stretch reflex oscillations and essential tremorjnnp.bmj.com/content/jnnp/50/6/691.full.pdf ·...
TRANSCRIPT

Journal of Neurology, Neurosurgery, and Psychiatry 1987;50:691-698
Stretch reflex oscillations and essential tremorRODGER J ELBLE, CONSTANCE HIGGINS, CHARLES J MOODY
From the Department ofMedicine, Division ofNeurology, Southern Illinois University School ofMedicine,Springfield, Illinois, USA
SUMMARY Using a computer-controlled torque motor and manipulandum, 50 ms torque pulsesand 70 second trains of binary pseudorandom torque disturbances were applied to the wrists of 10adult controls and 22 patients with essential tremor in order to study the interaction betweenmechanically-induced stretch-reflex oscillations and essential tremor. These two oscillations wereseparated by applying inertial and spring loads to the wrist. There was no evidence of increased orunstable stretch-reflex activity in the essential tremor patients, and stretch-reflex latencies did notcorrelate with the frequency of essential tremor. Essential tremor and mechanically-induced stretch-reflex oscillations are separate phenomena capable of complex interaction.
The pathophysiological role of the stretch reflex inessential tremor remains unclear. Lee and Stein' haveshown that brief mechanical wrist disturbances pro-duce variable resetting of the essential tremor rhythm,thus proving that the essential tremor oscillatorreceives peripheral sensory feedback. However,Marsden et al2 applied sinusoidal torque disturbancesto the fingers of essential tremor patients and foundthat essential tremor could not be entrained at fre-quencies differing by only [ 0 Hz from the spontane-ous tremor frequency. This failure to entrain essentialtremor reduces the importance of the stretch reflex intremor genesis and supports the notion of a centraloscillator mechanism.
Mechanical perturbations normally producedamped finger and wrist oscillations which are adirect result of the underdamped mechanical proper-ties of these joints and controlling musculature.3-SThese oscillations are detected by peripheral sensoryafferents and may thus induce reflex-evoked modu-lation of motor unit activity.56 This normalmechanical-reflex oscillation is expected to interactwith essential tremor, and depending upon thestrength of this interaction, one oscillation mightgreatly modify or entrain the other.7 8 Therefore, toidentify potential abnormalities in the mechanical-reflex system, one should first try to separate the
Address for reprint requests: Dr R Elble, Department of Medicine,Southern Illinois University School of Medicine, P.O. Box 3926,Springfield, Illinois 62708, USA
Received 5 September 1986 and in revised form 16 November 1986.Accepted 22 November 1986
mechanical-reflex and essential tremor oscillationsand then study the nature of their interaction. Sepa-ration of these two oscillations is possible because thefrequency of essential tremor is not significantlyaltered by external spring and inertial loads while thefrequency of the mechanical-reflex oscillation ischanged in a manner predicted by second-ordermechanics.9 50 Experiments of this type are nowdescribed.
Methods
Twenty-two patients with essential tremor and 10 age-matched healthy adults (ages 25-70 yr) were studied aftersigning informed consent. All subjects were selected from alarger population of patients and controls that participatedin a recently published companion study comparing phys-iological and essential tremor.9 The controls were equallydivided into two groups: those with and those without prom-inent 8- to 12-Hz tremor components. The patients hadtremor ranging from mild to severe and were free of medica-tions known to affect tremor. Caffeinated beverages andtobacco were prohibited on the days of study. To avoidfatigue, the following studies were conducted in two experi-mental sessions lasting approximately 2 hours each.
Bipolar forearm electromyograms (EMGs) were recordedsimultaneously from extensor and flexor muscles with 0-8 cmskin electrodes positioned longitudinally over the muscle,approximately 2 cm apart. Recordings were made from theextensor carpi radialis brevis, extensor digitorum communis,flexors carpi radialis and ulnaris, and palmaris longus.The right hand, with fingers fully extended, was strapped
to a plastic manipulandum attached directly to the shaft of aDC torque motor (Mavilor MT 300). The motor was moun-ted on a steel truss which also supported and restrained thehorizontally positioned forearm. This apparatus thusrestricted wrist movement to extension and flexion in the
691
by copyright. on 29 June 2018 by guest. P
rotectedhttp://jnnp.bm
j.com/
J Neurol N
eurosurg Psychiatry: first published as 10.1136/jnnp.50.6.691 on 1 June 1987. D
ownloaded from

692
horizontal plane. The combined inertia of the manipu-landum and torque motor drive shaft was 0-0024 kg m2. Thisis roughly equivalent to placing 240 g on the horizontallyextended hand as described in our companion study.9 Themotor was driven by a servo amplifier which was controlledby a Commodore VIC 20 computer and digital-to-analogconverter. Wrist angle was measured with a precision poten-tiometer attached directly to the motor shaft. Accelerationwas recorded using a miniature accelerometer attached tothe manipulandum. The wrist angle and acceleration signalswere high-pass filtered to remove DC content.
