storming and norming: sepsis, covid, and the critical
TRANSCRIPT

| health.ebsco.com1
Storming and Norming:
Sepsis, COVID, and the
Critical Importance of Early
Recognition and Response
Tuesday, September 15, 2020
To reduce background noise, all phone lines will
be muted during webinar.
Please submit questions via Q&A Panel on your
WebEx Console.
Following today’s webinar, all registrants will receive a follow-up
email from EBSCO Health with a copy of the presenter’s slides
and a link to a recording.
| health.ebsco.com2
Presenter
Diane Hanson MM, BSN, RN, FNAPChief Nursing Officer, EBSCO Clinical Decisions
Editor-in-Chief, Dynamic Health
@DianeHansonRN
After spending several years working in a hospital organization in various clinical and leadership
positions, Diane has been focused on improving quality and evidence-based practice at the point
of care through clinical decision support, health informatics and analytics. Diane brings over 25
years of experience in the healthcare industry to EBSCO Clinical Decisions, most recently as Vice
President of Product Strategy & Management at Vizient Inc. Diane is a published author and
speaker on evidence-based practice and clinical decision support. She holds a degree in nursing
from Grand Valley State University and a Masters in Management degree from Aquinas College.

| health.ebsco.com3
Presenter
Kathleen Walsh MSN, MBA, RN, CCRN Medical Writer & Lead Nurse Planner, Accreditation Programs
Dynamic Health
Kathleen Walsh is a nurse practitioner who serves as the Lead Nurse Planner for Dynamic
Health’s Nursing and Health Professions Continuing Education Department. She oversees the
accreditation and management for EBSCOs five largest accrediting agencies. Her background is
in surgical critical care nursing, focusing on trauma and organ transplant. Kathleen has taught
anatomy and physiology at the university level and worked as a hospital-based educator. Her
experience over the past 12 years at EBSCO as writer, senior editor, and team member with the
media group, is a great foundation for her work in our professional development programs.

| health.ebsco.com4
Presenter
Colleen Seeber-Combs MSN, RNSection Editor, Medical-Surgical
Dynamic Health
Colleen Seeber-Combs, MSN, RN, is a mastered-prepared registered nurse with 34 years of experience in a variety of settings. Colleen manages the medical-surgical collection for EBSCO’s Dynamic Health. She lives in Philadelphia, Pennsylvania, with her husband and two sons.

| health.ebsco.com5
Learning
Outcomes
• Review the medical and financial crisis
sepsis presents worldwide
• Recognize the causes and common clinical
symptoms of sepsis and septic shock
• Understand the best evidence elements of
the Hour-1 and Hour-6 treatment bundles
• Understand the role of pro-inflammatory
and anti-inflammatory cytokines in the
pathophysiology of sepsis
• Compare and contrast best practices for
Sepsis and Covid-19 according to the
latest guidelines

| health.ebsco.com6
Worldwide Impact of Sepsis
• Affects 45-50 million people annually worldwide, leading to 11 million deaths
• 1 in every 5 deaths worldwide is associated with sepsis
• Sepsis is the #1 cause of death in hospitals
• Single most expensive condition treated in hospitals
• #1 cause for readmissions– 20% of patients with sepsis are readmitted within
30 days
• Every 2.8 seconds someone dies from sepsis
• As many as 80% of sepsis deaths could be prevented with rapid diagnosis
and treatment

| health.ebsco.com7
Be
Sepsis
Smart
Take
The Test

| health.ebsco.com8
Mortality
increases
every hour
that treatment
is delayed
True False
| health.ebsco.com9
One can
only get
sepsis in the
hospital
True False

| health.ebsco.com10
Sepsis is
preventable True False
| health.ebsco.com11
Sepsis in a Nutshell…
Anyone can get an infection and almost
any infection and lead to sepsis.
Immune System Working Too Hard Sepsis
More is
NOT
Better!

| health.ebsco.com12
Sepsis – An Extreme Response to Infection
Former definition: Overwhelming and life-
threatening response to an infection, without
the appropriate and timely treatment, could
lead to organ failure, amputation, and death
2016: A life-threatening organ dysfunction
caused by a dysregulated host response to
infection
Rhodes, M.B., Evans, L.E., Alhazzani, W., et al. (2017)
Surviving Sepsis Campaign: International Guidelines for
Management of Sepsis and Septic Shock: 2016.
Critical Care Medicine, 45(3).

