stop the pressure: patient safety and tissue viability safety and... · patient safety and tissue...
TRANSCRIPT

Stop The Pressure: Patient Safety and
Tissue Viability
Portsmouth Hospitals NHS Trust
Alison ColeClaire BrettKaren Oakley

Etiology and cause of a pressure ulcerThe impact of pressure ulcers Identifying who is at risk and risk assessmentBraden Assessment Tool and SSKIN BundleSkin AssessmentClassification of pressure ulcersDifferential DiagnosisYour role in pressure ulcer prevention
Presentation FocusPresentation Focus

Introduction: Introduction: What is a Pressure Ulcer?What is a Pressure Ulcer?
‘A pressure ulcer is a localised injury to the skin and/ or underlying tissue, usually over a bony prominence, resulting from sustained pressure (including pressure associated with shear)’.

ShearShear• Shear stresses are thought to act alongside pressure to
produce the damage and ischemia (death) of the skin and deeper tissues that results in pressure ulcers.
• Shear injury will not be seen at the skin level because it happens beneath the skin.
• Shear is a mechanical force for example:
pulling the bones of the pelvis in one direction and the skin in the opposite direction.
Shear: Who is at Risk?Shear: Who is at Risk?
• Must have head of bed elevated• Difficult to reposition without sliding across surfaces• Those that slip/slide from a position they have been placed in• Those too weak to reposition independently without ‘dragging’
themselves across surfaces • Exposed to high pressure over a bony prominence• Moist, wet or macerated skin
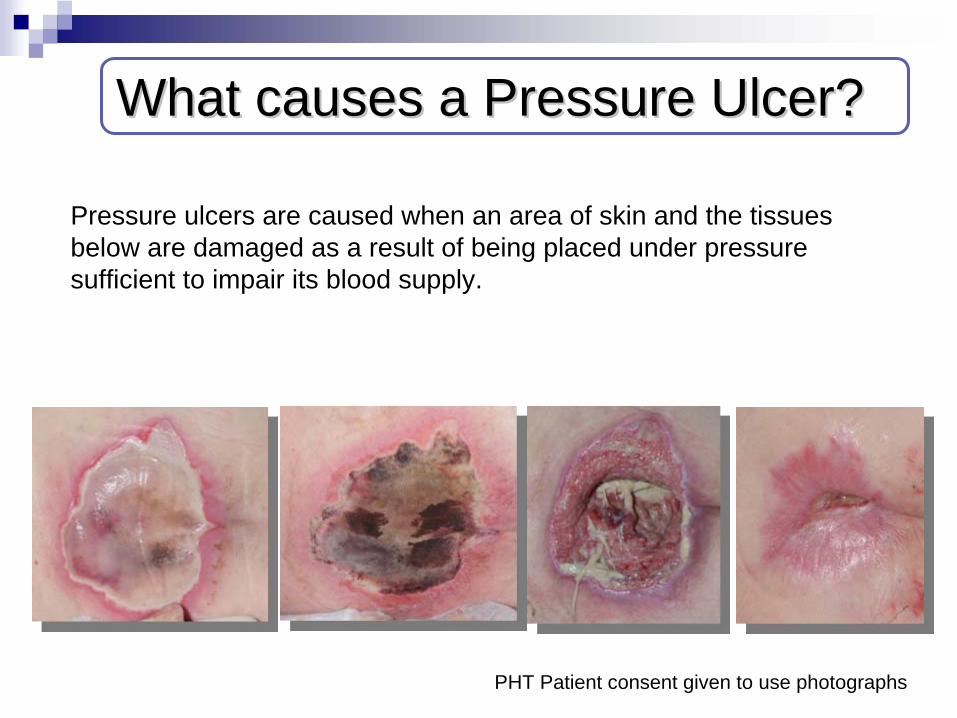
What causes a Pressure Ulcer?What causes a Pressure Ulcer?
Pressure ulcers are caused when an area of skin and the tissues below are damaged as a result of being placed under pressure sufficient to impair its blood supply.
PHT Patient consent given to use photographs
Why is it important?Why is it important?
• Impact on patient: pain, reduced quality of life, physical, psychological and social impact
• 186,617 patients develop a pressure ulcer in hospital each year
• Each pressure ulcer adds additional costs of care of over £4000
• Research suggests that 80-95% are avoidable
• 700,000 people are affected by pressure ulcers each year
• Quality indicator of our care

