37.3–64.9) <0.01
M protein level (gm/dl) 0.7 (0–6.1) 1.3 (0–5.7) 0.9
LDH (U/l) 184 (92–332) 187 (74–393) 0.5
CRP (mg/dl) 0.4 (0.1–6.4) 0.4 (0.1–9.2) 0.4
BM plasma cell % 13.6 (0.2–52) 13.2 (1–78) 0.4
Creatinine (mg/dl) 1.1 (0.7–6.5) 1.0 (0.7–4.3) 0.04
CD34 collected 8.3 (3–33.5) 10 (2–27.8) 0.28
n (%) n (%)
Transplant <12 months
from diagnosis
28 (85) 48 (80) NS
Male gender 25 (76) 38 (63) 0.3
b2 microglobulin >3.5 lg/ml 11 (33) 11 (18) 0.2
Bone disease 28 (85) 45 (75) 0.3
Response to initial therapy 25 (72) 58 (80) 0.4
Relapsed/refractory disease
at transplant
15 (45) 24 (40) NS
Conditioning
Mel 200 23 (70) 57 (95) 0.001
Mel 140 10 (30) 3 (5)
TABLE III. Post-Transplant Factors
Variable
Elderly (�70)
(n 5 33)
Median (range)
Control (�65)
(n 5 60)
Median (range) P-value
Days hospitalized 8 (0–33) 3 (0–37) 0.06
n (%) n (%)
ANC > 500 by day 15 31 (94) 47 (78) 0.08
Platelets > 50,000 by day 30 25 (81) 47 (80) >0.99
Post-transplant
bacteremia incidence
14 (42) 27 (45) 0.8
Day 100 mortality 1 (3) 0 (0) 0.4
Overall response 32 (97) 57 (98) 0.9
CR 14 (42) 17 (28) 0.2
American Journal of Hematology 615

tion of novel therapies for treatment of newly diagnosedand relapsed disease. Prior to the introduction of thesenew drugs, randomized controlled trials had demonstrateda survival advantage for patients undergoing high dosetherapy and autologous stem cell transplantation [5,6].Although the new drugs have raised the question of therole of HDT in the treatment of myeloma, it is an effectivetreatment approach and remains the standard of care forpatients considered eligible to undergo the process.Although randomized trials clearly demonstrated the benefitfor HDT for patients under 65, the utility of this modality inthe older patients, especially those over 70 years has notbeen addressed in any prospective trials. It remains an im-portant question, given the proportion of patients over 70with a new diagnosis of myeloma.Trials have examined the role of high dose melphalan in
patients older than 65, but with two doses of intermediatedose melphalan (100 mg/m2) [MEL100]. One trial random-ized 194 newly diagnosed patients to either conventional
chemotherapy (six courses of oral melphalan and predni-sone) or intermediate-dose therapy (two courses of mel-phalan at 100 mg/m2 with stem cell support [14]. Whenpatients aged 65–70 were analyzed separately, the medianoverall survival was 58 months with MEL-100 comparedwith 37.2 months for the MP arm, a statistically significantdifference. However, the recently presented results of theIFM 99-06 trial, which randomized patients aged 65–75years to MP, MP plus THAL or MEL100 and stem celltransplant following two cycles of VAD did not confirm thesurvival advantage seen among elderly patients with inter-mediate dose melphalan in this trial [15].In the absence of randomized data, several retrospective
studies have examined the role of HDT in those over 65years [8,9,11,14,16–19]. Siegel et al. identified 49 patientsover age 65 from among 550 patients with MM undergoingHDT (median age, 67; range, 65–76 years)and comparedtheir outcome to that of a matched set of 49 patients under65 years. Patients were matched for cytogenetics, b2-microglobulin, C-reactive protein, albumin, and creatinineand all received high-dose melphalan-based therapy with76% of the younger and 65% of the older group completinga second transplant. Stem cell collection, engraftmentkinetics and toxicities were similar between the two groupsand the treatment-related mortality was 2% in younger and8% among older subjects. The two groups had similarevent free and overall survival. Badros et al. examined theirexperience with 70 patients over 70 years (median 72years; range, 70–82.6), of whom 34 had newly diagnosedmyeloma. Excessive mortality (16%) was noted among theinitial 25 patients and hence the remaining patientsreceived only 140 mg/m2 of melphalan. The engraftmentkinetics was comparable with those expected with a CRrate of 20% which improved to 27% for the 31 patients(44%) who went on to a tandem auto-SCT. However, boththese reports included patients on planned tandem trans-plant protocols from a single institution. Reece et al. exam-ined the data reported to the Autologous Blood and MarrowTransplant Registry and compared the outcome of 110patients �60 years (median 63; range, 60–73) with that of382 patients under 60 years (median 52; range, 30–59)[10]. Treatment-related mortality at 100 days and at 1 yearwas similar for the two groups as were the relapse rate,progression-free survival and overall survival. In anotherstudy, 22 myeloma patients over 65 years were comparedwith 79 patients treated on an identical HDT protocols. Thestem cell collection yields, engraftment and other mortalitywere similar for the two groups, while elderly patients hadmore mucositis and gastrointestinal toxicity. No differenceswere seen between the two groups in terms of responserates or overall and relapse free survival [11]. Similarresults were reached in another small study [18]. Otherstudies have suggested a shorter progression free survivalin elderly patients [20]. Although most of these studies sug-gested similar outcomes for selected older patients follow-ing HDT, outcome for patients over 70 years undergoing asingle HDT, as is the common practice, was not specificallyaddressed.In the current study, we demonstrate similar outcome for
patients older than 70 years, by comparing them to a groupof younger patients (under 65) with similar prognostic fac-tors. This matched analysis allows a better estimate of theoutcome of these patients, by eliminating the effect of dif-ferent prognostic factors that could often be biased in singlegroup retrospective studies. We did not observe any signifi-cant differences in the response rates or in the time toprogression following transplant between the two groups,despite a larger proportion of patients in the older groupreceiving reduced doses of melphalan. Similarly, the overall
Figure 2. Kaplan–Meier curves demonstrating median overall survival for the twogroups following stem cell transplantation.
Figure 1. Kaplan–Meier curves demonstrating median time to progression for thetwo groups following stem cell transplantation.
616 American Journal of Hematology

survival from diagnosis was similar for the two groups.There was a trend towards increased toxicity as reflected inthe longer hospital stay among the older patients. Datawere not available in terms of mucositis incidence and se-verity among these patients. Engraftment kinetics was simi-lar and treatment related mortality was no different in thetwo groups. Although this represents a single institution ex-perience and selects for patients tolerating the initial ther-apy and surviving to the time of transplant, the results helpin decision making when caring for an elderly patient withmyeloma.In conclusion, we demonstrate comparable benefit for
patients over 70 who are selected to undergo HDT therapyfor myeloma highlighting the fact that chronologic age aloneshould not be used to decide on transplant eligibility. Whilethe number of patients over 70 who may have beenexcluded from a transplant at our institution and the factorsthat went into such decision making cannot be estimated inthis retrospective study, selected patients with good perform-ance status should be offered the option of HDT. Dosereduction of melphalan should be considered in this popula-tion, given the benefit of HDT seen in this group of patients.
Patients and MethodsWe examined our transplant data base and identified 33 patients
who were 70 years or older at the time of the stem cell transplant formultiple myeloma. We attempted to identify two control patients foreach of the 33 patients, who were 65 years or younger at the time oftransplant. Each control patient was matched for timing of transplant(early transplant after induction therapy vs. delayed transplant at timeof relapse), disease status at transplant (in partial response versus re-fractory to initial therapy for early transplants), Durie Salmon stage attransplant, high or low bone marrow plasma cell labeling index, pres-ence or absence of abnormalities on conventional cytogenetics,presence or absence of circulating plasma cells, and the stem cell mo-bilization regimen used (growth factor alone versus growth factor andcyclophosphamide). These factors were used for matching in the orderof the priority as stated above with maximum weight given to the timingof transplant and the least priority for the mobilization regimen used.Patients receiving a second stem cell transplant, either autologous orallogeneic, were excluded from the study.
Data pertaining to the transplant patients are captured prospectivelyinto a database which is continuously updated. Complete follow-up wasavailable for all the patients. All patients had provided written informedconsent for use of their medical records. Approval of the Mayo Founda-tion Institutional Review Board was obtained in accordance with federalregulations and the Declaration of Helsinki.
Stem cells were collected using granulocyte colony-stimulating factor(G-CSF) priming in the majority of patients in both groups (Table I). G-CSF was administered subcutaneously (5 lg/kg) daily until the comple-tion of peripheral blood stem cell collection with apheresis beginning onthe fifth day after starting G-CSF. The remaining patients had stemcells collected after administration of cyclophosphamide 1.5 g/m2 perday for 2 consecutive days, followed by GM-CSF at 5 lg/kg starting onday 3 and continuing through the period of granulocytopenia. Apheresiswas performed once the total white blood cell count exceeded 500/ll.Prior to 1997 the target for the apheresis procedure was 5 3 108
mononuclear cells/kg, which was subsequently replaced by quantitationof CD341 cells and the target became 4 3 106 CD341 cells/kg for asingle stem cell transplant. Many of the patients, especially in theyounger age group had adequate number of stem cells collected tofacilitate additional transplants, either tandem transplants or salvagetransplants at the time of relapse.
The conditioning regimen in the majority of the patients consisted ofmelphalan alone, usually at 200 mg/m2 given over two days. In a smallnumber of patients (10 in the elderly group and 3 in the control group;Table I) melphalan was dose reduced to 140 mg/m2 due to advancedage, renal insufficiency or poor performance. Bone marrow plasma celllabeling index (PCLI), cytogenetics, b2 microglobulin and other labora-tory variables were assessed pre-transplantation. Labeling index whichis a measure of the cell kinetics is determined using a slide-based im-munofluorescence method on bone marrow samples, as previouslydescribed [21] and is classified as high when �1%.
Responses were defined by conventional criteria [22]. Treatmentrelated mortality was defined as death within 100 days of stem celltransplant, in a patient with disease in response or stable disease.Overall survival was defined as the time from transplantation or fromthe date of initial diagnosis of myeloma to the date of death or last fol-low-up. The v2 and Fisher exact tests were used to compare differen-ces among the patient groups for nominal variables and the t-test wasused for continuous variables. Kaplan–Meier analysis was used foroverall and progression free survival and differences between survivalcurves were tested for statistical significance using the two-tailed log-rank test [23].
References1. Bataille R, Harousseau JL. Multiple myeloma. N Engl J Med 1997;336:1657–
1664.2. Jemal A, Siegel R, Ward E, et al. Cancer statistics, 2007. CA Cancer J Clin
2007;57:43–66.3. Kyle RA. Long-term survival in multiple myeloma. N Engl J Med 1983;
308:314–316.4. Alexanian R, Bonnet J, Gehan E, et al. Combination chemotherapy for multi-
ple myeloma. Cancer 1972;30:382–389.5. Attal M, Harousseau JL, Stoppa AM, et al. A prospective, randomized trial of
autologous bone marrow transplantation and chemotherapy in multiple my-eloma. Intergroupe Francais du Myelome. N Engl J Med 1996;335:91–97.
6. Child JA, Morgan GJ, Davies FE, et al. High-dose chemotherapy with hema-topoietic stem-cell rescue for multiple myeloma. N Engl J Med 2003;348:1875–1883.
7. Fermand JP, Ravaud P, Chevret S, et al. High-dose therapy and autologousperipheral blood stem cell transplantation in multiple myeloma: Up-front orrescue treatment? Results of a multicenter sequential randomized clinicaltrial. Blood 1998;92:3131–3136.
8. Siegel DS, Desikan KR, Mehta J, et al. Age is not a prognostic variable withautotransplants for multiple myeloma. Blood 1999;93:51–54.
9. Badros A, Barlogie B, Siegel E, et al. Autologous stem cell transplantation inelderly multiple myeloma patients over the age of 70 years. Br J Haematol2001;114:600–607.
10. Reece DE, Bredeson C, Perez WS, et al. Autologous stem cell transplanta-tion in multiple myeloma patients <60 vs >/560 years of age. Bone MarrowTransplant 2003;32:1135–1143.
11. Jantunen E, Kuittinen T, Penttila K, et al. High-dose melphalan (200 mg/m2)supported by autologous stem cell transplantation is safe and effective in el-derly (>or565 years) myeloma patients: Comparison with younger patientstreated on the same protocol. Bone Marrow Transplant 2006;37:917–922.
12. Miller CB, Piantadosi S, Vogelsang GB, et al. Impact of age on outcome ofpatients with cancer undergoing autologous bone marrow transplant. J ClinOncol 1996;14:1327–1332.
13. Kusnierz-Glaz CR, Schlegel PG, Wong RM, et al. Influence of age on the out-come of 500 autologous bone marrow transplant procedures for hematologicmalignancies. J Clin Oncol 1997;15:18–25.
14. Palumbo A, Triolo S, Argentino C, et al. Dose-intensive melphalan with stemcell support (MEL100) is superior to standard treatment in elderly myelomapatients. Blood 1999;94:1248–1253.
15. Facon T, Mary JY, Hulin C, et al. Major superiority of melphalan - prednisone(MP) 1 thalidomide (THAL) over MP and autologous stem cell transplantationin the treatment of newly diagnosed elderly patients with multiple myeloma.ASH Annu Meet Abstr 2005;106:780.
16. Kumar S, Lacy M, Dispenzieri A, et al. Autologous stem cell transplantationfor multiple myeloma in patients over 70 years: A matched comparison withpatients under 65 years. ASH Annu Meet Abstr 2005;106:1173.
17. Palumbo A, Triolo S, Baldini L, et al. Dose-intensive melphalan with stem cellsupport (CM regimen) is effective and well tolerated in elderly myelomapatients. Haematologica 2000;85:508–513.
18. Sirohi B, Powles R, Treleaven J, et al. The role of autologous transplantationin patients with multiple myeloma aged 65 years and over. Bone MarrowTransplant 2000;25:533–539.
19. Morris CL, Siegel E, Barlogie B, et al. Mobilization of CD341 cells in elderlypatients (>/570 years) with multiple myeloma: Influence of age, prior ther-apy, platelet count and mobilization regimen. Br J Haematol 2003;120:413–423.
20. Dumontet C, Ketterer N, Espinouse D, et al. Reduced progression-free sur-vival in elderly patients receiving intensification with autologous peripheralblood stem cell reinfusion for multiple myeloma. Bone Marrow Transplant1998;21:1037–1041.
21. Greipp PR, Lust JA, O’Fallon WM, et al. Plasma cell labeling index and beta2-microglobulin predict survival independent of thymidine kinase and C-reac-tive protein in multiple myeloma. Blood 1993;81:3382–3387.
22. Blade J, Samson D, Reece D, et al. Criteria for evaluating disease responseand progression in patients with multiple myeloma treated by high-dose ther-apy and haemopoietic stem cell transplantation. Myeloma subcommittee ofthe EBMT. European group for blood and marrow transplant. Br J Haematol1998;102:1115–1123.
23. Kaplan E, Meier P. Non-parametric estimation from incomplete observations.J Am Stat Assoc 1958;53:457–481.
American Journal of Hematology 617
Access to Hematopoietic-cell Transplantation in the UnitedStates
Navneet S. Majhail, MD, MS1,2, Nancy A. Omondi, MBA, MS3, Ellen Denzen, MS3, ElizabethA. Murphy, EdD, RN3, and J Douglas Rizzo, MD, MS4,5
1Center for International Blood and Marrow Transplant Research, Minneapolis, MN2University of Minnesota, Minneapolis, MN3National Marrow Donor Program®, Minneapolis, MN4Center for International Blood and Marrow Transplant Research, Milwaukee, WI5Medical College of Wisconsin, Milwaukee, WI
AbstractHematopoietic cell-transplantation (HCT) is a highly specialized and resource-intense medicalprocedure that can be associated with disparities in access to transplantation. Barriers to access toHCT are multifactorial, complex and interrelated. Our current knowledge of specific barriers thatprevent access to HCT is very limited. As the utilization of HCT increases, it is imperative thatunderserved populations receive the benefit of this life-saving procedure. We review theprevailing literature on access to HCT and describe research priorities for eliminating disparities intransplantation. Better understanding of these complex barriers will minimize inequities, informhealth policy, guide development of interventions targeted to eliminate disparities and continue theexpansion of HCT in the future.
KeywordsHematopoietic-cell transplantation; autologous; allogeneic; access; underserved populations
INTRODUCTIONHematopoietic-cell transplantation (HCT) is curative therapy for a variety of malignant andnon-malignant hematologic disorders. The utilization of HCT has progressively increasedover the last four decades since reports of first successful transplantations in 1968 and anestimated 50,000 transplants are performed worldwide every year, including 20,000 in theUnited States.1 With emerging indications, improvements in technology and supportive care,and increasing availability of alternative graft sources and reduced intensity conditioningregimens, use of HCT can be expected to increase further in the future. However, HCT is ahighly specialized, technologically sophisticated, resource-intense and expensive procedurethat can be associated with health-care associated disparities. These health care disparitieshave clinical, ethical and policy implications. We review the available literature on access toHCT and describe barriers that need to be addressed to ensure equitable access to HCT forall populations.
Address for correspondence: Navneet Majhail, MD, MS, Assistant Professor, Division of Hematology, Oncology and Transplantation,University of Minnesota, 420 Delaware St SE, MMC 480, Minneapolis, MN 55455, Phone: 612 624 0123, Fax: 612 625 6919,[email protected].
NIH Public AccessAuthor ManuscriptBiol Blood Marrow Transplant. Author manuscript; available in PMC 2011 August 1.
Published in final edited form as:Biol Blood Marrow Transplant. 2010 August ; 16(8): 1070–1075. doi:10.1016/j.bbmt.2009.12.529.
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript

Access to Cancer CareAccess to health care has been defined as “the timely use of affordable personal healthservices to achieve the best possible health outcomes”.2,3 Mandelblatt et al have veryelegantly summarized the complexities of access to health care; according to them, “theprocess of gaining access to care represents dynamic interactions of diverse individuals intheir social context interfacing with health care providers, who, in turn, are operating in avariety of changing and often constrained medical care structures and environments”.3Disparities exist in the health care of minority populations in the United States andminorities do not have the same access to health care and as a result do not receive the samequality of health care and have poorer overall health status than non-minorities.4–6 TheInstitute of Medicine in its report, Unequal Treatment: Confronting Racial and EthnicDisparities in Healthcare, further concluded that even when other healthcare access-relatedfactors, such as ability to pay for care are the same, racial and ethnic minorities receivelower quality healthcare than Whites.5 The report recommended a comprehensive, multi-level strategy to eliminate these disparities, including increasing awareness amongproviders, patients, payors, health plan purchasers and the society at large, enhancingtraining and education and conducting research on interventions.
Cancer care is also associated with disparities in detection, treatment and outcomes forspecific high-risk populations. These high-risk populations include elderly patients, women,patients of Black or Hispanic race/ethnicity, the under- or un-insured, patients from thelower socioeconomic strata, patients with lower levels of health literacy and education, andpatients with rural residence.3,7–11 The origins of these inequities are multifactorial andcomplex. Patient barriers include demographics, language, acculturation, attitudes andfamily and cultural contexts.3 In addition, health care providers play an important role inensuring access to cancer care. Physician and provider specific barriers that have beenreported in the literature include age or race biases, biases and beliefs about screening andtreatment efficacy, deficient knowledge and training, lack of confidence, lack of culturallysensitive resources, lack of time, concerns about patient acceptance, cost concerns, andlogistic or organizational barriers.3,12–15 Finally, health care system barriers such asorganizational and structural factors and reimbursement and financial forces can facilitate orhinder access to optimal cancer care.3 Factors can also be closely interrelated; for instance,racial and ethnic minorities are more likely to be uninsured compared to Whites.16
Access to Hematopoietic-cell TransplantationHCT is most commonly performed for malignant hematologic disorders and barriers thatprevent access to cancer care may also be relevant for HCT. However, additional barriersmay also have a role since HCT is a high-cost and sophisticated medical procedure thatinvolves complex interactions between patient, provider and health-care system factors(Figure 1).
The available literature on access to HCT is very limited (Table 2). Studies have generallyhad insufficient statistical power to detect differences among access indicators and/or havefrequently utilized databases with limited applicability to understanding access issues,particularly their cause. Inpatient hospital discharge databases have been frequently utilizedin these studies. However, such databases may not be truly appropriate to health disparitiesresearch as they may not capture the universe of patients with hematologic malignancies orwho received transplants in a population cohort. Also, disease and procedure codes are usedto identify patients from these datasets; medical codes lack precision and importantprognostic factors such as disease stage and remission status which may affect decisionmaking regarding use of HCT could not be considered in these analyses. Furthermore,
Majhail et al. Page 2
Biol Blood Marrow Transplant. Author manuscript; available in PMC 2011 August 1.
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript

contemporaneous studies are lacking and the majority of studies addressed barriers in an erawhen present day transplantation techniques were not widely available.
Possible limitations in study design notwithstanding, previously conducted studies haveincreased our characterization of barriers that limit access to transplantation. For instance,current literature highlights substantial geographic variation in access to HCT. Mitchell et al,in a study that utilized hospital discharge data from four states (California, Massachusetts,Maryland and New York) for the years 1988 and 1991, showed state wise differences inaccess to HCT by insurance coverage and race.17 Compared to patients with privateinsurance, Medicaid beneficiaries in California, New York and Maryland/Massachusettswere 78%, 64% and 61% as likely to receive a transplant for leukemia and 69%, 56% and32% as likely to receive a transplant for lymphoma, respectively. Similarly, compared toWhites, Hispanics were significantly less likely to receive a transplant for lymphoma in NewYork but had similar rates of transplantation for lymphoma in California and for leukemia inall four states.
Specific disparities to access to HCT that have been identified in the literature include:
Age—Studies that have investigated age as a predictor of access to HCT indicate thatyounger patients are more likely to receive a transplant compared to older patients. Mitchellet al showed that each 10-year increase in age was associated with 10% to 18% (variation bystate) lower odds of receiving HCT for leukemia or lymphoma.17 In another study that usedinpatient discharge data for the state of Texas from 1999, Hwang et al reported that elderly(age ≥65 years) patients had a significantly lower likelihood of receiving a transplant forleukemia with each year increase in age; however, no age effect was noted among pediatric(age <18 years) and adult (age 18–64 years) recipients.18 In a study using Arizona hospitaldischarge data from 1997–2003, Cho has also reported that increasing age reduces theprobability of receiving a transplant for leukemia; they did not detect any effect of age onthe likelihood of transplantation for lymphoma.19 These previous studies pre-date the adventof reduced-intensity and non-myeloablative preparative regimens which are associated withlower risks of morbidity and mortality and now allow transplantation as a viable treatmentoption for older patients. Additional factors may impact utilization of HCT in older patients.Older patients may decline or their providers may not recommend aggressive therapies suchas HCT. Also, some differences in transplant utilization among older patients may beappropriate since older patients may have comorbidities and disease characteristics whichmay make them ineligible for transplantation; previous studies have not been able tosufficiently account for these important variables.
Gender—Mitchell et al and Cho found no impact of gender on the likelihood oftransplantation for leukemia or lymphoma.17,19 Hwang et al reported that elderly men weremore likely to receive a transplant for leukemia than elderly women, but they found noeffect of gender on pediatric and adult HCT recipients. In a study that specifically tried toaddress the issue of gender and access to HCT, Mehta et al used data for 1989–1999 fromthe International Bone Marrow Transplant Registry and Surveillance Epidemiology and EndResults (SEER) database.20 They concluded that there was no significant bias towards theuse of HCT in males compared to females. However, in a more recent and large study thatused data from the Center for International Blood and Marrow Transplant Research(CIBMTR) and SEER, Joshua et al showed that men were more likely to receive HCT thanwomen and this difference was primarily seen in autologous HCT for lymphoma ormyeloma, but not in allogeneic HCT.21 The reasons for gender specific disparities, if any,are unclear and need to be explored in future studies.
Majhail et al. Page 3
Biol Blood Marrow Transplant. Author manuscript; available in PMC 2011 August 1.
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript

Race—The role of race in access to HCT has to be interpreted with caution. Race is acomplex social, cultural and political construct and not a biological concept and accordingly,the definition of race has changed and evolved over time. Self-reported race is mostaccurate, but race is frequently assigned by centers or providers for a number of databases.Among the earliest studies of access to HCT, Mitchell et al showed that Blacks were lesslikely than Whites to undergo a transplant for leukemia or lymphoma in each of the fourstates investigated.17 Joshua et al have also shown that the likelihood of undergoing HCTfor leukemia, lymphoma and multiple myeloma is significantly lower for Blacks comparedto Whites and that these differences existed for autologous, matched sibling donor andunrelated donor HCT.21 On the other hand, Hwang et al and Cho did not find any impact ofrace of transplantation rates.18,19
Insurance Status—HCT is a costly procedure,22,23 and patients with no or limited healthinsurance coverage may have a lower likelihood of receiving HCT. Three previous studieshave attempted to address the impact of insurance coverage on access to HCT. Mitchell et alshowed that patients enrolled with Medicaid, self-paid (uninsured) patients and HealthMaintenance Organization (HMO) enrollees with leukemia or lymphoma were significantlyless likely to undergo HCT compared with patients with private insurance.17 The authorssuggested that the lower probability of getting a transplant among HMO enrollees could berelated to coverage restrictions or delay in approval for costly medical procedures such asHCT. Cho also reported that patients with less generous insurance coverage were less likelyto receive HCT for leukemia and lymphoma.19 However, Hwang et al did not find anyassociation between payor status (commercial insurance, HMO, Medicare, Medicaid, self-pay and other payor) and receipt of HCT for leukemia.18 Their findings were specific to thestate of Texas and authors commented that the lack of relationship between payor status andHCT use could be due to equitable access to HCT or lack of statistical power to identifysignificant associations. The interaction of insurance status with other sociodemographicfactors, albeit complex, has not been explored. For example, children may have greateraccess to HCT compared to adults due to the presence of hospital, state or federal programsthat may provide coverage for HCT.
Other barriers—Education status, estimated by Zip Code of residence, was not identifiedas a major factor associated with transplant access by Mitchell et al.17 Cho examined theassociation between hospital characteristics and likelihood of transplantation for leukemia inArizona.19 Patients with leukemia and lymphoma admitted to a minor teaching hospitals (vs.major teaching hospitals) and small or medium sized hospitals (vs. large hospitals, >250beds) were less likely to receive a transplant. Patients admitted to for-profit hospitals andgovernment-owned hospitals had comparable probabilities of transplantation.
Areas for Further ResearchResearch is needed to further characterize disparities in access to HCT, identify causes forany disparities deemed inappropriate and to investigate interventions to mitigate thosebarriers. However, health disparities research in HCT can be very challenging. Typically, avery large population cohort has to be assembled for studies of access to health-care. Areliable estimate of the ‘numerator’ (e.g., number of transplants for a disease) and‘denominator’ (e.g., total number of patients with that disease for whom a transplant isappropriate) for a cohort over a given period of time is also needed. Finally, comprehensiveinformation about the factors that may be associated with disparate access (e.g., race andethnicity, education status, socioeconomic status, cultural attitudes, insurance/paymentstatus) is required. Large administrative databases such as the SEER-Medicare dataset arefrequently used to identify disparities in access to cancer care. Since these large databasescannot robustly collect information about access indicators, surrogate variables are used to
Majhail et al. Page 4
Biol Blood Marrow Transplant. Author manuscript; available in PMC 2011 August 1.
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript

evaluate barriers that may impact access to treatment (e.g., Zip Code to assignsocioeconomic status, education status and place of residence). The majority of federal andclaims databases do not have robust information about hematologic malignancies and HCTand details of important prognostic factors (e.g. cytogenetic risk) that predict which patientsshould be considered for HCT are generally not available. However, good quality studiesusing administrative and claims databases may be possible in the near future due toenhanced data collection efforts by multiple groups. For example, SEER has collected dataon MDS and chronic myeloproliferative disorders since 2001. Since 2007, all allogeneictransplants in the United States should be reported to the CIBMTR under the requirementsof the Stem Cell Therapeutic and Research Act of 2005.
Database studies can be useful for identification of some aspects of health-care disparities.However, they are not optimal for evaluation of individual patient and provider levelbarriers or to identify the causes of disparate access. Additional health services researchmethodologies (e.g. patients and physician surveys, qualitative research methods such asfocus groups) will be needed to better understand obstacles to universal access to HCT andmust also account for inherent inequities in access to HCT due to biological and medicalfactors. For instance, ethnic and racial minorities have a lower probability of finding asuitable donor and have a higher prevalence of comorbidities that may make them ineligiblefor transplantation.24–26 Once etiologies of disparate access have been characterized, studiesevaluating targeted interventions to address barriers to access are also needed.
In order for underserved populations to obtain the benefit of a life-saving procedure such asHCT, it is imperative that the medical community work to reduce inappropriate disparitiesand ensure equitable access to transplantation. Our current knowledge about specific barriersthat prohibit access to HCT is very limited. While waiting for better information, themedical community, including payors, policy makers and healthcare providers must use thecurrent awareness of disparate access as a call to action to examine their own practices andwork to eliminate inappropriate disparities. Better understanding of these complex barrierswill minimize inequities, inform health policy, guide development of interventions targetedto eliminate disparities and continue the expansion of HCT in the future.
References1. Pasquini, MC.; Wang, Z.; Schneider, L. [Accessed 08/01/09] Current use and outcome of
hematopoietic stem cell transplantation: part I-CIBMTR Summary Slides, 2007; CIBMTRNewsletter. 2007. p. 5-9.Available at:http://www.cibmtr.org/PUBLICATIONS/Newsletter/index.html
2. Millman, M. Access to health care in America. Washingon, DC: National Academy Press; 1993.3. Mandelblatt JS, Yabroff KR, Kerner JF. Equitable access to cancer services: A review of barriers to
quality care. Cancer. 1999; 86:2378–2390. [PubMed: 10590381]4. Groman R, Ginsburg J. Racial and ethnic disparities in health care: a position paper of the American
College of Physicians. Ann Intern Med. 2004; 141:226–232. [PubMed: 15289223]5. Institute of Medicine. Unequal Treatment: Confronting Racial and Ethnic Disparities in Healthcare.
Washington, DC: The National Academies Press; 2003.6. Agency for Healthcare Research and Quality. 2008 National Healthcare Quality Report. Rockville,
MD: U.S. Department of Health and Human Services, Agency for Healthcare Research and Quality;2009.
7. Shavers VL, Brown ML. Racial and ethnic disparities in the receipt of cancer treatment. J NatlCancer Inst. 2002; 94:334–357. [PubMed: 11880473]
8. Ward E, Jemal A, Cokkinides V, et al. Cancer disparities by race/ethnicity and socioeconomicstatus. CA Cancer J Clin. 2004; 54:78–93. [PubMed: 15061598]
Majhail et al. Page 5
Biol Blood Marrow Transplant. Author manuscript; available in PMC 2011 August 1.
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
9. Albano JD, Ward E, Jemal A, et al. Cancer mortality in the United States by education level andrace. J Natl Cancer Inst. 2007; 99:1384–1394. [PubMed: 17848670]
10. Clegg LX, Li FP, Hankey BF, Chu K, Edwards BK. Cancer survival among US whites andminorities: a SEER (Surveillance, Epidemiology, and End Results) Program population-basedstudy. Arch Intern Med. 2002; 162:1985–1993. [PubMed: 12230422]
11. Clegg LX, Reichman ME, Miller BA, et al. Impact of socioeconomic status on cancer incidenceand stage at diagnosis: selected findings from the surveillance, epidemiology, and end results:National Longitudinal Mortality Study. Cancer Causes Control. 2009; 20:417–435. [PubMed:19002764]
12. Haggerty J, Tudiver F, Brown JB, Herbert C, Ciampi A, Guibert R. Patients’ anxiety andexpectations: how they influence family physicians’ decisions to order cancer screening tests. CanFam Physician. 2005; 51:1658–1659. [PubMed: 16926946]
13. Tudiver F, Guibert R, Haggerty J, et al. What influences family physicians’ cancer screeningdecisions when practice guidelines are unclear or conflicting? J Fam Pract. 2002; 51:760.[PubMed: 12366894]
14. Battista RN, Williams JI, MacFarlane LA. Determinants of primary medical practice in adultcancer prevention. Med Care. 1986; 24:216–224. [PubMed: 3951264]
15. Battista RN, Williams JI, MacFarlane LA. Determinants of preventive practices in fee-for-serviceprimary care. Am J Prev Med. 1990; 6:6–11. [PubMed: 2340192]
16. Ward E, Halpern M, Schrag N, et al. Association of insurance with cancer care utilization andoutcomes. CA Cancer J Clin. 2008; 58:9–31. [PubMed: 18096863]
17. Mitchell JM, Meehan KR, Kong J, Schulman KA. Access to bone marrow transplantation forleukemia and lymphoma: the role of sociodemographic factors. J Clin Oncol. 1997; 15:2644–2651. [PubMed: 9215836]
18. Hwang JP, Lam TP, Cohen DS, Donato ML, Geraci JM. Hematopoietic stem cell transplantationamong patients with leukemia of all ages in Texas. Cancer. 2004; 101:2230–2238. [PubMed:15484218]
19. Cho, C. [Accessed 08-01-2009] Factors affecting stem cell transplantation for leukemia andlymphoma. 2006. http://hdl.handle.net/1961/3595
20. Mehta P, Pollock BH, Nugent M, Horowitz M, Wingard JR. Access to stem cell transplantation: dowomen fare as well as men? Am J Hematol. 2003; 72:99–102. [PubMed: 12555212]
21. Joshua TV, Rizzo JD, Zhang MJ, Horowitz MM. Access to hematopoietic stem celltransplantation: Effect of race and gender. Biol Blood Marrow Transplant. 2007; 13 (Suppl):22.
22. Majhail NS, Mothukuri JM, Brunstein CG, Weisdorf DJ. Costs of hematopoietic celltransplantation: comparison of umbilical cord blood and matched related donor transplantation andthe impact of post-transplant complications. Biol Blood Marrow Transplant. 2009; 15:564–573.[PubMed: 19361748]
23. Saito AM, Cutler C, Zahrieh D, et al. Costs of allogeneic hematopoietic cell transplantation withhigh-dose regimens. Biol Blood Marrow Transplant. 2008; 14:197–207. [PubMed: 18215780]
24. Bonow RO, Grant AO, Jacobs AK. The cardiovascular state of the union: confronting healthcaredisparities. Circulation. 2005; 111:1205–1207. [PubMed: 15769758]
25. Kollman C, Weis T, Switzer GE, et al. Non-HLA barriers to unrelated donor stem celltransplantation. Bone Marrow Transplant. 2001; 27:581–587. [PubMed: 11319586]
26. Norris K, Nissenson AR. Race, gender, and socioeconomic disparities in CKD in the United States.J Am Soc Nephrol. 2008; 19:1261–1270. [PubMed: 18525000]
Majhail et al. Page 6
Biol Blood Marrow Transplant. Author manuscript; available in PMC 2011 August 1.
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript

Figure 1.Potential barriers to access to hematopoietic-cell transplantation
Majhail et al. Page 7
Biol Blood Marrow Transplant. Author manuscript; available in PMC 2011 August 1.
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript

NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
Majhail et al. Page 8
Tabl
e 1
Acc
ess t
o he
mat
opoi
etic
cel
l tra
nspl
anta
tion:
sum
mar
y of
pub
lishe
d st
udie
s
Ref
eren
ceA
cces
s foc
usD
ata
sour
ces
Stud
y de
sign
NPo
pula
tion
char
acte
rist
ics
Res
ults
Mitc
hell
et a
l(1
997)
17A
geG
ende
rR
ace
Educ
atio
nIn
sura
nce
Inpa
tient
hos
pita
ldi
scha
rge
data
for
Cal
iforn
ia,
Mar
ylan
d,M
assa
chus
etts
and
New
Yor
k
ICD
-9 c
odes
use
d to
iden
tify
inpa
tient
s with
leuk
emia
or l
ymph
oma
and
reci
pien
ts o
f aut
o or
allo
HC
T in
198
8 an
d 19
91
•38
,420
inpa
tient
sw
ith le
ukem
ia o
rly
mph
oma
•1,
655
HC
Tre
cipi
ents
•A
ML
13%
, ALL
15%
,C
ML
6%, N
HL
45%
•W
hite
s 72%
, Bla
cks 9
%
•B
lue
Cro
ss 5
3%,
Med
icai
d 18
%, H
MO
12%
•B
lack
s and
old
erpa
tient
s les
s lik
ely
tore
ceiv
e H
CT
•Pa
tient
s with
priv
ate
insu
ranc
e m
ore
likel
yto
rece
ive
HC
T
Meh
ta e
t al
(200
3)20
Gen
der
SEER
, IB
MTR
SEER
inci
denc
e ra
tes a
ndda
ta fr
om IB
MTR
use
d to
estim
ate
rate
s of a
llo H
CT
for A
ML,
ALL
and
CM
Lfr
om 1
989–
1999
*
•18
,932
pat
ient
sw
ith A
ML,
ALL
or C
ML
•13
,083
HC
Tre
cipi
ents
•A
ML
24%
, ALL
22%
,C
ML
54%
•N
o ge
nder
diff
eren
ces
in a
llo H
CT
utili
zatio
n
Hw
ang
et a
l(2
004)
18A
geG
ende
rR
ace
Insu
ranc
eC
omor
bidi
ty
Texa
s inp
atie
ntho
spita
l dis
char
geda
ta
ICD
-9 c
odes
use
d to
iden
tify
inpa
tient
s with
acut
e or
chr
onic
leuk
emia
’s a
nd re
cipi
ents
of a
uto
or a
llo H
CT
in19
99
•6,
574
inpa
tient
sw
ith le
ukem
ia
•1,
604
HC
Tre
cipi
ents
•A
ML
27%
, ALL
24%
,C
ML
13%
, CLL
31%
•W
hite
s 70%
, Bla
cks 8
%
•M
edic
are/
Med
icai
d 50
%,
com
mer
cial
pay
er 3
0%
•El
derly
(≥65
yea
rs)
wom
en le
ss li
kely
tore
ceiv
e H
CT
•N
o im
pact
of p
ayor
stat
us a
nd e
thni
city
on H
CT
utili
zatio
n
Cho
(200
6)19
†A
geG
ende
rR
ace
Insu
ranc
eC
ente
r fac
tors
Com
orbi
ditie
s
Ariz
ona
inpa
tient
hosp
ital d
isch
arge
data
ICD
-9 c
odes
use
d to
iden
tify
inpa
tient
s with
leuk
emia
or l
ymph
oma
and
reci
pien
ts o
f aut
o or
allo
HC
T fr
om 1
997–
2003
•6,
435
inpa
tient
sw
ith le
ukem
ia o
rly
mph
oma
•20
7 H
CT
reci
pien
ts
•A
ML
14%
, ALL
17%
,N
HL
43%
•Pr
ivat
e pa
yer 3
5%, H
MO
32%
, Med
icar
e/ M
edic
aid
24%
•Pa
tient
s with
priv
ate
insu
ranc
e m
ore
likel
yto
rece
ive
HC
T
•N
o im
pact
of g
ende
ran
d ra
ce o
n H
CT
utili
zatio
n
Josh
ua e
t al
(200
7)21
Gen
der
Rac
eSE
ER, U
S C
ensu
sB
urea
u an
dC
IBM
TR
SEER
inci
denc
e ra
tes a
ndda
ta fr
om C
IBM
TR u
sed
to e
stim
ate
rate
s of a
uto
and
allo
HC
T fo
r leu
kem
ia,
lym
phom
a an
d m
yelo
ma
from
199
7–20
02
•27
3,85
3 pa
tient
sw
ith le
ukem
ia,
lym
phom
a or
mye
lom
a
•45
,750
HC
Tre
cipi
ents
•A
ML
21%
, ALL
9%
,C
ML
11%
, NH
L 21
%,
MM
40%
•W
hite
90%
, Bla
cks 1
0%
•B
lack
s les
s lik
ely
tore
ceiv
e au
to o
r allo
HC
T
•W
omen
less
like
ly to
rece
ive
auto
HC
T
ICD
– in
tern
atio
nal c
lass
ifica
tion
of d
isea
ses;
aut
o –
auto
logo
us; a
llo –
allo
gene
ic; H
CT
– he
mat
opoi
etic
cel
l tra
nspl
anta
tion;
Inte
rnat
iona
l Cla
ssifi
catio
n of
Dis
ease
s; S
EER
– S
urve
illan
ce E
pide
mio
logy
and
End
Res
ults
; IB
MTR
– In
tern
atio
nal B
one
Mar
row
Tra
nspl
ant R
egis
try (n
ow C
IBM
TR);
CIB
MTR
– C
ente
r for
Inte
rnat
iona
l Blo
od a
nd M
arro
w T
rans
plan
t Res
earc
h; A
ML
– ac
ute
mye
loid
leuk
emia
;A
LL –
acu
te ly
mph
obla
stic
leuk
emia
; CM
L –
chro
nic
mye
loid
leuk
emia
; CLL
– c
hron
ic ly
mph
ocyt
ic le
ukem
ia; N
HL
– no
n-H
odgk
in’s
lym
phom
a; M
M –
mul
tiple
mye
lom
a; H
MO
– H
ealth
Mai
nten
ance
Org
aniz
atio
n
* HC
T re
porte
d to
IBM
TR fr
om 1
989–
1992
and
SEE
R in
cide
nce
estim
ates
from
199
2–19
99 w
ere
used
for t
his a
naly
sis
Biol Blood Marrow Transplant. Author manuscript; available in PMC 2011 August 1.

NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
Majhail et al. Page 9† N
on-p
eer r
evie
wed
man
uscr
ipt
Biol Blood Marrow Transplant. Author manuscript; available in PMC 2011 August 1.

Version 2.2012, 11/15/11 © National Comprehensive Cancer Network, Inc. 2011, All rights reserved. The NCCN Guidelines and this illustration may not be reproduced in any form without the express written permission of NCCN .® ®
NCCN Guidelines IndexSenior Adult Oncology TOC
Discussion
NCCN.org
Continue
NCCN Clinical Practice Guidelines in Oncology (NCCN Guidelines )®
Senior Adult Oncology
Version 2.2012
Version 2.2012, 11/15/11 © National Comprehensive Cancer Network, Inc. 2011, All rights reserved. The NCCN Guidelines and this illustration may not be reproduced in any form without the express written permission of NCCN .® ®
NCCN Guidelines IndexSenior Adult Oncology TOC
Discussion
NCCNMary Anne BergmanHema Sundar, PhD
Specialties Index
ContinueNCCN Guidelines Panel Disclosures
NCCN Guidelines Version 2.2012 Panel MembersSenior Adult Oncology
Arti Hurria, MD/Chair † Þ ₪City of Hope Comprehensive Cancer Center
Ilene S. Browner, MD † ₪The Sidney Kimmel Comprehensive Cancer
Center at Johns Hopkins
Harvey Jay Cohen, MD † ₪
Crystal S. Denlinger, MD †
†
†H. Lee Moffitt Cancer Center & Research
Institute
†UNMC Eppley Cancer Center at The
Nebraska Medical Center
Duke Cancer Institute
Fox Chase Cancer Center
Mollie deShazo, MDUniversity of Alabama at Birmingham
Comprehensive Cancer Center
Martine Extermann, MD, PhD
Apar Kishor P. Ganti, MD
Jimmie C. Holland, MDMemorial Sloan-Kettering Cancer Center
Holly M. Holmes, MD Þ ₪The University of Texas MD Anderson Cancer Center
Mohana B. Karlekar, MD ÞVanderbilt-Ingram Cancer Center
Nancy L. Keating, MD MPH ÞDana-Farber/Brigham and Women’s Cancer Center
June McKoy, MD, JD, MBA Þ £Robert H. Lurie Comprehensive Cancer Center
of Northwestern University
Bruno C. Medeiros, MD ‡Stanford Cancer Institute
Ewa Mrozek, MD † ‡The Ohio State University Comprehensive
Cancer Center - James Cancer Hospital and
Solove Research Institute
†
† ‡
�
�
Tracey O’Connor, MDRoswell Park Cancer Institute
Stephen H. Petersdorf, MDUniversity of Washington Medical Center/
Seattle Cancer Care Alliance
�
₪
Hope S. Rugo, MD † ‡UCSF Helen Diller Family Comprehensive
Cancer Center
Rebecca A. Silliman, MD, PhD, MPH ₪Consultant
William P. Tew, MD † ÞMemorial Sloan-Kettering Cancer Center
Louise C. Walter, MD ₪UCSF Helen Diller Family Comprehensive
Cancer Center
Alva B. Weir, III, MD † ‡St. Jude Children’s Research
Hospital/University of Tennessee Cancer
Institute
Tanya Wildes, MD †Siteman Cancer Center at Barnes-Jewish
Hospital and Washington University
† Medical oncology
‡ Hematology oncology
Þ Internal medicine, including Family practice,Preventive management
Psychiatry, psychology, including health behavior
Bone Marrow Transplantation
* Writing committee member
�
�
£ Supportive Care including Palliative and PainManagement
₪ Geriatric medicine
Pharmacology/Pharmacy�
NCCN gratefully acknowledges the review
of the Senior Adult Oncology Guidelines by
Efrat Dotan, MD †
*
*
*
*
*
*
*
*
*
Printed by Kelly Hayden on 10/12/2012 3:09:21 PM. For personal use only. Not approved for distribution. Copyright © 2012 National Comprehensive Cancer Network, Inc., All Rights Reserved.