| health.ebsco.com13
Q: Why is
sepsis different
from other
infections?
A: “Aberrant or dysregulated
host response and presence
of organ dysfunction” (Your
immune system response is
out of control and causes
organ damage and death)Singer M. Deutschman, C.S., Seymour C.W., et al (2016)
The Third International Consensus Definition
for Sepsis and Septic Shock (Sepsis-3).
The Journal of American Medical Association, 315(8)
| health.ebsco.com14
Sepsis: Who is at Risk
• Sepsis is non-discriminatory. There is no gender or race bias in
its victims. However, it does seek out the most vulnerable
patients
• Who is most at risk?
− Very young (children < 1 year of age)
− Older adults (> 65 years of age)
− Pregnant women (causes nearly 260,000 maternal deaths worldwide)
− People with chronic conditions (diabetes, kidney or lung disease)
− People with weakened immune systems (cancer, multiple sclerosis,
AIDS)

| health.ebsco.com15
The NEW Road to Sepsis
SIRS (SEP2)
Any 2 of the following:
• Temp > 38.3 C/100.9 F
or < 36.0 C/96.8 F
• HR > 90 beats/min
• RR > 20 breaths/min
• WBC > 12,000/mm3
(leukocytosis)
or < 4,000/mm3
(leukopenia) or 10%
Bands/Neutrophils
(PCO2 < 32 mmHg
[norm 35-45])
Sepsis (SEP3)
Confirmed or suspected
infection
+
2 of more qSOFA criteria*
*Issued by SCC
Consensus Committee but not
recommended as best practice
by SSC Guideline group
Severe Sepsis(SEP2)
Sepsis
+
Evidence of Organ
Dysfunction(Lactate >4 mmol)
Septic Shock (SEP3)
MODS* Amputation
Long-Term Morbidity)
Sepsis
+
Refractory Hypotension
(< SBP 90 mmHg)
+
Lactate > 2 mmol/L
Death
*MODS-Multiple Organ Dysfunction Syndrome
X X
Stop

| health.ebsco.com16
SOFA and qSOFA
qSOFA(Quick SOFA Score) “HAT”
Fast and easy bedside criteria to predict
morbidity/mortality in adult patients with sepsis (2 elements + known infection suggests organ dysfunction)
❑H – Hypotension (SBP 100 mmHg)
❑A – Altered mental status (GCS < 15)
❑T – Tachypnea (RR ≥ 22 breaths/min)
SOFA (Sequential Organ Failure Assessment Score)
Indicates severity of organ dysfunction by evaluating:
❑ Cardiovascular system
❑ CNS
❑ Coagulation
❑ Liver function
❑ Renal function
❑ Respiratory function
Note: qSOFA has been found to be poorly sensitive but reasonably specific for mortality risk.
SIRS ranks higher for screening purposes.
Annals of Internal Med 6 Feb 2018, 168(4), 266-275

| health.ebsco.com17
Sepsis Definition Common Clinical Symptoms
Confirmed or
Suspected Infection
Refractory
Hypotension*(SBP < 90 despite fluid resuscitation)
SEPSIS
Shivering (rigors), fever, very cold
Extreme pain (“worst ever”) or general discomfort
Pale or discolored, clammy or sweaty skin
Sleepy, difficult to rouse, confused, disoriented
“I feel like I might die” (sense of doom)
Shortness of breath
Abnormal heart rate
S
E
P
S
I
S
Factoids…
Q: Is sepsis the same as septicemia?
A: No. Septicemia (known as blood poising) is the condition
of bacteria entering the bloodstream. Sepsis is the
overwhelming of life-threatening response to infection.
Q: Is septicemia the same as bacteremia?
A: No. Bacteremia is the presence of bacteria in the blood
(likely occurs each time we brush our teeth). Septicemia is
the presence and multiplication of bacteria in the blood (has
a clinical component that involves inflammation).
Mortality
14.9%