Identifying individuals at riskIdentifying individuals at riskof developing pressure ulcersof developing pressure ulcers
ImmobilityOlder adults
Trauma
Spinal cord injury
Fractured hip
Acute/Chronic Illness
Diabetes
Critical care
Weight loss
Malnutrition
Sensory Loss
Vascular Disease
Incontinent
Bariatric patients Critically ill patients
Palliative care patients

Risk assessmentRisk assessment
“Risk assessment is an essential component of clinical practice that aims to identify individuals who are susceptible in order that appropriate interventions to prevent pressure ulcer occurrence can be planned and implemented”
• Implement and complete a risk assessment tool• Undertake a comprehensive skin assessment
(complete red alert sticker)• Consider additional risk factors• Use your clinical judgement• Repeat risk assessment as often as required by the
patients condition• Undertake reassessment if there is any significant
change in the patients’ condition

Risk assessment Tool:Risk assessment Tool:Braden ScoreBraden Score
15- 18: At Risk 13-14: Moderate Risk 10-12: High Risk 9 or Below: Very high risk

Risk assessment Tool:Risk assessment Tool:Braden Score ScenarioBraden Score Scenario
Example 1
Mrs Smith is 80 years old and has been admitted to hospital due to Shortness of Breath. All pressure areas were checked on admission and are all intact. Mrs Smith lives alone with a three times a day package of care. Mrs Smith has an Abbreviated Mental Test Score (AMTS) of 10/10, is urinary and faecally incontinent and is able to mobilize with her Zimmer frame with assistance of one. Mrs Smith tells us that she is able to reposition herself, however sometimes finds herself sliding in her chair. Mrs Smith has a good appetite and feeds herself independently, her BMI is 19.

Risk assessment Tool:Risk assessment Tool:Braden Score ScenarioBraden Score Scenario
Example 2
Mr Brown has been admitted to hospital following an episode of chest pain. All pressure areas checked on admission and Mr Brown has a grade 3 pressure ulcer to his sacrum. Mr Brown has an AMTS of 7/10. Mr Brown lives in a Residential home and is continent of urine and faeces. Mr Brown is pivot transferred from bed to chair with the assistance of two carers and is unable to mobilise. Mr Brown has lost two stone in weight in the 3 months and requires to be fed. Mr Brown’s BMI is 20.

Risk assessment Tool:Risk assessment Tool:Braden ScoreBraden Score
Mrs Smith:
Sensory Perception: 3Moisture: 1Activity: 3Mobility: 3Nutrition: 3Friction and Shear: 2
= 15 (At Risk)
Mr Brown:
Sensory Perception: 4Moisture: 4Activity: 2Mobility: 2Nutrition: 2Friction and Shear: 1
= 15 (At Risk)
Do not rely on the total score as a basis when assessing your patients’ risk.
Risk assessment tool sub-scale scores and other risk factors should also be examined to provide risk based planning
Use your clinicalJudgement
Documentation of risk assessment Documentation of risk assessment and a preventative care planand a preventative care plan
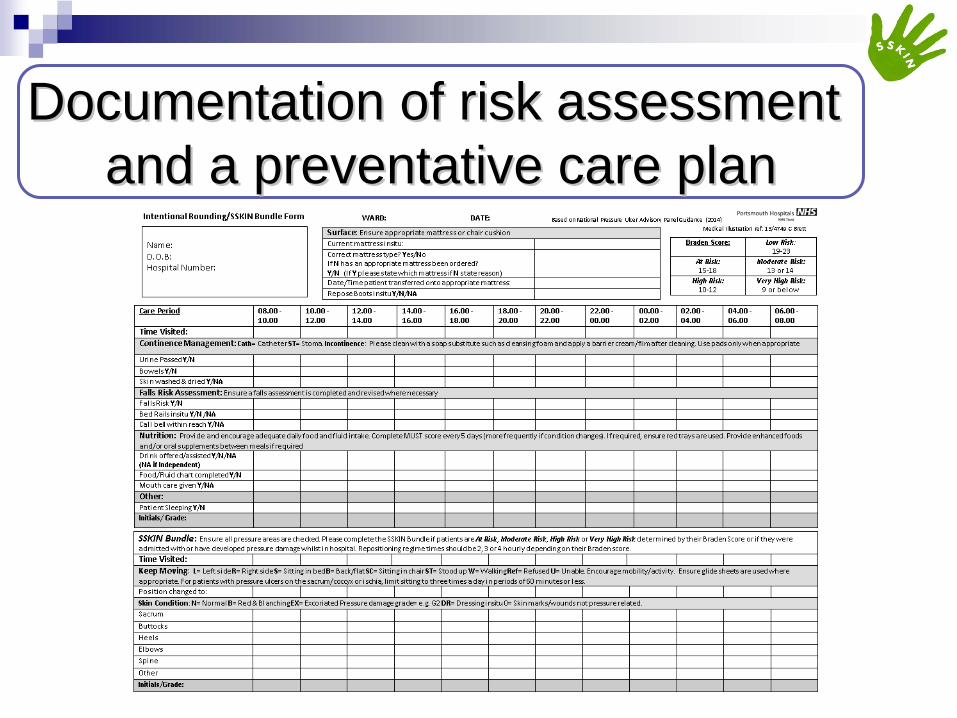
Documentation of risk assessment Documentation of risk assessment and a preventative care planand a preventative care plan