In one set of experiments, a series of 70 50 ms torquepulses was applied to the wrist. The direction (extension ver-sus flexion) of these perturbations was randomly variedusing the VIC 20. The interval between pulses varied ran-domly between 2 and 12 seconds, and the torque pulseamplitudes were systematically varied from 0 25 to 4 0 Nm.When comparing the amplitudes of our torque per-turbations with those of other authors (such as Lee andStein'), one must consider that a motor produces a torquewhich is attenuated by the manipulandum and mechanicalload, and the actual torque delivered to the wrist is thereforeconsiderably less. For example, Lee and Stein' reported theuse of 3-6 Nm perturbations but did not specify the inertia oftheir motor and manipulandum. In our experiments, torquedisturbances greater than 3 0 Nm were intolerable to all butour strongest patients and were used only during spring orinertial loading (see below). We therefore suspect that theinertia of our manipulandum was considerably less than thatof Lee and Stein. Our torque disturbances produced meanwrist excursions as great as ± 300, and to prevent injury,mechanical stops were us-' to prevent wrist excursionsgreater than + 50°. In all of these experiments, the torqueamplitude was systematically increased to the limit toleratedby each subject, but for most subjects, 0 75 to 1 5 Nm per-turbations produced the most consistent mechanical-reflexresponse in the absence of additional loads.
Mild essential tremor was frequently more evident in thefingers than in the entire hand. Therefore, five controls andfive mild essential tremor patients were also studied byapplying torque pulse disturbances to the right third meta-carpophalangeal (MP) joint. A much smaller manipu-landum (inertia 0 0004 kg m2) was attached to the extendedthird digit, and wrist movement was restricted by the steeltruss. This apparatus was frequently more suitable forstudying the effects of mechanical perturbations on mildessential tremor and the 8 to 12 Hz component of physio-logical tremor, as recorded from the extensor digitorumcommunis.
In a second set of experiments, a continuous 70 secondtrain of pseudorandom extension and flexion torque stepswas delivered to the wrist as described by Dufresne et al."1This torque train was structured to produce a uniform forc-ing from 0 to 50 Hz, the frequency range of physiologicalinterest. The frequency spectrum of this forcing was there-fore statistically flat. The torque train amplitude was system-atically varied from 0-25 to 4 0 Nm, but amplitudes greaterthan 1 0 Nm were too strong unless applied during externalloading.
During all perturbation experiments, the subjects weretold to stiffen their wrist (or metacarpophalangeal joint) inthe neutral position such that the joint returned passively tothis angle following the perturbations. Accuracy of joint
Elbke, Higgins, Moodyangle was not emphasised, and the subjects were specificallyinstructed not to react "voluntarily". After a few practiceruns, each subject quickly found the minimum muscle acti-vation required for approximate return ofjoint angle to thestarting position. Thus, every effort was made to measurepurely passive reflex responses.4 11Each subject underwent several trials of random torque
pulses and pseudorandom torque trains. These trials wereperformed with and without spring and inertial loadsapplied to the wrist. Inertial loads of 0 0045 and 0 0090 kgm2 were added by attaching 450 and 900 g respectively to themanipulandum. Spring loads were simulated by runningfeedback from the precision potentiometer to the motorservo amplifier. The natural frequency of the perturbation-induced wrist oscillations was directly proportional to thesquare root of the manipulandum stiffness (that is positionfeedback gain) and inversely proportional to the square rootof the inertial load.9 10
Wrist angle, manipulandum acceleration and forearmEMGs were recorded simultaneously on an 8-channel instru-ment tape recorder. A series of code pulses, produced by theVIC 20, was also recorded and provided a permanent recordof the precise timing and direction (extension versus flexion)of the torque perturbations. Prior to subsequent computeranalysis, the EMG signals were fullwave rectified and low-pass filtered (-3 db at 30 Hz) to produce the "integrated"(demodulated) EMG.9 12The integrated EMG, wrist angle, and acceleration data
acquired in the torque pulse experiments were analysed in thetime domain by the methods ofcomputed average transients(fig 1).13 Using a PDP 11/23 computer, thirty 1 5-secondepochs of these signals were simultaneously sampled, time-locked to the perturbations. The sampling of each epochbegan 0 3 seconds prior to each perturbation. The averagewrist angle and EMG response to perturbation were therebycomputed. Computer software was developed which allowedus to average these same data epochs on the essential tremorEMG burst preceding each perturbation and on any tremorburst following the perturbation. All perturbations wereapplied randomly with respect to the tremor cycle.
