strategies for treating gout gout dr. sultan al-mogairen assistant professor & consultant...
Post on 21-Dec-2015
225 views
TRANSCRIPT

STRATEGIES FOR STRATEGIES FOR TREATINGTREATING
GOUTGOUT
Dr. Sultan Al-MogairenDr. Sultan Al-MogairenAssistant Professor & ConsultantAssistant Professor & Consultant
Rheumatology DivisionRheumatology Division

Gout is clinical syndrome with Gout is clinical syndrome with monosodium urate deposition monosodium urate deposition characterized biochemically by characterized biochemically by extracellular urate supersaturation and extracellular urate supersaturation and clinically manifested by arthritis, tophi clinically manifested by arthritis, tophi and uric A nephrolithiasis.and uric A nephrolithiasis.
Gout continued to be a healthy problem Gout continued to be a healthy problem despite the availability of effective despite the availability of effective therapy.therapy.

EpidemiologyEpidemiology
In the West, the most frequent In the West, the most frequent microcrystalline arthritis affect microcrystalline arthritis affect approximately 0.5 to 2.8 of adult men and approximately 0.5 to 2.8 of adult men and 0.2 to 0.6% of adult women. The highest 0.2 to 0.6% of adult women. The highest incidence of Gout occurs between 30 & 45 incidence of Gout occurs between 30 & 45 yrs of age in men and between 55 & 70 yrs yrs of age in men and between 55 & 70 yrs of age in women. Prevalence of Gout of age in women. Prevalence of Gout increased in countries with a high standard increased in countries with a high standard changing in diet, lifestyle, increased use of changing in diet, lifestyle, increased use of thiazid diuretics and Aspirin. A review in thiazid diuretics and Aspirin. A review in Saudi Arabia, a population with rare alcohol Saudi Arabia, a population with rare alcohol consumption revealed prevalence of HPU consumption revealed prevalence of HPU 8.42% and no cases of Gout.8.42% and no cases of Gout.

CLINICAL FEATURESCLINICAL FEATURES♦♦More in male and in elderlyMore in male and in elderly
♦♦ More equal gender distributionMore equal gender distribution
♦♦ About 80% of initial attack are monoarticular.About 80% of initial attack are monoarticular.
♦♦ Polyarticular first attack are more common in Polyarticular first attack are more common in elderly women and in patients with Gout elderly women and in patients with Gout accompanying myeloproliferative disorder or the accompanying myeloproliferative disorder or the use of cyclosporin.use of cyclosporin.
♦♦ Common sites include instep, ankle, heel, knee, Common sites include instep, ankle, heel, knee, elbow (olecranon bursa) wrist & fingerelbow (olecranon bursa) wrist & finger
♦♦ Rare sites: shoulders, sternoclav, spine, Rare sites: shoulders, sternoclav, spine, sacroiliac and hips.sacroiliac and hips.
There is an association with the following:There is an association with the following:
-- DM, hyperlipidemia, obesity, HTN, renal DM, hyperlipidemia, obesity, HTN, renal impairment, diuretic, and ethanol consumption. impairment, diuretic, and ethanol consumption.































MANAGEMENTMANAGEMENT
Aims of TherapyAims of Therapy1.1. Anti-inflammatoryAnti-inflammatory
2.2. Anti-hyperuricemiaAnti-hyperuricemia
3.3. ProphylacticProphylactic
4.4. Nutritional strategiesNutritional strategies
5.5. Avoid ethanol consumption and Avoid ethanol consumption and drugs inducing drugs inducing HPUHPU
6.6. Prevention and reversal of Prevention and reversal of morbid morbid consequences of HPT, hyperlipidconsequences of HPT, hyperlipid

ANTI-INFLAMMATORYANTI-INFLAMMATORY
NSAID, Colchicine, CSTNSAID, Colchicine, CST
♦♦Do not reverse HPU or urate deposition.Do not reverse HPU or urate deposition.
♦♦Often reverse pain and inflammation and Often reverse pain and inflammation and disability within several days rather than disability within several days rather than several weeks as in untreated patients.several weeks as in untreated patients.
♦♦Best response if started in 1Best response if started in 1stst few hrs and if few hrs and if patient well educated give instruction for Tt patient well educated give instruction for Tt with 1with 1stst twinge to be terminated in 1 to 3 twinge to be terminated in 1 to 3 days or colchicine 0.6 mg/hr till relief or days or colchicine 0.6 mg/hr till relief or total dose 6 mg or S/E, or Indomethacin 50 total dose 6 mg or S/E, or Indomethacin 50 mg x 3 & other NSAID alternative routes mg x 3 & other NSAID alternative routes PR (NSAID). PR (NSAID).