Skin Inspection/assessmentSkin Inspection/assessment
• Skin assessment is crucial in pressure ulcer prevention because it can serve as an indicator of early signs of pressure damage.
• Skin and tissue assessment underpins the selection and evaluation of appropriate preventative interventions.
• Early inspection means early detection
Skin Inspection/assessmentSkin Inspection/assessment
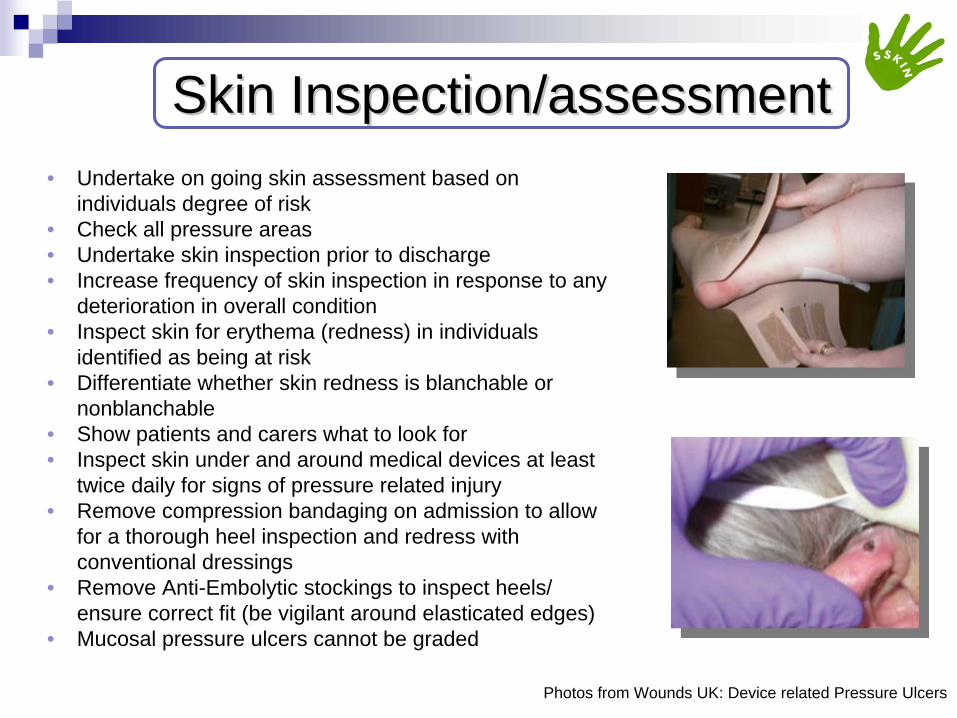
Photos from Wounds UK: Device related Pressure Ulcers
• Undertake on going skin assessment based on individuals degree of risk
• Check all pressure areas• Undertake skin inspection prior to discharge• Increase frequency of skin inspection in response to any
deterioration in overall condition• Inspect skin for erythema (redness) in individuals
identified as being at risk • Differentiate whether skin redness is blanchable or
nonblanchable• Show patients and carers what to look for • Inspect skin under and around medical devices at least
twice daily for signs of pressure related injury• Remove compression bandaging on admission to allow
for a thorough heel inspection and redress with conventional dressings
• Remove Anti-Embolytic stockings to inspect heels/ ensure correct fit (be vigilant around elasticated edges)
• Mucosal pressure ulcers cannot be graded