Short and medium latency reflex responses (Ml and M2 ofLee and Tatton14) were obtained from the averaged inte-grated EMG responses to torque pulse perturbations with noexternal loading. The amplitudes of Ml and M2 (relative tothe background EMG) were divided by the average back-ground EMG level to produce "normalised" response ampli-tudes that could be compared across subjects. Ml and M2onset and peak latencies were also measured. We found thatreproducible reflex responses were obtained from all subjectswith perturbations of 0 75 to 1 5 Nm and that stronger per-turbations did not alter reflex amplitude or latency. Thereported Ml and M2 values were obtained with the optimumperturbation strength (0 75, 1 0, or 1-5 Nm) for each subject.Ml and M2 amplitude and latency values did not differamong the muscles studied, and we therefore averaged ourMl and M2 values to obtain the generic values reported inthis paper (mean + SD). Reflex latency and amplitude val-ues for patients and controls were compared using bothStudent's t test and Mann-Whitney rank-sum techniques.Similarly, both Pearson and Spearman correlation methodswere used to look for relationships between (1) essentialtremor frequency and reflex latencies and (2) tremor andreflex amplitudes. The null hypothesis (no difference or no
by copyright. on 29 June 2018 by guest. P
rotectedhttp://jnnp.bm
j.com/
J Neurol N
eurosurg Psychiatry: first published as 10.1136/jnnp.50.6.691 on 1 June 1987. D
ownloaded from
Stretch reflex oscillations and essential tremor
Time domain analysis50ms
. . I
Torque pulseperturbation
Freauencv domain_ , _ w_ _-- _
Neuromuscularsystemand load
System response
analYsis
UL. UU UUL System responsePseudorandom torqueperturbation
Computedaverage _
Notransient V tanalyiAveragetransient
Spectral(Fourier)analysis J.LK*
fn HzFrequencyspectrum
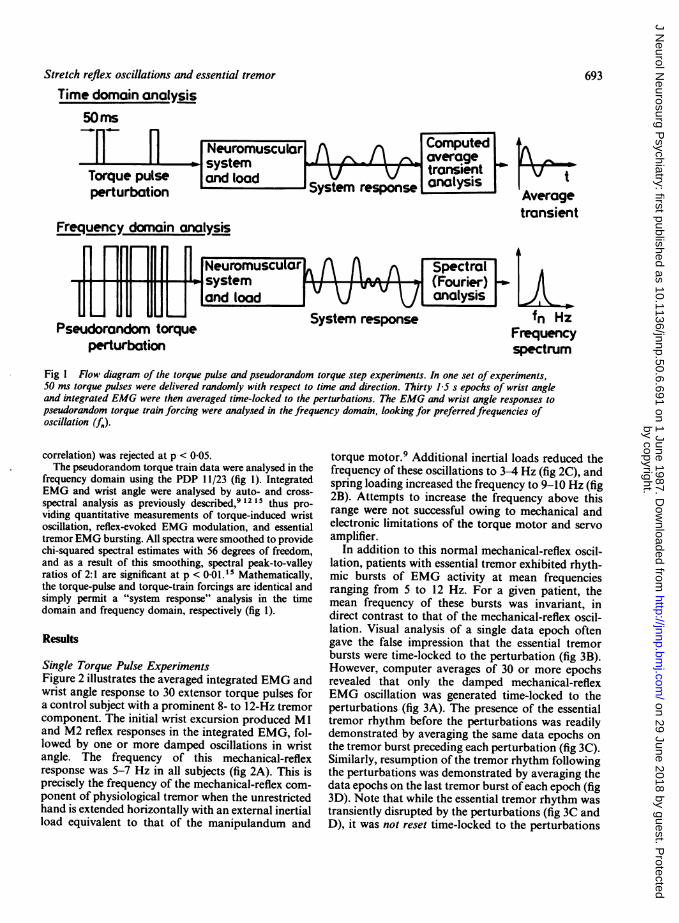
Fig I Flow diagram of the torque pulse and pseudorandom torque step experiments. In one set of experiments,50 ms torque pulses were delivered randomly with respect to time and direction. Thirty 15 s epochs of wrist angleand integrated EMG were then averaged time-locked to the perturbations. The EMG and wrist angle responses topseudorandom torque train forcing were analysed in the frequency domain, looking for preferred frequencies ofoscillation (fe).
correlation) was rejected at p < 0-05.The pseudorandom torque train data were analysed in the
frequency domain using the PDP 11/23 (fig 1). IntegratedEMG and wrist angle were analysed by auto- and cross-spectral analysis as previously described,9 12 15 thus pro-viding quantitative measurements of torque-induced wristoscillation, reflex-evoked EMG modulation, and essentialtremor EMG bursting. All spectra were smoothed to providechi-squared spectral estimates with 56 degrees of freedom,and as a result of this smoothing, spectral peak-to-valleyratios of 2:1 are significant at p < 0.01.15 Mathematically,the torque-pulse and torque-train forcings are identical andsimply permit a "system response" analysis in the timedomain and frequency domain, respectively (fig 1).
Results
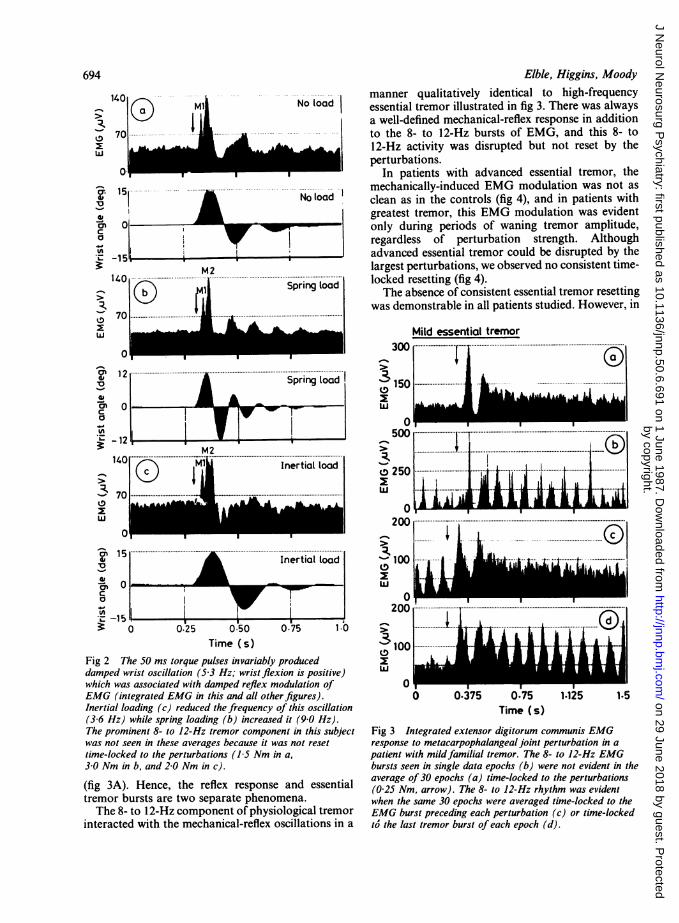
Single Torque Pulse ExperimentsFigure 2 illustrates the averaged integrated EMG andwrist angle response to 30 extensor torque pulses fora control subject with a prominent 8- to 12-Hz tremorcomponent. The initial wrist excursion produced Mland M2 reflex responses in the integrated EMG, fol-lowed by one or more damped oscillations in wristangle. The frequency of this mechanical-reflexresponse was 5-7 Hz in all subjects (fig 2A). This isprecisely the frequency of the mechanical-reflex com-ponent of physiological tremor when the unrestrictedhand is extended horizontally with an external inertialload equivalent to that of the manipulandum and
torque motor.9 Additional inertial loads reduced thefrequency of these oscillations to 3-4 Hz (fig 2C), andspring loading increased the frequency to 9-10 Hz (fig2B). Attempts to increase the frequency above thisrange were not successful owing to mechanical andelectronic limitations of the torque motor and servoamplifier.
