strengthening the referral services in tanzania mrose
TRANSCRIPT

Strengthening the link between VIA/Cryotherapy
and referral services in Tanzania
Mary Rose Giattas MD,MPH
CECAP TA Jhpiego, Tanzania
Jhpiego/MOHSW collaboration

Presentation Framework
Overview of the CECAP program in Tanzania
Rationale for strengthening the link between
VIA/Cryotherapy and referral services
Experience on the referral strengthening in three
Regions in Tanzania
Lessons learnt
Conclusion and recommendation
2

Rationale for Supporting CECAP Services in Tanzania
Trend at Ocean Road Cancer Institute 2006 - 2011
Type of Cancer 2006 2007 2008 2009 2010 2011
Cervical cancer 955 1006 1288 1374 1510 1881
Kaposi sarcoma 295 404 418 447 681 814
Breast cancer 244 245 275 322 386 526
Esophageal
cancer 181 256 282 307 380 511
Head and neck 155 206 244 272 289 361
Lymphomas 201 199 226 245 186 269
Leukemias 46 78 87 103 142 261
Urinary bladder 46 88 87 98 109 153
Skin cancer 40 108 111 123 129 141
Eye cancers 46 76 80 95 84 119
Others 598 472 382 390 299 208
TOTAL 2807 3138 3480 3776 4195 5224

National CECAP and Control Program
Reproductive and Child Health Section (RCHS)
Ag; Director-RCHS
Reproductive Health Cancer Unit
Collaborate with Partners
RHCa-Coordinator
Regional Health Management Team
[RRCHCO]
Council Health Management Team
[DRCHCO]
Health
Facilities
> 120 CCS
11 LEEP
RC
1 Cancer
Centre

Jhpiego/MOHSW CECAP Program
USAID funded
Duration: 2010-2013
The project has been part
of the grander MAISHA
program (Mothers and
Infants, Safe, Healthy and
Alive)
Geographic focus: four
Regions
5

In collaboration with the Ministry of Health
Laying the ground work
National cervical cancer service delivery guidelines
Training resource package
IEC materials (in collaboration with IMA World/ICAP)
HMIS tools- client registers, monthly summary forms and
now discussion of introducing CECAP in the DHIS
CECAP advocacy package
Support partners (GFH,ICAP,EGPAF,MST,PSI,UMATI) in
training/supervision (added > 70 sites & TOT)
Technical input-National Strategic Plan (WHO/Merck)
6

7
• Integration
• Breast Cancer
Screening &
PITC
• Facility &
outreach
Health
Centre District
Hospital Regional
Hospital
VIA ,Cryo ,LEEP,
Biopsy VIA, Cryo,Biopsy
Service Delivery Model
1.Advocacy-buy in /ownership
2.Site Assessment
3.Equipments and supplies
4.Capacity building-providers/managers
5.Community outreach +education
6.Supportive supervision
7.Strengthen referrals / CECAP +CTC
linkage
8.Monitoring System
VIA, Cryo

VIA/Cryo service delivery and referrals
VIA (RCH,OPD,HIV Clinic,GYN OPD)
30-50 yrs & HIV Positive of any age (routine/designated days)
Negative Positive
Follow up 3 years
(HIV-)
Follow up 1 year
( HIV+)
Treat Immediately
Cryotherapy
Refer/Treat
with LEEP
Repeat VIA after
1 year
Suspect
Cancer
Refer

Program Coverage- 21 sites April 2010 – June 2013
9
4 Regions ; Morogoro (9) , Iringa (6), Njombe (5)
&DSM (1)
• 21 sites-phased approach; o April 2010- 3 sites
o April 2011-7 sites
o April 2012-5 sites + 2 LEEP
referral sites
o Mar-April 2013-6 sites
(Include MNH)
o August 2013 -1 LEEP referral
site (MNH)
• All sites offer VIA/Cryotherapy
• 3 Hospitals offer VIA, Cryo &
LEEP services
Iringa
Morogoro
Njombe
DSM
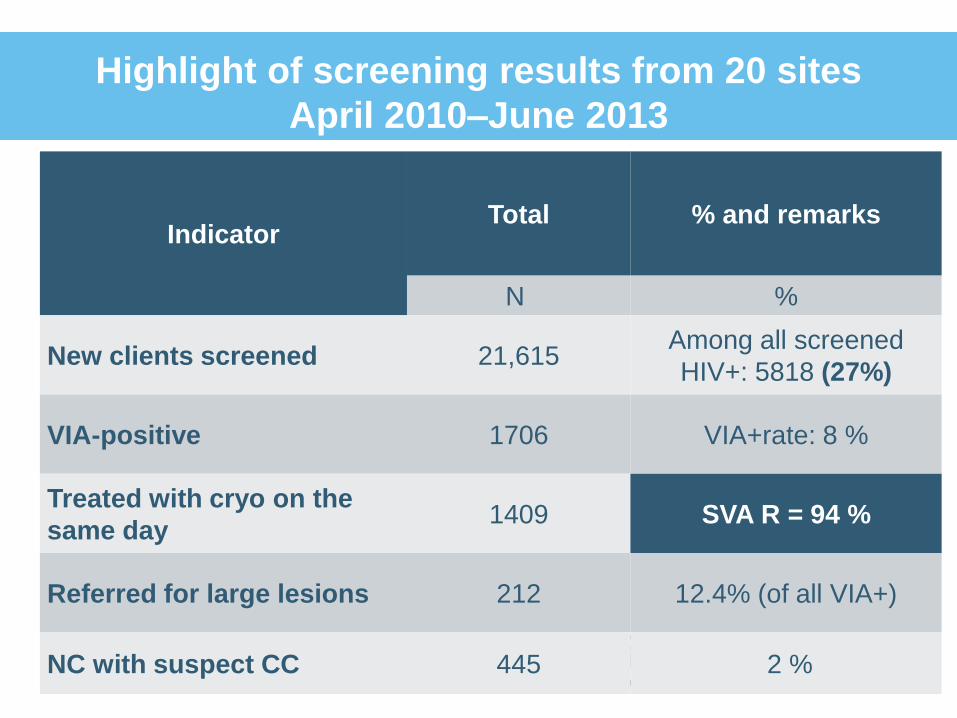
Highlight of screening results from 20 sites
April 2010–June 2013
10
Indicator Total % and remarks
N %
New clients screened 21,615 Among all screened
HIV+: 5818 (27%)
VIA-positive 1706 VIA+rate: 8 %
Treated with cryo on the
same day 1409 SVA R = 94 %
Referred for large lesions 212 12.4% (of all VIA+)
NC with suspect CC 445 2 %