Blanchable Erythema Blanchable Erythema
Erythema= redness
Visible skin redness that becomes white when pressure is applied and reddens when pressure is relieved
Photos: PUCLAS

NonNon--blanchable Erythemablanchable Erythema
Visible skin redness that persists with the application of pressure. It indicates structural damage to the capillary bed.
Photos PUCLAS

Classification of Pressure UlcersClassification of Pressure Ulcers
Category/Stage I: Non-blanchable erythema Intact skin with non-blanchable redness of a localized area usually over a bony prominence. Darkly pigmented skin may not have visible blanching; its colour may differ from the surrounding area. The area may be painful, firm, soft, warmer or cooler as compared to adjacent tissue. Category I may be difficult to detect in individuals with dark skin tones. May indicate “at risk” persons.

Classification of Pressure UlcersClassification of Pressure Ulcers
Category/Stage II: Partial thickness
Partial thickness loss of dermis presenting as a shallow open ulcer with a red pink wound bed, without slough. May also present as an intact or open/ruptured serum- filled or sero-sanginous filled blister. Presents as a shiny or dry shallow ulcer without slough or bruising*. This category should not be used to describe skin tears, tape burns, incontinence associated dermatitis, maceration or excoriation. *Bruising indicates deep tissue injury.

Classification of Pressure UlcersClassification of Pressure Ulcers
Category/Stage III: Full thickness skin loss
Full thickness tissue loss. Subcutaneous fat may be visible but bone, tendon or muscle are not exposed. Slough may be present but does not obscure the depth of tissue loss. May include undermining and tunneling. The depth of a Category/Stage III pressure ulcer varies by anatomical location. The bridge of the nose, ear, occiput and malleolus do not have (adipose) subcutaneous tissue and Category/Stage III ulcers can be shallow. In contrast, areas of significant adiposity can develop extremely deep Category/Stage III pressure ulcers. Bone/tendon is not visible or directly palpable.