In addition to this normal mechanical-reflex oscil-lation, patients with essential tremor exhibited rhyth-mic bursts of EMG activity at mean frequenciesranging from 5 to 12 Hz. For a given patient, themean frequency of these bursts was invariant, indirect contrast to that of the mechanical-reflex oscil-lation. Visual analysis of a single data epoch oftengave the false impression that the essential tremorbursts were time-locked to the perturbation (fig 3B).However, computer averages of 30 or more epochsrevealed that only the damped mechanical-reflexEMG oscillation was generated time-locked to theperturbations (fig 3A). The presence of the essentialtremor rhythm before the perturbations was readilydemonstrated by averaging the same data epochs onthe tremor burst preceding each perturbation (fig 3C).Similarly, resumption of the tremor rhythm followingthe perturbations was demonstrated by averaging thedata epochs on the last tremor burst of each epoch (fig3D). Note that while the essential tremor rhythm wastransiently disrupted by the perturbations (fig 3C andD), it was not reset time-locked to the perturbations
693
a I - I
by copyright. on 29 June 2018 by guest. P
rotectedhttp://jnnp.bm
j.com/
J Neurol N
eurosurg Psychiatry: first published as 10.1136/jnnp.50.6.691 on 1 June 1987. D
ownloaded from
140 M2 ... .....................
(i) :l| ~ ~~~Spring toad
12 ...................... .................................................Spring load
-12tM2
140 E( Mi i Inertial load
0I - I I
15 ~ ^;Inertial load
0
-150 0.25 0.50 0.75
Elble, Higgins, Moody
manner qualitatively identical to high-frequencyessential tremor illustrated in fig 3. There was alwaysa well-defined mechanical-reflex response in additionto the 8- to 12-Hz bursts of EMG, and this 8- to12-Hz activity was disrupted but not reset by theperturbations.
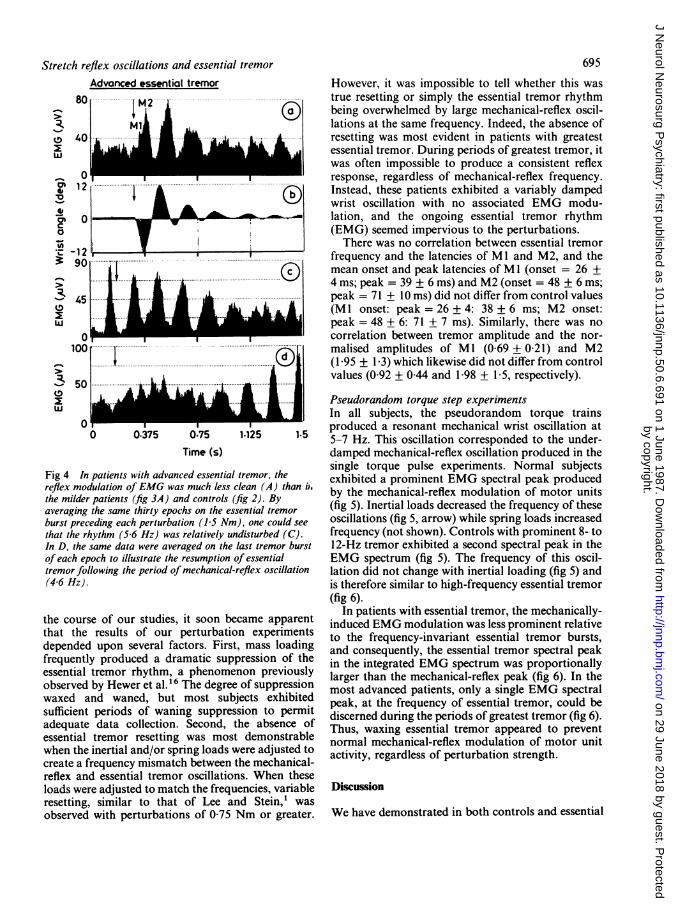
In patients with advanced essential tremor, themechanically-induced EMG modulation was not asclean as in the controls (fig 4), and in patients withgreatest tremor, this EMG modulation was evidentonly during periods of waning tremor amplitude,regardless of perturbation strength. Althoughadvanced essential tremor could be disrupted by thelargest perturbations, we observed no consistent time-locked resetting (fig 4).The absence of consistent essential tremor resetting
was demonstrable in all patients studied. However, in
Mild essential tremor
1.0Time (s)
Fig 2 The 50 ms torque pulses invariably produceddamped wrist oscillation (5 3 Hz; wrist flexion is positive)which was associated with damped reflex modulation ofEMG (integrated EMG in this and all other figures).Inertial loading (c) reduced the frequency of this oscillation(3 6 Hz) while spring loading (b) increased it (9 0 Hz).The prominent 8- to 12-Hz tremor component in this subjectwas not seen in these averages because it was not resettime-locked to the perturbations (15 Nm in a,3 0 Nm in b, and 2-0 Nm in c).