Version 2.2012, 11/15/11 © National Comprehensive Cancer Network, Inc. 2011, All rights reserved. The NCCN Guidelines and this illustration may not be reproduced in any form without the express written permission of NCCN .® ®
NCCN Guidelines IndexSenior Adult Oncology TOC
Discussion
NCCN Guidelines Version 2.2012 Sub-CommitteesSenior Adult Oncology
ContinueNCCN Guidelines Panel Disclosures
Psychosocial/Palliative Care
Jimmie C. Holland, MD
Memorial Sloan-Kettering Cancer
Center
Mohana B. Karlekar, MD Þ
Vanderbilt-Ingram Cancer Center
�
Breast/Gynecological Cancers
Tracey O’Connor, MD †
Roswell Park Cancer Institute
Ewa Mrozak, MD † ‡
The Ohio State University Comprehensive
Cancer Center-James Cancer Center and
Solove Research Institute
Hope S. Rugo, MD † ‡
UCSF Helen Diller Family Comprehensive
Cancer Center
William P. Tew, MD † Þ
Memorial Sloan-Kettering Cancer Center
Mollie deShazo, MD †
University of Alabama at Birmingham
Comprehensive Cancer Center
Bladder, Kidney and Prostate Cancers
Geriatric AssessmentHarvey Jay Cohen, MD †Duke Cancer Institute
Martine Extermann, MD, PhD †
H. Lee Moffitt Cancer Center &
Research Institute
Holly M. Holmes, MD Þ
The University of Texas
MD Anderson Cancer Center
June McKoy, MD, JD, MBA
Robert H. Lurie Comprehensive Cancer
Center of Northwestern University
Nancy L. Keating, MD, MPH Þ
Dana-Farber/Brigham and Women’s
Cancer Center
Rebecca A. Silliman, MD, PhD, MPH
Consultant
Louise Walter, MD
UCSF Helen Diller Family Comprehensive
Cancer Center
Þ £
₪
₪
₪
₪
₪
�
Hematologic MalignanciesTanya Wildes, MD †Siteman Cancer Center at Barnes-Jewish Hospital
and Washington University School of Medicine
Bruno C. Medeiros, MD
Stanford Cancer Institute
Stephen H. Petersdorf, MD †
University of Washington Medical Center/Seattle
Cancer Care Alliance
‡
‡ �
Specialties Index
† Medical oncology
‡ Hematology oncology
Þ Internal medicine, including Family practice,Preventive management
Psychiatry, psychology, including health behavior
Bone Marrow Transplantation
�
�
£ Supportive Care including Palliative and PainManagement
₪ Geriatric medicine
Pharmacology/Pharmacy�
GI Cancers
Crystal S. Denlinger, MD †
Fox Chase Cancer Center
Ilene S. Browner, MD †
The Sidney Kimmel Comprehensive
Cancer Center at Johns Hopkins
₪
Apar Kishor P. Ganti, MD †
UNMC Eppley Cancer Center/
Nebraska Medical Center
Non-Small Cell Lung Cancers
Alva B. Weir, III, MD, MBA † ‡
St. Jude Children’s Research Hospital/
University of Tennessee Cancer Institute
Head and Neck Cancers/CNS
Arti Hurria, MD/Chair † Þ ₪
Genitourinary, Lung and Central Nervous
System (CNS) Cancers
Printed by Kelly Hayden on 10/12/2012 3:09:21 PM. For personal use only. Not approved for distribution. Copyright © 2012 National Comprehensive Cancer Network, Inc., All Rights Reserved.

Version 2.2012, 11/15/11 © National Comprehensive Cancer Network, Inc. 2011, All rights reserved. The NCCN Guidelines and this illustration may not be reproduced in any form without the express written permission of NCCN .® ®
NCCN Guidelines IndexSenior Adult Oncology TOC
Discussion
NCCN Senior Adult Oncology Panel Members
NCCN Senior Adult Oncology Sub-Committee Members
Summary of the Guidelines Updates
Approach to Decision Making in the Older Adult (SAO-1)
Assessment of Risk Factors (SAO-2)
Special Considerations for Treatment (SAO-3 and SAO-4)
Upper, Middle, and Lower Percentiles of Life Expectancy for Women and Men at
Selected Ages (SAO-A)
Disease-Specific Issues Related to Age (SAO-B)
Comprehensive Geriatric Assessment (SAO-C)
Procedure for Functional Assessment Screening in Elderly Persons (SAO-D)
Clinical Trials:
Categories of Evidence andConsensus:NCCN
All recommendationsare Category 2A unless otherwisespecified.
Thebelieves that the best managementfor any cancer patient is in a clinicaltrial. Participation in clinical trials isespecially encouraged.
NCCN
To find clinical trials online at NCCNmember institutions, click here:nccn.org/clinical_trials/physician.html
See NCCN Categories of Evidenceand Consensus
The NCCN Guidelines are a statement of evidence and consensus of the authors regarding their views of currently accepted approaches to treatment.
Any clinician seeking to apply or consult the NCCN Guidelines is expected to use independent medical judgment in the context of individual clinical
circumstances to determine any patient’s care or treatment. The National Comprehensive Cancer Network (NCCN ) makes no representations or
warranties of any kind regarding their content, use or application and disclaims any responsibility for their application or use in any way. The NCCN
Guidelines are copyrighted by National Comprehensive Cancer Network . All rights reserved. The NCCN Guidelines and the illustrations herein may not
be reproduced in any form without the express written permission of NCCN. ©2011.
®
® ®
®
NCCN Guidelines Version 2.2012Senior Adult Oncology
Table of Contents
Printed by Kelly Hayden on 10/12/2012 3:09:21 PM. For personal use only. Not approved for distribution. Copyright © 2012 National Comprehensive Cancer Network, Inc., All Rights Reserved.

Version 2.2012, 11/15/11 © National Comprehensive Cancer Network, Inc. 2011, All rights reserved. The NCCN Guidelines and this illustration may not be reproduced in any form without the express written permission of NCCN .® ®
NCCN Guidelines IndexSenior Adult Oncology TOC
Discussion
NCCN Guidelines Version 2.2012Senior Adult Oncology
Updates
Note: All recommendations are category 2A unless otherwise indicated.
Clinical Trials: NCCN believes that the best management of any cancer patient is in a clinical trial. Participation in clinical trials is especially encouraged.
SAO-1
SAO-2
SAO-3
SAO-4
See NCCN Palliative Care GuidelinesSee NCCN Palliative Care Guidelines
SAO-B
�
�
�
�
�
�
���
This page now includes “Approach to decision making in the older adult.”
This page has been extensively revised. Footnote “e” is new to the page.
Surgery:“Emergency surgery carries increased risk of complications; special effort should be made to prevent/avoid emergency surgery” is new to
the page.
Radiation therapy:Changed Nutrition to “Nutritional support.Removed the following:Use caution with concurrent RT/Chemotherapy, dose modification of chemotherapy may be necessary,Consider amifostine for head and neck cancer,Hearing evaluation if ear in RT Fields.
Under Cardiac toxicity: removed, Assessment of ventricular function.
Footnotes to “g” and “h” are new to the page regarding trastuzumab.
Falls” is new to the page, “Consider PT evaluation in patient with history/risk of falls.”To Diarrhea added the link, .
This page has been extensively revised.
This page now includes “Assessment of risk factors.”
”
“
To Constipation added the link, .To Renal toxicity added “Calculate creatinine clearance to access renal function.”Drug holiday if prolonged infusion and Oral prophylaxis were removed from mucositis.
Deleted title: Specific Issues Related To The Management of Cancer in Older PatientsChanged the page title to: “Disease-Specific Issues Related to Age”This page now includes disease specific issues along with corresponding references in the management of the following malignancies:
�
�
�
�
�
�
��
���
UPDATES
1 of 2
Continue
�
�
�
Bladder cancerBreast cancerCentral Nervous System (CNS) Cancers
�
�
�
Multiple myelomaNon-small cell lung cancerProstate cancer
�
�
�
Colorectal cancerHead and Neck cancersKidney cancer
Updates in Version 1.2012 of the NCCN Senior Adult Oncology Guidelines from Version 1.2011 include:
Summary of changes in the 2.2012 version of the Senior Adult Oncology Guidelines from the 1.2012 version include:
The discussion section was updated to reflect the changes in the algorithm ( ).� MS-1
Printed by Kelly Hayden on 10/12/2012 3:09:21 PM. For personal use only. Not approved for distribution. Copyright © 2012 National Comprehensive Cancer Network, Inc., All Rights Reserved.
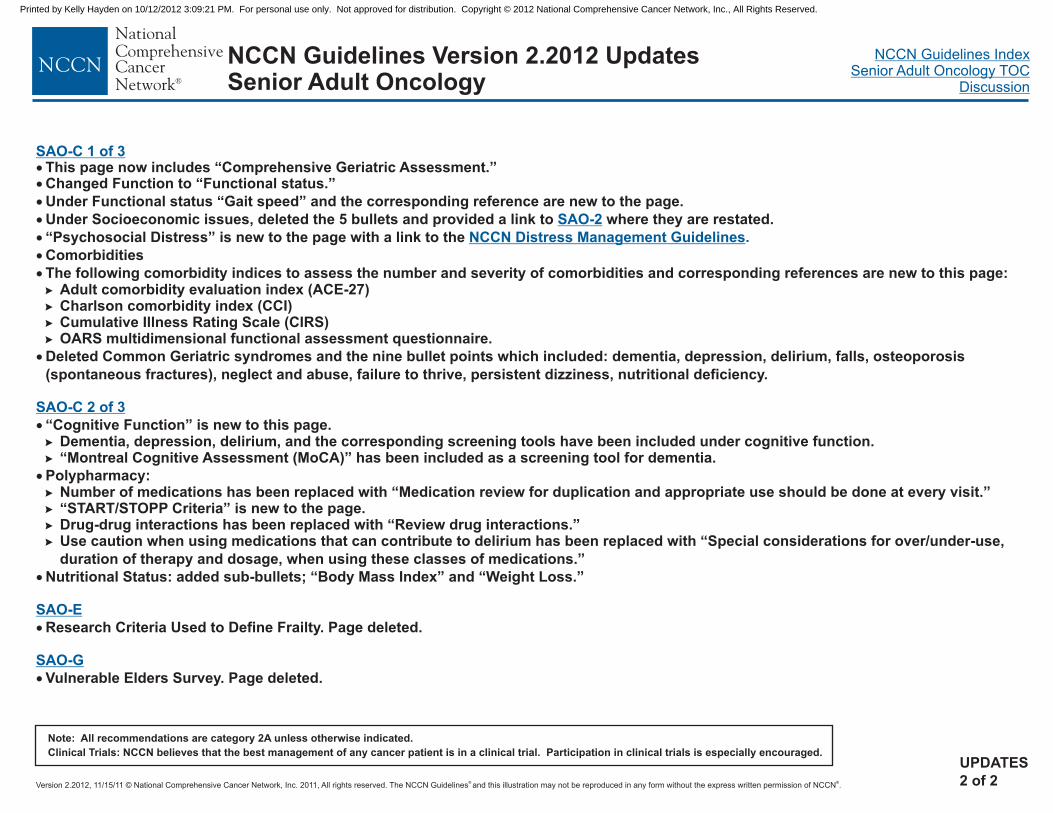
Version 2.2012, 11/15/11 © National Comprehensive Cancer Network, Inc. 2011, All rights reserved. The NCCN Guidelines and this illustration may not be reproduced in any form without the express written permission of NCCN .® ®
NCCN Guidelines IndexSenior Adult Oncology TOC
Discussion
NCCN Guidelines Version 2.2012Senior Adult Oncology
Updates
Note: All recommendations are category 2A unless otherwise indicated.
Clinical Trials: NCCN believes that the best management of any cancer patient is in a clinical trial. Participation in clinical trials is especially encouraged.UPDATES
2 of 2
SAO-C 1 of 3
SAO-2
NCCN Distress Management Guidelines
SAO-C 2 of 3
SAO-E
SAO-G
.
��
�
�
�
�
�
�
�
�
�
�
This page now includes “Comprehensive Geriatric Assessment.”Changed Function to “Functional status.”
Under Functional status “Gait speed” and the corresponding reference are new to the page.
Under Socioeconomic issues, deleted the 5 bullets and provided a link to where they are restated.
“Psychosocial Distress” is new to the page with a link to the
Comorbidities
The following comorbidity indices to assess the number and severity of comorbidities and corresponding references are new to this page:Adult comorbidity evaluation index (ACE-27)Charlson comorbidity index (CCI)Cumulative Illness Rating Scale (CIRS)OARS multidimensional functional assessment questionnaire.
Deleted Common Geriatric syndromes and the nine bullet points which included: dementia, depression, delirium, falls, osteoporosis
(spontaneous fractures), neglect and abuse, failure to thrive, persistent dizziness, nutritional deficiency.
“Cognitive Function” is new to this page.Dementia, depression, delirium, and the corresponding screening tools have been included under cognitive function.“Montreal Cognitive Assessment (MoCA)” has been included as a screening tool for dementia.
Polypharmacy:Number of medications has been replaced with “Medication review for duplication and appropriate use should be done at every visit.”“START/STOPP Criteria” is new to the page.Drug-drug interactions has been replaced with “Review drug interactions.”Use caution when using medications that can contribute to delirium has been replaced with “Special considerations for over/under-use,
duration of therapy and dosage, when using these classes of medications.”
Nutritional Status: added sub-bullets; “Body Mass Index” and “Weight Loss.”
Research Criteria Used to Define Frailty. Page deleted.
Vulnerable Elders Survey. Page deleted.
�
�
�
�
��
�
�
�
�
�
Printed by Kelly Hayden on 10/12/2012 3:09:21 PM. For personal use only. Not approved for distribution. Copyright © 2012 National Comprehensive Cancer Network, Inc., All Rights Reserved.

Version 2.2012, 11/15/11 © National Comprehensive Cancer Network, Inc. 2011, All rights reserved. The NCCN Guidelines and this illustration may not be reproduced in any form without the express written permission of NCCN .® ®
NCCN Guidelines IndexSenior Adult Oncology TOC
Discussion
APPROACH TO DECISION MAKING IN THE OLDER ADULT
Does this patient have
a life expectancy that puts
him or her at moderate or
high risk of dying or
suffering from cancer
during the lifetime?a
Yes
NoSymptom management/supportive care
See NCCN Supportive Care Guidelines
Does this patient
have decision-making
capacity?b
Obtain information from patient’s proxy. Consider consult from
ethics committee in patient without decision-making capacity.
Are the patient goals and values
consistent with wanting cancer
treatment?c
Symptom management/supportive careSee NCCN Supportive Care Guidelines
Assessment of Risk Factors ( )See SAO-2
NCCN Guidelines Version 2.2012Senior Adult Oncology
Note: All recommendations are category 2A unless otherwise indicated.
Clinical Trials: NCCN believes that the best management of any cancer patient is in a clinical trial. Participation in clinical trials is especially encouraged.
SAO-1
Yes
No
Yes
No
a
bSessums LL, Zembrzuska H, Jackson JL. Does this patient have medical decision-making capacity? JAMA 2011;306:420-427.Harrington SE, Smith TJ. The role of chemotherapy at the end of life: when is enough, enough? JAMA 2008;299:2667-2678.c
See histograms for age-specific life expectancy (SAO-A).
Printed by Kelly Hayden on 10/12/2012 3:09:21 PM. For personal use only. Not approved for distribution. Copyright © 2012 National Comprehensive Cancer Network, Inc., All Rights Reserved.

Version 2.2012, 11/15/11 © National Comprehensive Cancer Network, Inc. 2011, All rights reserved. The NCCN Guidelines and this illustration may not be reproduced in any form without the express written permission of NCCN .® ®
NCCN Guidelines IndexSenior Adult Oncology TOC
Discussion
Does the patient have risk factors for adverse
outcomes from cancer treatment?
Comorbiditiescongestive heart failurerenal insufficiencyneuropathyanemiaosteoporosisGI problemsdiabeteslung diseasehearing or vision loss
Geriatric Syndromes
fallsdementiadeliriumdepressionnutritional deficiencypolypharmacy
Socioeconomic Issuespoor living conditionsno caregiverlow incomeno transportationlack of prescription drug coverage
�
�
�
d
d
�
�
�
�
�
�
�
�
�
�
�
�
�
�
�
�
�
�
�
(CHF)
functional dependency (ADL, IADL)mobility problems
e
�
�
�
Yes
NoTreat as recommended in disease specific treatment guidelinesSee Disease-Specific Issues Related to Age (SAO-B)and NCCN Guidelines for Treatment of Cancer by Site
Are the risk
factors modifiable?
Treat risk factors
Consider alternate
treatment options
to reduce toxicity
Symptom management/
supportive careSee NCCN SupportiveCare Guidelines
See special considerations for patients able to tolerate treatment ( )SAO-3
Note: All recommendations are category 2A unless otherwise indicated.
Clinical Trials: NCCN believes that the best management of any cancer patient is in a clinical trial. Participation in clinical trials is especially encouraged.
SAO-2
d .eThe Panel recommends calculation of creatinine clearance to assess renal function for all patients.
See Comprehensive Geriatric Assessment (SAO-C)
ASSESSMENT OF RISK FACTORSd
Yes
No
Yes
No
NCCN Guidelines Version 2.2012Senior Adult Oncology
Printed by Kelly Hayden on 10/12/2012 3:09:21 PM. For personal use only. Not approved for distribution. Copyright © 2012 National Comprehensive Cancer Network, Inc., All Rights Reserved.

Version 2.2012, 11/15/11 © National Comprehensive Cancer Network, Inc. 2011, All rights reserved. The NCCN Guidelines and this illustration may not be reproduced in any form without the express written permission of NCCN .® ®
NCCN Guidelines IndexSenior Adult Oncology TOC
Discussion
Surgery
Radiation therapy�
�
Use caution with concurrent RT/Chemotherapy, dose
modification of chemotherapy may be necessaryNutritional support and pain control if RT induced mucositis
SAO-3
fMonitor the patient’s functional status, comorbidities, social circumstances, pain, nutritional status and distress.
Note: All recommendations are category 2A unless otherwise indicated.
Clinical Trials: NCCN believes that the best management of any cancer patient is in a clinical trial. Participation in clinical trials is especially encouraged.
NCCN Guidelines Version 2.2012Senior Adult Oncology
SPECIAL CONSIDERATIONS FOR PATIENTS ABLE TO TOLERATE TREATMENT f
�
�
�
In general, age is not a primary consideration for surgical riskEmergency surgery carries increased risk of complications; special effort
should be made to prevent/avoid emergency surgeryAssess physiologic status (Using standard surgical evaluation tools)
See SAO-4Chemotherapy
Printed by Kelly Hayden on 10/12/2012 3:09:21 PM. For personal use only. Not approved for distribution. Copyright © 2012 National Comprehensive Cancer Network, Inc., All Rights Reserved.

Version 2.2012, 11/15/11 © National Comprehensive Cancer Network, Inc. 2011, All rights reserved. The NCCN Guidelines and this illustration may not be reproduced in any form without the express written permission of NCCN .® ®
NCCN Guidelines IndexSenior Adult Oncology TOC
Discussion
NCCN Guidelines Version 2.2012Senior Adult Oncology
Note: All recommendations are category 2A unless otherwise indicated.
Clinical Trials: NCCN believes that the best management of any cancer patient is in a clinical trial. Participation in clinical trials is especially encouraged.
SAO-4
Chemotherapy
Neurotoxicity
Cardiac toxicity
Bone marrow
suppression
�
�
�
�
Consider alternative regimens with non-neurotoxic drugsMonitor hearing loss and avoid neurotoxic agents if significant hearing loss presentMonitor cerebellar function if high dose cytarabineMonitor for peripheral neuropathy
� Symptomatic or asymptomaticCaution with use of anthracyclines,Caution with use of trastuzumab (among patients with a normal ejection fraction, risk factors for CHF
include receipt of an anthracycline-based regimen, baseline LVEF of 50-54%, and on hypertensive
medicines)
CHFconsider alternative treatment�
�g,h
�
�
�
Prophylactic colony stimulating factors when dose intensity required for response or cure
Decreased dose of chemotherapy if palliation is the goal(See NCCN Myeloid Growth Factor Guidelines)
See NCCN Cancer and Treatment Related Anemia Guidelines
Mucositis�
�
�
Early hospitalization in patients who develop dysphagia/diarrheaNutritional supportSee NCCN Task Force: Prevention and Management of Mucositis in Cancer Care
Diarrhea�
�
Consider early aggressive rehydrationManagement with octreotide if oral preparations are ineffective ( )See NCCN Palliative Care Guidelines
Nausea/vomiting See NCCN Antiemesis Guidelines
Constipation See NCCN Palliative Care Guidelines
Falls � Consider PT evaluation in patient with history/risk of falls
fMonitor the patient’s functional status, comorbidities, social circumstances, pain, nutritional status and distress.
Piccart-Gebhart M, Procter M, Leyland-Jones B, et al. Trastuzumab after Adjuvant Chemotherapy in HER2-Positive Breast Cancer. N Engl J Med 2005;353:1659-72.
Romond E, Perez E, Bryant J, et al. Trastuzumab plus Adjuvant Chemotherapy for Operable HER2-Positive Breast Cancer. N Engl J Med 2005;353(16):1673-84.
g
h
Renal toxicity� Calculate creatinine clearance to assess renal function� Adjust dose for glomerular filtration rate (GFR) to reduce systemic toxicity
SPECIAL CONSIDERATIONS FOR PATIENTS ABLE TO TOLERATE TREATMENT f
Printed by Kelly Hayden on 10/12/2012 3:09:21 PM. For personal use only. Not approved for distribution. Copyright © 2012 National Comprehensive Cancer Network, Inc., All Rights Reserved.
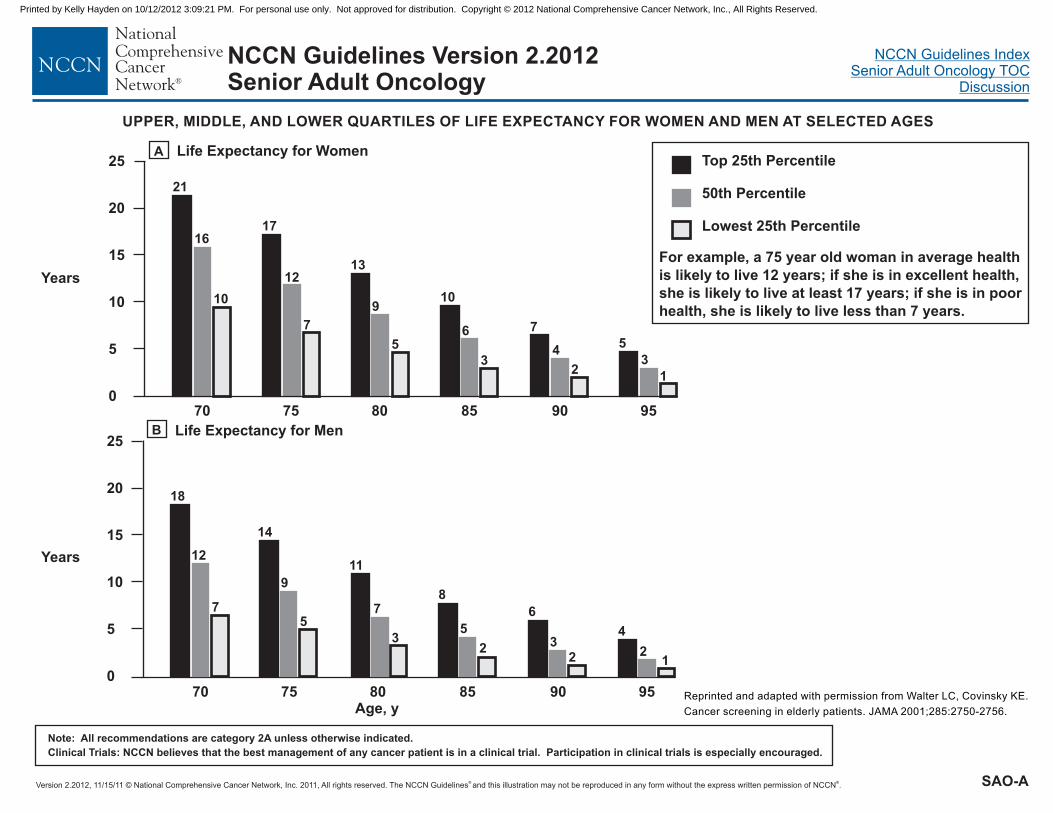
Version 2.2012, 11/15/11 © National Comprehensive Cancer Network, Inc. 2011, All rights reserved. The NCCN Guidelines and this illustration may not be reproduced in any form without the express written permission of NCCN .® ®
NCCN Guidelines IndexSenior Adult Oncology TOC
Discussion
Note: All recommendations are category 2A unless otherwise indicated.
Clinical Trials: NCCN believes that the best management of any cancer patient is in a clinical trial. Participation in clinical trials is especially encouraged.
SAO-A
UPPER, MIDDLE, AND LOWER QUARTILES OF LIFE EXPECTANCY FOR WOMEN AND MEN AT SELECTED AGES
Reprinted and adapted with permission from Walter LC, Covinsky KE.
Cancer screening in elderly patients. JAMA 2001;285:2750-2756.
Top 25th Percentile
50th Percentile
Lowest 25th Percentile
B Life Expectancy for Men25
20
15
10
5
070 75 80 85 90 95
Age, y
12
4
23
6
2
5
8
3
7
11
5
9
14
18
12
7
Years
A Life Expectancy for Women25
20
15
10
5
070 75 80 85 90 95
16
21
10
17
12
7
13
9
5
10
6
3
7
4
2
5
3
1
Years
For example, a 75 year old woman in average health
is likely to live 12 years; if she is in excellent health,
she is likely to live at least 17 years; if she is in poor
health, she is likely to live less than 7 years.
NCCN Guidelines Version 2.2012Senior Adult Oncology
Printed by Kelly Hayden on 10/12/2012 3:09:21 PM. For personal use only. Not approved for distribution. Copyright © 2012 National Comprehensive Cancer Network, Inc., All Rights Reserved.
Version 2.2012, 11/15/11 © National Comprehensive Cancer Network, Inc. 2011, All rights reserved. The NCCN Guidelines and this illustration may not be reproduced in any form without the express written permission of NCCN .® ®
NCCN Guidelines IndexSenior Adult Oncology TOC
Discussion
NCCN Guidelines Version 2.2012Senior Adult Oncology
DISEASE-SPECIFIC ISSUES RELATED TO AGE
Note: All recommendations are category 2A unless otherwise indicated.
Clinical Trials: NCCN believes that the best management of any cancer patient is in a clinical trial. Participation in clinical trials is especially encouraged.
Bladder Cancer
�
�
BCG treatment for superficial bladder carcinoma has decreased efficacy in the very old (> age 80).
The improvement in disease-specific survival from neoadjuvant chemotherapy is preserved with age.
1,2
4
� Age alone should not be a criterion for decisions regarding cystectomy, radiation, and chemotherapy in the elderly.3,4
1
2
3
4
Joudi FN, Smith BJ, O'Donnell MA, Konety BR. The impact of age on the response of patients with superficial bladder cancer to intravesical immunotherapy.J Urol 2006;175:1634-1639.
Herr HW. Age and outcome of superficial bladder cancer treated with bacille Calmette-Guerin therapy. Urology 2007;70:65-68.
Chamie K, Hu B, Devere White RW, Ellison LM. Cystectomy in the elderly: does the survival benefit in younger patients translate to the octogenarians?BJU Int 2008;102:284-290.
Grossman HB, Natale RB, Tangen CM, et al. Neoadjuvant chemotherapy plus cystectomy compared with cystectomy alone for locally advanced bladder cancer.N Engl J Med 2003;349:859-866.
SAO-B1 of 13
Printed by Kelly Hayden on 10/12/2012 3:09:21 PM. For personal use only. Not approved for distribution. Copyright © 2012 National Comprehensive Cancer Network, Inc., All Rights Reserved.

Version 2.2012, 11/15/11 © National Comprehensive Cancer Network, Inc. 2011, All rights reserved. The NCCN Guidelines and this illustration may not be reproduced in any form without the express written permission of NCCN .® ®
NCCN Guidelines IndexSenior Adult Oncology TOC
Discussion
NCCN Guidelines Version 2.2012Senior Adult Oncology
Note: All recommendations are category 2A unless otherwise indicated.
Clinical Trials: NCCN believes that the best management of any cancer patient is in a clinical trial. Participation in clinical trials is especially encouraged.
�
�
�
�
�
�
Older adults (65 or older) with breast cancer enrolled on cooperative group trials of adjuvant chemotherapy derive similar benefits (disease
free and overall survival) compared to younger patients. However, older patients have an increased risk of side effects and treatment-related
mortality.
A select group of older adults enroll on clinical trials. A review of CALGB studies for node-positive breast cancer demonstrated that only
(542/6487) of patients enrolled on cooperative group trials were 65 and older and only 159/6487) of patients were age 70 or older.
In the adjuvant treatment of breast cancer, single-agent capecitabine is inferior to cyclophosphamide, methotrexate, and fluorouracil (CMF)
or doxorubicin and cyclophosphamide (AC) in patients age 65 or older. Unplanned subset analysis suggested that the greatest difference
was seen in women with hormone receptor-negative tumors.
Patients age 70 or older with Stage I ER-positive breast cancer who undergo a lumpectomy with negative margins and are receiving
endocrine therapy may consider omission of radiation therapy. Omission of radiation therapy was associated with a modest increased risk
of local recurrence (4% vs. 1% at 5 years; 9% vs. 2% at 10 years); however, there was no difference in overall survival or distant metastatic
disease.
Women over the age of 75 receive less aggressive treatment and have higher mortality from early-stage breast cancer than younger
women.
In the absence of definitive data demonstrating superior survival from the performance of axillary lymph node dissection, for patients who
have particularly favorable tumors, for patients for whom the selection of adjuvant systemic therapy is unlikely to be affected, for the elderly,
or for those with serious comorbid conditions, the performance of axillary lymph node dissection may be considered optional.
( ).
1
1
2
3,4
5,6,7
8,9,10
8% 2% (
See NCCN Breast Cancer Guidelines
Breast CancerDISEASE-SPECIFIC ISSUES RELATED TO AGE
SAO-B2 of 13
1
10
Muss HB, Woolf S, Berry D, et al. Adjuvant chemotherapy in older and younger women with lymph node-positive breast cancer. JAMA 2005;293:1073-1081.
Muss HB, Berry DA, Cirrincione CT, et al. Adjuvant chemotherapy in older women with early-stage breast cancer. N Engl J Med 2009;360:2055-2065.
Hughes KS, Schnaper LA, Berry D, et al. Lumpectomy plus tamoxifen with or without irradiation in women 70 years of age or older with early breast cancer.N Engl J Med 2004;351:971-977.
Hughes KS, Schnaper LA, Cirrincione C, et al. Lumpectomy plus tamoxifen with or without irradiation in women age 70 or older with early breast cancer [abstract].J Clin Oncol 2010;28(Suppl 15):Abstract 507.
Bouchardy C, Rapiti E, Fioretta G, et al. Undertreatment strongly decreases prognosis of breast cancer in elderly women. J Clin Oncol 2003;21:3580-3587.
Schonberg MA, Marcantonio ER, Li D, et al. Breast cancer among the oldest old: tumor characteristics, treatment choices, and survival.J Clin Oncol 2010;28:2038-2045.
Yood MU, Owusu C, Buist DSM, et al. Mortality impact of less-than-standard therapy in older breast cancer patients. J Am Coll Surg 2008;206:66-75.
Martelli G, Miceli R, Daidone MG, et al. Axillary dissection versus no axillary dissection in elderly patients with breast cancer and no palpable axillary nodes: results after15 years of follow-up. Ann Surg Oncol 2011;18:125-133.
Rudenstam CM, Zahrieh D, Forbes JF, et al. Randomized trial comparing axillary clearance versus no axillary clearance in older patients with breast cancer: first resultsof International Breast Cancer Study Group Trial 10-93. J Clin Oncol 2006;24:337-344.
Giuliano AE, Hunt KK, Ballman KV, et al. Axillary dissection vs no axillary dissection in women with invasive breast cancer and sentinel node metastasis: a randomizedclinical trial. JAMA 2011;305:569-575.
2
3
4
5
6
7
8
9
Printed by Kelly Hayden on 10/12/2012 3:09:21 PM. For personal use only. Not approved for distribution. Copyright © 2012 National Comprehensive Cancer Network, Inc., All Rights Reserved.

Version 2.2012, 11/15/11 © National Comprehensive Cancer Network, Inc. 2011, All rights reserved. The NCCN Guidelines and this illustration may not be reproduced in any form without the express written permission of NCCN .® ®
NCCN Guidelines IndexSenior Adult Oncology TOC
Discussion
NCCN Guidelines Version 2.2012Senior Adult Oncology
Note: All recommendations are category 2A unless otherwise indicated.
Clinical Trials: NCCN believes that the best management of any cancer patient is in a clinical trial. Participation in clinical trials is especially encouraged.
Central Nervous System (CNS) Cancers
DISEASE-SPECIFIC ISSUES RELATED TO AGE
�
�
�
�
�
Patients over the age of 70 with glioblastoma who are treated surgically with gross total resection achieve a greater overall survival than
those who are treated with lesser resection. Just as in younger patients, it is difficult to be certain that this is a direct effect of the surgical
procedure or a result of selection bias.
Postsurgical radiation alone is effective in improving outcomes in patients over 70 with glioblastoma and shorter course regimens are
reasonable to consider.
The addition of temozolomide concurrently with radiation therapy followed by at least 6 months of adjuvant temozolomide improves survival
in patients between the ages of 60 and 70. Concurrent chemotherapy with radiation for patients over the age of 70 with glioblastoma
multiforme is of unclear benefit, but is likely to be helpful in “fit” elderly, based on single institution, retrospective data.
In recurrent glioblastoma bevacizumab likely improves quality of life (and possibly overall survival) in patients aged 55 or greater.
Patients over 60 with primary CNS lymphoma should be treated primarily with chemotherapy, saving radiation for salvage therapy.
1,2
3,4
6
7
8,9
5
1
2
3
4
5
6
7
8
9
Martinez R, Janka M, Soldner F, Behr R. Gross total resection of malignant glioma in elderly patients: implications in survival. Zentrabl Neurchir. 2007;68:176-181.
Vuorinen V, Hinkka S, Farkkila M, Jaaskelainen J. Debulking or biopsy of malignant glioma in elderly people. A randomized study. Acta Neurochir 2003;145: 5-10.
Keime-Guibert F, Chinot O, Taillandier L, et al. Radiotherapy for glioblastoma in the elderly. N Engl J Med 2007;356:1527-1535.
Roa W, Brasher PM, Bauman G, et al. Abbreviated course of radiation therapy in older patients with glioblastoma multiforme: a prospective randomized trial.J Clin Oncol 2004;22:1583-1588.
Stupp R, Hegi M, Mason W, et al. Effects of radiotherapy with concomitant and adjuvant temozolomide versus radiotherapy alone on survival in glioblastoma in arandomized phase III study: 5-year analysis of the EORTC-NCIC trial. Lancet Oncol 2009;10:459-466.
Scott J, Suh J, Elson P, et al. Aggressive treatment is appropriate for glioblastoma multiforme patients 70 years old or older:a retrospective review of 206 cases.Neuro-Oncol 2011;13:428-436.
Nghiemphu PL, Liu W, Lee Y, et al. Bevacizumab and chemotherapy for recurrent glioblastoma: a single-institution experience. Neurology 2009;72:1217-1222.
Gavrilovic I, Hormigo A, Yahalom J, et al. Long term follow-up of high-dose methotrexate-based therapy with and without whole brain irradiation for newly diagnosedprimary CNS lymphoma. J Clin Oncol 2006;24:4570-4574.
Zhu J-J, Gerstner ER, Engler DA, et al. High-dose methotrexate for elderly patients with primary CNS lymphoma. Neuro Oncol 2009;11:211-215.
SAO-B3 of 13
Printed by Kelly Hayden on 10/12/2012 3:09:21 PM. For personal use only. Not approved for distribution. Copyright © 2012 National Comprehensive Cancer Network, Inc., All Rights Reserved.
Version 2.2012, 11/15/11 © National Comprehensive Cancer Network, Inc. 2011, All rights reserved. The NCCN Guidelines and this illustration may not be reproduced in any form without the express written permission of NCCN .® ®
NCCN Guidelines IndexSenior Adult Oncology TOC
Discussion
NCCN Guidelines Version 2.2012Senior Adult Oncology
Note: All recommendations are category 2A unless otherwise indicated.
Clinical Trials: NCCN believes that the best management of any cancer patient is in a clinical trial. Participation in clinical trials is especially encouraged.
Colorectal Cancer
DISEASE-SPECIFIC ISSUES RELATED TO AGE
Surgery:
Age alone should not be a contraindication for curative surgery in early stage colon cancer and in resectable metastatic colon cancer.
Careful pre-operative planning and non-emergent surgery are more likely to result in optimal outcomes.
Adjuvant Therapy:
Older adults derive the same relative benefit as younger patients (in terms of disease free and overall survival) with 5-FU-based therapy for
adjuvant treatment. Older adults are at increased risk for hematologic toxicities.
The relative benefit from adjuvant treatment is similar across age groups; however, the absolute benefit of chemotherapy may be smaller due
to competing causes of death.
Pooled data from adjuvant studies (17% of patients over 70) did not show a benefit in disease free or overall survival with the addition of
oxaliplatin to 5-FU-based therapy in patients over 70. Due to the lack of prospective randomized data, adjuvant oxaliplatin based therapy in
adults 70 years of age should be considered on an individual patient basis.
Metastatic Disease:
Older adults derive the same relative benefit as younger patients (in terms of disease free and overall survival) with 5-FU-based therapy for
metastatic treatment. Older adults are at increased risk for hematologic toxicities.
Stop-and-go or maintenance monotherapy strategies during combination chemotherapy may be desirable for elderly patients to minimize
toxicity.
A prospective study of dose reduced oxaliplatin in addition to 5-FU-based therapy in older (median age 75) and frail patients failed to show a
statistically significant benefit in progression free survival. The addition of oxaliplatin to 5-FU-based therapy led to a numerical improvement
in progression-free survival that was of borderline statistical significance. Patients treated with capecitabine in comparison to 5-FU had a
higher risk of grade 3 or higher toxicity and no improvement in quality-of-life.
Retrospective analyses suggest acceptable toxicity profiles with anti-EGFR antibodies in elderly patients, although data is limited. Similar
benefits with anti-EGFR antibodies are seen in young and elderly patients.
Elderly patients derive similar clinical benefit from the use of bevacizumab with chemotherapy in the metastatic setting as younger patients,
but have higher rate of toxicities, mainly arterial thromboembolic events.
�
�
�
�
�
�
�
�
�
1,2,3,4,5
6
7
9
10
11,12
13,14
>
8
SAO-B4 of 13
Continue
Printed by Kelly Hayden on 10/12/2012 3:09:21 PM. For personal use only. Not approved for distribution. Copyright © 2012 National Comprehensive Cancer Network, Inc., All Rights Reserved.
Version 2.2012, 11/15/11 © National Comprehensive Cancer Network, Inc. 2011, All rights reserved. The NCCN Guidelines and this illustration may not be reproduced in any form without the express written permission of NCCN .® ®
NCCN Guidelines IndexSenior Adult Oncology TOC
Discussion
NCCN Guidelines Version 2.2012Senior Adult Oncology
Note: All recommendations are category 2A unless otherwise indicated.
Clinical Trials: NCCN believes that the best management of any cancer patient is in a clinical trial. Participation in clinical trials is especially encouraged.
1
2
3
4
5
6
7
8
Stocchi L, Nelson H, Young-Fadok TM, et al. Safety and advantages of laparoscopic vs. open colectomy in the elderly: matched-control study.Dis Colon Rectum 2000;43:326-332.
Ong ES, Alassas M, Dunn KB, Rajput A. Colorectal cancer surgery in the elderly: acceptable morbidity? Am J Surg 2008;195:344-348.
Schiffmann L, Ozcan S, Schwarz F, et al. Colorectal cancer in the elderly: surgical treatment and long-term survival. Int J Colorectal Dis 2008;23:601-610.
Fong Y, Blumgart LH, Fortner JG, Brennan MF. Pancreatic or liver resection for malignancy is safe and effective for the elderly. Ann Surg 1995;222:426-434.
Adam R, Frilling A, Elias D, et al. Liver resection of colorectal metastases in elderly patients. Br J Surg 2010;97:366-376.
Sargent DJ, Goldberg RM, Jacobson SD, et al. A pooled analysis of adjuvant chemotherapy for resected colon cancer in elderly patients.N Engl J Med 2001;345:1091-1097.
Jackson McCleary NA, Meyerhardt J, Green E, et al. Impact of older age on the efficacy of newer adjuvant therapies in >12,500 patients (pts) with stage II/III coloncancer: Findings from the ACCENT Database. ASCO Meeting Abstracts 2009;27:4010.
Folprecht G, Cunningham D, Ross P, et al. Efficacy of 5-fluorouracil-based chemotherapy in elderly patients with metastatic colorectal cancer: a pooled analysis ofclinical trials. Ann Oncol 2004;15:1330-1338.
Figer A, Perez-Staub N, Carola E, et al. FOLFOX in patients aged between 76 and 80 years with metastatic colorectal cancer: an exploratory cohort of the OPTIMOX1study. Cancer 2007;110:2666-2671.
Seymour MT, Thompson LC, Wasan HS, et al. Chemotherapy options in elderly and frail patients with metastatic colorectal cancer (MRC FOCUS2): an open-label,randomised factorial trial. Lancet 2011;377:1749-1759.
Van Cutsem E, Peeters M, Siena S, et al. Open-label phase III trial of panitumumab plus best supportive care compared with best supportive care alone in patientswith chemotherapy-refractory metastatic colorectal cancer. J Clin Oncol 2007;25:1658-1664.
Bouchahda M, Macarulla T, Spano JP, et al. Cetuximab efficacy and safety in a retrospective cohort of elderly patients with heavily pretreated metastatic colorectalcancer. Crit Rev Oncol Hematol 2008;67:255-262.
Cassidy J, Saltz LB, Giantonio BJ, et al. Effect of bevacizumab in older patients with metastatic colorectal cancer: pooled analysis of four randomized studies.J Cancer Res Clin Oncol 2010;136:737-743.
Kozloff MF, Berlin J, Flynn PJ, et al. Clinical outcomes in elderly patients with metastatic colorectal cancer receiving bevacizumab and chemotherapy: results from theBRiTE observational cohort study. Oncology 2010;78:329-339.
9
10
11
12
13
14
DISEASE-SPECIFIC ISSUES RELATED TO AGE
SAO-B5 of 13
(References)Colorectal Cancer
Printed by Kelly Hayden on 10/12/2012 3:09:21 PM. For personal use only. Not approved for distribution. Copyright © 2012 National Comprehensive Cancer Network, Inc., All Rights Reserved.