Classification of Pressure UlcersClassification of Pressure Ulcers
Category/Stage IV: Full thickness tissue loss
Full thickness tissue loss with exposed bone, tendon or muscle. Slough or eschar may be present. Often includes undermining and tunneling. The depth of a Category/Stage IV pressure ulcer varies by anatomical location. The bridge of the nose, ear, occiput and malleolus do not have (adipose) subcutaneous tissue and these ulcers can be shallow. Category/Stage IV ulcers can extend into muscle and/or supporting structures (e.g., fascia, tendon or joint capsule) making osteomyelitis likely to occur. Exposed bone/muscle is visible or directly palpable.
Classification of Pressure UlcersClassification of Pressure Ulcers
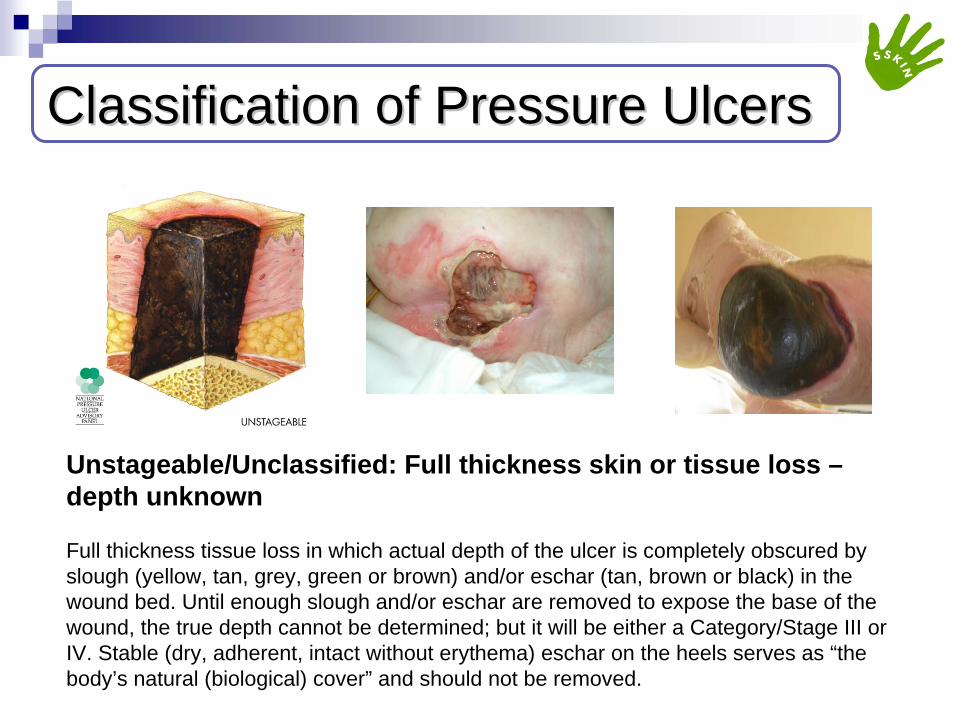
Unstageable/Unclassified: Full thickness skin or tissue loss – depth unknown
Full thickness tissue loss in which actual depth of the ulcer is completely obscured by slough (yellow, tan, grey, green or brown) and/or eschar (tan, brown or black) in the wound bed. Until enough slough and/or eschar are removed to expose the base of the wound, the true depth cannot be determined; but it will be either a Category/Stage III or IV. Stable (dry, adherent, intact without erythema) eschar on the heels serves as “the body’s natural (biological) cover” and should not be removed.

Classification of Pressure UlcersClassification of Pressure Ulcers
Suspected Deep Tissue Injury – depth unknown
Purple or maroon localized area of discoloured intact skin or blood-filled blister due to damage of underlying soft tissue from pressure and/or shear. The area may be preceded by tissue that is painful, firm, mushy, boggy, warmer or cooler as compared to adjacent tissue. Deep tissue injury may be difficult to detect in individuals with dark skin tones. Evolution may include a thin blister over a dark wound bed. The wound may further evolve and become covered by thin eschar. Evolution may be rapid exposing additional layers of tissue even with optimal treatment.

Differential DiagnosisDifferential Diagnosis
Pressure and shear
FrictionTrauma
Burn
Diabetic foot ulcer
Arterial/venous leg ulcer
Moisture lesion
Excoriation
Old wound
Shingles
Indentation of skinPhysical/chemical irritation
Scar
Abscess
Allergic reaction

Differential diagnosis: Differential diagnosis: Moisture LesionsMoisture Lesions
Photos: Welsh Wound Network, PUCLAS

How to prevent Moisture LesionsHow to prevent Moisture Lesions
Welsh wound network
• Avoid positioning patient on an area of redness (erythema) whenever possible
• Keep the skin clean and dry• Use a pH balanced skin cleanser• Do not massage or vigorously rub
skin that is at risk of pressure damage (shear)
• Implement an individualised continence management plan
• Cleanse the skin promptly following episodes of incontinence
• Protect skin with a barrier product in order to reduce the risk of pressure damage
NHS Midlands and East STP

SurfaceSurfaceSupport surfaces alone neither prevent nor heal pressure ulcers. They are used along side a management plan for pressure ulcer prevention and treatment. The following points should be considered:•Examine the appropriateness and functionality of the support surface on every encounter•Continue to reposition patients placed on a pressure redistribution support surface •Apply repose boots where necessary as this reduces the risk of pressure damage to the heels. Repose boots are designed for use in bed or with the feet elevated •Place legs on a pillow to ‘float heels’ off the bed•Use an ‘active support surface’ (overlay or pressure redistribution surface) for individuals at higher risk when frequent manual repositioning is not possible •Foam mattresses can be used for individuals with Category 1 and 2 pressure ulcers depending on their Braden score and use of clinical judgement

