“stop smoking in its tracks”: an incentives- based smoking cessation program for australian...
TRANSCRIPT

“Stop Smoking in its Tracks”:An incentives- based smoking cessation program for Australian Aboriginal women provided by antenatal services – a pilot study
Megan Passey, Rob Sanson-Fisher and Janelle StirlingUK National Smoking Cessation Conference
London, June 2014
1

Collaborative projectUCRH, University of Sydney: Megan Passey, Jenny Gale, Janelle
Stirling, Cathy Malla Aboriginal Maternal & Infant Health Strategy (AMIHS) program:
Catherine Leatherday, Brenda Holt, Cathy Powell, Sue Rogers, Paula Craig
University of Newcastle: Rob Sanson-FisherCommunity Reference Group: Aunty Bertha Kapeen, Delta Kay,
Virginia Paden, Laurel Rogers, Careena Roberts, Janina Roberts, Dana Lavelle, Joyce Roberts, Akarna King, Edith King
2


4
Prevalence of smokingAustralian adult population in 2008:
Aboriginal and Torres Strait Islander Australians – 47.0%Non-Indigenous Australians – 17.5%
Pregnant women in Australia in 2010:Aboriginal and Torres Strait Islander women – 50.9%Non-Indigenous women – 14.4%
Among Aboriginal and Torres Strait Islander women:Highest in outer regional areas, lowest in citiesDeclines slightly with age
(Scollo and Winstanley 2012)Laws and Sullivan, 2009
5
Request to help develop quitting program Few published articles addressing smoking or cessation by
pregnant Aboriginal women Much of the Indigenous research available was done in
remote settingsGeneral smoking cessation literature gives little guidance
on Indigenous specific issuesLittle relevant grey literature; lots of anecdoteOnly one properly controlled trial of a smoking cessation
intervention with pregnant Indigenous Australian women – not effective (Eades et al, 2012)

Formative research to help design the quitting program
1. Qualitative study on North Coast Interviews with women Focus groups with women and service providers
2. Survey of antenatal staff caring for Aboriginal women
3. Survey of pregnant Aboriginal women
6

7
Social drivers of smokingSmoking ‘normal’ in Aboriginal
communities When you don’t smoke you stand out a bit, you feel a
bit odd…. Cause everyone around you smokes. Everyone that I know smokes. There is not one person that I know in [town] who doesn’t smoke. So like, it is a bit hard. 24 year old smoker
Cultural issues and smoking Relationships, obligations and need to
belong identified as barrier to quittingSharing cigarette and having a yarn
contribute to social cohesion and sense of belonging
(Passey et al, 2011)

More barriers to quitting
High levels of stress and previous trauma
Partner and other household members smoking
Low self-efficacy for somePoor knowledge of risk and lack of salience
of risk informationAddiction and habitPleasure of smoking

9
Tobacco, cannabis and alcohol
Survey with pregnant Aboriginal women in NSW
and NT (n=257):
46% reported smoking tobacco
15% reported smoking cannabis
21% reported drinking alcohol
Smokers more likely to also: Drink alcohol (OR=4.3; 95%CI: 2.12, 9.13)
Smoke cannabis (OR=10.2; 95%CI: 3.73, 34.52)

Assess & support all
women
Contingency based
rewards
Free NRT Resources:Brochures,
magnets etc
Post-partum support
Social support groups
Other drugs (alcohol, cannabis
referrals)
Household members
Assist AMIHS
team to quit
Build on existing services - AMIHS:• Regular antenatal visits• Good relationships• Ongoing support
• Widely accepted in community & homes
• Cultural & community knowledge• Reinforcing each others messages
Empowerment approachG o a l s , p e r s o n a l r e w a r d s , b e l i e f i n a b i l i t y t o q u i t

Schedule for visits and rewards
Starts at first antenatal visitTwice weekly for 3 weeksWeekly for next 4 weeksFortnightly till the birthWeekly for 6 weeks post-partumFortnightly till 6 months postpartumValue starts at $10, increasing by $2 each visit if
confirmed non-smoking
11