Regarding NSAIDS, no clear Regarding NSAIDS, no clear advantages of one over another.advantages of one over another.
NSAIDNSAID ColchicineColchicine
Effect: More predictableEffect: More predictable Unpredictable and Unpredictable and when startedwhen started
after 1after 1stst 24 hr, decreased 24 hr, decreased thera-thera-
peutic effectpeutic effectGenerally, better toleratedGenerally, better tolerated Narrow benefit to Narrow benefit to
toxicity ratiotoxicity ratioif normal kidif normal kid (abdp.) (abdp.) Onset: 1 hr.Onset: 1 hr. Slow 12 hrs.Slow 12 hrs.CostCost CheaperCheaper

Once anti-HPU drugs has been initiated, it Once anti-HPU drugs has been initiated, it should not be interrupted during acute should not be interrupted during acute attacksattacks..
CST after securing Dx & r/o infection ifCST after securing Dx & r/o infection if::
11..Co-existing medical illness contraindicating Co-existing medical illness contraindicating 11stst line (NSAID & Colchicine), or line (NSAID & Colchicine), or
22..Due to intolerance to them, use steroid IV, Due to intolerance to them, use steroid IV, IM or IA according to number of joints IM or IA according to number of joints involvedinvolved..
33..Precaution for IA inj if patient has skin Precaution for IA inj if patient has skin infection or on anticoagulant. However, the infection or on anticoagulant. However, the effect of CST are inconsistent and rebound effect of CST are inconsistent and rebound attacks after Tt D/C are frequently seenattacks after Tt D/C are frequently seen..


Potential drawbacks of ACTH:Potential drawbacks of ACTH:
1.1. Depends on response of Depends on response of ΔΔ and and might bemight be
suboptimal if on steroid suboptimal if on steroid previously.previously.
2.2. Failure to deliver precise Failure to deliver precise dose.dose.
3.3. Increased release of Androgen Increased release of Androgen andand
mineralo cort.mineralo cort.


PROPHYLAXIS FOR ACUTE ATTACKS PROPHYLAXIS FOR ACUTE ATTACKS DURING INITIATION OF ANTI-HPU DRUGSDURING INITIATION OF ANTI-HPU DRUGS
Increased urinary Ur A excreted early in the Increased urinary Ur A excreted early in the course of uricosuric Tt can promote course of uricosuric Tt can promote (urinary stone formation).(urinary stone formation).
In addition, acute fall in S. urate conc often In addition, acute fall in S. urate conc often precipitate (Acute Gouty Arthritis).precipitate (Acute Gouty Arthritis).
Mech: Uncertain, but probably with Mech: Uncertain, but probably with decreased S. Ur A PMNs more efficient in decreased S. Ur A PMNs more efficient in phagocytosis.phagocytosis.

Risks of relapse can be Risks of relapse can be minimized by long-term use of:minimized by long-term use of:
1.1. Colchicine orColchicine or
2.2. NSAIDNSAID
Colchicine induced neuromyopathies and Colchicine induced neuromyopathies and NSAID induced PUD and Rend imp. by NSAID induced PUD and Rend imp. by
D/C drugs after persistent D/C drugs after persistent normouricemia.normouricemia.

Others said that pot toxicity of Others said that pot toxicity of prolonged use of Colchicine prolonged use of Colchicine (neuropathies, myelotoxicity) and the (neuropathies, myelotoxicity) and the fact that the only minority (10 to 15%) fact that the only minority (10 to 15%) of patients develop flare-up of Gouty of patients develop flare-up of Gouty Arthritis. After initiation of Allup. or Arthritis. After initiation of Allup. or uricosuric Tt, instead, many clinicians uricosuric Tt, instead, many clinicians advocate the temporary use of advocate the temporary use of supplemental NSAID or Colchicine to supplemental NSAID or Colchicine to control these attacks.control these attacks.