Keep MovingKeep Moving
Pressure ulcers cannot form without pressure on the skin and underlying tissues.
•Reposition all patients who are at risk of or have existing pressure ulcers (unless contraindicated)•When considering the frequency of repositioning your patient considerations should be given to:-Level of activity and mobility-General medical condition-Overall treatment objectives-Skin condition-Comfort -Encourage and educate patients and family/carers/friends of the importance of repositioning-Encourage independent repositioning if able

Keep Moving: RepositioningKeep Moving: Repositioning
• Reposition the patient in such a way that pressure is relieved or redistributed
• Avoid repositioning patient on bony prominences with existing pressure damage
• Avoid subjecting the skin to pressure and shear forces• Avoid positioning the patient directly onto medical devices such as tubes,
drainage systems or other foreign objects• Do not leave an individual on a bed pan longer than necessary• Use 30 degree tilted side-lying • Limit head-of-bed elevation to 30 degrees for patients on bed rest (unless
contraindicated)• Continue to reposition the individual regardless of the support surface (as
a minimum of 2-4 hours)• If seating is necessary for patients with pressure ulcers on the
sacrum/coccyx or ischia, limit seating to 3 times a day in periods of 60 minutes or less with a pressure relieving cushion in place.
Best practice management of Best practice management of Incontinence and MoistureIncontinence and Moisture
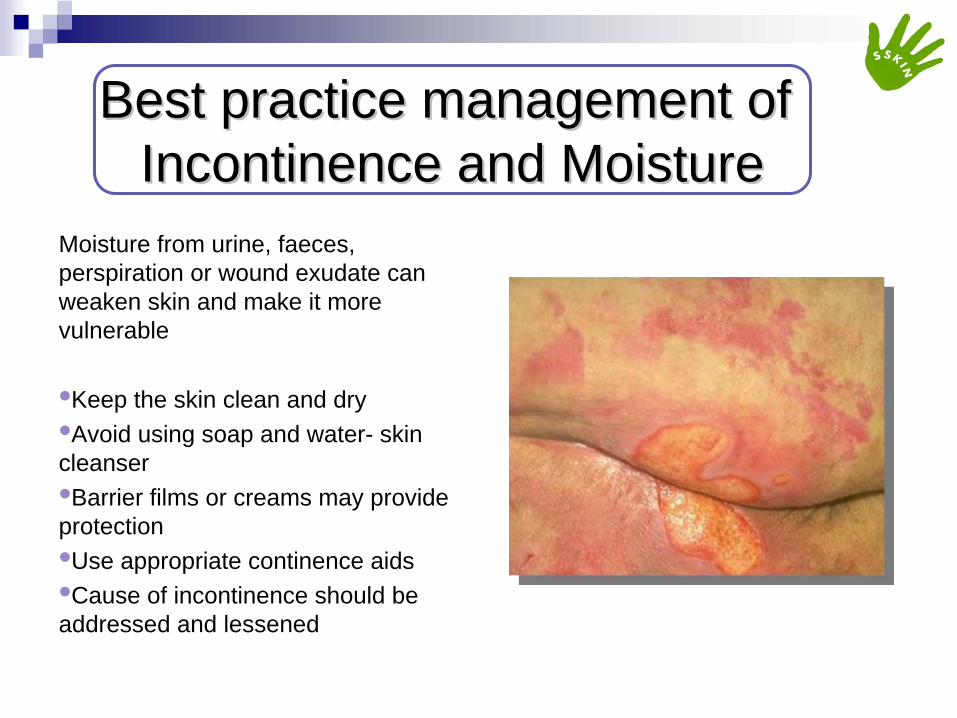
Moisture from urine, faeces, perspiration or wound exudate can weaken skin and make it more vulnerable
•Keep the skin clean and dry•Avoid using soap and water- skin cleanser•Barrier films or creams may provide protection•Use appropriate continence aids•Cause of incontinence should be addressed and lessened

NutritionNutrition
• Undertake a nutritional assessment as per hospital policy (5 days using MUST Tool)
• Consider referring patients screened to be at risk of malnutrition and patients with existing pressure ulcer to a dietician
• Assess the patients’ ability to eat independently • Use red trays where necessary• Ensure meals are in reach for patients who can feed
themselves• Provide enhanced foods and/or oral supplements
between meals if required (Discuss with medical team)

Process of ReportingProcess of Reporting
• Datix report all category 1, 2, 3 and 4’s• Safeguarding for all category 3 and 4’s• Medical Photography for all category 3 and 4’s• Tissue Viability referral (Electronic form on intranet) for
all Hospital - acquired category 2, 3 and 4’s• Tissue Viability referral for all community acquired
category 3 and 4’s• Duty of Candour for all category 3 and 4’s

Your Role in Your Role in Pressure Ulcer PreventionPressure Ulcer Prevention
Have You…

Any Questions?Any Questions?