Pilot testing Stop Smoking in its Tracks2 AMIHS sites trained and provided with resources
and supportAssessed:
Feasibility – provider views, implementation indicators, notes from meetings
Acceptability – to women and providers – interviews, participation rates, notes
Impact – on smoking behaviour, other impacts – record keeping by providers, notes
12
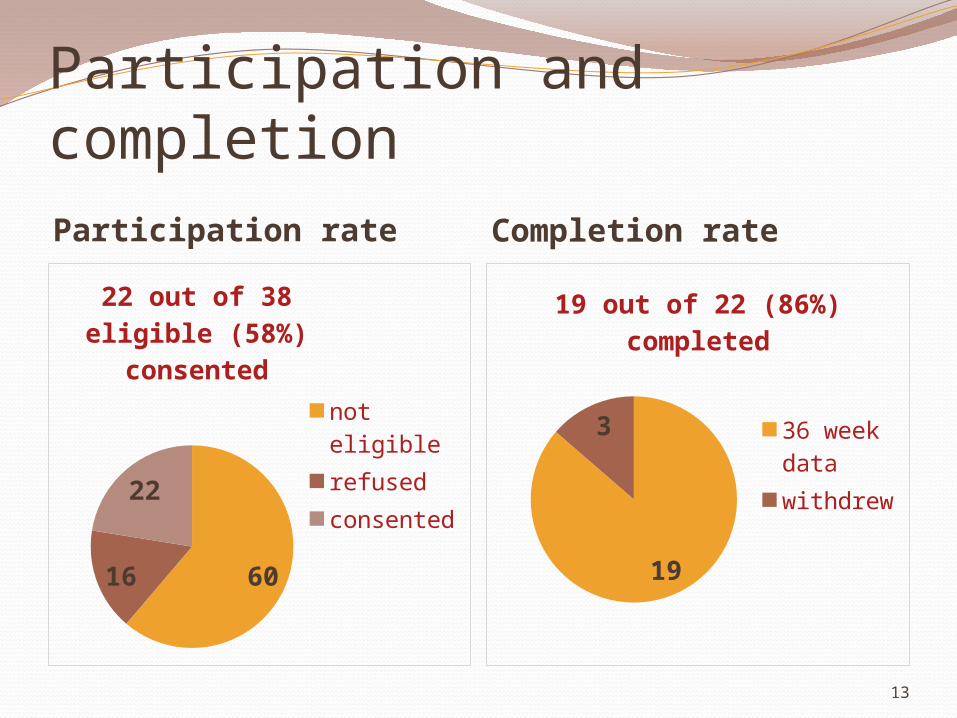
Participation and completionParticipation rate Completion rate
6016
22
22 out of 38 eligible (58%) consented
not eligiblerefusedconsented
19
3
19 out of 22 (86%) completed
36 week datawithdrew
13

Quit rates – (confirmed by expired CO)
quit attempt successful quit quit at 36 weeks0%
10%
20%
30%
40%
50%
60%
70%
80%
90%
84%79%
42%
14

Rewards issuedAmount per woman ranged from $56 to $820Median amount issued was $294
Majority used at electrical appliances stores, then pharmacies
15

FeasibilityTeam capacity
Frequency of visits
Running groups
Distance and transport
NRT expiry dates
16

Women’s views
Loved the frequency of support, especially when trying to quit or maintain quit status
Rewards very motivating AMIHS always mentioning smoking helped women
realise how important it wasOngoing support helping women with strategies was
valued “it seems like they really care”
17

AMIHS team views
Good to have something to offer women to help them quit – much more powerful than usual care
Combination of rewards with the other support was really effective
Women who quit were very proud of their successThought that most women really valued the rewards
and the frequency of the support
18

Views on RewardsConsidered powerful motivator in one site, but not as
powerful with some women in other siteHelped women maintain their motivation and
prevent relapse
“I think the biggest word is proud. They were just so proud of themselves that they got enough vouchers to get a hair straightener or a – one got a fridge”
19

Conclusions - the program was:Acceptable to both women and the providersFeasible to implement but needs adequate staffing levels and
capacity Impact – high rates of quitting behaviour with confirmed
quitting in late pregnancy similar to other programs including incentives
Modifications – consider reducing duration of frequent visits and/or dropping the groups
Next phase – larger trial to assess impact in pregnancy & postpartum; adverse effects; feasibility in different settings

Thank you!Acknowledgement of FundingStudies funded by the Australian Department of
Health and Ageing under the Indigenous Tobacco Control Initiative
Currently supported by fellowships from the NHMRC and the NSW Cancer Institute
Contact: [email protected]
21