| health.ebsco.com18
Septic Shock
SepsisTwo or More
qSOFA Criteria(Hypotension, ALOC, Tachypnea)
Lactate > 2 mmol/L
Septic Shock Risk Factors
Suppressed immune system
Extreme age
People who’ve revived an organ transplant
Surgical procedures
Indwelling devices
Sickness
S
E
P
S
I
S
Mortality
34.2%

| health.ebsco.com19
Sepsis is a Healthcare Crisis and Requires Emergency Response
More people have heard about Ebola (non-existent in the U.S.) than
sepsis. More than 40% of American adults DO NOT KNOW what sepsis is!
Family and Friends Message!
If you suspect sepsis (observe a combination of the
common S/S), see your medical professional
immediately, CALL 911, or go to a hospital with an
advocate and say, “I AM CONCERNED ABOUT
SEPSIS.” Don’t just sit in the ED waiting room, hoping
someone will recognize sepsis. TIME IS TISSUE!!
Sepsis Cliff
• Rapid deterioration is common in septic patients
• 2/3 of patients in the ED with normal BP in triage became
hypotensive (MAP< 65 mmHg) within 2 ½ hours *
*Shirvanian, et al. Sepsis Cliff: Development
of Hypotension While in the Emergency
Department

| health.ebsco.com20
Mortality as
a function of
failing organs
Sepsis
Severe Sepsis
Septic Shock
Incidence
37%
30%
15%
ICU Mortality
27%
32%
54.1%
Organ dysfunction
evidence by ≥
One of the Following:
• SBP < 90 or NAP < 65, of SBP
decreased of more than
40mmHg from previous SBP
• Creatinine > 2.0 or urine output <
0.5 ml/kg/hour for 2 hours
• Bilirubin > 2 mgldl
• Platelet count < 100,000
• INR > 1.5 or aPTT > 60 sec
• Lactate > 2 mmol/L

| health.ebsco.com21
AHRQ Failure to Rescue Definition
• Inability to save a patient’s life (or prevent a permanent disability)
after the development of a complication that was not present on
admission
• Failure to Recognize: Vital signs or status deteriorating over time
with no response by caregiver
• Failure to Communicate: Delay in physician response to a call for
assistance; inadequate communication between caregivers
• Failure to Plan: Deterioration of a patient while waiting for a transition
in care
AHRQ.org (Agency for Healthcare Research and Quality)

| health.ebsco.com22
The Bundles
Sepsis/Septic Shock
Hour-1* Treatment Bundle
• Draw initial lactate level**
• Draw blood cultures prior to antibiotics (to be
drawn from 2 different areas)
• Administer broad spectrum antibiotics (administer asap w/in 1 hour if possible)
• Rapid administration of 30 mL/kg crystalloid
for hypotension (≥ 65 mmHg) or lactate ≥ 4
mmol/L• Pt weight/kg: ______
• Crystalloid (NS) total volume: ___mL
• Draw initial lactate level**
*Time zero is measured from triage in ED or from earliest
chart annotation consistent with all elements of septic
shock
**Repeat lactate if > 2 mmol/L
Sepsis/Septic Shock
Hour-6* Treatment Bundle
• Vasopressor for refractory hypotension to
maintain MAP ≥ 65 mmHg
• Reassess volume status and tissue perfusion
if persistent hypotension (< 65 mmHg) or if
initial lactate ≥ 4 mmol/L
• Redraw lactate if initial level elevated (> 2
mmol/L
• Document:
• CVP measurement
• ScvO2 measurement
• Bedside cardiovascular ultrasound
• Passive leg raise or fluid challenge
• CVP (central venous pressure) – poor predictor of fluid
responsiveness
• ScvO2 (central venous oxygen saturation) - used to
detect change in oxygen delivery and consumption
• PLR (raising both legs 45-10% increase in pulse
pressure of arterial tracing) 11x more likely to respond
to fluids

| health.ebsco.com23
What’s behind the Hour-1 SEP3 controversy?
• Triage time not realistic – many patients develop organ
dysfunction over time, not within 1 hour in ED
• Foster unnecessary abx administration
• Drown patients with fluids - risk to CHF and ESRD patients)
• Fear that CMS would rapidly adopt 1-hour bundle and facilities
would be unable to comply
Pulmonary-Critical Care docs gathered 6,000
signatures to protest 1-hour bundle