Version 2.2012, 11/15/11 © National Comprehensive Cancer Network, Inc. 2011, All rights reserved. The NCCN Guidelines and this illustration may not be reproduced in any form without the express written permission of NCCN .® ®
NCCN Guidelines IndexSenior Adult Oncology TOC
Discussion
� Elderly patients with head and neck cancer appear to have similar efficacy outcomes with surgery but higher complication rates which
increase with comorbidities.Patients > 70 with squamous cell carcinoma of the head and neck (SCCHN) who are treated with radiation therapy experience similar overall
survival in comparison to younger patients. Older adults are at increased risk for acute mucosal toxicities; however, there were no
significant differences in late toxicities seen in older patients compared to those younger than 70 (median of 3 years of follow-up).Regarding primary therapy for head and neck cancer, there are not enough data in patients over the age of 70 to draw firm conclusions
regarding a survival advantage of adding concurrent chemotherapy to radiation therapy.Concurrent chemotherapy with radiation and cisplatin improves laryngeal sparing over radiation alone in patients with localized T2 and T3
laryngeal cancer in patients both older and younger than 60.There is limited evidence for or against the benefit of cetuximab in combination with radiation therapy to treat locally advanced SCCHN in
patients older than 64. That available evidence in patients over the age of 64 does not allow one to draw firm conclusions regarding a
survival benefit of adding concurrent cetuximab to radiation.There is limited evidence for or against the benefit of adding cetuximab to chemotherapy in treating recurrent or metastatic SCCHN in
patients older than 64.Few patients over the age of 70 have been included in induction chemotherapy trials. There is limited data on the efficacy and toxicity of
such an approach in this subset of patients.In the adjuvant therapy of resected SCCHN, too few patients over the age of 70 have been evaluated to support or reject the addition of
cisplatin to radiation therapy.Retrospective studies suggest an increase in toxicity with chemotherapy when used alone and when used in combination with radiation
therapy in elderly patients.
1,2
4
5
6
7
8,9
10,11
12,13
�
�
�
�
�
�
�
�
3
NCCN Guidelines Version 2.2012Senior Adult Oncology
Head and Neck Cancers
DISEASE-SPECIFIC ISSUES RELATED TO AGE
Note: All recommendations are category 2A unless otherwise indicated.
Clinical Trials: NCCN believes that the best management of any cancer patient is in a clinical trial. Participation in clinical trials is especially encouraged.
SAO-B6 of 13
Continue
Printed by Kelly Hayden on 10/12/2012 3:09:21 PM. For personal use only. Not approved for distribution. Copyright © 2012 National Comprehensive Cancer Network, Inc., All Rights Reserved.
Version 2.2012, 11/15/11 © National Comprehensive Cancer Network, Inc. 2011, All rights reserved. The NCCN Guidelines and this illustration may not be reproduced in any form without the express written permission of NCCN .® ®
NCCN Guidelines IndexSenior Adult Oncology TOC
Discussion
NCCN Guidelines Version 2.2012Senior Adult Oncology
DISEASE-SPECIFIC ISSUES RELATED TO AGE
Continue
SAO-B7 of 13
Note: All recommendations are category 2A unless otherwise indicated.
Clinical Trials: NCCN believes that the best management of any cancer patient is in a clinical trial. Participation in clinical trials is especially encouraged.
DISEASE-SPECIFIC ISSUES RELATED TO AGE
1
2
3
13
Sanabria A, Carvalho AL, Melo RL, et al. Predictive factors for complications inelderly patients who underwent head and neck oncologic surgery. Head Neck2008;30:170-177.
Zabrodsky M, Calabrese L, Tosoni A, et al. Major surgery in elderly head andneck cancer patients: immediate and long-term surgical results andcomplication rates. Surg Oncol 2004;13:249-255.
Pignon T, Horiot JC, Van den Bogaert W, et al. No age limit for radicalradiotherapy in head and neck tumours. Eur J Cancer 1996;32A:2075-2081.
Pignon JP, le Maitre A, Maillard E, Bourhis J. Meta-analysis of chemotherapy inhead and neck cancer (MACH-NC): an update on 93 randomised trials and17,346 patients. Radiother Oncol 2009;92:4-14.
Forastiere AA, Goepfert H, Maor M, et al. Concurrent chemotherapy andradiotherapy for organ preservation in advanced laryngeal cancer.N Engl J Med 2003;349:2091-2098.
Bonner JA, Harari PM, Giralt J, et al. Radiotherapy plus cetuximab forlocoregionally advanced head and neck cancer: 5-year survival data from aphase 3 randomised trial, and relation between cetuximab-induced rash andsurvival. Lancet Oncol 2010;11:21-28.
Vermorken JB, Mesia R, Rivera F, et al. Platinum-based chemotherapy pluscetuximab in head and neck cancer. N Engl J Med 2008;359:1116-1127.
Vermorken JB, Remenar E, van Herpen C, et al. Cisplatin, fluorouracil, anddocetaxel in unresectable head and neck cancer. N Engl J Med2007;357:1695-1704.
Posner MR, Hershock DM, Blajman CR, et al. Cisplatin and fluorouracil aloneor with docetaxel in head and neck cancer. N Engl J Med 2007;357:1705-1715.
Cooper JS, Pajak TF, Forastiere AA, et al. Postoperative concurrentradiotherapy and chemotherapy for high-risk squamous-cell carcinoma of thehead and neck. N Engl J Med 2004;350:1937-1944.
Bernier J, Domenge C, Ozsahin M, et al. Postoperative irradiation with orwithout concomitant chemotherapy for locally advanced head and neck cancer.N Engl J Med 2004;350:1945-1952.
Machtay M, Moughan J, Trotti A, et al. Factors associated with severe latetoxicity after concurrent chemoradiation for locally advanced head and neckcancer: an RTOG analysis. J Clin Oncol 2008;26:3582-3589.
Argiris A, Li Y, Murphy BA, et al. Outcome of elderly patients with recurrent ormetastatic head and neck cancer treated with cisplatin-based chemotherapy.J Clin Oncol 2004;22:262-268.
4
5
6
7
8
9
10
11
12
(References)Head and Neck Cancers
Printed by Kelly Hayden on 10/12/2012 3:09:21 PM. For personal use only. Not approved for distribution. Copyright © 2012 National Comprehensive Cancer Network, Inc., All Rights Reserved.

Version 2.2012, 11/15/11 © National Comprehensive Cancer Network, Inc. 2011, All rights reserved. The NCCN Guidelines and this illustration may not be reproduced in any form without the express written permission of NCCN .® ®
NCCN Guidelines IndexSenior Adult Oncology TOC
Discussion
SAO-B8 of 13
Note: All recommendations are category 2A unless otherwise indicated.
Clinical Trials: NCCN believes that the best management of any cancer patient is in a clinical trial. Participation in clinical trials is especially encouraged.
1Bukowski RM, Stadler WM, McDermott DF, et al. Safety and efficacy of sorafenib in elderly patients treated in the North American advanced renal cell carcinomasorafenib expanded access program. Oncology 2010;78:340-347.Gore ME, Szczylik C, Porta C, et al. Safety and efficacy of sunitinib for metastatic renal-cell carcinoma: an expanded-access trial. Lancet Oncol 2009;10:757-763.Bajetta E, Ravaud A, Bracarda S, et al. Efficacy and safety of first-line bevacizumab (BEV) plus interferon-{alpha}2a (IFN) in patients (pts) >=65 years with metastaticrenal cell carcinoma (mRCC). ASCO Meeting Abstracts 2008;26:5095.
Osanto S, Hutson TE, Calvo E, et al. Efficacy and safety of everolimus in elderly patients (pts) with metastatic renal cell carcinoma (mRCC). ASCO Meeting Abstracts2010;28:4608.
Bellmunt J, Negrier S, Escudier B, et al. The medical treatment of metastatic renal cell cancer in the elderly: position paper of a SIOG Taskforce.Crit Rev Oncol Hematol 2009;69:64-72.
Eisen T, Oudard S, Szczylik C, et al. Sorafenib for older patients with renal cell carcinoma: subset analysis from a randomized trial.J Natl Cancer Inst 2008;100:1454-1463.
Hudes G, Carducci M, Tomczak P, et al. Temsirolimus, interferon alfa, or both for advanced renal-cell carcinoma. N Engl J Med 2007;356:2271-2281.
2
3
4
5
6
7
8Hutson TE, Bukowski RM, Rini BI, et al. A pooled analysis of the efficacy and safety of sunitinib in elderly patients (pts) with metastatic renal cell carcinoma (mRCC).ASCO Meeting Abstracts 2011;29:4604.
DISEASE-SPECIFIC ISSUES RELATED TO AGE
Kidney Cancer
�
�
�
Sorafenib and Sunitinib have similar efficacy in younger and older patients. Some adverse events, including fatigue, occur with increased
frequency.
Everolimus has similar efficacy in older and younger adults; however, older adults are at increased risk for adverse events (most commonly
stomatitis, anemia, and infection). The frequency of grade 3/4 for adverse events is low.
Interferon is not recommended for first line treatment. It has increased toxicity in patients 65 or older compared to temsirolimus, including
asthenia, nausea, fever and neutropenia.
1,2,5, 8
4
3,5,7
6,
NCCN Guidelines Version 2.2012Senior Adult Oncology
Printed by Kelly Hayden on 10/12/2012 3:09:21 PM. For personal use only. Not approved for distribution. Copyright © 2012 National Comprehensive Cancer Network, Inc., All Rights Reserved.
Version 2.2012, 11/15/11 © National Comprehensive Cancer Network, Inc. 2011, All rights reserved. The NCCN Guidelines and this illustration may not be reproduced in any form without the express written permission of NCCN .® ®
NCCN Guidelines IndexSenior Adult Oncology TOC
Discussion
NCCN Guidelines Version 2.2012Senior Adult Oncology
DISEASE-SPECIFIC ISSUES RELATED TO AGE
Note: All recommendations are category 2A unless otherwise indicated.
Clinical Trials: NCCN believes that the best management of any cancer patient is in a clinical trial. Participation in clinical trials is especially encouraged.
Multiple Myeloma
�
�
�
�
�
�
�
�
�
�
Choice of treatment might be dependent on the side effect profile but also the ability to travel for IV therapy.
In elderly patients receiving thalidomide based regimen, DVT) prophylaxis is recommended. Low molecular weight
heparin ( is superior to warfarin or aspirin.
VMP (Bortezomib, melphalan, and prednisone) in comparison to MP is associated with an increased response rate and overall survival at the
cost of increased toxicity (peripheral neuropathy, cytopenias, fatigue). The survival benefit is maintained across age groups.
VMP vs VTP (Bortezomib, thalidomide, and prednisone) have similar response rates and overall survival but differing side effect profiles
[VMP (hematologic toxicity, infection) and VTP (cardiac complications)]. Rates of neuropathy were similar in both groups.
VMPT (Bortezomib, melphalan, prednisone and thalidomide) followed by maintance VT (Bortezomib and thalidomide) vs VMP is associated
with higher response rate but does not improve overall survival. Weekly bortezomib is associated with a decreased rate of peripheral
neuropathy without a decrement in response.
High dose dexamethasone is associated with an increased risk of mortality and severe hematologic toxicities in comparison to
melphalan/prednisone.
Lenalidomide plus low-dose dexamethasone (in comparison to lenalidomide plus high-dose dexamethasone) is associated with an
improvement in overall survival and lower toxicity (less DVT, infections, and fatigue).
Older adults with multiple myeloma receiving MPT (melphalan, prednisone, and thalidomide) in comparison to MP (melphalan and
prednisone) had a higher response rate at the cost of increased toxicity (constipation, fatigue, increased venous thromboembolism (VTE),
neuropathy, cytopenias, and infection).
A survival benefit has been seen with MPT, although studies are conflicting and varying doses of thalidomide have been used.
MPT is associated with higher response rate and overall survival than transplant intermediate dose melphalan (MEL 100).
deep vein thrombosis (
LMWH)
1-9
1-9
2
10
11, 12
13
14
15
16
SAO-B9 of 13
Continue
Printed by Kelly Hayden on 10/12/2012 3:09:21 PM. For personal use only. Not approved for distribution. Copyright © 2012 National Comprehensive Cancer Network, Inc., All Rights Reserved.

Version 2.2012, 11/15/11 © National Comprehensive Cancer Network, Inc. 2011, All rights reserved. The NCCN Guidelines and this illustration may not be reproduced in any form without the express written permission of NCCN .® ®
NCCN Guidelines IndexSenior Adult Oncology TOC
Discussion
1
2
3
4
5
Beksac M, Haznedar R, Firatli-Tuglular T, et al. Addition of thalidomide to oral melphalan/prednisone in patients with multiple myeloma not eligible for transplantation:results of a randomized trial from the Turkish Myeloma Study Group. Eur J Haematol 2011;86:16-22.
Facon T, Mary JY, Hulin C, et al. Melphalan and prednisone plus thalidomide versus melphalan and prednisone alone or reduced-intensity autologous stem celltransplantation in elderly patients with multiple myeloma (IFM 99-06): a randomised trial. Lancet 2007;370:1209-1218.
Hulin C, Facon T, Rodon P, et al. Efficacy of melphalan and prednisone plus thalidomide in patients older than 75 years with newly diagnosed multiple myeloma: IFM01/01 trial. J Clin Oncol 2009;27:3664-3670.
Kapoor P, Rajkumar SV, Dispenzieri A, et al. Melphalan and prednisone versus melphalan, prednisone and thalidomide for elderly and/or transplant-ineligible patientswith multiple myeloma: a meta-analysis. Leukemia 2011;25:1523-1524.
Ludwig H, Hajek R, Tothova E, et al. Thalidomide-dexamethasone compared with melphalan-prednisolone in elderly patients with multiple myeloma.Blood 2009;113:3435-3442.
6
7
8
9
10
11
12
13
14
15
16
Palumbo A, Bringhen S, Caravita T, et al. Oral melphalan and prednisone chemotherapy plus thalidomide compared with melphalan and prednisone alone in elderlypatients with multiple myeloma: randomised controlled trial. Lancet 2006;367:825-831.
Palumbo A, Bringhen S, Liberati AM, et al. Oral melphalan, prednisone, and thalidomide in elderly patients with multiple myeloma: updated results of a randomizedcontrolled trial. Blood 2008;112:3107-3114.
Waage A, Gimsing P, Fayers P, et al. Melphalan and prednisone plus thalidomide or placebo in elderly patients with multiple myeloma. Blood 2010;116:1405-1412.
Wijermans P, Schaafsma M, Termorshuizen F, et al. Phase III study of the value of thalidomide added to melphalan plus prednisone in elderly patients with newlydiagnosed multiple myeloma: the HOVON 49 Study. J Clin Oncol 2010;28:3160-3166.
Palumbo A, Cavo M, Bringhen S, et al. Aspirin, warfarin, or enoxaparin thromboprophylaxis in patients with multiple myeloma treated with thalidomide: a phase III,open-label, randomized trial. J Clin Oncol 2011;29:986-993.
Mateos M-V, Richardson PG, Schlag R, et al. Bortezomib plus melphalan and prednisone compared with melphalan and prednisone in previously untreated multiplemyeloma: updated follow-up and impact of subsequent therapy in the phase III VISTA trial. J Clin Oncol 2010;28:2259-2266.
San Miguel JF, Schlag R, Khuageva NK, et al. Bortezomib plus melphalan and prednisone for initial treatment of multiple myeloma. N Engl J Med 2008;359:906-917.
Mateos M-V, Oriol A, Martinez-Lopez J, et al. Bortezomib, melphalan, and prednisone versus bortezomib, thalidomide, and prednisone as induction therapy followedby maintenance treatment with bortezomib and thalidomide versus bortezomib and prednisone in elderly patients with untreated multiple myeloma: a randomised trial.Lancet Oncol 2010;11:934-941.
Palumbo A, Bringhen S, Rossi D, et al. Bortezomib-melphalan-prednisone-thalidomide followed by maintenance with bortezomib-thalidomide compared withbortezomib-melphalan-prednisone for initial treatment of multiple myeloma: a randomized controlled trial. J Clin Oncol 2010;28:5101-5109.
Facon T, Mary J-Y, Pegourie B, et al. Dexamethasone-based regimens versus melphalan-prednisone for elderly multiple myeloma patients ineligible for high-dosetherapy. Blood 2006;107:1292-1298.
Rajkumar SV, Jacobus S, Callander NS, et al. Lenalidomide plus high-dose dexamethasone versus lenalidomide plus low-dose dexamethasone as initial therapy fornewly diagnosed multiple myeloma: an open-label randomised controlled trial. Lancet Oncol 2010;11:29-37.
Note: All recommendations are category 2A unless otherwise indicated.
Clinical Trials: NCCN believes that the best management of any cancer patient is in a clinical trial. Participation in clinical trials is especially encouraged.
NCCN Guidelines Version 2.2012Senior Adult Oncology
DISEASE-SPECIFIC ISSUES RELATED TO AGE
SAO-B10 of 13
(References)Multiple Myeloma
Printed by Kelly Hayden on 10/12/2012 3:09:21 PM. For personal use only. Not approved for distribution. Copyright © 2012 National Comprehensive Cancer Network, Inc., All Rights Reserved.

Version 2.2012, 11/15/11 © National Comprehensive Cancer Network, Inc. 2011, All rights reserved. The NCCN Guidelines and this illustration may not be reproduced in any form without the express written permission of NCCN .® ®
NCCN Guidelines IndexSenior Adult Oncology TOC
Discussion
NCCN Guidelines Version 2.2012Senior Adult Oncology
DISEASE-SPECIFIC ISSUES RELATED TO AGE
Note: All recommendations are category 2A unless otherwise indicated.
Clinical Trials: NCCN believes that the best management of any cancer patient is in a clinical trial. Participation in clinical trials is especially encouraged.
Non-Small Cell Lung Cancer
Surgery
Adjuvant Chemotherapy
Locally Advanced Disease
Advanced Disease
1-6
7-8
9-12
13-22
�
�
�
�
�
�
�
�
Few prospective studies.
Retrospective analyses demonstrate that older patients who are selected for surgery tolerate it well.
Caution with pneumonectomy in older adults.
The benefits of adjuvant chemotherapy are similar with age.
Combined modality therapy: While efficacy is maintained, older adults (especially those with a KPS <90) are more likely to have side effects
(esophagitis, pneumonitis, myelosuppression).
As in younger patients, chemotherapy is associated with improved QOL in comparison to best supportive care.
Emerging data is confirming the survival benefit of doublet chemotherapy in comparison to single agent treatment.
Use Bevacizumab with caution in patients 70 years or older. Toxicities are increased in older adult (caution with myelosuppression). See
for the growth factor support.NCCN Myeloid Growth Factor Guidelines
1 Cangemi V, Volpino P, D'Andrea N, et al. Lung cancer surgery in elderly patients. Tumori 1996;82:237-241.
Naunheim KS, Kesler KA, D'Orazio SA, et al. Lung cancer surgery in the octogenarian. Eur J Cardiothorac Surg 1994;8:453-456.
Jack CI, Lye M, Lesley F, et al. Surgery for lung cancer: age alone is not a contraindication. Int J Clin Pract 1997;51:423-426.
Morandi U, Stefani A, Golinelli M, et al. Results of surgical resection in patients over the age of 70 years with non small-cell lung cancer. Eur J Cardiothorac Surg1997;11:432-439.
Ishida T, Yokoyama H, Kaneko S, et al. Long-term results of operation for non-small cell lung cancer in the elderly. Ann Thorac Surg 1990;50:919-922.
Mizushima Y, Noto H, Sugiyama S, et al. Survival and prognosis after pneumonectomy for lung cancer in the elderly. Ann Thorac Surg 1997;64:193-198.
Pepe C, Hasan B, Winton TL, et al. Adjuvant vinorelbine and cisplatin in elderly patients: National Cancer Institute of Canada and Intergroup Study JBR.10.J Clin Oncol 2007;25:1553-1561.
Chemotherapy in non-small cell lung cancer: a meta-analysis using updated data on individual patients from 52 randomised clinical trials. Non-small Cell Lung CancerCollaborative Group. BMJ 1995;311:899-909.
Movsas B, Scott C, Sause W, et al. The benefit of treatment intensification is age and histology-dependent in patients with locally advanced non-small cell lung cancer(NSCLC): a quality-adjusted survival analysis of radiation therapy oncology group (RTOG) chemoradiation studies. Int J Radiat Oncol Biol Phys 1999;45:1143-1149.
2
3
4
5
6
7
8
9
SAO-B11 of 13
Continue
Printed by Kelly Hayden on 10/12/2012 3:09:21 PM. For personal use only. Not approved for distribution. Copyright © 2012 National Comprehensive Cancer Network, Inc., All Rights Reserved.
Version 2.2012, 11/15/11 © National Comprehensive Cancer Network, Inc. 2011, All rights reserved. The NCCN Guidelines and this illustration may not be reproduced in any form without the express written permission of NCCN .® ®
NCCN Guidelines IndexSenior Adult Oncology TOC
Discussion
10 Werner-Wasik M, Scott C, Cox JD, et al. Recursive partitioning analysis of 1999 Radiation Therapy Oncology Group (RTOG) patients with locally-advanced non-small-cell lung cancer (LA-NSCLC): identification of five groups with different survival. Int J Radiat Oncol Biol Phys 2000;48:1475-1482.
11
12
13
14
15
16
17
18
19
20
21
22
Langer CJ, Hsu C, Curran WJ, et al. Elderly patients (pts) with locally advanced non-small cell lung cancer (LA-NSCLC) benefit from combined modality therapy:secondary analysis of Radiation Therapy Oncology Group (RTOG) 94-10. Proc Am Soc Clin Oncol 2002;21:Abstract 1193.
Schild SE, Stella PJ, Geyer SM, et al. The outcome of combined-modality therapy for stage III non-small-cell lung cancer in the elderly.J Clin Oncol 2003;21:3201-3206.
Kelly K, Giarritta S, Akerley W, et al. Should Older Patients (Pts) Receive Combination Chemotherapy for Advanced Stage Non-Small Cell Lung Cancer (NSCLC)? AnAnalysis of Southwest Oncology Trials 9509 and 9308. Proc Am Soc Clin Oncol 2001;20:Abstract 1313.
Langer CJ, Manola J, Bernardo P, et al. Cisplatin-based therapy for elderly patients with advanced non-small-cell lung cancer: implications of Eastern CooperativeOncology Group 5592, a randomized trial. J Natl Cancer Inst 2002;94:173-181.
Langer CJ, Vangel M, Schiller J, et al. Age-specific subanalysis of ECOG 1594: Fit elderly patients (70-80 YRS) with NSCLC do as well as younger pts (<70).Proc Am Soc Clin Oncol 2003;22:Abstract 2571.
Lilenbaum RC, Herndon JE, List MA, et al. Single-agent versus combination chemotherapy in advanced non-small-cell lung cancer: the cancer and leukemia group B(study 9730). J Clin Oncol 2005;23:190-196.
Ramalingam SS, Dahlberg SE, Langer CJ, et al. Outcomes for elderly, advanced-stage non small-cell lung cancer patients treated with bevacizumab in combinationwith carboplatin and paclitaxel: analysis of Eastern Cooperative Oncology Group Trial 4599. J Clin Oncol 2008;26:60-65.
Gridelli C. The ELVIS trial: a phase III study of single-agent vinorelbine as first-line treatment in elderly patients with advanced non-small cell lung cancer. Elderly LungCancer Vinorelbine Italian Study. Oncologist 2001;6 Suppl 1:4-7.
Frasci G, Lorusso V, Panza N, et al. Gemcitabine plus vinorelbine yields better survival outcome than vinorelbine alone in elderly patients with advanced non-smallcell lung cancer. A Southern Italy Cooperative Oncology Group (SICOG) phase III trial. Lung Cancer 2001;34 Suppl 4:65-69.
Gridelli C, Perrone F, Gallo C, et al. Chemotherapy for elderly patients with advanced non-small-cell lung cancer: the Multicenter Italian Lung Cancer in the ElderlyStudy (MILES) phase III randomized trial. J Natl Cancer Inst 2003;95:362-372.
Kudoh S, Takeda K, Nakagawa K, et al. Phase III study of docetaxel compared with vinorelbine in elderly patients with advanced non-small-cell lung cancer: results ofthe West Japan Thoracic Oncology Group Trial (WJTOG 9904). J Clin Oncol 2006;24:3657-3663.
Quoix E, Zalcman G, Oster JP, et al. Carboplatin and weekly paclitaxel doublet chemotherapy compared with monotherapy in elderly patients with advanced non-small-cell lung cancer: IFCT-0501 randomised, phase 3 trial. Lancet 2011;378:1079-1088.
NCCN Guidelines Version 2.2012Senior Adult Oncology
DISEASE-SPECIFIC ISSUES RELATED TO AGE
Note: All recommendations are category 2A unless otherwise indicated.
Clinical Trials: NCCN believes that the best management of any cancer patient is in a clinical trial. Participation in clinical trials is especially encouraged.
SAO-B12 of 13
(References)Non-Small Cell Lung Cancer (continued)
Printed by Kelly Hayden on 10/12/2012 3:09:21 PM. For personal use only. Not approved for distribution. Copyright © 2012 National Comprehensive Cancer Network, Inc., All Rights Reserved.

Version 2.2012, 11/15/11 © National Comprehensive Cancer Network, Inc. 2011, All rights reserved. The NCCN Guidelines and this illustration may not be reproduced in any form without the express written permission of NCCN .® ®
NCCN Guidelines IndexSenior Adult Oncology TOC
Discussion
NCCN Guidelines Version 2.2012Senior Adult Oncology
Prostate Cancer
DISEASE-SPECIFIC ISSUES RELATED TO AGE
Note: All recommendations are category 2A unless otherwise indicated.
Clinical Trials: NCCN believes that the best management of any cancer patient is in a clinical trial. Participation in clinical trials is especially encouraged.
�
�
�
For treatment of clinically localized or locally advanced prostate cancer, see
There are no age-related differences in docetaxel efficacy in patients with castration-resistant prostate cancer. Growth factor support should
be considered in patients 65 or older to decrease the risk of neutropenic complications. See .
There are no age-related differences in cabazitaxel efficacy in patients with castration-resistant prostate cancer. Growth factor support is
strongly recommended in patients 65 or older to decrease the risk of neutropenic complications in the elderly.
.
1,2
3,4 See
.
NCCN Prostate Cancer Guidelines
NCCN Myeloid Growth Factors Guidelines
NCCN Myeloid Growth
Factors Guidelines
SAO-B13 of 13
Continue
1
2
3
4
Tannock IF, de Wit R, Berry WR, et al. Docetaxel plus prednisone or mitoxantrone plus prednisone for advanced prostate cancer. N Engl J Med 2004;351:1502-1512.
Sinibaldi VJ. Docetaxel treatment in the elderly patient with hormone refractory prostate cancer. Clin Interv Aging 2007;2:555-560.
Pal SK, Twardowski P, Sartor O. Critical appraisal of cabazitaxel in the management of advanced prostate cancer. Clin Interv Aging 2010;5:395-402.
de Bono JS, Oudard S, Ozguroglu M, et al. Prednisone plus cabazitaxel or mitoxantrone for metastatic castration-resistant prostate cancer progressing after docetaxeltreatment: a randomised open-label trial. Lancet 2010;376:1147-1154.
Printed by Kelly Hayden on 10/12/2012 3:09:21 PM. For personal use only. Not approved for distribution. Copyright © 2012 National Comprehensive Cancer Network, Inc., All Rights Reserved.
Version 2.2012, 11/15/11 © National Comprehensive Cancer Network, Inc. 2011, All rights reserved. The NCCN Guidelines and this illustration may not be reproduced in any form without the express written permission of NCCN .® ®
NCCN Guidelines IndexSenior Adult Oncology TOC
Discussion
COMPREHENSIVE GERIATRIC ASSESSMENT
Functional status
Socioeconomic issues: ( )
Psychosocial Distress:
i
�
�
�
�
�
�
�
Activities of daily living (ADL) - Eating, dressing, continence, grooming, transferring, using the bathroom
Instrumental activities of daily living (IADL) - Using transportation, managing money, taking medications, shopping, preparing meals,
doing laundry, doing housework, using telephone
Performance status
Falls
Gait speed
Comorbidities
May affect treatment decisions in 4 ways:Cancer treatment may interact with comorbidity to impact functional status or worsen the comorbidity. This includes any drug-drug
interactions.Cancer treatment may be too risky because of the type and severity of comorbidityCancer treatment may not impact future life expectancy due to risk of morbidity associated with comorbid condition. The effect of
comorbidity on life expectancy should be evaluated before patient receives treatment.Comorbidity may affect treatment outcome.
Number and severity of comorbidities should be assessed.Adult comorbidity evaluation index (ACE-27)Charlson comorbidity index (CCI)Cumulative Illness Rating Scale (CIRS)OARS multidimensional functional assessment questionnaire
1
j
2
3
4
5
��
�
�
�
�
�
�
See SAO-2
See NCCN Distress Management Guidelines
Note: All recommendations are category 2A unless otherwise indicated.
Clinical Trials: NCCN believes that the best management of any cancer patient is in a clinical trial. Participation in clinical trials is especially encouraged.
NCCN Guidelines Version 2.2012Senior Adult Oncology
i
jMortality can be predicted using weight, body mass index, nutrition, fatigue and existing medical conditions.
See Procedure for Functional Assessment Screening in Elderly Persons (SAO-D).
See references SAO-C 3 of 3
SAO-C1 of 3
Printed by Kelly Hayden on 10/12/2012 3:09:21 PM. For personal use only. Not approved for distribution. Copyright © 2012 National Comprehensive Cancer Network, Inc., All Rights Reserved.
Version 2.2012, 11/15/11 © National Comprehensive Cancer Network, Inc. 2011, All rights reserved. The NCCN Guidelines and this illustration may not be reproduced in any form without the express written permission of NCCN .® ®
NCCN Guidelines IndexSenior Adult Oncology TOC
Discussion
NCCN Guidelines Version 2.2012Senior Adult Oncology
SAO-C2 of 3
Note: All recommendations are category 2A unless otherwise indicated.
Clinical Trials: NCCN believes that the best management of any cancer patient is in a clinical trial. Participation in clinical trials is especially encouraged.
Cognitive function
DementiaMini Mental State Examination (MMSE)Montreal Cognitive Assessment (MoCA)
DepressionGeriatric Depression Scale (GDS)
DeliriumConfusion Assessment Method and/or Memorial Delirium Assessment Scale
Polypharmacy
Medication review for duplication and appropriate use should be performed at every visitMedication Appropriateness IndexBeers CriteriaSTART/STOPP Criteria
Review drug interactions
Special considerations for over/under-use, duration of therapy and dosage when using these classes of medicationsBenzodiazepinesAnticholinergicsAntipsychoticsOpioidsCorticosteroids
Nutritional StatusBody Mass IndexWeight lossNutritional deficiency--Mini-Nutritional Assessment (MNA)
OsteoporosisDexa scan
�
�
�
�
�
�
�
�
�
�
�
�
�
�
�
�
�
6,7
13
14
15,16
18,19
8
9,10
11,12
17
20,21
http://www.mocatest.org/
See NCCN Distress Management Guidelines
See NCCN Palliative Care Guidelines and NCCN Distress Management Guidelines
See NCCN Bone Health Task Force
�
�
�
�
�
�
�
�
COMPREHENSIVE GERIATRIC ASSESSMENT
See references SAO-C 3 of 3
Printed by Kelly Hayden on 10/12/2012 3:09:21 PM. For personal use only. Not approved for distribution. Copyright © 2012 National Comprehensive Cancer Network, Inc., All Rights Reserved.

Version 2.2012, 11/15/11 © National Comprehensive Cancer Network, Inc. 2011, All rights reserved. The NCCN Guidelines and this illustration may not be reproduced in any form without the express written permission of NCCN .® ®
NCCN Guidelines IndexSenior Adult Oncology TOC
Discussion
NCCN Guidelines Version 2.2012Senior Adult Oncology
Note: All recommendations are category 2A unless otherwise indicated.
Clinical Trials: NCCN believes that the best management of any cancer patient is in a clinical trial. Participation in clinical trials is especially encouraged.
1
2
3
4
5
8
11
13
14
15
16
Studenski S, Perera S, Patel K, et al. Gait speed and survival in older adults. JAMA 2011;305:50-58.Piccirillo JF, Tierney RM, Costas I, et al. Prognostic importance of comorbidity in a hospital-based cancer registry. JAMA 2004;291:2441-2447.Charlson ME, Pompei P, Ales KL, MacKenzie CR. A new method of classifying prognostic comorbidity in longitudinal studies: development and validation.J Chronic Dis 1987;40:373-383.Linn BS, Linn MW, Gurel L. Cumulative illness rating scale. J Am Geriatr Soc 1968;16:622-626.Fillenbaum GG, Smyer MA. The development, validity, and reliability of the OARS multidimensional functional assessment questionnaire. Journal of gerontology1981;36:428-34.Tombaugh TN, McIntyre NJ. The mini-mental state examination: a comprehensive review. J Am Geriatr Soc.1992;40(9):922-935.Crum RM, Anthony JC, Bassett SS, Folstein MF. Population-based norms for the Mini-Mental State Examination by age and educational level. JAMA.1993;269(18):2386-2391.Nasreddine ZS, Phillips NA, Bedirian V, et al. The Montreal Cognitive Assessment, MoCA: a brief screening tool for mild cognitive impairment. J Am Geriatr Soc.2005;53:695-699.
Yesavage JA, Brink TL, Rose TL, et al. Development and validation of a geriatric depression screening scale: a preliminary report. J Psychiatr Res. 1982;17(1):37-49.
D'Ath P, Katona P, Mullan E, Evans S, Katona C. Screening, Detection and Management of Depression in Elderly Primary Care Attenders: The Acceptability andPerformance of the 15 Item Geriatric Depression Scale (GDS15) and the Development of Short Versions. Fam. Pract. 1994;11(3):260-266.
Inouye SK, van Dyck CH, Alessi CA, et al. Clarifying confusion: the confusion assessment method. A new method for detection of delirium. Ann Intern Med.1990;113:941-948.
Lawlor PG, Nekolaichuk C, Gagnon B, et al. Clinical utility, factor analysis, and further validation of the memorial delirium assessment scale in patients with advancedcancer: Assessing delirium in advanced cancer. Cancer. 2000;88:2859-2867.
Samsa GP, Hanlon JT, Schmader KE, Weinberger M, Clipp EC, Uttech KM, Lewis IK, Landsman, Cohen HJ. A summated score for the medication appropriatenessindex: development and assessment of clinimetric properties including content validity. J Clin Epidemiology. 1994;47(8):891-6.
Fick DM, Cooper JW, Wade WE, Waller JL, Maclean JR, Beers MH. Updating the Beers criteria for potentially inappropriate medications use in older adults: results ofa US consensus panel of experts. Archives of Internal Medicene. 2003;163(22):2716-24.
Barry PJ, Gallagher P, Ryan C, O'Mahony D. START (screening tool to alert doctors to the right treatment) – an evidence-based screening tool to detect prescribingomissions in elderly patients. Age and Ageing 2007;36:632-638.Gallagher P and O'Mahony D. STOPP (Screening Tool of Older Persons' potentially inappropriate Prescriptions): application to acutely ill elderly patients andcomparison with Beers' criteria. Age and Ageing 2008;37:673-679.
Vellas B, Guigoz Y, Garry PJ, et al. The Mini Nutritional Assessment (MNA) and its use in grading the nutritional state of elderly patients. Nutrition.1999;15(2):116-122.
Rubenstein LZ, Harker JO, Salva A, Guigoz Y, Vellas B. Screening for Undernutrition in Geriatric Practice: Developing the Short-Form Mini-Nutritional Assessment(MNA-SF). J Gerontol A Biol Sci Med Sci. 2001;56(6):M366-372.
6
7
9
10
12
20
21
17
18
19
Riechelmann RP, Saad ED. A systemic review on drug interactions in oncology. Cancer Investigation. 2006;24:704-712.
Hilmer SN, Mager DE, Simonsick EM, Cao Y, Ling SM, Windham, G, Harris TB, Hanlon JT, Rubin SM, Shorr RI, Bauer DC, Abernathy DR. A drug burden index todefine the functional burden of medications in older people. Archives of Internal Medicine. 2007;167:781-787.
Chew ML, Mulsant BH, Pollock BG, et al. Anticholinergic activity of the 107 medications commonly used by older adults. J Am Geriatr Soc 2008;56:1333-1341.
REFERENCES
SAO-C3 of 3
Printed by Kelly Hayden on 10/12/2012 3:09:21 PM. For personal use only. Not approved for distribution. Copyright © 2012 National Comprehensive Cancer Network, Inc., All Rights Reserved.
Version 2.2012, 11/15/11 © National Comprehensive Cancer Network, Inc. 2011, All rights reserved. The NCCN Guidelines and this illustration may not be reproduced in any form without the express written permission of NCCN .® ®
NCCN Guidelines IndexSenior Adult Oncology TOC
Discussion
NCCN Guidelines Version 2.2012Senior Adult Oncology
Note: All recommendations are category 2A unless otherwise indicated.
Clinical Trials: NCCN believes that the best management of any cancer patient is in a clinical trial. Participation in clinical trials is especially encouraged.
Target Area
Vision
Hearing
Arm
Leg
Urinaryincontinence
Nutrition
Mental status
Depression
ADL-IADL
Homeenvironment
Social support
PROCEDURE FOR FUNCTIONAL ASSESSMENT SCREENING IN ELDERLY PERSONS
Assessment Procedure
Test each eye with Jaeger card while patient wearscorrective lenses (if applicable)
Whisper a short, easily answered question, such as“What is your name?” in each ear while theexaminer's face is out of direct view.
Proximal: “Touch the back of your head with bothhands.”Distal: “Pick up the spoon.”
Observe the patient after asking “Rise from yourchair, walk 10 ft, return, and sit down.”*
Ask patient: “Do you ever lose your urine and getwet?”
Weigh the patient. Measure height.
Tell the patient: “I am going to name three objects(pencil, truck, book). I will ask you to repeat theirnames now and then again a few minutes fromnow.”†
Ask patient: “Do you often feel sad or depressed?”
Ask patient: “Can you get out of bed yourself?”; “Canyou dress yourself?”; “Can you make your ownmeals?”; “Can you do your own shopping?”
Ask patient: “Do you have trouble with stairs inside oroutside of your home?”; ask about potential hazardsinside the home with bathtubs, rugs, or lighting.
Ask patient: “Who would be able to help you in caseof illness or emergency?”
Abnormal Result
Inability to read > 20/40
Inability to answerquestion
Inability to dotask
Inability to walk ortransfer out of chair
Yes
Weight is below accept-able range for height
Inability to recall all 3objects after 1 min
Yes
No to any question
Yes
…
Suggested Intervention
Refer to ophthalmologist
Examine auditory canals for cerumen and clean if necessary. Repeat test; if stillabnormal in either ear, refer for audiometry and possible prosthesis.
Examine the arm fully (muscle, joint, and nerve) paying attention to pain,weakness, limited range of motion.Consider referral for physical therapy and occupational therapy.
Do full neurologic and musculoskeletal evaluation, paying attention to strength,pain, range of motion, balance, and traditional assessment of gait. Considerreferral for physical therapy and occupational therapy.
Ascertain frequency and amount. Search for remediable causes including localirritations, polyuric states, and medications. Consider urologic referral.
Do appropriate medical evaluation.Consider dietician referral.
Administer Folstein mini-mental status examination. If score is < 24, search forcauses of cognitive impairment. Ascertain onset, duration, and fluctuation ofovert symptoms. Review medications. Assess consciousness and affect. Doappropriate laboratory tests.
Administer Geriatric Depression Scale. If positive (normal score, 0 to 10),check for antihypertensive, psychotropic, or other pertinent medications.Consider appropriate pharmaceutical or psychiatric treatment.
Corroborate responses with patient's appearance; question family members ifaccuracy is uncertain. Determine reasons for the inability (motivation comparedwith physical limitation). Institute appropriate medical, social, or environmentalinterventions.
Evaluate home safety and institute appropriate countermeasures.
List identified persons in the medical record. Become familiar with availableresources for the elderly in the community. Consider social worker referral.
ADL, activities of daily living; IADL, instrumental activities of daily living.Adapted with permission from Lachs MS, Feinstein AR, Cooney LM Jr, et al. A simple procedure forgeneral screening for functional disability in elderly patients. Ann Intern Med 1990;112:699-706.*This test is similar to the “timed up and go” (TUG) test, except that for the TUG test patients arealso asked to walk 20 ft briskly. For the TUG test, a score of “one” is assigned for each of these
findings: (1) use of the arms to get up, (2) uncertain steps, and/or (3) more than 10 seconds tocomplete the activity. The higher the total score, the higher the risk of functional dependence anddeath.†This test is also referred to as the “three-item recall.” It can be supplemented by the clockdrawing test to assist in assessment for dementia.
SAO-D
Printed by Kelly Hayden on 10/12/2012 3:09:21 PM. For personal use only. Not approved for distribution. Copyright © 2012 National Comprehensive Cancer Network, Inc., All Rights Reserved.
Version 2.2012, 11/15/11 © National Comprehensive Cancer Network, Inc. 2011, All rights reserved. The NCCN Guidelines® and this illustration may not be reproduced in any form without the express written permission of NCCN®. MS-1
NCCN Guidelines IndexSenior Adult Oncology TOC
Discussion
NCCN Guidelines Version 2.2012 Senior Adult Oncolo gy
Discussion
NCCN Categories of Evidence and Consensus
Category 1: Based upon high-level evidence, there is uniform NCCN
consensus that the intervention is appropriate.
Category 2A: Based upon lower-level evidence, there is uniform
NCCN consensus that the intervention is appropriate.
Category 2B: Based upon lower-level evidence, there is NCCN
consensus that the intervention is appropriate.
Category 3: Based upon any level of evidence, there is major NCCN
disagreement that the intervention is appropriate.
All recommendations are category 2A unless otherwise noted.
Overview Cancer is the leading cause of death in women and men aged 60 to 79 years.1 More than 50% of all cancers and more than 70% of cancer-related deaths in the United States occur in patients who are 65 years or older.2 It is estimated that by 2030 approximately 70% of all cancers will be diagnosed in adults 65 years or older.3 Older individuals are more prone to develop cancer than younger individuals. Furthermore, the aging in the US population and increased life expectancy of the elderly mean that cancer in older adults is becoming an increasingly common problem.
There are unique issues to consider when caring for an older adult with cancer. The biology of certain neoplasms and responsiveness to therapy changes with the patient’s age.4 Furthermore, the patient’s physiologic status, comorbidities, and preferences may influence the
selection and tolerance to certain therapies. Together, these age-related issues form the basis for the development of guidelines that address special considerations in older adults with cancer.
Older adults with cancer are under-represented in clinical trials for new cancer therapies.5 Therefore there is less evidence based data to guide the treatment of these patients. However, advanced age alone should not preclude the use of effective cancer treatment that could improve quality of life or extend meaningful survival.6,7 Treatment that diminishes quality of life with no significant survival benefit should be avoided. The available data suggests that older patients in good performance status are able to tolerate commonly used chemotherapy regimens as well as younger patients, particularly when adequate supportive care is provided.8-10 However, there have been few studies that have addressed patients at the extremes of age or those with poor performance status. The physiological changes associated with aging, may impact an older adult’s ability to tolerate cancer therapy and should be considered in the treatment decision making process.
The NCCN Senior Adult Oncology guidelines address specific issues related to the management of cancer in older individuals including screening and comprehensive geriatric assessment, assessing the risks and benefits of treatment, preventing or decreasing complications from therapy, disease-specific issues, and management of patients unfit for standard treatment.
Comprehensive Geriatric Assessment Older patients can be classified into three categories: (1) young old patients are 65-75 years of age; (2) old patients are 76-85 years of age; and (2) oldest old patients are more than 85 years of age.11 Proper selection of patients is the key to administering effective and safe cancer treatment. The challenge of managing the older cancer patient
Printed by Kelly Hayden on 10/12/2012 3:09:21 PM. For personal use only. Not approved for distribution. Copyright © 2012 National Comprehensive Cancer Network, Inc., All Rights Reserved.