(fig 3A). Hence, the reflex response and essentialtremor bursts are two separate phenomena.The 8- to 12-Hz component of physiological tremor
interacted with the mechanical-reflex oscillations in a
"k100w
0
0....... 1DI
Time (s)
Fig 3 Integrated extensor digitorum communis EMGresponse to metacarpophalangeal joint perturbation in apatient with mildfamilial tremor. The 8- to 12-Hz EMGbursts seen in single data epochs (b) were not evident in theaverage of 30 epochs (a) time-locked to the perturbations(0 25 Nm, arrow). The 8- to 12-Hz rhythm was evidentwhen the same 30 epochs were averaged time-locked to theEMG burst preceding each perturbation (c) or time-lockedto' the last tremor burst of each epoch (d).
694
3x
w
U.0
CJca
-4-
._
W
.-
3._
3
z
w
l00
3:
w
a}
a'1-C.0
U'.
I
I I
by copyright. on 29 June 2018 by guest. P
rotectedhttp://jnnp.bm
j.com/
J Neurol N
eurosurg Psychiatry: first published as 10.1136/jnnp.50.6.691 on 1 June 1987. D
ownloaded from
Stretch reflex oscillations and essential tremorAdvanced essential tremor
1
0 40
LUkll.j --k .,-
Ob
1-opV
v6C0
3:-
L.
3LU
0 0.375 0-75 1.125 1-5Time (s)
Fig 4 In patients with advanced essential tremor, thereflex modulation ofEMG was much less clean (A) than i.the milder patients (fig 3A) and controls (fig 2). Byaveraging the same thirty epochs on the essential tremorburst preceding each perturbation (15 Nm), one could seethat the rhythm (5 6 Hz) was relatively undisturbed (C).In D, the same data were averaged on the last tremor burstof each epoch to illustrate the resumption of essentialtremor following the period of mechanical-reflex oscillation(4-6 Hz).
the course of our studies, it soon became apparentthat the results of our perturbation experimentsdepended upon several factors. First, mass loadingfrequently produced a dramatic suppression of theessential tremor rhythm, a phenomenon previouslyobserved by Hewer et al."6 The degree of suppressionwaxed and waned, but most subjects exhibitedsufficient periods of waning suppression to permitadequate data collection. Second, the absence ofessential tremor resetting was most demonstrablewhen the inertial and/or spring loads were adjusted tocreate a frequency mismatch between the mechanical-reflex and essential tremor oscillations. When theseloads were adjusted to match the frequencies, variableresetting, similar to that of Lee and Stein,' wasobserved with perturbations of 0-75 Nm or greater.
695
However, it was impossible to tell whether this wastrue resetting or simply the essential tremor rhythmbeing overwhelmed by large mechanical-reflex oscil-lations at the same frequency. Indeed, the absence ofresetting was most evident in patients with greatestessential tremor. During periods of greatest tremor, itwas often impossible to produce a consistent reflexresponse, regardless of mechanical-reflex frequency.Instead, these patients exhibited a variably dampedwrist oscillation with no associated EMG modu-lation, and the ongoing essential tremor rhythm(EMG) seemed impervious to the perturbations.
There was no correlation between essential tremorfrequency and the latencies of Ml and M2, and themean onset and peak latencies of M1 (onset = 26 +4 ms; peak = 39 + 6 ms) and M2 (onset = 48 + 6 ms;peak = 71 + 10 ms) did not differ from control values(Ml onset: peak = 26 + 4: 38 + 6 ms; M2 onset:peak = 48 + 6: 71 + 7 ms). Similarly, there was nocorrelation between tremor amplitude and the nor-malised amplitudes of MI (0-69 + 0-21) and M2(I 95 + 1 3) which likewise did not differ from controlvalues (0 92 + 0A44 and 1-98 + 15, respectively).