| health.ebsco.com24
Early Therapy = Survival

| health.ebsco.com25
So, how do we save lives?
• Sepsis alerts for sepsis and septic shock – EMR Software
• Hardwiring bundles for early implementation
• Physician order sets and nursing standardized procedures
• Automatic lactate orders for lab redraws, critical result notification
for LA >4
• Screen all patients in ED and once a shift on the INP units
• Critical result notification for LA >4
• Immediate access (in the units) to broad spectrum antibiotics
• Code Sepsis (Code Sepsis varies with facility. Typically includes Sepsis 1-Hour Bundle, rapid evaluation by attending
clinician supported by infectious disease specialist, and initiation of a Sepsis hand-off form in preparation for transfer to ICU)

| health.ebsco.com26
Post-Sepsis
Symptoms
(PSS)*Requires
Ongoing
ManagementSepsis survivors…
• Have a shortened life-expectancy
• Suffer life-long consequences of sepsis – 38 sepsis-related
amputations daily, psychological and cognitive disabilities
• Are 42% are more likely to commit suicide
- Global Sepsis Alliance
| health.ebsco.com27
YOU Can Make a Difference!
• TIMELY screening of
patients for sepsis
• TIMELY identification of
septic patients
• TIMELY treatment of septic
patients
Sepsis MnemonicUse this mnemonic to help improve
sepsis outcomes
S – SOFA Score – Calculate it!
E – Early Recognition
P – Protocols – Follow Them!
S – Start Treatment Right Away
I – Improve Outcomes
S – Share Results

| health.ebsco.com28
A Closer Look at Pathophysiology
This Photo by Unknown Author is licensed under CC BY-SA
| health.ebsco.com29
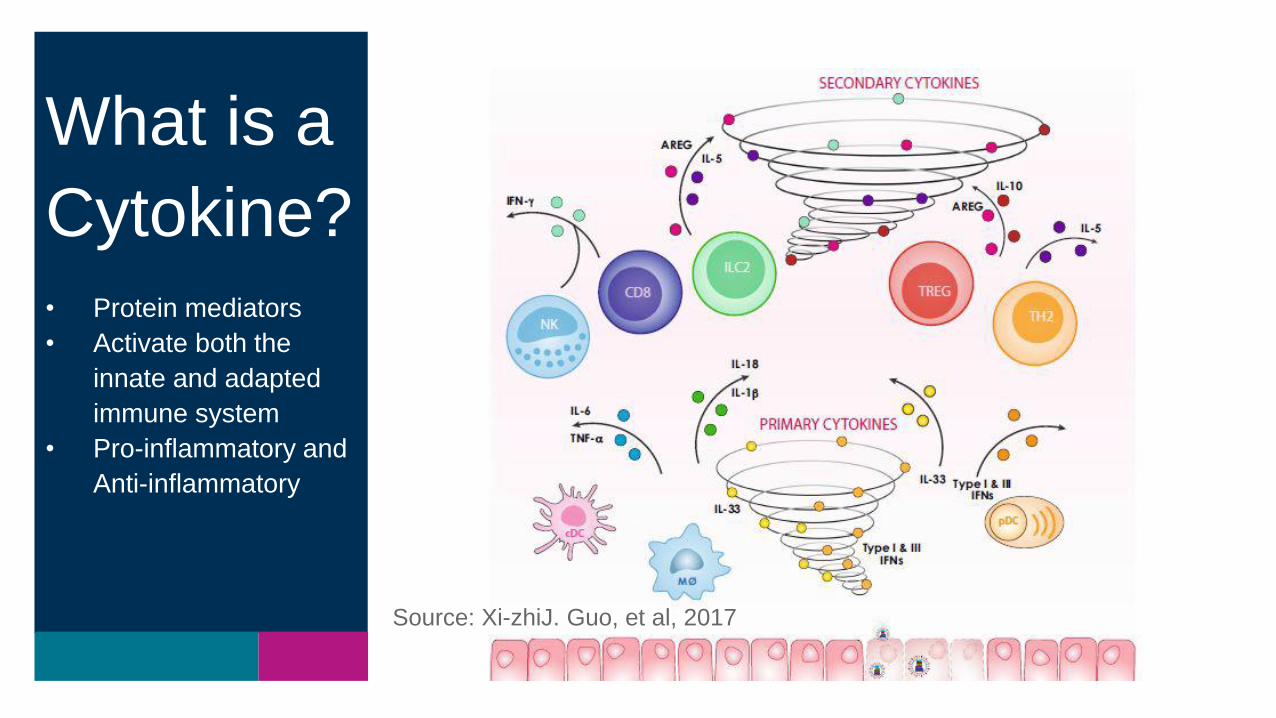
Source: Xi-zhiJ. Guo, et al, 2017
What is a
Cytokine?
-Protein mediators
-Activate both the
innate and adapted
immune system
-Pro-inflammatory and
Anti-inflammatory
What is a
Cytokine?• Protein mediators
• Activate both the
innate and adapted
immune system
• Pro-inflammatory and
Anti-inflammatory