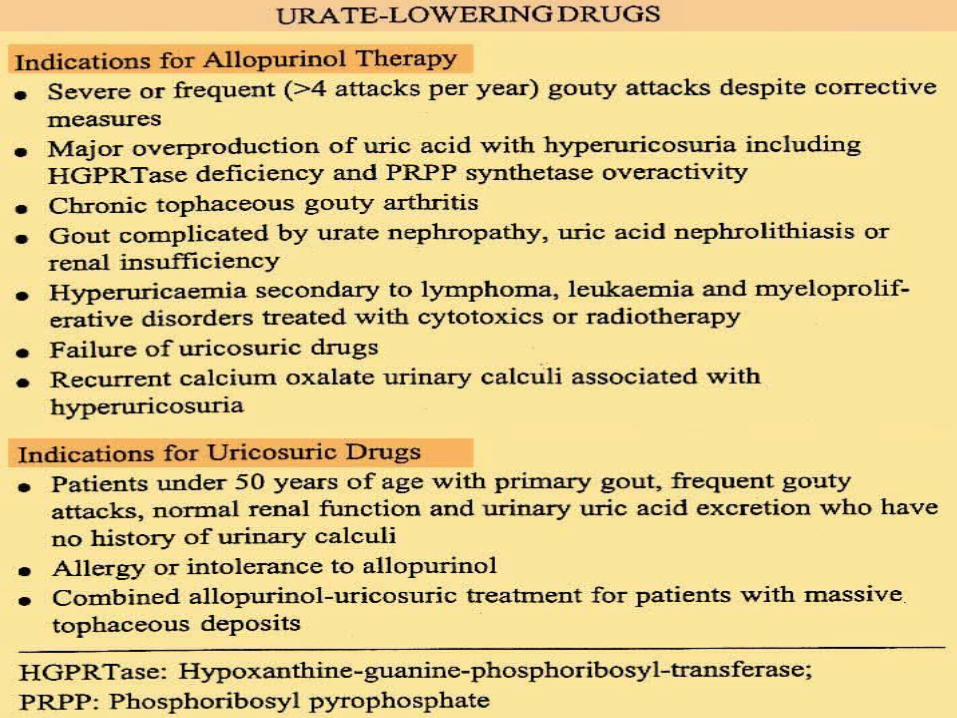
ANTIHYPERURICEMIA DRUGSANTIHYPERURICEMIA DRUGS
Goals: To reduce and maintain S. urate not Goals: To reduce and maintain S. urate not just to just to within normal range but within normal range but to the mid to lowerto the mid to lower
half of normal range (6.8 mg/dL = half of normal range (6.8 mg/dL = 404 404 mmol/L) below range of which mmol/L) below range of which S. urate S. urate saturate the extracellular saturate the extracellular fluid (6.8 mg/dL=fluid (6.8 mg/dL=
404 mmol/L).404 mmol/L).
This will prevent the gouty attack and This will prevent the gouty attack and promotepromoteresorption of tophaceous deposits.resorption of tophaceous deposits.

In the absence of clear indication In the absence of clear indication for Tt with Allup, some for Tt with Allup, some Rheumatologist recommend Rheumatologist recommend uricosuric because it is safe and uricosuric because it is safe and do not influence purine and do not influence purine and pyramidine metabolism.pyramidine metabolism.


DIETDIET
A severely purine restricted diet has A severely purine restricted diet has traditionally been recommended for traditionally been recommended for patient with Gout. Such a diet can patient with Gout. Such a diet can reduce urinary Ur A excretion by 200 reduce urinary Ur A excretion by 200 to 400 mg/day. However, mean S. to 400 mg/day. However, mean S. urate conc decrease only about 1 urate conc decrease only about 1 mg/dL (59 µmol/L).mg/dL (59 µmol/L).

Diet with restricted purine and protein Diet with restricted purine and protein contents are unpalatable and often contents are unpalatable and often neither practical nor effective in the neither practical nor effective in the management of HPU and Gout in management of HPU and Gout in patients with normal dietary habit. patients with normal dietary habit. Furthermore, with availability of Furthermore, with availability of potent anti-HPU drugs, this dietary potent anti-HPU drugs, this dietary approach is rarely employed except approach is rarely employed except in those with severe renal in those with severe renal insufficiency or intolerance to insufficiency or intolerance to pharmacologic therapy. pharmacologic therapy.

If dietary changes are employed to If dietary changes are employed to manage Gout, it may be preferable to manage Gout, it may be preferable to recommend increasing dietary recommend increasing dietary protein intake from low fat dairy protein intake from low fat dairy product and to decrease the amount product and to decrease the amount of red meat and fish ingestion.of red meat and fish ingestion.