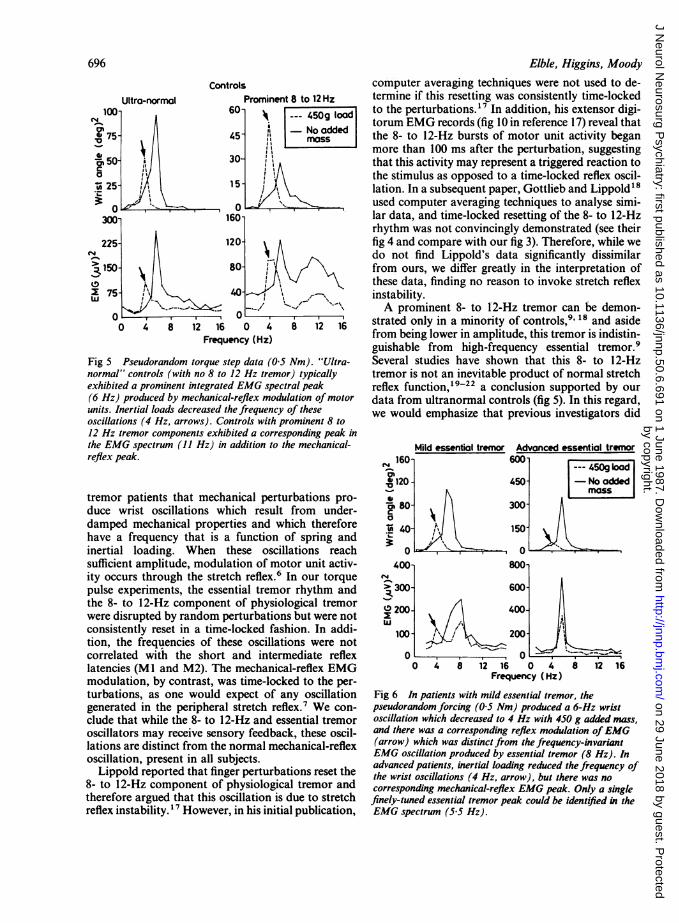
Pseudorandom torque step experimentsIn all subjects, the pseudorandom torque trainsproduced a resonant mechanical wrist oscillation at5-7 Hz. This oscillation corresponded to the under-damped mechanical-reflex oscillation produced in thesingle torque pulse experiments. Normal subjectsexhibited a prominent EMG spectral peak producedby the mechanical-reflex modulation of motor units(fig 5). Inertial loads decreased the frequency of theseoscillations (fig 5, arrow) while spring loads increasedfrequency (not shown). Controls with prominent 8- to12-Hz tremor exhibited a second spectral peak in theEMG spectrum (fig 5). The frequency of this oscil-lation did not change with inertial loading (fig 5) andis therefore similar to high-frequency essential tremor(fig 6).
In patients with essential tremor, the mechanically-induced EMG modulation was less prominent relativeto the frequency-invariant essential tremor bursts,and consequently, the essential tremor spectral peakin the integrated EMG spectrum was proportionallylarger than the mechanical-reflex peak (fig 6). In themost advanced patients, only a single EMG spectralpeak, at the frequency of essential tremor, could bediscerned during the periods of greatest tremor (fig 6).Thus, waxing essential tremor appeared to preventnormal mechanical-reflex modulation of motor unitactivity, regardless of perturbation strength.
Discussion
We have demonstrated in both controls and essential
by copyright. on 29 June 2018 by guest. P
rotectedhttp://jnnp.bm
j.com/
J Neurol N
eurosurg Psychiatry: first published as 10.1136/jnnp.50.6.691 on 1 June 1987. D
ownloaded from
66Elbie, Higgins, Moody
ControlsUltra-normal
OL-
0 4 8 12 16 0 4Frequency (Hz)
Fig 5 Pseudorandom torque step data (05normal" controls (with no 8 to 12 Hz tremorexhibited a prominent integrated EMG specti(6 Hz) produced by mechanical-reflex modulunits. Inertial loads decreased the frequency ioscillations (4 Hz, arrows). Controls with pr12 Hz tremor components exhibited a corresjthe EMG spectrum (11 Hz) in addition to threflex peak.
tremor patients that mechanical pertu,duce wrist oscillations which resultdamped mechanical properties and wi
have a frequency that is a function cinertial loading. When these oscillsufficient amplitude, modulation of molity occurs through the stretch reflex.6 I
pulse experiments, the essential tremorthe 8- to 12-Hz component of physiolwere disrupted by random perturbationsconsistently reset in a time-locked fasbtion, the frequencies of these oscillaticorrelated with the short and internlatencies (Ml and M2). The mechanicamodulation, by contrast, was time-lockturbations, as one would expect of argenerated in the peripheral stretch refl4clude that while the 8- to 12-Hz and essoscillators may receive sensory feedbacllations are distinct from the normal mecoscillation, present in all subjects.Lippold reported that finger perturbal
8- to 12-Hz component of physiologicatherefore argued that this oscillation is (reflex instability. 7 However, in his initia
computer averaging techniques were not used to de-8 to 12 Hz termine if this resetting was consistently time-locked
450g load to the perturbations.'7 In addition, his extensor digi-No odded torum EMG records (fig 10 in reference 17) reveal thatNosadded the 8- to 12-Hz bursts of motor unit activity began
more than 100 ms after the perturbation, suggestingthat this activity may represent a triggered reaction tothe stimulus as opposed to a time-locked reflex oscil-
< lation. In a subsequent paper, Gottlieb and Lippold'8used computer averaging techniques to analyse simi-lar data, and time-locked resetting of the 8- to 12-Hzrhythm was not convincingly demonstrated (see theirfig 4 and compare with our fig 3). Therefore, while wedo not find Lippold's data significantly dissimilarfrom ours, we differ greatly in the interpretation ofthese data, finding no reason to invoke stretch reflexinstability.A prominent 8- to 12-Hz tremor can be demon-
8 12 16 strated only in a minority of controls,9 18 and asidefrom being lower in amplitude, this tremor is indistin-guishable from high-frequency essential tremor.9
Nm). "Ultra- Several studies have shown that this 8- to 12-Hzr) typically tremor is not an inevitable product of normal stretchral peak reflex function, 19-22 a conclusion supported by ourlation of motor data from ultranormal controls (fig 5). In this regard,of these we would emphasize that previous investigators didominent 8 toponding peak inWe mechanical- Mild essential tremor Advanced essential tremor
N 160- 600-
= 120 - 450- -No addedrbations pro- 8 300from under-
U30
iich therefore t A,
Lf spring and 15ations reach 0 0tor unit activ- 400- 800In our torque 4
r rhythm and > 300- 600-
ogical tremor 0 200- 400-s butwerenotlion. In addi- 100o- 200-ons were not ,iediate reflex 0 0l-reflex EMG o 4 8 12 16 0 4 8 12 16ed to the per- Frequency (Hz)ny oscillation Fig 6 In patients with mild essential tremor, theex.7 We con- pseudorandom forcing (05 Nm) produced a 6-Hz wristsential tremor oscillation which decreased to 4 Hz with 450 g added mass,k, these oscil- and there was a corresponding reflex modulation ofEMGh'anical-reflex (arrow) which was distinct from the frequency-invariant
EMG oscillation produced by essential tremor (8 Hz). In
tions reset the advanced patients, inertial loading reduced the frequency ofthe wrist oscillations (4 Hz, arrow), but there was no11 tremor and corresponding mechanical-reflex EMG peak. Only a singledue to stretch finely-tuned essential tremor peak could be identified in theLI publication, EMG spectrum (5 5 Hz).