Version 2.2012, 11/15/11 © National Comprehensive Cancer Network, Inc. 2011, All rights reserved. The NCCN Guidelines® and this illustration may not be reproduced in any form without the express written permission of NCCN®. MS-2
NCCN Guidelines IndexSenior Adult Oncology TOC
Discussion
NCCN Guidelines Version 2.2012 Senior Adult Oncolo gy
is to assess whether the expected benefits of treatment are superior to the risk in a population with decreased life expectancy and decreased tolerance to stress. Chronological age by itself is not reliable in estimating life expectancy. functional reserve, or the risk of treatment complications.12 While it is not possible for a physician to predict the exact life expectancy of an individual patient, it is possible to provide an estimate of whether a patient is likely to live longer or shorter than an average person of similar age. Life expectancy at a given age can be estimated using life table data as suggested by Walter and Covinsky.13 For example, about 25% of the healthiest 75-year-old women will live more than 17 years, 50% will live at least 12 years, and 25% will live less than 7 years. Lee and colleagues developed and validated a potentially useful tool for clinicians to estimate the 4-year mortality risk.14 Patients can be stratified into three groups of varying risk of mortality (high, intermediate or low) based on the prognostic index which incorporates demographic variables (age and sex), self-reported comorbid conditions and functional measures.14 Carey and colleagues also developed a similar functional morbidity index based on self-reported functional status, age and gender to stratify elders into varying risk groups for 2-year mortality.15 In pooled analysis of individual data from 9 selected cohorts, Studenski et al reported that gait speed was associated with survival in older adults.
Comprehensive geriatric assessment (CGA) is a multidisciplinary in depth evaluation to assess life expectancy and risk of morbidity from cancer in elderly patients.16-18 CGA includes assessment tools to predict the functional age of elderly patients with cancer based on functional status, comorbidities that may interfere with cancer treatment, polypharmacy, nutritional status, cognitive function,
psychological status, socioeconomic issues and geriatric syndromes. The feasibility of CGA has been demonstrated in elderly patients with cancer.19-21 Balducci and Extermann studied CGA in the older cancer patient including an evaluation of functional status, comorbidity, socioeconomic conditions, cognitive and emotional function, nutritional status, polypharmacy and geriatric syndromes.19 Ingram et al used a self-administered CGA including demographics, comorbid conditions, functional status, pain, financial well being, social support, emotional state, spiritual well-being, and quality of life to characterize older cancer patients.20 Repetto et al demonstrated that CGA adds substantial information on the functional assessment of elderly cancer patients (65 or older).21 Among patients with a good performance status, 13% had two or more comorbidities; 9.3% and 37.7% had ADL or IADL limitations, respectively.
CGA components (comorbid conditions, functional status, geriatric syndromes and nutritional status) have been associated with the type of cancer treatment and survival in elderly patients with cancer.22-26 For example, in women 65 years or older diagnosed with stage I-III primary breast cancer, the all-cause and breast-cancer-specific death rate at 5 and 10 years was consistently approximately two times higher in women with 3 or more cancer-specific CGA deficits, regardless of age and stage of disease.25 In another prospective study of 375 consecutive elderly patients with cancer (ELCAPA study), in a multivariate analysis, a lower ADL score and malnutrition were independently associated with cancer treatment changes.26
Although CGA is helpful for physicians to develop a coordinated plan for cancer treatment as well as to guide appropriate interventions to the patient’s problems, it can be time consuming and may not be practical for all patients. Hurria and colleagues have developed a brief but comprehensive, geriatric assessment of older patients with cancer.27, 28
Printed by Kelly Hayden on 10/12/2012 3:09:21 PM. For personal use only. Not approved for distribution. Copyright © 2012 National Comprehensive Cancer Network, Inc., All Rights Reserved.

Version 2.2012, 11/15/11 © National Comprehensive Cancer Network, Inc. 2011, All rights reserved. The NCCN Guidelines® and this illustration may not be reproduced in any form without the express written permission of NCCN®. MS-3
NCCN Guidelines IndexSenior Adult Oncology TOC
Discussion
NCCN Guidelines Version 2.2012 Senior Adult Oncolo gy
A multicenter study involving 500 older patients (median age: 73) with cancer demonstrated that this brief geriatric assessment (including functional status, comorbidity, cognition, psychological status, social functioning and support, and nutritional status) is largely self-administered and can be completed by the majority of older patients without assistance.27 The geriatric assessment also identified deficits and problems that may impact morbidity and mortality.28 Recent results from the CALGB 360401 study demonstrated the feasibility of including this brief, primarily self-administered geriatric assessment tool in future cooperative group clinical trial.29 Overcash et al have developed an abbreviated CGA that could be helpful in screening for those elderly patients who would benefit from an entire CGA.30, 31
Functional Status
Functional status in older patients with cancer can be evaluated based on their ability to complete activities of daily living (ADL) and instrumental activities of daily living (IADL).32, 33 IADLs encompass complex skills that are necessary for maintaining independence in the community and ADLs encompass more basic functions required to maintain independence in the home. In older patients with cancer, independence in IADLs has been associated with improved treatment tolerance and improved survival.22-24, 34 In addition to ADL and IADL scales, other screening tests (discussed below) have also been used to determine the functional status in elderly cancer patients.
A quick screening test to assess mobility is the “timed up and go” (TUG) test. Older individuals are asked to get up from an armchair without using their arms, walk 10 feet forward at their usual pace, turn around, walk back to the chair, and then sit down again. This tool can be utilized to assess overall motor function and the score has been predictive of the risk of falls in older adults.
Lachs and colleagues developed a screening tool consisting of vision, hearing, arm/leg mobility, urinary incontinence, nutrition and mental status, and depression, disabilities in the activities of daily living (ADL), instrumental activities of daily living (IADL), home environment, and social support. Lachs’ screening test is done by a physician (or office staff); it may be very useful to assess if a CGA is necessary.35
Saliba and colleagues have developed a useful questionnaire called the Vulnerable Elders Survey (VES-13) that can predict the probability of death and functional decline in older patients.36,37 A score of 3 or more on the VES-13 indicates that patients are vulnerable. Patients can quickly fill out this survey at home or in the office. Saliba and colleagues tested the questionnaire in 6205 Medicare beneficiaries aged 65 years and older.36 The VES-13 assesses whether elderly patients are at risk for functional decline or death. The advantage of this questionnaire is that it minimizes the amount of time required to examine patients in the office; this survey assesses age, self-rated health, limitation in physical function, and functional disabilities. Recently, Luciani and colleagues have reported that the VES-13 is highly predictive of impaired functional status and can be considered as a useful preliminary means of assessing older patients with cancer before undertaking a full CGA.38
In the future, laboratory tests may be used to assess which elderly patients are at increased risk for functional decline or mortality. Cohen and colleagues have demonstrated that high levels interleukin-6 and D-dimer were associated with mortality and functional dependence in home dwelling individuals aged 71 years and older.39 Higher levels interleukin-6 and C-reactive protein have been associated with slower walking speed and poor grip strength in adults older than 70 years.40 In addition, cognitive decline has been found to be associated with elevated levels of D-dimer.41 Thus, assessment of markers of
Printed by Kelly Hayden on 10/12/2012 3:09:21 PM. For personal use only. Not approved for distribution. Copyright © 2012 National Comprehensive Cancer Network, Inc., All Rights Reserved.

Version 2.2012, 11/15/11 © National Comprehensive Cancer Network, Inc. 2011, All rights reserved. The NCCN Guidelines® and this illustration may not be reproduced in any form without the express written permission of NCCN®. MS-4
NCCN Guidelines IndexSenior Adult Oncology TOC
Discussion
NCCN Guidelines Version 2.2012 Senior Adult Oncolo gy
inflammation and coagulation (such as interleukin-6 and D-dimer) may be used to predict the physiologic age of elderly patients.
Comorbidities
Older adults have an increased prevalence of comorbidities which can impact cancer prognosis and treatment tolerance.42,43 Cardiovascular problems including congestive heart failure (CHF), diabetes, renal insufficiency, dementia, depression, anemia and osteoporosis are some frequently encountered comorbid conditions in elderly cancer patients.
Specific comorbidities have been shown to have an impact on prognosis and treatment outcome in patients with cancer.44,45, 46 For example, in a series of 5077 men (median age, 69.5 years) with localized or locally advanced prostate cancer, neoadjuvant hormonal therapy was significantly associated with an increased risk of all-cause mortality (26.3% vs. 11.2%) among men with a history of coronary artery disease, CHF or myocardial infarction after a median follow-up of 5.1 years.44 In a randomized adjuvant chemotherapy trial of 3,759 patients with high-risk stage II and stage III colon cancer, patients with diabetes mellitus experienced a significantly higher rate of overall mortality and cancer recurrence. At 5 years, the disease-free survival (48% vs. 59%), overall survival (57% vs. 66%) and recurrence-free survival (56% vs 64%) were significantly worse for patients with diabetes compared with patients without diabetes.45 In the Surveillance, Epidemiology, and End Results (SEER)-Medicare database analysis of elderly patients (66 years or older) diagnosed with stages I-III breast cancer, those with diabetes had increased rate of hospitalizations for any chemotherapy toxicity and higher all-cause mortality.46 In elderly cancer patients with comorbidities, the interaction of cancer treatment with comorbidity may impact functional status, or worsen the comorbidity. Cancer treatment may be too risky due to the type and severity of comorbidity and finally cancer or cancer treatment
may not have any impact on life expectancy due to the risk of morbidity or mortality associated with the comorbid condition. The effect of comorbidity on life expectancy should be evaluated prior to initiation of treatment.
The guidelines recommend that the number and severity of comorbidities should be assessed. The adult comorbidity evaluation-27 (ACE-27) index,47 the Charlson Comorbidity Index (CCI),48 the Cumulative Illness Rating Scale (CIRS)49 and the OARS Multidimensional Functional Assessment Questionnaire50 are the commonly used indices to determine the risk of mortality associated with comorbidity in elderly patients. ACE-27,51, 52 CCI53-55 and CIRS56, 57 have also been used to determine treatment tolerance in elderly cancer patients. In a study of 310 elderly patients (70 or older) with head and neck cancer, comorbidity as measured by the ACE-27 index was an indicator of overall survival.58 In a randomized trial that compared vinorelbine alone or in combination with gemcitabine in elderly patients with locally advanced NSCLC, a CCI of greater than 2 was associated with a higher risk of early treatment suspension (82% vs. 30% respectively).53 In a phase III trial comparing platinum-doublet therapy as first-line treatment in patients with stage IIIB or IV NSCLC, patients with severe comorbidities (as measured by CIRS) benefited from and tolerated platinum-doublet chemotherapy as well as patients with no comorbidities.56 However, the former group had a higher risk of neutropenic fever and death from neutropenic infections.
Polypharmacy
Polypharmacy can be defined in various ways, including the use of increased no. of medications (5 or more), more than is clinically indicated; the use of potentially inappropriate medications; medication underuse and medication duplication.59, 60 Although polypharmacy can be an issue across all age groups, it can be a more serious problem in
Printed by Kelly Hayden on 10/12/2012 3:09:21 PM. For personal use only. Not approved for distribution. Copyright © 2012 National Comprehensive Cancer Network, Inc., All Rights Reserved.
Version 2.2012, 11/15/11 © National Comprehensive Cancer Network, Inc. 2011, All rights reserved. The NCCN Guidelines® and this illustration may not be reproduced in any form without the express written permission of NCCN®. MS-5
NCCN Guidelines IndexSenior Adult Oncology TOC
Discussion
NCCN Guidelines Version 2.2012 Senior Adult Oncolo gy
elderly patients due to the presence of increased comorbid conditions treated with one or more drugs. In this patient population, the use of drugs for the management of cancer-related symptoms or side effects can result in polypharmacy.61-63
The use of multiple medications can lead to increased incidences of adverse drug reactions (which can lead to functional decline and geriatric syndromes), drug-drug interactions and non-adherence.59,64, 65 Among cancer patients receiving systemic anticancer therapy for solid tumors, one or more drug-drug interactions were observed in 27% of patients which increased to 31% among cancer patients receiving palliative care only.65, 66 Older patients, those with comorbid conditions, brain tumor patients, and those taking many medications are at greater risk of drug interactions.66
Alterations in pharmacokinetics and pharmacodynamics of drug metabolism in elderly population can also contribute to adverse drug interactions.59 Most of the commonly prescribed medications such as opioids, antidepressants, antibiotics, and antipsychotics as well as anticancer drugs induce or inhibit cytochrome P-450 enzymes. In a retrospective analysis, Popa et al assessed the impact of polypharmacy on toxicity from chemotherapy in 290 elderly patients (70 or older).67 The results of this study demonstrated that cytochrome P-450 inhibition may contribute to non-hematologic toxicities whereas hematological toxicities may be associated with protein binding interactions. The role of protein binding and cytochrome P-450 inhibition should be further explored.
The use of one or more potentially inappropriate medications among elderly patients has also been documented in several studies.68-70 In one study, the use of inappropriate medications increased from 29% to 48% among cancer patients in the palliative care setting.69 In a more
recent study of 500 elderly cancer patients (65 or older) starting a new chemotherapy regimen, polypharmacy (5 or more drugs) was observed in 48% of patients and the use of potentially inappropriate medications was seen in 11-18%.70 While polypharmacy did not increase the risk of chemotherapy-related toxicity in this cohort, it was associated with a higher frequency of hospitalization and early discontinuation of chemotherapy.70
Evaluation of polypharmacy
The guidelines recommend medication review for duplication and appropriate use should be done at every visit. Beers criteria and Medication appropriateness index (MAI) are two of the most common approaches used to evaluate potentially inappropriate medication use in older patients. The screening tool of older persons’ prescriptions (STOPP) and the screening tool to alert doctors to right treatment (START) criteria have been recently developed to evaluate drug interactions, medication duplication and medication underuse.
Beers criteria The Beers' Criteria identifies inappropriate medications that have potential risks that outweigh potential benefits based on the risk of toxicity and the presence of potential drug-disease interaction in elderly cancer patients.71, 72 The criteria are appropriate for persons older than 65 years of age and provide a rating of severity for adverse outcomes as well as a descriptive summary of the prescribing information associated with the medication. The updated 2003 Beers criteria have been used to evaluate polypharmacy in older patients with cancer both in an oncology-specific acute care unit [oncology-acute care for elders (OACE); n = 47 with a median age 73.5 years] and in the outpatient setting (n = 154 with a median age 74 years).73, 74 The Beers criteria based polypharmacy was observed in 21% and 11% of patients respectively. Both of these studies had included medication review and
Printed by Kelly Hayden on 10/12/2012 3:09:21 PM. For personal use only. Not approved for distribution. Copyright © 2012 National Comprehensive Cancer Network, Inc., All Rights Reserved.

Version 2.2012, 11/15/11 © National Comprehensive Cancer Network, Inc. 2011, All rights reserved. The NCCN Guidelines® and this illustration may not be reproduced in any form without the express written permission of NCCN®. MS-6
NCCN Guidelines IndexSenior Adult Oncology TOC
Discussion
NCCN Guidelines Version 2.2012 Senior Adult Oncolo gy
pharmacist-based interventions improve the appropriateness of prescribing. In OACE study, 53% had a subsequent alteration in their medication regimen and 28% had a potentially inappropriate medication discontinued.73 In the outpatient study, 50% of patients required specific interventions following geriatric management evaluation.74
Medication appropriateness index MAI was developed to measure appropriate prescribing based on a 10-item list and a 3-point rating scale.75 Samsa and colleagues subsequently modified the MAI to include a single summated MAI score per medication which demonstrated acceptable reliability in assessing medication appropriateness among 1644 medications prescribed to 208 elderly veterans from the same clinic.76 This modified MAI appears to be a valid and relatively reliable measure to detect medication appropriateness and inappropriateness in the community pharmacy setting as well as in ambulatory elderly patients on multiple medications.77, 78 MAI scores were significantly lower for medications with a high potential for adverse effects compared with those with a low potential (1.8 vs. 2.9).77 Higher MAI scores were also associated with lower self-related health scores in older adults.79 MAI has not been evaluated extensively in elderly cancer patients.
STOPP/START criteria STOPP /START criteria were established by a Delphi consensus process in which 18 experts in geriatric pharmacotherapy from Ireland and the United Kingdom.80 The STOPP criteria is comprised of 65 indicators for potentially inappropriate prescribing including drug–drug and drug-disease interactions, therapeutic duplication and drugs that increase the risks of geriatric syndromes whereas the START criteria incorporate 22 evidence-based indicators to identify prescribing omissions in older people.81,82 In a randomized trial of 400 hospitalized patients (65 or older), unnecessary polypharmacy, the use of drugs at
incorrect doses, and potential drug-drug and drug-disease interactions were significantly lower in the group assigned to screening with STOPP/START criteria with recommendations provided to their attending physicians compared to control group assigned to routine pharmaceutical care.83 Significant improvements in prescribing appropriateness were sustained for 6 months after discharge.
Nutritional Status
Nutritional deficiency or malnutrition is a common and serious condition in older patients. While some of the malnutrition is attributed to the underlying illness, in most of the patients it is due to inadequate intake of calories. Mini-Nutritional Assessment (MNA) has been designed and validated to provide a single, rapid assessment of nutritional status in elderly patients in the outpatient settings.84, 85 MNA is composed of simple measurements and brief questions that help to identify people at risk for malnutrition before severe changes in weight or albumin levels occur. Rubenstein et al have developed a shortened version of MNA which also has good diagnostic accuracy.86 Special attention should also be devoted to the deficiency of Vitamin D since that may be related to osteoporosis and fractures.87
Cognitive Function
Geriatric patients with cancer who are cognitively impaired have an increased risk of functional dependence, higher incidence of depression, and are at greater risk for death. Cognitive function was also predictive of medication adherence across diagnoses, regardless of the complexity of regimen.88 In addition, the association between cognitive impairment and the ability to weigh the risks and benefits of cancer treatment decisions needs to be considered. Cognitively impaired patients should be cared for by an experienced multidisciplinary geriatric oncology team along with good supportive
Printed by Kelly Hayden on 10/12/2012 3:09:21 PM. For personal use only. Not approved for distribution. Copyright © 2012 National Comprehensive Cancer Network, Inc., All Rights Reserved.
Version 2.2012, 11/15/11 © National Comprehensive Cancer Network, Inc. 2011, All rights reserved. The NCCN Guidelines® and this illustration may not be reproduced in any form without the express written permission of NCCN®. MS-7
NCCN Guidelines IndexSenior Adult Oncology TOC
Discussion
NCCN Guidelines Version 2.2012 Senior Adult Oncolo gy
care throughout the treatment.89 Anticholinergics, antipsychotics, benzodiazepines, corticosteroids and opioids can be associated with cognitive impairment in older adults.90 Special considerations for over or under-use, duration of therapy and dosage should be in place with the use of these classes of medications. Hilmer and colleagues have developed a drug burden index which is a useful evidence-based tool for assessing the effect of medications on the physical and cognitive performance in elderly people.91
Dementia and delirium are two of the most common causes for cognitive impairment.92 See the section on Geriatric Syndromes for the assessment of dementia and delirium in older cancer patients.
Socioeconomic Issues
Social ties have been identified as significant predictors of mortality in older adults.93, 94 In a study of 2,835 women diagnosed with breast cancer, socially isolated women had an elevated risk of mortality after a diagnosis of breast cancer.95 An evaluation of social support is an integral part of geriatric assessment. The patient’s treatment goals should be discussed with them. In addition, the patient’s living conditions, presence and adequacy of care giver and financial status should also be taken into consideration. Consultation with a social worker should be encouraged. Consultation with a financial expert to discuss the cost and coverage options of treatment would also be beneficial.
Geriatric Syndromes
Dementia, delirium, depression, distress, osteoporosis, falls, fatigue and frailty are some of the most common syndromes in elderly cancer patients.96 Elderly patients with cancer experience a high prevalence of geriatric syndromes than those without cancer. In analysis of a national sample of 12,480 community-based elders, 60.3% of patients with
cancer reported one or more geriatric syndromes compared with 53.2% of those without cancer.97 In this cohort, the prevalence of hearing trouble, urinary incontinence, falls, depression, and osteoporosis were significantly higher in patients with cancer than those without cancer.
Dementia
Dementia is a permanent cognitive impairment and is often present in elderly patients as a comorbid condition. In a SEER database analysis, elderly patients with colon cancer (67 years or older) and dementia were less likely to receive invasive diagnostic methods or therapies with curative intent.98 Preexisting dementia was also associated with high mortality, mostly from noncancer causes in patients 68 years or older diagnosed with breast, colon, or prostate cancer.99
Blessed orientation-memory-concentration test (BOMC), Mini-mental state examination (MMSE) or the Montreal cognitive assessment (MoCA) can be used to screen for cognitive impairment in older adults.100-103 BOMC is a 6-item derivative of the blessed information-memory-concentration test.102 MMSE is an 11-item screening test which quantitatively assesses the severity of cognitive impairment and documents cognitive changes occurring over a period of time.100, 101 However, MMSE is not adequate for mild cognitive impairment and does not predict future decline. MoCA is a brief screening tool with high sensitivity and specificity for detecting mild cognitive impairment in patients performing in the normal range on the MMSE.103 MoCA has been shown to be a superior prognostic indicator than the MMSE in patients with brain metastases.104, 105 In a feasibility study of MoCA in patients with brain metastases, cognitive impairment was detected in 80% of the patients by the MoCA compared with 30% by the MMSE.104 Among the 28 patients with a normal MMSE, 71% had cognitive impairment according to the MoCA.
Printed by Kelly Hayden on 10/12/2012 3:09:21 PM. For personal use only. Not approved for distribution. Copyright © 2012 National Comprehensive Cancer Network, Inc., All Rights Reserved.
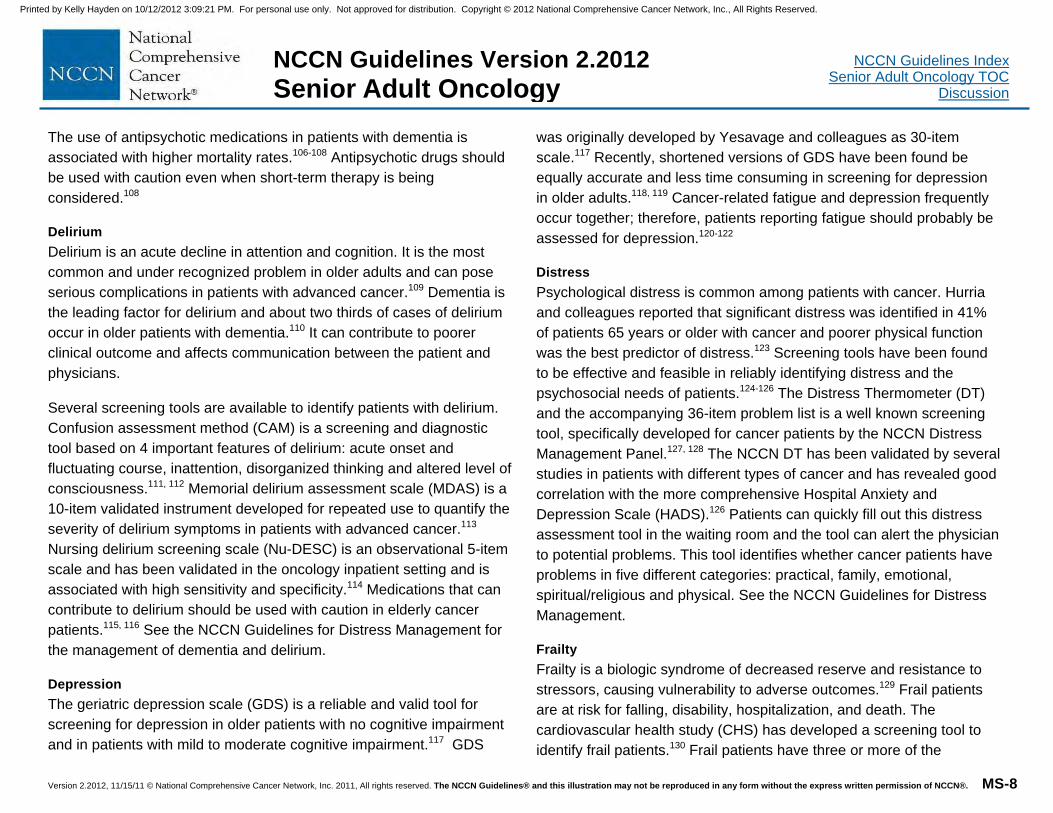
Version 2.2012, 11/15/11 © National Comprehensive Cancer Network, Inc. 2011, All rights reserved. The NCCN Guidelines® and this illustration may not be reproduced in any form without the express written permission of NCCN®. MS-8
NCCN Guidelines IndexSenior Adult Oncology TOC
Discussion
NCCN Guidelines Version 2.2012 Senior Adult Oncolo gy
The use of antipsychotic medications in patients with dementia is associated with higher mortality rates.106-108 Antipsychotic drugs should be used with caution even when short-term therapy is being considered.108
Delirium
Delirium is an acute decline in attention and cognition. It is the most common and under recognized problem in older adults and can pose serious complications in patients with advanced cancer.109 Dementia is the leading factor for delirium and about two thirds of cases of delirium occur in older patients with dementia.110 It can contribute to poorer clinical outcome and affects communication between the patient and physicians.
Several screening tools are available to identify patients with delirium. Confusion assessment method (CAM) is a screening and diagnostic tool based on 4 important features of delirium: acute onset and fluctuating course, inattention, disorganized thinking and altered level of consciousness.111, 112 Memorial delirium assessment scale (MDAS) is a 10-item validated instrument developed for repeated use to quantify the severity of delirium symptoms in patients with advanced cancer.113 Nursing delirium screening scale (Nu-DESC) is an observational 5-item scale and has been validated in the oncology inpatient setting and is associated with high sensitivity and specificity.114 Medications that can contribute to delirium should be used with caution in elderly cancer patients.115, 116 See the NCCN Guidelines for Distress Management for the management of dementia and delirium.
Depression
The geriatric depression scale (GDS) is a reliable and valid tool for screening for depression in older patients with no cognitive impairment and in patients with mild to moderate cognitive impairment.117 GDS
was originally developed by Yesavage and colleagues as 30-item scale.117 Recently, shortened versions of GDS have been found be equally accurate and less time consuming in screening for depression in older adults.118, 119 Cancer-related fatigue and depression frequently occur together; therefore, patients reporting fatigue should probably be assessed for depression.120-122
Distress
Psychological distress is common among patients with cancer. Hurria and colleagues reported that significant distress was identified in 41% of patients 65 years or older with cancer and poorer physical function was the best predictor of distress.123 Screening tools have been found to be effective and feasible in reliably identifying distress and the psychosocial needs of patients.124-126 The Distress Thermometer (DT) and the accompanying 36-item problem list is a well known screening tool, specifically developed for cancer patients by the NCCN Distress Management Panel.127, 128 The NCCN DT has been validated by several studies in patients with different types of cancer and has revealed good correlation with the more comprehensive Hospital Anxiety and Depression Scale (HADS).126 Patients can quickly fill out this distress assessment tool in the waiting room and the tool can alert the physician to potential problems. This tool identifies whether cancer patients have problems in five different categories: practical, family, emotional, spiritual/religious and physical. See the NCCN Guidelines for Distress Management.
Frailty
Frailty is a biologic syndrome of decreased reserve and resistance to stressors, causing vulnerability to adverse outcomes.129 Frail patients are at risk for falling, disability, hospitalization, and death. The cardiovascular health study (CHS) has developed a screening tool to identify frail patients.130 Frail patients have three or more of the
Printed by Kelly Hayden on 10/12/2012 3:09:21 PM. For personal use only. Not approved for distribution. Copyright © 2012 National Comprehensive Cancer Network, Inc., All Rights Reserved.

Version 2.2012, 11/15/11 © National Comprehensive Cancer Network, Inc. 2011, All rights reserved. The NCCN Guidelines® and this illustration may not be reproduced in any form without the express written permission of NCCN®. MS-9
NCCN Guidelines IndexSenior Adult Oncology TOC
Discussion
NCCN Guidelines Version 2.2012 Senior Adult Oncolo gy
following criteria: unintentional weight loss (10 pounds or more in past year), self-reported exhaustion, weakness (grip strength), slow walking speed, and/or low physical activity.130 Fit, frail, and prefrail patients had different 5-year mortality rates and different risks of developing functional dependence at 3 and 7 years. The CHS screening tool has been tested in 5317 men and women who were 65 years and older.
Fatigue
Cancer-related fatigue is a persistent, subjective sense of tiredness related to cancer or cancer treatment that interferes with usual functioning. In advanced cancer, the prevalence of fatigue is greater than 50-70%.131 In a study that evaluated the prevalence of common symptoms in patients with advanced cancer, fatigue was independently associated with chemotherapy, hemoglobin level and other symptoms such as pain and depression.132 Patients perceive fatigue to be one of the most distressing symptoms associated with cancer and its treatment; fatigue is more distressing than pain or nausea and vomiting.133, 134 In contrast to normal fatigue, cancer-related fatigue is refractory to sleep and rest, perhaps because cancer patients have aberrant sleep patterns. It is reasonable to expect that fatigue may precipitate functional dependence, especially in patients who are already dependent in IADL.135-137
Multiple factors can contribute to fatigue, including pain, emotional distress, anemia, comorbidities, and/or sleep disturbance; many of them are treatable. Certainly, the best strategy is avoidance of any fatigue that may precipitate functional dependence in older individuals. Energy conservation, exercise programs, stress management, sleep therapy, and psychostimulants are some of the interventions that have proved valuable. Screening for fatigue can be done using a brief screening questionnaire: “Since your last visit, how would you rate your
worst fatigue on a scale of 0 to 10 (0 = no fatigue and 10 = worst fatigue)?” See the NCCN Guidelines for Cancer-Related Fatigue.
Falls
Falls are one of most common geriatric syndromes. Risk factors include older age, muscle weakness and impairments in gait, balance, vision, cognition and activities of daily living.138 In a prospective study of incidences of falls in patients with advanced cancer, 52% of patients fell during follow-up of up to 6 months, regardless of age. The median time to fall was 85 days and 80 days respectively, for those aged younger than 65 and 65 years or older.139 Evidence from a meta-analysis of randomized trials and a systematic review identified interventions (multifactorial falls risk assessment and management, exercise, environmental modifications, and education) that are very effective in preventing falls in older adults and they also reduce both the risk and rate of falling.140 Multifactorial risk assessment and management was the most effective intervention for both the risk of falling and monthly rate of falls. Exercise programs were effective in reducing the risk of falling but did not have a beneficial effect in reducing the monthly fall rate.140
The American Geriatrics Society/British Geriatrics Society Clinical Practice Guideline for Prevention of Falls in Older Persons recommend a multifactorial risk assessment followed by multicomponent interventions to address the identified risks and prevent falls in elderly patients 75 years or older with two or more falls in the past 12 months or difficulty with walking or balance or gait difficulties.141 Recommended interventions include minimizing the number of medications; providing tailored exercise program to improve strength, balance, gait, and coordination; treating vision impairment (including cataracts); management of postural hypotension, heart rate and rhythm abnormalities as well as foot and footwear problems; supplement with
Printed by Kelly Hayden on 10/12/2012 3:09:21 PM. For personal use only. Not approved for distribution. Copyright © 2012 National Comprehensive Cancer Network, Inc., All Rights Reserved.

Version 2.2012, 11/15/11 © National Comprehensive Cancer Network, Inc. 2011, All rights reserved. The NCCN Guidelines® and this illustration may not be reproduced in any form without the express written permission of NCCN®. MS-10
NCCN Guidelines IndexSenior Adult Oncology TOC
Discussion
NCCN Guidelines Version 2.2012 Senior Adult Oncolo gy
vitamin D; modifying the home environment and providing education and necessary information.141
Osteoporosis
Osteoporosis and its associated increase in fracture is a major risk factor in cancer patients especially in women receiving chemotherapy or hormonal therapy for breast cancer and in men receiving hormonal therapy for prostate cancer. Osteoporosis can be prevented with appropriate screening, lifestyle interventions and therapy. The diagnosis of osteoporosis is based on assessment of bone density by dual energy x-ray absorptiometry (DEXA) scan. Management of bone health has become an integral part of comprehensive cancer care. Elderly patients should be made aware of the impact of cancer therapies on bone health and should adhere to treatment recommendations for maintaining bone health.142 The NCCN Task force report on Bone Health in Cancer Care discusses effective screening and therapeutic options for the management of treatment-related bone loss.143
Approach to Decision Making in Older Cancer Patients The risk of morbidity from cancer is generally established by the stage at diagnosis, the aggressiveness of the tumor and risk of recurrence and progression. Following initial screening and CGA, patients with a low risk of dying or suffering from cancer during their lifetime, can receive symptom management and supportive care as detailed in the appropriate NCCN Guidelines for Supportive Care. Patients in the moderate or high risk group can be further evaluated to asses their functional dependency, decision-making capacity, overall goals and desire for proposed treatment.144, 145
Irrespective of age, a person who is functionally independent and without serious comorbidities should be a good candidate for most
forms of cancer treatment. Functionally independent patients with contraindications to treatment and patients with major functional impairment with or without complex comorbidity should be managed according to the appropriate NCCN Guidelines for Supportive Care. Patients who are dependent in some IADLs, with or without severe comorbidities are at increased risk of treatment complications. For these patients with intermediate functional impairment who have milder problems (such as dependence in one or more IADL, milder comorbidity, depression, minor memory disorder, mild dementia, inadequate caregiver), treatment may still be administered with special individualized precautions, including attempts to reverse the problem and cautious dosing of treatment.146, 147 In patients without decision-making capacity, the guidelines recommend considering consultation from ethics committee.
The benefits of cancer treatment include prolonged survival, maintenance and improvement of quality of life and function, as well as palliation of symptoms. For patients who are able to tolerate curative treatment, options include surgery, radiation therapy (RT), chemotherapy and targeted therapies. Symptom management and supportive care as detailed in the appropriate NCCN Guidelines for Supportive Care is recommended for all patients.
Surgery
In general, age is not a primary consideration for surgical risk, although the physiologic status of the patient needs to be assessed. Performance status and comorbidities of the patient are more important factors than the age when considering surgical treatment options for older adults.148 Special efforts should be made to prevent or avoid emergency surgery since it carries increased risk of complications. Following surgery, physical and/or occupational therapy should be
Printed by Kelly Hayden on 10/12/2012 3:09:21 PM. For personal use only. Not approved for distribution. Copyright © 2012 National Comprehensive Cancer Network, Inc., All Rights Reserved.

Version 2.2012, 11/15/11 © National Comprehensive Cancer Network, Inc. 2011, All rights reserved. The NCCN Guidelines® and this illustration may not be reproduced in any form without the express written permission of NCCN®. MS-11
NCCN Guidelines IndexSenior Adult Oncology TOC
Discussion
NCCN Guidelines Version 2.2012 Senior Adult Oncolo gy
considered to expedite the patient’s return to their preoperative functional level.
The Surgical Task Force report from SIOG (International Society for Geriatric Oncology) reported that in many malignancies (breast, gastric and liver) the surgical outcomes in older patients with cancer were not significantly different from their younger counterparts.149 Preoperative Assessment of Cancer in Elderly (PACE) was developed to determine the suitability of older patients for surgical intervention.150 PACE incorporates CGA, brief fatigue inventory (BFI), performance status (PS) and American Society Anesthesiologists (ASA) grade. In an international prospective study 460 consecutive older patients completed PACE prior to surgery.151, 152 In a multivariate analysis, moderate to severe fatigue, a dependent IADL and an abnormal PS were identified as the most important independent predictors of post-surgical complications. Disability assessed by ADL, IADL and PS were associated with an extended hospital stay. This study demonstrated that PACE is a useful tool which will enable the physicians in evaluating the fitness of older patients with cancer for surgery. The reliability of this tool has to be confirmed in large prospective trials as applied to specific cancer types in elderly patients.
Radiation Therapy
RT (external beam RT or brachytherapy) can be offered either in the curative or in the palliative setting.153 Hypofractionated RT may be an alternative treatment option in patients who are unable to tolerate conventional dose RT.154 Available data from the literature indicate that radiation therapy is highly effective, well tolerated and age is not a limiting factor in elderly cancer patients.155-157 Concurrent chemoradiation, however, should be used with extreme caution; dose modification of chemotherapy may be necessary to reduce toxic side
effects. Nutritional support and pain control for RT-included mucositis are recommended for patients received RT.
Chemotherapy
Several retrospective studies have reported that the toxicity of chemotherapy is not more severe or prolonged in persons older than 70 years.158-162 However, the results of these studies cannot be generalized for the following reasons:
Only a few patients were 80 years or older; therefore, minimal information is available on the oldest patients.
The older patients involved in these studies were highly selected by the eligibility criteria of the cooperative group protocols and were not representative of the general older population, because they were probably healthier than most older patients.
Many of the treatment regimens used in these trials had lower dose intensity than those in current use.
Nevertheless, these studies are important, because they demonstrate that age, by itself, is not a contraindication to cancer chemotherapy. Therefore, patient selection is extremely important to maximize the benefits of adjuvant chemotherapy in older patients with breast, non-small cell lung and colon cancer.
Tolerance to Chemotherapy
Age has been associated with pharmacokinetic and pharmacodynamic changes and with increased susceptibility of normal tissues to toxic complications. In general, all of these changes increase the risks of chemotherapy.163,164 Pharmacodynamic changes of interest include reduced repair of DNA damage and increased risk of toxicity. Pharmacokinetic changes of major concern include decrease in the glomerular filtration rate (GFR) and volume of distribution of
Printed by Kelly Hayden on 10/12/2012 3:09:21 PM. For personal use only. Not approved for distribution. Copyright © 2012 National Comprehensive Cancer Network, Inc., All Rights Reserved.
Version 2.2012, 11/15/11 © National Comprehensive Cancer Network, Inc. 2011, All rights reserved. The NCCN Guidelines® and this illustration may not be reproduced in any form without the express written permission of NCCN®. MS-12
NCCN Guidelines IndexSenior Adult Oncology TOC
Discussion
NCCN Guidelines Version 2.2012 Senior Adult Oncolo gy
hydrosoluble drugs. Although the hepatic uptake of drugs and the activity of cytochrome P450 enzymes also decrease with age, the influence of these changes on cancer chemotherapy is not clear. Intestinal absorption may decrease with age, but it does not appear to affect the bioavailability of anticancer agents. The pharmacokinetics of antineoplastic drugs is unpredictable to some extent; thus, drug doses should be adjusted according to the degree of toxicity that develops. However, adequate dosing is necessary to ensure the effectiveness of therapy.
Extermann and colleagues have devised the MAX2 index for estimating the average per patient risk for toxicity from chemotherapy.165 In a retrospective analysis, Shayne et al identified advanced age (65 or older), greater body surface area, comorbidities, anthracycline-based regimens, a 28-day schedule and febrile neutropenia as independent predictors of reduced dose intensity among patients with early stage breast cancer receiving adjuvant chemotherapy.166 In another retrospective analysis of elderly patients (65 or older) with invasive breast cancer, the type of adjuvant chemotherapy regimen was a better predictor of toxicity than increased age or comorbidity score.54 Anthracycline-based regimen resulted in greater grade 3 or 4 toxicity, hospitalization and/or febrile neutropenia whereas treatment delays due to myelosuppression were more frequent with cyclophosphamide containing regimen. Among elderly patients with ovarian cancer, those receiving standard dose chemotherapy were more likely to experience cumulative toxicity and delays in therapy.55
Other investigators have developed tools incorporating components of CGA to assess the individual risk of severe toxicity from chemotherapy in older patients.34, 167, 168 Extermann et al have developed the chemotherapy risk assessment scale for high-age patients (CRASH) score which could be useful in predicting significant differences in the
risk of severe toxicity in older cancer patients starting a new chemotherapy.167 In this model, diastolic blood pressure, IADL, lactate dehydrogenase, and the type of therapy were the best predictors of hematologic toxicity whereas performance status, cognitive function, nutritional status, and the type of therapy were the best predictors of non-hematological toxicity. Hurria and colleagues have developed a scoring algorithm for predicting chemotherapy toxicity in older adults with cancer.168 The following factors were predictive of grade 3 to 5 chemotherapy toxicity: (1) age 72 or older, (2) cancer type (gastrointestinal or genitourinary), (3) standard dosing of chemotherapy, (4) polychemotherapy, (5) hemoglobin (male: less than 11g/dL, female: less than 10g/dL), (6) creatinine clearance less than 34 ml/min (Jelliffe formula using ideal weight),169 (7) hearing impairment described as fair or worse, (8) one or more falls in last 6 months, (9) limited in walking one block, (10) the need for assistance with taking medications, and (11) decreased social activities due to physical or emotional health.168
Adherence to therapy
Adherence to the prescribed regimen, especially oral therapy is essential to derive maximal clinical benefit. Older adults are at increased risk for poor adherence to oral therapy for a variety of reasons including cognitive impairment, comorbid conditions and polypharmacy, higher risk of side- effects due to drug interactions, limited insurance coverage, social isolation and inadequate social support.170 Several studies have evaluated the adherence to adjuvant therapy in older patients with estrogen-receptor-positive breast cancer.171-174 In one study, the discontinuation rate was 49% before the completion of 5 years, with women aged 75 years or older with an increase in the number of cardiopulmonary comorbidities at 3 years as well as those who had received breast-conserving surgery without RT
Printed by Kelly Hayden on 10/12/2012 3:09:21 PM. For personal use only. Not approved for distribution. Copyright © 2012 National Comprehensive Cancer Network, Inc., All Rights Reserved.