| health.ebsco.com30

| health.ebsco.com31
Proinflammatory cytokines
Anti-inflammatory cytokines
Pathophysiology
| health.ebsco.com32
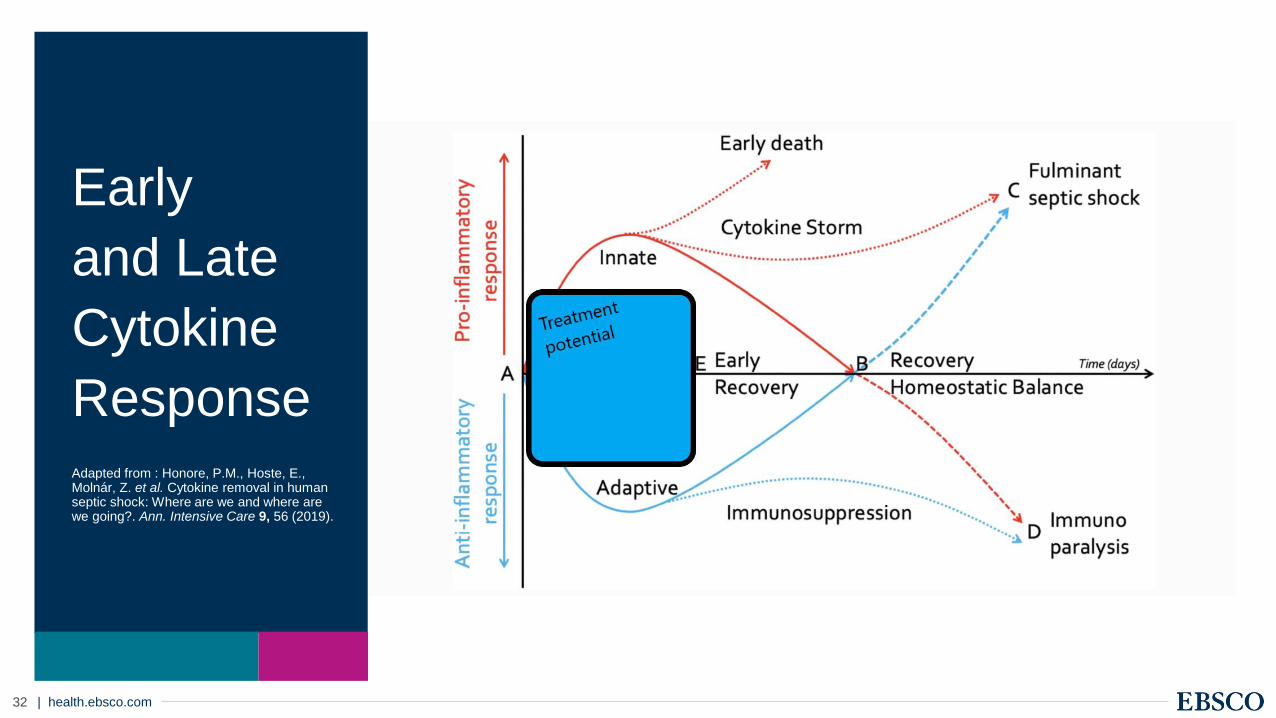
Early
and Late
Cytokine
ResponseAdapted from : Honore, P.M., Hoste, E., Molnár, Z. et al. Cytokine