696
by copyright. on 29 June 2018 by guest. P
rotectedhttp://jnnp.bm
j.com/
J Neurol N
eurosurg Psychiatry: first published as 10.1136/jnnp.50.6.691 on 1 June 1987. D
ownloaded from
Stretch reflex oscillations and essential tremor
not report 8- to 12-Hz oscillations following wrist"6and finger3 perturbations in adult controls. Further-more, most normal subjects exhibit little or no evi-dence of motor unit synchronisation except duringfatigue,9 23 24 and the activated ("enhanced") phys-iological tremor typically seen in fatigue is themechanical-reflex oscillation, not the 8- to 12-Hztremor.6 10 19
Because the frequency of the 8- to 12-Hz and essen-tial tremors is independent of peripheral mechanicalfactors and reflex latencies, a central oscillator prob-ably plays a key mechanistic role. Our study andothers' 2 indicate that the central oscillator(s) res-ponsible for these tremors are coupled to the stretchreflex. The stretch reflex may therefore play a role ingoverning the amplitude of these oscillations, but itdoes not produce the essential tremor rhythm.Furthermore, the interaction between these coupledoscillators may be synergistic or competitive,depending upon the experimental conditions.7-8Basic oscillator theory tells us that this interactionwill depend upon (1) the relative strengths of the twooscillations, (2) the relative frequencies of the twooscillations, and (3) the strength of coupling betweenthe two oscillations.25Our hypothesis ofcoupled stretch reflex and central
oscillators explains the apparent conflicts between thework of Lee and Stein' and Marsden et al.2 In experi-ments very- similar to ours, Lee -and Stein' reportedvariable resetting of advanced essential tremor but didnot separate the mechanical-reflex and essentialtremor oscillations. Strong perturbations to thesemutually-entrained oscillators would be expected toproduce the high degree of time-locked resetting ob-served in their experiments. Similarly, we observedgreatest essential tremor resetting when two condi-tions were met: (1) the mechanical-reflex oscillationwas much larger than the ongoing essential tremorand (2) there was no frequency mismatch between thetwo oscillations. During a frequency mismatch, how-ever, the two oscillations were clearly competitive,with the stronger oscillation tending to disrupt andobscure the other.
Lee and Stein did not find complete resetting in anyof their patients and therefore emphasised that acentral oscillator may play a role in tremor genesis.Such a role is also indicated by the work of Marsdenet al,2 who demonstrated that essential tremor has apreferred frequency and cannot be entrained bymechanically-imposed reflex oscillations at a slightlydifferent frequency. In effect, Marsden et al imposeda frequency mismatch between essential tremor andmechanical-reflex oscillators, thus testing their rela-tive strengths and coupling. Instead of entrainment,they observed predictable beats in the essential tremorrhythm.2 The experiments of Marsden et al2 are
697
analogous to our torque train studies with inertialloading in advanced tremor patients. Resonantmechanical wrist oscillations at frequencies above andbelow the frequency of essential tremor produced noentrainment of essential tremor (fig 6).
Essential tremor and normal mechanical-reflextremor have distinctly different EMG/wrist oscillationamplitude relationships which are consistent with themechanisms we have proposed. The mechanical-reflexwrist oscillation is primarily the result of under-damped limb mechanics, and its EMG modulation isin response to this oscillation rather than its directcause. Unless this oscillation is accentuated by fatigue(increased reflex gain?) or external perturbations,there is little discernible EMG modulation. Con-sequently, mechanical-reflex tremor is usually largerelative to its EMG. By contrast, the wrist tremor ofany central oscillator will be proportionally smallerrelative to its EMG. This is because a central oscillatorproduces tremor directly by rhythmic EMG modu-lation. However, the effect of this modulation is min-imised by the attenuating properties of skeletalmuscle, limb mechanics and external loads. Therefore,prominent essential tremor and 8- to 12-Hz phys-iologic tremor are commonly detectable in the EMGwith little discernible wrist oscillation, precisely theopposite relationship observed for mechanical-reflextremor (figs 5 and 6, and figs 1-3 in reference 9).Tremor research is historically riddled with heated
controversy regarding the relative roles played bystretch-reflex and central oscillators. Because anunderdamped mechanical-reflex system is present ineveryone, the possibility of coupled oscillators mustbe considered in the study of any tremor. Theoreticalstudies by Stein and coworkers7-8 have vividly illus-trated the complexities which may result from suchoscillator interaction, and our study as well as thoseof Lee and Stein' and of Marsden et a12 support therelevance of coupled oscillator theory in any dis-cussion of essential tremor. We would also arguethat the coupled oscillator model applies to themechanical-reflex and 8- to 12-Hz components ofphysiological tremor.