THANK YOUTHANK YOU

آية اإلسراء آية سورة اإلسراء 2424--2323سورة
ا� اًن �ْح�َس� ِإ �ِن� �َد�ْي �َو�اِل �اِل َو�ِب �اُه� �ْي ِإ � �َّال ِإ � �َد�َوا �ْع�ُب َت � َّال� َأ �َك� ِب َر� �ا َو�َق�َض�ى اًن �ْح�َس� ِإ �ِن� �َد�ْي �َو�اِل �اِل َو�ِب �اُه� �ْي ِإ � �َّال ِإ � �َد�َوا �ْع�ُب َت � َّال� َأ �َك� ِب َر� َو�َق�َض�ى
�ُق�ل َت � َف�َال �ُه�َم�ا �َال ِك َو�� َأ ْح�َد�ُه�َم�ا
� َأ �َر� �ُب �ِك اِل ِع�نَد�َك� �َغ�ِن� �ُل �ُب ْي �َّم�ا �ُق�ل ِإ َت � َف�َال �ُه�َم�ا �َال ِك َو�� َأ ْح�َد�ُه�َم�ا
� َأ �َر� �ُب �ِك اِل ِع�نَد�َك� �َغ�ِن� �ُل �ُب ْي �َّم�ا ِإ�َر�ْيَم�ا ِك � َق�َو�َّال �ُه�َم�ا ِل َو�َق�ل ُه�َم�ا �ُه�َر� �ن َت � َو�َّال ٍّف0
� َأ �ُه�َم�آ �َر�ْيَم�ا ِل ِك � َق�َو�َّال �ُه�َم�ا ِل َو�َق�ل ُه�َم�ا �ُه�َر� �ن َت � َو�َّال ٍّف0� َأ �ُه�َم�آ ِل
3ِّب َر� َو�َق�ل ْح�َم�ِة� اِلَر� َّم�ِن� اِلُّذ�ِّل3 �اَح� ن َج� �ُه�َم�ا ِل ِّب3 َو�اْخ�ِف�ْض� َر� َو�َق�ل ْح�َم�ِة� اِلَر� َّم�ِن� اِلُّذ�ِّل3 �اَح� ن َج� �ُه�َم�ا ِل َو�اْخ�ِف�ْض�ا َص�َغ�يَر� �ي �اًن �ي ِب َر� �َم�ا ِك ْح�َم�ُه�َم�ا ا اَر� َص�َغ�يَر� �ي �اًن �ي ِب َر� �َم�ا ِك ْح�َم�ُه�َم�ا اَر�

. اِلصَوت َرَفع َوِعَدم اِلِكَالم َفي .اِلتُلطف اِلصَوت َرَفع َوِعَدم اِلِكَالم َفي اِلتُلطف َفي َّمَرات ثَالث األَقل ِعُلى زْياَرَتُهَما ِعُلى َتحَرص َّمْعُهَما َتَسِكِن ِلم َفي ِإذا َّمَرات ثَالث األَقل ِعُلى زْياَرَتُهَما ِعُلى َتحَرص َّمْعُهَما َتَسِكِن ِلم ِإذا
األسُبَوع.األسُبَوع.. َوًنِفَسيتُهَما ُهَما َّمشاِعَر ِعُلى .اِلحَرص َوًنِفَسيتُهَما ُهَما َّمشاِعَر ِعُلى اِلحَرص. ًنِفس ِبطيب اِلَماِليِة ْحاَجاَتُهَما .َتُلُبيِة ًنِفس ِبطيب اِلَماِليِة ْحاَجاَتُهَما َتُلُبيِة. َّمنَك ْيحتاَجاًنه َّما طُلب َفي َتَردد َوَّال ِبحَرج ْيشْعَران .َّال َّمنَك ْيحتاَجاًنه َّما طُلب َفي َتَردد َوَّال ِبحَرج ْيشْعَران َّال. َوسياَرة َوسائق َجَواِّل َّمِن اإلَتصاِّل َوسائل َتَوَفيَر ِعُلى .اِلحَرص َوسياَرة َوسائق َجَواِّل َّمِن اإلَتصاِّل َوسائل َتَوَفيَر ِعُلى اِلحَرص. سنَوْيِة ُهَدْيِة .ِإُهَدائُهَما سنَوْيِة ُهَدْيِة ِإُهَدائُهَما. ِلُلَمَستشِفى َوَّمَراَجْعتَما اِلصحي َوضْعُهَما .َّمتاِبْعِة ِلُلَمَستشِفى َوَّمَراَجْعتَما اِلصحي َوضْعُهَما َّمتاِبْعِة. َصيِفا اِلَسِفَر َفي ْحاَجاَتُهَما َوَتُلُبيِة اِلشُهَر َفي َّمَرة َوِلَو اِلُبيت ْخاَرج .َتَرَوْيحُهَما َصيِفا اِلَسِفَر َفي ْحاَجاَتُهَما َوَتُلُبيِة اِلشُهَر َفي َّمَرة َوِلَو اِلُبيت ْخاَرج َتَرَوْيحُهَما . ِعنُهَما . اِلصَدَقِة ِعنُهَما اِلصَدَقِة
اِلنجاَح اِلنجاَح دَرَجِة Passing MarkPassing Mark ((7/107/10 ) )دَرَجِة