Version 2.2012, 11/15/11 © National Comprehensive Cancer Network, Inc. 2011, All rights reserved. The NCCN Guidelines® and this illustration may not be reproduced in any form without the express written permission of NCCN®. MS-13
NCCN Guidelines IndexSenior Adult Oncology TOC
Discussion
NCCN Guidelines Version 2.2012 Senior Adult Oncolo gy
being at higher risk of discontinuation.173 In a cohort of 161 elderly women receiving oral adjuvant chemotherapy with capecitabine for breast cancer (CALGB 49907 study), 25% of the patients took fewer than 80% of the planned doses.174 Non-adherence was more likely among women with node-negative disease and mastectomy. Although nonadherence was not associated with shorter relapse-free survival in this study (may be due to limited sample size), Hershman et al recently reported that early discontinuation and non-adherence to adjuvant hormonal therapy are associated with increased mortality in women with breast cancer.175 Therefore, interventions designed to educate older patients about the benefits and risks of oral therapy may help to reduce non-adherence.
Side Effects of Chemotherapy
In older patients undergoing chemotherapy, the most common complications include myelosuppression resulting in neutropenia, anemia or thrombocytopenia, mucositis, renal toxicity, cardiac toxicity and neurotoxicity. Older patients appear to be at special risk for severe and prolonged myelosuppression and mucositis, increased risk of cardiomyopathy, as well as increased risk of central and peripheral neuropathy. In addition, they are also at risk for infection (with or without neutropenia), dehydration, electrolyte disorders, and malnutrition either as a side effect of the chemotherapy or directly from the tumor. Chemotherapy can also affect cognition, function, balance, vision, hearing, continence, and mood.92 The combination of these complications enhances the risk of delirium and functional dependence. It is essential to detect and correct these complications (that may interfere with treatment) in order to achieve maximum benefit from chemotherapy. Prevention and/or amelioration of some of the common chemotherapy-related complications are discussed below.
Cardiac Toxicity
Anthracyclines are associated with increased cardiac toxicity resulting in congestive heart failure (CHF). Other antineoplastic drugs may have additional effect on anthracycline-induced cardiac toxicity.176 Risk factors for anthracycline-induced cardiotoxicity include an existing or history of heart failure or cardiac dysfunction, hypertension, diabetes and coronary artery disease, older age (independent of comorbidities and performance status), prior treatment with anthracyclines, higher cumulative doses and short infusion duration.177, 178
Trastuzumab has also been associated with cardiac dysfunction and CHF in patients with metastatic breast cancer.179 Other trials including NSABP-31 study 180 and NCCTG N9831 study181 which evaluated trastuzumab in combination with doxorubicin and cyclophosphamide followed by paclitaxel in patients with HER-2-positive breast cancer, older age (50 years or more), lower left ventricular ejection fraction (LVEF) and the use antihypertensive medications were identified as risk factors for cardiac dysfunction in patients receiving trastuzumab. However, in the long-term follow-up of the HERA trial the incidence of severe CHF, left ventricular dysfunction and discontinuation of trastuzumab as a result of cardiac disorders remained low (0.8%, 9.8% and 5.1% respectively) in patients who received trastuzumab.182 A combined review of cardiac data from the NSABP-31 and NCCTG N9831 clinical trials also showed that the incidence of symptomatic heart failure events was 2.0% in patients treated with adjuvant trastuzumab and the majority of these patients recovered with appropriate treatment.183
In a recently published single center retrospective analysis of elderly patients (70 years or older; n = 45) with breast cancer, Serrano et al. reported an increased incidence of cardiotoxicity among patients with a history of cardiac disease and/or diabetes treated with trastuzumab.184
Printed by Kelly Hayden on 10/12/2012 3:09:21 PM. For personal use only. Not approved for distribution. Copyright © 2012 National Comprehensive Cancer Network, Inc., All Rights Reserved.
Version 2.2012, 11/15/11 © National Comprehensive Cancer Network, Inc. 2011, All rights reserved. The NCCN Guidelines® and this illustration may not be reproduced in any form without the express written permission of NCCN®. MS-14
NCCN Guidelines IndexSenior Adult Oncology TOC
Discussion
NCCN Guidelines Version 2.2012 Senior Adult Oncolo gy
Asymptomatic cardiotoxicity was observed in 12.5% of patients with early stage breast cancer and 24% of those with advanced breast cancer and 8.9% of all patients with advanced breast cancer, developed symptomatic CHF.
Emerging data from clinical studies (BCIRG 006 and BCIRG 007) suggest that trastuzumab when used in combination with non-anthracycline-based chemotherapy has similar efficacy with lower rates of cardiac events in patients with early stage as well as metastatic HER2-positive breast cancer.185, 186 However, median age of all patients in both these trials is 50-52 years. Additional data regarding the tolerability of these regimens in older adults is needed.
In patients 65 or older with both HER2-positive and HER2-negative early stage breast cancer, the US Oncology Research Trial 9735 demonstrated that non-anthracycline-based adjuvant chemotherapy with docetaxel and cyclophosphamide was associated with a disease-free and overall survival benefit compared to doxorubicin plus cyclophosphamide.187 In this study, 160 of the 1,016 enrolled patients (16%) were 65 years or older.
Dexrazoxane, an iron chelator has been shown to reduce anthracycline-induced cardiac toxicity in randomized clinical trials involving patients with advanced or metastatic breast cancer.188-190
Renal Toxicity
The GFR decreases with age, which in turn delays elimination of many drugs. Delayed renal excretion may enhance the toxicity of drugs whose parent compounds are excreted by the kidneys (carboplatin, oxaliplatin, methotrexate, bleomycin) and drugs that are converted to active (idarubicin, daunorubicin) or toxic metabolites (high-dose
cytarabine).11 Dose adjustment to the measured GFR should be considered for these drugs to decrease systemic toxicity.
Renal insufficiency is common in elderly cancer patients, particularly in patients receiving nephrotoxic drugs, patients with genitourinary cancers or multiple myeloma. In patients with preexisting renal problems who are at a greater risk of renal impairment, the use of nephrotoxic drugs should be limited or avoided. The International Association of Geriatric Oncology (SIOG) Task Force provides a number of recommendations for the clinical management of older adults with cancer with renal insufficiency.191 Dose adjustments and calculation of creatinine clearance to assess renal function is recommended for all patients.
Neurotoxicity
Neurotoxicity is also a dose-limiting toxicity associated with chemotherapy.192 Vinca alkaloids, cisplatin and taxanes induce peripheral neurotoxicity. Methotrexate, cytarabine and ifosfamide are associated with central neurotoxic side effect. Purine analogs (eg. fludarabine, cladribine and pentostatin) are associated with life-threatening neurotoxicity at significantly higher doses than the recommended clinical dose.193 High dose cytarabine can cause an acute cerebellar syndrome. Patient’s age (greater than 60 years), drug dose and schedule, renal and hepatic dysfunction are the most important risk factors for cytarabine-induced cerebellar toxicity.194, 195
Management of neurotoxicity mainly consists of dose reductions or lower dose intensities. Older patients are particularly susceptible to the toxicity of cytarabine-based regimens due to decreased renal excretion of the toxic metabolite ara-uridine, and increased vulnerability of the cerebellum. Particular attention should be paid to the use of cytarabine in high doses especially in patients with renal insufficiency. Dose
Printed by Kelly Hayden on 10/12/2012 3:09:21 PM. For personal use only. Not approved for distribution. Copyright © 2012 National Comprehensive Cancer Network, Inc., All Rights Reserved.

Version 2.2012, 11/15/11 © National Comprehensive Cancer Network, Inc. 2011, All rights reserved. The NCCN Guidelines® and this illustration may not be reproduced in any form without the express written permission of NCCN®. MS-15
NCCN Guidelines IndexSenior Adult Oncology TOC
Discussion
NCCN Guidelines Version 2.2012 Senior Adult Oncolo gy
reductions are necessary in patients with reduced GFR. The guidelines recommend monitoring for cerebellum function, hearing loss and peripheral neuropathy. Alternative regimens with non-neurotoxic drugs should be considered particularly in patients with significant hearing loss.
Myelosuppression
Available data from various studies has shown that the risk of myelosuppression increases substantially by age 65 years.196-201 The risk of myelosuppression is decreased by 50% when using growth factors.202-204 Dose reductions may compromise the effectiveness of treatment. The use of growth factors in these circumstances does not appear to be associated with increased cost and may even be cost saving if it prevents lengthy hospitalizations from neutropenic infections in older persons.
Neutropenia Neutropenia is the major dose-limiting toxicity associated with chemotherapy, especially in older patients. Several prospective studies of older patients with large cell lymphoma have shown that older age is a risk factor for neutropenic infections in patients treated with regimens like CHOP (cyclophosphamide, doxorubicin, vincristine and prednisone).204-210 In patients 60 years or older receiving induction or consolidation chemotherapy for acute myeloid leukemia (AML), the prophylactic use of hematopoietic growth factors results in faster recovery of neutrophil and shorter hospitalization, but it does not impact overall survival.211, 212
Meta-analysis of controlled clinical trials on the prophylactic use of recombinant granulocyte colony stimulating factors (G-CSF) has confirmed their effectiveness in reducing the risk of febrile neutropenia.213 Some concerns have been expressed that the
combination of growth factors and topoisomerase II inhibitors may be associated with increased risk of acute leukemia; however, these data are contoversial.214,215 Despite these caveats, the use of growth factors appears to be the best established strategy to improve treatment in this group of patients.216 The EORTC has issued similar recommendations for the prophylactic use of G-CSF in older patients with cancer.217 The NCCN Guidelines for Myeloid Growth Factors address the use of G-CSFs in patients with solid tumors and non-myeloid malignancies.
Anemia Anemia has been shown to be a risk factor for chemotherapy related toxicity and it is one of the factors responsible for reduction in volume of distribution, which may result in increased peak concentration and in increased toxicity of drugs.218 Anemia is also associated with cardiovascular disease, congestive heart failure, coronary death, and dementia.219-222
In patients with severe anemia, blood transfusions are necessary to prevent serious clinical consequences. There is increasing controversy regarding the use of erythropoietic stimulating agents (ESAs). ESAs have been demonstrated to decrease the need for transfusion in patients receiving chemotherapy.223 It also appears to be beneficial to complement the administration of erythropoietin with oral or parenteral iron although this is not specific for elderly patients. However, recent randomized studies have reported decreased survival and poorer tumor control among cancer patients receiving erythropoietic drugs for correction of anemia and target hemoglobin levels greater than 12 g/dL.224 The use of ESAs in patients with cancer is also associated with increased risks of venous thromboembolism (VTE) and mortality.225 The risks of shortened survival and the disease progression have not been excluded when ESAs are dosed to a target of hemoglobin levels of less than 12 g/dL.
Printed by Kelly Hayden on 10/12/2012 3:09:21 PM. For personal use only. Not approved for distribution. Copyright © 2012 National Comprehensive Cancer Network, Inc., All Rights Reserved.

Version 2.2012, 11/15/11 © National Comprehensive Cancer Network, Inc. 2011, All rights reserved. The NCCN Guidelines® and this illustration may not be reproduced in any form without the express written permission of NCCN®. MS-16
NCCN Guidelines IndexSenior Adult Oncology TOC
Discussion
NCCN Guidelines Version 2.2012 Senior Adult Oncolo gy
In July 2008 based on the results of these trials, Food and Drug Administration (FDA) strengthened its warnings to alert the physicians of increased risk of tumor progression and shortened survival in patients with advanced breast, cervical, head and neck, lymphoid and non-small cell lung cancers. Physicians were advised to use the lowest dose necessary to avoid transfusion. In addition, the use of ESAs is restricted to the treatment of anemia specifically related to myelosuppressive chemotherapy without curative intent. ESAs should be discontinued once the course of chemotherapy has been completed, and the anemia has resolved. The panel recommends that anemia in elderly cancer patients should be managed as outlined in the NCCN Guidelines for Cancer and chemotherapy-induced anemia.
Thrombocytopenia Chemotherapy-induced thrombocytopenia (CIT) is a common hematologic toxicity associated with cytotoxic and myeloablative chemotherapy. Dose reductions and/or interruptions of chemotherapy regimens are necessary in patients with severe thrombocytopenia. While chemotherapy-induced anemia and neutropenia can be managed with hematopoietic growth factors, safe and effective treatment of CIT is still a significant problem. Recombinant interleukin-11 is the only currently approved for the treatment of CIT in patients with nonmyeloid malignancies.226 However, it is toxic and of minimal clinical benefit. Ongoing clinical trials are also evaluating the efficacy of thrombopoietin-like agents such as romiplostim and eltrombopag for the treatment of CIT.227
Diarrhea
Diarrhea is a well recognized side effect associated with a number of chemotherapeutic agents, particularly greater for regimens containing 5-fluorouracil and irinotecan. Chemotherapy-induced diarrhea can lead to discontinuation of chemotherapy and poorer clinical outcomes. Loss
of fluid associated with persistent and severe diarrhea can lead to dehydration, renal insufficiency and electrolyte imbalance. Older adults with chemotherapy-induced diarrhea should be treated with early rehydration. The American Society of Clinical Oncology (ASCO) has published guidelines for the treatment of chemotherapy-induced diarrhea.228 These guidelines recommend comprehensive evaluation at the onset of diarrhea to determine the severity. Based on the results from various clinical trials, ASCO guidelines recommend loperamide therapy for mild to moderate diarrhea; octreotide (subcutaneous or intravenous if the patient is severely dehydrated) treatment for severe diarrhea or for treatment of chemotherapy-induced diarrhea that is refractory to loperamide therapy.
Mucositis
Oral and gastrointestinal mucositis are significant complications of radiotherapy and chemotherapy. The risk of mucositis increases with age. The Multinational Association of Supportive Care in Cancer and the International Society for Oral Oncology has developed guidelines for preventing, evaluating, and treating oral as well as gastrointestinal mucositis.229 The NCCN Task force has also published a comprehensive approach to the management of mucositis in patients with cancer.230 Once mucositis has occurred, patients should be kept well hydrated with intravenous fluids and hospitalization if necessary. Until recently, no pharmacological agents have been shown to effectively treat mucositis. In 2004, FDA approved palifermin (human keratinocyte growth factor) for the treatment of oral mucositis in patients with hematologic malignancies receiving myelotoxic therapy requiring hematopoietic stem cell support.231 Rosen et al have reported that palifermin was well tolerated and resulted in significant reduction of oral mucositis in patients with metastatic colorectal cancer treated with fluorouracil-based chemotherapy.232 However, the safety and efficacy of palifermin is yet to be firmly established in non-hematologic
Printed by Kelly Hayden on 10/12/2012 3:09:21 PM. For personal use only. Not approved for distribution. Copyright © 2012 National Comprehensive Cancer Network, Inc., All Rights Reserved.
Version 2.2012, 11/15/11 © National Comprehensive Cancer Network, Inc. 2011, All rights reserved. The NCCN Guidelines® and this illustration may not be reproduced in any form without the express written permission of NCCN®. MS-17
NCCN Guidelines IndexSenior Adult Oncology TOC
Discussion
NCCN Guidelines Version 2.2012 Senior Adult Oncolo gy
malignancies. A new time-released preparation of glutamine has shown promising results in the management of oral mucositis in patients with breast cancer receiving anthracycline-based chemotherapy.233
Targeted Therapies
In recent years the emergence of targeted therapies such as monoclonal antibodies and tyrosine kinase inhibitors have revolutionized the treatment and improved outcomes in a variety of malignancies. There is limited but growing data available on the toxicity of these targeted therapies in older adults with cancer and the use of targeted therapies should be individualized.234 In patients who are not able to tolerate cytotoxic chemotherapy, the risk-benefit ratio should be considered prior to initiation of targeted therapy. Prospective clinical trials which include sufficiently large number of older patients are needed to accurately determine the efficacy and tolerability of targeted therapies in this cohort of patients. See the section “Disease-specific issues” for the efficacy and tolerability of specific targeted therapies in elderly cancer patients.
Disease-specific Issues
Since the biologic characteristics of certain cancers are different in older patients compared to their younger counterparts and partly because of the decreased tolerance of treatment by older patients, chemotherapy should be individualized based the nature of the disease and the performance status of the patient. Disease-specific issues related to age in some cancer types are discussed below.
AML
Older patients with AML may have decreased sensitivity to chemotherapy due to increased prevalence of multi-drug resistance and unfavorable cytogenetic profiles.235 In view of the seriousness of the complications of AML treatment, the panel recommends that older
patients with AML should be treated according to the NCCN Guidelines for AML in centers skilled in the management and supportive care of AML.
Bladder cancer
Intravesical immunotherapy with bacille Calmette-Guérin (BCG) has decreased efficacy, particularly in patients older than 80 years.236, 237 In one study, at a median followup of 24 months, the cancer-free survival rates were 39% and 61% respectively for patients older than 80 years and patients 61-70 years old treated with BCG (p = 0.0002).236 Age was an independent risk factor for response after taking into account the stage, grade, sex and prior treatment.236 In the second study, the percent free from disease at 5 years after BCG therapy was 27% and 37% respectively (p = 0.005), for patients 70 years or older and patients younger than 70 years.237
Age alone should not be a criterion for making decisions regarding cystectomy, RT and chemotherapy in elderly patients. Radical cystectomy with pelvic lymph node dissection (PLND) is the standard treatment for patients with muscle invasive bladder cancer. In a SEER database analysis of 10,807 patients diagnosed with muscle-invasive bladder cancer, radical cystectomy resulted in a longer overall survival than treatment with RT in all age groups.238 While the overall survival benefit was significantly higher in the radical cystectomy arm for patients 70-79 years (33 months vs. 19 months), the survival benefit was smaller in patients 80 years or older (18 months vs.15 months). In patients 80 or older, there was a small overall survival benefit for radical cystectomy with PLND compared to bladder preservation with RT (21 months vs.15 months respectively).238 In a randomized study that compared neoadjuvant chemotherapy plus cystectomy with cystectomy alone, the addition of neoadjuvant chemotherapy resulted in improved survival among patients with locally advanced cancer.239 Median
Printed by Kelly Hayden on 10/12/2012 3:09:21 PM. For personal use only. Not approved for distribution. Copyright © 2012 National Comprehensive Cancer Network, Inc., All Rights Reserved.

Version 2.2012, 11/15/11 © National Comprehensive Cancer Network, Inc. 2011, All rights reserved. The NCCN Guidelines® and this illustration may not be reproduced in any form without the express written permission of NCCN®. MS-18
NCCN Guidelines IndexSenior Adult Oncology TOC
Discussion
NCCN Guidelines Version 2.2012 Senior Adult Oncolo gy
survival was 46 months and 77 months respectively (p = 0.06), for patients assigned to cystectomy and cystectomy plus neoadjuvant chemotherapy and the survival benefit was preserved with age.239
Breast cancer
Breast cancer in older women is associated with a more favorable tumor biology due to the high prevalence of hormone receptor-positive, HER2-negative, slowly proliferating tumors.240, 241 However, women older than 75 receive less aggressive treatment and have higher mortality rates from early stage breast cancer than younger women.242-244
Axillary lymph node dissection (ALND) in patients with early breast cancer improves locoregional control and provides staging information but is also associated with undesirable morbidity. Data from a randomized clinical trial suggest that ALND did not result in improvement in disease-free or overall survival compared to sentinel lymph node dissection alone in patients with invasive breast cancer (T1/T2) with limited sentinel lymph node involvement who were treated with breast conservation and systemic therapy.245 Elderly patients with early stage and clinically node negative breast cancer also did not benefit from ALND in terms of breast cancer mortality or survival.246, 247 In the absence of definitive evidence demonstrating superior survival associated with ALND, this procedure can be considered optional for elderly patients with particularly favorable tumors, those with serious comorbid conditions and for patients for whom the selection of adjuvant systemic therapy is unlikely to affected.
RT as a component of breast conserving therapy is not always necessary in selected women 70 years of age or older with stage I breast cancer. In a study which randomized women (70 years or older) with clinical stage I, estrogen receptor-positive breast cancer, to receive
lumpectomy and tamoxifen with whole breast RT or lumpectomy and tamoxifen for 5 years, there were no differences in overall survival or breast cancer specific survival.248, 249 However, locoregional recurrence was higher among women who did not receive RT (4% vs.1% for those who received RT).
Older women with stage I-III breast cancer derive similar clinical benefits from adjuvant chemotherapy compared to younger patients. However, older patients have an increased risk of treatment-related side effects and mortality.250 Adjuvant chemotherapy with CMF (cyclophosphamide, methotrexate, and fluorouracil) or doxorubicin plus cyclophosphamide was superior to capecitabine alone.251 The 3-year relapse-free survival rates were 68% and 85%, respectively for the capecitabine group and the standard chemotherapy group (p < 0.001).The corresponding overall survival rates were 86% and 91% respectively (p = 0.02).251 The benefit was pronounced in women with hormone receptor-negative tumors (p < 0.001).
Trastuzumab is approved for the treatment of patients with HER-2-positive early stage and metastatic breast cancer. However, few elderly patients (70 years or older) have been included in the pivotal trastuzumab trials.252, 253 Cardiac toxicity has been a concern in patients receiving trastuzumab-based therapy.180 Age is a risk factor for CHF in patients receiving trastuzumab-based regimens. In elderly patients (70 or older), trastuzumab-related cardiotoxicity was associated with a history of cardiac disease and diabetes.184 See Cardiac toxicity under Side effects of chemotherapy in this manuscript.
Central nervous system cancers
Glioblastoma multiforme Surgery is the primary treatment option for newly diagnosed patients with glioblastoma multiforme. Available evidence suggest that gross
Printed by Kelly Hayden on 10/12/2012 3:09:21 PM. For personal use only. Not approved for distribution. Copyright © 2012 National Comprehensive Cancer Network, Inc., All Rights Reserved.

Version 2.2012, 11/15/11 © National Comprehensive Cancer Network, Inc. 2011, All rights reserved. The NCCN Guidelines® and this illustration may not be reproduced in any form without the express written permission of NCCN®. MS-19
NCCN Guidelines IndexSenior Adult Oncology TOC
Discussion
NCCN Guidelines Version 2.2012 Senior Adult Oncolo gy
total resection is associated with greater overall survival in patients 70 years or older.254, 255 In a small, randomized study involving patients 65 years or older (n = 30), the estimated median survival time was longer after open craniotomy and resection of the tumor (171 days compared to 85 days after the stereotactic biopsy; p = 0.035).254 For patients 65 or older, gross total resection was associated with a longer survival compared to biopsy and subtotal resection in a retrospective analysis.255 It is difficult to be certain, given the small size of the randomized trials studies and the retrospective nature of other studies, whether the improved survival is a direct effect of the degree of surgery or related to selection bias. Furthermore, the median survival after resection alone is less than 12 months, indicating that additional treatment options are needed. In a retrospective review, aggressive treatment with all three components (RT, chemotherapy, and surgery) was associated with best overall survival.256
Postoperative RT alone or in combination with temozolomide has been effective in improving clinical outcomes in elderly patients.257-259 In a small randomized study, (70 years or older; n = 85), at a median follow-up of 21 weeks, median survival was longer for those who received postoperative RT plus supportive care compared to supportive care alone (29 weeks and 17 weeks respectively).258 RT was not associated with severe adverse events and the results of quality-of-life and cognitive evaluations over time also did not differ significantly between the treatment groups. In another randomized trial, overall survival times were similar for postoperative standard RT (5.1 months) and shorter-course RT (5.6 months) for elderly patients (60 years or older, n = 100).257 However, among those who completed RT as planned, more patients who received standard RT required a post treatment increase in corticosteroid dosage (49% compared to only 23% of those who received shorter-course RT). These results suggest
that postoperative shorter-course RT is a reasonable treatment option for patients 70 years or older.
In a phase III randomized trial, the addition of temozolomide concurrently with RT followed by 6 months of adjuvant temozolomide improved survival rates in patients between the ages 60-70 years with newly diagnosed patients with glioblastoma multiforme.259 At 5-year follow-up, overall survival rates were 27%, 16%, 12% and 9.8% at 2, 3, 4 and 5 years respectively for those who received RT with concurrent temozolomide. The corresponding survival rates were 11%, 4%, 3% and 2% for those treated with RT alone. However, the benefit of concurrent chemoradiation therapy is unclear in patients older than 70, but is likely to be helpful in selected “fit” patients.260
Bevacizumab, an anti-vascular endothelial growth factor receptor (VEGFR) antibody, resulted in a significant improvement in progression-free and overall survival in patients 55 years or older and poor performance status, in a single institution retrospective analysis.261 VEGFR expression was also significantly higher in patients 55 years older, implying that bevacizumab could be beneficial for this group of patients with recurrent glioblastoma multiforme.261
Primary CNS lymphoma Methotrexate-based chemotherapy is associated with superior outcome in elderly patients with primary CNS lymphoma. In patients older than 60 years, high-dose methotrexate-based chemotherapy with or without whole brain RT resulted in a median overall survival of 29 months.262 However, there was a striking increase in neurotoxicity in patients older than 60 compared to younger patients (75% vs. 26%). In a more recent retrospective analysis, Ney et al also reported similar median overall survival (25 months) in elderly patients treated with chemotherapy alone.263 In another retrospective review of 31 elderly patients (70
Printed by Kelly Hayden on 10/12/2012 3:09:21 PM. For personal use only. Not approved for distribution. Copyright © 2012 National Comprehensive Cancer Network, Inc., All Rights Reserved.

Version 2.2012, 11/15/11 © National Comprehensive Cancer Network, Inc. 2011, All rights reserved. The NCCN Guidelines® and this illustration may not be reproduced in any form without the express written permission of NCCN®. MS-20
NCCN Guidelines IndexSenior Adult Oncology TOC
Discussion
NCCN Guidelines Version 2.2012 Senior Adult Oncolo gy
years or older), high-dose methotrexate induced an overall radiographic response rate of radiographic response rate was 97%; the progression-free and overall survival rates were 7 months and 37 months, respectively.264 These results indicate that patients 60 years or older with primary CNS lymphoma should be treated initially with chemotherapy, saving whole brain RT for those with recurrent or refractory disease, given the increase in neurotoxicity.
Colorectal cancers
Age alone should not be a contraindication for curative surgery in elderly patients with early stage and in resectable colorectal cancer.265-267 Results of a retrospective study which evaluated age-related surgical risk and outcome in patients with colorectal cancer showed that the long-term results after surgery were more dependent on the stage of disease and on the type of adjuvant or palliative treatment, than on age.265 In the metastatic setting, a study by Adam et al compared the outcome of liver resection for colorectal metastases in elderly patients with that of younger patients; the 3-year overall survival was 57% in elderly and 60% in younger patients (p < 0.001).268 The overall survival was similar among patients aged 70-75, 75-80 or at least 80 years (58%, 55% and 54%, respectively; p = 0.160). Careful preoperative planning and non-emergent surgery are more likely to result in optimal outcomes.268
In the adjuvant setting, older patients derive similar benefit from 5-FU-based chemotherapy as younger patients.10, 269 However, older patients may be at an increased risk for hematological toxicities. In a pooled analysis of adjuvant chemotherapy trials, the relative benefit of overall survival from adjuvant chemotherapy was similar across all age groups, with no increased incidence of toxicities among patients 70 or older, with the exception of leukopenia in one study.10 The 5-year overall survival rate was 71% for those who received adjuvant
chemotherapy compared to 64% for those untreated. However, after 5 years, the absolute benefit of chemotherapy was smaller in patients 70 or older due to competing causes of deaths. Pooled analyses of data from adjuvant trials using newer regimens containing oxaliplatin did not show significant benefit in disease-free or overall survival compared to 5-fluorouracil and leucovorin in patients 70 years or older.270 Scant data are available among patients older than 80 years. Due to the lack of data from prospective randomized studies, adjuvant chemotherapy with newer regimens should be considered on an individual basis for patients 70 years of older.
For patients with metastatic disease, 5-FU-based palliative chemotherapy resulted in equal overall survival (10.8 months and 11.3 months respectively; p = 0.31) and progression-free survival (5.5 months and 5.3 months respectively; p = 0.01) in elderly (70 years or older) and younger patients with metastatic colorectal cancer.271 Infusional 5-FU was more effective than bolus 5-FU in both age groups. A recent prospective randomized trial (MRC FOCUS2) reported some improvement in median progression-free survival with the addition of reduced dose oxaliplatin to 5-FU-based chemotherapy in elderly and frail patients with metastatic colorectal cancer, but the difference was not significant (5.8 months vs. 4.5 months; p = 0.07).272 The replacement of 5-FU with capecitabine resulted in higher risk of grade 3 or higher toxicity and no improvement in quality of life. In the OPTIMOX1 study, oxaliplatin-based chemotherapy stop-and-go (FOLFOX7 for 6 cycles, maintenance without oxaliplatin for 12 cycles, and reintroduction of FOLFOX7) had similar efficacy and tolerability compared to standard oxaliplatin-based regimen (FOLFOX4) regimen in patients aged between 76 and 80 years with metastatic colorectal cancer,273 implying that stop-and-go strategies or maintenance 5-FU
Printed by Kelly Hayden on 10/12/2012 3:09:21 PM. For personal use only. Not approved for distribution. Copyright © 2012 National Comprehensive Cancer Network, Inc., All Rights Reserved.

Version 2.2012, 11/15/11 © National Comprehensive Cancer Network, Inc. 2011, All rights reserved. The NCCN Guidelines® and this illustration may not be reproduced in any form without the express written permission of NCCN®. MS-21
NCCN Guidelines IndexSenior Adult Oncology TOC
Discussion
NCCN Guidelines Version 2.2012 Senior Adult Oncolo gy
based chemotherapy may be desirable for elderly patients with metastatic disease to minimize toxicities.
Bevacizumab274, 275 and anti-epidermal growth factor receptor (EGFR) antibodies, cetuximab 276-278 and panitumumab279, 280 have also been evaluated for the treatment of elderly patients with metastatic colorectal cancer. Data from retrospective studies has shown that cetuximab as a single agent or in combination with irinotecan has a favorable safety profile in heavily pretreated elderly patients (70 years or older) with metastatic colorectal cancer and the efficacy was similar to that observed in younger patients with acceptable tolerability.276, 277 Response rates and progression-free survival were significantly higher for elderly patients (70 or older) with wild type-KRAS mutations compared to those with KRAS mutations.277 In a phase II clinical trial, cetuximab was safe and moderately active when used as a first-line single agent in fit elderly patients with metastatic colorectal cancer.278
In the phase III trial that evaluated the activity of panitumumab plus best supportive care vs. best supportive care alone in patients with metastatic colorectal cancer, panitumumab had a favorable effect on progression-free survival regardless of age (hazard ratio = 0.51 and 0.60, respectively, for patients younger than 65 and older than 65).279 Progression-free survival, overall survival and overall response rates were similar in elderly and younger patients. In this study, the efficacy of panitumumab is confined to patients with wild type-KRAS mutations.280 The safety and efficacy of bevacizumab in elderly patients (65 years or older) were comparable to that of younger patients.274, 275 In the BRiTE study, the median progression-free survival was similar across all age cohorts. However, median overall survival and survival beyond progression declined with age.275 In a retrospective analysis, the addition of bevacizumab to chemotherapy significantly improved progression-free and overall survival in patients 65 years or older with
metastatic colorectal cancer.274 However, it is associated with higher rate of arterial thromboembolic events in elderly patients.
Head and Neck cancers
Surgery is associated with good clinical outcomes with acceptable complication rates in elderly patients, however complication rates increase with comorbidities.52, 281 In retrospective analysis of elderly patients (70 or older), overall complication rate was 63% and 54% of patients experienced clinically important surgical and/or medical complications.281 Bilateral neck dissection, male sex, presence of two or more comorbidities and advanced stage of disease were associated with postoperative complications.52
Elderly patients (70 or older) with squamous cell carcinoma of the head and neck (SCCHN) who are treated with radiation therapy experience similar overall survival in comparison to younger patients.282 Although there were no significant differences in late toxicities in older patients compared to those younger than 70 (median of 3 years of follow-up), severe grade 3 and 4 functional acute toxicity was significantly more frequent in older patients (67% for patients 65 or older compared to 49% in younger patients).282 Few patients over the age of 70 have been included in trials evaluating induction chemotherapy and there is limited data on the efficacy and toxicity of such an approach in this subset of patients.283, 284 Randomized trials and meta-analyses have reported that concurrent chemoradiation offers greater benefit than RT or induction chemotherapy alone.285, 286 In a prospective randomized study which included 255 patients 60 years or older, concurrent chemoradiation was superior to RT alone or induction chemotherapy followed by RT for laryngeal preservation and locoregional control in patients (both older and younger than 60 years) with localized laryngeal cancer.285 In the meta-analysis of chemotherapy in head and neck cancer (MACH-NC), concurrent chemoradiation offered a significant overall survival benefit
Printed by Kelly Hayden on 10/12/2012 3:09:21 PM. For personal use only. Not approved for distribution. Copyright © 2012 National Comprehensive Cancer Network, Inc., All Rights Reserved.
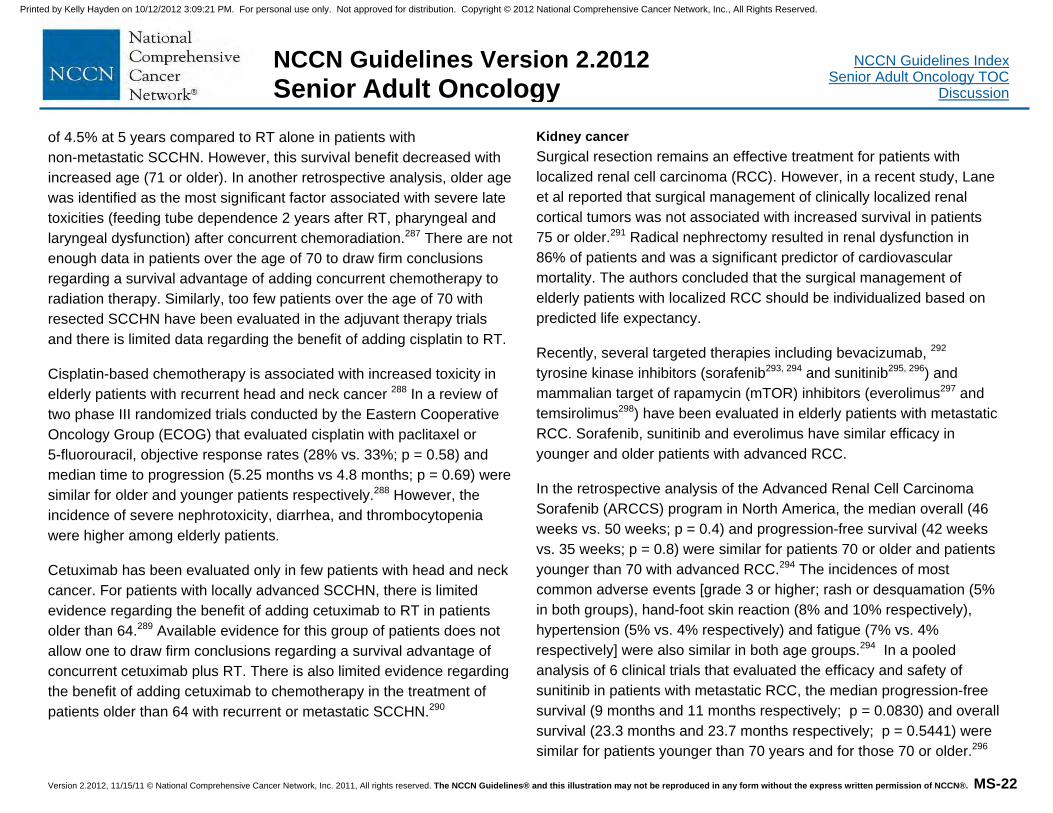
Version 2.2012, 11/15/11 © National Comprehensive Cancer Network, Inc. 2011, All rights reserved. The NCCN Guidelines® and this illustration may not be reproduced in any form without the express written permission of NCCN®. MS-22
NCCN Guidelines IndexSenior Adult Oncology TOC
Discussion
NCCN Guidelines Version 2.2012 Senior Adult Oncolo gy
of 4.5% at 5 years compared to RT alone in patients with non-metastatic SCCHN. However, this survival benefit decreased with increased age (71 or older). In another retrospective analysis, older age was identified as the most significant factor associated with severe late toxicities (feeding tube dependence 2 years after RT, pharyngeal and laryngeal dysfunction) after concurrent chemoradiation.287 There are not enough data in patients over the age of 70 to draw firm conclusions regarding a survival advantage of adding concurrent chemotherapy to radiation therapy. Similarly, too few patients over the age of 70 with resected SCCHN have been evaluated in the adjuvant therapy trials and there is limited data regarding the benefit of adding cisplatin to RT.
Cisplatin-based chemotherapy is associated with increased toxicity in elderly patients with recurrent head and neck cancer 288 In a review of two phase III randomized trials conducted by the Eastern Cooperative Oncology Group (ECOG) that evaluated cisplatin with paclitaxel or 5-fluorouracil, objective response rates (28% vs. 33%; p = 0.58) and median time to progression (5.25 months vs 4.8 months; p = 0.69) were similar for older and younger patients respectively.288 However, the incidence of severe nephrotoxicity, diarrhea, and thrombocytopenia were higher among elderly patients.
Cetuximab has been evaluated only in few patients with head and neck cancer. For patients with locally advanced SCCHN, there is limited evidence regarding the benefit of adding cetuximab to RT in patients older than 64.289 Available evidence for this group of patients does not allow one to draw firm conclusions regarding a survival advantage of concurrent cetuximab plus RT. There is also limited evidence regarding the benefit of adding cetuximab to chemotherapy in the treatment of patients older than 64 with recurrent or metastatic SCCHN.290
Kidney cancer
Surgical resection remains an effective treatment for patients with localized renal cell carcinoma (RCC). However, in a recent study, Lane et al reported that surgical management of clinically localized renal cortical tumors was not associated with increased survival in patients 75 or older.291 Radical nephrectomy resulted in renal dysfunction in 86% of patients and was a significant predictor of cardiovascular mortality. The authors concluded that the surgical management of elderly patients with localized RCC should be individualized based on predicted life expectancy.
Recently, several targeted therapies including bevacizumab, 292 tyrosine kinase inhibitors (sorafenib293, 294 and sunitinib295, 296) and mammalian target of rapamycin (mTOR) inhibitors (everolimus297 and temsirolimus298) have been evaluated in elderly patients with metastatic RCC. Sorafenib, sunitinib and everolimus have similar efficacy in younger and older patients with advanced RCC.
In the retrospective analysis of the Advanced Renal Cell Carcinoma Sorafenib (ARCCS) program in North America, the median overall (46 weeks vs. 50 weeks; p = 0.4) and progression-free survival (42 weeks vs. 35 weeks; p = 0.8) were similar for patients 70 or older and patients younger than 70 with advanced RCC.294 The incidences of most common adverse events [grade 3 or higher; rash or desquamation (5% in both groups), hand-foot skin reaction (8% and 10% respectively), hypertension (5% vs. 4% respectively) and fatigue (7% vs. 4% respectively] were also similar in both age groups.294 In a pooled analysis of 6 clinical trials that evaluated the efficacy and safety of sunitinib in patients with metastatic RCC, the median progression-free survival (9 months and 11 months respectively; p = 0.0830) and overall survival (23.3 months and 23.7 months respectively; p = 0.5441) were similar for patients younger than 70 years and for those 70 or older.296
Printed by Kelly Hayden on 10/12/2012 3:09:21 PM. For personal use only. Not approved for distribution. Copyright © 2012 National Comprehensive Cancer Network, Inc., All Rights Reserved.
Version 2.2012, 11/15/11 © National Comprehensive Cancer Network, Inc. 2011, All rights reserved. The NCCN Guidelines® and this illustration may not be reproduced in any form without the express written permission of NCCN®. MS-23
NCCN Guidelines IndexSenior Adult Oncology TOC
Discussion
NCCN Guidelines Version 2.2012 Senior Adult Oncolo gy
The incidences of adverse events were also similar, although some (fatigue, decreased appetite/weight, cough, peripheral edema, thrombocytopenia and anemia) were more common in elderly patients.
Temsirolimus was associated with improved overall survival (p = 0.008) and progression-free survival (p < 0.001) compared to interferon among patients with metastatic RCC and poor prognosis.298 In a multicenter, randomized phase III trial, the median overall survival was 10.9 months for temsirolimus group compared to 7.3 months and 8.4 months, respectively in the groups treated with interferon alfa alone or in combination with temsirolimus. Temsirolimus alone was associated with fewer incidences of grade 3 or 4 adverse events than interferon. Interferon is not recommended for elderly patients because of its increased toxicity. In a subgroup analysis of phase III trial that evaluated the safety and efficacy of everolimus in patients with metastatic RCC, median progression-free survival was 5.36 months and 5.13 months, respectively (p < 0.001), for patients 65 or older and 70 or older.297 Older patients were at increased risk of adverse events including stomatitis, anemia and infection.
Multiple Myeloma
In elderly patients with newly diagnosed multiple myeloma, induction chemotherapy with the combination of melphalan, prednisone thalidomide (MPT) was associated with a significantly superior response rates, progression-free survival, time-to-treatment progression and event-free survival compared with melphalan and prednisone (MP) in randomized studies.299-306 However, overall survival benefit for MPT was reported only in two of these studies. In the IFM 99-06 trial which compared MPT, MP or reduced intensity autologous stem cell transplant, median overall survival times were 51.6 months, 33.2 months and 38.3 months, respectively for the three treatment groups; MPT regimen was associated with a significantly better overall
survival than MP regimen (p = 0.0006) or reduced intensity autologous stem cell transplant (p = 0.027).301 In the IFM 01/01 trial, median overall survival times were 44 months and 29 months respectively (p = 0.028), for elderly patients (75 or older) treated with MPT and MP.302 However, MPT was associated with significant toxicity [constipation, fatigue, VTE, neuropathy, cytopenias and infection].306 Deep vein thrombosis (DVT) prophylaxis with low molecular weight heparin (LMWH) is recommended for elderly patients receiving thalidomide-based regimens. In a phase III randomized trial, aspirin and fixed low-dose warfarin showed similar safety and efficacy in reducing thromboembolic complications compared to LMWH in patients with myeloma treated with thalidomide-based regimen whereas in elderly patients LMWH was more effective than warfarin.307
Bortezomib, melphalan and prednisone (VMP) was superior to MP alone in patients (median age 71 years) with newly diagnosed with multiple myeloma that were ineligible for high-dose therapy and the survival benefit was seen across all age groups.308, 309 However, the rates of adverse events (peripheral neuropathy, cytopenias, and fatigue) were higher among patients in the VMP group than the MP group. The subgroup analyses of the VISTA trial showed that VMP resulted in longer overall survival among patients younger than 75 compared to those 75 or older (3-year overall survival rates were 74.1% and 55.5% respectively; p = 0.011).309 In another randomized trial, in the induction phase, bortezomib, thalidomide and prednisone (VTP) and VMP resulted in similar response rates (partial response rates were 81% and 80% respectively) and overall survival, with different side effect profiles.310 Incidences of infection were higher in the VMP group and VTP was associated with higher incidences of cardiac events. In the maintenance setting, complete response rates were higher with bortezomib and thalidomide (44%) compared to bortezomib and
Printed by Kelly Hayden on 10/12/2012 3:09:21 PM. For personal use only. Not approved for distribution. Copyright © 2012 National Comprehensive Cancer Network, Inc., All Rights Reserved.

Version 2.2012, 11/15/11 © National Comprehensive Cancer Network, Inc. 2011, All rights reserved. The NCCN Guidelines® and this illustration may not be reproduced in any form without the express written permission of NCCN®. MS-24
NCCN Guidelines IndexSenior Adult Oncology TOC
Discussion
NCCN Guidelines Version 2.2012 Senior Adult Oncolo gy
prednisone (39%); however, peripheral neuropathy was higher with bortezomib and thalidomide.310 In a phase III study, the 4-drug combination of bortezomib, melphalan, prednisone and thalidomide (VMPT) followed by maintenance with bortezomib and thalidomide (VT) was associated with higher response rates and progression-free survival compared to VMP alone but did not result in an improvement in overall survival.311 The 3-year overall survival rates were 89% and 87%, respectively for VMPT followed by VT and with VMP (p = 0.77). VMPT followed by VT was also associated with higher grade 3 or 4 toxicities (neutropenia, cardiologic and thromboembolic events).
Dexamethasone-based regimens are associated with increased mortality and severe hematologic toxicities compared to MP in elderly patients with newly diagnosed multiple myeloma not eligible for high-dose therapy.312, 313 In a large randomized trial (IFM 95-01), which compared MP with dexamethasone-based regimens (dexamethasone, alone or in combination with melphalan or interferon), while there was no difference in overall survival between the 4 treatment groups, the response rate was significantly higher in patients receiving dexamethasone and melphalan; progression-free-survival was significantly better for patients receiving MP and melphalan and dexamethasone; however, the toxicities associated with dexamethasone-based regimens (severe pyogenic infections in the melphalan-dexamethasone arm; hemorrhage, severe diabetes, gastrointestinal and psychiatric complications in the dexamethasone arms) were significantly higher than with MP.312 The results of a recent randomized trial suggest the low-dose dexamethasone used in combination with lenalidomide is associated with better short-term overall survival and lower toxicity than high-dose dexamethasone and lenalidomide in patients with newly diagnosed myeloma.313
Non-Hodgkin’s Lymphoma (NHL)
In randomized clinical trials, the outcome in older patients who received full dose anthracycline-based therapy was comparable to that of younger patients. However, the complete response rates drop to 45% in patients 70 years or older.314 Age and serum interleukin-6 levels have been identified as an independent prognostic factors for complete response and failure-free survival in patients with diffuse large B-cell lymphoma (DLBCL).315-319 Rituximab (an anti CD-20 monoclonal antibody) has been well-tolerated and effective in the treatment of elderly patients with DLBCL with no apparent increase in toxicity. A number of randomized trials which included older adults exclusively have shown that the addition of rituximab to CHOP improves survival in patients with advanced stage DLBCL.210, 320-322
Hepatitis B virus (HBV) reactivation has been reported to occur in patients treated with chemotherapy with or without rituximab; treatment with rituximab alone is also a risk for HBV reactivation.323 Antiviral prophylaxis has been shown to prevent chemoimmunotherapy associated HBV reactivation.324-326 Due to the significant of risk of HBV reactivation associated with rituximab, the panel recommends that elderly patients receiving rituximab should be monitored for HBV reactivation as outlined in the NCCN Guidelines for NHL.
NSCLC
Surgery is the standard treatment for patients with localized NSCLC. Retrospective studies have demonstrated that age alone is not a contraindication for surgery and surgery is well tolerated in carefully selected patients.327-331 Long-term follow-up of elderly patients (70 or older) showed that the mortality and prognosis were similar to those in younger patients.327 The postoperative mortality and the 5-year survival rates were 3% and 48% respectively for elderly patients. However, pneumonectomy was associated with a higher mortality rate in patients
Printed by Kelly Hayden on 10/12/2012 3:09:21 PM. For personal use only. Not approved for distribution. Copyright © 2012 National Comprehensive Cancer Network, Inc., All Rights Reserved.