Page 3- National Pressure Ulcer Advisory Panel, European Pressure Ulcer Advisory Panel and Pan Pacific Pressure Injury Alliance (2014) ‘Prevention and Treatment of Pressure Ulcers: Clinical Practice Guideline’. Cambridge Media: Perth, AustraliaPage 4- National Institute for Health and Care Excellence (2014) ‘Pressure ulcers: prevention and management of pressure ulcers’. Available at: https://www.nice.org.uk/guidance/cg179Page 5- Stop the Pressure (2013) ‘Stop the Pressure: Helping to prevent pressure ulcers’. Available at: http://nhs.stopthepressure.co.uk/Page 6, 7, - National Pressure Ulcer Advisory Panel, European Pressure Ulcer Advisory Panel and Pan Pacific Pressure Injury Alliance (2014) ‘Prevention and Treatment of Pressure Ulcers: Clinical Practice Guideline’. Cambridge Media: Perth, AustraliaPage 8- BJ,. and Bergstron (1988) ‘Braden Scale for predicting pressure sore risk’. Available at: www.bradenscale.comPage 12- NHS Midlands and East (2012) ‘Guidelines to support Pressure ulcer Bundle’. Available at: http://www.google.co.uk/url?url=http://nhs.stopthepressure.co.uk/Path/docs/Bundles%2520Guidelines%2520final%2520v2.pdf&rct =j&frm=1&q=&esrc=s&sa=U&ei=Jwg-VeKKO5G0aePHgdgG&ved=0CCsQFjAD&usg=AFQjCNFAG2n4pIPabEv-ix5CLckAb45IcgPage 13- C Brett (Revised 2015) ‘Intentional Rounding/SSKIN Bundle Form’. Ref 13/4749 from Medical IllustrationsPage 14- NHS Midlands and East (2012) ‘Guidelines to support Pressure ulcer Bundle’. Available at: http://www.google.co.uk/url?url=http://nhs.stopthepressure.co.uk/Path/docs/Bundles%2520Guidelines%2520final%2520v2.pdf&rct =j&frm=1&q=&esrc=s&sa=U&ei=Jwg-VeKKO5G0aePHgdgG&ved=0CCsQFjAD&usg=AFQjCNFAG2n4pIPabEv-ix5CLckAb45Icg National Pressure Ulcer Advisory Panel, European Pressure Ulcer Advisory Panel and Pan Pacific Pressure Injury Alliance (2014) ‘Prevention and Treatment of Pressure Ulcers: Clinical Practice Guideline’. Cambridge Media: Perth, AustraliaPage 15, 16, 17, 18, 19, 20, 21, 22, 23, - National Pressure Ulcer Advisory Panel, European Pressure Ulcer Advisory Panel and Pan Pacific Pressure Injury Alliance (2014) ‘Prevention and Treatment of Pressure Ulcers: Clinical Practice Guideline’. Cambridge Media: Perth, AustraliaPage 24, 25- International review. Pressure ulcer prevention: pressure, shear, friction and microclimate in context. A consensus document. London: Wounds International, 2010Page 27- Yates, S. (2012) ‘Differentiating between pressure ulcers and moisture lesions’. Wounds Essentials Vol 2.Page 28, 30, 31, 32, 33- National Pressure Ulcer Advisory Panel, European Pressure Ulcer Advisory Panel and Pan Pacific Pressure Injury Alliance (2014) ‘Prevention and Treatment of Pressure Ulcers: Clinical Practice Guideline’. Cambridge Media: Perth, AustraliaPage 30- (NRS-UK, 2014)
ReferencesReferences