removal in human septic shock: Where are we and where are we going?. Ann. Intensive Care 9, 56 (2019).
| health.ebsco.com33
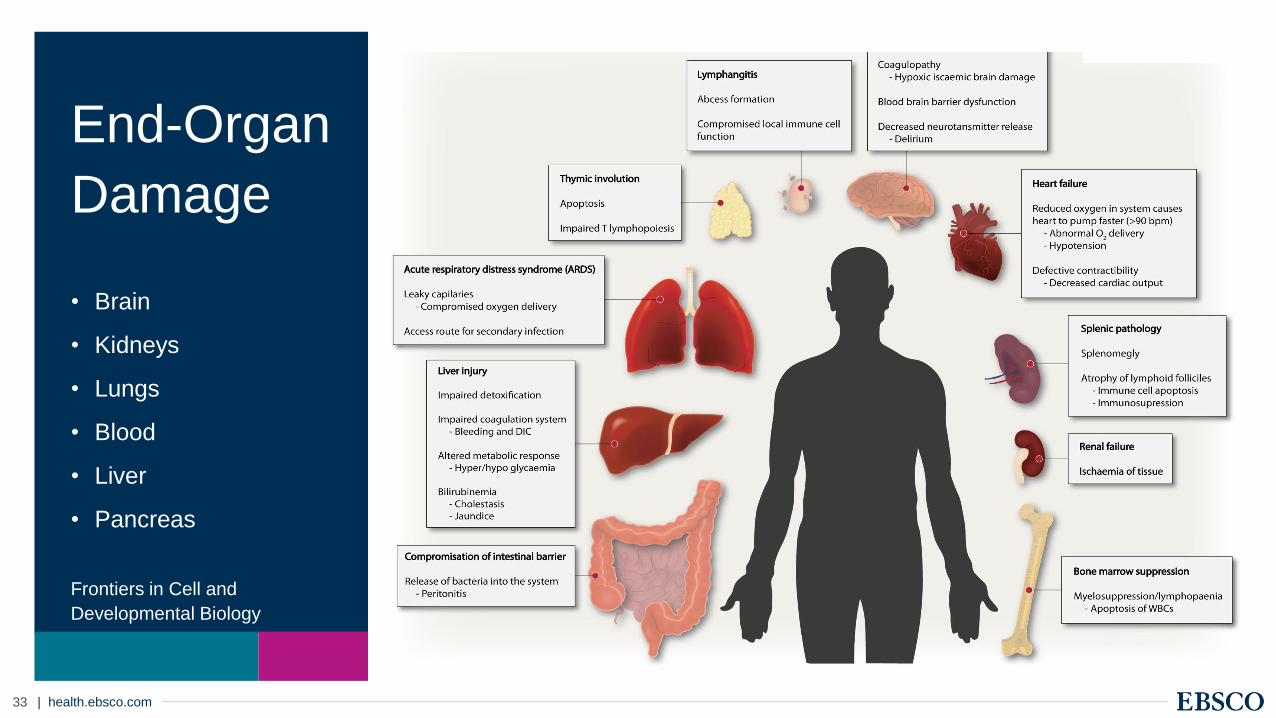
End-Organ
Damage
• Brain
• Kidneys
• Lungs
• Blood
• Liver
• Pancreas
Frontiers in Cell and
Developmental Biology