Version 2.2012, 11/15/11 © National Comprehensive Cancer Network, Inc. 2011, All rights reserved. The NCCN Guidelines® and this illustration may not be reproduced in any form without the express written permission of NCCN®. MS-25
NCCN Guidelines IndexSenior Adult Oncology TOC
Discussion
NCCN Guidelines Version 2.2012 Senior Adult Oncolo gy
70 or older than younger patients (22% and 3.2% respectively; p < 0.005).332 Therefore, pneumonectomy should be performed with caution in elderly patients.
Older patients with completely resected NSCLC derive similar survival benefits with adjuvant chemotherapy as younger patients.333-335 A pooled analysis of 4,584 patients from five trials of adjuvant cisplatin-based chemotherapy showed that elderly patients had a survival benefit that was similar to that of their younger counterparts, without significant toxicity.335 Another retrospective analysis of the Intergroup study (JBR.10) also showed that adjuvant vinorelbine and cisplatin improved survival in patients older than 65 years with acceptable toxicity.334
Combined modality therapy is feasible and effective in elderly patients with locally advanced disease, however it is associated with more toxicities (esophagitis, pneumonitis and myelosuppression) especially in patients with poor performance status (KPS less than 90).336, 337 Langer et al reported that concurrent chemotherapy with once daily RT was beneficial to elderly patients with locally advanced NSCLC. Median survival time was 22.4 months with concurrent chemotherapy with daily RT compared to 16.4 months and 10.8 months, respectively for concurrent chemotherapy with twice-daily RT, and sequential chemotherapy and daily RT. Short-term toxicities were more pronounced in the elderly patients.336 Schild et al also reported that elderly and younger patients had similar survival benefit from concurrent chemoradiation therapy.337 The 2- and 5-year survival rates were 36% and 13%, respectively, in elderly patients with locally advanced disease compared to 39% and 18%, respectively, in patients younger than 70 years (p = 0.4). Pneumonitis and myelosuppression were more pronounced in the elderly patients. In some studies,
combined modality treatment was associated with excess toxicity and no survival benefit for the elderly.338, 339
Chemotherapy is associated with improved quality of care in comparison to best supportive care in elderly patients with advanced disease.340, 341 In the ELVIS study, vinorelbine plus best supportive care was superior to best supportive care alone, in terms of both survival and quality of life.340 Median survival and 1-year survival were significantly better in the vinorelbine arm. The results of the subgroup analyses of phase III trials evaluating chemotherapy for patients with advanced NSCLC have shown elderly patients in good performance status derive similar clinical benefit with combination chemotherapy as the younger patients; however the incidences of toxicities are higher among elderly patients.336, 342, 343 The two trials that have compared the combination of vinorelbine and gemcitabine with single agent vinorelbine or gemcitabine in elderly patients with advanced NSCLC have shown conflicting results.344, 345 The results of the Southern Italy Cooperative Oncology Group (SICOG) phase III trial showed that the combination of gemcitabine and vinorelbine was associated with a significantly better survival than vinorelbine alone in elderly NSCLC patients344 whereas in the MILES study, the combination of gemcitabine and vinorelbine was more toxic and failed to show any survival advantage over single agent therapy with vinorelbine or gemcitabine alone.345 There is emerging data confirming the survival benefit of 2-drug regimens compared to single agent therapy for patients with advanced disease. In the recent multicenter randomized phase III trial (IFCT-0501), the combination of paclitaxel and carboplatin was associated a significantly longer survival in patients 70 years or older (PS 0-2) with advanced NSCLC than single agent therapy with vinorelbine or gemcitabine, despite an increased risk of side effects (including febrile neutropenia, asthenia, toxic death rate) with
Printed by Kelly Hayden on 10/12/2012 3:09:21 PM. For personal use only. Not approved for distribution. Copyright © 2012 National Comprehensive Cancer Network, Inc., All Rights Reserved.

Version 2.2012, 11/15/11 © National Comprehensive Cancer Network, Inc. 2011, All rights reserved. The NCCN Guidelines® and this illustration may not be reproduced in any form without the express written permission of NCCN®. MS-26
NCCN Guidelines IndexSenior Adult Oncology TOC
Discussion
NCCN Guidelines Version 2.2012 Senior Adult Oncolo gy
combination therapy.346 Median overall survival was 10.3 months and 6.2 months, respectively and the 1-year survival rates were 44.5% and 25.4%, respectively.
Bevacizumab347 and erlotinib, an EGFR inhibitor348,349 have been evaluated in elderly patients with advanced NSCLC. In a subset analysis of phase III study (ECOG 4599), elderly patients with NSCLC who were randomized to paclitaxel and carboplatin with bevacizumab experienced a higher degree of toxicity with no improvement in overall survival compared to those who received paclitaxel and carboplatin.347 Bevacizumab should be used with caution in older patients. Erlotinib, although active and relatively well tolerated in chemotherapy-naive elderly patients (70 years or older) with advanced NSCLC, is associated with higher incidences of interstitial lung disease and toxicity-related discontinuation (5% and 12% respectively),348 compared to only 1% and 5% observed in the erlotinib arm of the BR.21 trial where the median age was only 62 years. A recent subgroup analysis of the BR.21 trial also confirmed that elderly patients experienced greater toxicity and prolonged dose interruptions compared to younger patients, even though survival and quality-of-life benefits were similar for both groups.349
Prostate cancer
Management of elderly patients with prostate cancer is similar to that of younger patients.350 Treatment options are based on anticipated life expectancy of the individual patient and whether they are symptomatic. See the NCCN Guidelines for Prostate cancer for the management of patients with localized or locally advanced disease.
Docetaxel-based chemotherapy has been effective in elderly patients with metastatic castration-resistant prostate cancer.351, 352 In the subgroup analysis of the TAX 327 trial, the survival benefit of 3-weekly
docetaxel prednisone compared with mitoxantrone with prednisone was seen across all age groups; median overall survival was 18.1 months for patients 69 or older compared to 17.6 months for patients 68 or younger.353 The hazard ratios for younger and older patients were 0.81 and 0.77, respectively. The hazard ratio was 0.80 with the age cutoff of 75 years.
Recently, cabazitaxel has demonstrated activity in patients with metastatic castration-resistant prostate cancer that has progressed on docetaxel-based chemotherapy.354 In a randomized phase III trial, cabazitaxel with prednisone improved overall survival compared to mitoxantrone plus prednisone. The survival benefit was seen across all age groups.355 The hazard ratios for overall survival were 0.62 and 0.81 respectively for older (65 or older) and younger patients. Growth factor support is strongly recommended for patients 65 years or older receiving cabazitaxel due to the increased risk of neutropenia in these patients.
Summary Cancer is the leading cause of death in women and men aged 60 to 79 years. The biologic characteristics of certain cancers are different in older patients compared to their younger counterparts and older patients also have decreased tolerance to chemotherapy. Nevertheless, advanced age alone should not be the only criteria to preclude effective cancer treatment that could improve quality of life or lead to a survival benefit in older patients. Treatment should be individualized based the nature of the disease, the physiologic status of the patient and patient’s preferences.
Chronological age is not reliable in estimating life expectancy, functional reserve, or the risk of treatment complications. The best guide as to whether cancer treatment is appropriate may be provided
Printed by Kelly Hayden on 10/12/2012 3:09:21 PM. For personal use only. Not approved for distribution. Copyright © 2012 National Comprehensive Cancer Network, Inc., All Rights Reserved.

Version 2.2012, 11/15/11 © National Comprehensive Cancer Network, Inc. 2011, All rights reserved. The NCCN Guidelines® and this illustration may not be reproduced in any form without the express written permission of NCCN®. MS-27
NCCN Guidelines IndexSenior Adult Oncology TOC
Discussion
NCCN Guidelines Version 2.2012 Senior Adult Oncolo gy
by careful assessment of the older patient. CGA can be utilized to assess life expectancy and risk of morbidity from cancer in elderly patients. CGA in turn enables physicians to develop a coordinated plan for cancer treatment as well as guide interventions tailored to the patient’s problems.
Printed by Kelly Hayden on 10/12/2012 3:09:21 PM. For personal use only. Not approved for distribution. Copyright © 2012 National Comprehensive Cancer Network, Inc., All Rights Reserved.

Version 2.2012, 11/15/11 © National Comprehensive Cancer Network, Inc. 2011, All rights reserved. The NCCN Guidelines® and this illustration may not be reproduced in any form without the express written permission of NCCN®. REF-1
NCCN Guidelines IndexSenior Adult Oncology TOC
Discussion
NCCN Guidelines Version 2.2012 Senior Adult Oncolo gy
References 1. Jemal A, Siegel R, Xu J, Ward E. Cancer statistics, 2010. CA Cancer J Clin 2010;60:277-300. Available at: http://www.ncbi.nlm.nih.gov/pubmed/20610543.
2. Altekruse SF KC, Krapcho M, Neyman N, Aminou R, Waldron W, Ruhl J, Howlader N, Tatalovich Z, Cho H, Mariotto A, Eisner MP, Lewis DR, Cronin K, Chen HS, Feuer EJ, Stinchcomb DG, Edwards BK (eds). SEER Cancer Statistics Review, 1975-2007: National Cancer Institute. Bethesda, MD, based on November 2009 SEER data submission, posted to the SEER web site, 2010. Available at: http://seer.cancer.gov/csr/1975_2007/.
3. Smith BD, Smith GL, Hurria A, et al. Future of cancer incidence in the United States: burdens upon an aging, changing nation. J Clin Oncol 2009;27:2758-2765. Available at: http://www.ncbi.nlm.nih.gov/pubmed/19403886.
4. Balducci L, Beghe C. Cancer and age in the USA. Crit Rev Oncol Hematol 2001;37:137-145. Available at: http://www.ncbi.nlm.nih.gov/pubmed/11166587.
5. Talarico L, Chen G, Pazdur R. Enrollment of elderly patients in clinical trials for cancer drug registration: a 7-year experience by the US Food and Drug Administration. J Clin Oncol 2004;22:4626-4631. Available at: http://www.ncbi.nlm.nih.gov/pubmed/15542812.
6. Saltzstein SL, Behling CA. 5- and 10-year survival in cancer patients aged 90 and older: a study of 37,318 patients from SEER. J Surg Oncol 2002;81:113-116; dicussion 117. Available at: http://www.ncbi.nlm.nih.gov/pubmed/12407720.
7. Extermann M. Management issues for elderly patients with breast cancer. Curr Treat Options Oncol 2004;5:161-169. Available at: http://www.ncbi.nlm.nih.gov/pubmed/14990210.
8. Chen H, Cantor A, Meyer J, et al. Can older cancer patients tolerate chemotherapy? A prospective pilot study. Cancer 2003;97:1107-1114. Available at: http://www.ncbi.nlm.nih.gov/pubmed/12569613.
9. Christman K, Muss HB, Case LD, Stanley V. Chemotherapy of metastatic breast cancer in the elderly. The Piedmont Oncology Association experience [see comment]. JAMA 1992;268:57-62. Available at: http://www.ncbi.nlm.nih.gov/pubmed/1608114.
10. Sargent DJ, Goldberg RM, Jacobson SD, et al. A pooled analysis of adjuvant chemotherapy for resected colon cancer in elderly patients. N Engl J Med 2001;345:1091-1097. Available at: http://www.ncbi.nlm.nih.gov/pubmed/11596588.
11. Balducci L. Management of cancer in the elderly. Oncology (Williston Park) 2006;20:135-143;. Available at: http://www.ncbi.nlm.nih.gov/pubmed/16562648.
12. Wedding U, Honecker F, Bokemeyer C, et al. Tolerance to chemotherapy in elderly patients with cancer. Cancer Control 2007;14:44-56. Available at: http://www.ncbi.nlm.nih.gov/pubmed/17242670.
13. Walter LC, Covinsky KE. Cancer screening in elderly patients: a framework for individualized decision making. JAMA 2001;285:2750-2756. Available at: http://www.ncbi.nlm.nih.gov/pubmed/11386931.
14. Lee SJ, Lindquist K, Segal MR, Covinsky KE. Development and validation of a prognostic index for 4-year mortality in older adults. JAMA 2006;295:801-808. Available at: http://www.ncbi.nlm.nih.gov/pubmed/16478903.
15. Carey EC, Walter LC, Lindquist K, Covinsky KE. Development and validation of a functional morbidity index to predict mortality in community-dwelling elders. J Gen Intern Med 2004;19:1027-1033. Available at: http://www.ncbi.nlm.nih.gov/pubmed/15482555.
Printed by Kelly Hayden on 10/12/2012 3:09:21 PM. For personal use only. Not approved for distribution. Copyright © 2012 National Comprehensive Cancer Network, Inc., All Rights Reserved.
Version 2.2012, 11/15/11 © National Comprehensive Cancer Network, Inc. 2011, All rights reserved. The NCCN Guidelines® and this illustration may not be reproduced in any form without the express written permission of NCCN®. REF-2
NCCN Guidelines IndexSenior Adult Oncology TOC
Discussion
NCCN Guidelines Version 2.2012 Senior Adult Oncolo gy
16. Extermann M, Hurria A. Comprehensive geriatric assessment for older patients with cancer. J Clin Oncol 2007;25:1824-1831. Available at: http://www.ncbi.nlm.nih.gov/pubmed/17488980.
17. Pal SK, Katheria V, Hurria A. Evaluating the older patient with cancer: understanding frailty and the geriatric assessment. CA Cancer J Clin 2010;60:120-132. Available at: http://www.ncbi.nlm.nih.gov/pubmed/20173172.
18. Rodin MB, Mohile SG. A practical approach to geriatric assessment in oncology. J Clin Oncol 2007;25:1936-1944. Available at: http://www.ncbi.nlm.nih.gov/pubmed/17488994.
19. Balducci L, Extermann M. Management of cancer in the older person: a practical approach. Oncologist 2000;5:224-237. Available at: http://www.ncbi.nlm.nih.gov/pubmed/10884501.
20. Ingram SS, Seo PH, Martell RE, et al. Comprehensive assessment of the elderly cancer patient: the feasibility of self-report methodology. J Clin Oncol 2002;20:770-775. Available at: http://www.ncbi.nlm.nih.gov/pubmed/11821460.
21. Repetto L, Fratino L, Audisio RA, et al. Comprehensive geriatric assessment adds information to Eastern Cooperative Oncology Group performance status in elderly cancer patients: an Italian Group for Geriatric Oncology Study. J Clin Oncol 2002;20:494-502. Available at: http://www.ncbi.nlm.nih.gov/pubmed/11786579.
22. Maione P, Perrone F, Gallo C, et al. Pretreatment quality of life and functional status assessment significantly predict survival of elderly patients with advanced non-small-cell lung cancer receiving chemotherapy: a prognostic analysis of the multicenter Italian lung cancer in the elderly study. J Clin Oncol 2005;23:6865-6872. Available at: http://www.ncbi.nlm.nih.gov/pubmed/16192578.
23. Koroukian SM, Xu F, Bakaki PM, et al. Comorbidities, functional limitations, and geriatric syndromes in relation to treatment and survival patterns among elders with colorectal cancer. J Gerontol A Biol Sci
Med Sci 2010;65:322-329. Available at: http://www.ncbi.nlm.nih.gov/pubmed/20018824.
24. Winkelmann N, Petersen I, Kiehntopf M, et al. Results of comprehensive geriatric assessment effect survival in patients with malignant lymphoma. J Cancer Res Clin Oncol 2011;137:733-738. Available at: http://www.ncbi.nlm.nih.gov/pubmed/20602238.
25. Clough-Gorr KM, Thwin SS, Stuck AE, Silliman RA. Examining five- and ten-year survival in older women with breast cancer using cancer-specific geriatric assessment. Eur J Cancer 2011. Available at: http://www.ncbi.nlm.nih.gov/pubmed/21741826.
26. Caillet P, Canoui-Poitrine F, Vouriot J, et al. Comprehensive Geriatric Assessment in the Decision-Making Process in Elderly Patients With Cancer: ELCAPA Study. J Clin Oncol 2011;29:3636. Available at: http://www.ncbi.nlm.nih.gov/pubmed/21709194.
27. Hurria A, Gupta S, Zauderer M, et al. Developing a cancer-specific geriatric assessment: a feasibility study. Cancer 2005;104:1998-2005. Available at: http://www.ncbi.nlm.nih.gov/pubmed/16206252.
28. Hurria A, Mohile S, Lichtman S, et al. Geriatric assessment of older adults with cancer: Baseline data from a 500 patient multicenter study [abstract]. J Clin Oncol 2009;27 (Suppl 15):Abstract 9546. Available at: http://meeting.ascopubs.org/cgi/content/abstract/27/15S/9546.
29. Hurria A, Cirrincione CT, Muss HB, et al. Implementing a Geriatric Assessment in Cooperative Group Clinical Cancer Trials: CALGB 360401. J Clin Oncol 2011:1290-1296. Available at: http://www.ncbi.nlm.nih.gov/pubmed/21357782.
30. Overcash JA, Beckstead J, Extermann M, Cobb S. The abbreviated comprehensive geriatric assessment (aCGA): a retrospective analysis. Crit Rev Oncol Hematol 2005;54:129-136. Available at: http://www.ncbi.nlm.nih.gov/pubmed/15843095
Printed by Kelly Hayden on 10/12/2012 3:09:21 PM. For personal use only. Not approved for distribution. Copyright © 2012 National Comprehensive Cancer Network, Inc., All Rights Reserved.

Version 2.2012, 11/15/11 © National Comprehensive Cancer Network, Inc. 2011, All rights reserved. The NCCN Guidelines® and this illustration may not be reproduced in any form without the express written permission of NCCN®. REF-3
NCCN Guidelines IndexSenior Adult Oncology TOC
Discussion
NCCN Guidelines Version 2.2012 Senior Adult Oncolo gy
31. Overcash JA, Beckstead J, Moody L, et al. The abbreviated comprehensive geriatric assessment (aCGA) for use in the older cancer patient as a prescreen: scoring and interpretation. Crit Rev Oncol Hematol 2006;59:205-210. Available at: http://www.ncbi.nlm.nih.gov/pubmed/16904902.
32. Katz S, Ford AB, Moskowitz RW, et al. Studies of Illness in the Aged. The Index of Adl: A Standardized Measure of Biological and Psychosocial Function. JAMA 1963;185:914-919. Available at: http://www.ncbi.nlm.nih.gov/pubmed/14044222.
33. Lawton MP. Scales to measure competence in everyday activities. Psychopharmacol Bull 1988;24:609-614. Available at: http://www.ncbi.nlm.nih.gov/pubmed/3074322.
34. Freyer G, Geay JF, Touzet S, et al. Comprehensive geriatric assessment predicts tolerance to chemotherapy and survival in elderly patients with advanced ovarian carcinoma: a GINECO study. Ann Oncol 2005;16:1795-1800. Available at: http://www.ncbi.nlm.nih.gov/pubmed/16093275.
35. Lachs MS, Feinstein AR, Cooney LM, et al. A simple procedure for general screening for functional disability in elderly patients. Ann Intern Med 1990;112:699-706. Available at: http://www.ncbi.nlm.nih.gov/pubmed/2334082.
36. Saliba D, Elliott M, Rubenstein LZ, et al. The Vulnerable Elders Survey: a tool for identifying vulnerable older people in the community. J Am Geriatr Soc 2001;49:1691-1699. Available at: http://www.ncbi.nlm.nih.gov/pubmed/11844005.
37. Min L, Yoon W, Mariano J, et al. The vulnerable elders-13 survey predicts 5-year functional decline and mortality outcomes in older ambulatory care patients. J Am Geriatr Soc 2009;57:2070-2076. Available at: http://www.ncbi.nlm.nih.gov/pubmed/19793154.
38. Luciani A, Ascione G, Bertuzzi C, et al. Detecting disabilities in older patients with cancer: comparison between comprehensive
geriatric assessment and vulnerable elders survey-13. J Clin Oncol 2010;28:2046-2050. Available at: http://www.ncbi.nlm.nih.gov/pubmed/20308657.
39. Cohen HJ, Harris T, Pieper CF. Coagulation and activation of inflammatory pathways in the development of functional decline and mortality in the elderly. Am J Med 2003;114:180-187. Available at: http://www.ncbi.nlm.nih.gov/pubmed/12637131.
40. Taaffe DR, Harris TB, Ferrucci L, et al. Cross-sectional and prospective relationships of interleukin-6 and C-reactive protein with physical performance in elderly persons: MacArthur studies of successful aging. J Gerontol A Biol Sci Med Sci 2000;55:M709-715. Available at: http://www.ncbi.nlm.nih.gov/pubmed/11129392.
41. Wilson CJ, Cohen HJ, Pieper CF. Cross-linked fibrin degradation products (D-dimer), plasma cytokines, and cognitive decline in community-dwelling elderly persons. J Am Geriatr Soc 2003;51:1374-1381. Available at: http://www.ncbi.nlm.nih.gov/pubmed/14511156.
42. Extermann M. Interaction between comorbidity and cancer. Cancer Control 2007;14:13-22. Available at: http://www.ncbi.nlm.nih.gov/pubmed/17242667.
43. Pal SK, Hurria A. Impact of age, sex, and comorbidity on cancer therapy and disease progression. J Clin Oncol 2010;28:4086-4093. Available at: http://www.ncbi.nlm.nih.gov/pubmed/20644100.
44. Nanda A, Chen MH, Braccioforte MH, et al. Hormonal therapy use for prostate cancer and mortality in men with coronary artery disease-induced congestive heart failure or myocardial infarction. JAMA 2009;302:866-873. Available at: http://www.ncbi.nlm.nih.gov/pubmed/19706860.
45. Meyerhardt JA, Catalano PJ, Haller DG, et al. Impact of diabetes mellitus on outcomes in patients with colon cancer. J Clin Oncol
Printed by Kelly Hayden on 10/12/2012 3:09:21 PM. For personal use only. Not approved for distribution. Copyright © 2012 National Comprehensive Cancer Network, Inc., All Rights Reserved.

Version 2.2012, 11/15/11 © National Comprehensive Cancer Network, Inc. 2011, All rights reserved. The NCCN Guidelines® and this illustration may not be reproduced in any form without the express written permission of NCCN®. REF-4
NCCN Guidelines IndexSenior Adult Oncology TOC
Discussion
NCCN Guidelines Version 2.2012 Senior Adult Oncolo gy
2003;21:433-440. Available at: http://www.ncbi.nlm.nih.gov/pubmed/12560431.
46. Srokowski TP, Fang S, Hortobagyi GN, Giordano SH. Impact of diabetes mellitus on complications and outcomes of adjuvant chemotherapy in older patients with breast cancer. J Clin Oncol 2009;27:2170-2176. Available at: http://www.ncbi.nlm.nih.gov/pubmed/19307509.
47. Piccirillo JF, Tierney RM, Costas I, et al. Prognostic importance of comorbidity in a hospital-based cancer registry. JAMA 2004;291:2441-2447. Available at: http://www.ncbi.nlm.nih.gov/pubmed/15161894.
48. Charlson ME, Pompei P, Ales KL, MacKenzie CR. A new method of classifying prognostic comorbidity in longitudinal studies: development and validation. J Chronic Dis 1987;40:373-383. Available at: http://www.ncbi.nlm.nih.gov/pubmed/3558716.
49. Linn BS, Linn MW, Gurel L. Cumulative illness rating scale. J Am Geriatr Soc 1968;16:622-626. Available at: http://www.ncbi.nlm.nih.gov/pubmed/5646906.
50. Fillenbaum GG, Smyer MA. The development, validity, and reliability of the OARS multidimensional functional assessment questionnaire. J Gerontol 1981;36:428-434. Available at: http://www.ncbi.nlm.nih.gov/pubmed/7252074.
51. Breccia M, Latagliata R, Stagno F, et al. Charlson comorbidity index and adult comorbidity evaluation-27 scores might predict treatment compliance and development of pleural effusions in elderly patients with chronic myeloid leukemia treated with second-line dasatinib. Haematologica 2011;96:1457-1461. Available at: http://www.ncbi.nlm.nih.gov/pubmed/21685471.
52. Sanabria A, Carvalho AL, Melo RL, et al. Predictive factors for complications in elderly patients who underwent head and neck
oncologic surgery. Head Neck 2008;30:170-177. Available at: http://www.ncbi.nlm.nih.gov/pubmed/17694555.
53. Frasci G, Lorusso V, Panza N, et al. Gemcitabine plus vinorelbine versus vinorelbine alone in elderly patients with advanced non-small-cell lung cancer. J Clin Oncol 2000;18:2529-2536. Available at: http://www.ncbi.nlm.nih.gov/pubmed/10893283.
54. Hurria A, Brogan K, Panageas KS, et al. Patterns of toxicity in older patients with breast cancer receiving adjuvant chemotherapy. Breast Cancer Res Treat 2005;92:151-156. Available at: http://www.ncbi.nlm.nih.gov/pubmed/15986124.
55. Fader AN, von Gruenigen V, Gibbons H, et al. Improved tolerance of primary chemotherapy with reduced-dose carboplatin and paclitaxel in elderly ovarian cancer patients. Gynecol Oncol 2008;109:33-38. Available at: http://www.ncbi.nlm.nih.gov/pubmed/18261784.
56. Gronberg BH, Sundstrom S, Kaasa S, et al. Influence of comorbidity on survival, toxicity and health-related quality of life in patients with advanced non-small-cell lung cancer receiving platinum-doublet chemotherapy. Eur J Cancer 2010;46:2225-2234. Available at: http://www.ncbi.nlm.nih.gov/pubmed/20471248.
57. Ngeow J, Leong SS, Gao F, et al. Impact of comorbidities on clinical outcomes in non-small cell lung cancer patients who are elderly and/or have poor performance status. Crit Rev Oncol Hematol 2010;76:53-60. Available at: http://www.ncbi.nlm.nih.gov/pubmed/19939700.
58. Sanabria A, Carvalho AL, Vartanian JG, et al. Comorbidity is a prognostic factor in elderly patients with head and neck cancer. Ann Surg Oncol 2007;14:1449-1457. Available at: http://www.ncbi.nlm.nih.gov/pubmed/17235712.
59. Tam-McDevitt J. Polypharmacy, aging, and cancer. Oncology (Williston Park) 2008;22:1052-1055, discussion 1055, 1058, 1060. Available at: http://www.ncbi.nlm.nih.gov/pubmed/18777955.
Printed by Kelly Hayden on 10/12/2012 3:09:21 PM. For personal use only. Not approved for distribution. Copyright © 2012 National Comprehensive Cancer Network, Inc., All Rights Reserved.

Version 2.2012, 11/15/11 © National Comprehensive Cancer Network, Inc. 2011, All rights reserved. The NCCN Guidelines® and this illustration may not be reproduced in any form without the express written permission of NCCN®. REF-5
NCCN Guidelines IndexSenior Adult Oncology TOC
Discussion
NCCN Guidelines Version 2.2012 Senior Adult Oncolo gy
60. Maggiore RJ, Gross CP, Hurria A. Polypharmacy in older adults with cancer. Oncologist 2010;15:507-522. Available at: http://www.ncbi.nlm.nih.gov/pubmed/20418534.
61. Sokol KC, Knudsen JF, Li MM. Polypharmacy in older oncology patients and the need for an interdisciplinary approach to side-effect management. J Clin Pharm Ther 2007;32:169-175. Available at: http://www.ncbi.nlm.nih.gov/pubmed/17381667.
62. Puts MT, Costa-Lima B, Monette J, et al. Medication problems in older, newly diagnosed cancer patients in Canada: How common are they? A prospective pilot study. Drugs Aging 2009;26:519-536. Available at: http://www.ncbi.nlm.nih.gov/pubmed/19591526.
63. Lees J, Chan A. Polypharmacy in elderly patients with cancer: clinical implications and management. Lancet Oncol 2011. Available at: http://www.ncbi.nlm.nih.gov/pubmed/21741307.
64. Riechelmann RP, Saad ED. A systematic review on drug interactions in oncology. Cancer Invest 2006;24:704-712. Available at: http://www.ncbi.nlm.nih.gov/pubmed/17118781.
65. Riechelmann RP, Tannock IF, Wang L, et al. Potential drug interactions and duplicate prescriptions among cancer patients. J Natl Cancer Inst 2007;99:592-600. Available at: http://www.ncbi.nlm.nih.gov/pubmed/17440160.
66. Riechelmann RP, Zimmermann C, Chin SN, et al. Potential drug interactions in cancer patients receiving supportive care exclusively. J Pain Symptom Manage 2008;35:535-543. Available at: http://www.ncbi.nlm.nih.gov/pubmed/18243638.
67. Popa M, Wallace K, Brunello A, Extermann M. The impact of polypharmacy on toxicity from chemotherapy in elderly patients: Focus on cytochrome P-450 inhibition and protein binding effects [abstract]. J Clin Oncol 2008;26(Suppl 15):Abstract 9505. Available at: http://meeting.ascopubs.org/cgi/content/abstract/26/15_suppl/9505.
68. Steinman MA, Seth Landefeld C, Rosenthal GE, et al. Polypharmacy and Prescribing Quality in Older People. Journal of the American Geriatrics Society 2006;54:1516-1523. Available at: http://dx.doi.org/10.1111/j.1532-5415.2006.00889.x.
69. Currow DC, Stevenson JP, Abernethy AP, et al. Prescribing in palliative care as death approaches. J Am Geriatr Soc 2007;55:590-595. Available at: http://www.ncbi.nlm.nih.gov/pubmed/17397439.
70. Maggiore RJ, Gross CP, Hardt M, et al. Polypharmacy, potentially inappropriate medications, and chemotherapy-related adverse events among older adults with cancer. J Clin Oncol 2011;29:e19501. Available at: http://meeting.ascopubs.org/cgi/content/abstract/29/15_suppl/e19501.
71. Beers MH. Explicit criteria for determining potentially inappropriate medication use by the elderly. An update. Arch Intern Med 1997;157:1531-1536. Available at: http://www.ncbi.nlm.nih.gov/pubmed/9236554.
72. Fick DM, Cooper JW, Wade WE, et al. Updating the Beers criteria for potentially inappropriate medication use in older adults: results of a US consensus panel of experts. Arch Intern Med 2003;163:2716-2724. Available at: http://www.ncbi.nlm.nih.gov/pubmed/14662625.
73. Flood KL, Carroll MB, Le CV, Brown CJ. Polypharmacy in hospitalized older adult cancer patients: experience from a prospective, observational study of an oncology-acute care for elders unit. Am J Geriatr Pharmacother 2009;7:151-158. Available at: http://www.ncbi.nlm.nih.gov/pubmed/19616183.
74. Lichtman SM, Boparai MK. Geriatric medication management: Evaluation of pharmacist interventions and potentially inappropriate medication (PIM) use in older (>=65 years) cancer patients. J Clin Oncol 2009;27:9507. Available at: http://meeting.ascopubs.org/cgi/content/abstract/27/15S/9507.
Printed by Kelly Hayden on 10/12/2012 3:09:21 PM. For personal use only. Not approved for distribution. Copyright © 2012 National Comprehensive Cancer Network, Inc., All Rights Reserved.

Version 2.2012, 11/15/11 © National Comprehensive Cancer Network, Inc. 2011, All rights reserved. The NCCN Guidelines® and this illustration may not be reproduced in any form without the express written permission of NCCN®. REF-6
NCCN Guidelines IndexSenior Adult Oncology TOC
Discussion
NCCN Guidelines Version 2.2012 Senior Adult Oncolo gy
75. Hanlon JT, Schmader KE, Samsa GP, et al. A method for assessing drug therapy appropriateness. J Clin Epidemiol 1992;45:1045-1051. Available at: http://www.ncbi.nlm.nih.gov/pubmed/1474400.
76. Samsa GP, Hanlon JT, Schmader KE, et al. A summated score for the medication appropriateness index: development and assessment of clinimetric properties including content validity. J Clin Epidemiol 1994;47:891-896. Available at: http://www.ncbi.nlm.nih.gov/pubmed/7730892.
77. Schmader K, Hanlon JT, Weinberger M, et al. Appropriateness of medication prescribing in ambulatory elderly patients. J Am Geriatr Soc 1994;42:1241-1247. Available at: http://www.ncbi.nlm.nih.gov/pubmed/7983285.
78. Kassam R, Martin LG, Farris KB. Reliability of a modified medication appropriateness index in community pharmacies. Ann Pharmacother 2003;37:40-46. Available at: http://www.ncbi.nlm.nih.gov/pubmed/12503931.
79. Hanlon JT, Artz MB, Pieper CF, et al. Inappropriate medication use among frail elderly inpatients. Ann Pharmacother 2004;38:9-14. Available at: http://www.ncbi.nlm.nih.gov/pubmed/14742785.
80. Gallagher P, Baeyens JP, Topinkova E, et al. Inter-rater reliability of STOPP (Screening Tool of Older Persons' Prescriptions) and START (Screening Tool to Alert doctors to Right Treatment) criteria amongst physicians in six European countries. Age Ageing 2009;38:603-606. Available at: http://www.ncbi.nlm.nih.gov/pubmed/19435757.
81. Gallagher P, O'Mahony D. STOPP (Screening Tool of Older Persons' potentially inappropriate Prescriptions): application to acutely ill elderly patients and comparison with Beers' criteria. Age Ageing 2008;37:673-679. Available at: http://www.ncbi.nlm.nih.gov/pubmed/18829684.
82. Barry PJ, Gallagher P, Ryan C, O'Mahony D. START (screening tool to alert doctors to the right treatment)--an evidence-based screening tool to detect prescribing omissions in elderly patients. Age Ageing 2007;36:632-638. Available at: http://www.ncbi.nlm.nih.gov/pubmed/17881418.
83. Gallagher PF, O'Connor MN, O'Mahony D. Prevention of potentially inappropriate prescribing for elderly patients: a randomized controlled trial using STOPP/START criteria. Clin Pharmacol Ther 2011;89:845-854. Available at: http://www.ncbi.nlm.nih.gov/pubmed/21508941.
84. Guigoz Y, Lauque S, Vellas BJ. Identifying the elderly at risk for malnutrition. The Mini Nutritional Assessment. Clin Geriatr Med 2002;18:737-757. Available at: http://www.ncbi.nlm.nih.gov/pubmed/12608501.
85. Vellas B, Guigoz Y, Garry PJ, et al. The Mini Nutritional Assessment (MNA) and its use in grading the nutritional state of elderly patients. Nutrition 1999;15:116-122. Available at: http://www.ncbi.nlm.nih.gov/pubmed/9990575.
86. Rubenstein LZ, Harker JO, Salva A, et al. Screening for undernutrition in geriatric practice: developing the short-form mini-nutritional assessment (MNA-SF). J Gerontol A Biol Sci Med Sci 2001;56:M366-372. Available at: http://www.ncbi.nlm.nih.gov/pubmed/11382797.
87. Bjorkman MP, Sorva AJ, Risteli J, Tilvis RS. Low parathyroid hormone levels in bedridden geriatric patients with vitamin D deficiency. J Am Geriatr Soc 2009;57:1045-1050. Available at: http://www.ncbi.nlm.nih.gov/pubmed/19473453.
88. Stilley CS, Bender CM, Dunbar-Jacob J, et al. The impact of cognitive function on medication management: three studies. Health Psychol 2010;29:50-55. Available at: http://www.ncbi.nlm.nih.gov/pubmed/20063935.
Printed by Kelly Hayden on 10/12/2012 3:09:21 PM. For personal use only. Not approved for distribution. Copyright © 2012 National Comprehensive Cancer Network, Inc., All Rights Reserved.
Version 2.2012, 11/15/11 © National Comprehensive Cancer Network, Inc. 2011, All rights reserved. The NCCN Guidelines® and this illustration may not be reproduced in any form without the express written permission of NCCN®. REF-7
NCCN Guidelines IndexSenior Adult Oncology TOC
Discussion
NCCN Guidelines Version 2.2012 Senior Adult Oncolo gy
89. Extermann M. Older patients, cognitive impairment, and cancer: an increasingly frequent triad. J Natl Compr Canc Netw 2005;3:593-596. Available at: http://www.ncbi.nlm.nih.gov/pubmed/16038648.
90. Chew ML, Mulsant BH, Pollock BG, et al. Anticholinergic activity of 107 medications commonly used by older adults. J Am Geriatr Soc 2008;56:1333-1341. Available at: http://www.ncbi.nlm.nih.gov/pubmed/18510583.
91. Hilmer SN, Mager DE, Simonsick EM, et al. A drug burden index to define the functional burden of medications in older people. Arch Intern Med 2007;167:781-787. Available at: http://www.ncbi.nlm.nih.gov/pubmed/17452540.
92. Naeim A, Reuben D. Geriatric syndromes and assessment in older cancer patients. Oncology (Williston Park) 2001;15:1567-1577. Available at: http://www.ncbi.nlm.nih.gov/pubmed/11780701.
93. Seeman TE, Kaplan GA, Knudsen L, et al. Social network ties and mortality among the elderly in the Alameda County Study. Am J Epidemiol 1987;126:714-723. Available at: http://www.ncbi.nlm.nih.gov/pubmed/3631060.
94. Tomaka J, Thompson S, Palacios R. The relation of social isolation, loneliness, and social support to disease outcomes among the elderly. J Aging Health 2006;18:359-384. Available at: http://www.ncbi.nlm.nih.gov/pubmed/16648391.
95. Kroenke CH, Kubzansky LD, Schernhammer ES, et al. Social networks, social support, and survival after breast cancer diagnosis. J Clin Oncol 2006;24:1105-1111. Available at: http://www.ncbi.nlm.nih.gov/pubmed/16505430.
96. Flood KL, Carroll MB, Le CV, et al. Geriatric syndromes in elderly patients admitted to an oncology-acute care for elders unit. J Clin Oncol 2006;24:2298-2303. Available at: http://www.ncbi.nlm.nih.gov/pubmed/16710027.
97. Mohile SG, Fan L, Reeve E, et al. Association of cancer with geriatric syndromes in older Medicare beneficiaries. J Clin Oncol 2011;29:1458-1464. Available at: http://www.ncbi.nlm.nih.gov/pubmed/21402608.
98. Gupta SK, Lamont EB. Patterns of presentation, diagnosis, and treatment in older patients with colon cancer and comorbid dementia. J Am Geriatr Soc 2004;52:1681-1687. Available at: http://www.ncbi.nlm.nih.gov/pubmed/15450045.
99. Raji MA, Kuo YF, Freeman JL, Goodwin JS. Effect of a dementia diagnosis on survival of older patients after a diagnosis of breast, colon, or prostate cancer: implications for cancer care. Arch Intern Med 2008;168:2033-2040. Available at: http://www.ncbi.nlm.nih.gov/pubmed/18852406.
100. Crum RM, Anthony JC, Bassett SS, Folstein MF. Population-based norms for the Mini-Mental State Examination by age and educational level. JAMA 1993;269:2386-2391. Available at: http://www.ncbi.nlm.nih.gov/pubmed/8479064.
101. Tombaugh TN, McIntyre NJ. The mini-mental state examination: a comprehensive review. J Am Geriatr Soc 1992;40:922-935. Available at: http://www.ncbi.nlm.nih.gov/pubmed/1512391.
102. Kawas C, Karagiozis H, Resau L, et al. Reliability of the Blessed Telephone Information-Memory-Concentration Test. J Geriatr Psychiatry Neurol 1995;8:238-242. Available at: http://www.ncbi.nlm.nih.gov/pubmed/8561839.
103. Nasreddine ZS, Phillips NA, Bedirian V, et al. The Montreal Cognitive Assessment, MoCA: a brief screening tool for mild cognitive impairment. J Am Geriatr Soc 2005;53:695-699. Available at: http://www.ncbi.nlm.nih.gov/pubmed/15817019.
104. Olson RA, Chhanabhai T, McKenzie M. Feasibility study of the Montreal Cognitive Assessment (MoCA) in patients with brain
Printed by Kelly Hayden on 10/12/2012 3:09:21 PM. For personal use only. Not approved for distribution. Copyright © 2012 National Comprehensive Cancer Network, Inc., All Rights Reserved.