Supported by grants from the National Institute ofNeurological and Communicative Disorders andStroke (ROI-NS20973) and from the American Par-kinson Disease Association.
Presented in part at the thirty-eighth annual meet-ing of the American Academy of Neurology, NewOrleans, LA, and at the fifteenth annual meeting ofthe Society for Neuroscience, Dallas TX.The authors are indebted to James Adelman and
John Holcomb for their technical assistance and toRita Cerar for typing this manuscript.
by copyright. on 29 June 2018 by guest. P
rotectedhttp://jnnp.bm
j.com/
J Neurol N
eurosurg Psychiatry: first published as 10.1136/jnnp.50.6.691 on 1 June 1987. D
ownloaded from
698
References
I Lee RG, Stein RB. Resetting of tremor by mechanicalperturbations: a comparison of essential tremor andparkinsonian tremor. Ann Neurol 1981;10:523-31.
2 Marsden CD, Obeso JA, Rothwell JC. Benign essentialtremor is not a single entity. In: Yahr MD, ed. CurrentConcepts of Parkinson Disease and Related Disorders,Amsterdam: Excerpta Medica, 1981:31-46.
3 Kelso JAS, Holt KG. Exploring a vibratory systemsanalysis of human movement production. J Neuro-physiol 1980;43:1 183-96.
4 Neilson PD, Neilson MD. The role of action reflexes inthe damping of mechanical oscillations. Brain Res1978;142:439-53.
5 Stiles RN. Lightly damped hand oscillations:acceleration-related feedback and system damping. JNeurophysiol 1983;50:327-43.
6 Hagbarth K-E, Young RR. Participation of the stretchreflex in human physiological tremor. Brain1979;102:509-26.
7 Stein RB, Gordon T, Oguztoreli MN, Lee RG. Classi-fying sensory patterns and their effects on locomotionand tremor. Can J Physiol Pharmacol 198 1;59:645-55.
8 Stein RB, Lee RG. Tremor and clonus. In: Brooks V, ed.Handbook of Physiology, Motor Control, Baltimore:Williams and Wilkins, 1981:325-43.
9 Elble RJ. Physiologic and essential tremor. Neurology1986;36:225-3 1.
10 Elble RJ, Randall JE. Mechanistic components ofnormal hand tremor. Electroencephalogr ClinNeurophysiol 1978;44:72-82.
11 Dufresne JR, Soechting JF, Terzuolo CA. Reflex motoroutput to torque pulses in man: identification of short-and long-latency loops with individual feedbackparameters. Neurosci 1979;4:1493-1500.
12 Elble RJ, Randall JE. Motor-unit activity responsible forthe 8- to 12- Hz component of human physiologicalfinger tremor. J Neurophysiol 1976;39:370-83.
Elble, Higgins, Moody13 Glaser EM, Ruchkin DS. Principles of Neurobiologic
Signal Analysis. New York: Academic Press,1976:177-290.
14 Lee RG, Tatton WG. Motor responses to sudden limbdisplacement in primates with specific CNS lesionsand in human patients with motor system disorders.Can J Neurol Sci 1975;2:205-93.
15 Jenkins GM, Watts DG. Spectral Analysis and Its Appli-cations. San Francisco: Holden-Day, 1968:209-57.
16 Hewer RL, Cooper R, Morgan MH. An investigationinto the value of treating intention tremor by weight-ing the affected limb. Brain 1972;95:579-90.
17 Lippold OCJ. Oscillation in the stretch reflex arc and therhythmical 8-12 c/s component of physiologicaltremor. J Physiol (Lond) 1970;206:359-82.
18 Gottlieb S, Lippold OCJ. The 4-6 Hz tremor duringsustained contraction in normal human subjects.J Physiol (Lond) 1983;336:499-509.
19 Stiles RN. Mechanical and neural feedback factors inpostural hand tremor of normal subjects. J Neuro-physiol 1980;44:40-9.
20 Andrews CJ, Burke D, Lance JW. The comparison oftremors in normal, parkinsonian and athetotic man.J Neurol Sci 1973;19:53-61.
21 Brown TIH, Rack PMH, Ross HF. Different types oftremor in the human thumb. J Physiol (Lond)1982;332:1 13-23.
22 Marsden CD, Meadows JC, Lange GW, Watson RS.Effect of deafferentation on human physiologicaltremor. Lancet 1967;2:700-2.
23 Dietz V., Bischofberger E, Witz C, Freund H-J. Cor-relation between the discharges of two simultaneouslyrecorded motor units and physiological tremor. Elec-troencephalogr Clin Neurophysiol 1976;40:97-105.
24 Freund H-J. Motor unit and muscle activity in voluntarymotor control. Physiol Rev 1983;63:387-436.
25 McMahon TA. Muscles, Reflexes, and Locomotion.Princeton, NJ: Princeton University Press,1984:174-80.
by copyright. on 29 June 2018 by guest. P
rotectedhttp://jnnp.bm
j.com/
J Neurol N
eurosurg Psychiatry: first published as 10.1136/jnnp.50.6.691 on 1 June 1987. D
ownloaded from