| health.ebsco.com34
ARDS

| health.ebsco.com35
Wiersinga WJ, Rhodes A, Cheng AC, Peacock SJ, Prescott HC. (COVID-19): A Review
[published online ahead of print, 2020 Jul 10]. JAMA. 2020

| health.ebsco.com36
DIC
Baishideng Publishing Group Inc. All
rights reserved. World J Crit Care
Med. May 4, 2015).

| health.ebsco.com37
Sepsis
Phenotypes
Alpha: This was the most common, least fatal
Beta: Older adults most chronic illnesses and
renal dysfunction.
Gamma: Elevated measures of inflammation
and pulmonary dysfunction.
Delta: Least common liver dysfunction and
shock highest in-hospital mortality rate
| health.ebsco.com38
COVID-19COVID-19

| health.ebsco.com39
1.Crystalloids
2.Avoid hydroxyethyl starch
3.Avoid dopamine
4.Supplemental O2 for Sat less
than 92%
5.Avoid incremental PEEP
SSC COVID-19 Guidelines and Sepsis

| health.ebsco.com40
COVID-19
Guidelines
• Fitted N-95 masks or
respirators
• Neg pressure rooms
• Vasopressin for
second line agent
• Target O2 sat (92-
96%)
• High flow oxygen
• Higher PEEP
• Careful use of fluids

| health.ebsco.com41
Surviving
Sepsis
Campaign
survivingsepsis.org
• Since its inception in 2002, the Campaign has
achieved several key milestones.
• Goals of Campaign to reduce mortality from sepsis
using a 7-point agenda:
• Building awareness of sepsis
• Improving diagnosis
• Increasing the use of appropriate treatment
• Educating healthcare professionals
• Improving post-ICU and discharge care
• Developing guidelines of care
• Implementing a performance improvement
program

| health.ebsco.com42
Questions?
Kathleen Walsh MSN, MBA, RN, CCRN
Colleen Seeber-Combs, MSN, RN
Diane Hanson, MM, BSN, RN, FNAP
| health.ebsco.com43
References
• Alhazzani W, Møller MH, Arabi YM, et al. Surviving Sepsis Campaign:
Guidelines on the Management of Critically Ill Adults with Coronavirus
Disease 2019 (COVID-19). Crit Care Med. 2020;48(6):e440-e469.
doi:10.1097/CCM.0000000000004363
• Cancer Therapy Advisor: Pediatric Respiratory Failure – Acute Hypoxemic
Respiratory Failure – ARDS
• Guo XJ, Thomas PG. New fronts emerge in the influenza cytokine storm.
Semin Immunopathol. 2017;39(5):541-550. doi:10.1007/s00281-017-0636-y
• Henderson LA, Canna SW, Friedman KG, et al. American College of
Rheumatology Clinical Guidance for Pediatric Patients with Multisystem
Inflammatory Syndrome in Children (MIS-C) Associated with SARS-CoV-2
and Hyperinflammation in COVID-19. Version 1 [published online ahead of
print, 2020 Jul 23]. Arthritis Rheumatol. 2020;10.1002/art.41454.
doi:10.1002/art.41454
• Honore, P.M., Hoste, E., Molnár, Z. et al. Cytokine removal in human septic
shock: Where are we and where are we going?. Ann. Intensive Care 9, 56
(2019
• Howell MD, Davis AM. Management of Sepsis and Septic Shock. JAMA.
2017;317(8):847–848. doi:10.1001/jama.2017.0131
• Nedeva C, Menassa J, Puthalakath H. Sepsis: Inflammation Is a Necessary
Evil. Front Cell Dev Biol. 2019;7:108. Published 2019 Jun 20.
doi:10.3389/fcell.2019.00108
• Prescott HC, Girard TD. Recovery From Severe COVID-19: Leveraging the
Lessons of Survival From Sepsis. JAMA. 2020;324(8):739-740.
doi:10.1001/jama.2020.14103
• Rhodes A, Evans LE, Alhazzani W, et al. Surviving Sepsis Campaign:
International Guidelines for Management of Sepsis and Septic Shock: 2016.
Intensive Care Med. 2017;43(3):304-377. doi:10.1007/s00134-017-4683-6
• Seymour CW, Kennedy JN, Wang S, et al. Derivation, Validation, and
Potential Treatment Implications of Novel Clinical Phenotypes for Sepsis.
JAMA. 2019;321(20):2003-2017. doi:10.1001/jama.2019.5791
• Singer M, Deutschman CS, Seymour CW, et al. The Third International
Consensus Definitions for Sepsis and Septic Shock (Sepsis-3). JAMA.
2016;315(8):801-810. doi:10.1001/jama.2016.0287
• Sinha P, Matthay MA, Calfee CS. Is a "Cytokine Storm" Relevant to COVID-
19? [published online ahead of print, 2020 Jun 30]. JAMA Intern Med.
2020;10.1001/jamainternmed.2020.3313.
• Venet F, Rimmelé T, Monneret G. Management of Sepsis-Induced
Immunosuppression. Crit Care Clin. 2018;34(1):97-106.
doi:10.1016/j.ccc.2017.08.007
• Wiersinga WJ, Rhodes A, Cheng AC, Peacock SJ, Prescott HC. (COVID-
19): A Review [published online ahead of print, 2020 Jul 10]. JAMA. 2020