Version 2.2012, 11/15/11 © National Comprehensive Cancer Network, Inc. 2011, All rights reserved. The NCCN Guidelines® and this illustration may not be reproduced in any form without the express written permission of NCCN®. REF-8
NCCN Guidelines IndexSenior Adult Oncology TOC
Discussion
NCCN Guidelines Version 2.2012 Senior Adult Oncolo gy
metastases. Support Care Cancer 2008;16:1273-1278. Available at: http://www.ncbi.nlm.nih.gov/pubmed/18335256.
105. Olson RA, Iverson GL, Carolan H, et al. Prospective comparison of two cognitive screening tests: diagnostic accuracy and correlation with community integration and quality of life. J Neurooncol 2011. Available at: http://www.ncbi.nlm.nih.gov/pubmed/21520004.
106. Schneider LS, Dagerman KS, Insel P. Risk of death with atypical antipsychotic drug treatment for dementia: meta-analysis of randomized placebo-controlled trials. JAMA 2005;294:1934-1943. Available at: http://www.ncbi.nlm.nih.gov/pubmed/16234500.
107. Kales HC, Valenstein M, Kim HM, et al. Mortality risk in patients with dementia treated with antipsychotics versus other psychiatric medications. Am J Psychiatry 2007;164:1568-1576; quiz 1623. Available at: http://www.ncbi.nlm.nih.gov/pubmed/17898349.
108. Rochon PA, Normand SL, Gomes T, et al. Antipsychotic therapy and short-term serious events in older adults with dementia. Arch Intern Med 2008;168:1090-1096. Available at: http://www.ncbi.nlm.nih.gov/pubmed/18504337.
109. Bush SH, Bruera E. The assessment and management of delirium in cancer patients. Oncologist 2009;14:1039-1049. Available at: http://www.ncbi.nlm.nih.gov/pubmed/19808772.
110. Inouye SK. Delirium in older persons. N Engl J Med 2006;354:1157-1165. Available at: http://www.ncbi.nlm.nih.gov/pubmed/16540616.
111. Inouye SK, van Dyck CH, Alessi CA, et al. Clarifying confusion: the confusion assessment method. A new method for detection of delirium. Ann Intern Med 1990;113:941-948. Available at: http://www.ncbi.nlm.nih.gov/pubmed/2240918.
112. Wei LA, Fearing MA, Sternberg EJ, Inouye SK. The Confusion Assessment Method: a systematic review of current usage. J Am
Geriatr Soc 2008;56:823-830. Available at: http://www.ncbi.nlm.nih.gov/pubmed/18384586.
113. Lawlor PG, Nekolaichuk C, Gagnon B, et al. Clinical utility, factor analysis, and further validation of the memorial delirium assessment scale in patients with advanced cancer: Assessing delirium in advanced cancer. Cancer 2000;88:2859-2867. Available at: http://www.ncbi.nlm.nih.gov/pubmed/10870073.
114. Gaudreau JD, Gagnon P, Harel F, et al. Fast, systematic, and continuous delirium assessment in hospitalized patients: the nursing delirium screening scale. J Pain Symptom Manage 2005;29:368-375. Available at: http://www.ncbi.nlm.nih.gov/pubmed/15857740.
115. Gaudreau JD, Gagnon P, Harel F, et al. Psychoactive medications and risk of delirium in hospitalized cancer patients. J Clin Oncol 2005;23:6712-6718. Available at: http://www.ncbi.nlm.nih.gov/pubmed/16170179.
116. Gaudreau JD, Gagnon P, Roy MA, et al. Opioid medications and longitudinal risk of delirium in hospitalized cancer patients. Cancer 2007;109:2365-2373. Available at: http://www.ncbi.nlm.nih.gov/pubmed/17469164.
117. Yesavage JA, Brink TL, Rose TL, et al. Development and validation of a geriatric depression screening scale: a preliminary report. J Psychiatr Res 1982;17:37-49. Available at: http://www.ncbi.nlm.nih.gov/pubmed/7183759.
118. D'Ath P, Katona P, Mullan E, et al. Screening, detection and management of depression in elderly primary care attenders. I: The acceptability and performance of the 15 item Geriatric Depression Scale (GDS15) and the development of short versions. Fam Pract 1994;11:260-266. Available at: http://www.ncbi.nlm.nih.gov/pubmed/7843514.
119. Jongenelis K, Pot AM, Eisses AMH, et al. Diagnostic accuracy of the original 30-item and shortened versions of the Geriatric Depression
Printed by Kelly Hayden on 10/12/2012 3:09:21 PM. For personal use only. Not approved for distribution. Copyright © 2012 National Comprehensive Cancer Network, Inc., All Rights Reserved.
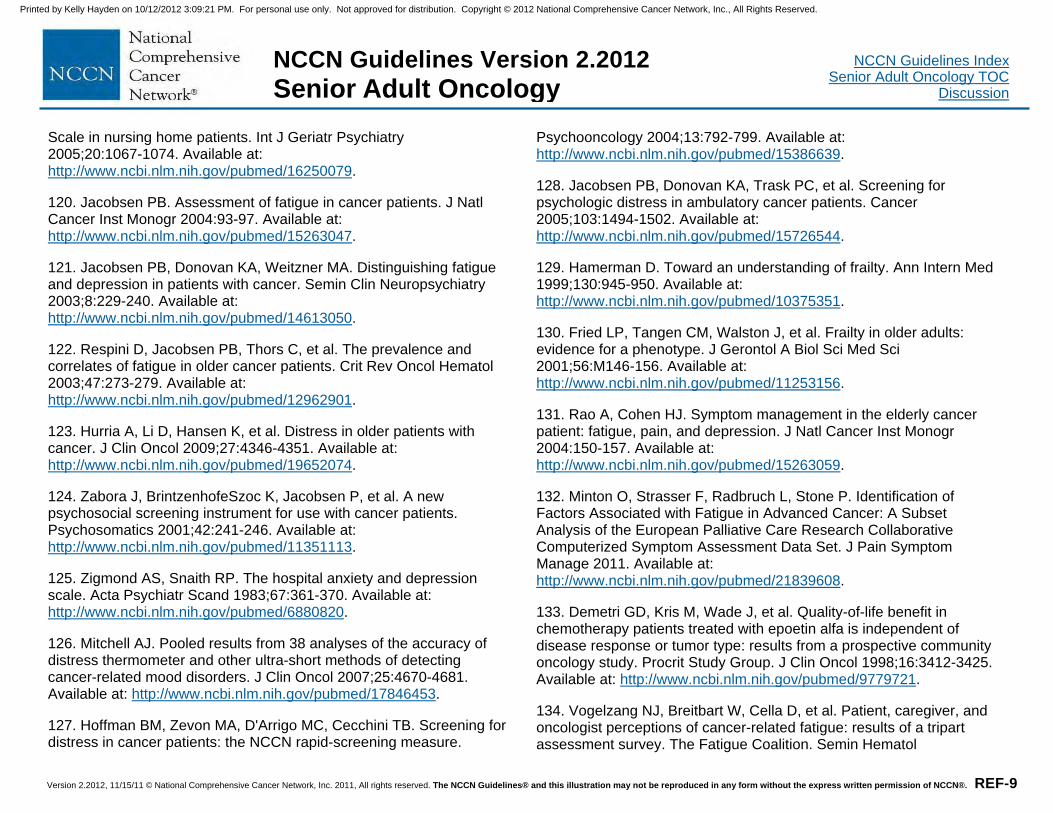
Version 2.2012, 11/15/11 © National Comprehensive Cancer Network, Inc. 2011, All rights reserved. The NCCN Guidelines® and this illustration may not be reproduced in any form without the express written permission of NCCN®. REF-9
NCCN Guidelines IndexSenior Adult Oncology TOC
Discussion
NCCN Guidelines Version 2.2012 Senior Adult Oncolo gy
Scale in nursing home patients. Int J Geriatr Psychiatry 2005;20:1067-1074. Available at: http://www.ncbi.nlm.nih.gov/pubmed/16250079.
120. Jacobsen PB. Assessment of fatigue in cancer patients. J Natl Cancer Inst Monogr 2004:93-97. Available at: http://www.ncbi.nlm.nih.gov/pubmed/15263047.
121. Jacobsen PB, Donovan KA, Weitzner MA. Distinguishing fatigue and depression in patients with cancer. Semin Clin Neuropsychiatry 2003;8:229-240. Available at: http://www.ncbi.nlm.nih.gov/pubmed/14613050.
122. Respini D, Jacobsen PB, Thors C, et al. The prevalence and correlates of fatigue in older cancer patients. Crit Rev Oncol Hematol 2003;47:273-279. Available at: http://www.ncbi.nlm.nih.gov/pubmed/12962901.
123. Hurria A, Li D, Hansen K, et al. Distress in older patients with cancer. J Clin Oncol 2009;27:4346-4351. Available at: http://www.ncbi.nlm.nih.gov/pubmed/19652074.
124. Zabora J, BrintzenhofeSzoc K, Jacobsen P, et al. A new psychosocial screening instrument for use with cancer patients. Psychosomatics 2001;42:241-246. Available at: http://www.ncbi.nlm.nih.gov/pubmed/11351113.
125. Zigmond AS, Snaith RP. The hospital anxiety and depression scale. Acta Psychiatr Scand 1983;67:361-370. Available at: http://www.ncbi.nlm.nih.gov/pubmed/6880820.
126. Mitchell AJ. Pooled results from 38 analyses of the accuracy of distress thermometer and other ultra-short methods of detecting cancer-related mood disorders. J Clin Oncol 2007;25:4670-4681. Available at: http://www.ncbi.nlm.nih.gov/pubmed/17846453.
127. Hoffman BM, Zevon MA, D'Arrigo MC, Cecchini TB. Screening for distress in cancer patients: the NCCN rapid-screening measure.
Psychooncology 2004;13:792-799. Available at: http://www.ncbi.nlm.nih.gov/pubmed/15386639.
128. Jacobsen PB, Donovan KA, Trask PC, et al. Screening for psychologic distress in ambulatory cancer patients. Cancer 2005;103:1494-1502. Available at: http://www.ncbi.nlm.nih.gov/pubmed/15726544.
129. Hamerman D. Toward an understanding of frailty. Ann Intern Med 1999;130:945-950. Available at: http://www.ncbi.nlm.nih.gov/pubmed/10375351.
130. Fried LP, Tangen CM, Walston J, et al. Frailty in older adults: evidence for a phenotype. J Gerontol A Biol Sci Med Sci 2001;56:M146-156. Available at: http://www.ncbi.nlm.nih.gov/pubmed/11253156.
131. Rao A, Cohen HJ. Symptom management in the elderly cancer patient: fatigue, pain, and depression. J Natl Cancer Inst Monogr 2004:150-157. Available at: http://www.ncbi.nlm.nih.gov/pubmed/15263059.
132. Minton O, Strasser F, Radbruch L, Stone P. Identification of Factors Associated with Fatigue in Advanced Cancer: A Subset Analysis of the European Palliative Care Research Collaborative Computerized Symptom Assessment Data Set. J Pain Symptom Manage 2011. Available at: http://www.ncbi.nlm.nih.gov/pubmed/21839608.
133. Demetri GD, Kris M, Wade J, et al. Quality-of-life benefit in chemotherapy patients treated with epoetin alfa is independent of disease response or tumor type: results from a prospective community oncology study. Procrit Study Group. J Clin Oncol 1998;16:3412-3425. Available at: http://www.ncbi.nlm.nih.gov/pubmed/9779721.
134. Vogelzang NJ, Breitbart W, Cella D, et al. Patient, caregiver, and oncologist perceptions of cancer-related fatigue: results of a tripart assessment survey. The Fatigue Coalition. Semin Hematol
Printed by Kelly Hayden on 10/12/2012 3:09:21 PM. For personal use only. Not approved for distribution. Copyright © 2012 National Comprehensive Cancer Network, Inc., All Rights Reserved.

Version 2.2012, 11/15/11 © National Comprehensive Cancer Network, Inc. 2011, All rights reserved. The NCCN Guidelines® and this illustration may not be reproduced in any form without the express written permission of NCCN®. REF-10
NCCN Guidelines IndexSenior Adult Oncology TOC
Discussion
NCCN Guidelines Version 2.2012 Senior Adult Oncolo gy
1997;34:4-12. Available at: http://www.ncbi.nlm.nih.gov/pubmed/9253778.
135. Berger AM, Farr L. The influence of daytime inactivity and nighttime restlessness on cancer-related fatigue. Oncol Nurs Forum 1999;26:1663-1671. Available at: http://www.ncbi.nlm.nih.gov/pubmed/10573683.
136. Hardy SE, Studenski SA. Fatigue and function over 3 years among older adults. J Gerontol A Biol Sci Med Sci 2008;63:1389-1392. Available at: http://www.ncbi.nlm.nih.gov/pubmed/19126853.
137. Luciani A, Jacobsen PB, Extermann M, et al. Fatigue and functional dependence in older cancer patients. Am J Clin Oncol 2008;31:424-430. Available at: http://www.ncbi.nlm.nih.gov/pubmed/18838877.
138. Rao SS. Prevention of falls in older patients. Am Fam Physician 2005;72:81-88. Available at: http://www.ncbi.nlm.nih.gov/pubmed/16035686.
139. Stone C, Lawlor PG, Nolan B, Kenny RA. A Prospective Study of the Incidence of Falls in Patients with Advanced Cancer. J Pain Symptom Manage 2011. Available at: http://www.ncbi.nlm.nih.gov/pubmed/21444189.
140. Chang JT, Morton SC, Rubenstein LZ, et al. Interventions for the prevention of falls in older adults: systematic review and meta-analysis of randomised clinical trials. BMJ 2004;328:680-680. Available at: http://www.ncbi.nlm.nih.gov/pubmed/15031239.
141. Summary of the Updated American Geriatrics Society/British Geriatrics Society clinical practice guideline for prevention of falls in older persons. J Am Geriatr Soc 2011;59:148-157. Available at: http://www.ncbi.nlm.nih.gov/pubmed/21226685.
142. Balducci L. Bone complications of cancer treatment in the elderly. Oncology (Williston Park) 2010;24:741-747. Available at: http://www.ncbi.nlm.nih.gov/pubmed/20718254.
143. Gralow JR, Biermann JS, Farooki A, et al. NCCN Task Force Report: Bone Health in Cancer Care. J Natl Compr Canc Netw 2009;7 Suppl 3:S1-S32; quiz S33-S35. Available at: http://www.ncbi.nlm.nih.gov/pubmed/19555589.
144. Sessums LL, Zembrzuska H, Jackson JL. Does this patient have medical decision-making capacity? JAMA 2011;306:420-427. Available at: http://www.ncbi.nlm.nih.gov/pubmed/21791691.
145. Harrington SE, Smith TJ. The role of chemotherapy at the end of life: "when is enough, enough?". JAMA 2008;299:2667-2678. Available at: http://www.ncbi.nlm.nih.gov/pubmed/18544726.
146. Balducci L, Extermann M. Cancer and aging. An evolving panorama. Hematol Oncol Clin North Am 2000;14:1-16. Available at: http://www.ncbi.nlm.nih.gov/pubmed/10680068.
147. Monfardini S, Ferrucci L, Fratino L, et al. Validation of a multidimensional evaluation scale for use in elderly cancer patients. Cancer 1996;77:395-401. Available at: http://www.ncbi.nlm.nih.gov/pubmed/8625250.
148. Ramesh H, Pope D, Gennari R, Audisio R. Optimising surgical management of elderly cancer patients. World J Surg Oncol 2005;3:17. Available at: http://www.ncbi.nlm.nih.gov/pubmed/15788092.
149. Audisio RA, Bozzetti F, Gennari R, et al. The surgical management of elderly cancer patients; recommendations of the SIOG surgical task force. Eur J Cancer 2004;40:926-938. Available at: http://www.ncbi.nlm.nih.gov/pubmed/15093567.
150. Audisio RA, Ramesh H, Longo WE, et al. Preoperative assessment of surgical risk in oncogeriatric patients. Oncologist
Printed by Kelly Hayden on 10/12/2012 3:09:21 PM. For personal use only. Not approved for distribution. Copyright © 2012 National Comprehensive Cancer Network, Inc., All Rights Reserved.

Version 2.2012, 11/15/11 © National Comprehensive Cancer Network, Inc. 2011, All rights reserved. The NCCN Guidelines® and this illustration may not be reproduced in any form without the express written permission of NCCN®. REF-11
NCCN Guidelines IndexSenior Adult Oncology TOC
Discussion
NCCN Guidelines Version 2.2012 Senior Adult Oncolo gy
2005;10:262-268. Available at: http://www.ncbi.nlm.nih.gov/pubmed/15821246.
151. Pope D, Ramesh H, Gennari R, et al. Pre-operative assessment of cancer in the elderly (PACE): a comprehensive assessment of underlying characteristics of elderly cancer patients prior to elective surgery. Surg Oncol 2006;15:189-197. Available at: http://www.ncbi.nlm.nih.gov/pubmed/17531743.
152. Audisio RA, Pope D, Ramesh HS, et al. Shall we operate? Preoperative assessment in elderly cancer patients (PACE) can help. A SIOG surgical task force prospective study. Crit Rev Oncol Hematol 2008;65:156-163. Available at: http://www.ncbi.nlm.nih.gov/pubmed/18082416.
153. Zachariah B, Balducci L. Radiation therapy of the older patient. Hematol Oncol Clin North Am 2000;14:131-167. Available at: http://www.ncbi.nlm.nih.gov/pubmed/10680076.
154. Donato V, Valeriani M, Zurlo A. Short course radiation therapy for elderly cancer patients. Evidences from the literature review. Crit Rev Oncol Hematol 2003;45:305-311. Available at: http://www.ncbi.nlm.nih.gov/pubmed/12633841.
155. Mitsuhashi N, Hayakawa K, Yamakawa M, et al. Cancer in patients aged 90 years or older: radiation therapy. Radiology 1999;211:829-833. Available at: http://www.ncbi.nlm.nih.gov/pubmed/10352612.
156. Wasil T, Lichtman SM, Gupta V, Rush S. Radiation therapy in cancer patients 80 years of age and older. Am J Clin Oncol 2000;23:526-530. Available at: http://www.ncbi.nlm.nih.gov/pubmed/11039517.
157. Zachariah B, Balducci L, Venkattaramanabalaji GV, et al. Radiotherapy for cancer patients aged 80 and older: a study of effectiveness and side effects. Int J Radiat Oncol Biol Phys
1997;39:1125-1129. Available at: http://www.ncbi.nlm.nih.gov/pubmed/9392554.
158. Gelman RS, Taylor SG. Cyclophosphamide, methotrexate, and 5-fluorouracil chemotherapy in women more than 65 years old with advanced breast cancer: the elimination of age trends in toxicity by using doses based on creatinine clearance. J Clin Oncol 1984;2:1404-1413. Available at: http://www.ncbi.nlm.nih.gov/pubmed/6512583.
159. Ibrahim NK, Frye DK, Buzdar AU, et al. Doxorubicin-based chemotherapy in elderly patients with metastatic breast cancer. Tolerance and outcome. Arch Intern Med 1996;156:882-888. Available at: http://www.ncbi.nlm.nih.gov/pubmed/8774207.
160. Giovanazzi-Bannon S, Rademaker A, Lai G, Benson AB. Treatment tolerance of elderly cancer patients entered onto phase II clinical trials: an Illinois Cancer Center study. J Clin Oncol 1994;12:2447-2452. Available at: http://www.ncbi.nlm.nih.gov/pubmed/7964962.
161. Newcomb PA, Carbone PP. Cancer treatment and age: patient perspectives. J Natl Cancer Inst 1993;85:1580-1584. Available at: http://www.ncbi.nlm.nih.gov/pubmed/8411231.
162. Lichtman SM, Wildiers H, Chatelut E, et al. International Society of Geriatric Oncology Chemotherapy Taskforce: evaluation of chemotherapy in older patients--an analysis of the medical literature. J Clin Oncol 2007;25:1832-1843. Available at: http://www.ncbi.nlm.nih.gov/pubmed/17488981.
163. Balducci L, Corcoran MB. Antineoplastic chemotherapy of the older cancer patient. Hematol Oncol Clin North Am 2000;14:193-212. Available at: http://www.ncbi.nlm.nih.gov/pubmed/10680078.
164. Hurria A, Lichtman SM. Clinical pharmacology of cancer therapies in older adults. Br J Cancer 2008;98:517-522. Available at: http://www.ncbi.nlm.nih.gov/pubmed/18256586.
Printed by Kelly Hayden on 10/12/2012 3:09:21 PM. For personal use only. Not approved for distribution. Copyright © 2012 National Comprehensive Cancer Network, Inc., All Rights Reserved.

Version 2.2012, 11/15/11 © National Comprehensive Cancer Network, Inc. 2011, All rights reserved. The NCCN Guidelines® and this illustration may not be reproduced in any form without the express written permission of NCCN®. REF-12
NCCN Guidelines IndexSenior Adult Oncology TOC
Discussion
NCCN Guidelines Version 2.2012 Senior Adult Oncolo gy
165. Extermann M, Bonetti M, Sledge GW, et al. MAX2--a convenient index to estimate the average per patient risk for chemotherapy toxicity; validation in ECOG trials. Eur J Cancer 2004;40:1193-1198. Available at: http://www.ncbi.nlm.nih.gov/pubmed/15110883.
166. Shayne M, Crawford J, Dale DC, et al. Predictors of reduced dose intensity in patients with early-stage breast cancer receiving adjuvant chemotherapy. Breast Cancer Res Treat 2006;100:255-262. Available at: http://www.ncbi.nlm.nih.gov/pubmed/16705366.
167. Extermann M, Boler I, Reich R, et al. The Chemotherapy Risk Assessment Scale for High-Age Patients (CRASH) score: Design and validation [abstract]. J Clin Oncol 2010;28 (Suppl 15):Abstract 9000. Available at: http://meeting.ascopubs.org/cgi/content/abstract/28/15_suppl/9000.
168. Hurria A, Togawa K, Mohile SG, et al. Predicting Chemotherapy Toxicity in Older Adults With Cancer: A Prospective Multicenter Study. Journal of Clinical Oncology 2011;29:3457-3465. Available at: http://www.ncbi.nlm.nih.gov/pubmed/21810685.
169. Jelliffe RW, Jelliffe SM. Estimation of creatinine clearance from changing serum-creatinine levels. Lancet 1971;2:710. Available at: http://www.ncbi.nlm.nih.gov/pubmed/4105743.
170. Maloney KW, Kagan SH. Adherence and oral agents with older patients. Semin Oncol Nurs 2011;27:154-160. Available at: http://www.ncbi.nlm.nih.gov/pubmed/21514484.
171. Demissie S, Silliman RA, Lash TL. Adjuvant tamoxifen: predictors of use, side effects, and discontinuation in older women. J Clin Oncol 2001;19:322-328. Available at: http://www.ncbi.nlm.nih.gov/pubmed/11208822.
172. Fink AK, Gurwitz J, Rakowski W, et al. Patient beliefs and tamoxifen discontinuance in older women with estrogen receptor--positive breast cancer. J Clin Oncol 2004;22:3309-3315. Available at: http://www.ncbi.nlm.nih.gov/pubmed/15310774.
173. Owusu C, Buist DS, Field TS, et al. Predictors of tamoxifen discontinuation among older women with estrogen receptor-positive breast cancer. J Clin Oncol 2008;26:549-555. Available at: http://www.ncbi.nlm.nih.gov/pubmed/18071188.
174. Partridge AH, Archer L, Kornblith AB, et al. Adherence and persistence with oral adjuvant chemotherapy in older women with early-stage breast cancer in CALGB 49907: adherence companion study 60104. J Clin Oncol 2010;28:2418-2422. Available at: http://www.ncbi.nlm.nih.gov/pubmed/20368559.
175. Hershman DL, Shao T, Kushi LH, et al. Early discontinuation and non-adherence to adjuvant hormonal therapy are associated with increased mortality in women with breast cancer. Breast Cancer Res Treat 2011;126:529-537. Available at: http://www.ncbi.nlm.nih.gov/pubmed/20803066.
176. Floyd JD, Nguyen DT, Lobins RL, et al. Cardiotoxicity of cancer therapy. J Clin Oncol 2005;23:7685-7696. Available at: http://www.ncbi.nlm.nih.gov/pubmed/16234530.
177. Hershman DL, McBride RB, Eisenberger A, et al. Doxorubicin, cardiac risk factors, and cardiac toxicity in elderly patients with diffuse B-cell non-Hodgkin's lymphoma. J Clin Oncol 2008;26:3159-3165. Available at: http://www.ncbi.nlm.nih.gov/pubmed/18591554.
178. Aapro M, Bernard-Marty C, Brain EGC, et al. Anthracycline cardiotoxicity in the elderly cancer patient: a SIOG expert position paper. Annals of Oncology 2011;22:257-267. Available at: http://www.ncbi.nlm.nih.gov/pubmed/20956616.
179. Suter TM, Procter M, van Veldhuisen DJ, et al. Trastuzumab-associated cardiac adverse effects in the herceptin adjuvant trial. J Clin Oncol 2007;25:3859-3865. Available at: http://www.ncbi.nlm.nih.gov/pubmed/17646669.
180. Tan-Chiu E, Yothers G, Romond E, et al. Assessment of cardiac dysfunction in a randomized trial comparing doxorubicin and
Printed by Kelly Hayden on 10/12/2012 3:09:21 PM. For personal use only. Not approved for distribution. Copyright © 2012 National Comprehensive Cancer Network, Inc., All Rights Reserved.

Version 2.2012, 11/15/11 © National Comprehensive Cancer Network, Inc. 2011, All rights reserved. The NCCN Guidelines® and this illustration may not be reproduced in any form without the express written permission of NCCN®. REF-13
NCCN Guidelines IndexSenior Adult Oncology TOC
Discussion
NCCN Guidelines Version 2.2012 Senior Adult Oncolo gy
cyclophosphamide followed by paclitaxel, with or without trastuzumab as adjuvant therapy in node-positive, human epidermal growth factor receptor 2-overexpressing breast cancer: NSABP B-31. J Clin Oncol 2005;23:7811-7819. Available at: http://www.ncbi.nlm.nih.gov/pubmed/16258083.
181. Perez EA, Suman VJ, Davidson NE, et al. Cardiac safety analysis of doxorubicin and cyclophosphamide followed by paclitaxel with or without trastuzumab in the North Central Cancer Treatment Group N9831 adjuvant breast cancer trial. J Clin Oncol 2008;26:1231-1238. Available at: http://www.ncbi.nlm.nih.gov/pubmed/18250349.
182. Procter M, Suter TM, de Azambuja E, et al. Longer-term assessment of trastuzumab-related cardiac adverse events in the Herceptin Adjuvant (HERA) trial. J Clin Oncol 2010;28:3422-3428. Available at: http://www.ncbi.nlm.nih.gov/pubmed/20530280.
183. Russell SD, Blackwell KL, Lawrence J, et al. Independent adjudication of symptomatic heart failure with the use of doxorubicin and cyclophosphamide followed by trastuzumab adjuvant therapy: a combined review of cardiac data from the National Surgical Adjuvant breast and Bowel Project B-31 and the North Central Cancer Treatment Group N9831 clinical trials. J Clin Oncol 2010;28:3416-3421. Available at: http://www.ncbi.nlm.nih.gov/pubmed/20530275.
184. Serrano C, Cortes J, De Mattos-Arruda L, et al. Trastuzumab-related cardiotoxicity in the elderly: a role for cardiovascular risk factors. Ann Oncol 2011. Available at: http://www.ncbi.nlm.nih.gov/pubmed/21828361.
185. Slamon D, Eiermann W, Robert N, et al. Phase III randomized trial comparing doxorubicin and cyclophosphamide followed by docetaxel (AC→T) with doxorubicin and cyclophosphamide followed by docetaxel and trastuzumab (AC→TH) with docetaxel, carboplatin and trastuzumab (TCH) in her2neu positive early breast cancer patients: BCIRG 006 study [abstract]. Presented at the 2009 SABCS. Abstract 62.
186. Valero V, Forbes J, Pegram MD, et al. Multicenter phase III randomized trial comparing docetaxel and trastuzumab with docetaxel, carboplatin, and trastuzumab as first-line chemotherapy for patients with HER2-gene-amplified metastatic breast cancer (BCIRG 007 study): two highly active therapeutic regimens. J Clin Oncol 2011;29:149-156. Available at: http://www.ncbi.nlm.nih.gov/pubmed/21115860.
187. Jones S, Holmes FA, O'Shaughnessy J, et al. Docetaxel With Cyclophosphamide Is Associated With an Overall Survival Benefit Compared With Doxorubicin and Cyclophosphamide: 7-Year Follow-Up of US Oncology Research Trial 9735. J Clin Oncol 2009;27:1177-1183. Available at: http://www.ncbi.nlm.nih.gov/pubmed/19204201.
188. Swain SM, Whaley FS, Gerber MC, et al. Delayed administration of dexrazoxane provides cardioprotection for patients with advanced breast cancer treated with doxorubicin-containing therapy. J Clin Oncol 1997;15:1333-1340. Available at: http://www.ncbi.nlm.nih.gov/pubmed/9193324.
189. Swain SM, Whaley FS, Gerber MC, et al. Cardioprotection with dexrazoxane for doxorubicin-containing therapy in advanced breast cancer. J Clin Oncol 1997;15:1318-1332. Available at: http://www.ncbi.nlm.nih.gov/pubmed/9193323.
190. Marty M, Espie M, Llombart A, et al. Multicenter randomized phase III study of the cardioprotective effect of dexrazoxane (Cardioxane) in advanced/metastatic breast cancer patients treated with anthracycline-based chemotherapy. Ann Oncol 2006;17:614-622. Available at: http://www.ncbi.nlm.nih.gov/pubmed/16423847.
191. Launay-Vacher V, Chatelut E, Lichtman SM, et al. Renal insufficiency in elderly cancer patients: International Society of Geriatric Oncology clinical practice recommendations. Ann Oncol 2007;18:1314-1321. Available at: http://www.ncbi.nlm.nih.gov/pubmed/17631561.
Printed by Kelly Hayden on 10/12/2012 3:09:21 PM. For personal use only. Not approved for distribution. Copyright © 2012 National Comprehensive Cancer Network, Inc., All Rights Reserved.

Version 2.2012, 11/15/11 © National Comprehensive Cancer Network, Inc. 2011, All rights reserved. The NCCN Guidelines® and this illustration may not be reproduced in any form without the express written permission of NCCN®. REF-14
NCCN Guidelines IndexSenior Adult Oncology TOC
Discussion
NCCN Guidelines Version 2.2012 Senior Adult Oncolo gy
192. Sul JK, Deangelis LM. Neurologic complications of cancer chemotherapy. Semin Oncol 2006;33:324-332. Available at: http://www.ncbi.nlm.nih.gov/pubmed/16769421.
193. Cheson BD, Vena DA, Foss FM, Sorensen JM. Neurotoxicity of purine analogs: a review. J Clin Oncol 1994;12:2216-2228. Available at: http://www.ncbi.nlm.nih.gov/pubmed/7931492.
194. Smith GA, Damon LE, Rugo HS, et al. High-dose cytarabine dose modification reduces the incidence of neurotoxicity in patients with renal insufficiency. J Clin Oncol 1997;15:833-839. Available at: http://www.ncbi.nlm.nih.gov/pubmed/9053511.
195. Rubin EH, Andersen JW, Berg DT, et al. Risk factors for high-dose cytarabine neurotoxicity: an analysis of a cancer and leukemia group B trial in patients with acute myeloid leukemia. J Clin Oncol 1992;10:948-953. Available at: http://www.ncbi.nlm.nih.gov/pubmed/1588374.
196. Balducci L, Repetto L. Increased risk of myelotoxicity in elderly patients with non-Hodgkin lymphoma. Cancer 2004;100:6-11. Available at: http://www.ncbi.nlm.nih.gov/pubmed/14692018.
197. Begg CB, Carbone PP. Clinical trials and drug toxicity in the elderly. The experience of the Eastern Cooperative Oncology Group. Cancer 1983;52:1986-1992. Available at: http://www.ncbi.nlm.nih.gov/pubmed/6354419.
198. Crivellari D. Results of adjuvant treatments in breast cancer patients over 70 years old: the IBCSG experience. International Breast Cancer Study Group. Tumori 2002;88:S81-82. Available at: http://www.ncbi.nlm.nih.gov/pubmed/11989935.
199. Langer CJ, Manola J, Bernardo P, et al. Cisplatin-based therapy for elderly patients with advanced non-small-cell lung cancer: implications of Eastern Cooperative Oncology Group 5592, a randomized trial. J Natl Cancer Inst 2002;94:173-181. Available at: http://www.ncbi.nlm.nih.gov/pubmed/11830607.
200. Rocha Lima CM, Herndon JE, 2nd, Kosty M, et al. Therapy choices among older patients with lung carcinoma: an evaluation of two trials of the Cancer and Leukemia Group B. Cancer 2002;94:181-187. Available at: http://www.ncbi.nlm.nih.gov/pubmed/11815975.
201. Neubauer M, Schwartz J, Caracandas J, et al. Results of a phase II study of weekly paclitaxel plus carboplatin in patients with extensive small-cell lung cancer with Eastern Cooperative Oncology Group Performance Status of 2, or age > or = 70 years. J Clin Oncol 2004;22:1872-1877. Available at: http://www.ncbi.nlm.nih.gov/pubmed/15143079.
202. Doorduijn JK, van der Holt B, van Imhoff GW, et al. CHOP compared with CHOP plus granulocyte colony-stimulating factor in elderly patients with aggressive non-Hodgkin's lymphoma. J Clin Oncol 2003;21:3041-3050. Available at: http://www.ncbi.nlm.nih.gov/pubmed/12915593.
203. Osby E, Hagberg H, Kvaloy S, et al. CHOP is superior to CNOP in elderly patients with aggressive lymphoma while outcome is unaffected by filgrastim treatment: results of a Nordic Lymphoma Group randomized trial. Blood 2003;101:3840-3848. Available at: http://www.ncbi.nlm.nih.gov/pubmed/12531794.
204. Zinzani PL, Pavone E, Storti S, et al. Randomized trial with or without granulocyte colony-stimulating factor as adjunct to induction VNCOP-B treatment of elderly high-grade non-Hodgkin's lymphoma. Blood 1997;89:3974-3979. Available at: http://www.ncbi.nlm.nih.gov/pubmed/9166835.
205. Armitage JO, Potter JF. Aggressive chemotherapy for diffuse histiocytic lymphoma in the elderly: increased complications with advancing age. J Am Geriatr Soc 1984;32:269-273. Available at: http://www.ncbi.nlm.nih.gov/pubmed/6368652.
206. Bastion Y, Blay JY, Divine M, et al. Elderly patients with aggressive non-Hodgkin's lymphoma: disease presentation, response to treatment, and survival--a Groupe d'Etude des Lymphomes de
Printed by Kelly Hayden on 10/12/2012 3:09:21 PM. For personal use only. Not approved for distribution. Copyright © 2012 National Comprehensive Cancer Network, Inc., All Rights Reserved.

Version 2.2012, 11/15/11 © National Comprehensive Cancer Network, Inc. 2011, All rights reserved. The NCCN Guidelines® and this illustration may not be reproduced in any form without the express written permission of NCCN®. REF-15
NCCN Guidelines IndexSenior Adult Oncology TOC
Discussion
NCCN Guidelines Version 2.2012 Senior Adult Oncolo gy
l'Adulte study on 453 patients older than 69 years. J Clin Oncol 1997;15:2945-2953. Available at: http://www.ncbi.nlm.nih.gov/pubmed/9256139.
207. Bertini M, Freilone R, Vitolo U, et al. The treatment of elderly patients with aggressive non-Hodgkin's lymphomas: feasibility and efficacy of an intensive multidrug regimen. Leuk Lymphoma 1996;22:483-493. Available at: http://www.ncbi.nlm.nih.gov/pubmed/8882962.
208. Gomez H, Mas L, Casanova L, et al. Elderly patients with aggressive non-Hodgkin's lymphoma treated with CHOP chemotherapy plus granulocyte-macrophage colony-stimulating factor: identification of two age subgroups with differing hematologic toxicity. J Clin Oncol 1998;16:2352-2358. Available at: http://www.ncbi.nlm.nih.gov/pubmed/9667250.
209. O'Reilly SE, Connors JM, Howdle S, et al. In search of an optimal regimen for elderly patients with advanced-stage diffuse large-cell lymphoma: results of a phase II study of P/DOCE chemotherapy. J Clin Oncol 1993;11:2250-2257. Available at: http://www.ncbi.nlm.nih.gov/pubmed/8229141.
210. Sonneveld P, de Ridder M, van der Lelie H, et al. Comparison of doxorubicin and mitoxantrone in the treatment of elderly patients with advanced diffuse non-Hodgkin's lymphoma using CHOP versus CNOP chemotherapy. J Clin Oncol 1995;13:2530-2539. Available at: http://www.ncbi.nlm.nih.gov/pubmed/7595704.
211. Amadori S, Suciu S, Jehn U, et al. Use of glycosylated recombinant human G-CSF (lenograstim) during and/or after induction chemotherapy in patients 61 years of age and older with acute myeloid leukemia: final results of AML-13, a randomized phase-3 study. Blood 2005;106:27-34. Available at: http://www.ncbi.nlm.nih.gov/pubmed/15761020.
212. Lowenberg B, van Putten W, Theobald M, et al. Effect of priming with granulocyte colony-stimulating factor on the outcome of
chemotherapy for acute myeloid leukemia. N Engl J Med 2003;349:743-752. Available at: http://www.ncbi.nlm.nih.gov/pubmed/12930926.
213. Lyman GH, Kuderer NM, Djulbegovic B. Prophylactic granulocyte colony-stimulating factor in patients receiving dose-intensive cancer chemotherapy: a meta-analysis. Am J Med 2002;112:406-411. Available at: http://www.ncbi.nlm.nih.gov/pubmed/11904116.
214. Relling MV, Boyett JM, Blanco JG, et al. Granulocyte colony-stimulating factor and the risk of secondary myeloid malignancy after etoposide treatment. Blood 2003;101:3862-3867. Available at: http://www.ncbi.nlm.nih.gov/pubmed/12531808.
215. Patt DA, Duan Z, Fang S, et al. Acute myeloid leukemia after adjuvant breast cancer therapy in older women: understanding risk. J Clin Oncol 2007;25:3871-3876. Available at: http://www.ncbi.nlm.nih.gov/pubmed/17664457.
216. Lyman GH, Kuderer N, Agboola O, Balducci L. Evidence-based use of colony-stimulating factors in elderly cancer patients. Cancer Control 2003;10:487-499. Available at: http://www.ncbi.nlm.nih.gov/pubmed/14652525.
217. Repetto L, Biganzoli L, Koehne CH, et al. EORTC Cancer in the Elderly Task Force guidelines for the use of colony-stimulating factors in elderly patients with cancer. Eur J Cancer 2003;39:2264-2272. Available at: http://www.ncbi.nlm.nih.gov/pubmed/14556916.
218. Pierelli L, Perillo A, Greggi S, et al. Erythropoietin addition to granulocyte colony-stimulating factor abrogates life-threatening neutropenia and increases peripheral-blood progenitor-cell mobilization after epirubicin, paclitaxel, and cisplatin combination chemotherapy: results of a randomized comparison. J Clin Oncol 1999;17:1288-1296. Available at: http://www.ncbi.nlm.nih.gov/pubmed/10561191.
219. Metivier F, Marchais SJ, Guerin AP, et al. Pathophysiology of anaemia: focus on the heart and blood vessels. Nephrol Dial Transplant
Printed by Kelly Hayden on 10/12/2012 3:09:21 PM. For personal use only. Not approved for distribution. Copyright © 2012 National Comprehensive Cancer Network, Inc., All Rights Reserved.
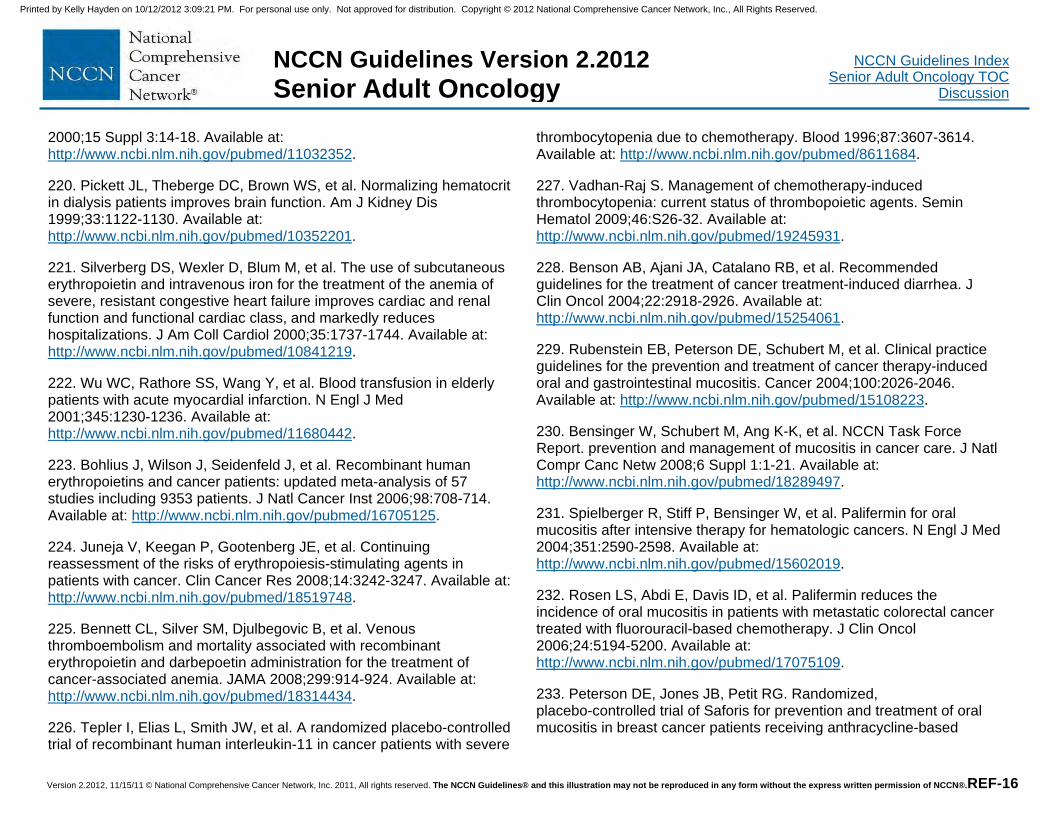
Version 2.2012, 11/15/11 © National Comprehensive Cancer Network, Inc. 2011, All rights reserved. The NCCN Guidelines® and this illustration may not be reproduced in any form without the express written permission of NCCN®. REF-16
NCCN Guidelines IndexSenior Adult Oncology TOC
Discussion
NCCN Guidelines Version 2.2012 Senior Adult Oncolo gy
2000;15 Suppl 3:14-18. Available at: http://www.ncbi.nlm.nih.gov/pubmed/11032352.
220. Pickett JL, Theberge DC, Brown WS, et al. Normalizing hematocrit in dialysis patients improves brain function. Am J Kidney Dis 1999;33:1122-1130. Available at: http://www.ncbi.nlm.nih.gov/pubmed/10352201.
221. Silverberg DS, Wexler D, Blum M, et al. The use of subcutaneous erythropoietin and intravenous iron for the treatment of the anemia of severe, resistant congestive heart failure improves cardiac and renal function and functional cardiac class, and markedly reduces hospitalizations. J Am Coll Cardiol 2000;35:1737-1744. Available at: http://www.ncbi.nlm.nih.gov/pubmed/10841219.
222. Wu WC, Rathore SS, Wang Y, et al. Blood transfusion in elderly patients with acute myocardial infarction. N Engl J Med 2001;345:1230-1236. Available at: http://www.ncbi.nlm.nih.gov/pubmed/11680442.
223. Bohlius J, Wilson J, Seidenfeld J, et al. Recombinant human erythropoietins and cancer patients: updated meta-analysis of 57 studies including 9353 patients. J Natl Cancer Inst 2006;98:708-714. Available at: http://www.ncbi.nlm.nih.gov/pubmed/16705125.
224. Juneja V, Keegan P, Gootenberg JE, et al. Continuing reassessment of the risks of erythropoiesis-stimulating agents in patients with cancer. Clin Cancer Res 2008;14:3242-3247. Available at: http://www.ncbi.nlm.nih.gov/pubmed/18519748.
225. Bennett CL, Silver SM, Djulbegovic B, et al. Venous thromboembolism and mortality associated with recombinant erythropoietin and darbepoetin administration for the treatment of cancer-associated anemia. JAMA 2008;299:914-924. Available at: http://www.ncbi.nlm.nih.gov/pubmed/18314434.
226. Tepler I, Elias L, Smith JW, et al. A randomized placebo-controlled trial of recombinant human interleukin-11 in cancer patients with severe
thrombocytopenia due to chemotherapy. Blood 1996;87:3607-3614. Available at: http://www.ncbi.nlm.nih.gov/pubmed/8611684.
227. Vadhan-Raj S. Management of chemotherapy-induced thrombocytopenia: current status of thrombopoietic agents. Semin Hematol 2009;46:S26-32. Available at: http://www.ncbi.nlm.nih.gov/pubmed/19245931.
228. Benson AB, Ajani JA, Catalano RB, et al. Recommended guidelines for the treatment of cancer treatment-induced diarrhea. J Clin Oncol 2004;22:2918-2926. Available at: http://www.ncbi.nlm.nih.gov/pubmed/15254061.
229. Rubenstein EB, Peterson DE, Schubert M, et al. Clinical practice guidelines for the prevention and treatment of cancer therapy-induced oral and gastrointestinal mucositis. Cancer 2004;100:2026-2046. Available at: http://www.ncbi.nlm.nih.gov/pubmed/15108223.
230. Bensinger W, Schubert M, Ang K-K, et al. NCCN Task Force Report. prevention and management of mucositis in cancer care. J Natl Compr Canc Netw 2008;6 Suppl 1:1-21. Available at: http://www.ncbi.nlm.nih.gov/pubmed/18289497.
231. Spielberger R, Stiff P, Bensinger W, et al. Palifermin for oral mucositis after intensive therapy for hematologic cancers. N Engl J Med 2004;351:2590-2598. Available at: http://www.ncbi.nlm.nih.gov/pubmed/15602019.
232. Rosen LS, Abdi E, Davis ID, et al. Palifermin reduces the incidence of oral mucositis in patients with metastatic colorectal cancer treated with fluorouracil-based chemotherapy. J Clin Oncol 2006;24:5194-5200. Available at: http://www.ncbi.nlm.nih.gov/pubmed/17075109.
233. Peterson DE, Jones JB, Petit RG. Randomized, placebo-controlled trial of Saforis for prevention and treatment of oral mucositis in breast cancer patients receiving anthracycline-based
Printed by Kelly Hayden on 10/12/2012 3:09:21 PM. For personal use only. Not approved for distribution. Copyright © 2012 National Comprehensive Cancer Network, Inc., All Rights Reserved.