When screening !!
11

Rationale for strengthening the linkage
Implement -comprehensive care /close the loop
High referrals of large lesion cases
Linkage with HIV care services-increased number
of referrals for large lesions
High referrals of suspect cervical cancer cases from
the district level facilities
Women who were referred for LEEP/high level of
care -difficult to ascertain their outcome
Lack of skilled LEEP service providers
12

What have we done to improve ?
Build Regional Capacity :
Site strengthening: provided- 3 LEEP machine/supplies
Trained service providers in three regional health facilities to offer
LEEP services (AMO,MD & Specialists)
o April 2012 (Two Facilities)
o August 2013 (One Facility)
Trained national LEEP trainers to support the MOHSW in
scaling up/supportive supervision
Established a system for biopsy processing with Hfacility
Support the cost of biopsy processing (LEEP/suspect cancer)
Build –monitoring system to track the referral cases &
provide feedback (referral log form/ documentation/
reporting)
13

LEEP Training and Site Monitoring
14

What else did we do to strengthen the
referral services ?
Provided cervical punch biopsies forceps to
District/Regional level facilities
On job training- how to take tissue biopsy from the cervix
Provide airtime to service providers to assist tracking the
referral cases
Support transportation cost of women to the referral site
Identified a focal person at Cancer Centre to support
cervical cancer referral cases
Ensure continuous availability of supplies
Conduct regular review meetings to monitor progress
Conduct quarterly supportive supervision
15

Outcome of referral service strengthening
16
45% (n=96))
0.4% (n=1)
54% (n=115)
212 LL cases identified since 2010 – June 2013 LEEP services started April, 2012
Treated with LEEP
Deceased
Lost to follow up

Results of LEEP Service Delivery
INDICATOR REGION HEALTH
FACILITY TOTAL
Number of clients
treated with LEEP
April 2012- June
2013
Morogoro Morogoro RH 40
Mafiga HC 4
Iringa Iringa RH 52
Dar Muhimbili* Started Aug 13
TOTAL
96
Number of HIV+
clients treated with
LEEP
Morogoro Morogoro RH 29
Iringa Iringa RH 38
Dar Muhimbili* Started Aug 13
TOTAL 67 (70%)
17

Before and after LEEP service initiation
2010 3 VIA/Cryo only
sites
Refer LL for LEEP-other
Regions
Lost to follow up/feedback +
tracking
2012 Established LEEP
services in two sites (Regional Level)
No need of travelling to other Regions for
LEEP services
2013 21 VIA/Cryo sites
Established the third referral LEEP site
>90% of women seen past 1 year diagnosed
with LL were treated with LEEP
18

Outcome of referral service strengthening
Improved referral system/ travel hours for patients
Improve linkage with pathology services-biopsy
results are received within two-three weeks
Large Lesion referral cases receive treatment (from
April 2012)
Cervical cancer cases are referred to cancer center
with confirmed diagnosis
Increased number of cancer cases treated with
radiotherapy
Improved tracking and feedback mechanism
19

Lessons Learnt
20
Where the specimen will
be processed /pathologist
The cost of biopsy
processing
Budget ??
Strong monitoring
system assist in
tracking the referral
cases
Collaboration/engaging
the MOHSW partners

Lessons Learnt
21
Linking VIA/Cryotherapy and referral services can be done !
Assess, Plan, Start small, Learn, Expand, Don’t Despair !!
Strong f/up skills and commitment - key to success !!

Challenges
Distance-referring facility and receiving end
Work overload for service providers in tracking the referral
cases
Tracking the referral cases- wrong mobile numbers/not
reachable/shift to another village
Cost:
Biopsy processing
LEEP service establishment
Transportation –referral cases
Increase in early cacx cases ..treatment ?!
Limited resource- implement based on existing circumstance
22

23
Key Points and Recommendations
Education:
community, providers,
planners/policy
makers
Equipment, supplies
Logistics
Government Ownership
Budget & Sustainability
Efficient M and E system Follow-up/tracking
Training- hands
on skills ?
Supervision
Collaboration
Strengthen
linkage;
Cancer Care
Centre
Pathology Lab