Version 2.2012, 11/15/11 © National Comprehensive Cancer Network, Inc. 2011, All rights reserved. The NCCN Guidelines® and this illustration may not be reproduced in any form without the express written permission of NCCN®. REF-17
NCCN Guidelines IndexSenior Adult Oncology TOC
Discussion
NCCN Guidelines Version 2.2012 Senior Adult Oncolo gy
chemotherapy. Cancer 2007;109:322-331. Available at: http://www.ncbi.nlm.nih.gov/pubmed/17154160.
234. Gonsalves W, Ganti AK. Targeted anti-cancer therapy in the elderly. Crit Rev Oncol Hematol 2011;78:227-242. Available at: http://www.ncbi.nlm.nih.gov/pubmed/20599391.
235. Sekeres MA. Treatment of older adults with acute myeloid leukemia: state of the art and current perspectives. Haematologica 2008;93:1769-1772. Available at: http://www.ncbi.nlm.nih.gov/pubmed/19050066.
236. Joudi FN, Smith BJ, O'Donnell MA, Konety BR. The impact of age on the response of patients with superficial bladder cancer to intravesical immunotherapy. J Urol 2006;175:1634-1639. Available at: http://www.ncbi.nlm.nih.gov/pubmed/16600718.
237. Herr HW. Age and outcome of superficial bladder cancer treated with bacille Calmette-Guerin therapy. Urology 2007;70:65-68. Available at: http://www.ncbi.nlm.nih.gov/pubmed/17656210.
238. Chamie K, Hu B, Devere White RW, Ellison LM. Cystectomy in the elderly: does the survival benefit in younger patients translate to the octogenarians? BJU Int 2008;102:284-290. Available at: http://www.ncbi.nlm.nih.gov/pubmed/18410437.
239. Grossman HB, Natale RB, Tangen CM, et al. Neoadjuvant chemotherapy plus cystectomy compared with cystectomy alone for locally advanced bladder cancer. N Engl J Med 2003;349:859-866. Available at: http://www.ncbi.nlm.nih.gov/pubmed/12944571.
240. Diab SG, Elledge RM, Clark GM. Tumor characteristics and clinical outcome of elderly women with breast cancer. J Natl Cancer Inst 2000;92:550-556. Available at: http://www.ncbi.nlm.nih.gov/pubmed/10749910.
241. Eppenberger-Castori S, Moore DH, Jr., Thor AD, et al. Age-associated biomarker profiles of human breast cancer. Int J
Biochem Cell Biol 2002;34:1318-1330. Available at: http://www.ncbi.nlm.nih.gov/pubmed/12200028.
242. Bouchardy C, Rapiti E, Fioretta G, et al. Undertreatment strongly decreases prognosis of breast cancer in elderly women. J Clin Oncol 2003;21:3580-3587. Available at: http://www.ncbi.nlm.nih.gov/pubmed/12913099.
243. Yood MU, Owusu C, Buist DSM, et al. Mortality impact of less-than-standard therapy in older breast cancer patients. J Am Coll Surg 2008;206:66-75. Available at: http://www.ncbi.nlm.nih.gov/pubmed/18155570.
244. Schonberg MA, Marcantonio ER, Li D, et al. Breast cancer among the oldest old: tumor characteristics, treatment choices, and survival. J Clin Oncol 2010;28:2038-2045. Available at: http://www.ncbi.nlm.nih.gov/pubmed/20308658.
245. Giuliano AE, Hunt KK, Ballman KV, et al. Axillary dissection vs no axillary dissection in women with invasive breast cancer and sentinel node metastasis: a randomized clinical trial. JAMA 2011;305:569-575. Available at: http://www.ncbi.nlm.nih.gov/pubmed/21304082.
246. Rudenstam CM, Zahrieh D, Forbes JF, et al. Randomized trial comparing axillary clearance versus no axillary clearance in older patients with breast cancer: first results of International Breast Cancer Study Group Trial 10-93. J Clin Oncol 2006;24:337-344. Available at: http://www.ncbi.nlm.nih.gov/pubmed/16344321.
247. Martelli G, Miceli R, Daidone MG, et al. Axillary dissection versus no axillary dissection in elderly patients with breast cancer and no palpable axillary nodes: results after 15 years of follow-up. Ann Surg Oncol 2011;18:125-133. Available at: http://www.ncbi.nlm.nih.gov/pubmed/20652755.
248. Hughes KS, Schnaper LA, Berry D, et al. Lumpectomy plus tamoxifen with or without irradiation in women 70 years of age or older
Printed by Kelly Hayden on 10/12/2012 3:09:21 PM. For personal use only. Not approved for distribution. Copyright © 2012 National Comprehensive Cancer Network, Inc., All Rights Reserved.

Version 2.2012, 11/15/11 © National Comprehensive Cancer Network, Inc. 2011, All rights reserved. The NCCN Guidelines® and this illustration may not be reproduced in any form without the express written permission of NCCN®. REF-18
NCCN Guidelines IndexSenior Adult Oncology TOC
Discussion
NCCN Guidelines Version 2.2012 Senior Adult Oncolo gy
with early breast cancer. N Engl J Med 2004;351:971-977. Available at: http://www.ncbi.nlm.nih.gov/pubmed/15342805.
249. Hughes KS, Schnaper LA, Cirrincione C, et al. Lumpectomy plus tamoxifen with or without irradiation in women age 70 or older with early breast cancer [abstract]. J Clin Oncol 2010;28(Suppl 15):Abstract 507. Available at: http://meeting.ascopubs.org/cgi/content/abstract/28/15_suppl/507.
250. Muss HB, Woolf S, Berry D, et al. Adjuvant chemotherapy in older and younger women with lymph node-positive breast cancer. JAMA 2005;293:1073-1081. Available at: http://www.ncbi.nlm.nih.gov/pubmed/15741529.
251. Muss HB, Berry DA, Cirrincione CT, et al. Adjuvant chemotherapy in older women with early-stage breast cancer. N Engl J Med 2009;360:2055-2065. Available at: http://www.ncbi.nlm.nih.gov/pubmed/19439741.
252. Piccart-Gebhart MJ, Procter M, Leyland-Jones B, et al. Trastuzumab after adjuvant chemotherapy in HER2-positive breast cancer. N Engl J Med 2005;353:1659-1672. Available at: http://www.ncbi.nlm.nih.gov/pubmed/16236737.
253. Romond EH, Perez EA, Bryant J, et al. Trastuzumab plus adjuvant chemotherapy for operable HER2-positive breast cancer. N Engl J Med 2005;353:1673-1684. Available at: http://www.ncbi.nlm.nih.gov/pubmed/16236738.
254. Vuorinen V, Hinkka S, Farkkila M, Jaaskelainen J. Debulking or biopsy of malignant glioma in elderly people. A randomized study. Acta Neurochir 2003;145: 5-10. Available at: http://www.ncbi.nlm.nih.gov/pubmed/12545256.
255. Martinez R, Janka M, Soldner F, Behr R. Gross total resection of malignant glioma in elderly patients: implications in survival. Zentrabl Neurchir. 2007;68:176-181. Available at: http://www.ncbi.nlm.nih.gov/pubmed/17963194.
256. Scott J, Suh J, Elson P, et al. Aggressive treatment is appropriate for glioblastoma multiforme patients 70 years old or older:a retrospective review of 206 cases. Neuro-Oncol 2011;13:428-436. Available at: http://www.ncbi.nlm.nih.gov/pubmed/21363881.
257. Roa W, Brasher PM, Bauman G, et al. Abbreviated course of radiation therapy in older patients with glioblastoma multiforme: a prospective randomized trial. J Clin Oncol 2004;22:1583-1588. Available at: http://www.ncbi.nlm.nih.gov/pubmed/15051755.
258. Keime-Guibert F, Chinot O, Taillandier L, et al. Radiotherapy for glioblastoma in the elderly. N Engl J Med 2007;356:1527-1535. Available at: http://www.ncbi.nlm.nih.gov/pubmed/17429084.
259. Stupp R, Hegi M, Mason W, et al. Effects of radiotherapy with concomitant and adjuvant temozolomide versus radiotherapy alone on survival in glioblastoma in a randomized phase III study: 5-year analysis of the EORTC-NCIC trial. Lancet Oncol 2009;10:459-466. Available at: http://www.ncbi.nlm.nih.gov/pubmed/19269895.
260. Lanzetta G, Minniti G. Treatment of glioblastoma in elderly patients: an overview of current treatments and future perspective. Tumori 2010;96:650-658. Available at: http://www.ncbi.nlm.nih.gov/pubmed/21302607.
261. Nghiemphu PL, Liu W, Lee Y, et al. Bevacizumab and chemotherapy for recurrent glioblastoma: a single-institution experience. Neurology 2009;72:1217-1222. Available at: http://www.ncbi.nlm.nih.gov/pubmed/19349600.
262. Gavrilovic I, Hormigo A, Yahalom J, et al. Long term follow-up of high-dose methotrexate-based therapy with and without whole brain irradiation for newly diagnosed primary CNS lymphoma. J Clin Oncol 2006;24:4570-4574. Available at: http://www.ncbi.nlm.nih.gov/pubmed/17008697.
263. Ney DE, Reiner AS, Panageas KS, et al. Characteristics and outcomes of elderly patients with primary central nervous system
Printed by Kelly Hayden on 10/12/2012 3:09:21 PM. For personal use only. Not approved for distribution. Copyright © 2012 National Comprehensive Cancer Network, Inc., All Rights Reserved.

Version 2.2012, 11/15/11 © National Comprehensive Cancer Network, Inc. 2011, All rights reserved. The NCCN Guidelines® and this illustration may not be reproduced in any form without the express written permission of NCCN®. REF-19
NCCN Guidelines IndexSenior Adult Oncology TOC
Discussion
NCCN Guidelines Version 2.2012 Senior Adult Oncolo gy
lymphoma: the Memorial Sloan-Kettering Cancer Center experience. Cancer 2010;116:4605-4612. Available at: http://www.ncbi.nlm.nih.gov/pubmed/20572045.
264. Zhu J-J, Gerstner ER, Engler DA, et al. High-dose methotrexate for elderly patients with primary CNS lymphoma. Neuro Oncol 2009;11:211-215. Available at: http://www.ncbi.nlm.nih.gov/pubmed/18757775.
265. Schiffmann L, Ozcan S, Schwarz F, et al. Colorectal cancer in the elderly: surgical treatment and long-term survival. Int J Colorectal Dis 2008;23:601-610. Available at: http://www.ncbi.nlm.nih.gov/pubmed/18343931.
266. Devon KM, Vergara-Fernandez O, Victor JC, McLeod RS. Colorectal cancer surgery in elderly patients: presentation, treatment, and outcomes. Dis Colon Rectum 2009;52:1272-1277. Available at: http://www.ncbi.nlm.nih.gov/pubmed/19571704.
267. Ong ES, Alassas M, Dunn KB, Rajput A. Colorectal cancer surgery in the elderly: acceptable morbidity? Am J Surg 2008;195:344-348. Available at: http://www.ncbi.nlm.nih.gov/pubmed/18222410.
268. Adam R, Frilling A, Elias D, et al. Liver resection of colorectal metastases in elderly patients. Br J Surg 2010;97:366-376. Available at: http://www.ncbi.nlm.nih.gov/pubmed/20101645.
269. Schrag D, Cramer LD, Bach PB, Begg CB. Age and adjuvant chemotherapy use after surgery for stage III colon cancer. J Natl Cancer Inst 2001;93:850-857. Available at: http://www.ncbi.nlm.nih.gov/pubmed/11390534.
270. Jackson McCleary NA, Meyerhardt J, Green E, et al. Impact of older age on the efficacy of newer adjuvant therapies in >12,500 patients (pts) with stage II/III colon cancer: Findings from the ACCENT Database. J Clin Oncol 2009;27:4010. Available at: http://meeting.ascopubs.org/cgi/content/abstract/27/15S/4010.
271. Folprecht G, Cunningham D, Ross P, et al. Efficacy of 5-fluorouracil-based chemotherapy in elderly patients with metastatic colorectal cancer: a pooled analysis of clinical trials. Ann Oncol 2004;15:1330-1338. Available at: http://www.ncbi.nlm.nih.gov/pubmed/15319237.
272. Seymour MT, Thompson LC, Wasan HS, et al. Chemotherapy options in elderly and frail patients with metastatic colorectal cancer (MRC FOCUS2): an open-label, randomised factorial trial. Lancet 2011;377:1749-1759. Available at: http://www.ncbi.nlm.nih.gov/pubmed/21570111.
273. Figer A, Perez-Staub N, Carola E, et al. FOLFOX in patients aged between 76 and 80 years with metastatic colorectal cancer: an exploratory cohort of the OPTIMOX1 study. Cancer 2007;110:2666-2671. Available at: http://www.ncbi.nlm.nih.gov/pubmed/17963264.
274. Cassidy J, Saltz LB, Giantonio BJ, et al. Effect of bevacizumab in older patients with metastatic colorectal cancer: pooled analysis of four randomized studies. J Cancer Res Clin Oncol 2010;136:737-743. Available at: http://www.ncbi.nlm.nih.gov/pubmed/19904559.
275. Kozloff MF, Berlin J, Flynn PJ, et al. Clinical outcomes in elderly patients with metastatic colorectal cancer receiving bevacizumab and chemotherapy: results from the BRiTE observational cohort study. Oncology 2010;78:329-339. Available at: http://www.ncbi.nlm.nih.gov/pubmed/20733336.
276. Bouchahda M, Macarulla T, Spano JP, et al. Cetuximab efficacy and safety in a retrospective cohort of elderly patients with heavily pretreated metastatic colorectal cancer. Crit Rev Oncol Hematol 2008;67:255-262. Available at: http://www.ncbi.nlm.nih.gov/pubmed/18400508.
277. Fornaro L, Baldi GG, Masi G, et al. Cetuximab plus irinotecan after irinotecan failure in elderly metastatic colorectal cancer patients: Clinical outcome according to KRAS and BRAF mutational status. Crit
Printed by Kelly Hayden on 10/12/2012 3:09:21 PM. For personal use only. Not approved for distribution. Copyright © 2012 National Comprehensive Cancer Network, Inc., All Rights Reserved.

Version 2.2012, 11/15/11 © National Comprehensive Cancer Network, Inc. 2011, All rights reserved. The NCCN Guidelines® and this illustration may not be reproduced in any form without the express written permission of NCCN®. REF-20
NCCN Guidelines IndexSenior Adult Oncology TOC
Discussion
NCCN Guidelines Version 2.2012 Senior Adult Oncolo gy
Rev Oncol Hematol 2010. Available at: http://www.ncbi.nlm.nih.gov/pubmed/20619672.
278. Sastre J, Aranda E, Gravalos C, et al. First-line single-agent cetuximab in elderly patients with metastatic colorectal cancer. A phase II clinical and molecular study of the Spanish group for digestive tumor therapy (TTD). Crit Rev Oncol Hematol 2011;77:78-84. Available at: http://www.ncbi.nlm.nih.gov/pubmed/20042346.
279. Van Cutsem E, Peeters M, Siena S, et al. Open-label phase III trial of panitumumab plus best supportive care compared with best supportive care alone in patients with chemotherapy-refractory metastatic colorectal cancer. J Clin Oncol 2007;25:1658-1664. Available at: http://www.ncbi.nlm.nih.gov/pubmed/17470858.
280. Amado RG, Wolf M, Peeters M, et al. Wild-type KRAS is required for panitumumab efficacy in patients with metastatic colorectal cancer. J Clin Oncol 2008;26:1626-1634. Available at: http://www.ncbi.nlm.nih.gov/pubmed/18316791.
281. Zabrodsky M, Calabrese L, Tosoni A, et al. Major surgery in elderly head and neck cancer patients: immediate and long-term surgical results and complication rates. Surg Oncol 2004;13:249-255. Available at: http://www.ncbi.nlm.nih.gov/pubmed/15615663.
282. Pignon T, Horiot JC, Van den Bogaert W, et al. No age limit for radical radiotherapy in head and neck tumours. Eur J Cancer 1996;32A:2075-2081. Available at: http://www.ncbi.nlm.nih.gov/pubmed/9014748.
283. Posner MR, Hershock DM, Blajman CR, et al. Cisplatin and fluorouracil alone or with docetaxel in head and neck cancer. N Engl J Med 2007;357:1705-1715. Available at: http://www.ncbi.nlm.nih.gov/pubmed/17960013.
284. Vermorken JB, Remenar E, van Herpen C, et al. Cisplatin, fluorouracil, and docetaxel in unresectable head and neck cancer. N
Engl J Med 2007;357:1695-1704. Available at: http://www.ncbi.nlm.nih.gov/pubmed/17960012.
285. Forastiere AA, Goepfert H, Maor M, et al. Concurrent chemotherapy and radiotherapy for organ preservation in advanced laryngeal cancer. N Engl J Med 2003;349:2091-2098. Available at: http://www.ncbi.nlm.nih.gov/pubmed/14645636.
286. Pignon JP, le Maitre A, Maillard E, Bourhis J. Meta-analysis of chemotherapy in head and neck cancer (MACH-NC): an update on 93 randomised trials and 17,346 patients. Radiother Oncol 2009;92:4-14. Available at: http://www.ncbi.nlm.nih.gov/pubmed/19446902.
287. Machtay M, Moughan J, Trotti A, et al. Factors associated with severe late toxicity after concurrent chemoradiation for locally advanced head and neck cancer: an RTOG analysis. J Clin Oncol 2008;26:3582-3589. Available at: http://www.ncbi.nlm.nih.gov/pubmed/18559875.
288. Argiris A, Li Y, Murphy BA, et al. Outcome of elderly patients with recurrent or metastatic head and neck cancer treated with cisplatin-based chemotherapy. J Clin Oncol 2004;22:262-268. Available at: http://www.ncbi.nlm.nih.gov/pubmed/14722034.
289. Bonner JA, Harari PM, Giralt J, et al. Radiotherapy plus cetuximab for locoregionally advanced head and neck cancer: 5-year survival data from a phase 3 randomised trial, and relation between cetuximab-induced rash and survival. Lancet Oncol 2010;11:21-28. Available at: http://www.ncbi.nlm.nih.gov/pubmed/19897418.
290. Vermorken JB, Mesia R, Rivera F, et al. Platinum-based chemotherapy plus cetuximab in head and neck cancer. N Engl J Med 2008;359:1116-1127. Available at: http://www.ncbi.nlm.nih.gov/pubmed/18784101.
291. Lane BR, Abouassaly R, Gao T, et al. Active treatment of localized renal tumors may not impact overall survival in patients aged 75 years
Printed by Kelly Hayden on 10/12/2012 3:09:21 PM. For personal use only. Not approved for distribution. Copyright © 2012 National Comprehensive Cancer Network, Inc., All Rights Reserved.

Version 2.2012, 11/15/11 © National Comprehensive Cancer Network, Inc. 2011, All rights reserved. The NCCN Guidelines® and this illustration may not be reproduced in any form without the express written permission of NCCN®. REF-21
NCCN Guidelines IndexSenior Adult Oncology TOC
Discussion
NCCN Guidelines Version 2.2012 Senior Adult Oncolo gy
or older. Cancer 2010;116:3119-3126. Available at: http://www.ncbi.nlm.nih.gov/pubmed/20564627.
292. Bajetta E, Ravaud A, Bracarda S, et al. Efficacy and safety of first-line bevacizumab (BEV) plus interferon-{alpha}2a (IFN) in patients (pts) >=65 years with metastatic renal cell carcinoma (mRCC) [abstract]. J Clin Oncol 2008;26(Suppl 15):Abstract 5095. Available at: http://meeting.ascopubs.org/cgi/content/abstract/26/15_suppl/5095.
293. Eisen T, Oudard S, Szczylik C, et al. Sorafenib for older patients with renal cell carcinoma: subset analysis from a randomized trial. J Natl Cancer Inst 2008;100:1454-1463. Available at: http://www.ncbi.nlm.nih.gov/pubmed/18840822.
294. Bukowski RM, Stadler WM, McDermott DF, et al. Safety and efficacy of sorafenib in elderly patients treated in the North American advanced renal cell carcinoma sorafenib expanded access program. Oncology 2010;78:340-347. Available at: http://www.ncbi.nlm.nih.gov/pubmed/20733337.
295. Gore ME, Szczylik C, Porta C, et al. Safety and efficacy of sunitinib for metastatic renal-cell carcinoma: an expanded-access trial. Lancet Oncol 2009;10:757-763. Available at: http://www.ncbi.nlm.nih.gov/pubmed/19615940.
296. Hutson TE, Bukowski RM, Rini BI, et al. A pooled analysis of the efficacy and safety of sunitinib in elderly patients (pts) with metastatic renal cell carcinoma (mRCC). J Clin Oncol 2011;29:4604. Available at: http://meeting.ascopubs.org/cgi/content/abstract/29/15_suppl/4604.
297. Osanto S, Hutson TE, Calvo E, et al. Efficacy and safety of everolimus in elderly patients (pts) with metastatic renal cell carcinoma (mRCC). J Clin Oncol 2010;28:4608. Available at: http://meeting.ascopubs.org/cgi/content/abstract/28/15_suppl/4608.
298. Hudes G, Carducci M, Tomczak P, et al. Temsirolimus, interferon alfa, or both for advanced renal-cell carcinoma. N Engl J Med
2007;356:2271-2281. Available at: http://www.ncbi.nlm.nih.gov/pubmed/17538086.
299. Palumbo A, Bringhen S, Caravita T, et al. Oral melphalan and prednisone chemotherapy plus thalidomide compared with melphalan and prednisone alone in elderly patients with multiple myeloma: randomised controlled trial. Lancet 2006;367:825-831. Available at: http://www.ncbi.nlm.nih.gov/pubmed/16530576.
300. Palumbo A, Bringhen S, Liberati AM, et al. Oral melphalan, prednisone, and thalidomide in elderly patients with multiple myeloma: updated results of a randomized controlled trial. Blood 2008;112:3107-3114. Available at: http://www.ncbi.nlm.nih.gov/pubmed/18505783.
301. Facon T, Mary JY, Hulin C, et al. Melphalan and prednisone plus thalidomide versus melphalan and prednisone alone or reduced-intensity autologous stem cell transplantation in elderly patients with multiple myeloma (IFM 99-06): a randomised trial. Lancet 2007;370:1209-1218. Available at: http://www.ncbi.nlm.nih.gov/pubmed/17920916.
302. Hulin C, Facon T, Rodon P, et al. Efficacy of melphalan and prednisone plus thalidomide in patients older than 75 years with newly diagnosed multiple myeloma: IFM 01/01 trial. J Clin Oncol 2009;27:3664-3670. Available at: http://www.ncbi.nlm.nih.gov/pubmed/19451428.
303. Waage A, Gimsing P, Fayers P, et al. Melphalan and prednisone plus thalidomide or placebo in elderly patients with multiple myeloma. Blood 2010;116:1405-1412. Available at: http://www.ncbi.nlm.nih.gov/pubmed/20448107.
304. Wijermans P, Schaafsma M, Termorshuizen F, et al. Phase III study of the value of thalidomide added to melphalan plus prednisone in elderly patients with newly diagnosed multiple myeloma: the HOVON 49 Study. J Clin Oncol 2010;28:3160-3166. Available at: http://www.ncbi.nlm.nih.gov/pubmed/20516439.
Printed by Kelly Hayden on 10/12/2012 3:09:21 PM. For personal use only. Not approved for distribution. Copyright © 2012 National Comprehensive Cancer Network, Inc., All Rights Reserved.

Version 2.2012, 11/15/11 © National Comprehensive Cancer Network, Inc. 2011, All rights reserved. The NCCN Guidelines® and this illustration may not be reproduced in any form without the express written permission of NCCN®. REF-22
NCCN Guidelines IndexSenior Adult Oncology TOC
Discussion
NCCN Guidelines Version 2.2012 Senior Adult Oncolo gy
305. Beksac M, Haznedar R, Firatli-Tuglular T, et al. Addition of thalidomide to oral melphalan/prednisone in patients with multiple myeloma not eligible for transplantation: results of a randomized trial from the Turkish Myeloma Study Group. Eur J Haematol 2011;86:16-22. Available at: http://www.ncbi.nlm.nih.gov/pubmed/20942865.
306. Kapoor P, Rajkumar SV, Dispenzieri A, et al. Melphalan and prednisone versus melphalan, prednisone and thalidomide for elderly and/or transplant-ineligible patients with multiple myeloma: a meta-analysis. Leukemia 2011;25:1523-1524. Available at: http://www.ncbi.nlm.nih.gov/pubmed/21233832.
307. Palumbo A, Cavo M, Bringhen S, et al. Aspirin, warfarin, or enoxaparin thromboprophylaxis in patients with multiple myeloma treated with thalidomide: a phase III, open-label, randomized trial. J Clin Oncol 2011;29:986-993. Available at: http://www.ncbi.nlm.nih.gov/pubmed/21282540.
308. San Miguel JF, Schlag R, Khuageva NK, et al. Bortezomib plus melphalan and prednisone for initial treatment of multiple myeloma. N Engl J Med 2008;359:906-917. Available at: http://www.ncbi.nlm.nih.gov/pubmed/18753647.
309. Mateos M-V, Richardson PG, Schlag R, et al. Bortezomib plus melphalan and prednisone compared with melphalan and prednisone in previously untreated multiple myeloma: updated follow-up and impact of subsequent therapy in the phase III VISTA trial. J Clin Oncol 2010;28:2259-2266. Available at: http://www.ncbi.nlm.nih.gov/pubmed/20368561.
310. Mateos M-V, Oriol A, Martinez-Lopez J, et al. Bortezomib, melphalan, and prednisone versus bortezomib, thalidomide, and prednisone as induction therapy followed by maintenance treatment with bortezomib and thalidomide versus bortezomib and prednisone in elderly patients with untreated multiple myeloma: a randomised trial. Lancet Oncol 2010;11:934-941. Available at: http://www.ncbi.nlm.nih.gov/pubmed/20739218.
311. Palumbo A, Bringhen S, Rossi D, et al. Bortezomib-melphalan-prednisone-thalidomide followed by maintenance with bortezomib-thalidomide compared with bortezomib-melphalan-prednisone for initial treatment of multiple myeloma: a randomized controlled trial. J Clin Oncol 2010;28:5101-5109. Available at: http://www.ncbi.nlm.nih.gov/pubmed/20940200.
312. Facon T, Mary J-Y, Pegourie B, et al. Dexamethasone-based regimens versus melphalan-prednisone for elderly multiple myeloma patients ineligible for high-dose therapy. Blood 2006;107:1292-1298. Available at: http://www.ncbi.nlm.nih.gov/pubmed/16174762.
313. Rajkumar SV, Jacobus S, Callander NS, et al. Lenalidomide plus high-dose dexamethasone versus lenalidomide plus low-dose dexamethasone as initial therapy for newly diagnosed multiple myeloma: an open-label randomised controlled trial. Lancet Oncol 2010;11:29-37. Available at: http://www.ncbi.nlm.nih.gov/pubmed/19853510.
314. Effect of age on the characteristics and clinical behavior of non-Hodgkin's lymphoma patients. The Non-Hodgkin's Lymphoma Classification Project. Ann Oncol 1997;8:973-978. Available at: http://www.ncbi.nlm.nih.gov/pubmed/9402170.
315. Seymour JF, Talpaz M, Cabanillas F, et al. Serum interleukin-6 levels correlate with prognosis in diffuse large-cell lymphoma. J Clin Oncol 1995;13:575-582. Available at: http://www.ncbi.nlm.nih.gov/pubmed/7884418.
316. Pedersen LM, Klausen TW, Davidsen UH, Johnsen HE. Early changes in serum IL-6 and VEGF levels predict clinical outcome following first-line therapy in aggressive non-Hodgkin's lymphoma. Ann Hematol 2005;84:510-516. Available at: http://www.ncbi.nlm.nih.gov/pubmed/15834569.
Printed by Kelly Hayden on 10/12/2012 3:09:21 PM. For personal use only. Not approved for distribution. Copyright © 2012 National Comprehensive Cancer Network, Inc., All Rights Reserved.
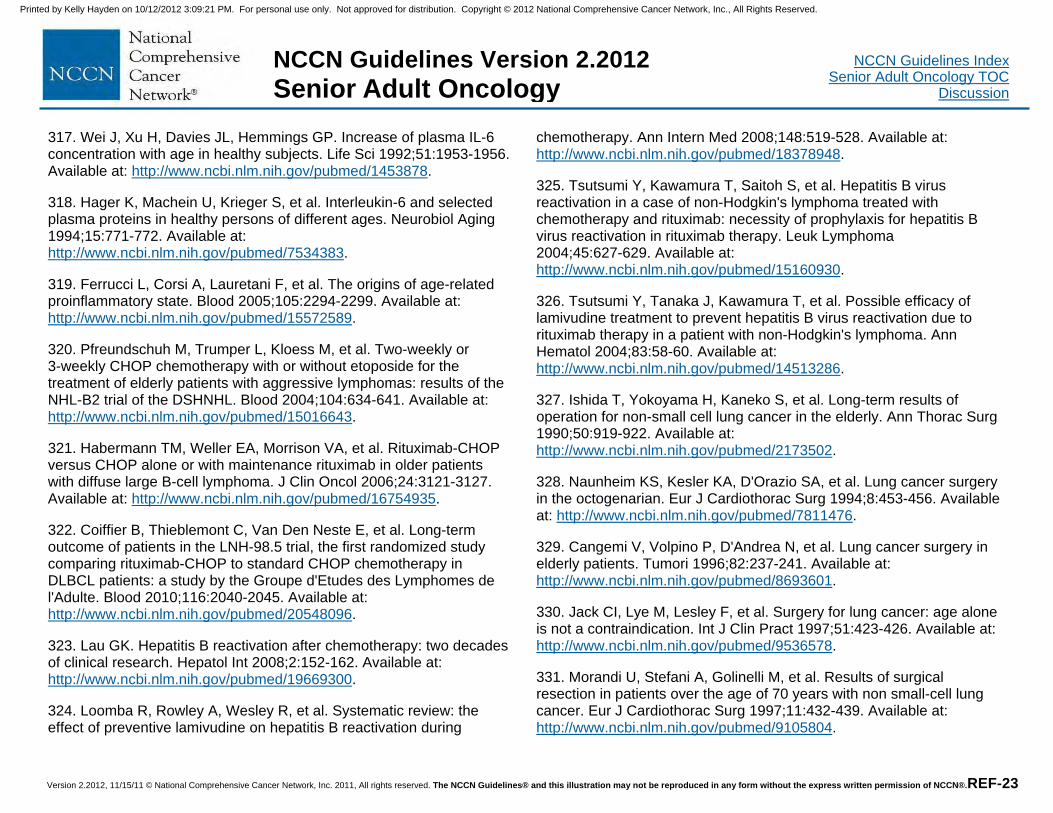
Version 2.2012, 11/15/11 © National Comprehensive Cancer Network, Inc. 2011, All rights reserved. The NCCN Guidelines® and this illustration may not be reproduced in any form without the express written permission of NCCN®. REF-23
NCCN Guidelines IndexSenior Adult Oncology TOC
Discussion
NCCN Guidelines Version 2.2012 Senior Adult Oncolo gy
317. Wei J, Xu H, Davies JL, Hemmings GP. Increase of plasma IL-6 concentration with age in healthy subjects. Life Sci 1992;51:1953-1956. Available at: http://www.ncbi.nlm.nih.gov/pubmed/1453878.
318. Hager K, Machein U, Krieger S, et al. Interleukin-6 and selected plasma proteins in healthy persons of different ages. Neurobiol Aging 1994;15:771-772. Available at: http://www.ncbi.nlm.nih.gov/pubmed/7534383.
319. Ferrucci L, Corsi A, Lauretani F, et al. The origins of age-related proinflammatory state. Blood 2005;105:2294-2299. Available at: http://www.ncbi.nlm.nih.gov/pubmed/15572589.
320. Pfreundschuh M, Trumper L, Kloess M, et al. Two-weekly or 3-weekly CHOP chemotherapy with or without etoposide for the treatment of elderly patients with aggressive lymphomas: results of the NHL-B2 trial of the DSHNHL. Blood 2004;104:634-641. Available at: http://www.ncbi.nlm.nih.gov/pubmed/15016643.
321. Habermann TM, Weller EA, Morrison VA, et al. Rituximab-CHOP versus CHOP alone or with maintenance rituximab in older patients with diffuse large B-cell lymphoma. J Clin Oncol 2006;24:3121-3127. Available at: http://www.ncbi.nlm.nih.gov/pubmed/16754935.
322. Coiffier B, Thieblemont C, Van Den Neste E, et al. Long-term outcome of patients in the LNH-98.5 trial, the first randomized study comparing rituximab-CHOP to standard CHOP chemotherapy in DLBCL patients: a study by the Groupe d'Etudes des Lymphomes de l'Adulte. Blood 2010;116:2040-2045. Available at: http://www.ncbi.nlm.nih.gov/pubmed/20548096.
323. Lau GK. Hepatitis B reactivation after chemotherapy: two decades of clinical research. Hepatol Int 2008;2:152-162. Available at: http://www.ncbi.nlm.nih.gov/pubmed/19669300.
324. Loomba R, Rowley A, Wesley R, et al. Systematic review: the effect of preventive lamivudine on hepatitis B reactivation during
chemotherapy. Ann Intern Med 2008;148:519-528. Available at: http://www.ncbi.nlm.nih.gov/pubmed/18378948.
325. Tsutsumi Y, Kawamura T, Saitoh S, et al. Hepatitis B virus reactivation in a case of non-Hodgkin's lymphoma treated with chemotherapy and rituximab: necessity of prophylaxis for hepatitis B virus reactivation in rituximab therapy. Leuk Lymphoma 2004;45:627-629. Available at: http://www.ncbi.nlm.nih.gov/pubmed/15160930.
326. Tsutsumi Y, Tanaka J, Kawamura T, et al. Possible efficacy of lamivudine treatment to prevent hepatitis B virus reactivation due to rituximab therapy in a patient with non-Hodgkin's lymphoma. Ann Hematol 2004;83:58-60. Available at: http://www.ncbi.nlm.nih.gov/pubmed/14513286.
327. Ishida T, Yokoyama H, Kaneko S, et al. Long-term results of operation for non-small cell lung cancer in the elderly. Ann Thorac Surg 1990;50:919-922. Available at: http://www.ncbi.nlm.nih.gov/pubmed/2173502.
328. Naunheim KS, Kesler KA, D'Orazio SA, et al. Lung cancer surgery in the octogenarian. Eur J Cardiothorac Surg 1994;8:453-456. Available at: http://www.ncbi.nlm.nih.gov/pubmed/7811476.
329. Cangemi V, Volpino P, D'Andrea N, et al. Lung cancer surgery in elderly patients. Tumori 1996;82:237-241. Available at: http://www.ncbi.nlm.nih.gov/pubmed/8693601.
330. Jack CI, Lye M, Lesley F, et al. Surgery for lung cancer: age alone is not a contraindication. Int J Clin Pract 1997;51:423-426. Available at: http://www.ncbi.nlm.nih.gov/pubmed/9536578.
331. Morandi U, Stefani A, Golinelli M, et al. Results of surgical resection in patients over the age of 70 years with non small-cell lung cancer. Eur J Cardiothorac Surg 1997;11:432-439. Available at: http://www.ncbi.nlm.nih.gov/pubmed/9105804.
Printed by Kelly Hayden on 10/12/2012 3:09:21 PM. For personal use only. Not approved for distribution. Copyright © 2012 National Comprehensive Cancer Network, Inc., All Rights Reserved.

Version 2.2012, 11/15/11 © National Comprehensive Cancer Network, Inc. 2011, All rights reserved. The NCCN Guidelines® and this illustration may not be reproduced in any form without the express written permission of NCCN®. REF-24
NCCN Guidelines IndexSenior Adult Oncology TOC
Discussion
NCCN Guidelines Version 2.2012 Senior Adult Oncolo gy
332. Mizushima Y, Noto H, Sugiyama S, et al. Survival and prognosis after pneumonectomy for lung cancer in the elderly. Ann Thorac Surg 1997;64:193-198. Available at: http://www.ncbi.nlm.nih.gov/pubmed/9236359.
333. Chemotherapy in non-small cell lung cancer: a meta-analysis using updated data on individual patients from 52 randomised clinical trials. Non-small Cell Lung Cancer Collaborative Group. BMJ 1995;311:899-909. Available at: http://www.ncbi.nlm.nih.gov/pubmed/7580546.
334. Pepe C, Hasan B, Winton TL, et al. Adjuvant vinorelbine and cisplatin in elderly patients: National Cancer Institute of Canada and Intergroup Study JBR.10. J Clin Oncol 2007;25:1553-1561. Available at: http://www.ncbi.nlm.nih.gov/pubmed/17442999.
335. Fruh M, Rolland E, Pignon J-P, et al. Pooled analysis of the effect of age on adjuvant cisplatin-based chemotherapy for completely resected non-small-cell lung cancer. J Clin Oncol 2008;26:3573-3581. Available at: http://www.ncbi.nlm.nih.gov/pubmed/18640938.
336. Langer CJ, Hsu C, Curran WJ, et al. Elderly patients (pts) with locally advanced non-small cell lung cancer (LA-NSCLC) benefit from combined modality therapy: secondary analysis of Radiation Therapy Oncology Group (RTOG) 94-10. Proc Am Soc Clin Oncol 2002;21:Abstract 1193. Available at:
337. Schild SE, Stella PJ, Geyer SM, et al. The outcome of combined-modality therapy for stage III non-small-cell lung cancer in the elderly. J Clin Oncol 2003;21:3201-3206. Available at: http://www.ncbi.nlm.nih.gov/pubmed/12874270.
338. Movsas B, Scott C, Sause W, et al. The benefit of treatment intensification is age and histology-dependent in patients with locally advanced non-small cell lung cancer (NSCLC): a quality-adjusted survival analysis of radiation therapy oncology group (RTOG) chemoradiation studies. Int J Radiat Oncol Biol Phys
1999;45:1143-1149. Available at: http://www.ncbi.nlm.nih.gov/pubmed/10613306.
339. Werner-Wasik M, Scott C, Cox JD, et al. Recursive partitioning analysis of 1999 Radiation Therapy Oncology Group (RTOG) patients with locally-advanced non-small-cell lung cancer (LA-NSCLC): identification of five groups with different survival. Int J Radiat Oncol Biol Phys 2000;48:1475-1482. Available at: http://www.ncbi.nlm.nih.gov/pubmed/11121651.
340. Gridelli C. The ELVIS trial: a phase III study of single-agent vinorelbine as first-line treatment in elderly patients with advanced non-small cell lung cancer. Elderly Lung Cancer Vinorelbine Italian Study. Oncologist 2001;6 Suppl 1:4-7. Available at: http://www.ncbi.nlm.nih.gov/pubmed/11181997.
341. Kudoh S, Takeda K, Nakagawa K, et al. Phase III study of docetaxel compared with vinorelbine in elderly patients with advanced non-small-cell lung cancer: results of the West Japan Thoracic Oncology Group Trial (WJTOG 9904). J Clin Oncol 2006;24:3657-3663. Available at: http://www.ncbi.nlm.nih.gov/pubmed/16877734.
342. Kelly K, Giarritta S, Akerley W, et al. Should Older Patients (Pts) Receive Combination Chemotherapy for Advanced Stage Non-Small Cell Lung Cancer (NSCLC)? An Analysis of Southwest Oncology Trials 9509 and 9308. Proc Am Soc Clin Oncol 2001;20:Abstract 1313. Available at:
343. Lilenbaum RC, Herndon JE, List MA, et al. Single-agent versus combination chemotherapy in advanced non-small-cell lung cancer: the cancer and leukemia group B (study 9730). J Clin Oncol 2005;23:190-196. Available at: http://www.ncbi.nlm.nih.gov/pubmed/15625373.
344. Frasci G, Lorusso V, Panza N, et al. Gemcitabine plus vinorelbine yields better survival outcome than vinorelbine alone in elderly patients with advanced non-small cell lung cancer. A Southern Italy Cooperative
Printed by Kelly Hayden on 10/12/2012 3:09:21 PM. For personal use only. Not approved for distribution. Copyright © 2012 National Comprehensive Cancer Network, Inc., All Rights Reserved.

Version 2.2012, 11/15/11 © National Comprehensive Cancer Network, Inc. 2011, All rights reserved. The NCCN Guidelines® and this illustration may not be reproduced in any form without the express written permission of NCCN®. REF-25
NCCN Guidelines IndexSenior Adult Oncology TOC
Discussion
NCCN Guidelines Version 2.2012 Senior Adult Oncolo gy
Oncology Group (SICOG) phase III trial. Lung Cancer 2001;34 Suppl 4:65-69. Available at: http://www.ncbi.nlm.nih.gov/pubmed/11742706.
345. Gridelli C, Perrone F, Gallo C, et al. Chemotherapy for elderly patients with advanced non-small-cell lung cancer: the Multicenter Italian Lung Cancer in the Elderly Study (MILES) phase III randomized trial. J Natl Cancer Inst 2003;95:362-372. Available at: http://www.ncbi.nlm.nih.gov/pubmed/12618501.
346. Quoix E, Zalcman G, Oster JP, et al. Carboplatin and weekly paclitaxel doublet chemotherapy compared with monotherapy in elderly patients with advanced non-small-cell lung cancer: IFCT-0501 randomised, phase 3 trial. Lancet 2011;378:1079-1088. Available at: http://www.ncbi.nlm.nih.gov/pubmed/21831418.
347. Ramalingam SS, Dahlberg SE, Langer CJ, et al. Outcomes for elderly, advanced-stage non small-cell lung cancer patients treated with bevacizumab in combination with carboplatin and paclitaxel: analysis of Eastern Cooperative Oncology Group Trial 4599. J Clin Oncol 2008;26:60-65. Available at: http://www.ncbi.nlm.nih.gov/pubmed/18165641.
348. Jackman DM, Yeap BY, Lindeman NI, et al. Phase II clinical trial of chemotherapy-naive patients > or = 70 years of age treated with erlotinib for advanced non-small-cell lung cancer. J Clin Oncol 2007;25:760-766. Available at: http://www.ncbi.nlm.nih.gov/pubmed/17228019.
349. Wheatley-Price P, Ding K, Seymour L, et al. Erlotinib for advanced non-small-cell lung cancer in the elderly: an analysis of the National Cancer Institute of Canada Clinical Trials Group Study BR.21. J Clin Oncol 2008;26:2350-2357. Available at: http://www.ncbi.nlm.nih.gov/pubmed/18467727.
350. Droz JP, Balducci L, Bolla M, et al. Management of prostate cancer in older men: recommendations of a working group of the International Society of Geriatric Oncology. BJU Int 2010;106:462-469. Available at: http://www.ncbi.nlm.nih.gov/pubmed/20346033.
351. Tannock IF, de Wit R, Berry WR, et al. Docetaxel plus prednisone or mitoxantrone plus prednisone for advanced prostate cancer. N Engl J Med 2004;351:1502-1512. Available at: http://www.ncbi.nlm.nih.gov/pubmed/15470213.
352. Sinibaldi VJ. Docetaxel treatment in the elderly patient with hormone refractory prostate cancer. Clin Interv Aging 2007;2:555-560. Available at: http://www.ncbi.nlm.nih.gov/pubmed/18225455.
353. Berthold DR, Pond GR, Soban F, et al. Docetaxel plus prednisone or mitoxantrone plus prednisone for advanced prostate cancer: updated survival in the TAX 327 study. J Clin Oncol 2008;26:242-245. Available at: http://www.ncbi.nlm.nih.gov/pubmed/18182665.
354. Pal SK, Twardowski P, Sartor O. Critical appraisal of cabazitaxel in the management of advanced prostate cancer. Clin Interv Aging 2010;5:395-402. Available at: http://www.ncbi.nlm.nih.gov/pubmed/21152241.
355. de Bono JS, Oudard S, Ozguroglu M, et al. Prednisone plus cabazitaxel or mitoxantrone for metastatic castration-resistant prostate cancer progressing after docetaxel treatment: a randomised open-label trial. Lancet 2010;376:1147-1154. Available at: http://www.ncbi.nlm.nih.gov/pubmed/20888992.
Printed by Kelly Hayden on 10/12/2012 3:09:21 PM. For personal use only. Not approved for distribution. Copyright © 2012 National Comprehensive Cancer Network, Inc., All Rights Reserved.